
Innovative Approaches to Early Detection of Cancer-Transforming Screening for Breast, Lung, and Hard-to-Screen Cancers


Simple Summary
Abstract
1. Introduction
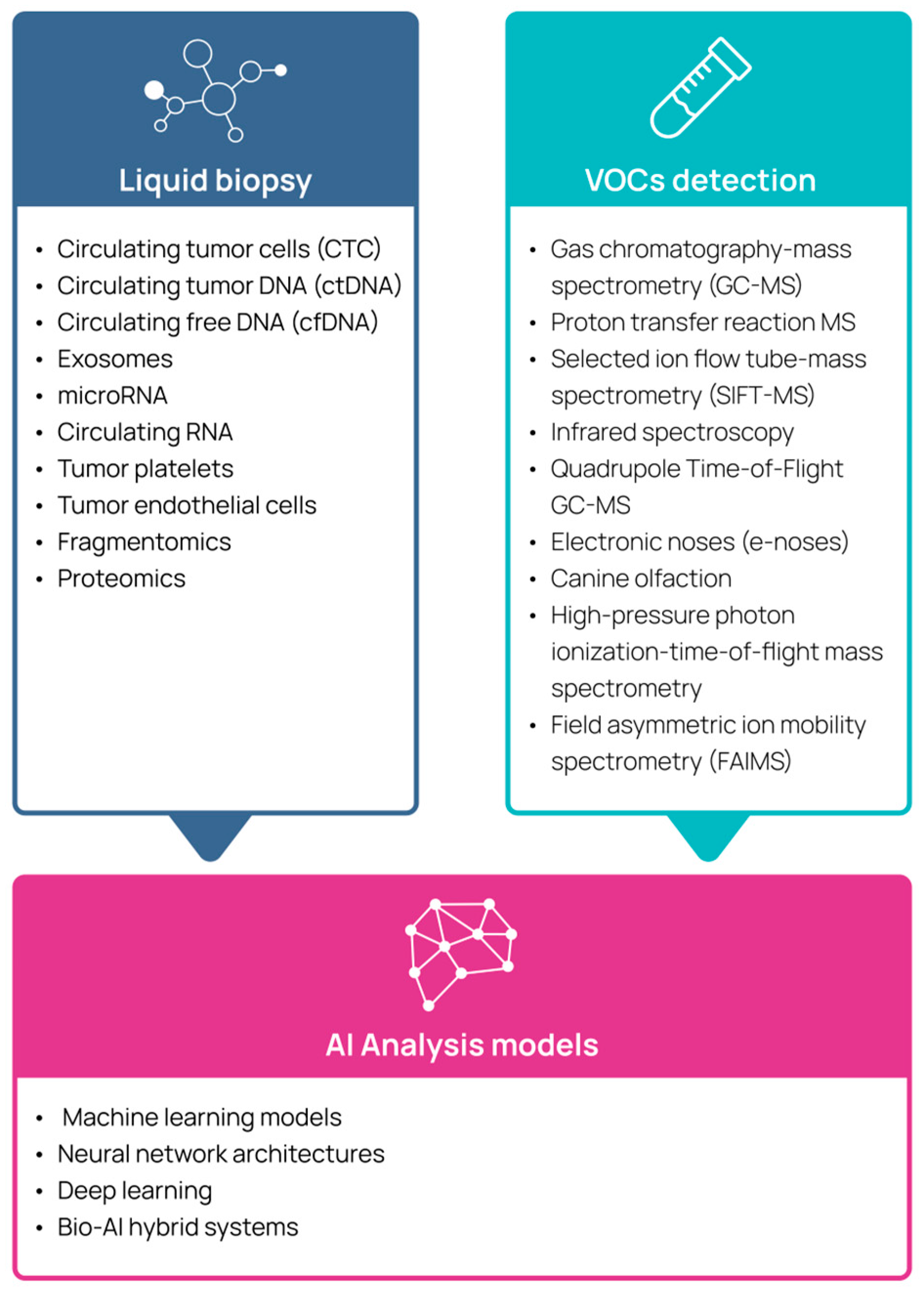
2. Liquid Biopsy
3. Volatile Organic Compounds
3.1. The Scientific Basis for the Use of Volatile Organic Compounds in Cancer Detection
3.2. Use of Electronic Noses for Volatile Organic Compound Detection
3.3. Use of Canines for Volatile Organic Compound Detection
3.4. Use of Volatile Organic Compound Analysis for Detection of Cancer
4. Using Artificial Intelligence in the Analysis of Volatile Organic Compounds and Liquid Biopsy
5. Schemes and Methods for Early Detection of Specific Cancers
5.1. Breast Cancer
5.1.1. Surveillance Schemes for Early Detection of Breast Cancer
5.1.2. Liquid Biopsy Analysis for Breast Cancer Detection
5.1.3. VOC Analysis for Breast Cancer Detection
5.2. Lung Cancer
5.2.1. Surveillance Schemes for Early Detection of Lung Cancer
5.2.2. Liquid Biopsy Analysis for Lung Cancer Detection
5.2.3. VOC Analysis for Early Detection of Lung Cancer
5.3. Pancreatic Cancer
5.3.1. Liquid Biopsy for Pancreatic Cancer Detection
5.3.2. VOC Analysis for Pancreatic Cancer Detection
5.4. Ovarian Cancer
5.4.1. Ovarian Cancer Screening
5.4.2. Liquid Biopsy for Ovarian Cancer Detection
5.4.3. VOCs for Ovarian Cancer Detection
6. Sex-Related Differences in Multicancer Early Detection for Pancreatic and Lung Cancer
7. Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ASR | Age-Standardized Rate |
| BC | Breast Cancer |
| CfDNA | Circulating Free DNA |
| CTC | Circulating Tumor Cells |
