

Efficacy of Compression Stockings in Prophylaxis of Lower Limb Lymphedema in Women Undergoing Treatment for Gynecological Malignancies: A Prospective Randomized Study

 , , and
, , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
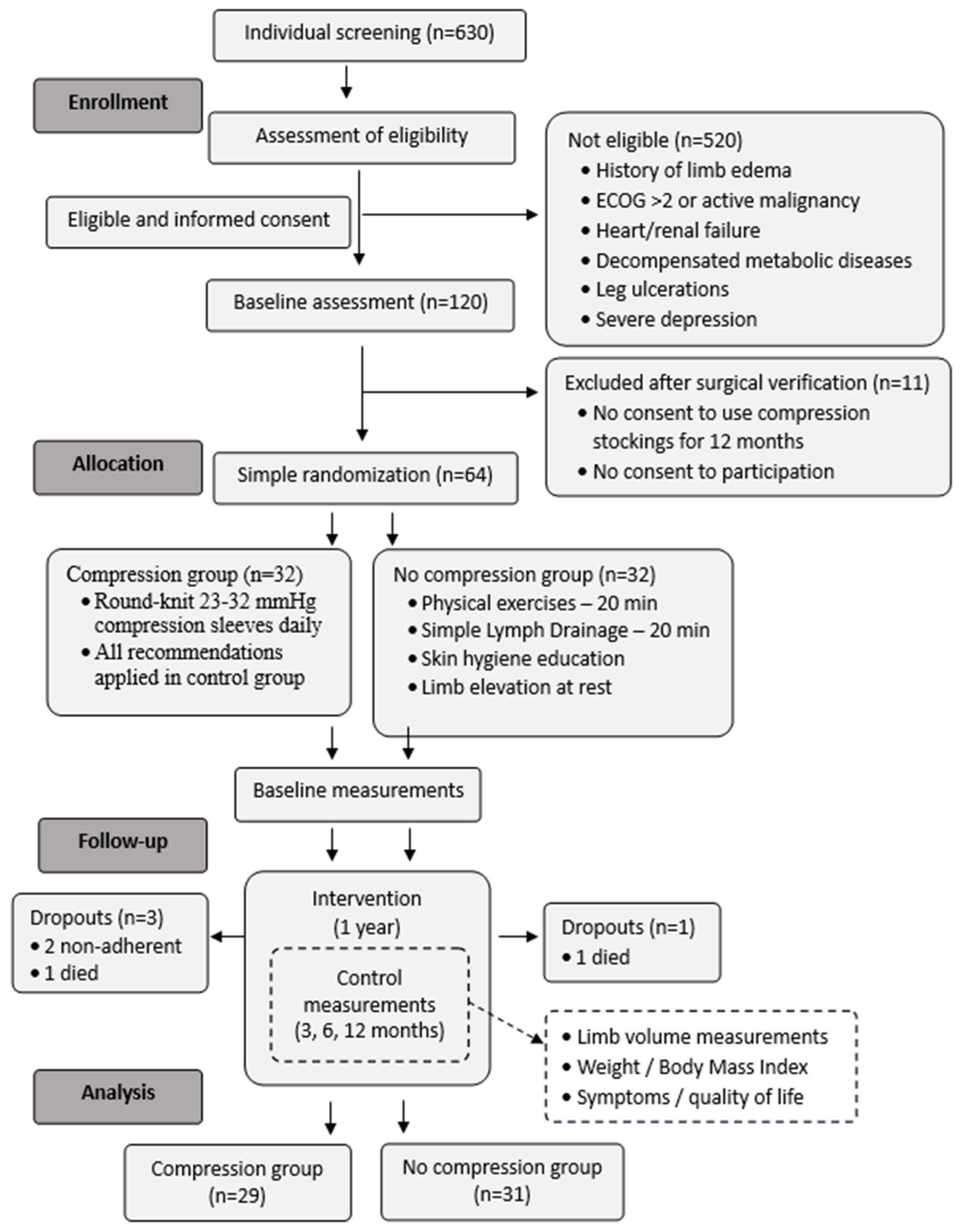
2.1. Participants
2.2. Intervention
2.3. Measurements
- Grade 1 = 2 mm;
- Grade 2 = 3–4 mm;
- Grade 3 = 5–6 mm;
- Grade 4 = ≥8 mm.
