
Impact of Preoperative Yttrium-90 Transarterial Radioembolization on Patients Undergoing Right or Extended Right Hepatectomy for Hepatocellular Carcinoma

 , , , and
, , , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
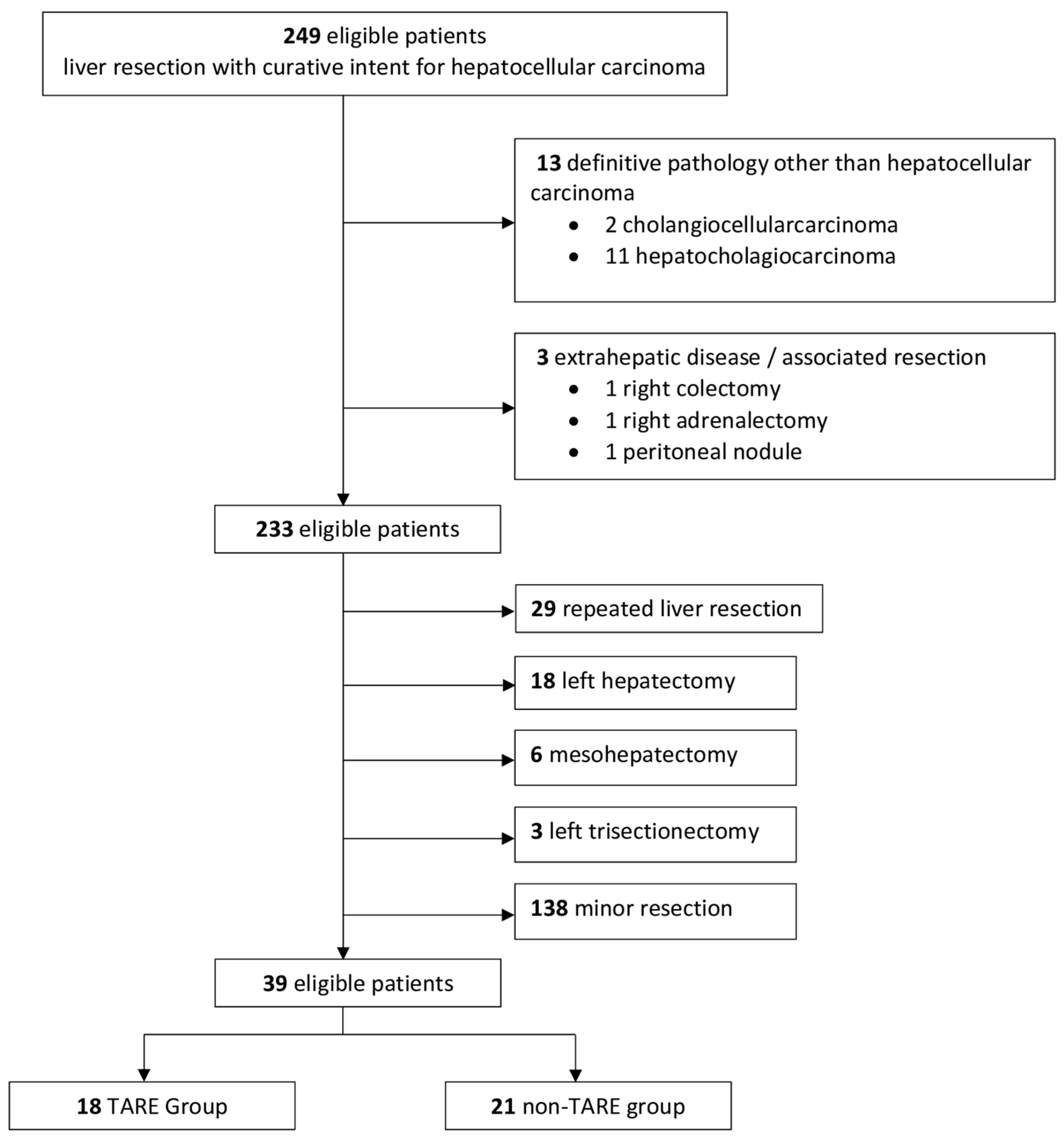
2.1. Patient Selection
2.2. Diagnosis and Preoperative Staging
2.3. TARE Protocol and Technique
2.4. Surgical Technique
2.5. Intra- and Postoperative Outcomes
2.6. Follow-Up
2.7. Definitions of Long-Term Outcomes
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Intraoperative Outcomes
3.3. Postoperative Outcomes and Histological Findings
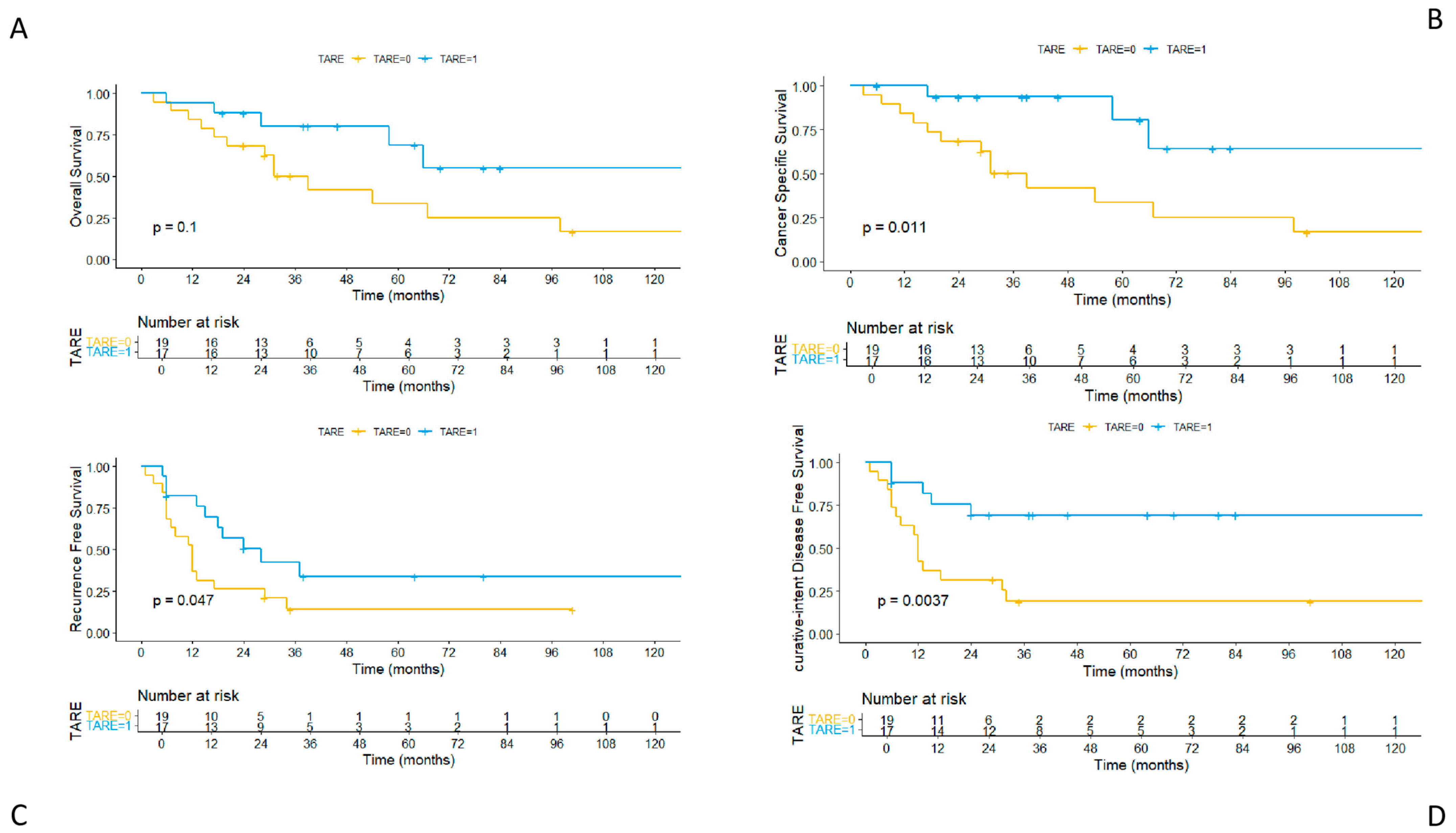
3.4. Long-Term Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HCC | Hepatocellular carcinoma |
| TARE | Yttrium-90 transarterial radioembolization |
| FLR | Future liver remnant |
| PVTT | Portal vein tumor thrombosis |
| OS | Overall survival |
| CSS | Cancer-specific survival |
| RFS | Recurrence-free survival |
| ciDFS | Curative-intent disease-free survival |
| AFP | Alpha-fetoprotein |
| PHLF | Post-hepatectomy liver failure |
References
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular Carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer Statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Llovet, J.M.; Yarchoan, M.; Mehta, N.; Heimbach, J.K.; Dawson, L.A.; Jou, J.H.; Kulik, L.M.; Agopian, V.G.; Marrero, J.A.; et al. AASLD Practice Guidance on Prevention, Diagnosis, and Treatment of Hepatocellular Carcinoma. Hepatology 2023, 78, 1922–1965. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the Management of Hepatocellular Carcinoma. J. Hepatol. 2025, 82, 315–374. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Taddei, T.H.; Brown, D.B.; Yarchoan, M.; Mendiratta-Lala, M.; Llovet, J.M. Critical Update: AASLD Practice Guidance on Prevention, Diagnosis, and Treatment of Hepatocellular Carcinoma. Hepatology 2025, 82, 272–274. [Google Scholar] [CrossRef]
