
CAR-Based Cell Therapy in Head and Neck Cancer: A Comprehensive Review on Clinical Applicability



Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
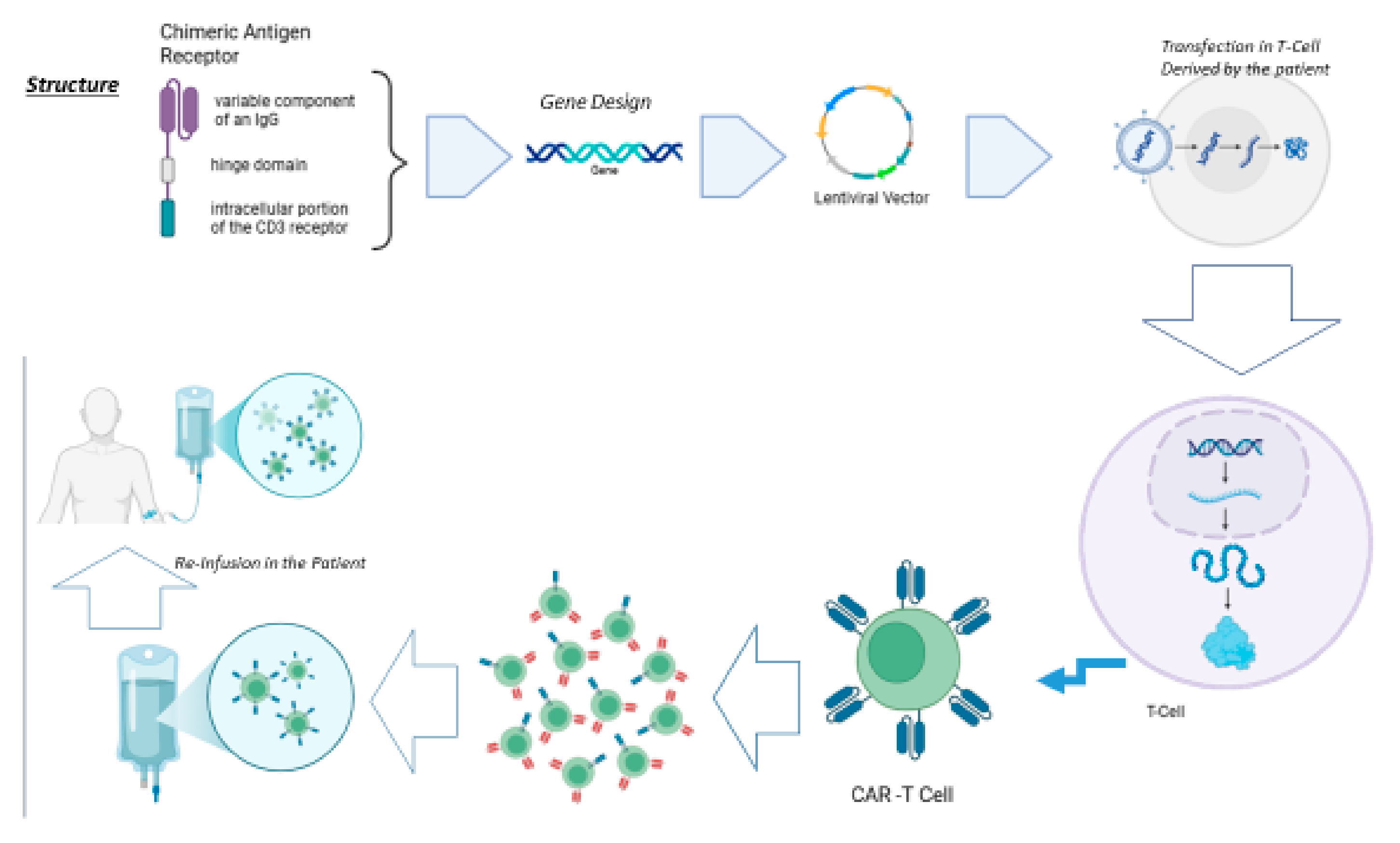
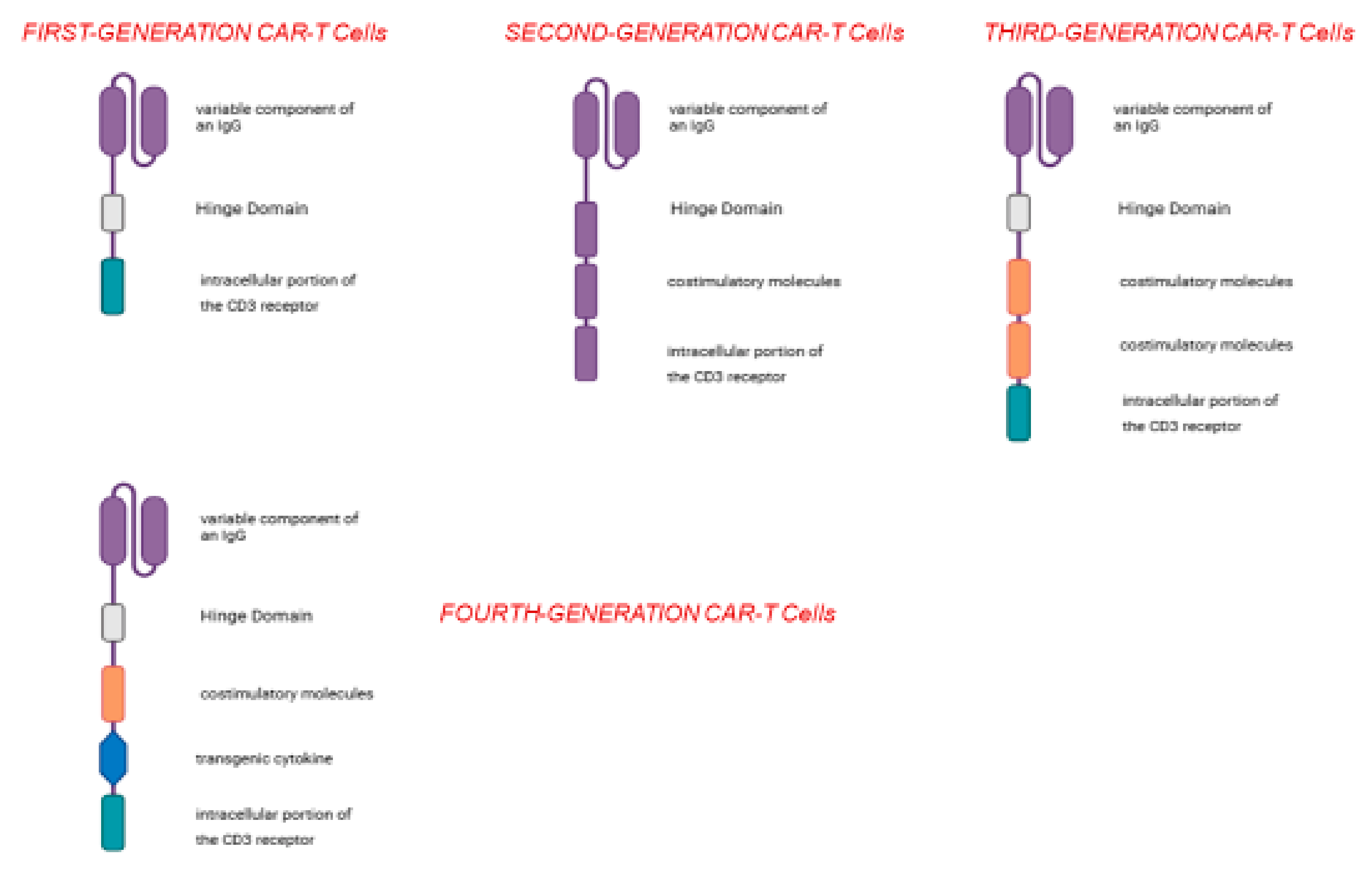
3.1. CARs Structure
3.2. Overview of CAR-T Applicability in HNC
3.3. CAR-T Cells in Preclinical Trials in HNC
3.3.1. Enhancing CAR-T Cell Infiltration and Persistence in the Tumor Microenvironment
3.3.2. Engineering Immune Function and Resistance to Immune Suppression
3.3.3. Targeting Tumor-Associated Antigens (TAAs) in HNSCC
- (i)
- The Ephrin type-B receptor 4 (EPHB4), a receptor tyrosine kinase, is notably overexpressed in oral squamous cell carcinoma (OSCC), and this overexpression correlates with poor prognosis, making EPHB4 a broadly relevant target in HNSCC and a promising candidate for CAR-T cell therapy [32,33,34,35,36,37,38]. Ito et al. demonstrated that EPHB4-CAR-T cells, especially when administered intratumorally, showed significant tumor regression and T infiltration in both OSCC xenograft and patient-derived xenograft (PDX) models [32].
