
MRI-Guided Multi-Catheter High-Dose-Rate Interstitial Brachytherapy for Uterine Cervical Cancer

 ,
,  , , , , ,
, , , , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient and Treatment
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MRI | Magnetic resonance imaging |
| ISBT | Interstitial brachytherapy |
| ICBT | Intracavitary brachytherapy |
| ICISBT | Intracavitary/interstitial brachytherapy |
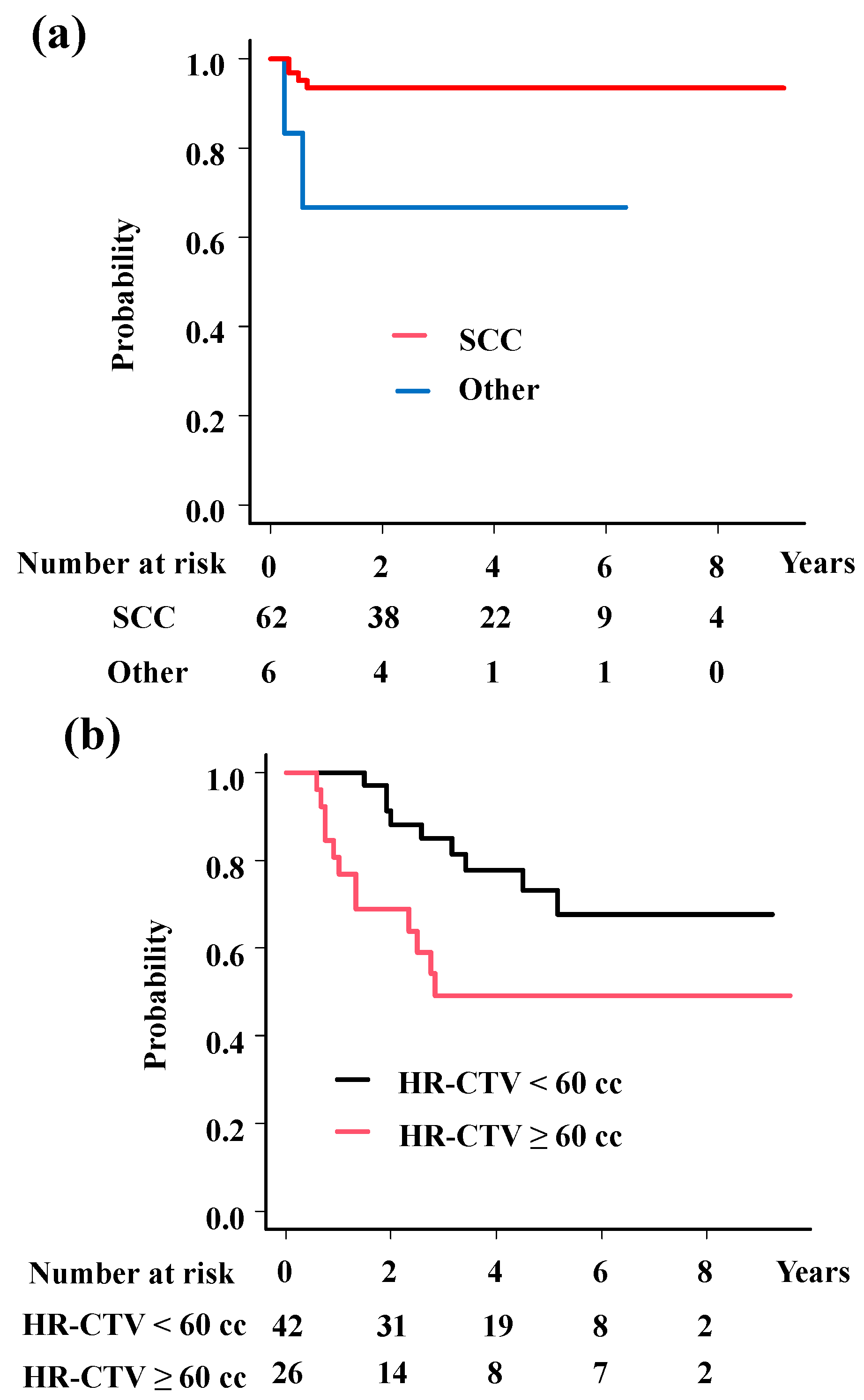
| HR-CTV | High-risk clinical target volume |
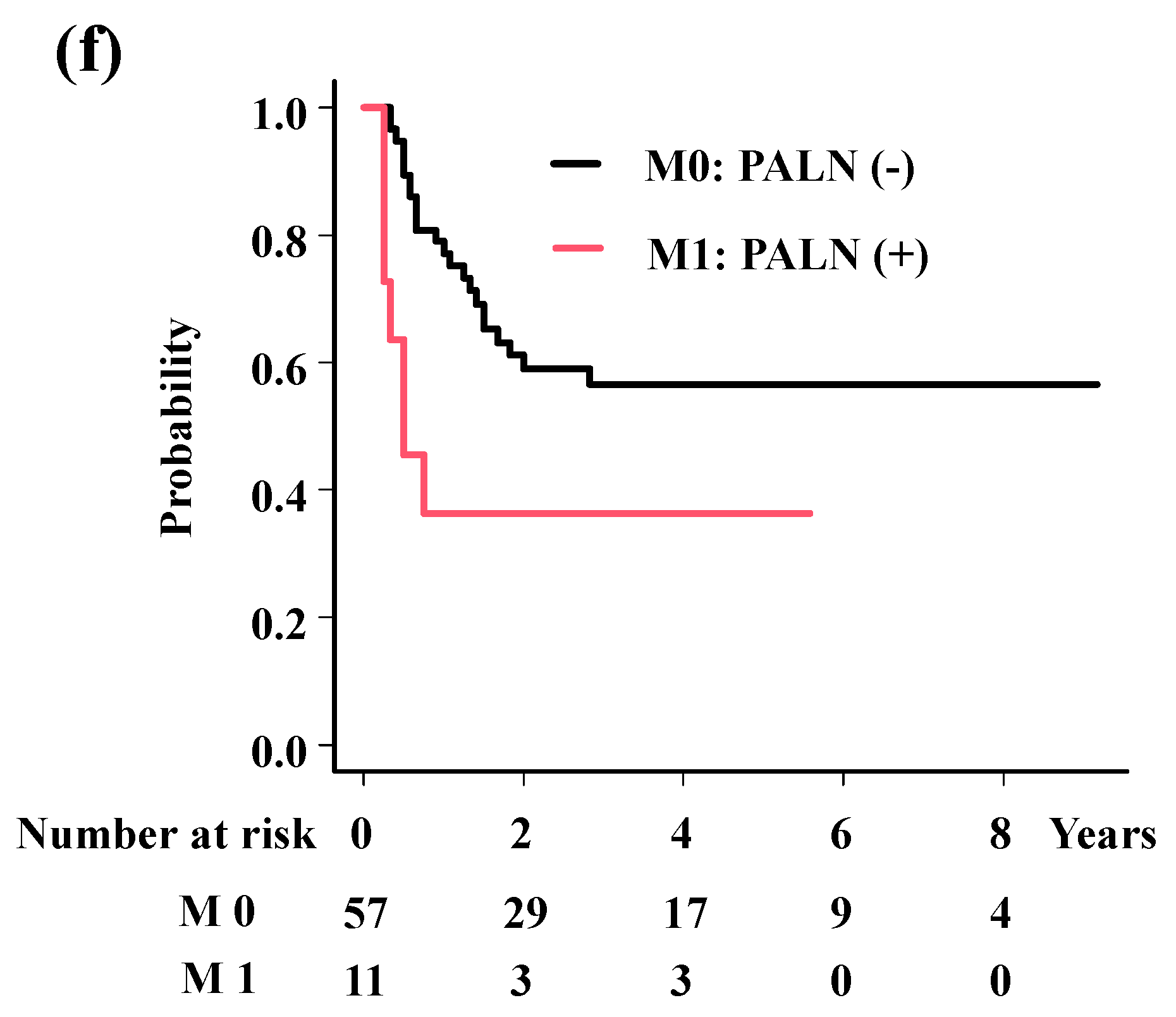
| PALN | Para-aortic lymph node |
| CS | Center-shielded |
| EBRT | External beam radiotherapy |
| EQD2 | The equivalent dose in 2 Gy fractions |
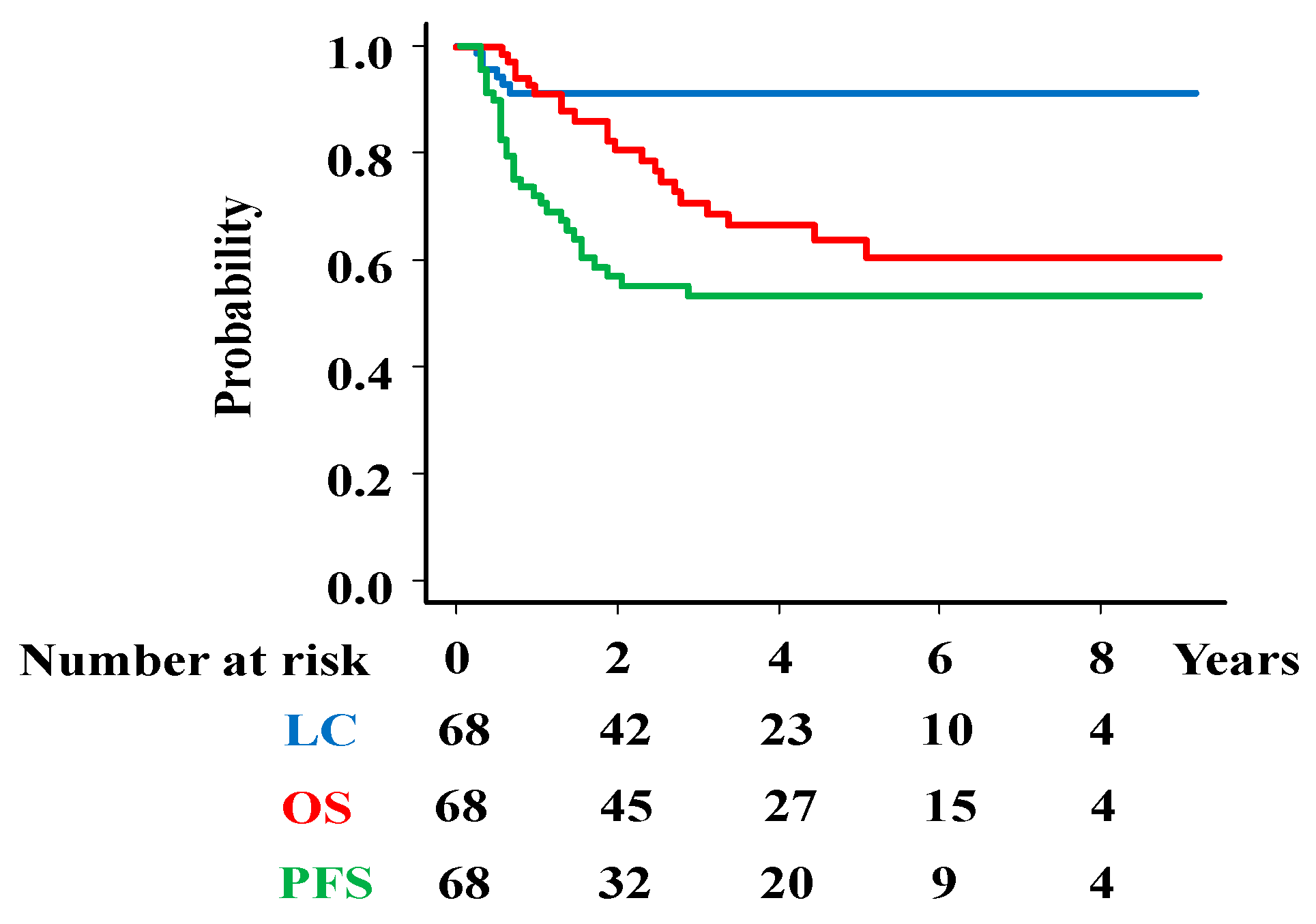
| OS | Overall survival |
| PFS | Progression-free survival |
| LC | Local control |
| OTT | Overall treatment time |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Green, J.A.; Kirwan, J.M.; Tierney, J.F.; Symonds, P.; Fresco, L.; Collingwood, M.; Williams, C.J. Survival and recurrence after concomitant chemotherapy and radiotherapy for cancer of the uterine cervix: A systematic review and meta-analysis. Lancet 2001, 358, 781–786. [Google Scholar] [CrossRef]
- Sturdza, A.; Pötter, R.; Fokdal, L.U.; Haie-Meder, C.; Tan, L.T.; Mazeron, R.; Petric, P.; Šegedin, B.; Jurgenliemk-Schulz, I.M.; Nomden, C.; et al. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother. Oncol. 2016, 120, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Haie-Meder, C.; Pötter, R.; Van Limbergen, E.; Briot, E.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Hellebust, T.P.; Kirisits, C.; Lang, S.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother. Oncol. 2005, 74, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Kirisits, C.; Lang, S.; Dimopoulos, J.; Berger, D.; Georg, D.; Pötter, R. The Vienna applicator for combined intracavitary and interstitial brachytherapy of cervical cancer: Design, application, treatment planning, and dosimetric results. