
Pressurized Intra-Peritoneal Aerosol Chemotherapy (PIPAC) for Peritoneal Malignancies with Palliative and Bidirectional Intent

 ,
,  , , , ,
, , , ,  ,
,  and
and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Measures
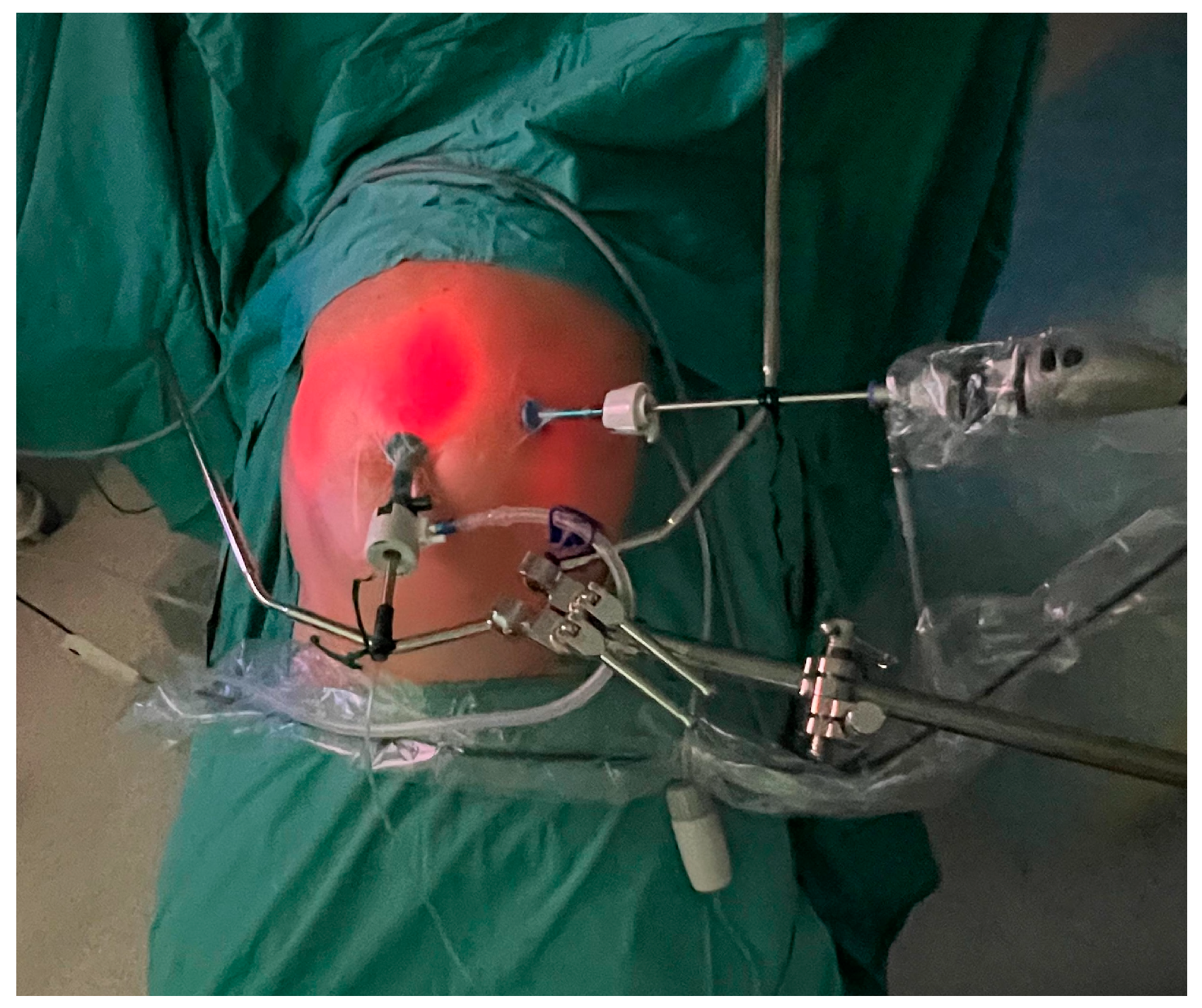
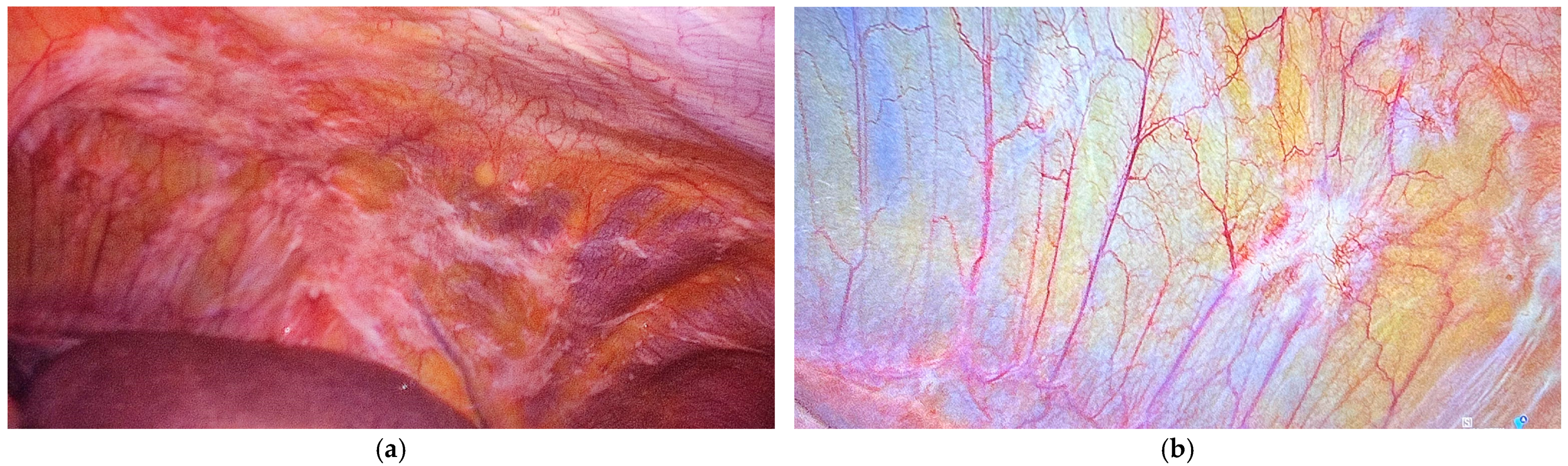
2.2. PIPAC Procedure
2.3. Endpoints
2.4. Statistics
3. Results
3.1. Clinical
3.2. Surgical
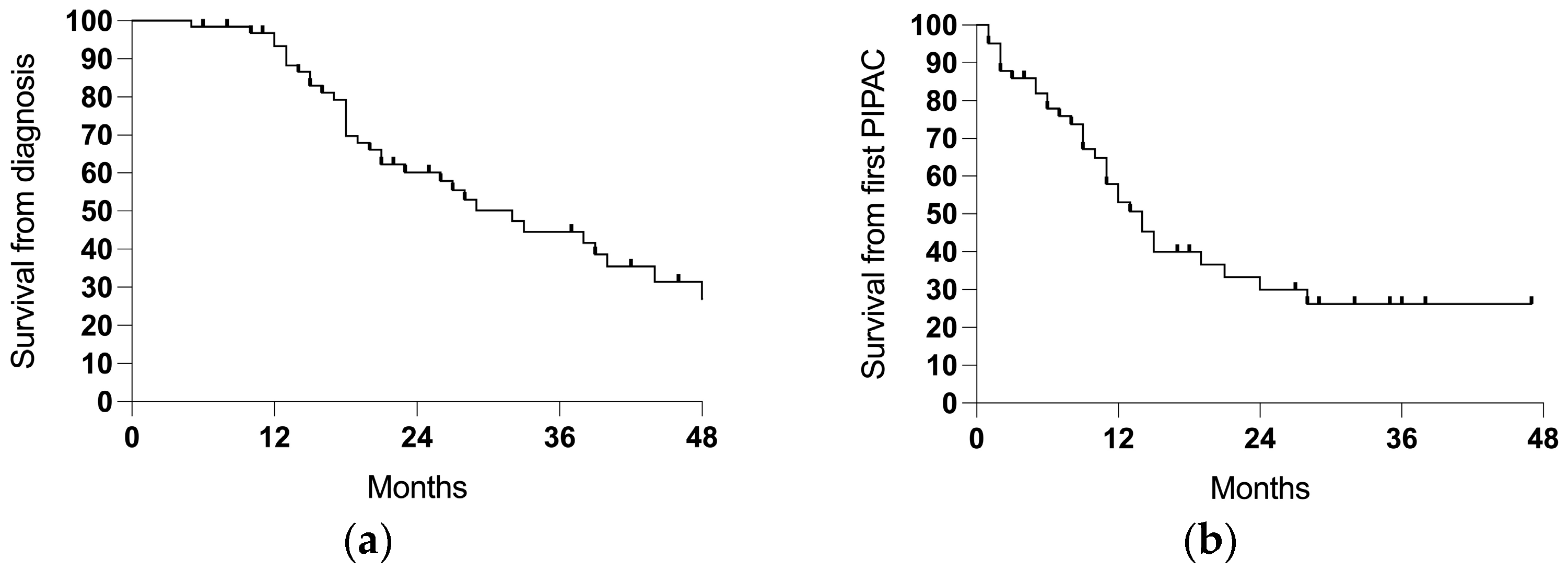
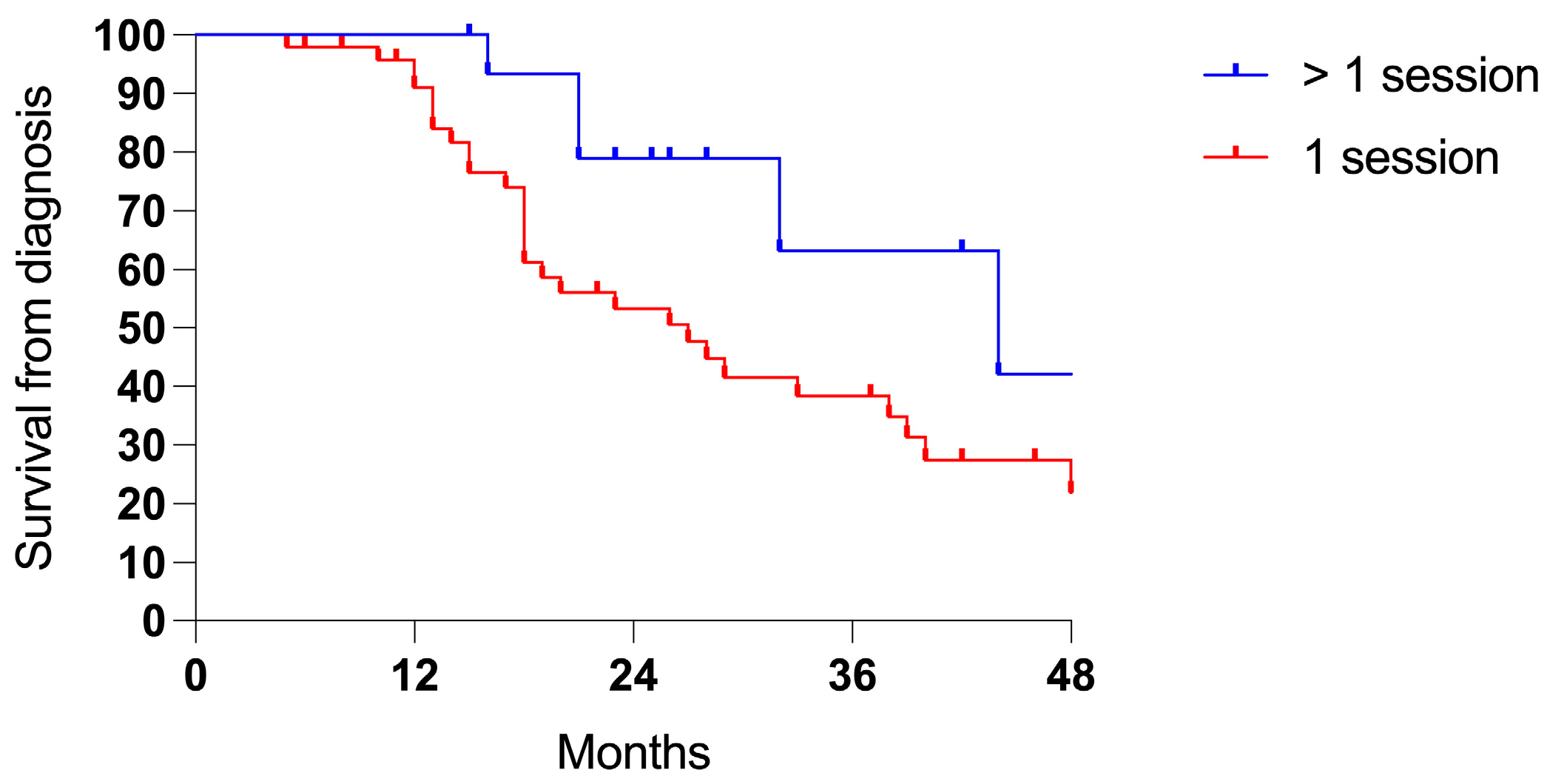
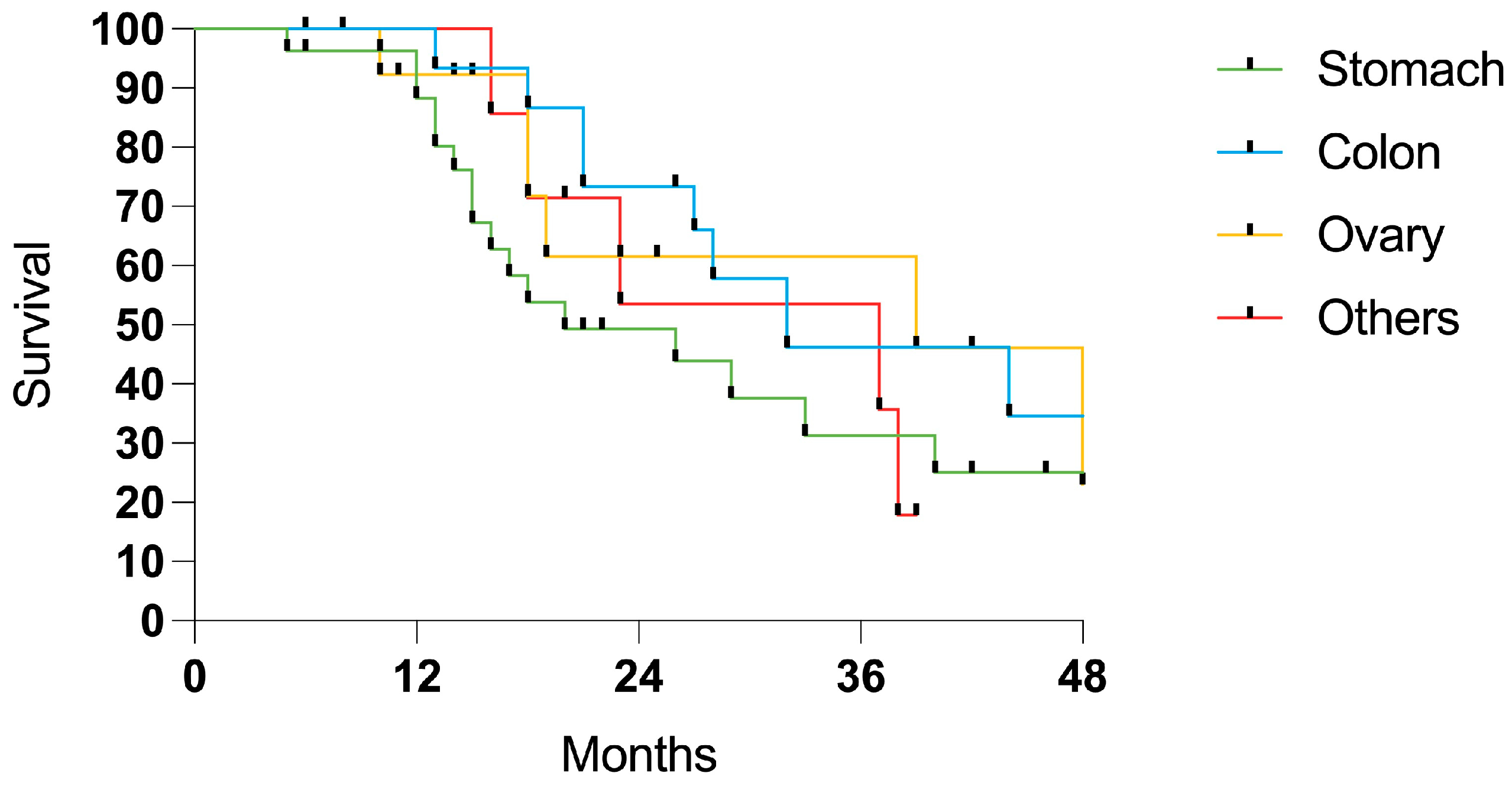
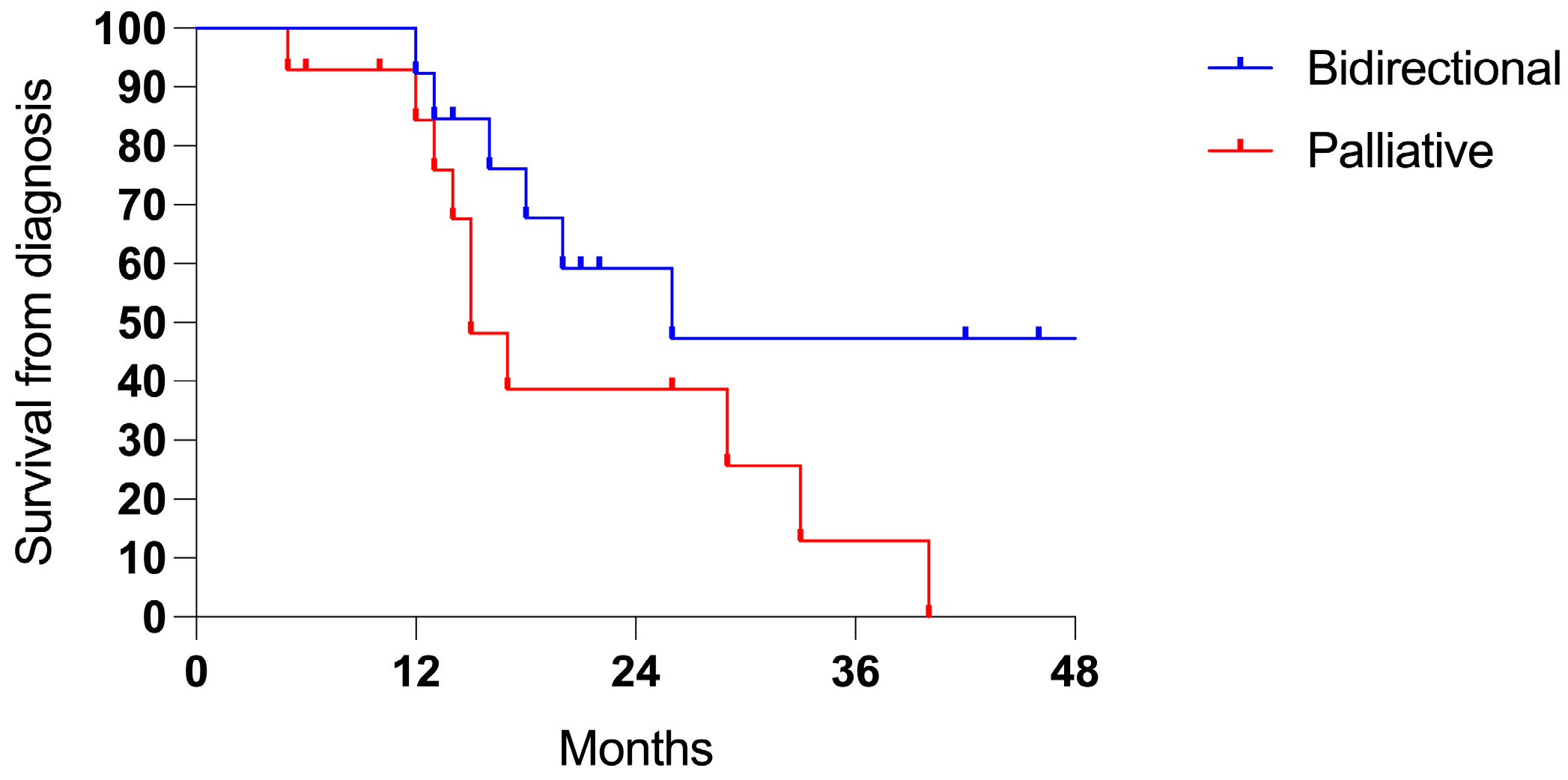
3.3. Survival
3.4. PSM from Gastric Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PSM | Peritoneal Surface Malignancies |
| PIPAC | Pressurized Intraperitoneal Aerosol Chemotherapy |
| CRS | Cytoreductive Surgery |
| HIPEC | Hyperthermic Intraperitoneal Chemotherapy |
| ECOG | Eastern Cooperative Oncology Group |
| PSS | Prior Surgical Score |
| PCI | Peritoneal Cancer Index |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| CTCAE | Common Terminology Criteria for Adverse Events |
| OS | Overall Survival |
| SD | Standard Deviation |
| IQR | Interquartile Range |
References
- Lemmens, V.E.; Klaver, Y.L.; Verwaal, V.J.; Rutten, H.J.; Coebergh, J.W.W.; de Hingh, I.H. Predictors and Survival of Synchronous Peritoneal Carcinomatosis of Colorectal Origin: A Population-based Study. Int. J. Cancer 2011, 128, 2717–2725. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Incognito, G.G.; Incognito, D.; Nibid, L.; Caruso, G.; Berretta, M.; Taffon, C.; Palumbo, M.; Perrone, G.; Roviello, F.; et al. Clinical Implications of Epithelial-to-Mesenchymal Transition in Cancers Which Potentially Spread to Peritoneum. Clin. Transl. Oncol. 2025. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Manzanedo, I.; Pereira, F.; Cascales-Campos, P.; Muñoz-Casares, C.; Asensio, E.; Torres-Melero, J.; Prada-Villaverde, A.; Caravaca-García, I.; Gutiérrez-Calvo, A.; Vaqué, J.; et al. Treatment of Peritoneal Surface Malignancies by Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Spain: Results of the National Registry of the Spanish Group of Peritoneal Oncologic Surgery (REGECOP). J. Clin. Med. 2023, 12, 3774. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.; de Hingh, I.; Van Der Speeten, K.; Hubner, M.; Deraco, M.; Bakrin, N.; Villeneuve, L.; Kusamura, S.; Glehen, O. HIPEC Methodology and Regimens: The Need for an Expert Consensus. Ann. Surg. Oncol. 2021, 28, 9098–9113. [Google Scholar] [CrossRef]
- Solass, W.; Kerb, R.; Mürdter, T.; Giger-Pabst, U.; Strumberg, D.; Tempfer, C.; Zieren, J.; Schwab, M.; Reymond, M.A. Intraperitoneal Chemotherapy of Peritoneal Carcinomatosis Using Pressurized Aerosol as an Alternative to Liquid Solution: First Evidence for Efficacy. Ann. Surg. Oncol. 2014, 21, 553–559. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. A Narrative Review of What Can HIPEC Do. Eur. J. Surg. Oncol. 2023, 49, 106976. [Google Scholar] [CrossRef]
- Alyami, M.; Hübner, M.; Grass, F.; Bakrin, N.; Villeneuve, L.; Laplace, N.; Passot, G.; Glehen, O.; Kepenekian, V. Pressurised Intraperitoneal Aerosol Chemotherapy: Rationale, Evidence, and Potential Indications. Lancet Oncol. 2019, 20, e368–e377. [Google Scholar] [CrossRef]
- Lurvink, R.J.; Rovers, K.P.; Nienhuijs, S.W.; Creemers, G.-J.; Burger, J.W.A.; de Hingh, I.H.J. Pressurized Intraperitoneal Aerosol Chemotherapy with Oxaliplatin (PIPAC-OX) in Patients with Colorectal Peritoneal Metastases—A Systematic Review. J. Gastrointest. Oncol. 2021, 12, S242–S258. [Google Scholar] [CrossRef]
- Marrelli, D.; Ansaloni, L.; Federici, O.; Asero, S.; Carbone, L.; Marano, L.; Baiocchi, G.; Vaira, M.; Coccolini, F.; Di Giorgio, A.; et al. Cytoreductive Surgery (CRS) and HIPEC for Advanced Ovarian Cancer with Peritoneal Metastases: Italian PSM Oncoteam Evidence and Study Purposes. Cancers 2022, 14, 6010. [Google Scholar] [CrossRef]
- Alyami, M.; Bonnot, P.-E.; Mercier, F.; Laplace, N.; Villeneuve, L.; Passot, G.; Bakrin, N.; Kepenekian, V.; Glehen, O. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) for Unresectable Peritoneal Metastasis from Gastric Cancer. Eur. J. Surg. Oncol. 2021, 47, 123–127. [Google Scholar] [CrossRef]