- (ii)
- (iii)
- The ErbB family of receptor tyrosine kinases (RTKs)—Epidermal Growth Factor Receptor (EGFR), Human EGFR Related 2 (HER2), Human EGFR Related 3 (HER3) and Human EGFR Related 4 (HER4)—is implicated in HNSCC pathogenesis [42]. EGFR is overexpressed in >90% of HNSCC, and its overexpression is due to a gene amplification. The result of this anomaly is the upregulation of some intracellular pathways related to cell survival, including PI3-K/Akt/mTHOR, JAK/STAT, and Ras/Raf/MEK/ERK-MAPK [43,44,45]. EGFR- CAR-T-cells induced the release of pro-inflammatory cytokines, such as IL-4, IL-10, TNF-α, and IFN-γ, enhancing downstream immune responses [7]. In addition to EGFR gene amplification, overexpression of the EGFR-Her2 heterodimer in HNSCC is also strongly involved in neoplastic progression and the development of distant metastases [46]. HER2 may be used as TAA to engineer specific CARs. Shaw et al. [47] hypothesized that modifying the TME before CAR-T cells injection could increase the efficacy of the treatment. In fact, the authors injected FaDu cells HER2-specific CAR-T cells when combined with a specific oncolytic adenovirus (CAd) encoding the PD-L1-blocking antibody, and IL-12p70 (CAd12_PDL1) produced tumor regression and extended survival in xerograft and orthotopic models [47].
- (iv)
- CD70 is a potent costimulatory molecule and plays a crucial role in immune-system activation, specifically by improving T-cell and B-cell activation, proliferation, and survival. Although they are overexpressed in only 20% of HNSCC, Park et al. showed that CD70-specific CAR-T cells specifically recognized and efficiently eliminated CD70-positive HNSCC cells in vitro [48,49,50].
- (v)
- c-MET is a transmembrane receptor, and its aberrant signal transduction stimulates tumorigenesis with the acquisition of invasive and metastatic phenotypes [51]. c-MET is overexpressed in nasopharyngeal carcinoma (NPC) [52]. Huo et al. demonstrated the efficacy of c-MET targeted CAR-T cells both in vitro and in xenograft models (SCID mice), highlighting its therapeutic relevance in NPC [53].
- (vi)
- CD44v6, a glycoprotein isoform associated with metastasis and tumor progression, is particularly overexpressed in HNSCC, and it can be used as a target for immunotherapy [54,55,56]. Both CAR-T cells and CAR-NK cells targeting CD44v6 showed high efficacy against HNSCC-derived cell lines, with CAR-NK cells offering enhanced safety due to their non-MHC-restricted mechanism of target recognition [57,58].
3.3.4. CAR-NK Cell Therapy: A Safer Alternative
3.4. CAR-T Cells in Phase I Clinical Trials in HNC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| HNC | Head neck cancer |
| TAAs | Tumor-associated antigens |
| MHC | Major histocompatibility complex |
| TME | Tumor microenvironment |
| T-Reg | Regulatory T cells |
| NK | Natural killer |
| ADCC | Antibody-dependent cellular cytotoxicity |
| EBV | Epstein–Barr virus |
| HPV | Human papillomavirus |
| CAR-T | Chimeric antigen receptor T cell |
| PD-1 | Programmed Death-1 |
| PD-L1 | Programmed Death-Ligand 1 |
| HNSCC | Head and neck squamous cell carcinoma |
| CPS | Combined positive score |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| CTLs | Cytotoxic T lymphocytes |
| ICIs | Immune checkpoint inhibitors |
| CAF | Cancer-associated fibroblasts |
| PTT | Photothermal therapy |