| CtDNA | Circulating Tumor DNA |
| GC | Gas Chromatography |
| HPPI-TOF-MS | High-Pressure Photon Ionization-Time-of-Flight Mass Spectrometry |
| LB | Liquid Biopsy |
| LC | Lung Cancer |
| MCED | Multi-Cancer Early Detection |
| MS | Mass Spectrometry |
| NCCN | National Comprehensive Cancer Network |
| OvC | Ovarian Cancer |
| PDAC | Pancreatic Ductal Adenocarcinoma |
| SIFT-MS | Selected Ion Flow Tube Mass Spectrometry |
| USPSTF | US Preventive Services Task Force |
| VOC | Volatile Organic Compounds |
References
- Ferlay, J.; Ervik, M.; Lam, F.; Laversanne, M.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2024. [Google Scholar]
- Crosby, D.; Bhatia, S.; Brindle, K.M.; Coussens, L.M.; Dive, C.; Emberton, M.; Esener, S.; Fitzgerald, R.C.; Gambhir, S.S.; Kuhn, P.; et al. Early detection of cancer. Science 2022, 375, eaay9040. [Google Scholar] [CrossRef] [PubMed]
- Spear, G.; Lee, K.; DePersia, A.; Lienhoop, T.; Saha, P. Updates in Breast Cancer Screening and Diagnosis. Curr. Treat. Options Oncol. 2024, 25, 1451–1460. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.M.D.; Oeffinger, K.C.; Shih, T.Y.; Walter, L.C.; Church, T.R.; Fontham, E.T.H.; Elkin, E.B.; Etzioni, R.D.; Guerra, C.E.; Perkins, R.B.; et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J. Clin. 2024, 74, 50–81. [Google Scholar] [CrossRef] [PubMed]
- Bandi, P.; Star, J.; Ashad-Bishop, K.; Kratzer, T.; Smith, R.; Jemal, A. Lung Cancer Screening in the US, 2022. JAMA Intern. Med. 2024, 184, 882–891. [Google Scholar] [CrossRef]
- State of Lung Cancer 2022; American Lung Association: Chicago, IL, USA, 2022.
