
Deficiency of MTAP Is Frequent and Mostly Homogeneous in Pancreatic Ductal Adenocarcinomas

 , , , , , , ,
, , , , , , ,  , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Tissue Microarray
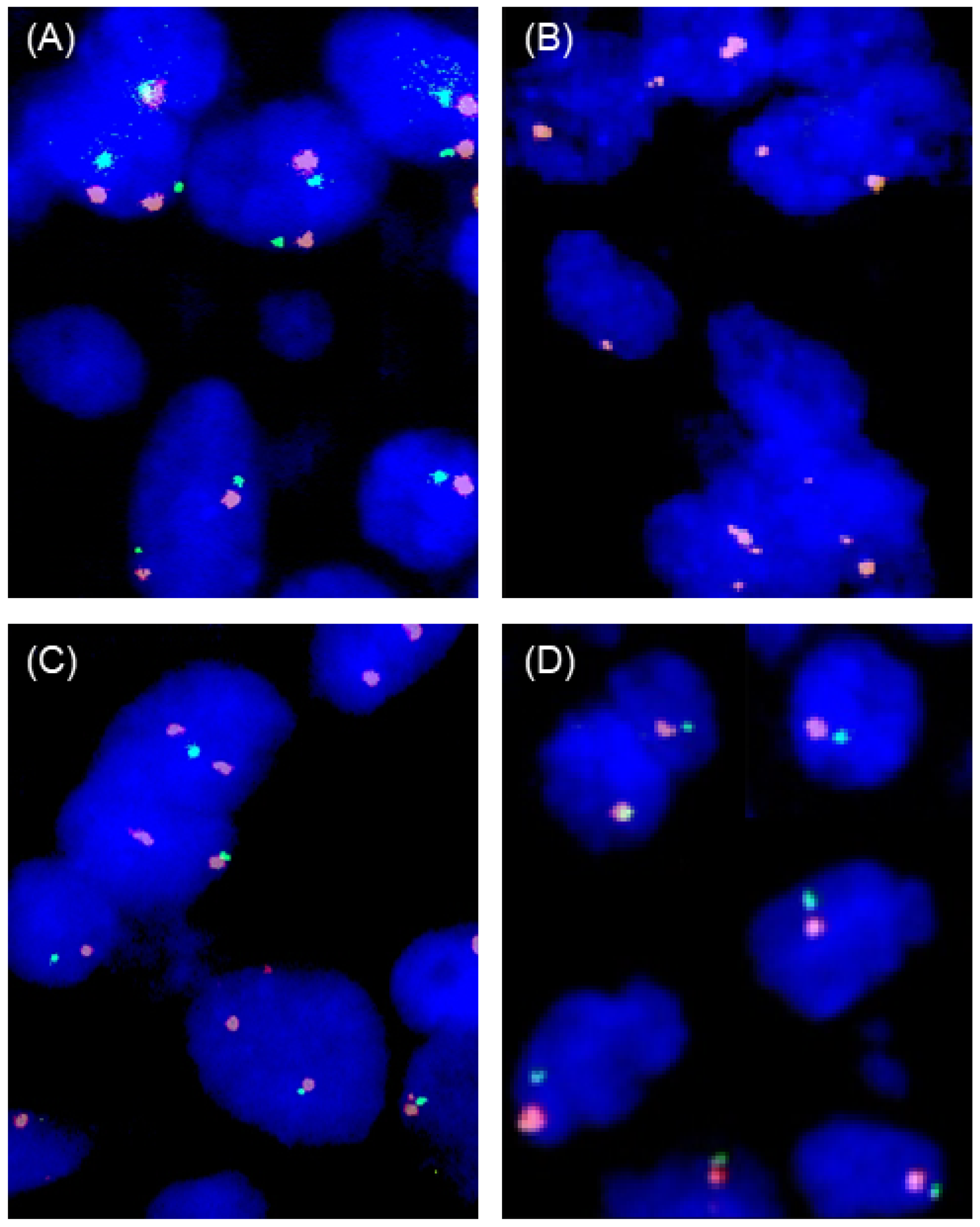
2.2. Fluorescence In Situ Hybridization (FISH)
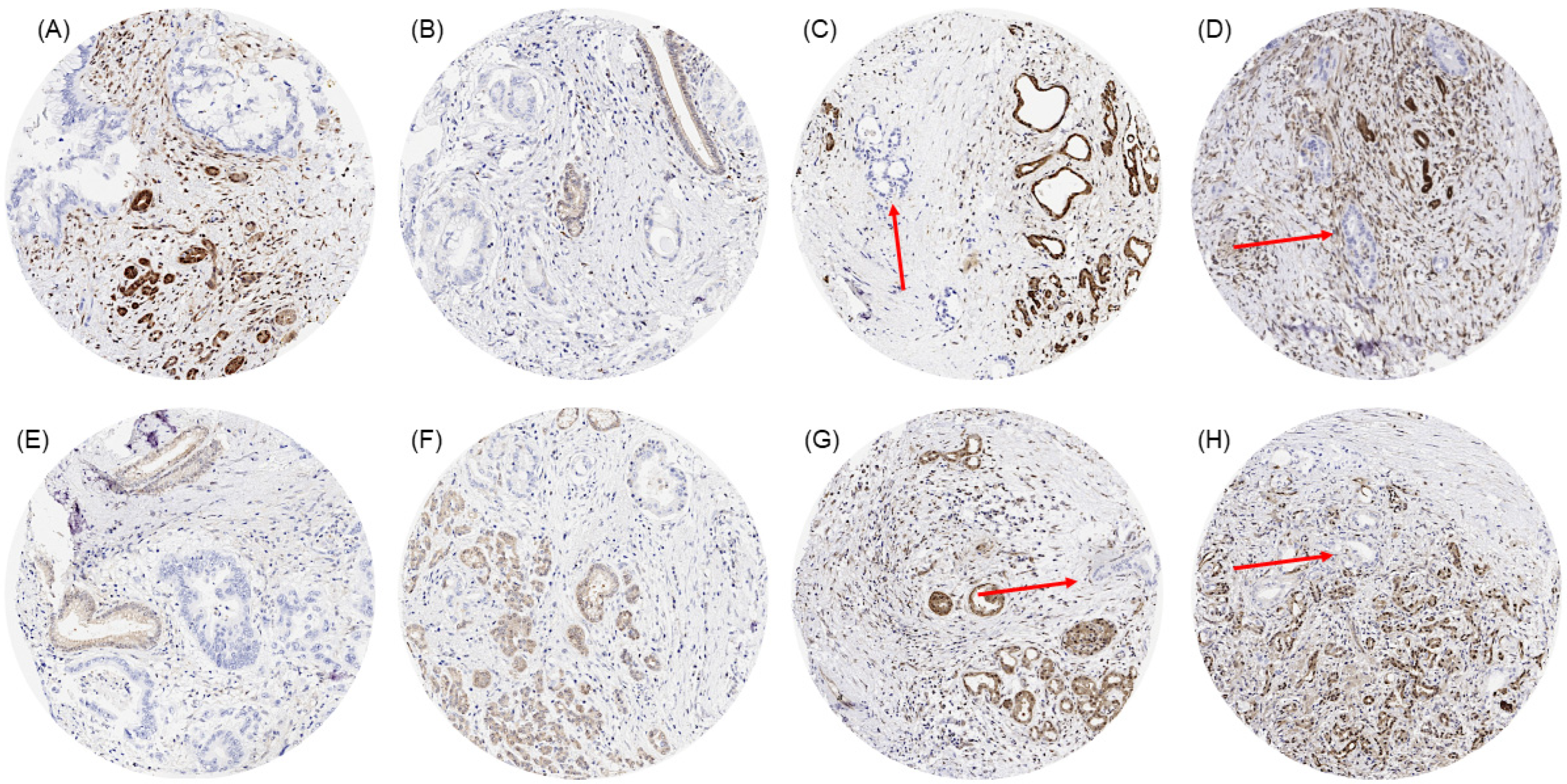
2.3. Immunohistochemistry (IHC)
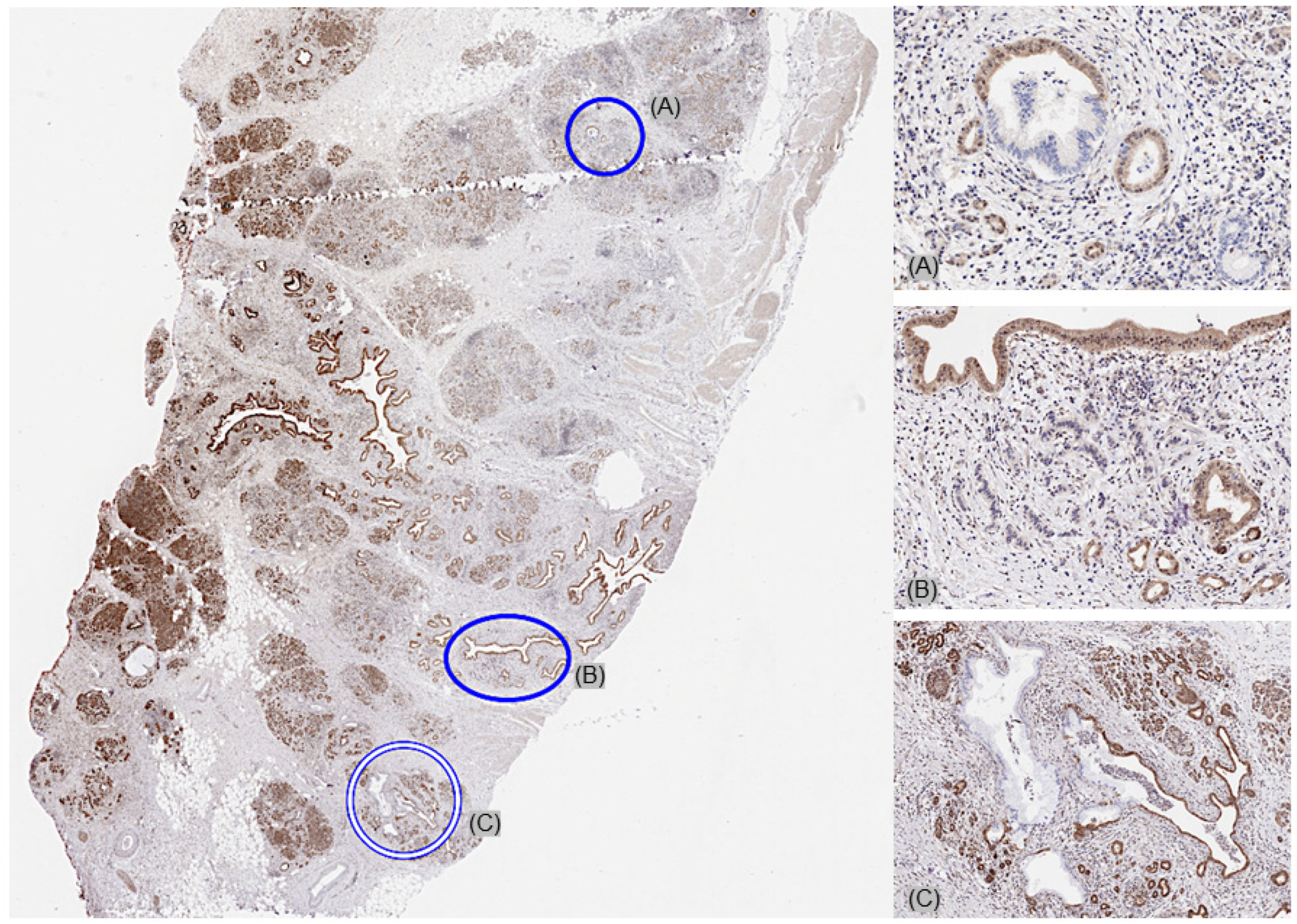
2.4. Whole-Section Validation and Heterogeneity Analysis
2.5. Statistics
3. Results
3.1. Technical Results
3.2. MTAP Deficiency in Primary Tumors
3.3. MTAP Heterogeneity
3.4. MTAP FISH vs. IHC Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Della Ragione, F.; Carteni-Farina, M.; Gragnaniello, V.; Schettino, M.I.; Zappia, V. Purification and characterization of 5′-deoxy-5′-methylthioadenosine phosphorylase from human placenta. J. Biol. Chem. 1986, 261, 12324–12329. [Google Scholar] [PubMed]
- Beroukhim, R.; Mermel, C.H.; Porter, D.; Wei, G.; Raychaudhuri, S.; Donovan, J.; Barretina, J.; Boehm, J.S.; Dobson, J.; Urashima, M.; et al. The landscape of somatic copy-number alteration across human cancers. Nature 2010, 463, 899–905. [Google Scholar] [CrossRef]
- ICGC/TCGA Pan-Cancer Analysis of Whole Genomes Consortium. Pan-cancer analysis of whole genomes. Nature 2020, 578, 82–93. [Google Scholar] [CrossRef]
- Harrison, P.W.; Amode, M.R.; Austine-Orimoloye, O.; Azov, A.G.; Barba, M.; Barnes, I.; Becker, A.; Bennett, R.; Berry, A.; Bhai, J.; et al. Ensembl 2024. Nucleic Acids Res. 2023, 52, D891–D899. [Google Scholar] [CrossRef]
- Zhang, H.; Chen, Z.H.; Savarese, T.M. Codeletion of the genes for p16INK4, methylthioadenosine phosphorylase, interferon-alpha1, interferon-beta1, and other 9p21 markers in human malignant cell lines. Cancer Genet. Cytogenet. 1996, 86, 22–28. [Google Scholar] [CrossRef]