| TIM-3 | Immunoglobulin and Mucin Domain-Containing 3 |
| iCAR-T | Inhibitory CAR-T |
| EPHB4 | Ephrin type-B receptor 4 |
| Eph | Erythropoietin-producing hepatocellular |
| OCSCC | Oral squamous cell carcinoma |
| PDX | Patient-derived xenograft |
| IHC | Immunoistochemistry |
| MUC1 | Mucin 1 |
| HIF-1 | Hypoxia inducible factor |
| RTKs | Receptor tyrosine kinases |
| Cad | Oncolytic adenovirus |
| HGF | Hepatocyte growth factor |
| NPC | Nasopharyngeal carcinoma |
| GvHD | Graft-versus-host disease |
| DLTs | Dose-limiting toxicities |
| EGFR | Epidermal growth factor receptor |
| HER2 | Human EGFR Related 2 |
| HER3 | Human EGFR Related 2 |
| HER4 | Human EGFR Related 4 |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Zhang, K.; Lam, A.K.; Huang, J.; Qiu, F.; Qiao, B.; Zhang, Y. MUC1 as a target for CAR-T therapy in head and neck squamous cell carinoma. Cancer Med. 2020, 9, 640–652. [Google Scholar] [CrossRef]
- Leemans, C.R.; Braakhuis, B.J.; Brakenhoff, R.H. The molecular biology of head and neck cancer. Nat. Rev. Cancer 2011, 11, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Prasad, V.; Kaestner, V. Nivolumab and pembrolizumab: Monoclonal antibodies against programmed cell death-1 (PD-1) that are interchangeable. Semin. Oncol. 2017, 44, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Dong, Y.H.; Ding, Y.M.; Guo, W.; Huang, J.W.; Yang, Z.; Zhang, Y.; Chen, X.H. The functional verification of EGFR-CAR T-cells targeted to hypopharyngeal squamous cell carcinoma. Onco Targets Ther. 2018, 11, 7053–7059. [Google Scholar] [CrossRef]
- Lu, J.; Jiang, G. The journey of CAR-T therapy in hematological malignancies. Mol. Cancer 2022, 21, 194. [Google Scholar] [CrossRef]
- Hu, C.; Liu, M.; Li, Y.; Zhao, Y.; Sharma, A.; Liu, H.; Schmidt-Wolf, I.G.H. Recent advances and future perspectives of CAR-T cell therapy in head and neck cancer. Front. Immunol. 2023, 14, 1213716. [Google Scholar] [CrossRef]
- Sterner, R.C.; Sterner, R.M. CAR-T cell therapy: Current limitations and potential strategies. Blood Cancer J. 2021, 11, 69. [Google Scholar] [CrossRef]
- Labanieh, L.; Mackall, C.L. CAR immune cells: Design principles, resistance and the next generation. Nature 2023, 614, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Summers, S.E.; Salih, V.; Foey, A.D. ErbB- and MUC1-targeted CAR-T cell immunotherapy of oral squamous cell carcinoma. Front. Dent. Med. 2023, 4, 1116402. [Google Scholar] [CrossRef] [PubMed]
- Harrington, K.J.; Burtness, B.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Brana, I.; Basté, N.; Neupane, P.; et al. Pembrolizumab With or Without Chemotherapy in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: Updated Results of the Phase III KEYNOTE-048 Study. J. Clin. Oncol. 2023, 41, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Harrington, K.J.; Ferris, R.L.; Blumenschein, G., Jr.; Colevas, A.D.; Fayette, J.; Licitra, L.; Kasper, S.; Even, C.; Vokes, E.E.; Worden, F.; et al. Nivolumab versus standard, single-agent therapy of investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck (CheckMate 141): Health-related quality-of-life results from a randomised, phase 3 trial. Lancet Oncol. 2017, 18, 1104–1115. [Google Scholar] [CrossRef]
- Perri, F.; Ionna, F.; Longo, F.; Della Vittoria Scarpati, G.; De Angelis, C.; Ottaiano, A.; Botti, G.; Caponigro, F. Immune Response Against Head and Neck Cancer: Biological Mechanisms and Implication on Therapy. Transl. Oncol. 2020, 13, 262–274. [Google Scholar] [CrossRef]
