
Dosimetric Study of Biaxially Rotational Dynamic Radiation Therapy for Hippocampal-Sparing Whole Brain Irradiation

 ,
,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Contouring of the Target and Organs at Risk
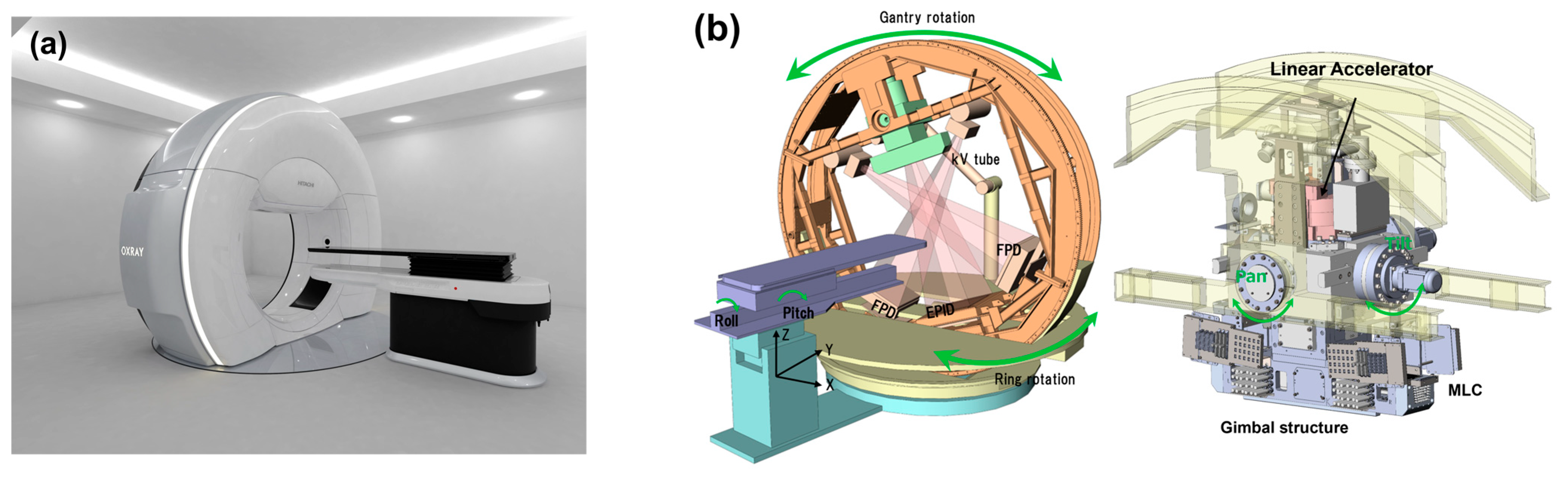
2.3. OXRAY System
2.4. Virtual Planning and Evaluation
2.5. Statistical Analysis
3. Results
3.1. PTV Dose–Volume Parameter Comparison Between BROAD-RT and Conv-VMAT Planning
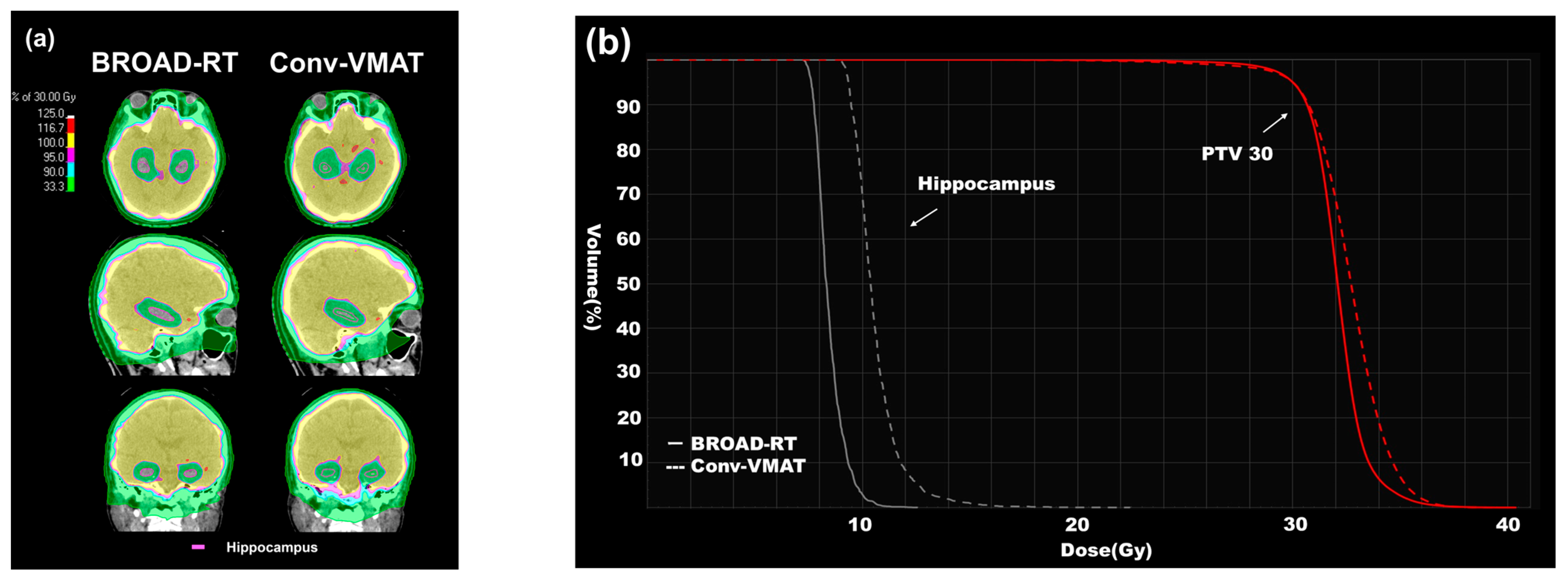
3.2. Hippocampus Dose–Volume Parameter Comparison Between BROAD-RT and Conv-VMAT Planning
3.3. Other Dose–Volume Parameter Comparisons Between BROAD-RT and Conv-VMAT Planning
3.4. Beam Delivery Time Comparison Between BROAD-RT and Conv-VMAT Planning
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HS-WBI | hippocampal-sparing whole-brain irradiation |
| WBI | whole brain irradiation |
| IMRT | intensity-modulated radiation therapy |
| IMPT | intensity-modulated proton therapy |
| VMAT | volumetric modulated arc therapy |
| BROAD-RT | biaxially rotational dynamic radiation therapy |
| CT | computed tomography |
| PTV | planning target volume |
| MU | monitor unit |
| Conv- | conventional |
| HI | homogeneity index |
| Vxx | volume receiving xx Gy |
| Dxx | dose receiving xx% of the volume |
| CBCT | cone beam CT |
References
- Posner, J.B. Management of brain metastases. Rev. Neurol. 1992, 148, 477–487. [Google Scholar] [PubMed]
- Graus, F.; Walker, R.W.; Allen, J.C. Brain metastases in children. J. Pediatr. 1983, 103, 558–561. [Google Scholar] [CrossRef]
- Wen, P.Y.; Loeffler, J.S. Management of brain metastases. Oncol 1999, 13, 941–954, 957–961; discussion 961–962, 969. [Google Scholar]
- Johnson, J.D.; Young, B. Demographics of brain metastasis. Neurosurg. Clin. N. Am. 1996, 7, 337–344. [Google Scholar] [CrossRef]
- Khuntia, D.; Brown, P.; Li, J.; Mehta, M.P. Whole-brain radiotherapy in the management of brain metastasis. J. Clin. Oncol. 2006, 24, 1295–1304. [Google Scholar] [CrossRef]
- Zimm, S.; Wampler, G.L.; Stablein, D.; Hazra, T.; Young, H.F. Intracerebral metastases in solid-tumor patients: Natural history and results of treatment. Cancer 1981, 48, 384–394. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1,960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 510–514. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J. Clin. Oncol. 2012, 30, 419–425. [Google Scholar] [CrossRef]
- Vogelbaum, M.A.; Brown, P.D.; Messersmith, H.; Brastianos, P.K.; Burri, S.; Cahill, D.; Dunn, I.F.; Gaspar, L.E.; Gatson, N.T.N.; Gondi, V.; et al. Treatment for brain metastases: ASCO-SNO-ASTRO guideline. J. Clin. Oncol. 2022, 40, 492–516. [Google Scholar] [CrossRef]
