
Ozone Treatment in the Management of Chemotherapy-Induced Peripheral Neuropathy: A Review of Rationale and Research Directions

 , , ,
, , ,  , ,
, ,  , , , , ,
, , , , ,  , and
, and 
Simple Summary
Abstract
1. Introduction
2. Chemotherapy-Induced Peripheral Neuropathy
2.1. Microtubule Disruption
2.2. Formation of Nuclear DNA Adducts
2.3. Mitochondrial Dysfunction
2.4. Ion Channel Dysregulation
2.5. Genetic Predisposition
2.6. Oxidative Stress
2.7. Neuroinflammation
2.8. The Role of the Brain in CIPN
2.9. The Role of the Gut Microbiota
3. Summary of Clinical Manifestations and Current Management Strategies of CIPN
3.1. Clinical Manifestations
3.2. Current Management Strategies
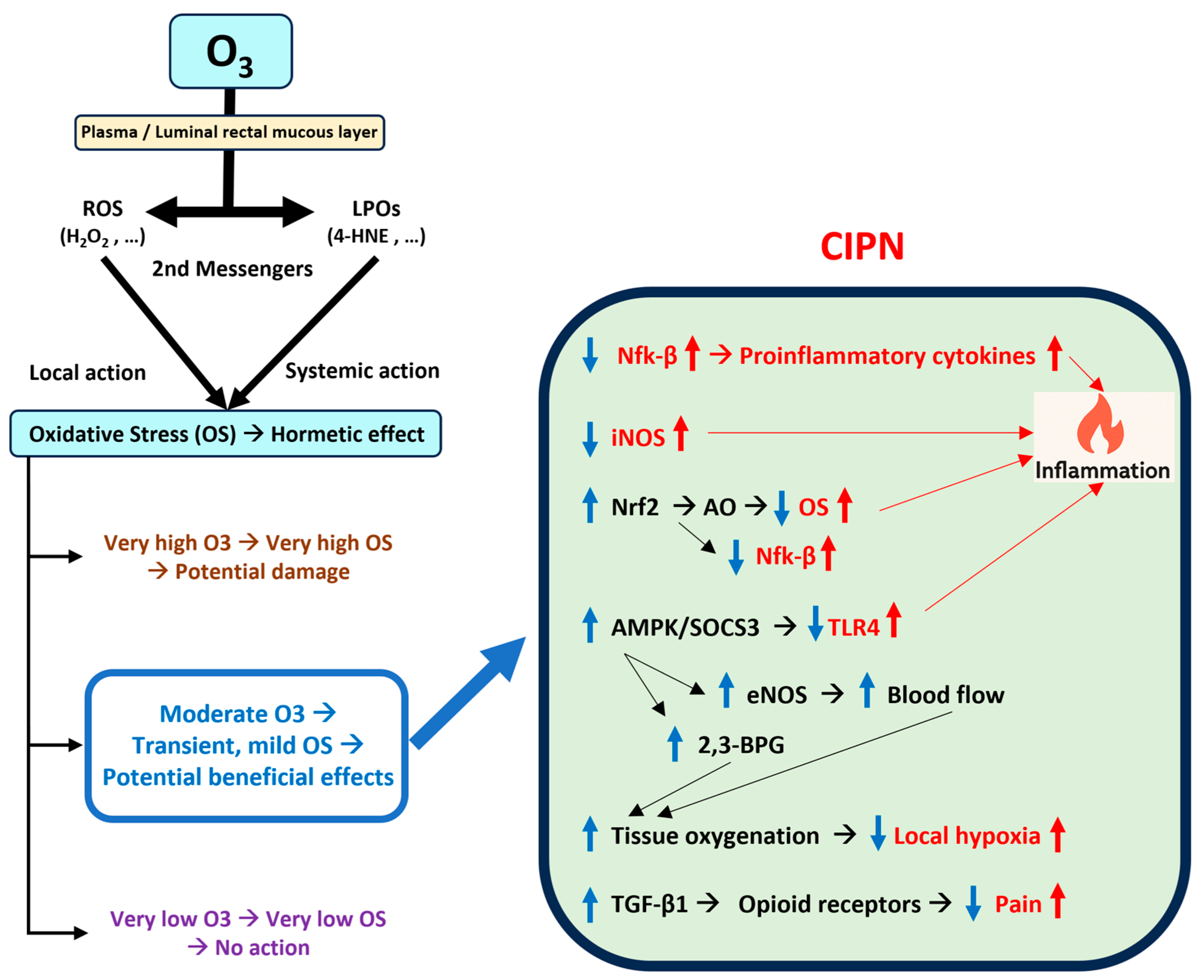
4. Ozone Treatment: Background and Mechanisms of Action
4.1. Activation of the Antioxidant System
4.2. System Modulation of Inflammation
4.3. Improvement in Microcirculation and Oxygen Delivery
5. Ozone Treatment: Preclinical and Clinical Studies
5.1. Preclinical Studies
5.2. Clinical Studies
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 2,3-BPG | 2,3-Bisiphosphoglycerate. |
| 4-HNE | 4-Hydroxynonenal. |
| ACTG1 | Actin Gamma 1. |
| c-FOS | FBJ Murine Osteosarcoma Viral Oncogene Homolog. |
| AMPK | Adenosine 5′-Monophosphate-Activated Protein Kinase. |
| ASCO | American Society of Clinical Oncology. |
| BPG | Bisphosphoglycerate. |
| CAPG | Capping Actin Protein, Gelsolin-Like. |
| CAT | Catalase. |
| CaV | Voltage-Gated Calcium Channel. |
| CGRP | Calcitonin Gene-Related Peptide. |
| CIPN | Chemotherapy-Induced Peripheral Neuropathy. |
| CTCAEs | Common Terminology Criteria for Adverse Events. |
| CYP | Cytochrome P450. |
| DRG | Dorsal Root Ganglion. |
| eNOS | Endothelial Nitric Oxide Synthase. |
| EQ-5D-5L™ | EuroQol-5 Dimension-5 Level Questionnaire. |
| EQ-VAS | Self-Perceived General Health Status. |
| GABA | Gamma-Aminobutyric Acid. |
| GPCRs | G-Coupled Protein Receptors. |
| GPx | Glutathione Peroxidase. |
| GSK3β | Glycogen Synthase Kinase 3 Beta. |
| GST | Glutathione S-Transferase. |
| GWAS | Genome-Wide Association Studies. |
| H2O2 | Hydrogen Peroxide. |
| HADS | Hospital Anxiety and Depression Scale. |
| HIF-1α | Hypoxia-Inducible Factor-1α. |
| HO-1 | Heme Oxygenase-1. |
| HRQOL | Health-Related Quality of Life. |
| HSI | Hyperspectral Imaging. |
| HSP70 | Heat Shock Protein 70. |
| IL | Interleukin. |
| iNOS | Inducible Nitric Oxide Synthase. |
| KV | Voltage-Gated Potassium Channel. |
| LOPs | Lipid Oxidation Products. |
| MAHT | Major Autohemotherapy. |
| MAPK | Mitogen-Activated Protein Kinase. |
| MAPT | Microtubule-Associated Protein Tau. |
| MMP | Matrix Metalloproteinase. |
| MRI | Magnetic Resonance Imaging. |
| NaV | Voltage-Gated Sodium Channel. |
| NF-κB | Nuclear Factor Kappa B. |
| NK | Natural Killer. |
| Nrf2 | Nuclear Factor Erythroid 2-Related Factor 2. |
| O3T | Ozone Treatment. |
| PROs | Patient-Reported Outcomes. |
| RCT | Randomized Controlled Trial. |
| ROS | Reactive Oxygen Species. |
| SNPs | Single-Nucleotide Polymorphisms. |
| SOCS3 | Suppressors Of Cytokine Signaling 3. |
| SOD | Superoxide Dismutase. |
| TF | Tissue Factor. |
| TGF-β1 | Transforming Growth Factor Beta 1. |
| TLR4 | Toll-Like Receptor 4. |
| TNF-α | Tumor Necrosis Factor-Alpha. |
| TRP | Transient Receptor Potential. |
| TUBB2A | Tubulin Beta 2A Class IIa. |
| VAS | Visual Analog Scale. |
References
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 3325–3348. [Google Scholar] [CrossRef]
- Burgess, J.; Ferdousi, M.; Gosal, D.; Boon, C.; Matsumoto, K.; Marshall, A.; Mak, T.; Marshall, A.; Frank, B.; Malik, R.A.; et al. Chemotherapy-Induced Peripheral Neuropathy: Epidemiology, Pathomechanisms and Treatment. Oncol. Ther. 2021, 9, 385–450. [Google Scholar] [CrossRef] [PubMed]