- Alhalabi, O.; Chen, J.; Zhang, Y.; Lu, Y.; Wang, Q.; Ramachandran, S.; Tidwell, R.S.; Han, G.; Yan, X.; Meng, J.; et al. MTAP deficiency creates an exploitable target for antifolate therapy in 9p21-loss cancers. Nat. Commun. 2022, 13, 1797. [Google Scholar] [CrossRef] [PubMed]
- Bray, C.; Balcells, C.; McNeish, I.A.; Keun, H.C. The potential and challenges of targeting MTAP-negative cancers beyond synthetic lethality. Front. Oncol. 2023, 13, 1264785. [Google Scholar] [CrossRef]
- Blanc, R.S.; Richard, S. Arginine Methylation: The Coming of Age. Mol. Cell 2017, 65, 8–24. [Google Scholar] [CrossRef]
- Lu, S.C.; Mato, J.M. S-adenosylmethionine in liver health, injury, and cancer. Physiol. Rev. 2012, 92, 1515–1542. [Google Scholar] [CrossRef]
- Murray, B.; Antonyuk, S.V.; Marina, A.; Lu, S.C.; Mato, J.M.; Hasnain, S.S.; Rojas, A.L. Crystallography captures catalytic steps in human methionine adenosyltransferase enzymes. Proc. Natl. Acad. Sci. USA 2016, 113, 2104–2109. [Google Scholar] [CrossRef]
- Kryukov, G.V.; Wilson, F.H.; Ruth, J.R.; Paulk, J.; Tsherniak, A.; Marlow, S.E.; Vazquez, F.; Weir, B.A.; Fitzgerald, M.E.; Tanaka, M.; et al. MTAP deletion confers enhanced dependency on the PRMT5 arginine methyltransferase in cancer cells. Science 2016, 351, 1214–1218. [Google Scholar] [CrossRef]
- Engstrom, L.D.; Aranda, R.; Waters, L.; Moya, K.; Bowcut, V.; Vegar, L.; Trinh, D.; Hebbert, A.; Smith, C.R.; Kulyk, S.; et al. MRTX1719 Is an MTA-Cooperative PRMT5 Inhibitor That Exhibits Synthetic Lethality in Preclinical Models and Patients with MTAP-Deleted Cancer. Cancer Discov. 2023, 13, 2412–2431. [Google Scholar] [CrossRef] [PubMed]
- Feustel, K.; Falchook, G.S. Protein Arginine Methyltransferase 5 (PRMT5) Inhibitors in Oncology Clinical Trials: A review. J. Immunother. Preci.s Oncol. 2022, 5, 58–67. [Google Scholar] [CrossRef]
- Belmontes, B.; Slemmons, K.K.; Su, C.; Liu, S.; Policheni, A.N.; Moriguchi, J.; Tan, H.; Xie, F.; Aiello, D.A.; Yang, Y.; et al. AMG 193, a Clinical Stage MTA-Cooperative PRMT5 Inhibitor, Drives Antitumor Activity Preclinically and in Patients with MTAP-Deleted Cancers. Cancer Discov. 2024, 15, 139–161. [Google Scholar] [CrossRef] [PubMed]