- Daher, D.; Seif El Dahan, K.; Cano, A.; Gonzales, M.; Ransom, C.; Jaurez, E.; Carranza, O.; Quirk, L.; Morgan, T.; Gopal, P.; et al. Hepatocellular Carcinoma Surveillance Patterns and Outcomes in Patients With Cirrhosis. Clin. Gastroenterol. Hepatol. 2024, 22, 295–304.e2. [Google Scholar] [CrossRef]
- Brown, Z.J.; Tsilimigras, D.I.; Ruff, S.M.; Mohseni, A.; Kamel, I.R.; Cloyd, J.M.; Pawlik, T.M. Management of Hepatocellular Carcinoma: A Review. JAMA Surg. 2023, 158, 410–420. [Google Scholar] [CrossRef]
- Valery, P.C.; Laversanne, M.; Clark, P.J.; Petrick, J.L.; McGlynn, K.A.; Bray, F. Projections of Primary Liver Cancer to 2030 in 30 Countries Worldwide. Hepatology 2018, 67, 600–611. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Rimassa, L.; Chan, S.L.; Sangro, B.; Lau, G.; Kudo, M.; Reig, M.; Breder, V.; Ryu, M.-H.; Ostapenko, Y.; Sukeepaisarnjaroen, W.; et al. Five-Year Overall Survival Update from the HIMALAYA Study of Tremelimumab plus Durvalumab in Unresectable HCC. J. Hepatol. 2025, 82, 1257–1265. [Google Scholar] [CrossRef]
- Vitale, A.; Romano, P.; Cillo, U.; Writing Group for the HE.RC.O.LE.S Collaborative Group; Writing Group for the ITA.LI.CA Collaborative Group; HE.RC.O.LE.S and ITA.LI.CA Collaborative Groups; Lauterio, A.; Sangiovanni, A.; Cabibbo, G.; Missale, G.; et al. Liver Resection vs Nonsurgical Treatments for Patients With Early Multinodular Hepatocellular Carcinoma. JAMA Surg. 2024, 159, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Imamura, H.; Seyama, Y.; Kokudo, N.; Maema, A.; Sugawara, Y.; Sano, K.; Takayama, T.; Makuuchi, M. One Thousand Fifty-Six Hepatectomies without Mortality in 8 Years. Arch. Surg. 2003, 138, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Kenjo, A.; Miyata, H.; Gotoh, M.; Kitagawa, Y.; Shimada, M.; Baba, H.; Tomita, N.; Kimura, W.; Sugihara, K.; Mori, M. Risk Stratification of 7,732 Hepatectomy Cases in 2011 from the National Clinical Database for Japan. J. Am. Coll. Surg. 2014, 218, 412–422. [Google Scholar] [CrossRef]
