

Development of an Intratumoral Holmium Microsphere Injection Method in Ex Vivo Human Pancreatic Ductal Adenocarcinoma: A Preclinical Feasibility Study
 , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
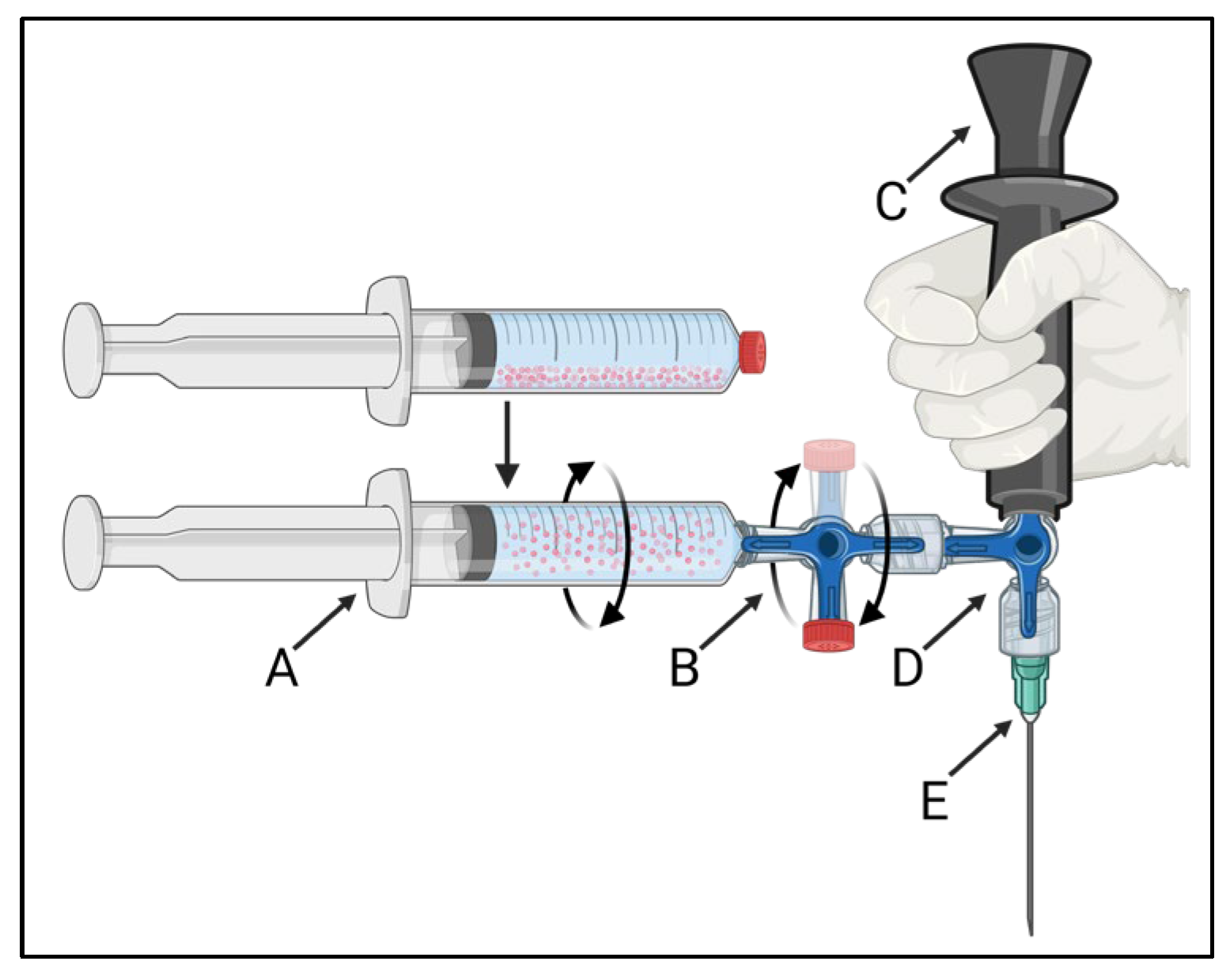
2.1. Injection System Design
2.2. Injection System Validation Testing
2.2.1. Microsphere Preparation
2.2.2. Laboratory Validation Testing
2.3. Ex Vivo Human Pancreatic Ductal Adenocarcinoma
2.4. Outcome Measures
Data Processing
3. Results
3.1. Injection System Development
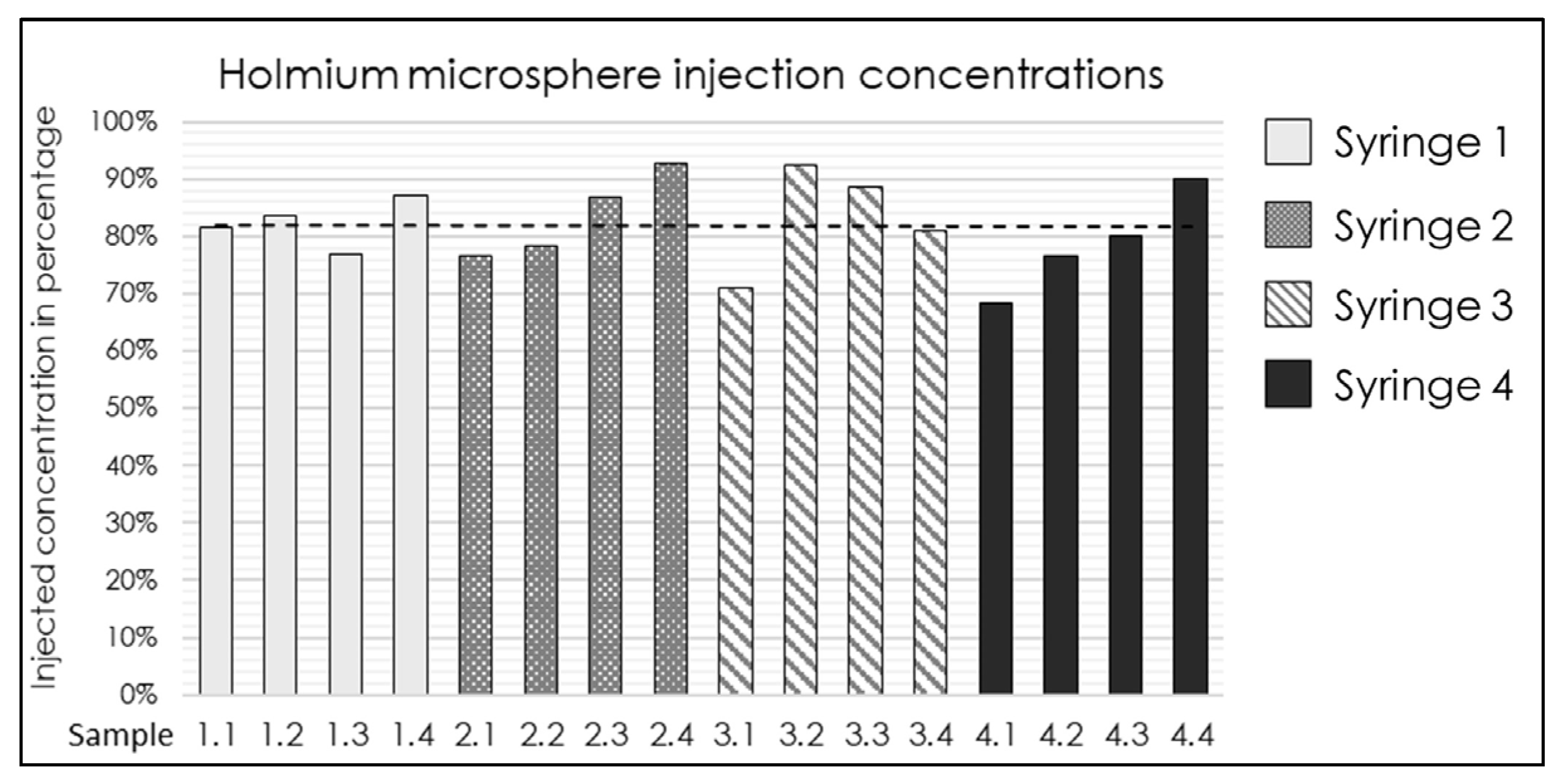
3.2. Injection System Validation