- van Schalkwyk, M.C.I.; Papa, S.E.; Jeannon, J.-P.; Guerrero Urbano, T.; Spicer, J.F.; Maher, J. Design of a phase I clinical trial to evaluate intratumoral delivery of ErbB-targeted chimeric antigen receptor T-cells in locally advanced or recurrent head andneck cancer. Hum. Gene Ther. Clin. Dev. 2013, 24, 134–142. [Google Scholar] [CrossRef]
- Okuyama, K.; Yanamoto, S. Comment on “The characterization of tumor immune microenvironment after neoadjuvant immunotherapy in head and neck squamous cell cancer using multiplex immunohistochemistry”. Oral. Oncol. 2025, 162, 107213. [Google Scholar] [CrossRef]
- Qu, H.; Zhao, J.; Zuo, X.; He, H.; Wang, X.; Li, H.; Zhang, K. TGF-β-mediated activation of fibroblasts in cervical cancer: Implications for tumor microenvironment and prognosis. PeerJ 2025, 13, e19072. [Google Scholar] [CrossRef]
- Wang, H.Q.; Fu, R.; Man, Q.W.; Yang, G.; Liu, B.; Bu, L.L. Advances in CAR-T Cell Therapy in Head and Neck Squamous Cell Carcinoma. J. Clin. Med. 2023, 12, 2173. [Google Scholar] [CrossRef]
- Ye, B.; Stary, C.M.; Li, X.; Gao, Q.; Kang, C.; Xiong, X. Engineering chimeric antigen receptor-T cells for cancer treatment. Mol. Cancer 2018, 17, 32. [Google Scholar] [CrossRef]
- Zhang, E.; Gu, J.; Xu, H. Prospects for chimeric antigen receptor-modified T cell therapy for solid tumors. Mol. Cancer 2018, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- van der Stegen, S.J.; Davies, D.M.; Wilkie, S.; Foster, J.; Sosabowski, J.K.; Burnet, J.; Whilding, L.M.; Petrovic, R.M.; Ghaem-Maghami, S.; Mather, S.; et al. Preclinical in vivo modeling of cytokine release syndrome induced by ErbB-retargeted human T cells: Identifying a window of therapeutic opportunity? J. Immunol. 2013, 191, 4589–4598. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Hu, Q.; Dukhovlinova, E.; Chen, G.; Ahn, S.; Wang, C.; Ogunnaike, E.A.; Ligler, F.S.; Dotti, G.; Gu, Z. Photothermal Therapy Promotes Tumor Infiltration and Antitumor Activity of CAR T Cells. Adv. Mater. 2019, 31, e1900192. [Google Scholar] [CrossRef]
- Yeku, O.O.; Purdon, T.J.; Koneru, M.; Spriggs, D.; Brentjens, R.J. Armored CAR T cells enhance antitumor efficacy and overcome the tumor microenvironment. Sci. Rep. 2017, 7, 10541. [Google Scholar] [CrossRef]
- Adachi, K.; Kano, Y.; Nagai, T.; Okuyama, N.; Sakoda, Y.; Tamada, K. IL-7 and CCL19 expression in CAR-T cells improves immune cell infiltration and CAR-T cell survival in the tumor. Nat. Biotechnol. 2018, 36, 346–351. [Google Scholar] [CrossRef]
- Chmielewski, M.; Abken, H. CAR T Cells Releasing IL-18 Convert to T-Bethigh FoxO1low Effectors that Exhibit Augmented Activity against Advanced Solid Tumors. Cell Rep. 2017, 21, 3205–3219. [Google Scholar] [CrossRef]
- Giuffrida, L.; Sek, K.; Henderson, M.A.; House, I.G.; Lai, J.; Chen, A.X.Y.; Todd, K.L.; Petley, E.V.; Mardiana, S.; Todorovski, I.; et al. IL-15 Preconditioning Augments CAR T Cell Responses to Checkpoint Blockade for Improved Treatment of Solid Tumors. Mol. Ther. 2020, 28, 2379–2393. [Google Scholar] [CrossRef]
- Ma, X.; Shou, P.; Smith, C.; Chen, Y.; Du, H.; Sun, C.; Porterfield Kren, N.; Michaud, D.; Ahn, S.; Vincent, B.; et al. Interleukin-23 engineering improves CAR T cell function in solid tumors. Nat. Biotechnol. 2020, 38, 448–459. [Google Scholar] [CrossRef]