- Zaydfudim, V.M.; Kerwin, M.J.; Turrentine, F.E.; Bauer, T.W.; Adams, R.B.; Stukenborg, G.J. The Impact of Chronic Liver Disease on the Risk Assessment of ACS NSQIP Morbidity and Mortality after Hepatic Resection. Surgery 2016, 159, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Vitale, A.; Cabibbo, G.; Iavarone, M.; Viganò, L.; Pinato, D.J.; Ponziani, F.R.; Lai, Q.; Casadei-Gardini, A.; Celsa, C.; Galati, G.; et al. Personalised Management of Patients with Hepatocellular Carcinoma: A Multiparametric Therapeutic Hierarchy Concept. Lancet Oncol. 2023, 24, e312–e322. [Google Scholar] [CrossRef]
- Salem, R.; Lewandowski, R.J.; Mulcahy, M.F.; Riaz, A.; Ryu, R.K.; Ibrahim, S.; Atassi, B.; Baker, T.; Gates, V.; Miller, F.H.; et al. Radioembolization for Hepatocellular Carcinoma Using Yttrium-90 Microspheres: A Comprehensive Report of Long-Term Outcomes. Gastroenterology 2010, 138, 52–64. [Google Scholar] [CrossRef]
- Garin, E.; Tselikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; de Baere, T.; Assenat, E.; Tacher, V.; Robert, C.; Terroir-Cassou-Mounat, M.; et al. Personalised versus Standard Dosimetry Approach of Selective Internal Radiation Therapy in Patients with Locally Advanced Hepatocellular Carcinoma (DOSISPHERE-01): A Randomised, Multicentre, Open-Label Phase 2 Trial. Lancet Gastroenterol. Hepatol. 2021, 6, 17–29. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Sposito, C.; Bhoori, S.; Romito, R.; Chiesa, C.; Morosi, C.; Maccauro, M.; Marchianò, A.; Bongini, M.; Lanocita, R.; et al. Yttrium-90 Radioembolization for Intermediate-Advanced Hepatocellular Carcinoma: A Phase 2 Study. Hepatology 2013, 57, 1826–1837. [Google Scholar] [CrossRef]
- Salem, R.; Johnson, G.E.; Kim, E.; Riaz, A.; Bishay, V.; Boucher, E.; Fowers, K.; Lewandowski, R.; Padia, S.A. Yttrium-90 Radioembolization for the Treatment of Solitary, Unresectable HCC: The LEGACY Study. Hepatology 2021, 74, 2342–2352. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Citterio, D.; Bhoori, S.; Bongini, M.; Miceli, R.; De Carlis, L.; Colledan, M.; Salizzoni, M.; Romagnoli, R.; Antonelli, B.; et al. Liver Transplantation in Hepatocellular Carcinoma after Tumour Downstaging (XXL): A Randomised, Controlled, Phase 2b/3 Trial. Lancet Oncol. 2020, 21, 947–956. [Google Scholar] [CrossRef]