2.4. Statistics
2.5. The Sample Size
3. Results
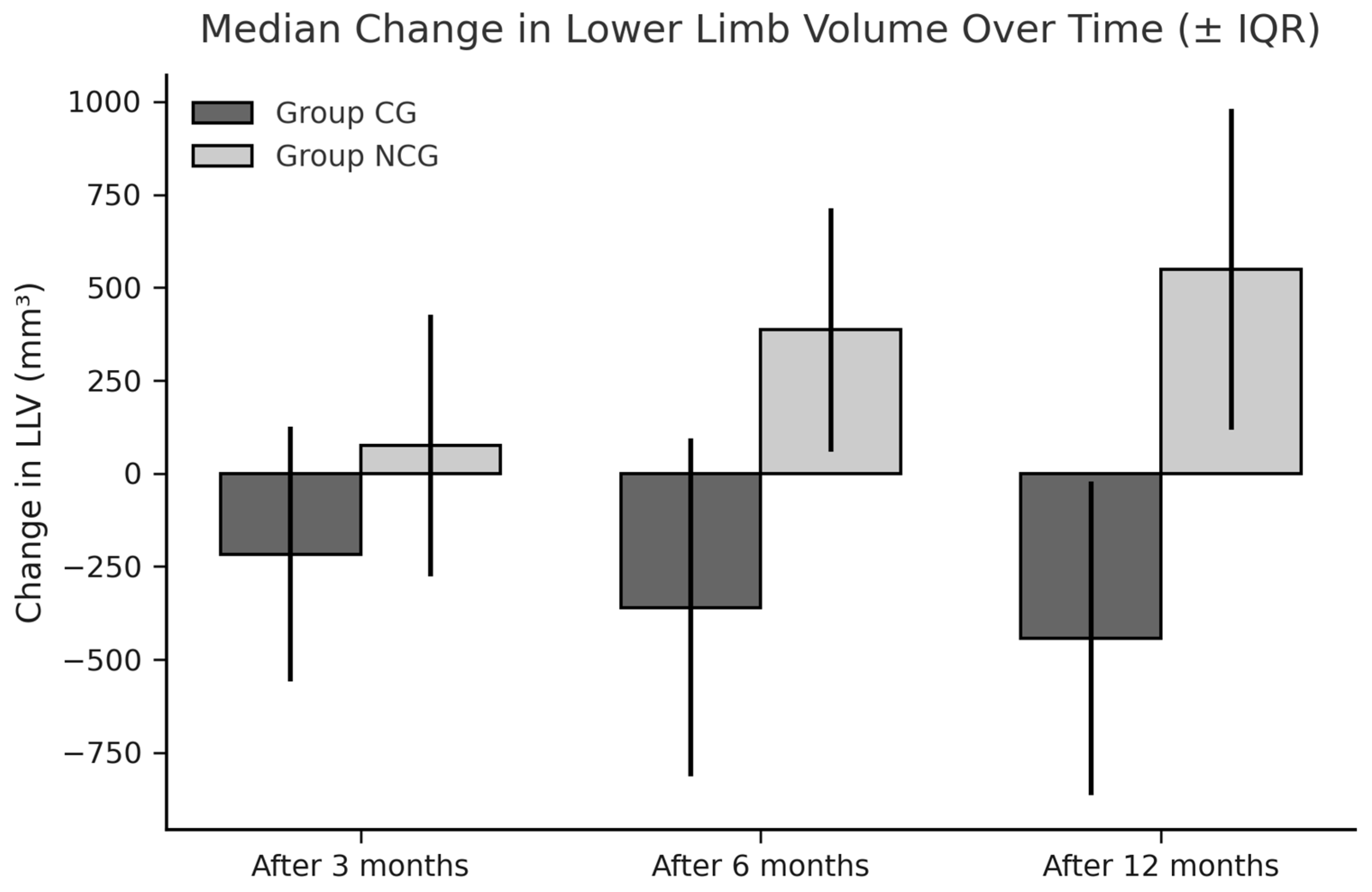
3.1. Limb Volumes and WAC
3.2. The Pitting Test
3.3. Compliance
- Walking more than 1 km per day (n = 27);
- Nordic walking (n = 17);
- Cycling (n = 11);
- Gymnastic exercises (n = 9).