3.3. Ex Vivo Intratumoral Injection
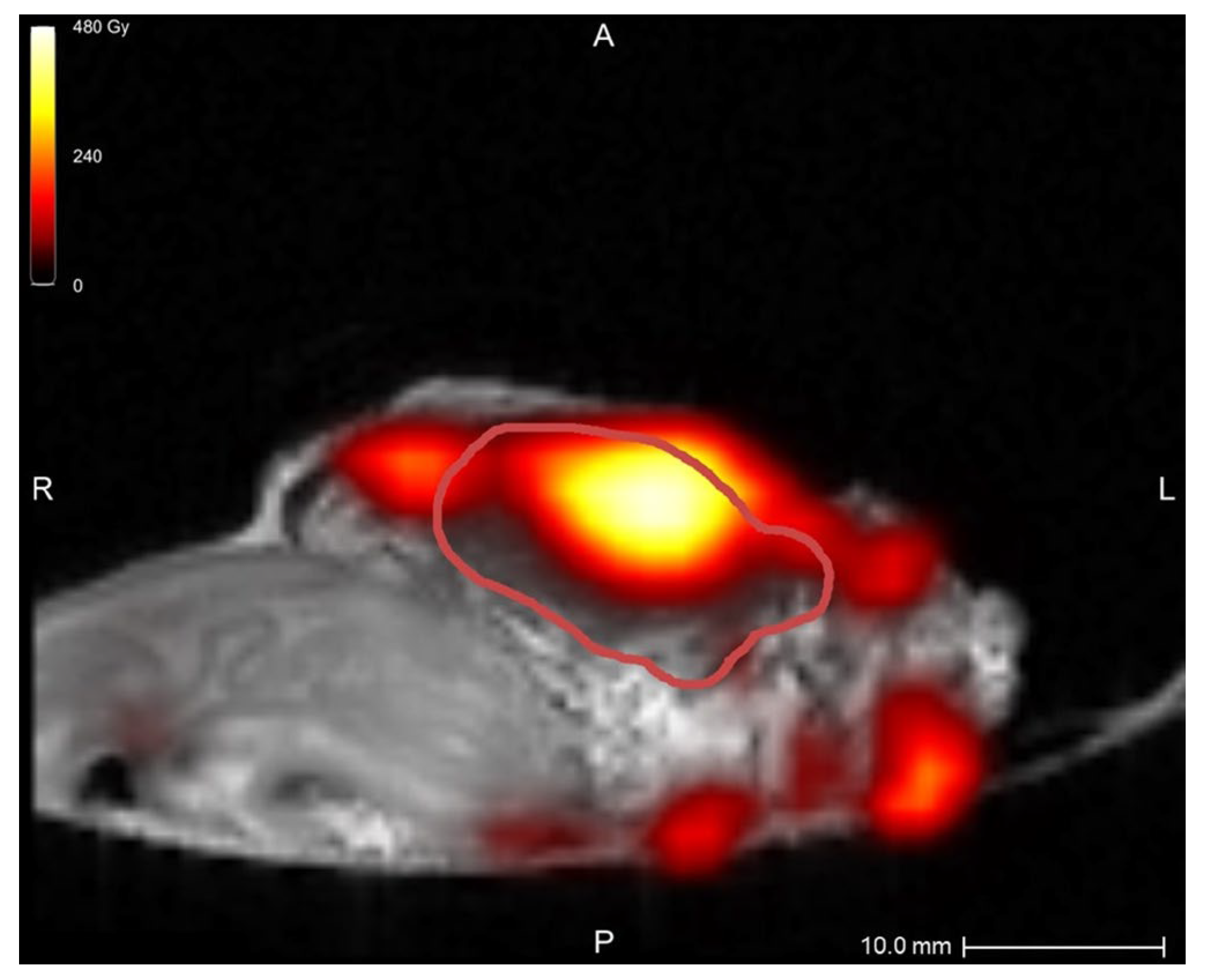
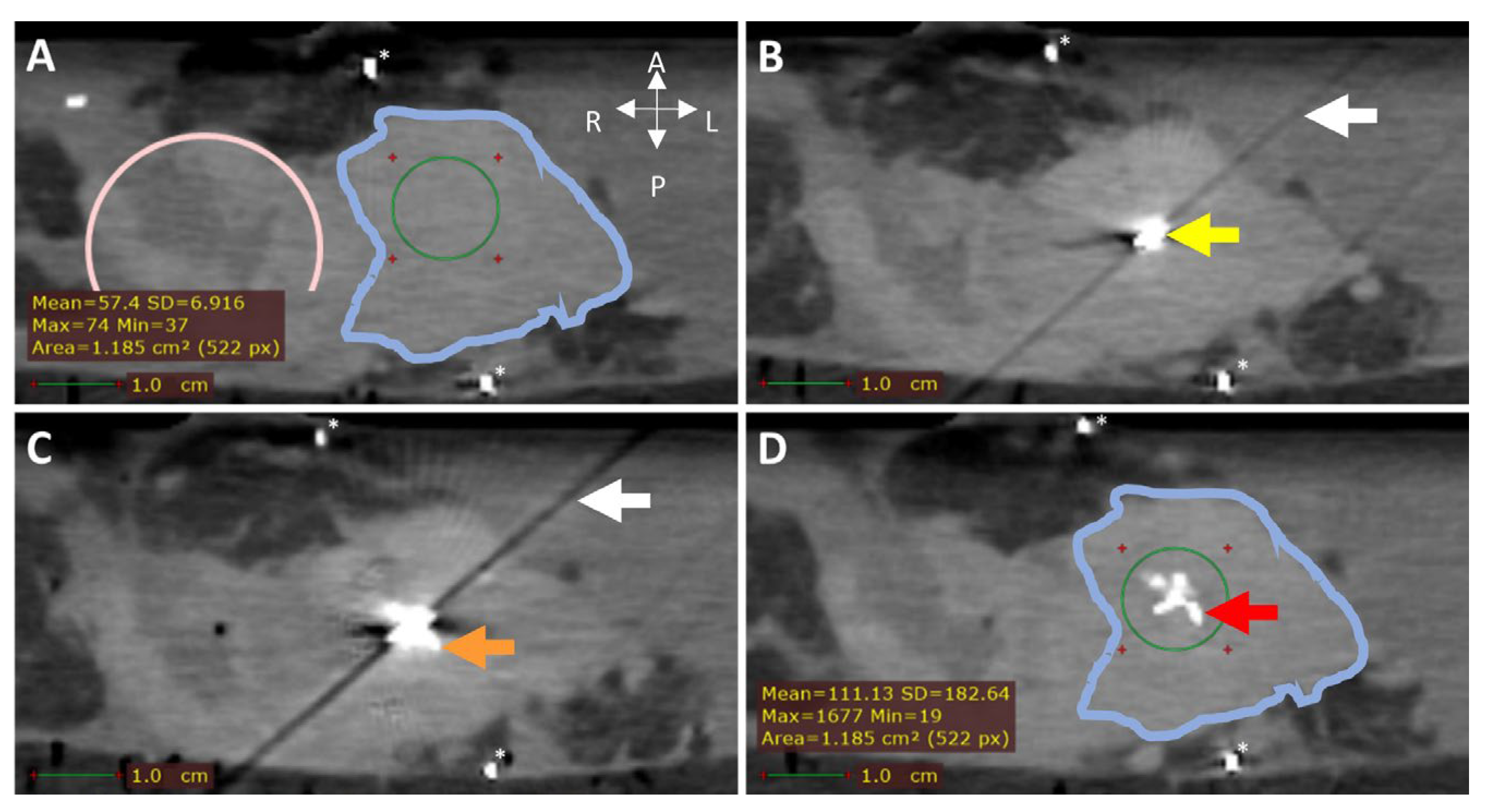
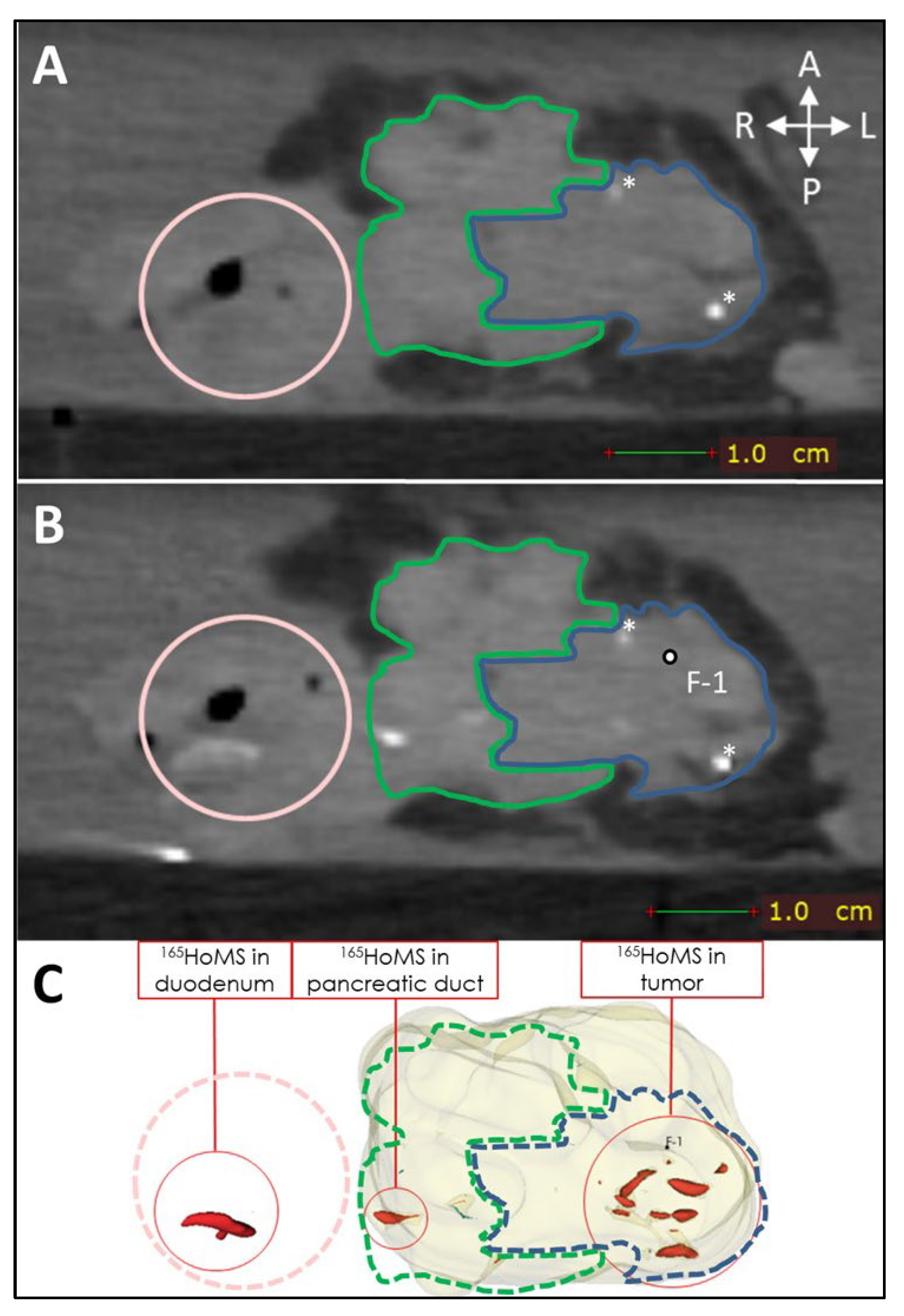
3.3.1. Image Guidance
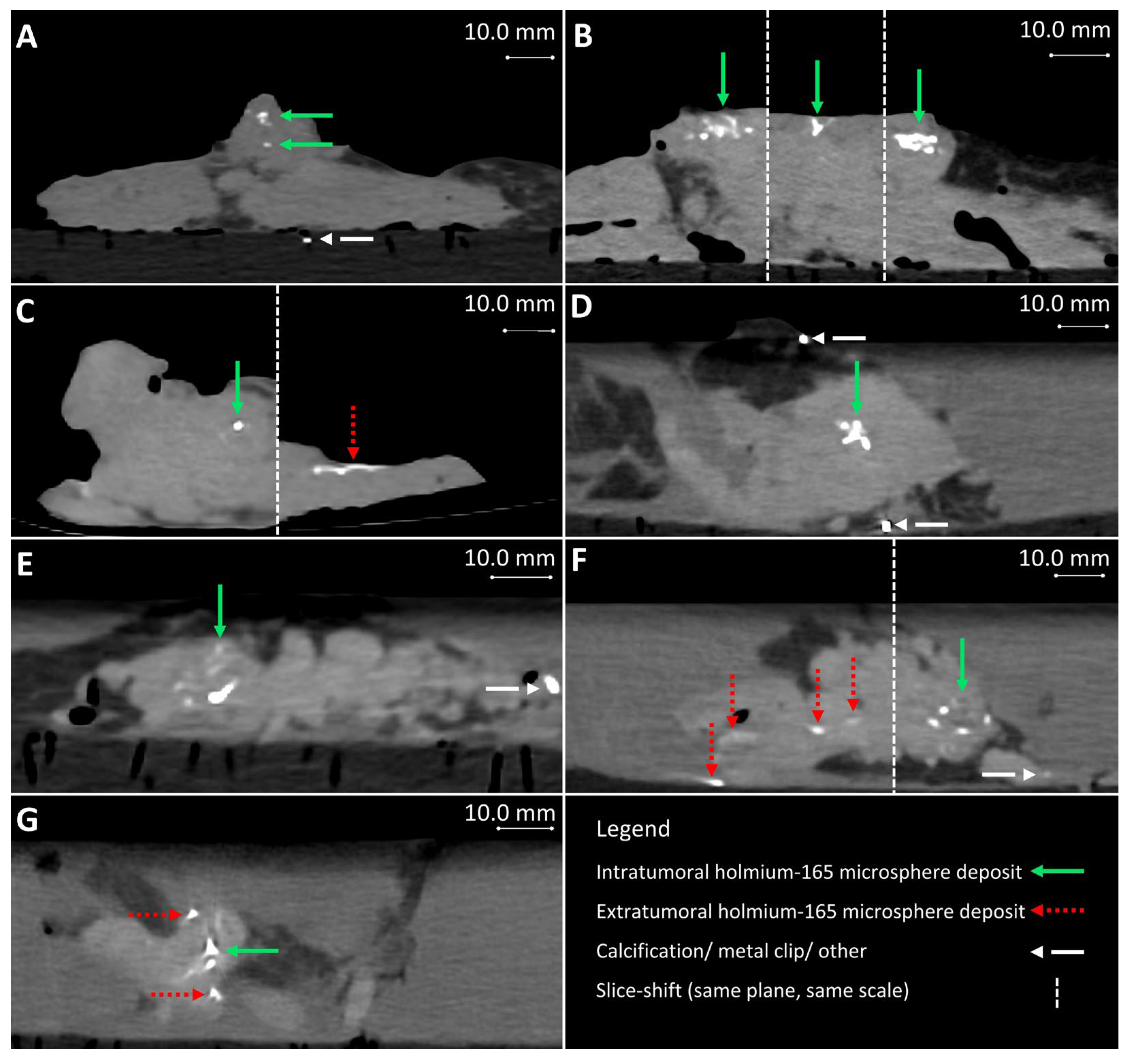
3.3.2. Injection Volume, Concentration, and Deposits
3.3.3. Leakage
3.3.4. Needle Blockage
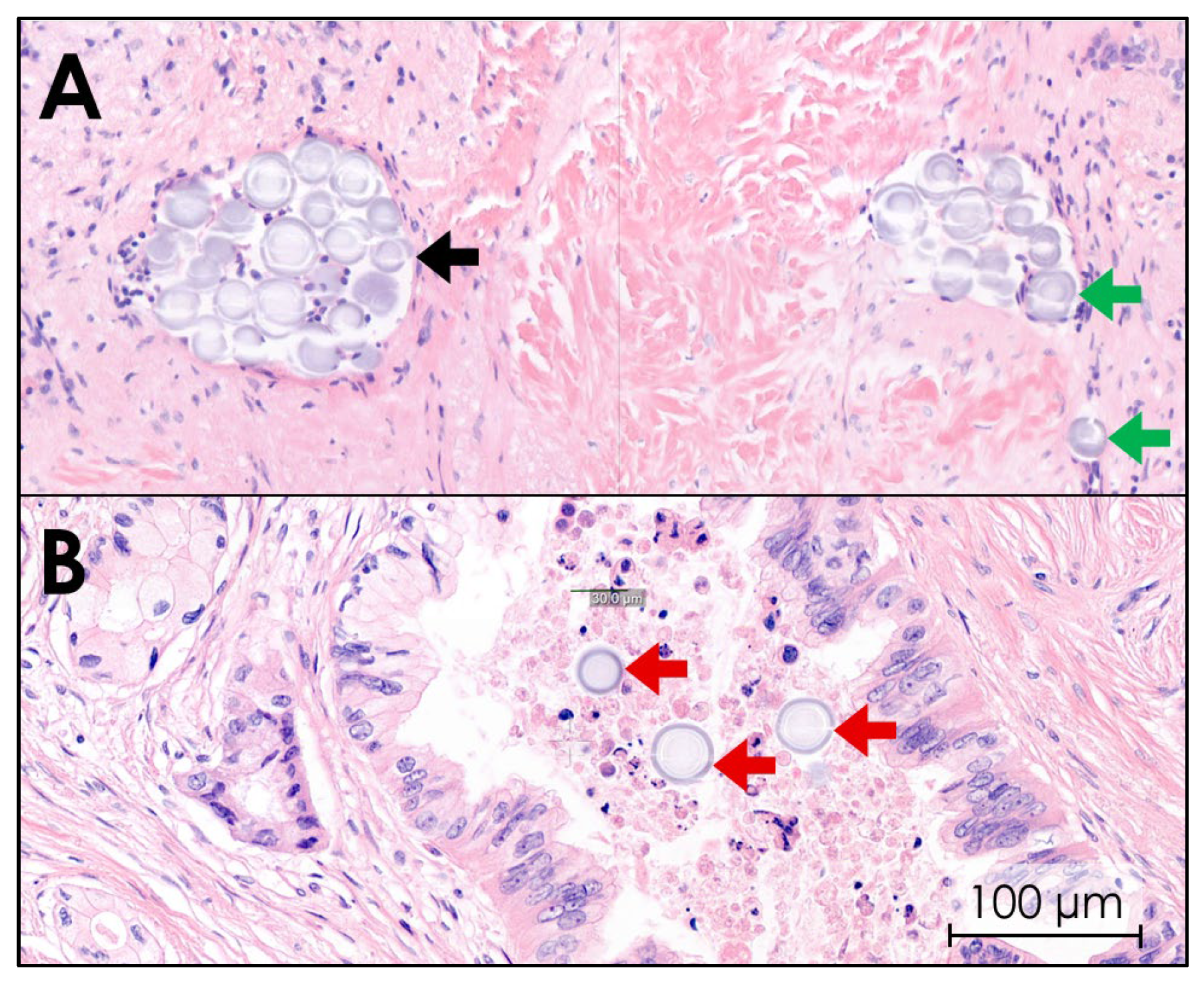
3.3.5. Histopathology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Extensive Injection System Development Results
- Syringe volume: 3.0 mL (range: 1.0–10.0 mL)Syringe volumes of 1.0 mL resulted in less homogeneous