- Giger-Pabst, U.; Demtröder, C.; Falkenstein, T.A.; Ouaissi, M.; Götze, T.O.; Rezniczek, G.A.; Tempfer, C.B. Pressurized IntraPeritoneal Aerosol Chemotherapy (PIPAC) for the Treatment of Malignant Mesothelioma. BMC Cancer 2018, 18, 442. [Google Scholar] [CrossRef] [PubMed]
- Horvath, P.; Beckert, S.; Struller, F.; Königsrainer, A.; Reymond, M.A. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) for Peritoneal Metastases of Pancreas and Biliary Tract Cancer. Clin. Exp. Metastasis 2018, 35, 635–640. [Google Scholar] [CrossRef] [PubMed]
- So, J.B.Y. Bi-Directional Chemotherapy for Peritoneal Metastases. Br. J. Surg. 2023, 110, 627–628. [Google Scholar] [CrossRef] [PubMed]
- Ploug, M.; Graversen, M.; Pfeiffer, P.; Mortensen, M.B. Bidirectional Treatment of Peritoneal Metastasis with Pressurized IntraPeritoneal Aerosol Chemotherapy (PIPAC) and Systemic Chemotherapy: A Systematic Review. BMC Cancer 2020, 20, 105. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Peritonectomy Procedures. Ann. Surg. 1995, 221, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, P.; Sugarbaker, P.H. Clinical Research Methodologies in Diagnosis and Staging of Patients with Peritoneal Carcinomatosis. In Peritoneal Carcinomatosis: Principles of Management; Springer: Boston, MA, USA, 1996; pp. 359–374. [Google Scholar]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Update and Clarification: From the RECIST Committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef]
- Solaß, W.; Giger-Pabst, U.; Zieren, J.; Reymond, M.A. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC): Occupational Health and Safety Aspects. Ann. Surg. Oncol. 2013, 20, 3504–3511. [Google Scholar] [CrossRef] [PubMed]
- Casella, F.; Bencivenga, M.; Brancato, G.; Torroni, L.; Ridolfi, C.; Puccio, C.; Alloggio, M.; Meloni, F.; Fusario, D.; Marrelli, D.; et al. Bidirectional Approach with PIPAC and Systemic Chemotherapy for Patients with Synchronous Gastric Cancer Peritoneal Metastases (GCPM). Ann. Surg. Oncol. 2023, 30, 5733–5742. [Google Scholar] [CrossRef]