- Chao, J.H.; Phillips, R.; Nickson, J.J. Roentgen-ray therapy of cerebral metastases. Cancer 1954, 7, 682–689. [Google Scholar] [CrossRef]
- Kurtz, J.M.; Gelber, R.; Brady, L.W.; Carella, R.J.; Cooper, J.S. The palliation of brain metastases in a favorable patient population: A randomized clinical trial by the Radiation Therapy Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 1981, 7, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Borgelt, B.; Gelber, R.; Kramer, S.; Brady, L.W.; Chang, C.H.; Davis, L.W.; Perez, C.A.; Hendrickson, F.R. The palliation of brain metastases: Final results of the first two studies by the Radiation Therapy Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 1980, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Greene-Schloesser, D.; Moore, E.; Robbins, M.E. Molecular pathways: Radiation-induced cognitive impairment. Clin. Cancer Res. 2013, 19, 2294–2300. [Google Scholar] [CrossRef] [PubMed]
- Laack, N.N.; Brown, P.D. Cognitive sequelae of brain radiation in adults. Semin. Oncol. 2004, 31, 702–713. [Google Scholar] [CrossRef]
- Saad, S.; Wang, T.J.C. Neurocognitive deficits after radiation therapy for brain malignancies. Am. J. Clin. Oncol. 2015, 38, 634–640. [Google Scholar] [CrossRef]
- Gondi, V.; Pugh, S.L.; Tome, W.A.; Caine, C.; Corn, B.; Kanner, A.; Rowley, H.; Kundapur, V.; DeNittis, A.; Greenspoon, J.N.; et al. Preservation of memory with conformal avoidance of the hippocampal neural stem-cell compartment during whole-brain radiotherapy for brain metastases (RTOG 0933): A phase II multi-institutional trial. J. Clin. Oncol. 2014, 32, 3810–3816. [Google Scholar] [CrossRef]
- Yang, W.C.; Chen, Y.F.; Yang, C.C.; Wu, P.F.; Chan, H.M.; Chen, J.L.; Chen, G.Y.; Cheng, J.C.; Kuo, S.H.; Hsu, F.M. Hippocampal avoidance whole-brain radiotherapy without memantine in preserving neurocognitive function for brain metastases: A phase II blinded randomized trial. Neuro Oncol. 2020, 23, 478–486. [Google Scholar] [CrossRef]
- Graham, J.A.; Redler, G.; Delozier, K.B.; Yu, H.M.; Oliver, D.E.; Rosenberg, S.A. Dosimetric feasibility of hippocampal avoidance whole brain radiotherapy with an MRI-guided linear accelerator. J. Appl. Clin. Med. Phys. 2022, 23, e13587. [Google Scholar] [CrossRef]
- Brown, P.D.; Gondi, V.; Pugh, S.; Tome, W.A.; Wefel, J.S.; Armstrong, T.S.; Bovi, J.A.; Robinson, C.; Konski, A.; Khuntia, D.; et al. Hippocampal avoidance during whole-brain radiotherapy plus memantine for patients with brain metastases: Phase III trial NRG oncology CC001. J. Clin. Oncol. 2020, 38, 1019–1029. [Google Scholar] [CrossRef]
