Evaluating the Predictive Capability of Radiomics Features of Perirenal Fat in Enhanced CT Images for Staging and Grading of UTUC Tumours Using Machine Learning

 , , and
, , and 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Adherence to Guidelines and Ethical Considerations
2.2. Patient Cohort Characteristics
2.3. CT Imaging Protocol
2.4. Image Segmentation
2.5. Feature Extraction and Analysis
2.6. Feature Stability and Selection
2.7. Machine Learning Models and Implementation
- Linear Models: Logistic Regression (LR), Support Vector Classifier (SVC), Quadratic Discriminant Analysis (QDA).
- Ensemble Methods: Random Forest Classifier (RFC), Extra Trees Classifier (ETC), Gradient Boosting Classifier (GBC), LightGBM Classifier (LGBM), CatBoost Classifier, and AdaBoost Classifier.
- Neural Networks: Multilayer Perceptron (MLPClassifier).
- Instance-Based Methods: K-Nearest Neighbours (KNN).
- Tree-Based Methods: Decision Tree Classifier (DTC).
2.8. Statistical Analysis
3. Results
3.1. Segmentation Results
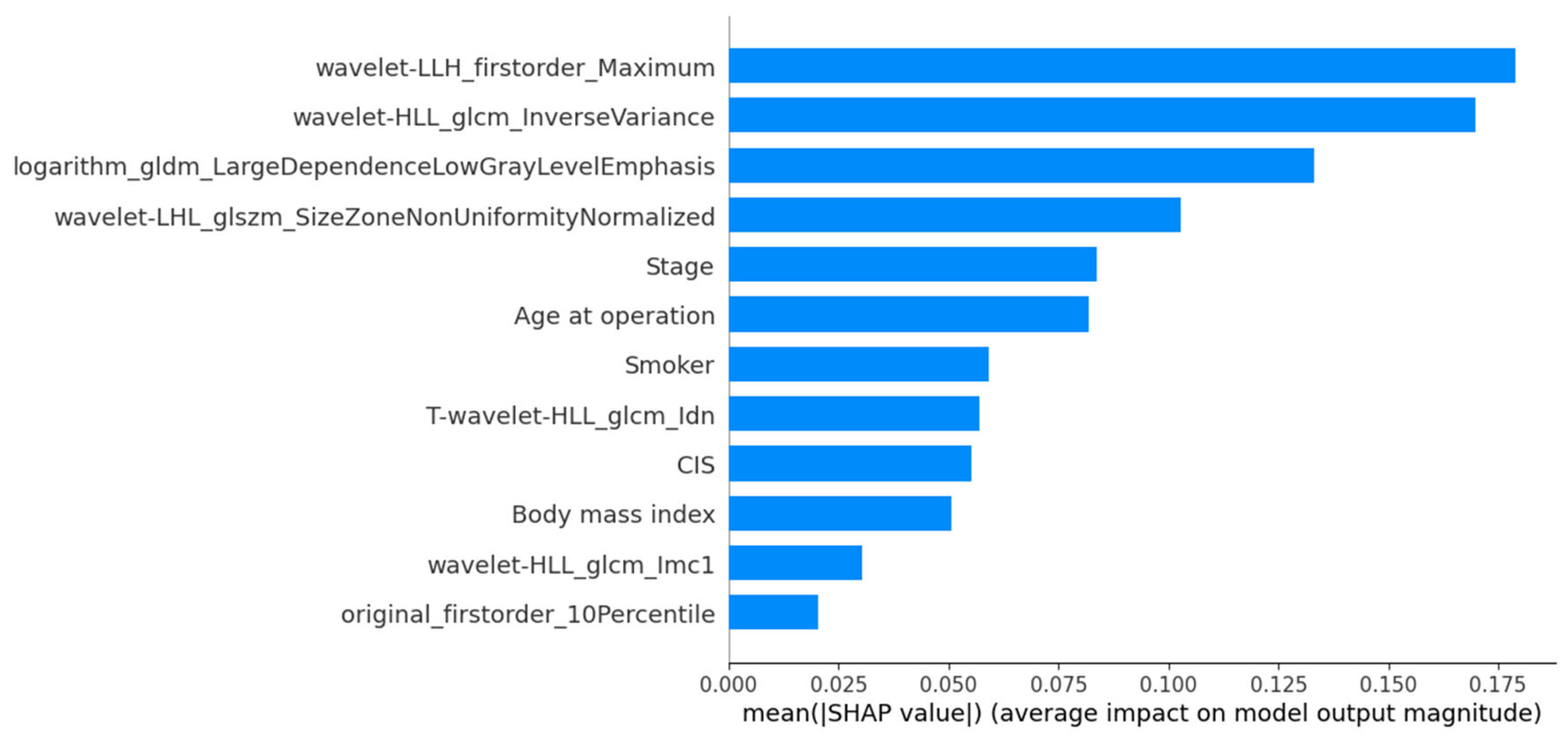
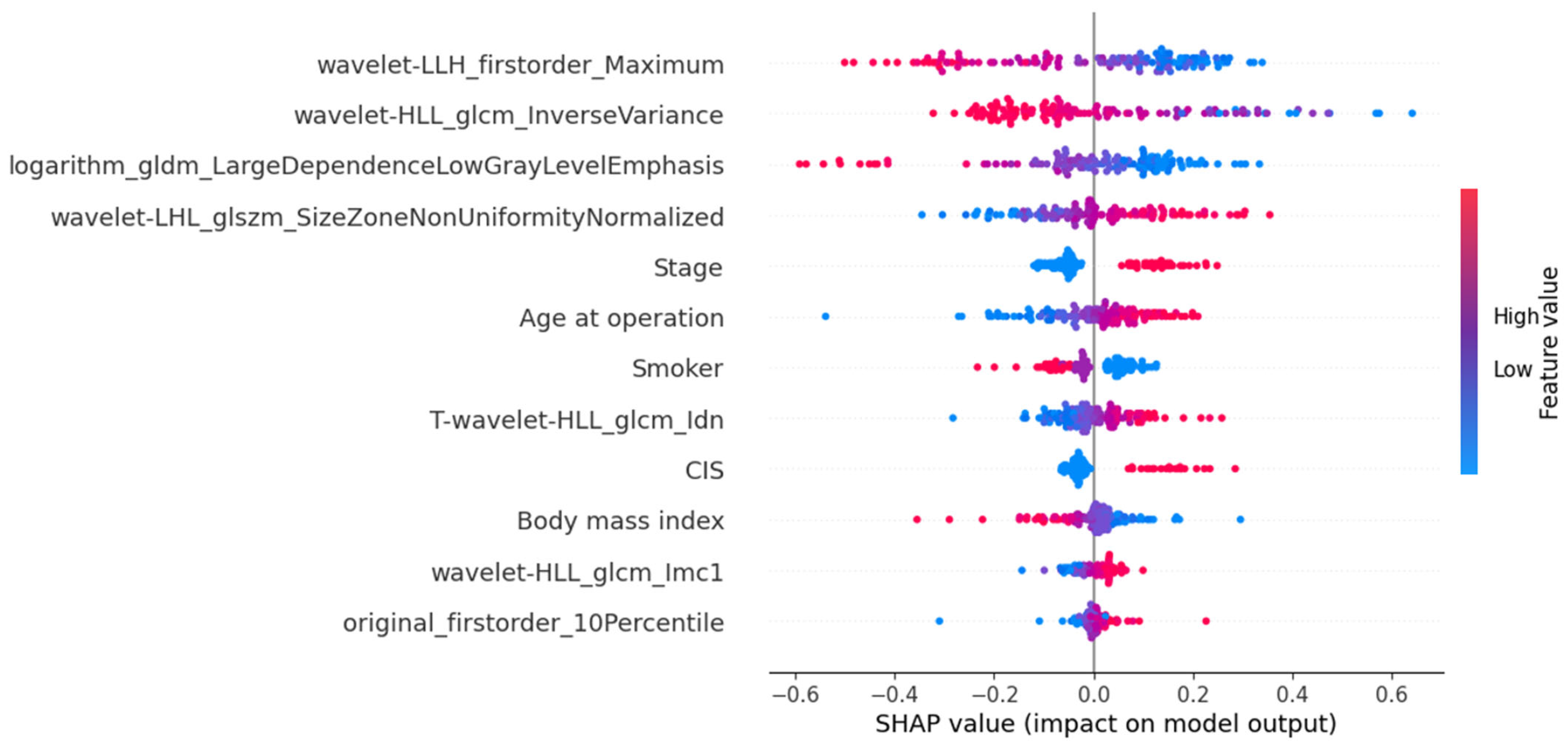
3.2. Radiomic Feature Selection
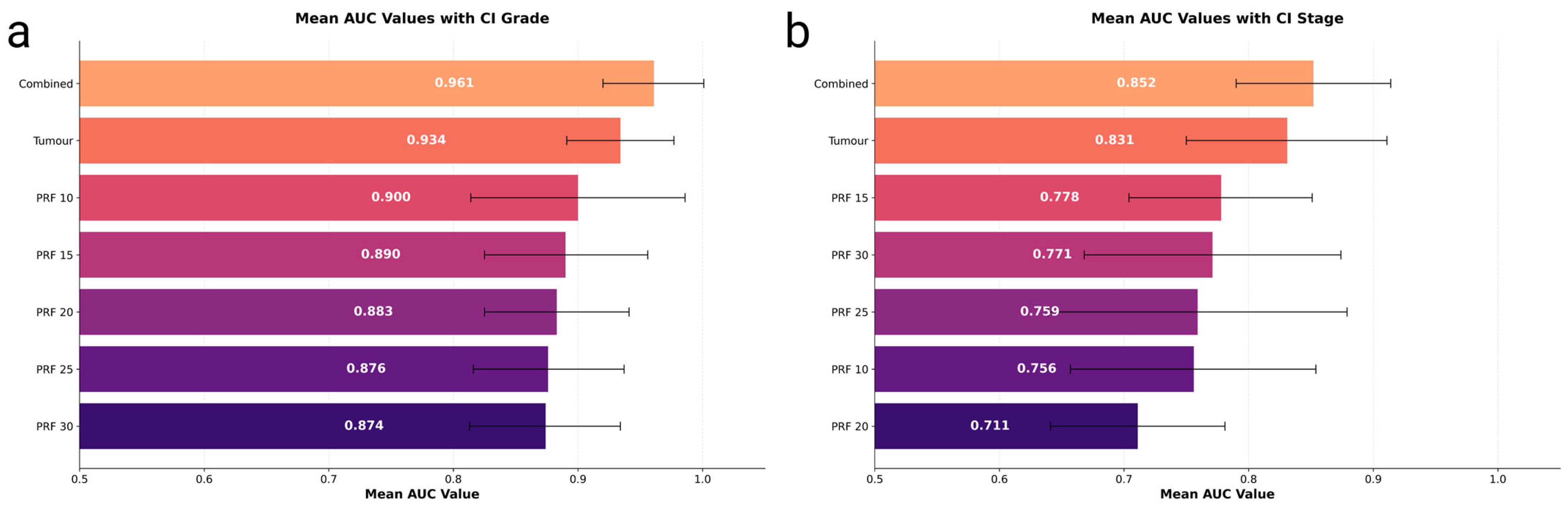
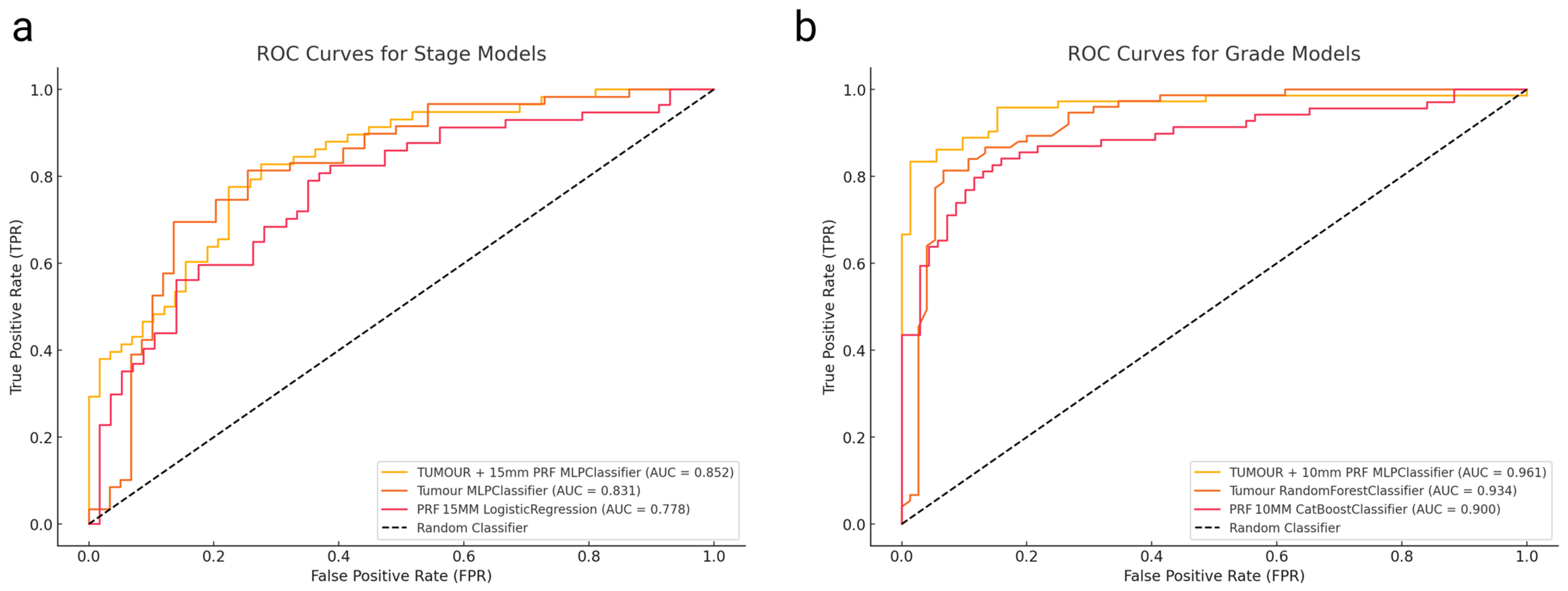
3.3. Model Performance for Tumour Grade Prediction
3.4. Model Performance for Tumour Stage Prediction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2021, 79, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Mbeutcha, A.; Rouprêt, M.; Kamat, A.M.; Karakiewicz, P.I.; Lawrentschuk, N.; Novara, G.; Raman, J.D.; Seitz, C.; Xylinas, E.; Shariat, S.F. Prognostic Factors and Predictive Tools for Upper Tract Urothelial Carcinoma: A Systematic Review. World J. Urol. 2017, 35, 337–353. [Google Scholar] [CrossRef] [PubMed]