suspensions and faster agglomeration, whereas syringes up to 10.0 mL resulted in excessive variation in the volume injected by manual injection due to the larger diameter.
- Rotation time: 120 s (range: ~1–120 s)Visual homogenization of the 165HoMS suspension was achieved after 120 s in all the cases, even if the 165HoMSs accumulated to one side of the syringe before rotation. There were no clear differences in injection concentrations when rotating over 120 s.
- Rotation speed: 60 RPM (range: 30–120 RPM)Since rotation of the syringe was performed manually, a rotation speed was evaluated which could be achieved for multiple minutes without exhausting the operator and did not cause visual agglomeration. Rotation speeds below 60 RPM caused moments of idleness, which resulted in agglomeration. When the suspension was injected, rotation of the syringe was not possible, and agglomeration of the suspension occurred within seconds. Therefore, between every separate injection, or every 0.5 mL of injection volume, the syringe was rotated again for at least 10 s.
- Injection speed: 0.2 mL/s (range: 0.05–1.0 mL/s)Faster injection up to 1.0 mL/s could cause volume overshoots and thus increase the chance of leakage. Since the syringe could not be rotated during injection, lower injection speeds caused more 165HoMS agglomeration and more injection pauses to homogenize the suspension again.
- Injection volumes: 0.3–1.0 mL (range: 0.1–1.0 mL)Because the injection system contains a dead volume, which is the lumen volume between the syringe exit and needle tip in which the 165HoMSs agglomerate, a minimal injection volume of 0.3 mL was used to ensure complete flow through the dead volume, and 0.5 mL when the plastic extension tube was attached.