- Donadon, M.; Torzilli, G. Parenchymal Sparing Anatomical Liver Resections for Hepatocellular Carcinoma. Hepatobiliary Surg. Nutr. 2024, 13, 706–708. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, T.; Fujiyama, Y.; Mishima, K.; Igarashi, K.; Nie, Y.; Berardi, G.; Alomari, M.; Colella, M.; Wakabayashi, G. Laparoscopically Limited Anatomic Liver Resections: A Single-Center Analysis for Oncologic Outcomes of the Conceptual Procedure. Ann. Surg. Oncol. 2024, 31, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
- Shindoh, J.; Makuuchi, M.; Matsuyama, Y.; Mise, Y.; Arita, J.; Sakamoto, Y.; Hasegawa, K.; Kokudo, N. Complete Removal of the Tumor-Bearing Portal Territory Decreases Local Tumor Recurrence and Improves Disease-Specific Survival of Patients with Hepatocellular Carcinoma. J. Hepatol. 2016, 64, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, S.; Makuuchi, M.; Kawasaki, S.; Kakazu, T. Criteria for Safe Hepatic Resection. Am. J. Surg. 1995, 169, 589–594. [Google Scholar] [CrossRef]
- Ikai, I.; Arii, S.; Okazaki, M.; Okita, K.; Omata, M.; Kojiro, M.; Takayasu, K.; Nakanuma, Y.; Makuuchi, M.; Matsuyama, Y.; et al. Report of the 17th Nationwide Follow-up Survey of Primary Liver Cancer in Japan. Hepatol. Res. 2007, 37, 676–691. [Google Scholar] [CrossRef]
- Kokudo, T.; Hasegawa, K.; Matsuyama, Y.; Takayama, T.; Izumi, N.; Kadoya, M.; Kudo, M.; Ku, Y.; Sakamoto, M.; Nakashima, O.; et al. Survival Benefit of Liver Resection for Hepatocellular Carcinoma Associated with Portal Vein Invasion. J. Hepatol. 2016, 65, 938–943. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- American Society of Anesthesiologists. ASA Physical Status Classification System. Last updated 2020. Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 5 April 2025).