- Seisen, T.; Peyronnet, B.; Dominguez-Escrig, J.L.; Bruins, H.M.; Yuan, C.Y.; Babjuk, M.; Böhle, A.; Burger, M.; Compérat, E.M.; Cowan, N.C.; et al. Oncologic Outcomes of Kidney-Sparing Surgery Versus Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: A Systematic Review by the EAU Non-Muscle Invasive Bladder Cancer Guidelines Panel. Eur. Urol. 2016, 70, 1052–1068. [Google Scholar] [CrossRef]
- Leow, J.J.; Orsola, A.; Chang, S.L.; Bellmunt, J. A Contemporary Review of Management and Prognostic Factors of Upper Tract Urothelial Carcinoma. Cancer Treat. Rev. 2015, 41, 310–319. [Google Scholar] [CrossRef]
- Favaretto, R.L.; Shariat, S.F.; Savage, C.; Godoy, G.; Chade, D.C.; Kaag, M.; Bochner, B.H.; Coleman, J.; Dalbagni, G. Combining Imaging and Ureteroscopy Variables in a Preoperative Multivariable Model for Prediction of Muscle-Invasive and Non-Organ Confined Disease in Patients with Upper Tract Urothelial Carcinoma. BJU Int. 2012, 109, 77–82. [Google Scholar] [CrossRef]
- Wojcik, E.M.; Kurtycz, D.F.I.; Rosenthal, D.L. We’ll Always Have Paris The Paris System for Reporting Urinary Cytology 2022. J. Am. Soc. Cytopathol. 2022, 11, 62–66. [Google Scholar] [CrossRef]
- Brimo, F.; Vollmer, R.T.; Case, B.; Aprikian, A.; Kassouf, W.; Auger, M. Accuracy of Urine Cytology and the Significance of an Atypical Category. Am. J. Clin. Pathol. 2009, 132, 785–793. [Google Scholar] [CrossRef]
- Yates, D.R.; Hupertan, V.; Colin, P.; Ouzzane, A.; Descazeaud, A.; Long, J.A.; Pignot, G.; Crouzet, S.; Rozet, F.; Neuzillet, Y.; et al. Cancer-Specific Survival after Radical Nephroureterectomy for Upper Urinary Tract Urothelial Carcinoma: Proposal and Multi-Institutional Validation of a Post-Operative Nomogram. Br. J. Cancer 2012, 106, 1083–1088. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; De Jong, E.E.C.; Van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The Bridge between Medical Imaging and Personalized Medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; Van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting More Information from Medical Images Using Advanced Feature Analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef]