- Cancer Trends Progress Report: Breast Cancer Screening. Available online: https://progressreport.cancer.gov/detection/breast_cancer (accessed on 6 March 2025).
- USPSTF. Final Recommendation Statement Breast Cancer: Screening. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/breast-cancer-screening (accessed on 6 March 2025).
- Xu, S.; Murtagh, S.; Han, Y.; Wan, F.; Toriola, A.T. Breast Cancer Incidence Among US Women Aged 20 to 49 Years by Race, Stage, and Hormone Receptor Status. JAMA Netw. Open 2024, 7, e2353331. [Google Scholar] [CrossRef]
- Jemal, A.; Schafer, E.J.; Sung, H.; Bandi, P.; Kratzer, T.; Islami, F.; Siegel, R.L. The Burden of Lung Cancer in Women Compared With Men in the US. JAMA Oncol. 2023, 9, 1727–1728. [Google Scholar] [CrossRef]
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502. [Google Scholar] [CrossRef]
- Pancreatic Cancer Statistics. Available online: https://www.wcrf.org/preventing-cancer/cancer-statistics/pancreatic-cancer-statistics/ (accessed on 6 March 2025).
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef]
- Wei, Y.-F.; Ning, L.; Xu, Y.-L.; Ma, J.; Li, D.-R.; Feng, Z.-F.; Liu, F.-H.; Li, Y.-Z.; Xu, H.-L.; Li, P.; et al. Worldwide patterns and trends in ovarian cancer incidence by histological subtype: A population-based analysis from 1988 to 2017. eClinicalMedicine 2025, 79, 102983. [Google Scholar] [CrossRef]
- SEER. Cancer Stat Facts: Pancreatic Cancer. Available online: https://seer.cancer.gov/statfacts/html/pancreas.html (accessed on 22 May 2025).
- Upadhyay, A.; Garg, V.; Mathur, S.; Singh Malik, P.; Bhatla, N.; Kumar, S.; Khurana, S.; Kumar, L. Early-Stage epithelial ovarian cancer: Predictors of survival. Gynecol. Oncol. Rep. 2022, 44, 101083. [Google Scholar] [CrossRef]
- Fu, S.W.; Tang, C.; Tan, X.; Srivastava, S. Liquid biopsy for early cancer detection: Technological revolutions and clinical dilemma. Expert. Rev. Mol. Diagn. 2024, 24, 937–955. [Google Scholar] [CrossRef] [PubMed]
- Batool, S.M.; Yekula, A.; Khanna, P.; Hsia, T.; Gamblin, A.S.; Ekanayake, E.; Escobedo, A.K.; You, D.G.; Castro, C.M.; Im, H.; et al. The Liquid Biopsy Consortium: Challenges and opportunities for early cancer detection and monitoring. Cell Rep. Med. 2023, 4, 101198. [Google Scholar] [CrossRef] [PubMed]
- Foser, S.; Maiese, K.; Digumarthy, S.R.; Puig-Butille, J.A.; Rebhan, C. Looking to the Future of Early Detection in Cancer: Liquid Biopsies, Imaging, and Artificial Intelligence. Clin. Chem. 2024, 70, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Guo, H.; Zhao, Y.; Liu, Z.; Wang, C.; Bu, J.; Sun, T.; Wei, J. Liquid biopsy in cancer current: Status, challenges and future prospects. Signal Transduct. Target. Ther. 2024, 9, 336. [Google Scholar] [CrossRef]
- Chakraborty, S.; Hosen, M.I.; Ahmed, M.; Shekhar, H.U. Onco-Multi-OMICS Approach: A New Frontier in Cancer Research. Biomed. Res. Int. 2018, 2018, 9836256. [Google Scholar] [CrossRef]
- Baldini, C.; Billeci, L.; Sansone, F.; Conte, R.; Domenici, C.; Tonacci, A. Electronic Nose as a Novel Method for Diagnosing Cancer: A Systematic Review. Biosensors 2020, 10, 84. [Google Scholar] [CrossRef]
