

Somatostatin Receptor Expression of Gastroenteropancreatic Neuroendocrine Tumors: A Comprehensive Analysis in the Era of Somatostatin Receptor PET Imaging

 , ,
, , 
Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cakir, M.; Dworakowska, D.; Grossman, A. Somatostatin receptor biology in neuroendocrine and pituitary tumours: Part 1—Molecular pathways. J. Cell Mol. Med. 2010, 14, 2570–2584. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zamora, V.; Cabanne, A.; Salanova, R.; Bestani, C.; Domenichini, E.; Marmissolle, F.; Giacomi, N.; O’Connor, J.; Méndez, G.; Roca, E.; et al. Immunohistochemical expression of somatostatin receptors in digestive endocrine tumours. Dig. Liver Dis. 2010, 42, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Wittenberg, M.; Schade-Brittinger, C.; Aminossadati, B.; Ronicke, E.; Gress, T.M.; Müller, H.H.; Arnold, R.; PROMID Study Group. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors (PROMID): Results of Long-Term Survival. Neuroendocrinology 2017, 104, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.R.; Caplin, M.E.; Kunz, P.L.; Ruszniewski, P.B.; Bodei, L.; Hendifar, A.; Mittra, E.; Wolin, E.M.; Yao, J.C.; Pavel, M.E.; et al. 177Lu-Dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (NETTER-1): Final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 1752–1763, Erratum in Lancet Oncol. 2022, 23, e59. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.R.; Naqvi, S.; Cohn, A.L.; Delpassand, E.S.; Wagner, V.J.; Torgue, J.; Woloski, R.; Manuel, A.; Maluccio, M.A. Safety, tolerability and efficacy of 212Pb-DOTAMTATE as a targeted alpha therapy for subjects with unresectable or metastatic somatostatin receptor-expressing gastroenteropancreatic neuroendocrine tumors (SSTR+ GEP-NETs): A phase 2 study. J. Clin. Oncol. 2024, 42, 4020. [Google Scholar] [CrossRef]
- Morris, M.; Ulaner, G.A.; Halperin, D.M.; Strosberg, J.; Mehr, S.H.; Li, D.; Soares, H.P.; Anthony, L.B.; Kotiah, S.D.; Jarcene, H.; et al. ACTION-1 phase Ib/3 trial of RYZ101 in somatostatin receptor subtype 2–expressing (SSTR2+) gastroenteropancreatic neuroendocrine tumors (GEP-NET) progressing after 177Lu somatostatin analogue (SSA) therapy: Initial safety analysis. J. Clin. Oncol. 2023, 41, 4132. [Google Scholar] [CrossRef]