- Winters-Stone, K.M.; Horak, F.; Jacobs, P.G.; Trubowitz, P.; Dieckmann, N.F.; Stoyles, S.; Faithfull, S. Falls, Functioning, and Disability Among Women with Persistent Symptoms of Chemotherapy-Induced Peripheral Neuropathy. J. Clin. Oncol. 2017, 35, 2604–2612. [Google Scholar] [CrossRef]
- McCrary, J.M.; Goldstein, D.; Trinh, T.; Timmins, H.C.; Li, T.; Menant, J.; Friedlander, M.; Lewis, C.R.; Hertzberg, M.; O’Neill, S.; et al. Balance Deficits and Functional Disability in Cancer Survivors Exposed to Neurotoxic Cancer Treatments. J. Natl. Compr. Canc Netw. 2019, 17, 949–955. [Google Scholar] [CrossRef]
- Zajaczkowska, R.; Kocot-Kepska, M.; Leppert, W.; Wrzosek, A.; Mika, J.; Wordliczek, J. Mechanisms of Chemotherapy-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2019, 20, 1451. [Google Scholar] [CrossRef] [PubMed]
- Bae, E.H.; Greenwald, M.K.; Schwartz, A.G. Chemotherapy-Induced Peripheral Neuropathy: Mechanisms and Therapeutic Avenues. Neurotherapeutics 2021, 18, 2384–2396. [Google Scholar] [CrossRef] [PubMed]
- Mattar, M.; Umutoni, F.; Hassan, M.A.; Wamburu, M.W.; Turner, R.; Patton, J.S.; Chen, X.; Lei, W. Chemotherapy-Induced Peripheral Neuropathy: A Recent Update on Pathophysiology and Treatment. Life 2024, 14, 991. [Google Scholar] [CrossRef]
- Markham, M.J.; Wachter, K.; Agarwal, N.; Bertagnolli, M.M.; Chang, S.M.; Dale, W.; Diefenbach, C.S.M.; Rodriguez-Galindo, C.; George, D.J.; Gilligan, T.D.; et al. Clinical Cancer Advances 2020: Annual Report on Progress Against Cancer From the American Society of Clinical Oncology. J. Clin. Oncol. 2020, 38, 1081. [Google Scholar] [CrossRef]
- Avallone, A.; Bimonte, S.; Cardone, C.; Cascella, M.; Cuomo, A. Pathophysiology and Therapeutic Perspectives for Chemotherapy-induced Peripheral Neuropathy. Anticancer. Res. 2022, 42, 4667–4678. [Google Scholar] [CrossRef]
- Desforges, A.D.; Hebert, C.M.; Spence, A.L.; Reid, B.; Dhaibar, H.A.; Cruz-Topete, D.; Cornett, E.M.; Kaye, A.D.; Urits, I.; Viswanath, O. Treatment and diagnosis of chemotherapy-induced peripheral neuropathy: An update. Biomed. Pharmacother. 2022, 147, 112671. [Google Scholar] [CrossRef]
- Clavo, B.; Martinez-Sanchez, G.; Rodriguez-Esparragon, F.; Rodriguez-Abreu, D.; Galvan, S.; Aguiar-Bujanda, D.; Diaz-Garrido, J.A.; Canas, S.; Torres-Mata, L.B.; Fabelo, H.; et al. Modulation by Ozone Therapy of Oxidative Stress in Chemotherapy-Induced Peripheral Neuropathy: The Background for a Randomized Clinical Trial. Int. J. Mol. Sci. 2021, 22, 2802. [Google Scholar] [CrossRef]
- Szklener, K.; Rudzińska, A.; Juchaniuk, P.; Kabała, Z.; Mańdziuk, S. Ozone in Chemotherapy-Induced Peripheral Neuropathy—Current State of Art, Possibilities, and Perspectives. Int. J. Mol. Sci. 2023, 24, 5279. [Google Scholar] [CrossRef] [PubMed]
- Baeza-Noci, J.; Pinto-Bonilla, R. Systemic Review: Ozone: A Potential New Chemotherapy. Int. J. Mol. Sci. 2021, 22, 11796. [Google Scholar] [CrossRef] [PubMed]
- Clavo, B.; Santana-Rodriguez, N.; Llontop, P.; Gutierrez, D.; Suarez, G.; Lopez, L.; Rovira, G.; Martinez-Sanchez, G.; Gonzalez, E.; Jorge, I.J.; et al. Ozone Therapy as Adjuvant for Cancer Treatment: Is Further Research Warranted? Evid. Based Complement. Alternat Med. 2018, 2018, 7931849. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Pu, R. Ozone Therapy for Breast Cancer: An Integrative Literature Review. Integr. Cancer Ther. 2024, 23, 15347354241226667. [Google Scholar] [CrossRef]
- Was, H.; Borkowska, A.; Bagues, A.; Tu, L.; Liu, J.Y.H.; Lu, Z.; Rudd, J.A.; Nurgali, K.; Abalo, R. Mechanisms of Chemotherapy-Induced Neurotoxicity. Front. Pharmacol. 2022, 13, 750507. [Google Scholar] [CrossRef]
- Salat, K. Chemotherapy-induced peripheral neuropathy: Part 1-current state of knowledge and perspectives for pharmacotherapy. Pharmacol. Rep. 2020, 72, 486–507. [Google Scholar] [CrossRef]