- Gondi, V.; Tolakanahalli, R.; Mehta, M.P.; Tewatia, D.; Rowley, H.; Kuo, J.S.; Khuntia, D.; Tomé, W.A. Hippocampal-sparing whole-brain radiotherapy: A “how-to” technique using helical tomotherapy and linear accelerator-based intensity-modulated radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1244–1252. [Google Scholar] [CrossRef]
- Zieminski, S.; Khandekar, M.; Wang, Y. Assessment of multi-criteria optimization (MCO) for volumetric modulated arc therapy (VMAT) in hippocampal avoidance whole brain radiation therapy (HA-WBRT). J. Appl. Clin. Med. Phys. 2018, 19, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.H.; Hua, W.; Gu, X.; Wang, X.L.; Li, J.; Liu, L.Q.; Huang, Y.X. Dosimetric study of different radiotherapy planning approaches for hippocampal avoidance whole-brain radiation therapy (HA-WBRT) based on fused CT and MRI imaging. Australas. Phys. Eng. Sci. Med. 2015, 38, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Rong, Y.; Evans, J.; Xu-Welliver, M.; Pickett, C.; Jia, G.; Chen, Q.; Zuo, L. Dosimetric evaluation of intensity-modulated radiotherapy, volumetric modulated arc therapy, and helical tomotherapy for hippocampal-avoidance whole brain radiotherapy. PLoS ONE 2015, 10, e0126222. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, K.; Kurosaki, H.; Oyoshi, H.; Miura, K.; Utsumi, N. Plan quality comparison between hippocampus-sparing whole-brain radiotherapy treated with halcyon and tomotherapy intensity-modulated radiotherapy. Technol. Cancer Res. Treat. 2022, 21, 15330338221108529. [Google Scholar] [CrossRef]
- Depuydt, T.; Verellen, D.; Haas, O.; Gevaert, T.; Linthout, N.; Duchateau, M.; Tournel, K.; Reynders, T.; Leysen, K.; Hoogeman, M.; et al. Geometric accuracy of a novel gimbals based radiation therapy tumor tracking system. Radiother. Oncol. 2011, 98, 365–372. [Google Scholar] [CrossRef]
- Mukumoto, N.; Nakamura, M.; Sawada, A.; Suzuki, Y.; Takahashi, K.; Miyabe, Y.; Kaneko, S.; Mizowaki, T.; Kokubo, M.; Hiraoka, M. Accuracy verification of infrared marker-based dynamic tumor-tracking irradiation using the gimbaled x-ray head of the Vero4DRT (MHI-TM2000). Med. Phys. 2013, 40, 041706. [Google Scholar] [CrossRef]
- Miura, H.; Ozawa, S.; Hayata, M.; Tsuda, S.; Yamada, K.; Nagata, Y. Effect of tumor amplitude and frequency on 4D modeling of Vero4DRT system. Rep. Pract. Oncol. Radiother. 2017, 22, 290–294. [Google Scholar] [CrossRef]