- Hope, T.A.; Bergsland, E.K.; Bozkurt, M.F.; Graham, M.; Heaney, A.P.; Herrmann, K.; Howe, J.R.; Kulke, M.H.; Kunz, P.L.; Mailman, J.; et al. Appropriate Use Criteria for Somatostatin Receptor PET Imaging in Neuroendocrine Tumors. J. Nucl. Med. 2018, 59, 66–74. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J.B.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R.J.; Kjaer, A.; et al. Antibes Consensus Conference participants. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine & Hybrid Imaging. Neuroendocrinology 2017, 105, 212–244. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, V.; Kunikowska, J.; Baudin, E.; Bodei, L.; Bouvier, C.; Capdevila, J.; Cremonesi, M.; de Herder, W.W.; Dromain, C.; Falconi, M.; et al. Consensus on molecular imaging and theranostics in neuroendocrine neoplasms. Eur. J. Cancer 2021, 146, 56–73. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kimura, N.; Pilichowska, M.; Date, F.; Kimura, I.; Schindler, M. Immunohistochemical expression of somatostatin type 2A receptor in neuroendocrine tumors. Clin. Cancer Res. 1999, 5, 3483–3487. [Google Scholar] [PubMed]
- Volante, M.; Brizzi, M.P.; Faggiano, A.; La Rosa, S.; Rapa, I.; Ferrero, A.; Mansueto, G.; Righi, L.; Garancini, S.; Capella, C.; et al. Somatostatin receptor type 2A immunohistochemistry in neuroendocrine tumors: A proposal of scoring system correlated with somatostatin receptor scintigraphy. Mod. Pathol. 2007, 20, 1172–1182. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Gonzalez, R.S.; Zhao, Z.; Koyama, T.; Cornish, T.C.; Hande, K.R.; Walker, R.; Sandler, M.; Berlin, J.; Liu, E.H. Liver metastases of small intestine neuroendocrine tumors: Ki-67 heterogeneity and World Health Organization grade discordance with primary tumors. Am. J. Clin. Pathol. 2015, 143, 398–404. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grillo, F.; Valle, L.; Ferone, D.; Albertelli, M.; Brisigotti, M.P.; Cittadini, G.; Vanoli, A.; Fiocca, R.; Mastracci, L. KI-67 heterogeneity in well differentiated gastro-entero-pancreatic neuroendocrine tumors: When is biopsy reliable for grade assessment? Endocrine 2017, 57, 494–502, Erratum in Endocrine 2017, 57, 503. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Tang, L.H.; Klimstra, D.S. Effect of tumor heterogeneity on the assessment of Ki67 labeling index in well-differentiated neuroendocrine tumors metastatic to the liver: Implications for prognostic stratification. Am. J. Surg. Pathol. 