- Girardot-Miglierina, A.; Clerc, D.; Alyami, M.; Villeneuve, L.; Sgarbura, O.; Reymond, M.-A.; Hübner, M. Consensus Statement on Safety Measures for Pressurized Intraperitoneal Aerosol Chemotherapy. Pleura Peritoneum 2021, 6, 139–149. [Google Scholar] [CrossRef]
- Sgarbura, O.; Eveno, C.; Alyami, M.; Bakrin, N.; Guiral, D.C.; Ceelen, W.; Delgadillo, X.; Dellinger, T.; Di Giorgio, A.; Kefleyesus, A.; et al. Consensus Statement for Treatment Protocols in Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC). Pleura Peritoneum 2022, 7, 1–7. [Google Scholar] [CrossRef]
- Dueck, A.C.; Mendoza, T.R.; Mitchell, S.A.; Reeve, B.B.; Castro, K.M.; Rogak, L.J.; Atkinson, T.M.; Bennett, A.V.; Denicoff, A.M.; O’Mara, A.M.; et al. Validity and Reliability of the US National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). JAMA Oncol. 2015, 1, 1051. [Google Scholar] [CrossRef] [PubMed]
- Solass, W.; Sempoux, C.; Detlefsen, S.; Carr, N.J.; Bibeau, F. Peritoneal Sampling and Histological Assessment of Therapeutic Response in Peritoneal Metastasis: Proposal of the Peritoneal Regression Grading Score (PRGS). Pleura Peritoneum 2016, 1, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Marrelli, D.; Petrioli, R.; Cassetti, D.; D’Ignazio, A.; Marsili, S.; Mazzei, M.A.; Lazzi, S.; Roviello, F. A Novel Treatment Protocol with 6 Cycles of Neoadjuvant Chemotherapy Followed by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Stage III Primary Ovarian Cancer. Surg. Oncol. 2021, 37, 101523. [Google Scholar] [CrossRef] [PubMed]
- Lambert, L.A.; Wiseman, J. Palliative Management of Peritoneal Metastases. Ann. Surg. Oncol. 2018, 25, 2165–2171. [Google Scholar] [CrossRef]
- Lurvink, R.J.; Van der Speeten, K.; Rovers, K.P.; de Hingh, I.H.J.T. The Emergence of Pressurized Intraperitoneal Aerosol Chemotherapy as a Palliative Treatment Option for Patients with Diffuse Peritoneal Metastases: A Narrative Review. J. Gastrointest. Oncol. 2021, 12, S259–S270. [Google Scholar] [CrossRef]
- Sgarbura, O.; Villeneuve, L.; Alyami, M.; Bakrin, N.; Torrent, J.J.; Eveno, C.; Hübner, M.; Abba, J.; Afifi, A.; Mortensen, M.B.; et al. Current Practice of Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC): Still Standardized or on the Verge of Diversification? Eur. J. Surg. Oncol. 2021, 47, 149–156. [Google Scholar] [CrossRef]