- Rodon, J.; Prenen, H.; Sacher, A.; Villalona-Calero, M.; Penel, N.; El Helali, A.; Rottey, S.; Yamamoto, N.; Ghiringhelli, F.; Goebeler, M.E.; et al. First-in-human study of AMG 193, an MTA-cooperative PRMT5 inhibitor, in patients with MTAP-deleted solid tumors: Results from phase I dose exploration. Ann. Oncol. 2024, 35, 1138–1147. [Google Scholar] [CrossRef]
- Sjostedt, E.; Zhong, W.; Fagerberg, L.; Karlsson, M.; Mitsios, N.; Adori, C.; Oksvold, P.; Edfors, F.; Limiszewska, A.; Hikmet, F.; et al. An atlas of the protein-coding genes in the human, pig, and mouse brain. Science 2020, 367, eaay5947. [Google Scholar] [CrossRef]
- UniProt, C. UniProt: The Universal Protein Knowledgebase in 2023. Nucleic Acids Res. 2023, 51, D523–D531. [Google Scholar] [CrossRef]
- Gorbokon, N.; Wossner, N.; Lennartz, M.; Dwertmann Rico, S.; Kind, S.; Reiswich, V.; Viehweger, F.; Lutz, F.; Fraune, C.; Luebke, A.M.; et al. Prevalence of S-methyl-5’-thioadenosine Phosphorylase (MTAP) Deficiency in Human Cancer: A Tissue Microarray Study on 13,067 Tumors from 149 Different Tumor Types. Am. J. Surg. Pathol. 2024, 48, 1245–1258. [Google Scholar] [CrossRef]
- Bengtsson, A.; Andersson, R.; Ansari, D. The actual 5-year survivors of pancreatic ductal adenocarcinoma based on real-world data. Sci. Rep. 2020, 10, 16425. [Google Scholar] [CrossRef]
- Kononen, J.; Bubendorf, L.; Kallioniemi, A.; Barlund, M.; Schraml, P.; Leighton, S.; Torhorst, J.; Mihatsch, M.J.; Sauter, G.; Kallioniemi, O.P. Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat. Med. 1998, 4, 844–847. [Google Scholar]