- System component diameters:System components with adjacent internal diameter changes, especially downstream narrowing, showed increased visual agglomeration of the 165HoMSs. Additionally, relatively large dead volumes, commonly found near Luer-lock connections, showed increased agglomeration when in a horizontal position. 165HoMS agglomeration within dead volumes caused a lower 165HoMS concentration; however, it could unexpectedly dislodge during injection and therefore suddenly increase the injected 165HoMS concentration.
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Bengtsson, A.; Andersson, R.; Ansari, D. The actual 5-year survivors of pancreatic ductal adenocarcinoma based on real-world data. Sci. Rep. 2020, 10, 16425. [Google Scholar] [CrossRef] [PubMed]
- Keane, M.G.; Bramis, K.; Pereira, S.P.; Fusai, G.K. Systematic review of novel ablative methods in locally advanced pancreatic cancer. World J. Gastroenterol. 2014, 20, 2267–2278. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- American Cancer Society. Cancer Facts & Figures 2022; American Cancer Society: Atlanta, GA, USA, 2022. [Google Scholar]
- Latenstein, A.E.J.; van der Geest, L.G.M.; Bonsing, B.A.; Groot Koerkamp, B.; Haj Mohammad, N.; de Hingh, I.; de Meijer, V.E.; Molenaar, I.Q.; van Santvoort, H.C.; van Tienhoven, G.; et al. Nationwide trends in incidence, treatment and survival of pancreatic ductal adenocarcinoma. Eur. J. Cancer 2020, 125, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Rombouts, S.J.; Walma, M.S.; Vogel, J.A.; van Rijssen, L.B.; Wilmink, J.W.; Mohammad, N.H.; van Santvoort, H.C.; Molenaar, I.Q.; Besselink, M.G. Systematic Review of Resection Rates and Clinical Outcomes After FOLFIRINOX-Based Treatment in Patients with Locally Advanced Pancreatic Cancer. Ann. Surg. Oncol. 2016, 23, 4352–4360. [Google Scholar] [CrossRef]
- Chen, Y.G.; Pan, H.H.; Dai, M.S.; Lin, C.; Lu, C.S.; Su, S.L.; Chang, P.Y.; Huang, T.C.; Chen, J.H.; Wu, Y.Y.; et al. Impact of Comorbidity and Age on Determinants Therapeutic Strategies in Advanced Pancreatic Head Cancer Patients With Obstructive Jaundices. Medicine 2015, 94, e1298. [Google Scholar] [CrossRef]
- Lee, L.; Cheung, W.Y.; Atkinson, E.; Krzyzanowska, M.K. Impact of comorbidity on chemotherapy use and outcomes in solid tumors: A systematic review. J. Clin. Oncol. 2011, 29, 106–117. [Google Scholar] [CrossRef]
- Sun, H.; Ma, H.; Hong, G.; Sun, H.; Wang, J. Survival improvement in patients with pancreatic cancer by decade: A period analysis of the SEER database, 1981–2010. Sci. Rep. 2014, 4, 6747. [Google Scholar] [CrossRef]
- Willink, C.Y.; Jenniskens, S.F.M.; Klaassen, N.J.M.; Stommel, M.W.J.; Nijsen, J.F.W. Intratumoral injection therapies for locally advanced pancreatic cancer: Systematic review. BJS Open 2023, 7, zrad052. [Google Scholar] [CrossRef]
- Bakker, R.C.; Lam, M.; van Nimwegen, S.A.; Rosenberg, A.; van Es, R.J.J.; Nijsen, J.F.W. Intratumoral treatment with radioactive beta-emitting microparticles: A systematic review. J. Radiat. Oncol. 2017, 6, 323–341. [Google Scholar] [CrossRef] [PubMed]
- Han, B.J.; Murphy, J.D.; Qin, S.; Ye, J.; Uccello, T.P.; Garrett-Larsen, J.; Belt, B.A.; Prieto, P.A.; Egilmez, N.K.; Lord, E.M.; et al. Microspheres Encapsulating Immunotherapy Agents Target the Tumor-Draining Lymph Node in Pancreatic Ductal Adenocarcinoma. Immunol. Investig. 2020, 49, 808–823. [Google Scholar] [CrossRef] [PubMed]
- Ross, P.J.; Wasan, H.S.; Croagh, D.; Nikfarjam, M.; Nguyen, N.; Aghmesheh, M.; Nagrial, A.M.; Bartholomeusz, D.; Hendlisz, A.; Ajithkumar, T.; et al. Results of a single-arm pilot study of (32)P microparticles in unresectable locally advanced pancreatic adenocarcinoma with gemcitabine/nab-paclitaxel or FOLFIRINOX chemotherapy. ESMO Open 2021, 7, 100356. [Google Scholar] [CrossRef]
- Morsink, C.; Klaassen, N.; van de Maat, G.; Boswinkel, M.; Arranja, A.; Bruggink, R.; van Houwelingen, I.; Schaafsma, I.; Hesselink, J.W.; Nijsen, F.; et al. Quantitative CT imaging and radiation-absorbed dose estimations of 166Ho microspheres: Paving the way for clinical application. Eur. Radiol. Exp. 2024, 8, 116. [Google Scholar] [CrossRef]
- van de Maat, G.H.; Seevinck, P.R.; Elschot, M.; Smits, M.L.; de Leeuw, H.; van Het Schip, A.D.; Vente, M.A.; Zonnenberg, B.A.; de Jong, H.W.; Lam, M.G.; et al. MRI-based biodistribution assessment of holmium-166 poly(L-lactic acid) microspheres after radioembolisation. Eur. Radiol. 2013, 23, 827–835. [Google Scholar] [CrossRef]