- Yun, H.D.; Goel, Y.; Gupta, K. Crosstalk of Mast Cells and Natural Killer Cells with Neurons in Chemotherapy-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2023, 24, 12543. [Google Scholar] [CrossRef]
- Chua, K.C.; El-Haj, N.; Priotti, J.; Kroetz, D.L. Mechanistic insights into the pathogenesis of microtubule-targeting agent-induced peripheral neuropathy from pharmacogenetic and functional studies. Basic Clin. Pharmacol. Toxicol. 2022, 130 (Suppl. 1), 60–74. [Google Scholar] [CrossRef]
- Starobova, H.; Vetter, I. Pathophysiology of Chemotherapy-Induced Peripheral Neuropathy. Front. Mol. Neurosci. 2017, 10, 174. [Google Scholar] [CrossRef]
- Lazic, A.; Popović, J.; Paunesku, T.; Woloschak, G.E.; Stevanović, M. Insights into platinum-induced peripheral neuropathy-current perspective. Neural Regen. Res. 2020, 15, 1623–1630. [Google Scholar] [PubMed]
- Salat, K. Chemotherapy-induced peripheral neuropathy-part 2: Focus on the prevention of oxaliplatin-induced neurotoxicity. Pharmacol. Rep. 2020, 72, 508–527. [Google Scholar] [CrossRef]
- Xu, Y.; Jiang, Z.; Chen, X. Mechanisms underlying paclitaxel-induced neuropathic pain: Channels, inflammation and immune regulations. Eur. J. Pharmacol. 2022, 933, 175288. [Google Scholar] [CrossRef]
- Areti, A.; Yerra, V.G.; Naidu, V.; Kumar, A. Oxidative stress and nerve damage: Role in chemotherapy induced peripheral neuropathy. Redox Biol. 2014, 2, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Makkar, T.K.; Goel, L.; Pahuja, M. Role of inflammation and oxidative stress in chemotherapy-induced neurotoxicity. Immunol. Res. 2022, 70, 725–741. [Google Scholar] [CrossRef] [PubMed]
- da Costa, R.; Passos, G.F.; Quintao, N.L.M.; Fernandes, E.S.; Maia, J.; Campos, M.M.; Calixto, J.B. Taxane-induced neurotoxicity: Pathophysiology and therapeutic perspectives. Br. J. Pharmacol. 2020, 177, 3127–3146. [Google Scholar] [CrossRef]
- Fumagalli, G.; Monza, L.; Cavaletti, G.; Rigolio, R.; Meregalli, C. Neuroinflammatory Process Involved in Different Preclinical Models of Chemotherapy-Induced Peripheral Neuropathy. Front. Immunol. 2020, 11, 626687. [Google Scholar] [CrossRef]
- Koyanagi, M.; Imai, S.; Matsumoto, M.; Iguma, Y.; Kawaguchi-Sakita, N.; Kotake, T.; Iwamitsu, Y.; Ntogwa, M.; Hiraiwa, R.; Nagayasu, K.; et al. Pronociceptive Roles of Schwann Cell-Derived Galectin-3 in Taxane-Induced Peripheral Neuropathy. Cancer Res. 2021, 81, 2207–2219. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Hu, L.; Wang, C.; Yang, X.; Song, L.; Jiang, C.; Li, Y.; Li, T.; Liu, W.T.; Feng, J. p38/TF/HIF-alpha Signaling Pathway Participates in the Progression of CIPN in Mice. Biomed. Res. Int. 2019, 2019, 5347804. [Google Scholar]
- Omran, M.; Belcher, E.K.; Mohile, N.A.; Kesler, S.R.; Janelsins, M.C.; Hohmann, A.G.; Kleckner, I.R. Review of the Role of the Brain in Chemotherapy-Induced Peripheral Neuropathy. Front. Mol. Biosci. 2021, 8, 693133. [Google Scholar] [CrossRef]
- Park, S.B.; Kwok, J.B.; Asher, R.; Lee, C.K.; Beale, P.; Selle, F.; Friedlander, M. Clinical and genetic predictors of paclitaxel neurotoxicity based on patient- versus clinician-reported incidence and severity of neurotoxicity in the ICON7 trial. Ann. Oncol. 2017, 28, 2733–2740. [Google Scholar] [CrossRef] [PubMed]
- Shatunova, S.; Aktar, R.; Peiris, M.; Lee, J.Y.P.; Vetter, I.; Starobova, H. The role of the gut microbiome in neuroinflammation and chemotherapy-induced peripheral neuropathy. Eur. J. Pharmacol. 2024, 979, 176818. [Google Scholar] [CrossRef]