- Gorbokon, N.; Wossner, N.; Ahlburg, V.; Plage, H.; Hofbauer, S.; Furlano, K.; Weinberger, S.; Bruch, P.G.; Schallenberg, S.; Rossner, F.; et al. Loss of MTAP expression is strongly linked to homozygous 9p21 deletion, unfavorable tumor phenotype, and noninflamed microenvironment in urothelial bladder cancer. J. Pathol. Clin. Res. 2025, 11, e70012. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Doyle, L.A.; Hornick, J.L.; Mito, J.K. The diagnostic utility of methylthioadenosine phosphorylase immunohistochemistry for pancreatic ductal adenocarcinoma in FNA and small biopsy specimens. Cancer Cytopathol. 2024, 132, 87–95. [Google Scholar] [CrossRef]
- Hu, Y.X.; Watanabe, H.; Ohtsubo, K.; Yamaguchi, Y.; Ha, A.; Okai, T.; Sawabu, N. Frequent loss of p16 expression and its correlation with clinicopathological parameters in pancreatic carcinoma. Clin. Cancer Res. 1997, 3, 1473–1477. [Google Scholar]
- Hustinx, S.R.; Hruban, R.H.; Leoni, L.M.; Iacobuzio-Donahue, C.; Cameron, J.L.; Yeo, C.J.; Brown, P.N.; Argani, P.; Ashfaq, R.; Fukushima, N.; et al. Homozygous deletion of the MTAP gene in invasive adenocarcinoma of the pancreas and in periampullary cancer: A potential new target for therapy. Cancer Biol. Ther. 2005, 4, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Ngoi, N.Y.L.; Tang, T.Y.; Gaspar, C.F.; Pavlick, D.C.; Buchold, G.M.; Scholefield, E.L.; Parimi, V.; Huang, R.S.P.; Janovitz, T.; Danziger, N.; et al. Methylthioadenosine Phosphorylase Genomic Loss in Advanced Gastrointestinal Cancers. Oncologist 2024, 29, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wu, Y.; Zhang, L.; Wang, Y.; Xu, G.; Deng, Y.; Han, L.; Li, E.; Ma, Q.; Xu, M.; et al. Loss of chromosome 9p21 is associated with a poor prognosis in adenosquamous carcinoma of the pancreas. Precis Clin. Med. 2023, 6, pbad030. [Google Scholar] [CrossRef]
- Uhlen, M.; Bandrowski, A.; Carr, S.; Edwards, A.; Ellenberg, J.; Lundberg, E.; Rimm, D.L.; Rodriguez, H.; Hiltke, T.; Snyder, M.; et al. A proposal for validation of antibodies. Nat. Methods 2016, 13, 823–827. [Google Scholar] [CrossRef]