- Grass, F.; Vuagniaux, A.; Teixeira-Farinha, H.; Lehmann, K.; Demartines, N.; Hübner, M. Systematic Review of Pressurized Intraperitoneal Aerosol Chemotherapy for the Treatment of Advanced Peritoneal Carcinomatosis. Br. J. Surg. 2017, 104, 669–678. [Google Scholar] [CrossRef]
- Alyami, M.; Mercier, F.; Siebert, M.; Bonnot, P.-E.; Laplace, N.; Villeneuve, L.; Passot, G.; Glehen, O.; Bakrin, N.; Kepenekian, V. Unresectable Peritoneal Metastasis Treated by Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) Leading to Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Eur. J. Surg. Oncol. 2021, 47, 128–133. [Google Scholar] [CrossRef]
- Baggaley, A.E.; Lafaurie, G.B.R.C.; Tate, S.J.; Boshier, P.R.; Case, A.; Prosser, S.; Torkington, J.; Jones, S.E.F.; Gwynne, S.H.; Peters, C.J. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC): Updated Systematic Review Using the IDEAL Framework. Br. J. Surg. 2022, 110, 10–18. [Google Scholar] [CrossRef]
- Tempfer, C.; Giger-Pabst, U.; Hilal, Z.; Dogan, A.; Rezniczek, G.A. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) for Peritoneal Carcinomatosis: Systematic Review of Clinical and Experimental Evidence with Special Emphasis on Ovarian Cancer. Arch. Gynecol. Obstet. 2018, 298, 243–257. [Google Scholar] [CrossRef]
- Nadiradze, G.; Giger-Pabst, U.; Zieren, J.; Strumberg, D.; Solass, W.; Reymond, M.-A. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) with Low-Dose Cisplatin and Doxorubicin in Gastric Peritoneal Metastasis. J. Gastrointest. Surg. 2016, 20, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Demtröder, C.; Solass, W.; Zieren, J.; Strumberg, D.; Giger-Pabst, U.; Reymond, M.-A. Pressurized Intraperitoneal Aerosol Chemotherapy with Oxaliplatin in Colorectal Peritoneal Metastasis. Color. Dis. 2016, 18, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, A.; Macrì, A.; Ferracci, F.; Robella, M.; Visaloco, M.; De Manzoni, G.; Sammartino, P.; Sommariva, A.; Biacchi, D.; Roviello, F.; et al. 10 Years of Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC): A Systematic Review and Meta-Analysis. Cancers 2023, 15, 1125. [Google Scholar] [CrossRef]