- Baratella, E.; Carbi, M.; Minelli, P.; Segalotti, A.; Ruaro, B.; Salton, F.; Polverosi, R.; Cova, M.A. Calcified Lung Nodules: A Diagnostic Challenge in Clinical Daily Practice. Tomography 2025, 11, 28. [Google Scholar] [CrossRef]
- Brahimetaj, R.; Willekens, I.; Massart, A.; Forsyth, R.; Cornelis, J.; Mey, J.D.; Jansen, B. Improved automated early detection of breast cancer based on high resolution 3D micro-CT microcalcification images. BMC Cancer 2022, 22, 162. [Google Scholar] [CrossRef]
- O’Connor, E.; Mullins, M.; O’Connor, D.; Phelan, S.; Bruzzi, J. The relationship between ultrasound microcalcifications and psammoma bodies in thyroid tumours: A single-institution retrospective study. Clin. Radiol. 2022, 77, e48–e54. [Google Scholar] [CrossRef]
- Porcelli, F.; Verri, M.; De Santis, S.; Crescenzi, A.; Bianchi, A.; Felici, A.C.; Sotgiu, G.; Romano, S.; Orsini, M. Considerations on chemical composition of psammoma bodies: Automated detection strategy by infrared microspectroscopy in ovarian and thyroid cancer tissues. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2023, 298, 122792. [Google Scholar] [CrossRef]
- Cena, B.; Melloul, E.; Demartines, N.; Dormond, O.; Labgaa, I. Basic Science with Preclinical Models to Investigate and Develop Liquid Biopsy: What Are the Available Data and Is It a Fruitful Approach? Int. J. Mol. Sci. 2022, 23, 5343. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabieres, C.; Marchetti, D.; Lang, J.E. Liquid biopsy: From concept to clinical application. Sci. Rep. 2023, 13, 21685. [Google Scholar] [CrossRef] [PubMed]
- Connal, S.; Cameron, J.M.; Sala, A.; Brennan, P.M.; Palmer, D.S.; Palmer, J.D.; Perlow, H.; Baker, M.J. Liquid biopsies: The future of cancer early detection. J. Transl. Med. 2023, 21, 118. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Li, C.; Zhou, Y.; Yao, Y.; Liu, J.; Wu, M.; Su, J. Liquid biopsies for cancer: From bench to clinic. MedComm (2020) 2023, 4, e329. [Google Scholar] [CrossRef]
- Schrag, D.; Beer, T.M.; McDonnell, C.H., 3rd; Nadauld, L.; Dilaveri, C.A.; Reid, R.; Marinac, C.R.; Chung, K.C.; Lopatin, M.; Fung, E.T.; et al. Blood-based tests for multicancer early detection (PATHFINDER): A prospective cohort study. Lancet 2023, 402, 1251–1260. [Google Scholar] [CrossRef]
- Nicholson, B.D.; Oke, J.; Virdee, P.S.; Harris, D.A.; O’Doherty, C.; Park, J.E.; Hamady, Z.; Sehgal, V.; Millar, A.; Medley, L.; et al. Multi-cancer early detection test in symptomatic patients referred for cancer investigation in England and Wales (SYMPLIFY): A large-scale, observational cohort study. Lancet Oncol. 2023, 24, 733–743. [Google Scholar] [CrossRef]
- Cohen, J.D.; Javed, A.A.; Thoburn, C.; Wong, F.; Tie, J.; Gibbs, P.; Schmidt, C.M.; Yip-Schneider, M.T.; Allen, P.J.; Schattner, M.; et al. Combined circulating tumor DNA and protein biomarker-based liquid biopsy for the earlier detection of pancreatic cancers. Proc. Natl. Acad. Sci. USA 2017, 114, 10202–10207. [Google Scholar] [CrossRef]
- Reese, K.L.; Pantel, K.; Smit, D.J. Multibiomarker panels in liquid biopsy for early detection of pancreatic cancer—A comprehensive review. J. Exp. Clin. Cancer Res. 2024, 43, 250. [Google Scholar] [CrossRef]