2011, 35, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Cao, F.; Zhao, X.; Xie, Q.; Lu, M.; Li, J.; Yang, Z.; Sun, Y. Correlation and Comparison of Somatostatin Receptor Type 2 Immunohistochemical Scoring Systems with 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography Imaging in Gastroenteropancreatic Neuroendocrine Neoplasms. Neuroendocrinology 2022, 112, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Laffi, A.; Spada, F.; Bagnardi, V.; Frassoni, S.; Pisa, E.; Rubino, M.; Barberis, M.; Fazio, N. Gastroenteropancreatic grade 3 neuroendocrine tumors: A single entity or a heterogeneous group? A retrospective analysis. J. Endocrinol. Investig. 2022, 45, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Lithgow, K.; Venkataraman, H.; Hughes, S.; Shah, H.; Vickrage, S.; Smith, S.; Humpries, S.; Elshafie, M.; Taniere, P.; Diaz-Cano, S.; et al. Well-differentiated gastroenteropancreatic G3 NET: Findings from a large single centre cohort. Sci. Rep. 2021, 11, 17947. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Al-Toubah, T.; Montilla-Soler, J.; El-Haddad, G.; Haider, M.; Strosberg, J. Somatostatin Receptor Expression in Lung Neuroendocrine Tumors: An Analysis of DOTATATE PET Scans. J. Nucl. Med. 2023, 64, 1895–1898. [Google Scholar] [CrossRef] [PubMed]
- Binderup, T.; Knigge, U.; Loft, A.; Federspiel, B.; Kjaer, A. 18F-fluorodeoxyglucose positron emission tomography predicts survival of patients with neuroendocrine tumors. Clin. Cancer Res. 2010, 16, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Has Simsek, D.; Kuyumcu, S.; Turkmen, C.; Sanlı, Y.; Aykan, F.; Unal, S.; Adalet, I. Can complementary 68Ga-DOTATATE and 18F-FDG PET/CT establish the missing link between histopathology and therapeutic approach in gastroenteropancreatic neuroendocrine tumors? J. Nucl. Med. 2014, 55, 1811–1817. [Google Scholar] [CrossRef] [PubMed]
- Naswa, N.; Sharma, P.; Gupta, S.K.; Karunanithi, S.; Reddy, R.M.; Patnecha, M.; Lata, S.; Kumar, R.; Malhotra, A.; Bal, C. Dual tracer functional imaging of gastroenteropancreatic neuroendocrine tumors using 68Ga-DOTA-NOC PET-CT and 18F-FDG PET-CT: Competitive or complimentary? Clin. Nucl. Med. 2014, 39, e27–e34. [Google Scholar] [CrossRef] [PubMed]