- Mortensen, M.B.; Glehen, O.; Horvath, P.; Hübner, M.; Hyung-Ho, K.; Königsrainer, A.; Pocard, M.; Reymond, M.A.; So, J.; Fristrup, C.W. The ISSPP PIPAC Database: Design, Process, Access, and First Interim Analysis. Pleura Peritoneum 2021, 6, 91–97. [Google Scholar] [CrossRef]
- Kitai, T.; Yamanaka, K. Conversion Surgery for Gastric Cancer with PM. J. Surg. Oncol. 2024, 130, 1306–1315. [Google Scholar] [CrossRef]
- Khomyakov, V.; Ryabov, A.; Ivanov, A.; Bolotina, L.; Utkina, A.; Volchenko, N.; Kaprin, A. Bidirectional Chemotherapy in Gastric Cancer with Peritoneal Metastasis Combining Intravenous XELOX with Intraperitoneal Chemotherapy with Low-Dose Cisplatin and Doxorubicin Administered as a Pressurized Aerosol: An Open-Label, Phase-2 Study (PIPAC-GA2). Pleura Peritoneum 2016, 1, 159–166. [Google Scholar] [CrossRef]
- Struller, F.; Horvath, P.; Solass, W.; Weinreich, F.-J.; Strumberg, D.; Kokkalis, M.K.; Fischer, I.; Meisner, C.; Königsrainer, A.; Reymond, M.A. Pressurized Intraperitoneal Aerosol Chemotherapy with Low-Dose Cisplatin and Doxorubicin (PIPAC C/D) in Patients with Gastric Cancer and Peritoneal Metastasis: A Phase II Study. Ther. Adv. Med. Oncol. 2019, 11, 1758835919846402. [Google Scholar] [CrossRef]
- Ramalho-Vasconcelos, F.; Gomes, R.; Bouça-Machado, R.; Aral, M.; Nogueiro, J.; Bouça-Machado, T.; Sousa-Pinto, B.; San-tos-Sousa, H. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) in the Treatment of Gastric Cancer: Feasibility, Efficacy and Safety—A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 3320. [Google Scholar] [CrossRef]
- Tidadini, F.; Abba, J.; Quesada, J.-L.; Baudrant, M.; Bonne, A.; Foote, A.; Faucheron, J.-L.; Glehen, O.; Villeneuve, L.; Arvieux, C. Effect of Pressurized Intraperitoneal Aerosol Chemotherapy on the Survival Rate of Patients with Peritoneal Carcinomatosis of Gastric Origin. J. Gastrointest. Cancer 2022, 53, 971–979. [Google Scholar] [CrossRef]