- Luchini, C.; Veronese, N.; Nottegar, A.; Cappelletti, V.; Daidone, M.G.; Smith, L.; Parris, C.; Brosens, L.A.A.; Caruso, M.G.; Cheng, L.; et al. Liquid Biopsy as Surrogate for Tissue for Molecular Profiling in Pancreatic Cancer: A Meta-Analysis Towards Precision Medicine. Cancers 2019, 11, 1152. [Google Scholar] [CrossRef]
- Sefrioui, D.; Blanchard, F.; Toure, E.; Basile, P.; Beaussire, L.; Dolfus, C.; Perdrix, A.; Paresy, M.; Antonietti, M.; Iwanicki-Caron, I.; et al. Diagnostic value of CA19.9, circulating tumour DNA and circulating tumour cells in patients with solid pancreatic tumours. Br. J. Cancer 2017, 117, 1017–1025. [Google Scholar] [CrossRef]
- Montoya Mira, J.L.; Quentel, A.; Patel, R.K.; Keith, D.; Sousa, M.; Minnier, J.; Kingston, B.R.; David, L.; Esener, S.C.; Sears, R.C.; et al. Early detection of pancreatic cancer by a high-throughput protease-activated nanosensor assay. Sci. Transl. Med. 2025, 17, eadq3110. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulou, L.; Lianidou, E.S. Liquid biopsy in ovarian cancer. Adv. Clin. Chem. 2020, 97, 13–71. [Google Scholar] [CrossRef] [PubMed]
- Balla, A.; Bhak, J.; Biro, O. The application of circulating tumor cell and cell-free DNA liquid biopsies in ovarian cancer. Mol. Cell Probes 2022, 66, 101871. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.W.; Charkhchi, P.; Akbari, M.R. Potential clinical utility of liquid biopsies in ovarian cancer. Mol. Cancer 2022, 21, 114. [Google Scholar] [CrossRef]
- Asante, D.B.; Calapre, L.; Ziman, M.; Meniawy, T.M.; Gray, E.S. Liquid biopsy in ovarian cancer using circulating tumor DNA and cells: Ready for prime time? Cancer Lett. 2020, 468, 59–71. [Google Scholar] [CrossRef]
- Kuo, Y.C.; Chuang, C.H.; Kuo, H.C.; Lin, C.T.; Chao, A.; Huang, H.J.; Wang, H.M.; Hsieh, J.C.; Chou, H.H. Circulating tumor cells help differentiate benign ovarian lesions from cancer before surgery: A literature review and proof of concept study using flow cytometry with fluorescence imaging. Oncol. Lett. 2024, 27, 234. [Google Scholar] [CrossRef]
- Farncombe, K.M.; Wong, D.; Norman, M.L.; Oldfield, L.E.; Sobotka, J.A.; Basik, M.; Bombard, Y.; Carile, V.; Dawson, L.; Foulkes, W.D.; et al. Current and new frontiers in hereditary cancer surveillance: Opportunities for liquid biopsy. Am. J. Hum. Genet. 2023, 110, 1616–1627. [Google Scholar] [CrossRef]
- Yao, M.; Amor, R.E.; Zheng, Y.; Haick, H.; Qian, Y.; Wu, W. Hybrid Volatilomics in Healthcare. In Volatile Biomarkers for Human Health: From Nature to Artificial Senses; Haick, H., Ed.; The Royal Society of Chemistry: London, UK, 2022. [Google Scholar]
- Allard-Coutu, A.; Singh, K.; David, D.; Dobson, V.; Dahmer, L.; Heller, B. Volatile organic compounds: A promising new frontier for cancer screening. Tumor Discov. 2024, 3, 2061. [Google Scholar] [CrossRef]
- Janfaza, S.; Khorsand, B.; Nikkhah, M.; Zahiri, J. Digging deeper into volatile organic compounds associated with cancer. Biol. Methods Protoc. 2019, 4, bpz014. [Google Scholar] [CrossRef]
- Sethi, S.; Nanda, R.; Chakraborty, T. Clinical application of volatile organic compound analysis for detecting infectious diseases. Clin. Microbiol. Rev. 2013, 26, 462–475. [Google Scholar] [CrossRef]