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, H.; Inoue, T.; Ikeda, H.; Tang, J.T.; Murayama, S.; Teshima, T.; Otani, M.; Kozuka, T. High-dose-rate remote afterloading intestinal radiotherapy employing the template technique for recurrent cancer in the pelvic area. Strahlenther. Onkol. 1993, 169, 481–485. [Google Scholar] [PubMed]
- Beriwal, S.; Bhatnagar, A.; Heron, D.E.; Selvaraj, R.; Mogus, R.; Kim, H.; Gerszten, K.; Kelley, J.; Edwards, R.P. High-dose-rate inter stitial brachytherapy for gynecologic malignancies. Brachytherapy 2006, 5, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Demanes, D.J.; Rodriguez, R.R.; Bendre, D.D.; Ewing, T.L. High dose rate transperineal interstitial brachytherapy for cervical cancer: High pelvic control and low complication rates. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 105–112. [Google Scholar] [CrossRef]
- Kuipers, T.; Hoekstra, C.J.; van’t Riet, A.; Mak, A.C.; Vonk, E.J.; Elders, L.H.; Koster, K.; Pop, L.A.M. HDR brachytherapy applied to cervical carcinoma with moderate lateral expansion: Modified principles of treatment. Radiother. Oncol. 2001, 58, 25–30. [Google Scholar] [CrossRef]
- Yoshida, K.; Yamazaki, H.; Takenaka, T.; Kotsuma, T.; Yoshida, M.; Furuya, S.; Tanaka, E.; Uegaki, T.; Kuriyama, K.; Matsumoto, H.; et al. A dose-volume analysis of magnetic resonance imaging-aided high-dose-rate image-based interstitial brachytherapy for uterine cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Kokabu, T.; Masui, K.; Tarumi, Y.; Noguchi, N.; Aoyama, K.; Kataoka, H.; Matsushima, H.; Yoriki, K.; Shimizu, D.; Yamazaki, H.; et al. 3D-Image-Guided Multi-Catheter Interstitial Brachytherapy for Bulky and High-Risk Stage IIB-IVB Cervical Cancer. Cancers 2022, 14, 1257. [Google Scholar] [CrossRef]