- Graversen, M.; Rouvelas, I.; Ainsworth, A.P.; Bjarnesen, A.P.; Detlefsen, S.; Ellebaek, S.B.; Fristrup, C.W.; Liljefors, M.G.; Lundell, L.; Nilsson, M.; et al. Feasibility and Safety of Laparoscopic D2 Gastrectomy in Combination with Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) in Patients with Gastric Cancer at High Risk of Recurrence-The PIPAC-OPC4 Study. Ann. Surg. Oncol. 2023, 30, 4433–4441. [Google Scholar] [CrossRef]
- Nowacki, M.; Alyami, M.; Villeneuve, L.; Mercier, F.; Hubner, M.; Willaert, W.; Ceelen, W.; Reymond, M.; Pezet, D.; Arvieux, C.; et al. Multicenter Comprehensive Methodological and Technical Analysis of 832 Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) Interventions Performed in 349 Patients for Peritoneal Carcinomatosis Treatment: An International Survey Study. Eur. J. Surg. Oncol. 2018, 44, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H.; Van der Speeten, K. PIPAC May Work but More Data Is Needed. J. Gastrointest. Oncol. 2021, 12, S271–S272. [Google Scholar] [CrossRef] [PubMed]
- Casella, F.; Bencivenga, M.; Rosati, R.; Fumagalli, U.R.; Marrelli, D.; Pacelli, F.; Macrì, A.; Donini, A.; Torroni, L.; Pavarana, M.; et al. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) in Multimodal Therapy for Patients with Oligometastatic Peritoneal Gastric Cancer: A Randomized Multicenter Phase III Trial PIPAC VEROne. Pleura Peritoneum 2022, 7, 135–141. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (%) | Entire Series (64) | Bidirectional (24) | Palliative (40) | p |
|---|---|---|---|---|
| Location | - | |||
| Gastric | 27 (42.2) | 13 (48.1) | 14 (51.9) | |
| Colorectal | 15 (23.4) | 3 (20.0) | 12 (80.0) | |
| Ovarian | 14 (21.9) | 6 (42.9) | 8 (57.1) | |
| Pancreatic | 4 (6.2) | 0 | 4 | |
| Breast | 1 (1.6) | 0 | 1 | |
| Mesothelioma | 3 (4.7) | 2 (66.7) | 1 (33.3) | |
| PCI at surgery, IQR | 14 (9–25) | 9.5 (5–14) | 23 (14–35) | <0.001 |
| Ascites | 39 (60.9) | 10 (25.6) | 29 (74.4) | 0.030 |
| Cytology+ | 31 (48.4) | 11 (35.5) | 20 (64.5) | 0.889 |
| PIPAC Sessions | 0.233 | |||
| 1 | 48 (75) | 16 (33.3) | 32 (66.7) | |
| 2 or more | 16 (25) | 8 (50) | 8 (50) | |
| Complications | 9 (14.1) | 3 (33.3) | 6 (66.7) | 0.839 |