- Zhong, S.; Zhou, Z.; Liang, Y.; Cheng, X.; Li, Y.; Teng, W.; Zhao, M.; Liu, C.; Guan, M.; Zhao, C. Targeting strategies for chemotherapy-induced peripheral neuropathy: Does gut microbiota play a role? Crit. Rev. Microbiol. 2019, 45, 369–393. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.; Lim, G.; You, Z.; Ding, W.; Huang, P.; Ran, C.; Doheny, J.; Caravan, P.; Tate, S.; Hu, K.; et al. Gut microbiota is critical for the induction of chemotherapy-induced pain. Nat. Neurosci. 2017, 20, 1213–1216. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, C.; Corleto, J.; Ruegger, P.M.; Logan, G.D.; Peacock, B.B.; Mendonca, S.; Yamaki, S.; Adamson, T.; Ermel, R.; McKemy, D.; et al. Dominant Role of the Gut Microbiota in Chemotherapy Induced Neuropathic Pain. Sci. Rep. 2019, 9, 20324. [Google Scholar] [CrossRef]
- Pachman, D.R.; Dockter, T.; Zekan, P.J.; Fruth, B.; Ruddy, K.J.; Ta, L.E.; Lafky, J.M.; Dentchev, T.; Le-Lindqwister, N.A.; Sikov, W.M.; et al. A pilot study of minocycline for the prevention of paclitaxel-associated neuropathy: ACCRU study RU221408I. Support. Care Cancer 2017, 25, 3407–3416. [Google Scholar] [CrossRef]
- Hu, S.; Huang, K.M.; Adams, E.J.; Loprinzi, C.L.; Lustberg, M.B. Recent Developments of Novel Pharmacologic Therapeutics for Prevention of Chemotherapy-Induced Peripheral Neuropathy. Clin. Cancer Res. 2019, 25, 6295–6301. [Google Scholar] [CrossRef]
- Chen, X.; Gan, Y.; Au, N.P.B.; Ma, C.H.E. Current understanding of the molecular mechanisms of chemotherapy-induced peripheral neuropathy. Front. Mol. Neurosci. 2024, 17, 1345811. [Google Scholar] [CrossRef]
- Flatters, S.J.L.; Dougherty, P.M.; Colvin, L.A. Clinical and preclinical perspectives on Chemotherapy-Induced Peripheral Neuropathy (CIPN): A narrative review. Br. J. Anaesth. 2017, 119, 737–749. [Google Scholar] [CrossRef]
- Smith, E.M.; Pang, H.; Cirrincione, C.; Fleishman, S.; Paskett, E.D.; Ahles, T.; Bressler, L.R.; Fadul, C.E.; Knox, C.; Le-Lindqwister, N.; et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: A randomized clinical trial. JAMA 2013, 309, 1359–1367. [Google Scholar] [CrossRef]
- Wang, C.; Chen, S.; Jiang, W. Treatment for chemotherapy-induced peripheral neuropathy: A systematic review of randomized control trials. Front. Pharmacol. 2022, 13, 1080888. [Google Scholar] [CrossRef]
- Chung, K.H.; Park, S.B.; Streckmann, F.; Wiskemann, J.; Mohile, N.; Kleckner, A.S.; Colloca, L.; Dorsey, S.G.; Kleckner, I.R. Mechanisms, Mediators, and Moderators of the Effects of Exercise on Chemotherapy-Induced Peripheral Neuropathy. Cancers 2022, 14, 1224. [Google Scholar] [CrossRef] [PubMed]
- Childs, D.S.; Le-Rademacher, J.G.; McMurray, R.; Bendel, M.; O’Neill, C.; Smith, T.J.; Loprinzi, C.L. Randomized Trial of Scrambler Therapy for Chemotherapy-Induced Peripheral Neuropathy: Crossover Analysis. J. Pain. Symptom Manag. 2021, 61, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Kavelaars, A.; Dougherty, P.M.; Heijnen, C.J. Beyond symptomatic relief for chemotherapy-induced peripheral neuropathy: Targeting the source. Cancer 2018, 124, 2289–2298. [Google Scholar] [CrossRef] [PubMed]
- Ollodart, J.; Steele, L.R.; Romero-Sandoval, E.A.; Strowd, R.E.; Shiozawa, Y. Contributions of neuroimmune interactions to chemotherapy-induced peripheral neuropathy development and its prevention/therapy. Biochem. Pharmacol. 2024, 222, 116070. [Google Scholar] [CrossRef]
- Bocci, V.A.; Zanardi, I.; Travagli, V. Ozone acting on human blood yields a hormetic dose-response relationship. J. Transl. Med. 2011, 9, 66. [Google Scholar] [CrossRef]
- Hidalgo-Tallon, F.J.; Torres-Morera, L.M.; Baeza-Noci, J.; Carrillo-Izquierdo, M.D.; Pinto-Bonilla, R. Updated Review on Ozone Therapy in Pain Medicine. Front. Physiol. 2022, 13, 840623. [Google Scholar] [CrossRef]
- Travagli, V.; Iorio, E.L. The Biological and Molecular Action of Ozone and Its Derivatives: State-of-the-Art, Enhanced Scenarios, and Quality Insights. Int. J. Mol. Sci. 2023, 24, 8465. [Google Scholar] [CrossRef]
- Bardellini, E.; Amadori, F.; Merlo, J.; Chiappini, D.; Majorana, A. Ozone therapy for the treatment of paediatric chemotherapy-induced oral mucositis: A randomized double blind controlled study. Support. Care Cancer 2017, 25, S130–S131. [Google Scholar]