- Smits, M.L.; Nijsen, J.F.; van den Bosch, M.A.; Lam, M.G.; Vente, M.A.; Mali, W.P.; van Het Schip, A.D.; Zonnenberg, B.A. Holmium-166 radioembolisation in patients with unresectable, chemorefractory liver metastases (HEPAR trial): A phase 1, dose-escalation study. Lancet Oncol. 2012, 13, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Roosen, J.; Westlund Gotby, L.E.L.; Arntz, M.J.; Futterer, J.J.; Janssen, M.J.R.; Konijnenberg, M.W.; van Wijk, M.W.M.; Overduin, C.G.; Nijsen, J.F.W. Intraprocedural MRI-based dosimetry during transarterial radioembolization of liver tumours with holmium-166 microspheres (EMERITUS-1): A phase I trial towards adaptive, image-controlled treatment delivery. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4705–4715. [Google Scholar] [CrossRef]
- Drescher, R.; Kohler, A.; Seifert, P.; Aschenbach, R.; Ernst, T.; Rauchfuss, F.; Freesmeyer, M. Clinical Results of Transarterial Radioembolization (TARE) with Holmium-166 Microspheres in the Multidisciplinary Oncologic Treatment of Patients with Primary and Secondary Liver Cancer. Biomedicines 2023, 11, 1831. [Google Scholar] [CrossRef]
- Kühnel, C.; Köhler, A.; Brachwitz, T.; Seifert, P.; Gühne, F.; Aschenbach, R.; Freudenberg, R.; Freesmeyer, M.; Drescher, R. Clinical Results of Holmium-166 Radioembolization with Personalized Dosimetry for the Treatment of Hepatocellular Carcinoma. J. Pers. Med. 2024, 14, 747. [Google Scholar] [CrossRef]
- Breedis, C.; Young, G. The blood supply of neoplasms in the liver. Am. J. Pathol. 1954, 30, 969–977. [Google Scholar]
- van Nimwegen, S.A.; Bakker, R.C.; Kirpensteijn, J.; van Es, R.J.J.; Koole, R.; Lam, M.; Hesselink, J.W.; Nijsen, J.F.W. Intratumoral injection of radioactive holmium (166Ho) microspheres for treatment of oral squamous cell carcinoma in cats. Vet. Comp. Oncol. 2017, 16, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Bakker, R.C.; van Es, R.J.J.; Rosenberg, A.; van Nimwegen, S.A.; Bastiaannet, R.; de Jong, H.; Nijsen, J.F.W.; Lam, M. Intratumoral injection of radioactive holmium-166 microspheres in recurrent head and neck squamous cell carcinoma: Preliminary results of first use. Nucl. Med. Commun. 2018, 39, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- DuFort, C.C.; DelGiorno, K.E.; Carlson, M.A.; Osgood, R.J.; Zhao, C.; Huang, Z.; Thompson, C.B.; Connor, R.J.; Thanos, C.D.; Scott Brockenbrough, J.; et al. Interstitial Pressure in Pancreatic Ductal Adenocarcinoma Is Dominated by a Gel-Fluid Phase. Biophys. J. 2016, 110, 2106–2119. [Google Scholar] [CrossRef] [PubMed]
- Order, S.E.; Siegel, J.A.; Principato, R.; Zeiger, L.E.; Johnson, E.; Lang, P.; Lustig, R.; Wallner, P.E. Selective tumor irradiation by infusional brachytherapy in nonresectable pancreatic cancer: A phase I study. Int. J. Radiat. Oncol. Biol. Phys. 1996, 36, 1117–1126. [Google Scholar] [CrossRef]
- Rosemurgy, A.; Luzardo, G.; Cooper, J.; Bowers, C.; Zervos, E.; Bloomston, M.; Al-Saadi, S.; Carroll, R.; Chheda, H.; Carey, L.; et al. 32P as an adjunct to standard therapy for locally advanced unresectable pancreatic cancer: A randomized trial. J. Gastrointest. Surg. 2008, 12, 682–688. [Google Scholar] [CrossRef]
- Westlin, J.E.; Andersson-Forsman, C.; Garske, U.; Linne, T.; Aas, M.; Glimelius, B.; Lindgren, P.G.; Order, S.E.; Nilsson, S. Objective responses after fractionated infusional brachytherapy of unresectable pancreatic adenocarcinomas. Cancer 1997, 80, 2743–2748. [Google Scholar] [CrossRef]
- Bhutani, M.S.; Klapman, J.B.; Tuli, R.; El-Haddad, G.E.; Hoffe, S.; Wong, F.C.L.; Fogelman, D.R.; Lo, S.; Nissen, N.N.; Hendifar, A.E.; et al. OncoPaC-1: An Open-label, Single-Arm Pilot Study of Phosphorus-32 Microparticles Brachytherapy in Combination with Gemcitabine +/- Nab-Paclitaxel in Unresectable Locally Advanced Pancreatic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, E236–E237. [Google Scholar] [CrossRef]
- Peng, M.; Ying, Y.; Zhang, Z.; Liu, L.; Wang, W. Reshaping the Pancreatic Cancer Microenvironment at Different Stages with Chemotherapy. Cancers 2023, 15, 2448. [Google Scholar] [CrossRef]
- Westlund Gotby, L.E.L.; Lobeek, D.; Roosen, J.; de Bakker, M.; Konijnenberg, M.W.; Nijsen, J.F.W. Accuracy of holmium-166 SPECT/CT quantification over a large range of activities. EJNMMI Phys. 2024, 11, 78. [Google Scholar] [CrossRef]