- Rubber gloves (n = 24);
- Slippery socks or foot aids (n = 15);
- Assistance from another person (n = 15).
- A rating of 8.4/10 immediately after donning;
- A rating of 8.6/10 later in the day.
3.4. Health-Related Quality of Life and Disease-Related Symptoms
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, X.; Liu, Y.; Zhu, D.; Wang, F.; Ji, J.; Yan, H. Early prevention of complex decongestive therapy and rehabilitation exercise for prevention of lower extremity lymphedema after operation of gynecologic cancer. Asian J. Surg. 2021, 44, 111–115. [Google Scholar] [CrossRef]
- Hayes, S.C.; Janda, M.; Ward, L.C.; Reul-Hirche, H.; Steele, M.L.; Carter, J.; Quinn, M.; Cornish, B.; Obermair, A. Lymphedema following gynecological cancer: Results from a prospective, longitudinal cohort study on prevalence, incidence and risk factors. Gynecol. Oncol. 2017, 146, 623–629. [Google Scholar] [CrossRef]
- Yoshihara, M.; Shimono, R.; Tsuru, S.; Kitamura, K.; Sakuda, H.; Oguchi, H.; Hirota, A. Risk factors for late-onset lower li mb lymphedema after gynecological cancer treatment: A multi-institutional retrospective study. Eur. J. Surg. Oncol. 2020, 46, 1334–1338. [Google Scholar] [CrossRef]
- Huang, J.; Yu, N.; Wang, X.; Long, X. Incidence of lower limb lymphedema after vulvar cancer: A systematic review and meta-analysis. Medicine 2017, 96, e8722. [Google Scholar] [CrossRef]
- Ward, L.C.; Covens, A.; Thomas, E.J.; Armer, J.M. Lymphedema measurements and associated patient outcomes: Toward standardization. Gynecol. Oncol. 2022, 160, 625–632. [Google Scholar] [CrossRef]
- Hsu, Y.Y.; Liu, C.Y.; Ho, C.L.; Hsu, K.F. Determinants of quality of life related to lower limb lymphedema in women with gynecological cancer surgery. Asia-Pac. J. Oncol. Nurs. 2023, 10, 100153. [Google Scholar] [CrossRef]
- Bowman, C.; Piedalue, K.A.; Baydoun, M.; Carlson, L.E. The quality of life and psychosocial implications of cancer-related lower-extremity lymphedema: A systematic review of the literature. J. Clin. Med. 2020, 9, 3200. [Google Scholar] [CrossRef]
- Tümkaya, M.N.; Seven, M. Interventions for prevention and management of gynecological cancer-related lower limb lymphedema: A systematic scoping review. Semin. Oncol. Nurs. 2024, in press. [Google Scholar] [CrossRef]
- Wang, X.; Ding, Y.; Cai, H.Y.; You, J.; Fan, F.Q.; Cai, Z.F.; An, P. Effectiveness of modified complex decongestive physiotherapy for preventing lower extremity lymphedema after radical surgery for cervical cancer: A randomized controlled trial. Int. J. Gynecol. Cancer 2020, 30, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Daggez, M.; Koyuncu, E.G.; Kocabaş, R.; Yener, C. Prophylactic complex physiotherapy in gynecologic cancer survivors: Patient-reported outcomes based on a lymphedema questionnaire. Int. J. Gynecol. Cancer 2023, 33, 1928–1933. [Google Scholar] [CrossRef] [PubMed]