- Tabone, M.; Calvo, A.; Russolillo, N.; Langella, S.; Carbonatto, P.; Lo Tesoriere, R.; Richetta, E.; Pellerito, R.; Ferrero, A. Downstaging Unresectable Hepatocellular Carcinoma by Radioembolization Using 90-Yttrium Resin Microspheres: A Single Center Experience. J. Gastrointest. Oncol. 2020, 11, 84–90. [Google Scholar] [CrossRef]
- Martelletti, C.; Ricotti, A.; Gesualdo, M.; Carucci, P.; Gaia, S.; Rolle, E.; Burlone, M.E.; Okolicsanyi, S.; Mattalia, A.; Pirisi, M.; et al. Radioembolization vs Sorafenib in Locally Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis: A Propensity Score and Bayesian Analysis. J. Dig. Dis. 2021, 22, 496–502. [Google Scholar] [CrossRef]
- Capussotti, L.; Ferrero, A.; Russolillo, N.; Langella, S.; Lo Tesoriere, R.; Viganò, L. Routine Anterior Approach during Right Hepatectomy: Results of a Prospective Randomised Controlled Trial. J. Gastrointest. Surg. 2012, 16, 1324–1332. [Google Scholar] [CrossRef]
- Ferrero, A.; Lo Tesoriere, R.; Russolillo, N. Ultrasound Liver Map Technique for Laparoscopic Liver Resections. World J. Surg. 2019, 43, 2607–2611. [Google Scholar] [CrossRef]
- Ferrero, A.; Russolillo, N.; Langella, S.; Forchino, F.; Stasi, M.; Fazio, F.; Lo Tesoriere, R. Ultrasound Liver Map Technique for Laparoscopic Liver Resections: Perioperative Outcomes Are Not Impaired by Technical Complexity. Updates Surg. 2019, 71, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Strasberg, S.M.; Phillips, C. Use and Dissemination of the Brisbane 2000 Nomenclature of Liver Anatomy and Resections. Ann. Surg. 2013, 257, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.-A. The Comprehensive Complication Index: A Novel Continuous Scale to Measure Surgical Morbidity. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef]
- Koch, M.; Garden, O.J.; Padbury, R.; Rahbari, N.N.; Adam, R.; Capussotti, L.; Fan, S.T.; Yokoyama, Y.; Crawford, M.; Makuuchi, M.; et al. Bile Leakage after Hepatobiliary and Pancreatic Surgery: A Definition and Grading of Severity by the International Study Group of Liver Surgery. Surgery 2011, 149, 680–688. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Maddern, G.; Koch, M.; Hugh, T.J.; Fan, S.T.; Nimura, Y.; Figueras, J.; Vauthey, J.-N.; et al. Post-Hepatectomy Haemorrhage: A Definition and Grading by the International Study Group of Liver Surgery (ISGLS). HPB 2011, 13, 528–535. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria; 2024. Available online: https://www.R-project.org/ (accessed on 5 April 2025).
- Vouche, M.; Lewandowski, R.J.; Atassi, R.; Memon, K.; Gates, V.L.; Ryu, R.K.; Gaba, R.C.; Mulcahy, M.F.; Baker, T.; Sato, K.; et al. Radiation Lobectomy: Time-Dependent Analysis of Future Liver Remnant Volume in Unresectable Liver Cancer as a Bridge to Resection. J. Hepatol. 2013, 59, 1029–1036. [Google Scholar] [CrossRef]
- Lewandowski, R.J.; Donahue, L.; Chokechanachaisakul, A.; Kulik, L.; Mouli, S.; Caicedo, J.; Abecassis, M.; Fryer, J.; Salem, R.; Baker, T. 90Y Radiation Lobectomy: Outcomes Following Surgical Resection in Patients with Hepatic Tumors and Small Future Liver Remnant Volumes. J. Surg. Oncol. 2016, 114, 99–105. [Google Scholar] [CrossRef]
- Gregory, J.; Tselikas, L.; Allimant, C.; de Baere, T.; Bargellini, I.; Bell, J.; Bilbao, J.I.; Bouvier, A.; Chapiro, J.; Chiesa, C.; et al. Defining Textbook Outcome for Selective Internal Radiation Therapy of Hepatocellular Carcinoma: An International Expert Study. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 921–928. [Google Scholar] [CrossRef]