- Wang, C.; Li, P.; Lian, A.; Sun, B.; Wang, X.; Guo, L.; Chi, C.; Liu, S.; Zhao, W.; Luo, S.; et al. Blood volatile compounds as biomarkers for colorectal cancer. Cancer Biol. Ther. 2014, 15, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Cavaco, C.; Pereira, J.A.M.; Taunk, K.; Taware, R.; Rapole, S.; Nagarajaram, H.; Câmara, J.S. Screening of salivary volatiles for putative breast cancer discrimination: An exploratory study involving geographically distant populations. Anal. Bioanal. Chem. 2018, 410, 4459–4468. [Google Scholar] [CrossRef] [PubMed]
- Monedeiro, F.; Dos Reis, R.B.; Peria, F.M.; Sares, C.T.G.; De Martinis, B.S. Investigation of sweat VOC profiles in assessment of cancer biomarkers using HS-GC-MS. J. Breath. Res. 2020, 14, 026009. [Google Scholar] [CrossRef]
- Bajo-Fernandez, M.; Souza-Silva, E.A.; Barbas, C.; Rey-Stolle, M.F.; Garcia, A. GC-MS-based metabolomics of volatile organic compounds in exhaled breath: Applications in health and disease. A review. Front. Mol. Biosci. 2023, 10, 1295955. [Google Scholar] [CrossRef] [PubMed]
- Hara, T.; Meng, S.; Arao, Y.; Saito, Y.; Inoue, K.; Alshammari, A.H.; Hatakeyama, H.; di Luccio, E.; Vecchione, A.; Hirotsu, T.; et al. Non-Invasive Detection of Tumors by Volatile Organic Compounds in Urine. Biomedicines 2025, 13, 109. [Google Scholar] [CrossRef]
- Kouremenos, K.A.; Johansson, M.; Marriott, P.J. Advances in gas chromatographic methods for the identification of biomarkers in cancer. J. Cancer 2012, 3, 404–420. [Google Scholar] [CrossRef]
- Wallace, M.A.G.; Pleil, J.D. Evolution of clinical and environmental health applications of exhaled breath research: Review of methods and instrumentation for gas-phase, condensate, and aerosols. Anal. Chim. Acta 2018, 1024, 18–38. [Google Scholar] [CrossRef]
- Einoch Amor, R.; Nakhleh, M.K.; Barash, O.; Haick, H. Breath analysis of cancer in the present and the future. Eur. Respir. Rev. 2019, 28, 190002. [Google Scholar] [CrossRef]
- Vassilenko, V.; Moura, P.C.; Raposo, M. Diagnosis of Carcinogenic Pathologies through Breath Biomarkers: Present and Future Trends. Biomedicines 2023, 11, 3029. [Google Scholar] [CrossRef]
- Karakaya, D.; Ulucan, O.; Turkan, M. Electronic Nose and Its Applications: A Survey. Int. J. Autom. Comput. 2020, 17, 179–209. [Google Scholar] [CrossRef]
- Scheepers, M.; Al-Difaie, Z.; Brandts, L.; Peeters, A.; van Grinsven, B.; Bouvy, N.D. Diagnostic Performance of Electronic Noses in Cancer Diagnoses Using Exhaled Breath: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2219372. [Google Scholar] [CrossRef] [PubMed]
- Pirrone, F.; Albertini, M. Olfactory detection of cancer by trained sniffer dogs: A systematic review of the literature. J. Vet. Behav. 2017, 19, 105–117. [Google Scholar] [CrossRef]
- Lippi, G.; Heaney, L.M. The “olfactory fingerprint”: Can diagnostics be improved by combining canine and digital noses? Clin. Chem. Lab. Med. 2020, 58, 958–967. [Google Scholar] [CrossRef] [PubMed]
- Padodara, R. Olfactory sense in different animals. Indian J. Vet. Sci. 2014, 2, 1–14. [Google Scholar]