- Sawan, S.; Mugnai, R.; de Barros Lopes, A.; Hughes, A.; Edmondson, R.J. Lower-limb lymphedema and vulval cancer: Feasibility of prophylactic compression garments and validation of leg volume measurement. Int. J. Gynecol. Cancer 2009, 19, 1649–1654. [Google Scholar] [CrossRef]
- Shallwani, S.M.; Towers, A.; Newman, A.; Salvador, S.; Yung, A.; Gilbert, L.; Gotlieb, W.H.; Zeng, X.; Thomas, D. Feasibility of a pilot randomized controlled trial examining a multidimensional intervention in women with gynecological cancer at risk of lymphedema. Curr. Oncol. 2021, 28, 455–470. [Google Scholar] [CrossRef]
- Stuiver, M.M.; de Rooij, J.D.; Lucas, C.; Nieweg, O.E.; Horenblas, S.; van Geel, A.N.; van Beurden, M.; Aaronson, N.K. No evidence of benefit from class-II compression stockings in the prevention of lower-limb lymphedema after inguinal lymph node dissection: Results of a randomized controlled trial. Lymphology 2013, 46, 120–131. [Google Scholar]
- Sitzia, J. Volume measurement in lymphoedema treatment: Examination of formulae. Eur. J. Cancer Care 1995, 4, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.L.; Specht, M.C.; Horick, N.; Skolny, M.N.; Jammallo, L.S.; O’Toole, J.; Taghian, A.G. A novel, validated method to quantify breast cancer-related lymphedema (BCRL) following bilateral breast surgery. Lymphology 2013, 46, 64–74. [Google Scholar] [PubMed]
- Devoogdt, N.; Partsch, H.; Heroes, A.K.; De Vrieze, T.; De Groef, A.; Geraerts, I.; Damstra, R.J.; Hafner, J.; Keeley, V.; Becker, A.; et al. The ICC Compression Questionnaire: A comprehensive tool to evaluate compression materials or devices applied in subjects with lymphedema or chronic venous disease. Lymphat Res Biol. 2022, 20, 191–202. [Google Scholar] [CrossRef]
- International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2023 Consensus document of the International Society of Lymphology. Lymphology 2023, 56, 1–25. [Google Scholar] [CrossRef]
- Liu, F.; Liu, N.F.; Wang, L.; Chen, J.; Han, L.; Yu, Z.; Sun, D. Treatment of secondary lower limb lymphedema after gynecologic cancer with complex decongestive therapy. Lymphology 2021, 54, 122–132. [Google Scholar] [CrossRef]
- Webb, E.; Bissett, B.; Neeman, T.; Bowden, F.; Preston, E.; Mumford, V. Compression therapy is cost-saving in the prevention of lower limb recurrent cellulitis in patients with chronic edema. Lymphat. Res. Biol. 2023, 21, 160–168. [Google Scholar] [CrossRef]
- Cavezzi, A.; Cornu-Thenard, A.; Bergan, J.J.; Di Ionna, G. Compression therapy, autonomic nervous system, and heart rate variability: A narrative review and our preliminary personal experience. Phlebology 2022, 37, 739–753. [Google Scholar] [CrossRef]
- Partsch, H. Compression therapy: Clinical and experimental evidence. Ann. Vasc. Dis. 2012, 5, 416–422. [Google Scholar] [CrossRef]