- Ahmed, A.; Stauffer, J.A.; LeGout, J.D.; Burns, J.; Croome, K.; Paz-Fumagalli, R.; Frey, G.; Toskich, B. The Use of Neoadjuvant Lobar Radioembolization prior to Major Hepatic Resection for Malignancy Results in a Low Rate of Post Hepatectomy Liver Failure. J. Gastrointest. Oncol. 2021, 12, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Berardi, G.; Guglielmo, N.; Cucchetti, A.; Usai, S.; Colasanti, M.; Meniconi, R.L.; Ferretti, S.; Mariano, G.; Angrisani, M.; Sciuto, R.; et al. Transarterial Radioembolization Can Downstage Intermediate and Advanced Hepatocellular Carcinoma to Liver Transplantation. Transplantation 2025, 109, e54–e63. [Google Scholar] [CrossRef] [PubMed]
- Labgaa, I.; Tabrizian, P.; Titano, J.; Kim, E.; Thung, S.N.; Florman, S.; Schwartz, M.; Melloul, E. Feasibility and Safety of Liver Transplantation or Resection after Transarterial Radioembolization with Yttrium-90 for Unresectable Hepatocellular Carcinoma. HPB 2019, 21, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Meerun, M.A.; Allimant, C.; Rivière, B.; Herrero, A.; Panaro, F.; Assenat, E.; Cassinotto, C.; Mariano-Goulart, D.; Guiu, B. Large, Multifocal or Portal Vein-Invading Hepatocellular Carcinoma (HCC) Downstaged by Y90 Using Personalized Dosimetry: Safety, Pathological Results and Outcomes after Surgery. Hepatobiliary Surg. Nutr. 2023, 12, 351–365. [Google Scholar] [CrossRef]
- Gabr, A.; Abouchaleh, N.; Ali, R.; Baker, T.; Caicedo, J.; Katariya, N.; Abecassis, M.; Riaz, A.; Lewandowski, R.J.; Salem, R. Outcomes of Surgical Resection after Radioembolization for Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2018, 29, 1502–1510.e1. [Google Scholar] [CrossRef]
- Son, S.Y.; Geevarghese, R.; Marinelli, B.; Zhao, K.; Covey, A.; Maxwell, A.; Wei, A.C.; Jarnagin, W.; D’Angelica, M.; Yarmohammadi, H. Conversion Therapy to Transplant or Surgical Resection in Patients with Unresectable Hepatocellular Carcinoma Treated with Boosted Dose of Yttrium-90 Radiation Segmentectomy. Cancers 2024, 16, 3024. [Google Scholar] [CrossRef]
- Mangieri, C.W.; Valenzuela, C.D.; Strode, M.A.; Erali, R.A.; Shen, P.; Howerton, R.; Clark, C.J. Effect of Preoperative Liver-Directed Therapy prior to Hepatic Resection. Am. J. Surg. 2023, 225, 703–708. [Google Scholar] [CrossRef]
- Shehta, A.; Lee, J.-M.; Suh, K.-S.; Kim, H.-C.; Hong, S.K.; Cho, J.-H.; Yi, N.-J.; Lee, K.-W. Bridging and Downstaging Role of Trans-Arterial Radio-Embolization for Expected Small Remnant Volume before Liver Resection for Hepatocellular Carcinoma. Ann. Hepatobiliary Pancreat. Surg. 2020, 24, 421–430. [Google Scholar] [CrossRef]
- Rognoni, C.; Ciani, O.; Sommariva, S.; Facciorusso, A.; Tarricone, R.; Bhoori, S.; Mazzaferro, V. Trans-Arterial Radioembolization in Intermediate-Advanced Hepatocellular Carcinoma: Systematic Review and Meta-Analyses. Oncotarget 2016, 7, 72343–72355. [Google Scholar] [CrossRef]
- Torzilli, G.; Belghiti, J.; Kokudo, N.; Takayama, T.; Capussotti, L.; Nuzzo, G.; Vauthey, J.-N.; Choti, M.A.; De Santibanes, E.; Donadon, M.; et al. A Snapshot of the Effective Indications and Results of Surgery for Hepatocellular Carcinoma in Tertiary Referral Centers: Is It Adherent to the EASL/AASLD Recommendations?: An Observational Study of the HCC East-West Study Group. Ann. Surg. 2013, 257, 929–937. [Google Scholar] [CrossRef]