- Zou, F.; Lu, L.; Liu, J.; Xia, B.; Zhang, W.; Hu, Q.; Liu, W.; Zhang, Y.; Lin, Y.; Jing, S.; et al. Engineered triple inhibitory receptor resistance improves anti-tumor CAR-T cell performance via CD56. Nat. Commun. 2019, 10, 4109. [Google Scholar] [CrossRef]
- Marofi, F.; Motavalli, R.; Safonov, V.A.; Thangavelu, L.; Yumashev, A.V.; Alexander, M.; Shomali, N.; Chartrand, M.S.; Pathak, Y.; Jarahian, M.; et al. CAR T cells in solid tumors: Challenges and opportunities. Stem Cell Res. Ther. 2021, 12, 81. [Google Scholar] [CrossRef]
- Sun, Z.; Wang, C.; Zhao, Y.; Ling, Q. CAR-T cell therapy in advanced thyroid cancer: From basic to clinical. Front. Immunol. 2024, 15, 1411300. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Suzuki, T.; Shimomura, M.; Takenouchi, K.; Ohnuki, K.; Shoda, K.; Kenmochi, Y.; Yagyu, S.; Matsuura, K.; Hayashi, R.; et al. Feasibility of Intratumoral Administration With EPHB4-CAR-T Cells for the Treatment of Oral Squamous Cell Carcinoma. Cancer Sci. 2025, 116, 1227–1238. [Google Scholar] [CrossRef] [PubMed]
- Gucciardo, E.; Sugiyama, N.; Lehti, K. Eph- and ephrin-dependent mechanisms in tumor and stem cell dynamics. Cell Mol. Life Sci. 2014, 71, 3685–3710. [Google Scholar] [CrossRef] [PubMed]
- Eph Nomenclature Committee. Unified nomenclature for Eph family receptors and their ligands, the ephrins. Cell 1997, 90, 403–404. [Google Scholar] [CrossRef]
- Nakamoto, M.; Bergemann, A.D. Diverse roles for the Eph family of receptor tyrosine kinases in carcinogenesis. Microsc. Res. Tech. 2002, 59, 58–67. [Google Scholar] [CrossRef]
- Noren, N.K.; Foos, G.; Hauser, C.A.; Pasquale, E.B. The EphB4 receptor suppresses breast cancer cell tumorigenicity through an Abl-Crk pathway. Nat. Cell Biol. 2006, 8, 815–825. [Google Scholar] [CrossRef]
- Yi, C.; Zhang, X.; Li, H.; Chen, G.; Zeng, B.; Li, Y.; Wang, C.; He, Y.; Chen, X.; Huang, Z.; et al. EPHB4 Regulates the Proliferation and Metastasis of Oral Squamous Cell Carcinoma through the HMGB1/NF-κB Signalling Pathway. J. Cancer 2021, 12, 5999–6011. [Google Scholar] [CrossRef]
- Kubo, H.; Yagyu, S.; Nakamura, K.; Yamashima, K.; Tomida, A.; Kikuchi, K.; Iehara, T.; Nakazawa, Y.; Hosoi, H. Development of non-viral, ligand-dependent, EPHB4-specific chimeric antigen receptor T cells for treatment of rhabdomyosarcoma. Mol. Ther. Oncolytics 2021, 20, 646–658. [Google Scholar] [CrossRef]
- Lee, M.Y.; Robbins, Y.; Sievers, C.; Friedman, J.; Abdul Sater, H.; Clavijo, P.E.; Judd, N.; Tsong, E.; Silvin, C.; Soon-Shiong, P.; et al. Chimeric antigen receptor engineered NK cellular immunotherapy overcomes the selection of T-cell escape variant cancer cells. J. Immunother. Cancer 2021, 9, e002128. [Google Scholar] [CrossRef]
- Utispan, K.; Koontongkaew, S. Mucin 1 regulates the hypoxia response in head and neck cancer cells. J. Pharmacol. Sci. 2021, 147, 331–339. [Google Scholar] [CrossRef]
- Swartz, J.E.; Pothen, A.J.; Stegeman, I.; Willems, S.M.; Grolman, W. Clinical implications of hypoxia biomarker expression in head and neck squamous cell carcinoma: A systematic review. Cancer Med. 2015, 4, 1101–1116. [Google Scholar] [CrossRef] [PubMed]