- King, M.; Deveaux, A.; White, H.; Rayson, D. Compression garments versus compression bandaging in decongestive lymphatic therapy for breast cancer-related lymphedema: A randomized controlled trial. Support Care Cancer 2012, 20, 1031–1036. [Google Scholar] [CrossRef]
- Rabe, E.; Partsch, H.; Hafner, J.; Lattimer, C.; Mosti, G.; Neumann, M.; Urbanek, T.; Huebner, M.; Gaillard, S.; Carpentier, P. Indications for medical compression stockings in venous and lymphatic disorders: An evidence-based consensus statement. Phlebology 2018, 33, 163–184. [Google Scholar] [CrossRef]
- Keeley, V. The early detection of breast cancer treatment-related lymphedema of the arm. Lymphat. Res. Biol. 2020, 19, 51–55. [Google Scholar] [CrossRef]
- Davies, C.; Levenhagen, K.; Ryans, K.; Perdomo, M.; Gilchrist, L. Interventions for breast cancer-related lymphedema: Clinical practice guideline from the academy of oncologic physical therapy of APTA. Phys. Ther. 2020, 100, 1163–1179. [Google Scholar] [CrossRef]
- Ochalek, K.; Gradalski, T.; Partsch, H. Preventing early postoperative arm swelling and lymphedema manifestation by compression sleeves after axillary lymph node interventions in breast cancer patients: A randomized controlled trial. J. Pain Symptom Manage. 2017, 54, 346–354. [Google Scholar] [CrossRef]
- Paramanandam, V.S.; Ridner, S.H.; Dietrich, M.S.; Deng, J.; Cormier, J.N.; Doerzaph, A.; Smith, K.; Armer, J.M.; Deutsch, M.; Shaitelman, S.F.; et al. Prophylactic use of compression sleeves reduces the incidence of arm swelling in women at high risk of breast cancer–related lymphedema: A randomized controlled trial. J Clin Oncol. 2022, 40, 2004–2012. [Google Scholar] [CrossRef]
- Zhang, J.; Zhou, C.; Ma, Q.; Zhang, Y.; Zhang, X. Preventing lower limb lymphedema after pelvic lymphadenectomy with progressive resistance exercise training: A randomized controlled trial. Asia-Pac. J. Oncol. Nurs. 2024, 11, 100333. [Google Scholar] [CrossRef] [PubMed]
- Woods, M.; Ruddell, S.; Sandsund, C.; Thomas, K.; Shaw, C. A service development evaluation of retrospective data exploring prophylactic risk-reducing advice for patients with gynecological cancers. J. Gynecol. Surg. 2020, 36, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Sayegh, H.E.; Asdourian, M.S.; Swaroop, M.N.; Brunelle, C.L.; Skolny, M.N.; Salama, L.; Taghian, A.G. Diagnostic methods, risk factors, prevention, and management of breast cancer-related lymphedema: Past, present, and future directions. Curr. Breast Cancer Rep. 2017, 9, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Sugisawa, R.; Unno, N.; Saito, T.; Yamamoto, N.; Inuzuka, K.; Tanaka, H.; Sano, M.; Katahashi, K.; Uranaka, H.; Marumo, T.; et al. Effects of compression stockings on elevation of leg lymph pumping pressure and improvement of quality of life in healthy female volunteers: A randomized controlled trial. Lymphat. Res. Biol. 2016, 14, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Stout, N.; Partsch, H.; Szolnoky, G.; Forner-Cordero, I.; Mosti, G.; Mortimer, P.; Flour, M.; Damstra, R.; Piller, N.; Geyer, M.J.; et al. Chronic edema of the lower extremities: International consensus recommendations for compression therapy clinical research trials. Int. Angiol. 2012, 31, 316–329. [Google Scholar] [PubMed]