- van der Sijde, F.; van Dam, J.L.; Groot Koerkamp, B.; Haberkorn, B.C.M.; Homs, M.Y.V.; Mathijssen, D.; Besselink, M.G.; Wilmink, J.W.; van Eijck, C.H.J. Treatment Response and Conditional Survival in Advanced Pancreatic Cancer Patients Treated with FOLFIRINOX: A Multicenter Cohort Study. J. Oncol. 2022, 2022, 8549487. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Holmium-166 Microsphere | Phosphorus-32 Microparticle |
|---|---|---|
| Material | Poly L-lactic acid | Silicon |
| Diameter | 30 µm (15–60 µm) | 30 µm (15–50 µm) |
| Isotope | Holmium-166 | Phosphorus-32 |
| Half-life | 26.8 h | 14.27 days |
| Emission type (yield) | Beta (93.3%), gamma (6.7%) | Beta (100%) |
| Maximum beta energy | 1.85 MeV | 1.711 MeV |
| Mean β− penetration | 2.5 mm | 2.76 mm |
| Maximum β− penetration | 8.7 mm | 8.2 mm |
| Imaging modalities | SPECT, CT, MRI | Bremsstrahlung SPECT |
| Parameter | Limit | Unit |
|---|---|---|
| Syringe volume | 3.0 | mL |
| Minimal rotation time | 120 | seconds |
| Intermittent rotation time 1 | 10 | seconds |
| Rotation speed | 60 | RPM |
| Minimal flush volume | 1.0 | mL |
| Minimal injection volume without tube | 0.3 | mL |
| Minimal injection volume with tube | 0.5 | mL |
| Injection speed | 0.2 | mL/s |
| Parameter | Limit | Unit |
|---|---|---|
| Tumor volume 1 | 2.5–15.6 | mL |
| Maximum injection volume | 20.0 | % of tumor volume |
| Maximum syringe angle to horizontal | 10.0 | Degrees |
| Number of needle insertions | 1–3 | - |
| Number of deposits | 1–3 | - |
| Volume per deposit 1 | 0.3–1.0 | mL |
| Holmium microsphere concentration in syringe 1 | 5.0–50.0 | mg/mL |
| Needle diameter 1 | 18–21 | Gauge |
| Needle length 1 | 50–150 | mm |
| Characteristics | Unit | Sample 1 | Sample 2 | Sample 3 | Sample 4 | Sample 5 | Sample 6 | Sample 7 | Sample 8 | Sample 9 | Sample 10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tumor volume | mL | 14.3 | 6.7 | 9.6 | 2.5 | 15.6 | 3.6 | 5.6 | 11.6 | 7.1 | 2.5 | |
| Extratumoral leakage observed | Yes/no | yes | yes | no | no | no | yes | no | no | yes | yes | |
| Observation remark | - | Over fractionated deposits | Needle overshoot | - | HVC 2 instead of injection fluid | - | Intentionally increased injection volume | Needle blockage due to syringe angle | - | Leakage through pancreatic duct | Intentionally increased injection volume | |
| Image guidance | - | - | - | US | US | US | US + CT | US + CT | US + CT | US + CT | US + CT | |
| Injection volume (as % of tumor volume) | mL (%) | 4.5 (31) | 2.3 (35) | 1.8 (19) | 0.2 (8) | 3.0 (19) | 3.0 (83) | 0.7 (13) | 2.0 (17) | 0.7 (10) | 1.0 (40) | |
| Number of needle insertions | - | 13 | 5 | 3 | 1 | 3 | 1 | 1 | 2 | 1 | 2 | |
| Number of deposits × volume per deposit | mL | 45 × 0.1 | 3 × 0.5 2 × 0.3 | 1 × 0.8 2 × 0.5 | 1 × 0.2 | 3 × 1.0 | 6 × 0.5 | 1 × 0.7 | 2 × 1.0 | 1 × 0.7 | 2 × 0.5 | |
| Concentration of 165HoMSs in syringe | mg/mL | 5.0 | 5.0 | 5.0 | 10.0 | 10.0 | 10.0 | 20.0 | 20.0 | 25.0 | 25.0 | 50.0 |
| HoMSs injected 1 | mg (mg/mL) | 18.5 (4.1) | 9.4 (4.1) | 7.4 (4.1) | 2.0 (10.0) 2 | 24.6 (8.2) | 24.6 (8.2) | 11.5 (16.4) | 32.8 (16.4) | 13.4 (20.5) | 10.3 (20.5) | 20.5 (41.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willink, C.Y.; Jenniskens, S.F.M.; Klaassen, N.J.M.; Stommel, M.W.J.; van Laarhoven, C.J.H.M.; Fütterer, J.J.; Nijsen, J.F.W. Development of an Intratumoral Holmium Microsphere Injection Method in Ex Vivo Human Pancreatic Ductal Adenocarcinoma: A Preclinical Feasibility Study. Cancers 2025, 17, 1028. https://doi.org/10.3390/cancers17061028
Willink CY, Jenniskens SFM, Klaassen NJM, Stommel MWJ, van Laarhoven CJHM, Fütterer JJ, Nijsen JFW. Development of an Intratumoral Holmium Microsphere Injection Method in Ex Vivo Human Pancreatic Ductal Adenocarcinoma: A Preclinical Feasibility Study. Cancers. 2025; 17(6):1028. https://doi.org/10.3390/cancers17061028
Chicago/Turabian StyleWillink, Coen Ysbrand, Sjoerd Franciscus Maria Jenniskens, Nienke Johanna Maria Klaassen, Martijn Willem Jan Stommel, Cornelis Johannes Henricus Martinus van Laarhoven, Jurgen J. Fütterer, and Johannes Frank Wilhelmus Nijsen. 2025. "Development of an Intratumoral Holmium Microsphere Injection Method in Ex Vivo Human Pancreatic Ductal Adenocarcinoma: A Preclinical Feasibility Study" Cancers 17, no. 6: 1028. https://doi.org/10.3390/cancers17061028
APA StyleWillink, C. Y., Jenniskens, S. F. M., Klaassen, N. J. M., Stommel, M. W. J., van Laarhoven, C. J. H. M., Fütterer, J. J., & Nijsen, J. F. W. (2025). Development of an Intratumoral Holmium Microsphere Injection Method in Ex Vivo Human Pancreatic Ductal Adenocarcinoma: A Preclinical Feasibility Study. Cancers, 17(6), 1028. https://doi.org/10.3390/cancers17061028