- Majorana, A.; Amadori, F.; Majorana, A.; Merlo, J. Ozonized water for treatment of oral mucositis in children: A pilot study. Support. Care Cancer 2021, 29, S114. [Google Scholar]
- Hayashi, K.; Onda, T.; Honda, H.; Ozawa, N.; Ohata, H.; Takano, N.; Shibahara, T. Effects of ozone nano-bubble water on mucositis induced by cancer chemotherapy. Biochem. Biophys. Rep. 2019, 20, 100697. [Google Scholar] [CrossRef]
- Ghorbani, F.; Yazdanian, M.; Tahmasebi, E.; Izadi, M.; Mofid, B.; Varpaei, H.A. Effect of Ozonated Water on Oral Mucositis and Pain Induced by Head and Neck Radiotherapy: A Cross-sectional Study. Arch. Neurosci. 2021, 8, e118914. [Google Scholar] [CrossRef]
- Clavo, B.; Gutierrez, D.; Martin, D.; Suarez, G.; Hernandez, M.A.; Robaina, F. Intravesical Ozone Therapy for Progressive Radiation-Induced Hematuria. J. Altern. Complement. Med. 2005, 11, 539–541. [Google Scholar] [CrossRef]
- Tricarico, G.; Travagli, V. The Relationship between Ozone and Human Blood in the Course of a Well-Controlled, Mild, and Transitory Oxidative Eustress. Antioxidants 2021, 10, 1946. [Google Scholar] [CrossRef] [PubMed]
- Viebahn-Haensler, R.; Leon Fernandez, O.S. Ozone as Redox Bioregulator in Preventive Medicine: The Molecular and Pharmacological Basis of the Low-Dose Ozone Concept-A Review. Int. J. Mol. Sci. 2023, 24, 15747. [Google Scholar] [CrossRef]
- Clavo, B.; Rodriguez-Esparragon, F.; Rodriguez-Abreu, D.; Martinez-Sanchez, G.; Llontop, P.; Aguiar-Bujanda, D.; Fernandez-Perez, L.; Santana-Rodriguez, N. Modulation of Oxidative Stress by Ozone Therapy in the Prevention and Treatment of Chemotherapy-Induced Toxicity: Review and Prospects. Antioxidants 2019, 8, 588. [Google Scholar] [CrossRef] [PubMed]
- Bocci, V.; Valacchi, G. Nrf2 activation as target to implement therapeutic treatments. Front. Chem. 2015, 3, 4. [Google Scholar] [CrossRef]
- Galie, M.; Covi, V.; Tabaracci, G.; Malatesta, M. The Role of Nrf2 in the Antioxidant Cellular Response to Medical Ozone Exposure. Int. J. Mol. Sci. 2019, 20, 4009. [Google Scholar] [CrossRef]
- Pecorelli, A.; Bocci, V.; Acquaviva, A.; Belmonte, G.; Gardi, C.; Virgili, F.; Ciccoli, L.; Valacchi, G. NRF2 activation is involved in ozonated human serum upregulation of HO-1 in endothelial cells. Toxicol. Appl. Pharmacol. 2013, 267, 30–40. [Google Scholar] [CrossRef]
- Re, L.; Martinez-Sanchez, G.; Bordicchia, M.; Malcangi, G.; Pocognoli, A.; Morales-Segura, M.A.; Rothchild, J.; Rojas, A. Is ozone pre-conditioning effect linked to Nrf2/EpRE activation pathway in vivo? A preliminary result. Eur. J. Pharmacol. 2014, 742, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Galie, M.; Costanzo, M.; Nodari, A.; Boschi, F.; Calderan, L.; Mannucci, S.; Covi, V.; Tabaracci, G.; Malatesta, M. Mild ozonisation activates antioxidant cell response by the Keap1/Nrf2 dependent pathway. Free Radic. Biol. Med. 2018, 124, 114–121. [Google Scholar] [CrossRef]
- Basu, P.; Averitt, D.L.; Maier, C.; Basu, A. The Effects of Nuclear Factor Erythroid 2 (NFE2)-Related Factor 2 (Nrf2) Activation in Preclinical Models of Peripheral Neuropathic Pain. Antioxidants 2022, 11, 430. [Google Scholar] [CrossRef] [PubMed]
- Buelna-Chontal, M.; Zazueta, C. Redox activation of Nrf2 & NF-kappaB: A double end sword? Cell Signal 2013, 25, 2548–2557. [Google Scholar]
- Cuadrado, A.; Martin-Moldes, Z.; Ye, J.; Lastres-Becker, I. Transcription factors NRF2 and NF-kappaB are coordinated effectors of the Rho family, GTP-binding protein RAC1 during inflammation. J. Biol. Chem. 2014, 289, 15244–15258. [Google Scholar] [CrossRef] [PubMed]
- Scassellati, C.; Galoforo, A.C.; Bonvicini, C.; Esposito, C.; Ricevuti, G. Ozone: A natural bioactive molecule with antioxidant property as potential new strategy in aging and in neurodegenerative disorders. Ageing Res. Rev. 2020, 63, 101138. [Google Scholar] [CrossRef]