- Hsu, Y.Y.; Nguyen, T.T.; Chou, Y.J.; Ho, C.L. Effects of exercise on lower limb lymphedema in gynecologic cancer: A systematic review and meta-analysis. Eur. J. Oncol. Nurs. 2024, 70, 102550. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American college of sports medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Hayes, S.C.; Singh, B.; Reul-Hirche, H.; Bloomquist, K.; Johansson, K.; Jönsson, C.; Plinsinga, M.L. The effect of exercise for the prevention and treatment of cancer-related lymphedema: A systematic review with meta-analysis. Med. Sci. Sports Exerc. 2022, 54, 2136–2147. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, T.; Tsuji, T.; Sano, Y.; Miyata, C.; Kamisako, M.; Hohri, H.; Yoshimura, C.; Asakura, M.; Okitsu, T.; Muraoka, K.; et al. Immediate effects of active exercise with compression therapy on lower-limb lymphedema. Support Care Cancer 2017, 25, 2603–2610. [Google Scholar] [CrossRef]
- Abe, K.; Tsuji, T.; Oka, A.; Shoji, J.; Kamisako, M.; Hohri, H.; Ishikawa, A.; Liu, M. Postural differences in the immediate effects of active exercise with compression therapy on lower limb lymphedema. Support Care Cancer 2021, 29, 6535–6543. [Google Scholar] [CrossRef]
- Liao, X.; Cao, G.; Yang, L.; Wang, C.; Tian, C. Postoperative effectiveness of comprehensive nursing intervention for lymphedema in gynecological cancer: A controlled study. Altern. Ther. Health Med. 2023, 29, 242–247. [Google Scholar]

{kind=link}
{kind=link}
| Parameter (n or Median, IQR) | CG (n = 29) | NCG (n = 31) | p-Value |
|---|---|---|---|
| Age (years) | 53.5 (15.25) | 58 (14.0) | 0.06 * |
| Height (m) | 1.61 (0.11) | 1.58 (0.09) | 0.3 * |
| Weight (kg) | 70.0 (16.5) | 75.0 (19.0) | 0.9 * |
| Body mass index (kg/m2) | 26.9 (4.6) | 28.0 (8.6) | 0.5 * |
| Professionally active | 19 | 16 | |
| Tumor localization (n) | |||
| Ovaries | 7 | 7 | 0.6 ** |
| Cervix uteri | 8 | 8 | |
| Corpus uteri | 12 | 15 | |
| Vulva | 2 | 1 | |
| Complementary therapy (n) | |||
| Lymphadenectomy | 29 | 31 | |
| Radiotherapy | 26 | 26 | 0.9 ** |
| Chemotherapy | 13 | 14 | |
| Limb volumes (L) | |||
| Right | 8.13 (1.36) | 7.82 (2.28) | 0.8 * |
| Left | 8.30 (1.93) | 7.90 (2.17) | 0.9 * |
| Right and left | 16.60 (3.58) | 15.95 (4.38) | 0.9 * |
| Parameter (n or Median, IQR) | CG (n = 29) | NCG (n = 31) | p-Value |
|---|---|---|---|
| Edema occurrence (n) | 1 | 12 | 0.003 * |
| Limb volume changes | |||
| Right limb | |||
| Within 3 months | −86.13 (349.40) | 97.05 (315.27) | 0.049 ** |
| Within 6 months | −157.33 (480.43) | 193 (836.04) | 0.022 ** |
| Within 12 months | −259.33 (540.99) | 250.05 (546.81) | 0.001 ** |