- Tebbutt, N.; Pedersen, M.W.; Johns, T.G. Targeting the ERBB family in cancer: Couples therapy. Nat. Rev. Cancer 2013, 13, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Sweeny, L.; Dean, N.R.; Magnuson, J.S.; Carroll, W.R.; Helman, E.E.; Hyde, S.O.; Desmond, R.L.; Rosenthal, E.L. EGFR expression in advanced head and neck cutaneous squamous cell carcinoma. Head. Neck 2012, 34, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Costa, V.; Kowalski, L.P.; Coutinho-Camillo, C.M.; Begnami, M.D.; Calsavara, V.F.; Neves, J.I.; Kaminagakura, E. EGFR amplification and expression in oral squamous cell carcinoma in young adults. Int. J. Oral. Maxillofac. Surg. 2018, 47, 817–823. [Google Scholar] [CrossRef]
- Papa, S.; Adami, A.; Metoudi, M.; Beatson, R.; George, M.S.; Achkova, D.; Williams, E.; Arif, S.; Reid, F.; Elstad, M.; et al. Intratumoral pan-ErbB targeted CAR-T for head and neck squamous cell carcinoma: Interim analysis of the T4 immunotherapy study. J. Immunother. Cancer 2023, 11, e007162. [Google Scholar] [CrossRef]
- Pollock, N.I.; Grandis, J.R. HER2 as a therapeutic target in head and neck squamous cell carcinoma. Clin. Cancer Res. 2015, 21, 526–533. [Google Scholar] [CrossRef]
- Rosewell Shaw, A.; Porter, C.E.; Watanabe, N.; Tanoue, K.; Sikora, A.; Gottschalk, S.; Brenner, M.K.; Suzuki, M. Adenovirotherapy Delivering Cytokine and Checkpoint Inhibitor Augments CAR T Cells against Metastatic Head and Neck Cancer. Mol. Ther. 2017, 25, 2440–2451. [Google Scholar] [CrossRef]
- Rav, E.; Maegawa, S.; Gopalakrishnan, V.; Gordon, N. Overview of CD70 as a Potential Therapeutic Target for Osteosarcoma. J. Immunol. 2023, 211, 1067–1072. [Google Scholar] [CrossRef]
- De Meulenaere, A.; Vermassen, T.; Aspeslagh, S.; Zwaenepoel, K.; Deron, P.; Duprez, F.; Ferdinande, L.; Rottey, S. CD70 Expression and Its Correlation with Clinicopathological Variables in Squamous Cell Carcinoma of the Head and Neck. Pathobiology 2016, 83, 327–333. [Google Scholar] [CrossRef]
- Park, Y.P.; Jin, L.; Bennett, K.B.; Wang, D.; Fredenburg, K.M.; Tseng, J.E.; Chang, L.J.; Huang, J.; Chan, E.K.L. CD70 as a target for chimeric antigen receptor T cells in head and neck squamous cell carcinoma. Oral. Oncol. 2018, 78, 145–150. [Google Scholar] [CrossRef]
- Szturz, P.; Raymond, E.; Abitbol, C.; Albert, S.; de Gramont, A.; Faivre, S. Understanding c-MET signalling in squamous cell carcinoma of the head & neck. Crit. Rev. Oncol. Hematol. 2017, 111, 39–51. [Google Scholar] [PubMed]
- Luan, T.; Yu, Y. Increased hepatocyte growth factor and c-Met receptor expression in nasopharyngeal carcinoma. Int. J. Clin. Exp. Med. 2014, 7, 5583–5587. [Google Scholar] [PubMed]
- Huo, Q.; Lv, J.; Zhang, J.; Huang, H.; Hu, H.; Zhao, Y.; Zhang, X.; Wang, Y.; Zhou, Y.; Qiu, J.; et al. c-Met is a chimeric antigen receptor T-cell target for treating recurrent nasopharyngeal carcinoma. Cytotherapy 2023, 25, 1037–1047. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Zhao, M.; Zhu, J.; Li, T.; Yan, M.; Xing, K.; Liu, P.; Yu, S.; Ma, J.; He, H. Natural killer cells: A future star for immunotherapy of head and neck squamous cell carcinoma. Front. Immunol. 2024, 15, 1442673. [Google Scholar] [CrossRef]
- Kim, C.; Han, M.; Kim, G.; Son, W.; Kim, J.; Gil, M.; Rhee, Y.H.; Sim, N.S.; Kim, C.G.; Kim, H.R. Preclinical investigation of anti-tumor efficacy of allogeneic natural killer cells combined with cetuximab for head and neck squamous cell carcinoma. Cancer Immunol. Immunother. 2025, 74, 144. [Google Scholar] [CrossRef]