- Yamamoto, S.; Egashira, N. Pathological Mechanisms of Bortezomib-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2021, 22, 888. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Chen, W.; Xia, J.; Lai, Z.; Yu, D.; Yao, J.; Cai, S. Effects of ozone autohemotherapy on blood VEGF, TGF-beta and PDGF levels after finger replantation. Ann. Palliat. Med. 2020, 9, 3332–3339. [Google Scholar] [CrossRef]
- Lantero, A.; Tramullas, M.; Pilar-Cuellar, F.; Valdizan, E.; Santillan, R.; Roques, B.P.; Hurle, M.A. TGF-beta and opioid receptor signaling crosstalk results in improvement of endogenous and exogenous opioid analgesia under pathological pain conditions. J. Neurosci. 2014, 34, 5385–5395. [Google Scholar] [CrossRef]
- Lu, L.; Pan, C.; Chen, L.; Hu, L.; Wang, C.; Han, Y.; Yang, Y.; Cheng, Z.; Liu, W.T. AMPK activation by peri-sciatic nerve administration of ozone attenuates CCI-induced neuropathic pain in rats. J. Mol. Cell Biol. 2017, 9, 132–143. [Google Scholar] [CrossRef]
- Valacchi, G.; Bocci, V. Studies on the biological effects of ozone: 11. Release of factors from human endothelial cells. Mediat. Inflamm. 2000, 9, 271–276. [Google Scholar] [CrossRef]
- Verrazzo, G.; Coppola, L.; Luongo, C.; Sammartino, A.; Giunta, R.; Grassia, A.; Ragone, R.; Tirelli, A. Hyperbaric oxygen, oxygen-ozone therapy, and rheologic parameters of blood in patients with peripheral occlusive arterial disease. Undersea Hyperb. Med. 1995, 22, 17–22. [Google Scholar]
- Giunta, R.; Coppola, A.; Luongo, C.; Sammartino, A.; Guastafierro, S.; Grassia, A.; Giunta, L.; Mascolo, L.; Tirelli, A.; Coppola, L. Ozonized autohemotransfusion improves hemorheological parameters and oxygen delivery to tissues in patients with peripheral occlusive arterial disease. Ann. Hematol. 2001, 80, 745–748. [Google Scholar] [CrossRef]
- Clavo, B.; Suarez, G.; Aguilar, Y.; Gutierrez, D.; Ponce, P.; Cubero, A.; Robaina, F.; Carreras, J.L. Brain ischemia and hypometabolism treated by ozone therapy. Forsch. Komplementmed 2011, 18, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Ruan, S.; Jia, R.; Hu, L.; Liu, Y.; Tian, Q.; Jiang, K.; Xia, X.; Tao, X.; Liu, W.T.; Pan, Y.; et al. Ozone promotes macrophage efferocytosis and alleviates neuropathic pain by activating the AMPK/Gas6-MerTK/SOCS3 signaling pathway. Front. Immunol. 2024, 15, 1455771. [Google Scholar] [CrossRef]
- Yu, Q.; Yang, X.; Zhang, C.; Zhang, X.; Wang, C.; Chen, L.; Liu, X.; Gu, Y.; He, X.; Hu, L.; et al. AMPK activation by ozone therapy inhibits tissue factor-triggered intestinal ischemia and ameliorates chemotherapeutic enteritis. FASEB J. 2020, 34, 13005–13021. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, Y.; Wu, H.; D’Alessandro, A.; Yegutkin, G.G.; Song, A.; Sun, K.; Li, J.; Cheng, N.Y.; Huang, A.; et al. Beneficial Role of Erythrocyte Adenosine A2B Receptor-Mediated AMP-Activated Protein Kinase Activation in High-Altitude Hypoxia. Circulation 2016, 134, 405–421. [Google Scholar] [CrossRef]
- Han, Y.; Smith, M.T. Pathobiology of cancer chemotherapy-induced peripheral neuropathy (CIPN). Front. Pharmacol. 2013, 4, 156. [Google Scholar] [CrossRef] [PubMed]
- Kocak, H.E.; Taskin, U.; Aydin, S.; Oktay, M.F.; Altinay, S.; Celik, D.S.; Yucebas, K.; Altas, B. Effects of ozone (O3) therapy on cisplatin-induced ototoxicity in rats. Eur. Arch. Otorhinolaryngol. 2016, 273, 4153–4159. [Google Scholar] [CrossRef]
- Zhang, X.T.; Zong, L.J.; Jia, R.M.; Qin, X.M.; Ruan, S.R.; Lu, L.L.; Wang, P.; Hu, L.; Liu, W.T.; Yang, Y.; et al. Ozone attenuates chemotherapy-induced peripheral neuropathy via upregulating the AMPK-SOCS3 axis. J. Cancer Res. Ther. 2023, 19, 1031–1039. [Google Scholar] [CrossRef]