- Ditonno, F.; Franco, A.; Veccia, A.; Bertolo, R.; Wu, Z.; Wang, L.; Abdollah, F.; Finati, M.; Simone, G.; Tuderti, G.; et al. Decisional and Prognostic Impact of Diagnostic Ureteroscopy in High-Risk Upper Tract Urothelial Carcinoma: A Multi-Institutional Collaborative Analysis (ROBUUST Collaborative Group). Urol. Oncol. Semin. Orig. Investig. 2024, 42, 290.e1–290.e9. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Quail, D.F.; Joyce, J.A. Microenvironmental Regulation of Tumor Progression and Metastasis. Nat. Med. 2013, 19, 1423–1437. [Google Scholar] [CrossRef] [PubMed]
- Pottier, C.; Wheatherspoon, A.; Roncarati, P.; Longuespée, R.; Herfs, M.; Duray, A.; Delvenne, P.; Quatresooz, P. The Importance of the Tumor Microenvironment in the Therapeutic Management of Cancer. Expert. Rev. Anticancer Ther. 2015, 15, 943–954. [Google Scholar] [CrossRef]
- Yanagi, M.; Terasaki, M.; Kiriyama, T.; Terasaki, Y.; Akatsuka, J.; Endo, Y.; Nishimura, T.; Shimizu, A.; Kondo, Y. Perirenal Fat Stranding as a Predictor of Disease Progression after Radical Nephroureterectomy for Renal Pelvic Urothelial Carcinoma: A Retrospective Study. Discov. Oncol. 2023, 14, 122. [Google Scholar] [CrossRef]
- Ceyhan, E.; Ileri, F.; Aki, F.T.; Yazici, M.S.; Karcaaltincaba, M.; Ertoy Baydar, D.; Bilen, C.Y. Pathology Associated with Adherent Perirenal Fat and Its Clinical Effect. Int. J. Clin. Pract. 2021, 75, e14518. [Google Scholar] [CrossRef]
- Chung, J.W.; Lee, J.N.; Park, K.M.; Byeon, K.H.; Cheon, H.; Ha, Y.S.; Choi, S.H.; Kim, B.S.; Kim, T.H.; Yoo, E.S.; et al. Prognostic Impact of Perirenal Fat Stranding on Oncologic Outcomes in Ureteral Urothelial Carcinoma. Investig. Clin. Urol. 2021, 62, 23. [Google Scholar] [CrossRef]