- Lodewijk, I.; Dueñas, M.; Paramio, J.M.; Rubio, C. CD44v6, STn & O-GD2: Promising tumor associated antigens paving the way for new targeted cancer therapies. Front. Immunol. 2023, 14, 1272681. [Google Scholar]
- Ciulean, I.S.; Fischer, J.; Quaiser, A.; Bach, C.; Abken, H.; Tretbar, U.S.; Fricke, S.; Koehl, U.; Schmiedel, D.; Grunwald, T. CD44v6 specific CAR-NK cells for targeted immunotherapy of head and neck squamous cell carcinoma. Front. Immunol. 2023, 14, 1290488. [Google Scholar] [CrossRef]
- Haist, C.; Poschinski, Z.; Bister, A.; Hoffmann, M.J.; Grunewald, C.M.; Hamacher, A.; Kassack, M.; Wiek, C.; Scheckenbach, K.; Hanenberg, H. Engineering a single-chain variable fragment of cetuximab for CAR T-cell therapy against head and neck squamous cell carcinomas. Oral. Oncol. 2022, 129, 105867. [Google Scholar] [CrossRef]
- Geldres, C.; Savoldo, B.; Hoyos, V.; Caruana, I.; Zhang, M.; Yvon, E.; Del Vecchio, M.; Creighton, C.J.; Ittmann, M.; Ferrone, S.; et al. T lymphocytes redirected against the chondroitin sulfate proteoglycan-4 control the growth of multiple solid tumors both in vitro and in vivo. Adv. Mater. 2019, 31, e1900192. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Type | Model | Technique | TAA | Results | |
|---|---|---|---|---|---|
| Cancer Sci. 2025 Mar 3 [32] | Pre-Clinical | Xenograft | 2 generation EPHB4-CAR-T cells | EPHB4 | Tumor volume reduction |
| Cancer Med. 2020; 9(2): 640–652. [39] | Pre-Clinical | HNSCC Cell Lines | 2 generation MUC1-directed CAR-T cells | MUC1 | Apoptosis cell lines |
| J Immunother Cancer. 2023; 11(6): e007162. [46] | Phase I—Clinical Trial | Patients with HNSCC | 4 generation T1E28z- and T4-engineered CAR-T cells | ErbB-ligand (TIE2) | DCR = 60% mOS = 285 days |
| Onco Targets Ther. 2018; 11: 7053–7059. [7] | Pre-Clinical | HNSCC Cell Lines | 2 generation EGFR-CAR-T-cells | EGFR | Apoptosis cell lines |
| Mol Ther. 2017; 25(11): 2440–2451. [47] | Pre-Clinical | HNSCC Cell Lines | 2 generation HER2-CAR-T-cells added to Oncolytic virus ”CAd12_PDL1” | HER2 | Apoptosis cell lines |
| Oral Oncol. 2018; 78: 145–150. [50] | Pre-Clinical | HNSCC Cell Lines | 2 generation CD70-CAR-T-cells | CD70 | Apoptosis cell lines |
| Cytotherapy. 2023; 25(10): 1037–1047. [53] | Pre-Clinical | NPC Cell Lines | 2 generation c-MET-CAR-T-cells | c-MET | Apoptosis cell lines |
| Front Immunol. 2023; 14: 1290488. [57] | Pre-Clinical | HNSCC Cell Lines | anti-CD44v6 CAR-NK cells | CD44v6 | Apoptosis cell lines |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perri, F.; Ottaviano, M.; Tomaciello, M.; De Felice, F. CAR-Based Cell Therapy in Head and Neck Cancer: A Comprehensive Review on Clinical Applicability. Cancers 2025, 17, 2215. https://doi.org/10.3390/cancers17132215
Perri F, Ottaviano M, Tomaciello M, De Felice F. CAR-Based Cell Therapy in Head and Neck Cancer: A Comprehensive Review on Clinical Applicability. Cancers. 2025; 17(13):2215. https://doi.org/10.3390/cancers17132215
Chicago/Turabian StylePerri, Francesco, Margaret Ottaviano, Miriam Tomaciello, and Francesca De Felice. 2025. "CAR-Based Cell Therapy in Head and Neck Cancer: A Comprehensive Review on Clinical Applicability" Cancers 17, no. 13: 2215. https://doi.org/10.3390/cancers17132215
APA StylePerri, F., Ottaviano, M., Tomaciello, M., & De Felice, F. (2025). CAR-Based Cell Therapy in Head and Neck Cancer: A Comprehensive Review on Clinical Applicability. Cancers, 17(13), 2215. https://doi.org/10.3390/cancers17132215