- Jee, J.; Fong, C.; Pichotta, K.; Tran, T.N.; Luthra, A.; Waters, M.; Fu, C.; Altoe, M.; Liu, S.Y.; Maron, S.B.; et al. Automated real-world data integration improves cancer outcome prediction. Nature 2024, 636, 728–736. [Google Scholar] [CrossRef]
- Berasain, C.; Hevia, H.; Fernandez-Irigoyen, J.; Larrea, E.; Caballeria, J.; Mato, J.M.; Prieto, J.; Corrales, F.J.; Garcia-Trevijano, E.R.; Avila, M.A. Methylthioadenosine phosphorylase gene expression is impaired in human liver cirrhosis and hepatocarcinoma. Biochim. Biophys. Acta 2004, 1690, 276–284. [Google Scholar] [CrossRef]
- Gu, A.; Li, J.; Li, M.Y.; Liu, Y. Patient-derived xenograft model in cancer: Establishment and applications. MedComm (2020) 2025, 6, e70059. [Google Scholar] [CrossRef]
- Navarro, G.; Gomez-Autet, M.; Morales, P.; Rebassa, J.B.; Llinas Del Torrent, C.; Jagerovic, N.; Pardo, L.; Franco, R. Homodimerization of CB(2) cannabinoid receptor triggered by a bivalent ligand enhances cellular signaling. Pharmacol. Res. 2024, 208, 107363. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liao, Z.-X. Research progress of microrobots in tumor drug delivery. Food Med. Homol. 2024, 1, 9420025. [Google Scholar] [CrossRef]
- Evrard, C.; Messina, S.; Sefrioui, D.; Frouin, E.; Auriault, M.L.; Chautard, R.; Zaanan, A.; Jaffrelot, M.; De La Fouchardiere, C.; Aparicio, T.; et al. Heterogeneity of Mismatch Repair Status and Microsatellite Instability between Primary Tumour and Metastasis and Its Implications for Immunotherapy in Colorectal Cancers. Int. J. Mol. Sci. 2022, 23, 4427. [Google Scholar] [CrossRef] [PubMed]
- Fraune, C.; Rosebrock, J.; Simon, R.; Hube-Magg, C.; Makrypidi-Fraune, G.; Kluth, M.; Buscheck, F.; Hoflmayer, D.; Schmalfeldt, B.; Muller, V.; et al. High homogeneity of MMR deficiency in ovarian cancer. Gynecol. Oncol. 2020, 156, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Mafficini, A.; Chatterjee, D.; Piredda, M.L.; Sciammarella, C.; Navale, P.; Malleo, G.; Mattiolo, P.; Marchegiani, G.; Pea, A.; et al. Histo-molecular characterization of pancreatic cancer with microsatellite instability: Intra-tumor heterogeneity, B2M inactivation, and the importance of metastatic sites. Virchows Arch. 2022, 480, 1261–1268. [Google Scholar] [CrossRef]