- Laffi, A.; Colandrea, M.; Buonsanti, G.; Frassoni, S.; Bagnardi, V.; Spada, F.; Pisa, E.; Barberis, M.; Rubino, M.; Grana, C.M.; et al. A Retrospective Analysis of the Correlation between Functional Imaging and Clinical Outcomes in Grade 3 Neuroendocrine Tumors (NETs G3). Diagnostics 2021, 11, 2401. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, Y.; Li, L.; Wang, H.; Huang, H.X.; Cao, D.; Ke, N.W.; Su, M.G.; Tian, R. Heterogeneous Uptake of 68 Ga-DOTATATE and 18 F-FDG in Initial Diagnosed Neuroendocrine Tumors Patients: Which Patients Are Suitable for Dual-Tracer PET Imaging? Clin. Nucl. Med. 2024, 49, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.L.; Pavlakis, N.; Schembri, G.P.; Bernard, E.J.; Hsiao, E.; Hayes, A.; Barnes, T.; Diakos, C.; Khasraw, M.; Samra, J.; et al. Dual Somatostatin Receptor/FDG PET/CT Imaging in Metastatic Neuroendocrine Tumours: Proposal for a Novel Grading Scheme with Prognostic Significance. Theranostics 2017, 7, 1149–1158. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chan, D.L.; Hayes, A.R.; Karfis, I.; Conner, A.; Furtado O’Mahony, L.; Mileva, M.; Bernard, E.; Roach, P.; Marin, G.; Pavlakis, N.; et al. Dual [68Ga]DOTATATE and [18F]FDG PET/CT in patients with metastatic gastroenteropancreatic neuroendocrine neoplasms: A multicentre validation of the NETPET score. Br. J. Cancer 2023, 128, 549–555. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chan, D.L.; Hayes, A.R.; Karfis, I.; Conner, A.; Furtado O’Mahony, L.; Mileva, M.; Bernard, E.; Roach, P.; Marin, G.; Pavlakis, N.; et al. [18F]FDG PET/CT-Avid Discordant Volume as a Biomarker in Patients with Gastroenteropancreatic Neuroendocrine Neoplasms: A Multicenter Study. J. Nucl. Med. 2024, 65, 185–191. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chan, D.L.; Ulaner, G.A.; Pattison, D.; Wyld, D.; Ladwa, R.; Kirchner, J.; Li, B.T.; Lai, W.V.; Pavlakis, N.; Roach, P.J.; et al. Dual PET Imaging in Bronchial Neuroendocrine Neoplasms: The NETPET Score as a Prognostic Biomarker. J. Nucl. Med. 2021, 62, 1278–1284. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Walter, T.; Brixi-Benmansour, H.; Lombard-Bohas, C.; Cadiot, G. New treatment strategies in advanced neuroendocrine tumours. Dig. Liver Dis. 2012, 44, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Modica, R.; Liccardi, A.; Minotta, R.; Cannavale, G.; Benevento, E.; Colao, A. Therapeutic strategies for patients with neuroendocrine neoplasms: Current perspectives. Expert Rev. Endocrinol. Metab. 2022, 17, 389–403. [Google Scholar] [CrossRef] [PubMed]
- Citterio, D.; Pusceddu, S.; Facciorusso, A.; Coppa, J.; Milione, M.; Buzzoni, R.; Bongini, M.; deBraud, F.; Mazzaferro, V. Primary tumour resection may improve survival in functional well-differentiated neuroendocrine tumours metastatic to the liver. Eur. J. Surg. Oncol. 2017, 43, 380–387. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