| p-value | 0.01 *** | 0.07 *** | |
| Left limb | |||
| Within 3 months | −155.66 (285.45) | 36.80 (388.09) | 0.051 ** |
| Within 6 months | −198.42 (94.43) | 151.37 (384.09) | 0.019 ** |
| Within 12 months | −137.10 (497.68) | 250.51 (366.36) | 0.002 ** |
| p-value | 0.011 *** | 0.06 *** | |
| Right and left limb | |||
| Within 3 months | −216.88 (684.90) | 75.34 (162.36) | 0.032 ** |
| Within 6 months | −359.81 (375.47) | 386.96 (655.08) | 0.004 ** |
| Within 12 months | −443.01 (841.88) | 549.07 (861.70) | 0.001 ** |
| p-value | 0.011 *** | 0.011 *** | |
| WAC | |||
| Right limb | |||
| Within 3 months | −0.01 (0.04) | 0.02 (0.06) | 0.004 ** |
| Within 6 months | −0.03 (0.06) | 0.03 (0.02) | 0.003 ** |
| Within 12 months | −0.06 (0.08) | 0.02 (0.05) | 0.001 ** |
| p-value | 0.001 *** | 0.9 *** | |
| Left limb | |||
| Within 3 months | −0.02 (0.05) | 0.01 (0.05) | 0.002 ** |
| Within 6 months | −0.03 (0.07) | 0.02 (0.05) | 0.003 ** |
| Within 12 months | −0.05 (0.07) | 0.02 (0.05) | 0.001 ** |
| p-value | 0.001 *** | 0.3 *** | |
| Right and left limb | |||
| Within 3 months | −0.02 (0.03) | 0.02 (0.03) | 0.001 ** |
| Within 6 months | −0.03 (0.05) | 0.02 (0.03) | <0.001 ** |
| Within 12 months | −0.05 (0.06) | 0.02 (0.04) | <0.001 ** |
| p-value | 0.001 *** | 0.4 *** |
| Problem Mean ± SD and Median (IQR) | CG (n = 29) | p-Value Within Groups ** | NCG (n = 31) | p-Value Within Groups ** | p-Value Between Groups * |
|---|---|---|---|---|---|
| Pain within the limbs | |||||
| At baseline | 1.39 ± 0.57 1.0 (1.0) | 1.33 ± 0.61 1.0 (0.75) | 0.049 | ||
| After 3 months | 1.41 ± 0.57 1.0 (1.0) | 1.0 | 1.50 ± 0.63 1.0 (1.0) | 0.07 | 0.6 |
| After 6 months | 1.29 ± 0.53 1.0 (0.25) | 0.2 | 1.57 ± 0.63 1.5 (1.0) | 0.04 | 0.6 |
| After 12 months | 1.32 ± 0.55 1.0 (1.0) | 0.5 | 1.59 ± 0.68 1.0 (1.0) | 0.05 | 0.1 |
| Limb heaviness | |||||
| At baseline | 1.26 ± 0.39 1.0 (0.5) | 1.23 ± 0.43 1.0 (0.0) | 0.8 | ||
| After 3 months | 1.33 ± 0.48 1.0 (1.0) | 0.5 | 1.27 ± 0.52 1.0 (0.0) | 0.8 | 0.5 |
| After 6 months | 1.33 ± 0.48 1.0 (1.0) | 0.5 | 1.73 ± 0.74 2.0 (1.0) | 0.004 | 0.036 |
| After 12 months | 1.54 ± 0.58 1.5 (1.0) | 0.06 | 1.62 ± 0.68 2.0 (1.0) | 0.003 | 0.7 |
| Skin tension | |||||
| At baseline | 1.18 ± 0.41 1.0 (0.0) | 1.23 ± 0.43 1.0 (0.0) | 0.7 | ||
| After 3 months | 1.28 ± 0.46 1.0 (1.0) | 0.5 | 1.43 ± 0.50 1.0 (1.0) | 0.04 | 0.3 |
| After 6 months | 1.43 ± 0.57 1.0 (1.0) | 0.2 | 1.60 ± 0.67 1.0 (1.0) | 0.003 | 0.1 |
| After 12 months | 1.43 ± 0.57 1.0 (1.0) | 0.008 | 1.48 ± 0.63 1.0 (1.0) | 0.04 | 0.8 |
| Limb numbness | |||||
| At baseline | 1.64 ± 0.68 1.0 (1.0) | 1.47 ± 0.50 1.0 (1.0) | 0.3 | ||
| After 3 months | 1.46 ± 0.58 1.0 (1.0) | 0.09 | 1.70 ± 0.65 2.0 (1.0) | 0.02 | 0.2 |
| After 6 months | 1.43 ± 0.50 1.0 (1.0) | 0.01 | 1.73 ± 0.64 2.0 (1.0) | 0.04 | 0.04 |
| After 12 months | 1.43 ± 0.50 1.0 (1.0) | 0.09 | 1.69 ± 0.60 2.0 (1.0) | 0.08 | |