- Tsili, A.C.; Goussia, A.C.; Baltogiannis, D.; Astrakas, L.; Sofikitis, N.; Malamou-Mitsi, V.; Argyropoulou, M.I. Perirenal Fat Invasion on Renal Cell Carcinoma: Evaluation with Multidetector Computed Tomography-Multivariate Analysis. J. Comput. Assist. Tomogr. 2013, 37, 450–457. [Google Scholar] [CrossRef]
- Ning, K.; Li, Z.; Liu, H.; Tian, X.; Wang, J.; Wu, Y.; Xiong, L.; Zou, X.; Peng, Y.; Zhou, Z.; et al. Perirenal Fat Thickness Significantly Associated with Prognosis of Metastatic Renal Cell Cancer Patients Receiving Anti-VEGF Therapy. Nutrients 2022, 14, 3388. [Google Scholar] [CrossRef]
- Alqahtani, A.; Bhattacharjee, S.; Almopti, A.; Li, C.; Nabi, G. Radiomics-Based Machine Learning Approach for the Prediction of Grade and Stage in Upper Urinary Tract Urothelial Carcinoma: A Step towards Virtual Biopsy. Int. J. Surg. 2024, 110, 3258–3268. [Google Scholar] [CrossRef]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Cavalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding Tumour Phenotype by Noninvasive Imaging Using a Quantitative Radiomics Approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Ibarrola, R.; Basulto-Martinez, M.; Heinze, A.; Gratzke, C.; Miernik, A. Cancers Radiomics Applications in Renal Tumor Assessment: A Comprehensive Review of the Literature. Cancers 2020, 12, 1387. [Google Scholar] [CrossRef]
- Kocak, B.; Baessler, B.; Bakas, S.; Cuocolo, R.; Fedorov, A.; Maier-Hein, L.; Mercaldo, N.; Müller, H.; Orlhac, F.; Pinto dos Santos, D.; et al. CheckList for EvaluAtion of Radiomics Research (CLEAR): A Step-by-Step Reporting Guideline for Authors and Reviewers Endorsed by ESR and EuSoMII. Insights Imaging 2023, 14, 75. [Google Scholar] [CrossRef]