- Seol, H.; Lee, H.J.; Choi, Y.; Lee, H.E.; Kim, Y.J.; Kim, J.H.; Kang, E.; Kim, S.W.; Park, S.Y. Intratumoral heterogeneity of HER2 gene amplification in breast cancer: Its clinicopathological significance. Mod. Pathol. 2012, 25, 938–948. [Google Scholar] [CrossRef]
- Grillo, F.; Fassan, M.; Sarocchi, F.; Fiocca, R.; Mastracci, L. HER2 heterogeneity in gastric/gastroesophageal cancers: From benchside to practice. World J. Gastroenterol. 2016, 22, 5879–5887. [Google Scholar] [CrossRef]
- Lei, H.; Ling, Y.; Yuan, P.; Yan, X.; Wang, L.; Shi, Y.; Yao, X.; Luo, H.; Shi, B.; Liu, J.; et al. Assessment of the expression pattern of HER2 and its correlation with HER2-targeting antibody-drug conjugate therapy in urothelial cancer. J. Natl. Cancer Cent. 2023, 3, 121–128. [Google Scholar] [CrossRef]
- Zito Marino, F.; Liguori, G.; Aquino, G.; La Mantia, E.; Bosari, S.; Ferrero, S.; Rosso, L.; Gaudioso, G.; De Rosa, N.; Scrima, M.; et al. Intratumor Heterogeneity of ALK-Rearrangements and Homogeneity of EGFR-Mutations in Mixed Lung Adenocarcinoma. PLoS ONE 2015, 10, e0139264. [Google Scholar] [CrossRef]
- Krohn, A.; Freudenthaler, F.; Harasimowicz, S.; Kluth, M.; Fuchs, S.; Burkhardt, L.; Stahl, P.; Tsourlakis, C.M.; Bauer, M.; Tennstedt, P.; et al. Heterogeneity and chronology of PTEN deletion and ERG fusion in prostate cancer. Mod. Pathol. 2014, 27, 1612–1620. [Google Scholar] [CrossRef]
- Tatematsu, T.; Sasaki, H.; Shimizu, S.; Hikosaka, Y.U.; Okuda, K.; Haneda, H.; Moriyama, S.; Yano, M.; Fujii, Y. Intra-tumor heterogeneity of BRAF V600E mutation in lung adenocarcinomas. Exp. Ther. Med. 2015, 9, 1719–1722. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathological Parameters | MTAP Status (%) | ||||