- Takenaka, T.; Yamazaki, H.; Suzuki, G.; Masui, K.; Shimizu, D.; Kotsuma, T.; Tanaka, E.; Yoshida, K.; Yamada, K. Initial tumor volume as an important predictor for indication of intra-cavitary brachytherapy, intra-cavitary/interstitial brachytherapy, and multi-catheter sole interstitial brachytherapy in cervical cancer patients treated with chemoradiotherapy. J. Contemp. Brachytherapy 2023, 15, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Nag, S.; Erickson, B.; Thomadsen, B.; Orton, C.; Demanes, J.D.; Petereit, D.; Society, A.B. The American Brachy therapy Society recommendations for high-dose-rate brachy therapy for carcinoma of the cervix. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 201–211. [Google Scholar] [CrossRef]
- Pötter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother. Oncol. 2006, 78, 67–77. [Google Scholar] [CrossRef]
- Viswanathan, A.N.; Beriwal, S.; De Los Santos, J.F.; Demanes, D.J.; Gaffney, D.; Hansen, J.; Jones, E.; Kirisits, C.; Thomadsen, B.; Erickson, B. American Brachytherapy Society. American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix. Part II: High-dose-rate brachytherapy. Brachytherapy 2012, 11, 47–52. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Hande, V.; Chopra, S.; Kalra, B.; Abdel-Wahab, M.; Kannan, S.; Tanderup, K.; Grover, S.; Zubizarreta, E.; Rubio, J.A.P. Point-A vs. volume-based brachytherapy for the treatment of cervix cancer: A meta-analysis. Radiother. Oncol. 2022, 170, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Pötter, R.; Tanderup, K.; Schmid, M.P.; Jürgenliemk-Schulz, I.; Haie-Meder, C.; Fokdal, L.U.; Sturdza, A.E.; Hoskin, P.; Mahantshetty, U.; Segedin, B.; et al. MRI-guided adaptive brachytherapy in locally advanced cervical cancer (EMBRACE-I): A multicentre prospective cohort study. Lancet Oncol. 