- Famularo, S.; Donadon, M.; Cipriani, F.; Giuliante, F.; Ferri, S.; Celsa, C.; Ferrero, A.; Foschi, F.G.; Baiocchi, G.L.; Biasini, E.; et al. Hepatectomy Versus Sorafenib in Advanced Nonmetastatic Hepatocellular Carcinoma: A Real-Life Multicentric Weighted Comparison. Ann. Surg. 2022, 275, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Juthani, R.; Malalur, P.; Manne, A.; Mittra, A. The Combined Use of Lenvatinib and Locoregional Therapies for the Management of Hepatocellular Carcinoma. Cancers 2025, 17, 1572. [Google Scholar] [CrossRef] [PubMed]
- Reinders, M.T.M.; Braat, A.J.A.T.; van Erpecum, K.J.; de Bruijne, J.; Bruijnen, R.C.G.; Sprengers, D.; de Man, R.; Vegt, E.; IJzermans, J.N.M.; Elias, S.G.; et al. Holmium-166 Radioembolisation Dosimetry in HCC. Eur. J. Nucl. Med. Mol. Imaging 2025, 52, 993–1003. [Google Scholar] [CrossRef]
- Arar, A.; Heglin, A.; Veluri, S.; Alnablsi, M.W.; Benjamin, J.L.; Choudhary, M.; Pillai, A. Radioembolization of HCC and Secondary Hepatic Tumors: A Comprehensive Review. Q. J. Nucl. Med. Mol. Imaging 2024, 68, 270–287. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Non-TARE Group n = 21 (53.8%) | TARE Group n = 18 (46.15%) | p-Value | |
|---|---|---|---|
| Age, median [IQR] | 72 [69.0, 77.0] | 74.50 [70.50, 76.0] | 0.489 |
| Male (%) | 16 (76.2) | 17 (94.4) | 0.190 |
| BMI, median [IQR] | 25.93 [21.80, 29.32] | 25.96 [23.99, 28.62] | 0.673 |
| Charlson Comorbidity Index, median [IQR] | 6 [5, 7] | 6 [6, 7] | 0.402 |
| ASA score (%) | |||
| 1 | 1 (4.8) | 0 (0.0) | 0.537 |
| 2 | 6 (28.6) | 3 (16.7) | |
| 3 | 12 (57.1) | 14 (77.8) | |
| 4 | 2 (9.5) | 1 (5.6) | |
| No Virus (%) | 15 (71.4) | 7 (38.9) | 0.033 |
| HBV (%) | 0 (0.0) | 4 (22.2) | |
| HCV (%) | 6 (28.6) | 7 (38.9) | |
| Metabolic Disease (%) | 9 (42.9) | 5 (27.8) | 0.504 |
| Child Pugh Score (%) | |||
| Child Pugh A (%) | 19 (90.5) | 18 (100) | 0.490 |
| Child Pugh B (%) | 2 (9.5) | 0 (0.0) | |
| MELD, median [IQR] | 7.00 [7.00, 8.00] | 7.50 [7.00, 8.75] | 0.588 |
| AFP ng/mL (%) | |||
| ≤100 | 14 (66.7) | 12 (66.7) | 1.000 |
| >100 | 6 (28.6) | 5 (27.8) | |
| Bilirubin preoperative, mg/dl, median [IQR] | 0.71 [0.60, 1.05] | 0.77 [0.61, 0.90] | 0.877 |
| 15′ ICG-RR, median [IQR] | 10.30 [4.30, 12.50] | 14.80 [9.85, 21.73] | 0.033 |
| Esophageal Varices (%) | 1 (4.8) | 2 (11.1) | 0.586 |
| Size of Node (preoperative), mm, median [IQR] | 80.00 [60.00, 150.00] | 70.00 [47.50, 80.00] | 0.171 |
| Single Node (%) | 18 (85.7) | 10 (55.6) | 0.218 |
| Multifocal Disease (%) | 3 (14.3) | 8 (44.4) | |
| Portal Vein Invasion Vp (%) | |||
| Vp0 | 16 (76.2) | 10 (55.6) | 0.043 |
| Vp1 | 0 (0.0) | 1 (5.6) | |
| Vp2 | 4 (19.0) | 1 (5.6) | |
| Vp3 | 1 (4.8) | 6 (33.3) | |
| Hepatic Vein Invasion VV (%) | |||
| VV0 | 10 (47.6) | 12 (66.7) | 0.093 |
| VV1 | 0 (0.0) | 2 (11.1) | |
| VV2 | 10 (47.6) | 4 (22.2) | |
| VV3 | 1 (4.8) | 0 (0.0) | |
| Right Portal Vein Invasion Vp3 (%) | 1 (4.8) | 6 (33.3) | 0.035 |
| Concomitant Portal and Hepatic Vein Invasion (%) | 3 (14.3) | 3 (16.7) | 1.000 |
| BCLC Stage (%) | 0.295 | ||
| A | 9 (42.9) | 5 (27.8) | |
| B | 1 (4.8) | 4 (22.2) | |
| C | 11 (52.4) | 9 (50.0) | |
| FLR/TLV pre-treatment, %, median [IQR] | 40.0 [37.0–47.3] | 39.1 [35.8–50.7] | 0.954 |
| FLR/TLV post-treatment, %, median [IQR] | 51.9 [51.0, 53.9] * | 56.9 [40.0, 62.2] | 0.737 |
| Non-TARE Group n = 21 (53.8%) | TARE Group n = 18 (46.15%) | p-Value | |
|---|---|---|---|
| Operative time, minutes, median [IQR] | 320 [300.00, 420.00] | 330.00 [302.50, 360.00] | 0.899 |
| Operative time (liver transection), minutes, median [IQR] | 90.00 [79.00, 100.00] | 86.50 [67.50, 106.75] | 0.888 |
| Pringle maneuver (%) | 15 (71.4) | 15 (83.3) | 0.464 |