- Khene, Z.E.; Bensalah, K.; Largent, A.; Shariat, S.; Verhoest, G.; Peyronnet, B.; Acosta, O.; DeCrevoisier, R.; Mathieu, R. Role of Quantitative Computed Tomography Texture Analysis in the Prediction of Adherent Perinephric Fat. World J. Urol. 2018, 36, 1635–1642. [Google Scholar] [CrossRef]
- Gill, T.S.; Varghese, B.A.; Hwang, D.H.; Cen, S.Y.; Aron, M.; Aron, M.; Duddalwar, V.A. Juxtatumoral Perinephric Fat Analysis in Clear Cell Renal Cell Carcinoma. Abdom. Radiol. 2019, 44, 1470–1480. [Google Scholar] [CrossRef]
- Al Mopti, A.; Alqahtani, A.; Alshehri, A.H.D.; Li, C.; Nabi, G. Perirenal Fat CT Radiomics-Based Survival Model for Upper Tract Urothelial Carcinoma: Integrating Texture Features with Clinical Predictors. Cancers 2024, 16, 3772. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (n = 103) | Low Grade (n = 30) | High Grade (n = 73) | Early Stage (T1) (n = 58) | Advanced Stage (T2–T4) (n = 45) |
|---|---|---|---|---|---|
| Age, median (range) | 74 (49–93) | 67 (49–85) * | 76 (52–93) * | 72 (49–88) * | 77 (56–93) * |
| Gender, n (%) | |||||
| Male | 61 (59%) | 16 (53%) * | 45 (62%) * | 35 (60%) * | 26 (58%) * |
| Female | 42 (41%) | 14 (47%) * | 28 (38%) * | 23 (40%) * | 19 (42%) * |
| Smoking Status, n (%) | |||||
| Current/Former | 80 (78%) | 20 (67%) * | 60 (82%) * | 44 (76%) * | 36 (80%) * |
| Never | 23 (22%) | 10 (33%) * | 13 (18%) * | 14 (24%) * | 9 (20%) * |
| BMI Category, n (%) | |||||
| Normal (18.5–24.9) | 34 (33%) | 12 (40%) * | 22 (30%) * | 19 (33%) * | 15 (33%) * |
| Overweight (25–29.9) | 35 (34%) | 10 (33%) * | 25 (34%) * | 20 (34%) * | 15 (33%) * |
| Obese (≥30) | 34 (33%) | 8 (27%) * | 26 (36%) * | 19 (33%) * | 15 (33%) * |
| Tumour Location, n (%) | |||||
| Renal Pelvis | 49 (48%) | 20 (67%) * | 29 (40%) * | 28 (48%) * | 21 (47%) * |
| Ureter | 54 (52%) | 10 (33%) * | 44 (60%) * | 30 (52%) * | 24 (53%) * |
| Carcinoma in situ, n (%) | 25 (23%) | 4 (13%) * | 21 (29%) * | 13 (22%) * | 12 (27%) * |