- Clavo, B.; Santana-Rodriguez, N.; Llontop, P.; Gutierrez, D.; Ceballos, D.; Mendez, C.; Rovira, G.; Suarez, G.; Rey-Baltar, D.; Garcia-Cabrera, L.; et al. Ozone Therapy in the Management of Persistent Radiation-Induced Rectal Bleeding in Prostate Cancer Patients. Evid. Based Complement. Alternat Med. 2015, 2015, 480369. [Google Scholar] [CrossRef]
- Clavo, B.; Navarro, M.; Federico, M.; Borrelli, E.; Jorge, I.J.; Ribeiro, I.; Rodriguez-Melcon, J.I.; Carames, M.A.; Santana-Rodriguez, N.; Rodriguez-Esparragon, F. Long-Term Results with Adjuvant Ozone Therapy in the Management of Chronic Pelvic Pain Secondary to Cancer Treatment. Pain. Med. 2021, 22, 2138–2141. [Google Scholar] [CrossRef] [PubMed]
- Clavo, B.; Rodríguez-Abreu, D.; Galván, S.; Federico, M.; Martínez-Sánchez, G.; Ramallo-Fariña, Y.; Antonelli, C.; Benítez, G.; Rey-Baltar, D.; Jorge, I.J.; et al. Long-term improvement by ozone treatment in chronic pain secondary to chemotherapy-induced peripheral neuropathy: A preliminary report. Front. Physiol. 2022, 13, 935269. [Google Scholar] [CrossRef] [PubMed]
- Clavo, B.; Rodriguez-Abreu, D.; Galvan-Ruiz, S.; Federico, M.; Canovas-Molina, A.; Ramallo-Farina, Y.; Antonilli, C.; Benitez, G.; Fabelo, H.; Garcia-Lourve, C.; et al. Long-Term Effects of Ozone Treatment in Patients with Persistent Numbness and Tingling Secondary to Chemotherapy-Induced Peripheral Neuropathy. A Retrospective Study. Integr. Cancer Ther. 2025, 24, 15347354241307038. [Google Scholar] [CrossRef] [PubMed]
- Clavo, B.; Canovas-Molina, A.; Ramallo-Farina, Y.; Federico, M.; Rodriguez-Abreu, D.; Galvan, S.; Ribeiro, I.; Marques da Silva, S.C.; Navarro, M.; Gonzalez-Beltran, D.; et al. Effects of Ozone Treatment on Health-Related Quality of Life and Toxicity Induced by Radiotherapy and Chemotherapy in Symptomatic Cancer Survivors. Int. J. Environ. Res. Public Health 2023, 20, 1479. [Google Scholar] [CrossRef]
- Clavo, B.; Canovas-Molina, A.; Diaz-Garrido, J.A.; Canas, S.; Ramallo-Farina, Y.; Laffite, H.; Federico, M.; Rodriguez-Abreu, D.; Galvan, S.; Garcia-Lourve, C.; et al. Effects of ozone therapy on anxiety and depression in patients with refractory symptoms of severe diseases: A pilot study. Front. Psychol. 2023, 14, 1176204. [Google Scholar] [CrossRef]
- Loprinzi, C.; Le-Rademacher, J.G.; Majithia, N.; McMurray, R.P.; O’Neill, C.R.; Bendel, M.A.; Beutler, A.; Lachance, D.H.; Cheville, A.; Strick, D.M.; et al. Scrambler therapy for chemotherapy neuropathy: A randomized phase II pilot trial. Support. Care Cancer 2020, 28, 1183–1197. [Google Scholar] [CrossRef]
- Molassiotis, A.; Suen, L.K.P.; Cheng, H.L.; Mok, T.S.K.; Lee, S.C.Y.; Wang, C.H.; Lee, P.; Leung, H.; Chan, V.; Lau, T.K.H.; et al. A Randomized Assessor-Blinded Wait-List-Controlled Trial to Assess the Effectiveness of Acupuncture in the Management of Chemotherapy-Induced Peripheral Neuropathy. Integr. Cancer Ther. 2019, 18, 1534735419836501. [Google Scholar] [CrossRef]
- Martinez-Vega, B.; Leon, R.; Fabelo, H.; Ortega, S.; Callico, G.M.; Suarez-Vega, D.; Clavo, B. Oxygen Saturation Measurement using Hyperspectral Imaging targeting Real-Time Monitoring. In Proceedings of the 24th Euromicro Conference on Digital System Design (DSD), Palermo, Italy, 1–3 September 2021; pp. 480–487. [Google Scholar]
- Martinez-Vega, B.; Leon, R.; Fabelo, H.; Ortega, S.; Quevedo, E.; Canovas-Molina, A.; Rodriguez-Esparragon, F.; Clavo, B.; Callico, G.M. Analysis of the behavior of ozone therapy in chemotherapy-induced neuropathy using hyperspectral imaging technology. In Proceedings of the 26th Euromicro Conference on Digital System Design (DSD), Durres, Albania, 6–8 September 2023. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Number of Patients | Experimental Design | Main Results |
|---|---|---|---|
| Clavo et al., Antioxidants 2019 [56]. | (review) | Review of preclinical and limited clinical data on using ozone for chemotherapy toxicity | O3T may reduce chemotherapy-induced toxicity via antioxidant effects; limited clinical data for CIPN |