| Duration Pringle maneuver, minutes, median [IQR] | 46.00 [0.00, 68.00] | 53.00 [24.75, 60.50] | 0.734 |
| Blood loss, ml, median [IQR] | 330.00 [190.00, 400.00] | 275.00 [200.00, 570.00] | 0.778 |
| Section plane cm2, median [IQR] | 75.00 [68.00, 101.00] | 64.50 [46.00, 82.00] | 0.143 |
| Type of surgery (%) | |||
| Right hepatectomy (%) | 17 (81.0) | 8 (44.4) | 0.024 |
| Extended right hepatectomy (%) | 4 (19.0) | 10 (55.6) | |
| Minimally invasive resection (%) | 5 (23.8) | 8 (44.4) | 0.196 |
| Intraoperative complication (%) | 3 (14.3) | 1 (5.6) | 0.609 |
| Non-TARE Group n = 21 (53.8%) | TARE Group n = 18 (46.15%) | p-Value | |
|---|---|---|---|
| Postoperative complications (%) | 8 (38.1) | 7 (38.9) | 1.000 |
| Blood transfusions (%) | 3 (14.3) | 1 (5.6) | 0.609 |
| PHLF (%) | 4 (19.0) | 2 (11.1) | 0.667 |
| Grade PHLF sec. ISGLS (%) | |||
| Grade A | 0 (0.0) | 1 (5.6) | 0.609 |
| Grade B | 2 (9.5) | 0 (0.0) | |
| Grade C | 2 (9.5) | 1 (5.6) | |
| Biliary fistula (%) | 3 (14.3) | 2 (11.1) | 1.000 |
| Clavien–Dindo ≥3 (%) | 5 (23.8) | 1 (5.6) | 0.190 |
| CCI ≥ 20.9 (%) | 8 (38.1) | 4 (22.2) | 0.322 |
| Readmission (%) | 2 (9.5) | 1 (5.6) | 1.000 |
| 90-day postoperative mortality (%) | 2 (9.5) | 1 (5.6) | 1.000 |
| Hospital stay, days, median [IQR] | 8.00 [5.00, 11.00] | 6.00 [5.00, 9.00] | 0.318 |
| Histology | |||
| Cirrhosis (%) | 3 (14.3) | 12 (66.7) | 0.001 |
| Multinodular disease (%) | 2 (9.5) | 7 (38.9) | 0.055 |
| Single node disease (%) | 19 (90.5) | 11 (61.1) | |
| Satellitosis (%) | 13 (61.9) | 6 (33.3) | 0.111 |
| Size of node, mm, median [IQR] | 80.00 [60.00, 150.00] | 46.50 [36.25, 77.50] | 0.020 |
| Necrosis percentage, median [IQR] | 10.00 [10.00, 20.00] | 70.00 [50.00, 87.50] | 0.002 |
| Resection margin, mm, median [IQR] | 10.00 [2.00, 15.00] | 2.00 [1.00, 10.00] | 0.032 |
| Positive margin, mm (%) | 1 (4.8) | 2 (11.1) | 0.586 |
| Microvascular invasion (%) | 19 (90.5) | 11 (61.1) | 0.055 |
| Edmonson Grade 3–4 (%) | 18 (85.7) | 10 (55.6) | 0.072 |
| Tumor capsule (%) | 15 (71.4) | 11 (61.1) | 0.520 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fontana, A.P.; Russolillo, N.; Maurino, L.; Marengo, A.; Calvo, A.; Ricotti, A.; Langella, S.; Tesoriere, R.L.; Ferrero, A. Impact of Preoperative Yttrium-90 Transarterial Radioembolization on Patients Undergoing Right or Extended Right Hepatectomy for Hepatocellular Carcinoma. Cancers 2025, 17, 2556. https://doi.org/10.3390/cancers17152556
Fontana AP, Russolillo N, Maurino L, Marengo A, Calvo A, Ricotti A, Langella S, Tesoriere RL, Ferrero A. Impact of Preoperative Yttrium-90 Transarterial Radioembolization on Patients Undergoing Right or Extended Right Hepatectomy for Hepatocellular Carcinoma. Cancers. 2025; 17(15):2556. https://doi.org/10.3390/cancers17152556
Chicago/Turabian StyleFontana, Andrea P., Nadia Russolillo, Ludovica Maurino, Andrea Marengo, Amedeo Calvo, Andrea Ricotti, Serena Langella, Roberto Lo Tesoriere, and Alessandro Ferrero. 2025. "Impact of Preoperative Yttrium-90 Transarterial Radioembolization on Patients Undergoing Right or Extended Right Hepatectomy for Hepatocellular Carcinoma" Cancers 17, no. 15: 2556. https://doi.org/10.3390/cancers17152556
APA StyleFontana, A. P., Russolillo, N., Maurino, L., Marengo, A., Calvo, A., Ricotti, A., Langella, S., Tesoriere, R. L., & Ferrero, A. (2025). Impact of Preoperative Yttrium-90 Transarterial Radioembolization on Patients Undergoing Right or Extended Right Hepatectomy for Hepatocellular Carcinoma. Cancers, 17(15), 2556. https://doi.org/10.3390/cancers17152556