| Hydronephrosis, n (%) | 25 (23%) | 5 (17%) * | 20 (27%) * | 12 (21%) * | 13 (29%) * |
| Multifocal, n (%) | 38 (35%) | 8 (27%) * | 30 (41%) * | 18 (31%) * | 20 (44%) * |
| Tumour Size, mean ± SD (cm) | 1.97 ± 0.83 | 1.70 ± 0.70 * | 2.08 ± 0.86 * | 1.85 ± 0.73 * | 2.10 ± 0.90 * |
| Deceased, n (%) | 58 (56%) | 8 (27%) * | 50 (68%) * | 28 (48%) * | 30 (67%) * |
| Recurrence, n (%) | 31 (29%) | 5 (17%) * | 26 (36%) * | 14 (24%) * | 17 (38%) * |
| Target | Data | Classifier | AUC Mean | AUC 95% CI | Sensitivity | Specificity | F1 Score |
|---|---|---|---|---|---|---|---|
| Grade | TUMOUR + 10 mm PRF | MLPClassifier | 0.961 | [0.920, 1.000] | 0.889 | 0.889 | 0.889 |
| Tumour | RandomForestClassifier | 0.934 | [0.891, 0.977] | 0.867 | 0.867 | 0.863 | |
| PRF 10 mm | CatBoostClassifier | 0.900 | [0.814, 0.986] | 0.783 | 0.884 | 0.841 | |
| PRF 15 mm | MLPClassifier | 0.890 | [0.825, 0.956] | 0.806 | 0.806 | 0.802 | |
| PRF 20 mm | LGBMClassifier | 0.883 | [0.825, 0.941] | 0.764 | 0.819 | 0.798 | |
| PRF 25 mm | RandomForestClassifier | 0.876 | [0.816, 0.937] | 0.778 | 0.792 | 0.784 | |
| PRF 30 mm | CatBoostClassifier | 0.874 | [0.813, 0.934] | 0.806 | 0.847 | 0.827 | |
| STAGE | TUMOUR + 15 mm PRF | MLPClassifier | 0.852 | [0.790, 0.914] | 0.776 | 0.776 | 0.772 |
| Tumour | MLPClassifier | 0.831 | [0.750, 0.911] | 0.780 | 0.746 | 0.765 | |
| PRF 15 mm | LogisticRegression | 0.778 | [0.704, 0.851] | 0.702 | 0.667 | 0.682 | |
| PRF 30 mm | ExtraTreesClassifier | 0.771 | [0.668, 0.874] | 0.638 | 0.690 | 0.669 | |
| PRF 25 mm | AdaBoostClassifier | 0.759 | [0.639, 0.879] | 0.672 | 0.707 | 0.680 | |
| PRF 10 mm | MLPClassifier | 0.756 | [0.657, 0.854] | 0.679 | 0.643 | 0.654 | |
| PRF 20 mm | MLPClassifier | 0.711 | [0.641, 0.781] | 0.724 | 0.500 | 0.642 |
| Model 1 | Model 2 | AUC 1 | AUC 2 | Z-Score | p-Value | |
|---|---|---|---|---|---|---|