2021, 22, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Schmid, M.P.; Lindegaard, J.C.; Mahantshetty, U.; Tanderup, K.; Jürgenliemk-Schulz, I.; Haie-Meder, C.; Fokdal, L.U.; Sturdza, A.; Hoskin, P.; Segedin, B.; et al. Risk Factors for Local Failure Following Chemoradiation and Magnetic Resonance Image-Guided Brachytherapy in Locally Advanced Cervical Cancer: Results from the EMBRACE-I Study. J. Clin. Oncol. 2023, 41, 1933–1942. [Google Scholar] [CrossRef] [PubMed]
- Mazeron, R.; Castelnau-Marchand, P.; Dumas, I.; del Campo, E.R.; Kom, L.K.; Martinetti, F.; Farha, G.; Tailleur, A.; Morice, P.; Chargari, C.; et al. Impact of treatment time and dose escalation on local control in locally advanced cervical cancer treated by chemoradiation and image-guided pulsed-dose rate adaptive brachytherapy. Radiother. Oncol. 2015, 114, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, D.; Xiang, Y.; Hasegawa, K.; Scambia, G.; Leiva, M.; Ramos-Elias, P.; Acevedo, A.; Sukhin, V.; Cloven, N.; de Santana Gomes, A.J.P.; et al. Pembrolizumab or placebo with chemoradiotherapy followed by pembrolizumab or placebo for newly diagnosed, high-risk, locally advanced cervical cancer (ENGOT-cx11/GOG-3047/KEYNOTE-A18): A randomised, double-blind, phase 3 clinical trial. Lancet 2024, 403, 1341–1350. [Google Scholar] [CrossRef]
- Okazaki, S.; Murata, K.; Noda, S.E.; Kumazaki, Y.; Hirai, R.; Igari, M.; Abe, T.; Komatsu, S.; Nakano, T.; Kato, S. Dose-volume parameters and local tumor control in cervical cancer treated with central-shielding external-beam radiotherapy and CT-based image-guided brachytherapy. J. Radiat. Res. 2019, 60, 490–500. [Google Scholar] [CrossRef]