| Clavo et al., IJMS 2021 [11]. | (review + trial protocol) | Review of mechanisms and clinical/experimental data; description of ongoing RCT | Suggests O3T may modulate oxidative stress/inflammation in CIPN; highlights need for RCTs |
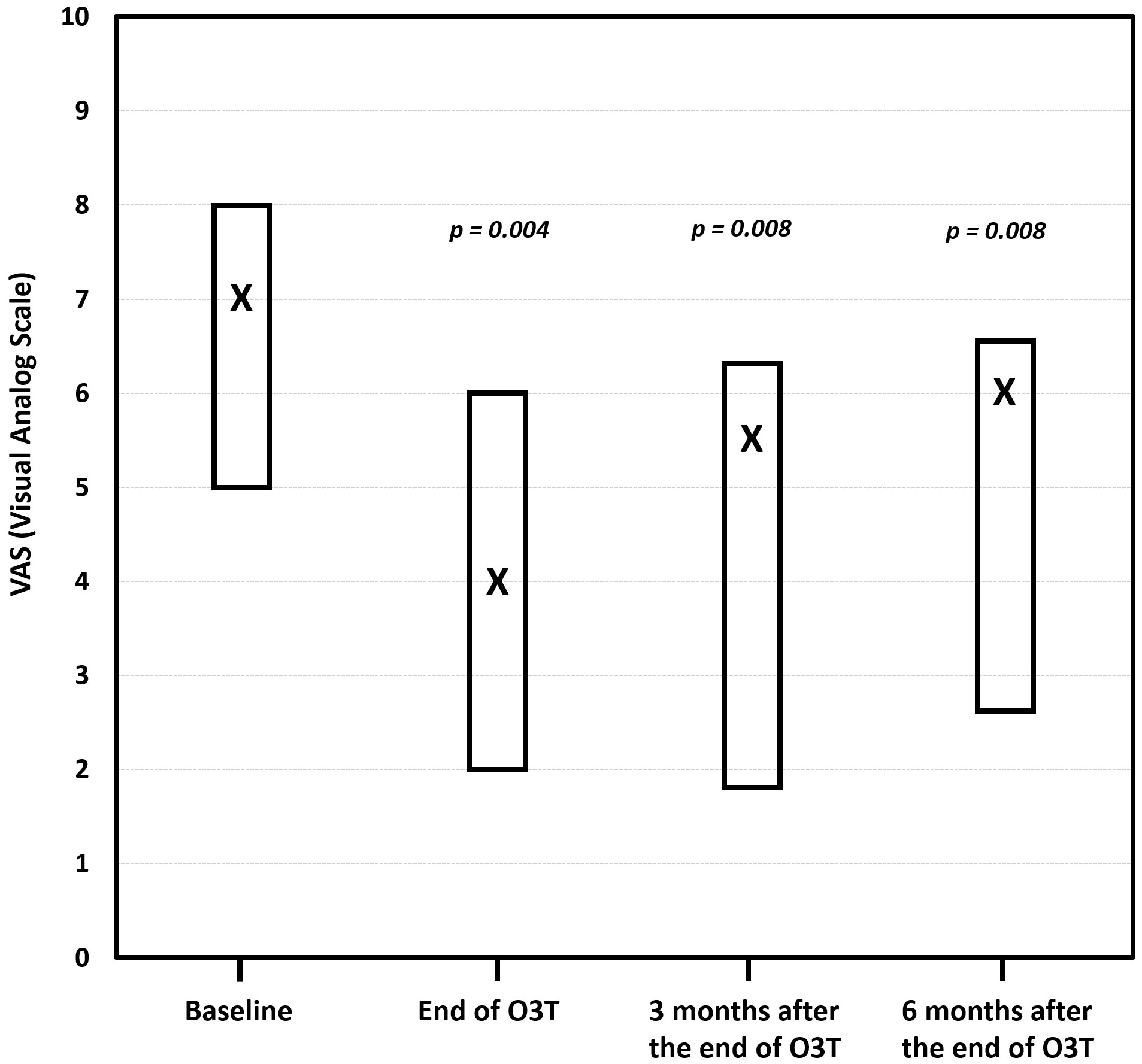
| Clavo et al., Front Physiol 2022 [82]. | 7 | Retrospective, preliminary report; rectal ozone insufflation in patients with chronic pain due to grade II/III CIPN; pain was assessed via VAS at baseline, end of treatment, and 3 and 6 months | Clinically relevant pain reduction in most patients; median VAS decreased from 7 to 4 at end of treatment; effect maintained at 3 and 6 months; CTCAE pain toxicity grade improved in 50% |
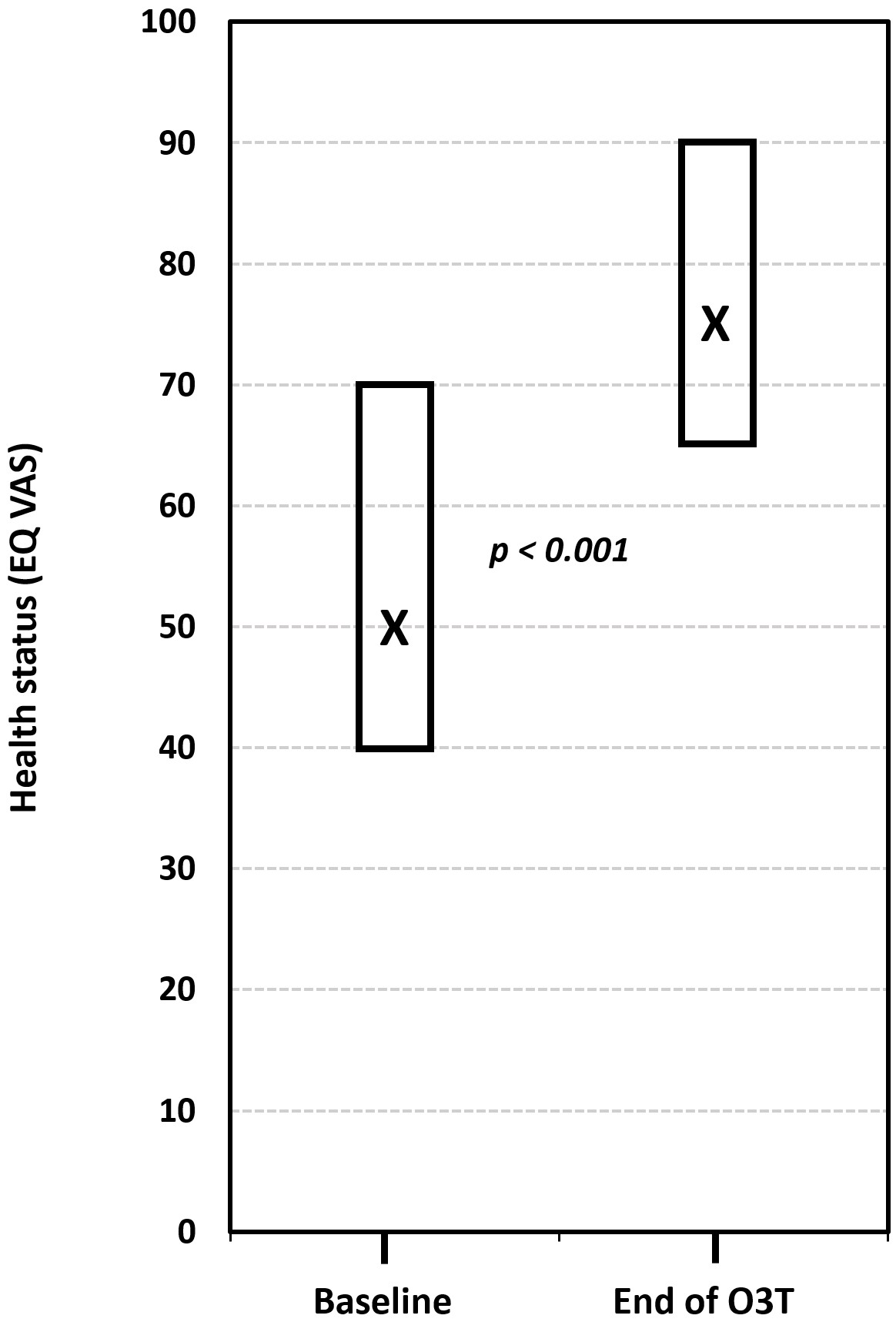
| Clavo et al., IJERPH 2023 [84]. | 26 (15 with CIPN) | Retrospective study; ozone in cancer survivors with chronic toxicity (radiotherapy/chemotherapy); HRQOL and toxicity assessed pre/post | Significant improvement in HRQOL and toxicity grade, including the subgroup of patients with CIPN |
| Szklener et al., IJMS 2023 [12] | (review) | Narrative review of ozone in CIPN | Summarizes rationale and limited clinical evidence; calls for RCTs |
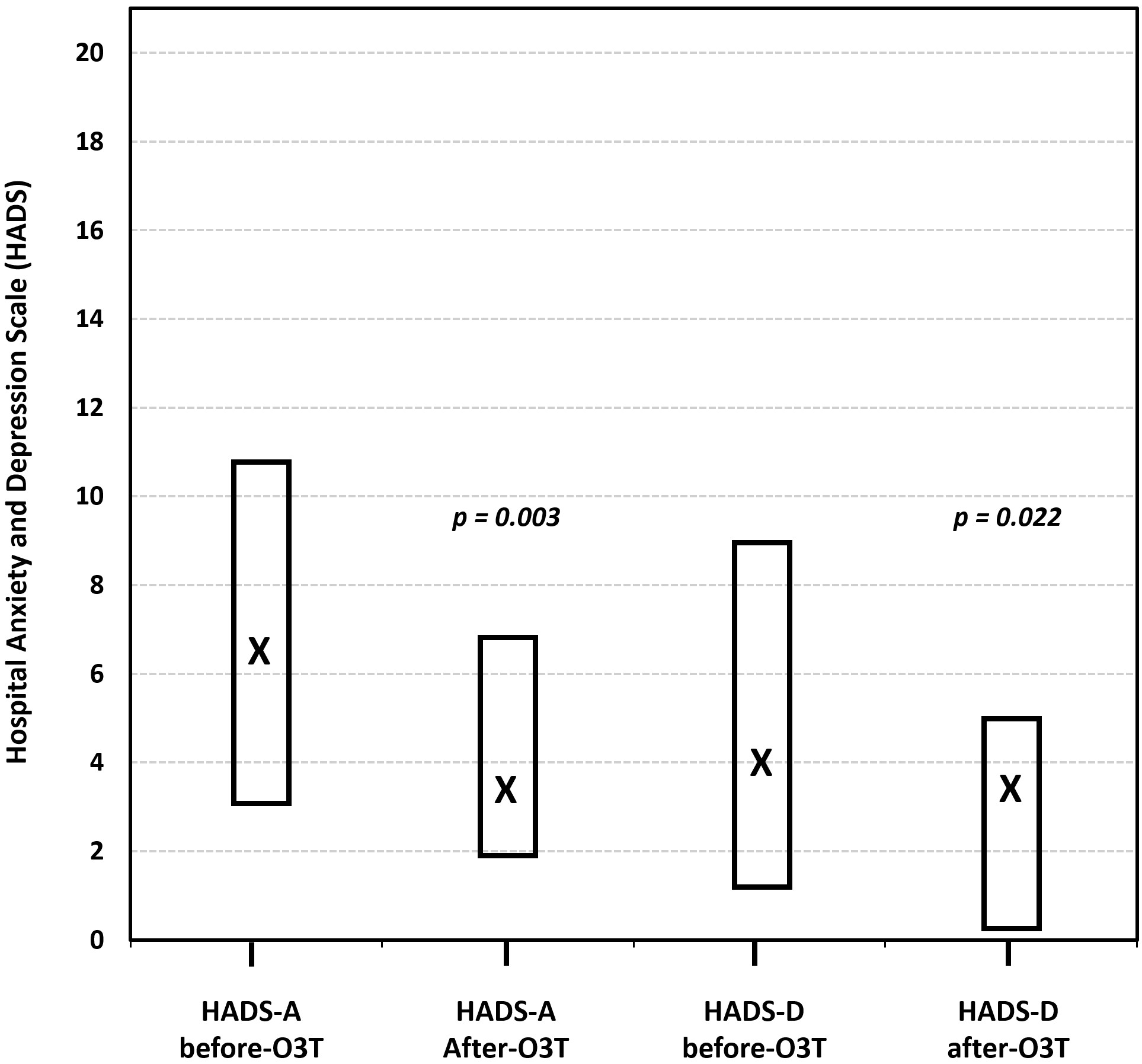
| Clavo et al., Front Psychol. 2023 [85] | 16 (8 with CIPN) | Retrospective study; several ozone treatments (mostly via rectal insufflation) in patients with refractory symptoms; assessment of anxiety and depression at baseline, post-treatment, and 3 and 6 months | Significant improvement in anxiety and depression measured via two questionnaires. Subgroup with CIPN not specified |
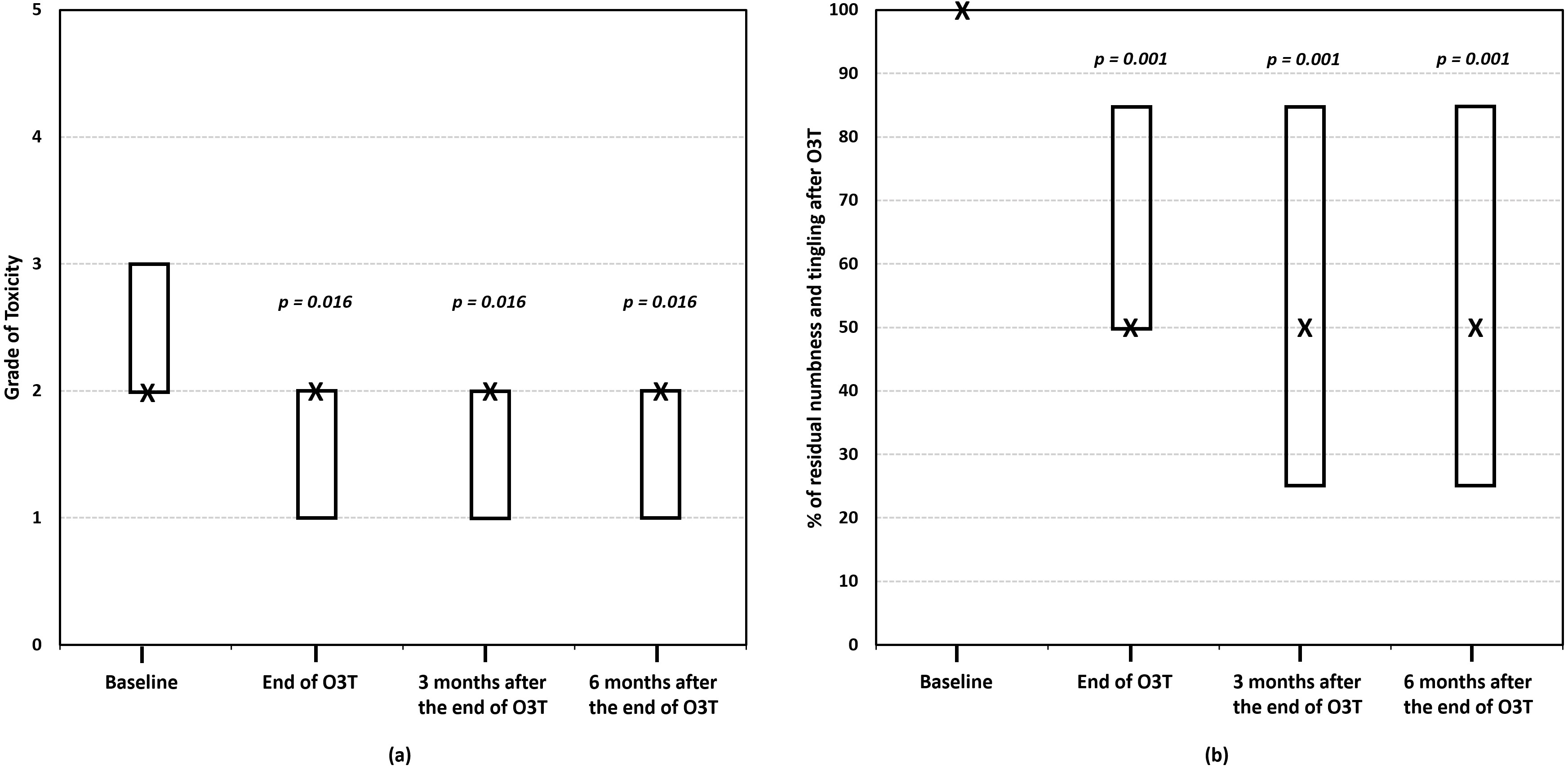
| Clavo et al., Integr Cancer Ther 2025 [83] | 15 | Retrospective study; rectal ozone insufflation (40 sessions over 4 months) in patients with persistent numbness/tingling due to grade II/III CIPN; assessment at baseline, post-treatment, and 3 and 6 months | 47% showed reduction in CIPN toxicity grade (p = 0.016); 67% reported ≥50% reduction in numbness/tingling (p = 0.002); effects sustained at 3 and 6 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clavo, B.; Cánovas-Molina, A.; Federico, M.; Martínez-Sánchez, G.; Benítez, G.; Galván, S.; Ramallo-Fariña, Y.; Fabelo, H.; Cazorla-Rivero, S.; Lago-Moreno, E.; et al. Ozone Treatment in the Management of Chemotherapy-Induced Peripheral Neuropathy: A Review of Rationale and Research Directions. Cancers 2025, 17, 2278. https://doi.org/10.3390/cancers17142278
Clavo B, Cánovas-Molina A, Federico M, Martínez-Sánchez G, Benítez G, Galván S, Ramallo-Fariña Y, Fabelo H, Cazorla-Rivero S, Lago-Moreno E, et al. Ozone Treatment in the Management of Chemotherapy-Induced Peripheral Neuropathy: A Review of Rationale and Research Directions. Cancers. 2025; 17(14):2278. https://doi.org/10.3390/cancers17142278
Chicago/Turabian StyleClavo, Bernardino, Angeles Cánovas-Molina, Mario Federico, Gregorio Martínez-Sánchez, Gretel Benítez, Saray Galván, Yolanda Ramallo-Fariña, Himar Fabelo, Sara Cazorla-Rivero, Elba Lago-Moreno, and et al. 2025. "Ozone Treatment in the Management of Chemotherapy-Induced Peripheral Neuropathy: A Review of Rationale and Research Directions" Cancers 17, no. 14: 2278. https://doi.org/10.3390/cancers17142278
APA StyleClavo, B., Cánovas-Molina, A., Federico, M., Martínez-Sánchez, G., Benítez, G., Galván, S., Ramallo-Fariña, Y., Fabelo, H., Cazorla-Rivero, S., Lago-Moreno, E., Antonilli, C., Díaz-Garrido, J. A., Jorge, I. J., Marrero-Callico, G., Rodríguez-Abreu, D., & Rodríguez-Esparragón, F. (2025). Ozone Treatment in the Management of Chemotherapy-Induced Peripheral Neuropathy: A Review of Rationale and Research Directions. Cancers, 17(14), 2278. https://doi.org/10.3390/cancers17142278