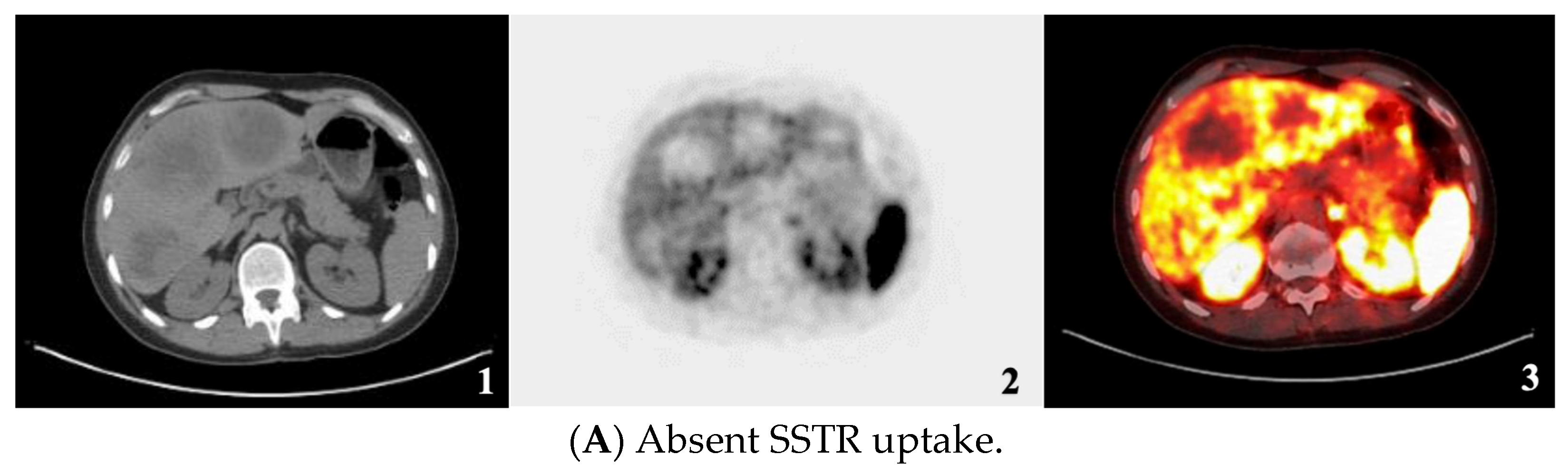
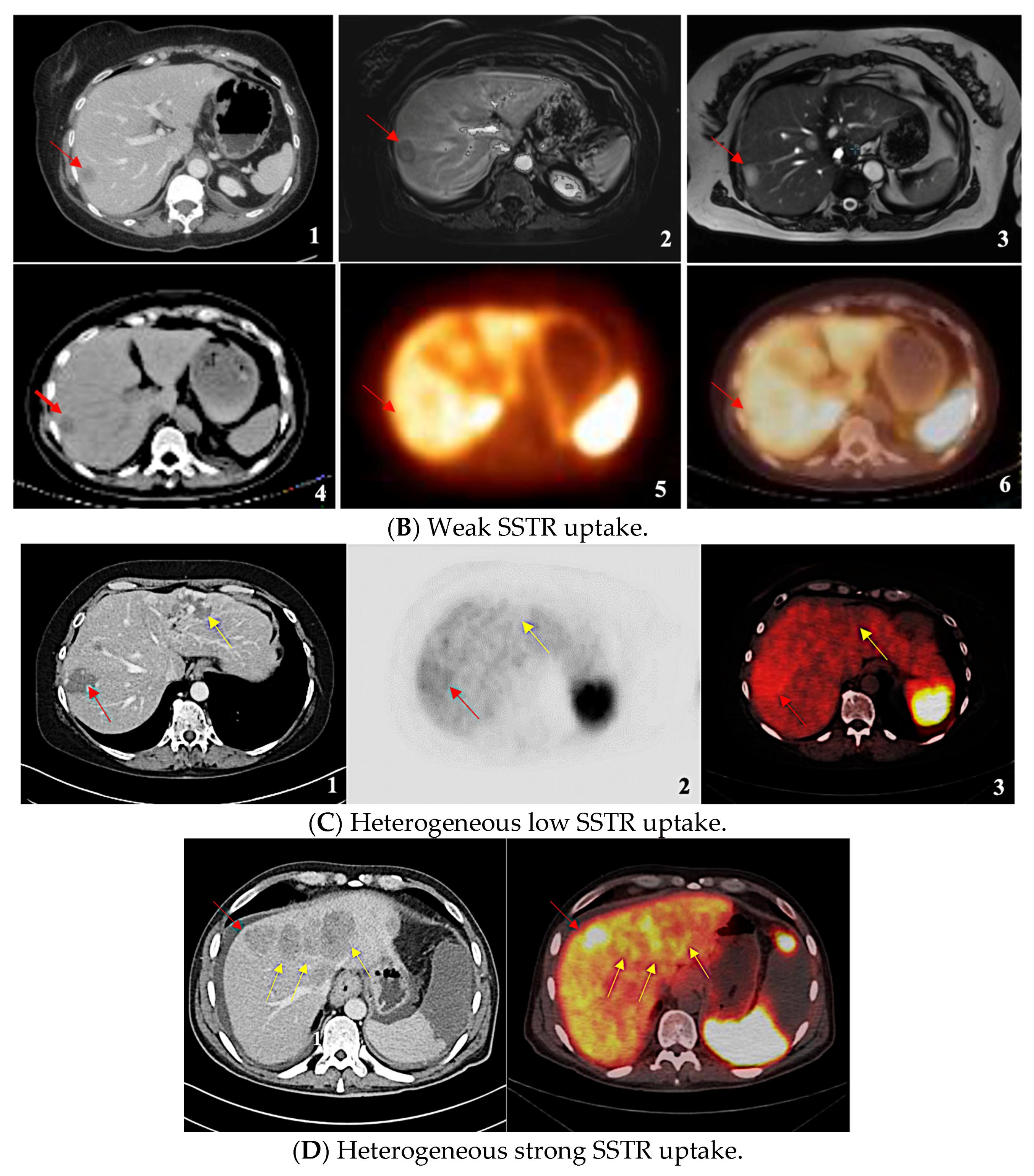
| SSTR Expression Assessment per Study | Krenning Score | Definition |
|---|---|---|
| Negative/Absent | 0 | No uptake |
| Homogeneous Weak | 1 | Much lower than liver |
| 2 | Slightly less than or equal to liver | |
| Homogeneous Strong | 3 | Greater than liver |
| 4 | Greater than spleen | |
| Heterogeneous Low | - | Mixture of absent and less than or equal to liver uptake lesions |
| Heterogeneous Strong | - | Mixture of strongly avid lesions combined with the absence or near absence of SSTR expression in at least one measurable tumor (primary or metastasis). |
| Parameter | N (=1192) | % |
|---|---|---|
| Sex | ||
| Female | 537 | 45.10% |
| Male | 655 | 54.90% |
| Grade | ||
| 1 | 389 | 32.60% |
| 2 | 613 | 51.40% |
| 3 | 95 | 8% |
| Unknown | 95 | 8% |
| Ki-67 | ||
| ≤2% | 389 | 32.60% |
| 3–20% | 581 | 48.70% |
| >20% | 95 | 8% |
| Unknown | 127 | 10.70% |
| Primary | ||
| Small Bowel | 784 | 65.80% |
| Pancreas | 302 | 25.30% |
| Gastric | 20 | 1.70% |
| Biliary-Tract | 8 | 0.70% |
| Appendix | 3 | 0.20% |
| Colorectal | 24 | 2% |
| Unknown | 51 | 4.30% |
| Hormone syndrome | ||
| Yes | 415 | 34.80% |
| No | 777 | 65.20% |
| SSTR Expression Assessment per Study | Total N = 1192 (100%) | [68Ga]-DOTATATE PET/CT N (%) | [64Cu]DOTATATE PET/CT N (%) |
|---|---|---|---|
| Negative/Absent | 26 (2.2%) | 20 (1.7%) | 6 (0.5%) |
| Homogeneous Weak | 27 (2.3%) | 26 (2.2%) | 1 (0.1%) |
| Homogeneous Strong | 1099 (92.2%) | 896 (75.2%) | 203 (17.0%) |
| Heterogeneous Low | 14 (1.2%) | 12 (1.0%) | 2 (0.2%) |
| Heterogeneous Strong | 26(2.2%) | 20 1.7(%) | 6 (0.5%) |
| SSTR Expression | G1 | G2 | G3 | N/A |
|---|---|---|---|---|
| Absent | 3 (0.8%) | 15 (2.4%) | 7 (7.4%) | 1 (1.1%) |
| Uniformly present low expression (<liver) | 12 (3.1%) | 13 (2.1%) | 2 (2.1%) | - |
| Uniformly present high expression (>liver) | 370 (95.1%) | 566 (92.3%) | 70 (73.7%) | 93 (97.9%) |
| Heterogeneous low expression (mixture of low and absent expression) | - | 4 (0.7%) | 10 (10.5%) | - |
| Heterogeneous strong expression (mixture of high and absent expression) | 4 (1.0%) | 15 (2.4%) | 6 (6.3%) | 1 (1.1%) |
| Total (100%) | 389 | 613 | 95 | 95 |
| SSTR Expression | SI-NET | Pan-NET | Other |
|---|---|---|---|
| Absent | 5 (0.6%) | 14 (4.6%) | 7 (6.6%) |