| Genital edema | |||||
| At baseline | 1.00 ± 0.00 1.0 (0.0) | 1.00 ± 0.00 1.0 (0.0) | 1.0 | ||
| After 3 months | 1.08 ± 0.27 1.0 (0.0) | 0.3 | 1.07 ± 0.25 1.0 (0.0) | 0.3 | 0.9 |
| After 6 months | 1.00 ± 0.00 1.0 (0.0) | 1.0 | 1.17 ± −0.46 1.0 (1.0) | 0.09 | 0.049 |
| After 12 months | 1.00 ± 0.00 1.0 (0.0) | 1.0 | 1.07 ± 0.26 1.0 (0.0) | 0.4 | 0.1 |
| Lymphorrhea | |||||
| At baseline | 1.00 ± 0.00 1.0 (0.0) | 1.00 ± 0.00 1.0 (0.0) | 1.0 | ||
| After 3 months | 1.00 ± 0.00 1.0 (0.0) | 1.0 | 1.03 ± 0.18 1.0 (0.0) | 1.0 | 0.4 |
| After 6 months | 1.00 ± 0.00 1.0 (0.0) | 1.0 | 1.13 ± 0.43 1.0 (0.0) | 0.2 | 0.09 |
| After 12 months | 1.00 ± 0.00 1.0 (0.0) | 1.0 | 1.00 ± 0.00 1.0 (0.0) | 1.0 | 1.0 |
| Parameter Median (IQR) | CG (n = 29) | NCG (n = 31) | p-Value |
|---|---|---|---|
| Global health status | 75 (25.0) | 66.67 (16.67) | 0.3 |
| Physical functioning | 93.33 (13.33) | 86.67 (20.0) | 0.03 |
| Role functioning | 100 (20.83) | 83.33 (16.67) | 0.8 |
| Emotional functioning | 83.33 (25.0) | 75.0 (25.0) | 0.9 |
| Cognitive functioning | 91.67 (33.33) | 83.33 (16.67) | 0.5 |
| Social functioning | 100 (16.67) | 100 (16.67) | 0.9 |
| Fatigue | 22.22 (33.33) | 22.22 (22.22) | 0.5 |
| Nausea and vomiting | 0.0 (0.0) | 0.0 (12.5) | 0.8 |
| Pain | 16.67 (33.3) | 25.0 (33.33) | 0.3 |
| Dyspnea | 0.0 (0.0) | 0.0 (33.33) | 0.2 |
| Insomnia | 33.33 (33.33) | 33.33 (33.33) | 0.9 |
| Appetite loss | 0.0 (0.0) | 0.0 (33.33) | 0.4 |
| Constipation | 16.67 (33.33) | 0.0 (33.33) | 0.4 |
| Diarrhea | 0.0 (0.0) | 0.0 (0.0) | 0.4 |
| Financial difficulties | 0.0 (33.3) | 0.0 (33.3) | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurpiewska-Pieniążek, J.; Ochałek, K.; Grądalski, T.; Szuba, A. Efficacy of Compression Stockings in Prophylaxis of Lower Limb Lymphedema in Women Undergoing Treatment for Gynecological Malignancies: A Prospective Randomized Study. Cancers 2025, 17, 2530. https://doi.org/10.3390/cancers17152530
Kurpiewska-Pieniążek J, Ochałek K, Grądalski T, Szuba A. Efficacy of Compression Stockings in Prophylaxis of Lower Limb Lymphedema in Women Undergoing Treatment for Gynecological Malignancies: A Prospective Randomized Study. Cancers. 2025; 17(15):2530. https://doi.org/10.3390/cancers17152530
Chicago/Turabian StyleKurpiewska-Pieniążek, Joanna, Katarzyna Ochałek, Tomasz Grądalski, and Andrzej Szuba. 2025. "Efficacy of Compression Stockings in Prophylaxis of Lower Limb Lymphedema in Women Undergoing Treatment for Gynecological Malignancies: A Prospective Randomized Study" Cancers 17, no. 15: 2530. https://doi.org/10.3390/cancers17152530
APA StyleKurpiewska-Pieniążek, J., Ochałek, K., Grądalski, T., & Szuba, A. (2025). Efficacy of Compression Stockings in Prophylaxis of Lower Limb Lymphedema in Women Undergoing Treatment for Gynecological Malignancies: A Prospective Randomized Study. Cancers, 17(15), 2530. https://doi.org/10.3390/cancers17152530