- Kamino, Y.; Takayama, K.; Kokubo, M.; Narita, Y.; Hirai, E.; Kawawda, N.; Mizowaki, T.; Nagata, Y.; Nishidai, T.; Hiraoka, M. Development of a four-dimensional image-guided radiotherapy system with a gimbaled x-ray head. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 271–278. [Google Scholar] [CrossRef]
- Kamino, Y.; Miura, S.; Kokubo, M.; Yamashita, I.; Hirai, E.; Hiraoka, M.; Ishikawa, J. Development of an ultrasmall C-band linear accelerator guide for a four-dimensional image-guided radiotherapy system with a gimbaled x-ray head. Med. Phys. 2007, 34, 1797–1808. [Google Scholar] [CrossRef]
- Sawada, A.; Kaneko, S.; Takayama, K.; Nagano, K.; Miyabe, Y.; Nakamura, M.; Narita, Y.; Kokubo, M.; Takahashi, K.; Mizowaki, T.; et al. SU-FF-T-285: Daily verification of isocenter alignment for a new image guided radiotherapy system, MHI-TM2000. Med. Phys. 2009, 36, 2586–2587. [Google Scholar] [CrossRef]
- Nakamura, M.; Sawada, A.; Ishihara, Y.; Takayama, K.; Mizowaki, T.; Kaneko, S.; Yamashita, M.; Tanabe, H.; Kokubo, M.; Hiraoka, M. Dosimetric characterization of a multileaf collimator for a new four-dimensional image-guided radiotherapy system with a gimbaled x-ray head, MHI-TM2000. Med. Phys. 2010, 37, 4684–4691. [Google Scholar] [CrossRef] [PubMed]
- Chera, B.S.; Amdur, R.J.; Patel, P.; Mendenhall, W.M. A radiation oncologist’s guide to contouring the hippocampus. Am. J. Clin. Oncol. 2009, 32, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Gondi, V.; Tome, W.A.; Marsh, J.; Struck, A.; Ghia, A.; Turian, J.V.; Bentzen, S.M.; Kuo, J.S.; Khuntia, D.; Mehta, M.P. Estimated risk of perihippocampal disease progression after hippocampal avoidance during whole-brain radiotherapy: Safety profile for RTOG 0933. Radiother. Oncol. 2010, 95, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez de Dios, N.; Couñago, F.; Murcia-Mejía, M.; Rico-Oses, M.; Calvo-Crespo, P.; Samper, P.; Vallejo, C.; Luna, J.; Trueba, I.; Sotoca, A.; et al. Randomized phase III trial of prophylactic cranial irradiation with or without hippocampal avoidance for small-cell lung cancer (Premer): A GICOR-GOECP-SEOR study. J. Clin. Oncol. 2021, 39, 3118–3127. [Google Scholar] [CrossRef]
- Takaoka, T.; Tomita, N.; Mizuno, T.; Hashimoto, S.; Tsuchiya, T.; Tomida, M.; Yanagi, T. Dosimetric comparison of helical tomotherapy and intensity-modulated proton therapy in hippocampus- and scalp-sparing whole brain radiotherapy. Technol. Cancer Res. Treat. 2021, 20, 15330338211060170. [Google Scholar] [CrossRef]