- Tamaki, T.; Noda, S.E.; Ohno, T.; Kumazaki, Y.; Kato, S.; Nakano, T. Dose-volume histogram analysis of composite EQD2 dose distributions using the central shielding technique in cervical cancer radiotherapy. Brachytherapy 2016, 15, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, T. Midline Block (Central Shielding). In Brachytherapy; Yoshioka, Y., Itami, J., Oguchi, M., Nakano, T., Eds.; Springer: Singapore, 2019; pp. 63–75. [Google Scholar] [CrossRef]
- Lindegaard, J.C.; Petric, P.; Schmid, M.P.; Nesvacil, N.; Haie-Meder, C.; Fokdal, L.U.; Sturdza, A.E.; Hoskin, P.; Mahantshetty, U.; Segedin, B.; et al. Prognostic Implications of Uterine Cervical Cancer Regression During Chemoradiation Evaluated by the T-Score in the Multicenter EMBRACE I Study. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 379–389. [Google Scholar] [PubMed]
- Ohtaka, T.; Ando, K.; Oike, T.; Noda, S.E.; Kaminuma, T.; Murata, K.; Ohno, T. The prognostic effect of tumor volume, reduction ratio, and cumulative doses on external beam radiotherapy with central-shielding method and image-guided adaptive brachytherapy for cervical cancer. Front. Oncol. 2024, 14, 1366777. [Google Scholar] [CrossRef]
- Schernberg, A.; Bockel, S.; Annede, P.; Fumagalli, I.; Escande, A.; Mignot, F.; Kissel, M.; Morice, P.; Bentivegna, E.; Gouy, S.; et al. Tumor Shrinkage During Chemoradiation in Locally Advanced Cervical Cancer Patients: Prognostic Significance, and Impact for Image-Guided Adaptive Brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Cordoba, A.; Durand, B.; Escande, A.; Taieb, S.; Amor, M.B.H.; Le Deley, M.C.; Michel, A.; Le Tinier, F.; Hudry, D.; Martinez, C.; et al. Prognostic impact of tumor size reduction assessed by magnetic resonance imaging after radiochemotherapy in patients with locally advanced cervical cancer. Front. Oncol. 2022, 12, 1046087. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wang, S.; Ye, W.; Wang, R.; Tan, M.; Zhang, H.; Zhou, J.; Li, M.; Wei, L.; Xu, P.; et al. The Prognostic Value of Tumor Size, Volume and Tumor Volume Reduction Rate During Concurrent Chemoradiotherapy in Patients With Cervical Cancer. Front. Oncol. 