|---|---|---|---|---|---|
| n | Loss | Retained | p-Value | ||
| Analyzable tumors | 478 | 37.9 | 62.1 | ||
| Tumor stage | pT1 | 11 | 54.6 | 45.5 | 0.6462 |
| pT2 | 72 | 40.3 | 59.7 | ||
| pT3 | 354 | 37.0 | 63.0 | ||
| pT4 | 37 | 35.1 | 64.9 | ||
| Nodal stage | pN0 | 111 | 39.6 | 60.4 | 0.5302 |
| pN+ | 336 | 36.3 | 63.7 | ||
| Grade | G1 | 21 | 33.3 | 66.7 | 0.7951 |
| G2 | 303 | 38.3 | 61.7 | ||
| G3 | 127 | 35.4 | 64.6 | ||
| Tumor size (mm) | mean ± SD | 347 | 38.4 ± 1.8 | 39.1 ± 1.4 | 0.7575 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorbokon, N.; Teljuk, K.; Reiswich, V.; Lennartz, M.; Minner, S.; Simon, R.; Sauter, G.; Wilczak, W.; Clauditz, T.S.; Schraps, N.; et al. Deficiency of MTAP Is Frequent and Mostly Homogeneous in Pancreatic Ductal Adenocarcinomas. Cancers 2025, 17, 1205. https://doi.org/10.3390/cancers17071205
Gorbokon N, Teljuk K, Reiswich V, Lennartz M, Minner S, Simon R, Sauter G, Wilczak W, Clauditz TS, Schraps N, et al. Deficiency of MTAP Is Frequent and Mostly Homogeneous in Pancreatic Ductal Adenocarcinomas. Cancers. 2025; 17(7):1205. https://doi.org/10.3390/cancers17071205
Chicago/Turabian StyleGorbokon, Natalia, Katharina Teljuk, Viktor Reiswich, Maximilian Lennartz, Sarah Minner, Ronald Simon, Guido Sauter, Waldemar Wilczak, Till Sebastian Clauditz, Nina Schraps, and et al. 2025. "Deficiency of MTAP Is Frequent and Mostly Homogeneous in Pancreatic Ductal Adenocarcinomas" Cancers 17, no. 7: 1205. https://doi.org/10.3390/cancers17071205
APA StyleGorbokon, N., Teljuk, K., Reiswich, V., Lennartz, M., Minner, S., Simon, R., Sauter, G., Wilczak, W., Clauditz, T. S., Schraps, N., Hackert, T., Uzunoglu, F. G., Kluth, M., Bubendorf, L., Matter, M., Viehweger, F., Freytag, M., Jacobsen, F., Möller, K., & Steurer, S. (2025). Deficiency of MTAP Is Frequent and Mostly Homogeneous in Pancreatic Ductal Adenocarcinomas. Cancers, 17(7), 1205. https://doi.org/10.3390/cancers17071205