| Uniformly present low expression (<liver) | 17 (2.2%) | 7 (2.3%) | 3 (2.8%) |
| Uniformly present high expression (>liver) | 748 (95.4%) | 259 (85.8%) | 92 (86.8%) |
| Heterogeneous low expression (mixture of low and absent expression) | 2 (0.3%) | 8 (2.6%) | 4 (3.8%) |
| Heterogeneous strong expression (mixture of high and absent expression) | 12 (1.5%) | 14 (4.6%) | - |
| Total (100%) | 784 | 302 | 106 |
| SSTR Expression Assessment per Study | Krenning Score | Definition | Mean SUVmax |
|---|---|---|---|
| Negative/Absent | 0 | No uptake | - |
| Homogeneous Weak | 1 | Much lower than liver | 9 |
| 2 | Slightly less than or equal to liver | ||
| Homogeneous Strong | 3 | Greater than liver | 31.2 |
| 4 | Greater than spleen | ||
| Heterogeneous Low | - | Mixture of absent and less than or equal to liver uptake lesions | 9.5 |
| Heterogeneous Strong | - | Mixture of strongly avid lesions combined with the absence or near absence of SSTR expression in at least one measurable tumor (primary or metastasis). | 42.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maratta, M.G.; Al-Toubah, T.; Montilla-Soler, J.; Pelle, E.; Haider, M.; El-Haddad, G.; Strosberg, J. Somatostatin Receptor Expression of Gastroenteropancreatic Neuroendocrine Tumors: A Comprehensive Analysis in the Era of Somatostatin Receptor PET Imaging. Cancers 2025, 17, 1937. https://doi.org/10.3390/cancers17121937
Maratta MG, Al-Toubah T, Montilla-Soler J, Pelle E, Haider M, El-Haddad G, Strosberg J. Somatostatin Receptor Expression of Gastroenteropancreatic Neuroendocrine Tumors: A Comprehensive Analysis in the Era of Somatostatin Receptor PET Imaging. Cancers. 2025; 17(12):1937. https://doi.org/10.3390/cancers17121937
Chicago/Turabian StyleMaratta, Maria Grazia, Taymeyah Al-Toubah, Jaime Montilla-Soler, Eleonora Pelle, Mintallah Haider, Ghassan El-Haddad, and Jonathan Strosberg. 2025. "Somatostatin Receptor Expression of Gastroenteropancreatic Neuroendocrine Tumors: A Comprehensive Analysis in the Era of Somatostatin Receptor PET Imaging" Cancers 17, no. 12: 1937. https://doi.org/10.3390/cancers17121937
APA StyleMaratta, M. G., Al-Toubah, T., Montilla-Soler, J., Pelle, E., Haider, M., El-Haddad, G., & Strosberg, J. (2025). Somatostatin Receptor Expression of Gastroenteropancreatic Neuroendocrine Tumors: A Comprehensive Analysis in the Era of Somatostatin Receptor PET Imaging. Cancers, 17(12), 1937. https://doi.org/10.3390/cancers17121937