| Grade | Tumour + 10 mm PRF MLPClassifier | Tumour Random Forest Classifier | 0.961 | 0.934 | 1.212807 | 0.225204 |
| Tumour + 10 mm PRF MLPClassifier | PRF 10 mm Cat Boost Classifier | 0.961 | 0.9 | 2.416159 | 0.015685 | |
| Tumour Random Forest Classifier | PRF 10 mm Cat Boost Classifier | 0.934 | 0.9 | 1.234756 | 0.216921 | |
| Stage | Tumour + 15 mm PRF MLPClassifier | Tumour MLPClassifier | 0.852 | 0.831 | 0.575251 | 0.565122 |
| Tumour + 15 mm PRF MLPClassifier | PRF 15 mm Logistic Regression | 0.852 | 0.778 | 1.914466 | 0.055561 | |
| Tumour MLPClassifier | PRF 15 mm Logistic Regression | 0.831 | 0.778 | 1.339403 | 0.18044 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Mopti, A.; Alqahtani, A.; Alshehri, A.H.D.; Li, C.; Nabi, G. Evaluating the Predictive Capability of Radiomics Features of Perirenal Fat in Enhanced CT Images for Staging and Grading of UTUC Tumours Using Machine Learning. Cancers 2025, 17, 1220. https://doi.org/10.3390/cancers17071220
Al Mopti A, Alqahtani A, Alshehri AHD, Li C, Nabi G. Evaluating the Predictive Capability of Radiomics Features of Perirenal Fat in Enhanced CT Images for Staging and Grading of UTUC Tumours Using Machine Learning. Cancers. 2025; 17(7):1220. https://doi.org/10.3390/cancers17071220
Chicago/Turabian StyleAl Mopti, Abdulrahman, Abdulsalam Alqahtani, Ali H. D. Alshehri, Chunhui Li, and Ghulam Nabi. 2025. "Evaluating the Predictive Capability of Radiomics Features of Perirenal Fat in Enhanced CT Images for Staging and Grading of UTUC Tumours Using Machine Learning" Cancers 17, no. 7: 1220. https://doi.org/10.3390/cancers17071220
APA StyleAl Mopti, A., Alqahtani, A., Alshehri, A. H. D., Li, C., & Nabi, G. (2025). Evaluating the Predictive Capability of Radiomics Features of Perirenal Fat in Enhanced CT Images for Staging and Grading of UTUC Tumours Using Machine Learning. Cancers, 17(7), 1220. https://doi.org/10.3390/cancers17071220