| CTCAE grade I | 5 (7.8) | 2 (40) | 3 (60) | |
| CTCAE grade II | 1 (1.6) | 0 (0) | 1 (100) | |
| CTCAE grade III | 3 (4.7) | 1 (33.3) | 2 (66.7) | |
| 30-day mortality | 2 (3.1) | 0 (0) | 2 (100) | 0.734 |
| All Series Median (3-y) | Bidirectional Median (3-y) | Palliative Median (3-y) | p | |
|---|---|---|---|---|
| Entire series | 32 (44.6%) | 24 (66.0%) | 19 (33.9%) | 0.011 |
| Stomach | 20 (31.3%) | 26 (47.4%) | 17 (21.6%) | 0.188 |
| Colon | 32 (46.2%) | 27 (0) | 30 (40.0%) | 0.560 |
| Ovary | 39 (61.5%) | 24 (80.0%) | 18 (42.9%) | 0.076 |
| Others | 37 (53.6%) | 38 (100%) | 26.5 (53.3%) | 0.480 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marrelli, D.; Carbone, L.; Fusario, D.; Petrioli, R.; Poto, G.E.; Grassi, G.; Piagnerelli, R.; Piccioni, S.A.; Ricci, C.; Bianco, M.T.; et al. Pressurized Intra-Peritoneal Aerosol Chemotherapy (PIPAC) for Peritoneal Malignancies with Palliative and Bidirectional Intent. Cancers 2025, 17, 1938. https://doi.org/10.3390/cancers17121938
Marrelli D, Carbone L, Fusario D, Petrioli R, Poto GE, Grassi G, Piagnerelli R, Piccioni SA, Ricci C, Bianco MT, et al. Pressurized Intra-Peritoneal Aerosol Chemotherapy (PIPAC) for Peritoneal Malignancies with Palliative and Bidirectional Intent. Cancers. 2025; 17(12):1938. https://doi.org/10.3390/cancers17121938
Chicago/Turabian StyleMarrelli, Daniele, Ludovico Carbone, Daniele Fusario, Roberto Petrioli, Gianmario Edoardo Poto, Giulia Grassi, Riccardo Piagnerelli, Stefania Angela Piccioni, Carmelo Ricci, Maria Teresa Bianco, and et al. 2025. "Pressurized Intra-Peritoneal Aerosol Chemotherapy (PIPAC) for Peritoneal Malignancies with Palliative and Bidirectional Intent" Cancers 17, no. 12: 1938. https://doi.org/10.3390/cancers17121938
APA StyleMarrelli, D., Carbone, L., Fusario, D., Petrioli, R., Poto, G. E., Grassi, G., Piagnerelli, R., Piccioni, S. A., Ricci, C., Bianco, M. T., Mazzei, M. A., Lazzi, S., & Roviello, F. (2025). Pressurized Intra-Peritoneal Aerosol Chemotherapy (PIPAC) for Peritoneal Malignancies with Palliative and Bidirectional Intent. Cancers, 17(12), 1938. https://doi.org/10.3390/cancers17121938