2022, 12, 934110. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Angeles, M.A.; Baissas, P.; Leblanc, E.; Lusque, A.; Ferron, G.; Ducassou, A.; Martínez-Gómez, C.; Querleu, D.; Martinez, A. Magnetic resonance imaging after external beam radiotherapy and concurrent chemotherapy for locally advanced cervical cancer helps to identify patients at risk of recurrence. Int. J. Gynecol. Cancer 2019, 29, 480–486. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Group | PTNO (%) or Median [Range] |
|---|---|---|
| n = 68 | ||
| Age | 64.00 [28.00, 84.00] | |
| Histology | Squamous cell carcinoma | 62 (91.2) |
| Other * | 6 (8.8) | |
| T category | 2 | 9 (13.2) |
| 3 | 44 (64.7) | |
| 4 | 15 (22.1) | |
| N category | 0 | 19 (27.9) |
| 1 | 49 (72.1) | |
| M category (paraaortic lymph node) | 0 | 57 (83.8) |
| 1 | 11 (16.2) | |
| Stage classification | 2A | 1 (1.5) |
| 2B | 1 (1.5) | |
| 3A | 6 (8.8) | |
| 3B | 35 (51.5) | |
| 4A | 14 (20.6) | |
| 4B | 11 (16.2) | |
| Treatment | ||
| EBRT (Dose) | (Gy) | 56.00 [44.00, 64.00] |
| EBRT (fractions) | 30.00 [20.00, 33.00] | |
| Whole pelvis | (Gy) | 50.00 [30.00, 50.47] |
| Central shield | (Gy) | 4.00 [0.00, 30.00] |
| ISBT (dose/ fraction) | (Gy) | 6.00 [5.00, 6.00] |
| ISBT total dose (dose) | 25.00 [24.00, 30.00] | |
| D90 of brachytherapy | (Gy) | 6.78 [5.03, 8.03] |
| HR-CTV volume at brachytherapy | (cc) | 53.20 [16.34, 147.03] |
| Total EQD2 | (Gy) | 89.5 [80–100] |
| Overall treatment time | (day) | 51.00 [31.00, 82.00] |
| Concurrent chemotherapy | No | 11 (16.2) |
| Yes | 57 (83.8) | |
| CDDP | 42 (61.8) | |
| Other drug | 15 (22.1) |
| Endpoint | Variable | Category | PTNO | 3-Year (%) | Hazard Ratio (95%CI) | p-Value |
|---|---|---|---|---|---|---|
| Local control | Histology | Squamous cell carcinoma | 62 | 93.5 | 0.16 (0.03–0.9) | 0.037 |