- Eisbruch, A.; Ten Haken, R.K.; Kim, H.M.; Marsh, L.H.; Ship, J.A. Dose, volume, and function relationships in parotid salivary glands following conformal and intensity-modulated irradiation of head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 577–587. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mean Volume (Range) | |
|---|---|
| PTV (cm3) | 1364.69 (1170.65–1439.43) |
| Hippocampus volume (cm3) | 6.53 (4.72–8.10) |
| Eye volume (cm3) | 16.81 (12.76–21.16) |
| Lens volume (cm3) | 0.36 (0.28–0.43) |
| BROAD-RT | Conv-VMAT | p-Values | ||
|---|---|---|---|---|
| PTV | ||||
| D98 (%) | 27.95 (0.54) | 28.21 (0.48) | 0.27 | |
| D50 (%) | 31.65 (0.26) | 31.58 (0.44) | 0.62 | |
| D2 (%) | 33.55 (0.49) | 33.26 (0.66) | 0.09 | |
| V30 (%) | 95.00 (0.00) | 95.00 (0.00) | - | |
| V35 (%) | 0.22 (0.26) | 0.17 (0.30) | 0.29 | |
| HI | 0.18 (0.02) | 0.16 (2.23) | 0.14 | |
| Hippocampus | ||||
| Dmax (Gy) | 11.10 (0.61) | 16.10 (0.57) | <0.01 | |
| Dmean (Gy) | 7.95 (0.20) | 9.89 (0.75) | <0.01 | |
| Dmin (Gy) | 7.01 (0.19) | 8.24 (0.34) | <0.01 | |
| V10 (%) | 0.42 (0.34) | 39.05 (25.89) | <0.01 | |
| Eye | ||||
| Dmax (Gy) | 16.17 (1.68) | 15.23 (1.58) | 0.20 | |
| Lens | ||||
| Dmax (Gy) | 3.76 (0.16) | 4.26 (0.32) | 0.13 | |
| Parotid glands | ||||
| Dmean (Gy) | 4.83 (0.35) | 4.35 (0.83) | 0.03 | |
| Chiasm | ||||
| Dmax (Gy) | 34.28 (1.04) | 34.66 (1.30) | 0.50 | |
| Dose count | ||||
| DMU (cGy/MU) | 1743.70 (151.44) | 1222.71 (280.20) | <0.01 | |
| Beam delivery time | ||||
| Time (s) | 313.60 (34.91) | 202.50 (14.46) | <0.01 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirotaki, K.; Makita, K.; Nakamura, M.; Wakabayashi, M.; Kitou, S.; Ninomiya, T.; Ito, M. Dosimetric Study of Biaxially Rotational Dynamic Radiation Therapy for Hippocampal-Sparing Whole Brain Irradiation. Cancers 2025, 17, 1949. https://doi.org/10.3390/cancers17121949
Hirotaki K, Makita K, Nakamura M, Wakabayashi M, Kitou S, Ninomiya T, Ito M. Dosimetric Study of Biaxially Rotational Dynamic Radiation Therapy for Hippocampal-Sparing Whole Brain Irradiation. Cancers. 2025; 17(12):1949. https://doi.org/10.3390/cancers17121949
Chicago/Turabian StyleHirotaki, Kouta, Kenji Makita, Masaki Nakamura, Masashi Wakabayashi, Satoe Kitou, Takashi Ninomiya, and Masashi Ito. 2025. "Dosimetric Study of Biaxially Rotational Dynamic Radiation Therapy for Hippocampal-Sparing Whole Brain Irradiation" Cancers 17, no. 12: 1949. https://doi.org/10.3390/cancers17121949
APA StyleHirotaki, K., Makita, K., Nakamura, M., Wakabayashi, M., Kitou, S., Ninomiya, T., & Ito, M. (2025). Dosimetric Study of Biaxially Rotational Dynamic Radiation Therapy for Hippocampal-Sparing Whole Brain Irradiation. Cancers, 17(12), 1949. https://doi.org/10.3390/cancers17121949