| Others | 6 | 66.7 | ||||
| Overall survival | HR-CTV volume | <60 cc | 53 | 77.1 | 5.76 (2.17–15.27) | 0.00044 |
| ≥60 cc | 15 | 49.5 | ||||
| OTT | <50 days | 30 | 85.9 | 6.69 (2.21–20.26) | 0.00078 | |
| ≥50 days | 38 | 57.5 | ||||
| Progression-free survival | HR-CTV volume | <60 cc | 53 | 58 | 2.19 (1.05–4.57) | 0.036 |
| ≥60 cc | 15 | 37.5 | ||||
| OTT | <50 days | 30 | 64.8 | 2.21 (1.02–4.77) | 0.045 | |
| ≥50 days | 38 | 43.3 | ||||
| M category | Para-aortic LN (+) | 11 | 36.4 | 2.47 (1.04–5.85) | 0.04 | |
| Para-aortic LN (−) | 57 | 56.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamazaki, H.; Masui, K.; Yoshida, K.; Suzuki, G.; Takenaka, T.; Yamada, K.; Kotsuma, T.; Takaoka, Y.; Fujiwara, K.; Tanaka, Y.; et al. MRI-Guided Multi-Catheter High-Dose-Rate Interstitial Brachytherapy for Uterine Cervical Cancer. Cancers 2025, 17, 770. https://doi.org/10.3390/cancers17050770
Yamazaki H, Masui K, Yoshida K, Suzuki G, Takenaka T, Yamada K, Kotsuma T, Takaoka Y, Fujiwara K, Tanaka Y, et al. MRI-Guided Multi-Catheter High-Dose-Rate Interstitial Brachytherapy for Uterine Cervical Cancer. Cancers. 2025; 17(5):770. https://doi.org/10.3390/cancers17050770
Chicago/Turabian StyleYamazaki, Hideya, Koji Masui, Ken Yoshida, Gen Suzuki, Tadashi Takenaka, Kei Yamada, Tadayuki Kotsuma, Yuji Takaoka, Kei Fujiwara, Yutaka Tanaka, and et al. 2025. "MRI-Guided Multi-Catheter High-Dose-Rate Interstitial Brachytherapy for Uterine Cervical Cancer" Cancers 17, no. 5: 770. https://doi.org/10.3390/cancers17050770
APA StyleYamazaki, H., Masui, K., Yoshida, K., Suzuki, G., Takenaka, T., Yamada, K., Kotsuma, T., Takaoka, Y., Fujiwara, K., Tanaka, Y., & Tanaka, E. (2025). MRI-Guided Multi-Catheter High-Dose-Rate Interstitial Brachytherapy for Uterine Cervical Cancer. Cancers, 17(5), 770. https://doi.org/10.3390/cancers17050770