- Angle, C.; Waggoner, L.P.; Ferrando, A.; Haney, P.; Passler, T. Canine Detection of the Volatilome: A Review of Implications for Pathogen and Disease Detection. Front. Vet. Sci. 2016, 3, 47. [Google Scholar] [CrossRef]
- Singletary, M.; Hagerty, S. Peripheral Olfactory Pathway Anatomy, Physiology, and Genetics. In Olfactory Research in Dogs; Lazarowski, L., Ed.; Springer International Publishing: Cham, Switzerland, 2023; pp. 3–37. [Google Scholar]
- Furton, K.G.; Caraballo, N.I.; Cerreta, M.M.; Holness, H.K. Advances in the use of odour as forensic evidence through optimizing and standardizing instruments and canines. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2015, 370, 20140262. [Google Scholar] [CrossRef]
- Jendrny, P.; Twele, F.; Meller, S.; Osterhaus, A.; Schalke, E.; Volk, H.A. Canine olfactory detection and its relevance to medical detection. BMC Infect. Dis. 2021, 21, 838. [Google Scholar] [CrossRef]
- Tan, S.Y.; Ma, Q.; Li, F.; Jiang, H.; Peng, X.Y.; Dong, J.; Ye, X.; Wang, Q.L.; You, F.M.; Fu, X.; et al. Does the last 20 years paradigm of clinical research using volatile organic compounds to non-invasively diagnose cancer need to change? Challenges and future direction. J. Cancer Res. Clin. Oncol. 2023, 149, 10377–10386. [Google Scholar] [CrossRef]
- da Costa, B.R.B.; De Martinis, B.S. Analysis of urinary VOCs using mass spectrometric methods to diagnose cancer: A review. Clin. Mass. Spectrom. 2020, 18, 27–37. [Google Scholar] [CrossRef]
- Goertzen, A.; Kidane, B.; Ahmed, N.; Aliani, M. Potential urinary volatile organic compounds as screening markers in cancer—A review. Front. Oncol. 2024, 14, 1448760. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, Q.; Lu, X.; Zhang, P.; Yang, R.; Chen, Y.; Xia, J.; Chen, D. Exhaled breath and urinary volatile organic compounds (VOCs) for cancer diagnoses, and microbial-related VOC metabolic pathway analysis: A systematic review and meta-analysis. Int. J. Surg. 2024, 110, 1755–1769. [Google Scholar] [CrossRef] [PubMed]
- Hintzen, K.F.H.; Grote, J.; Wintjens, A.; Lubbers, T.; Eussen, M.M.M.; van Schooten, F.J.; Bouvy, N.D.; Peeters, A. Breath analysis for the detection of digestive tract malignancies: Systematic review. BJS Open 2021, 5, zrab013. [Google Scholar] [CrossRef] [PubMed]
- Hanna, G.B.; Boshier, P.R.; Markar, S.R.; Romano, A. Accuracy and Methodologic Challenges of Volatile Organic Compound-Based Exhaled Breath Tests for Cancer Diagnosis: A Systematic Review and Meta-analysis. JAMA Oncol. 2019, 5, e182815. [Google Scholar] [CrossRef] [PubMed]
- Half, E.; Ovcharenko, A.; Shmuel, R.; Furman-Assaf, S.; Avdalimov, M.; Rabinowicz, A.; Arber, N. Non-invasive multiple cancer screening using trained detection canines and artificial intelligence: A prospective double-blind study. Sci. Rep. 2024, 14, 28204. [Google Scholar] [CrossRef]
- Haripriya, P.; Rangarajan, M.; Pandya, H.J. Breath VOC analysis and machine learning approaches for disease screening: A review. J. Breath. Res. 2023, 17, 024001. [Google Scholar] [CrossRef]
- Hunter, B.; Hindocha, S.; Lee, R.W. The Role of Artificial Intelligence in Early Cancer Diagnosis. Cancers 2022, 14, 1524. [Google Scholar] [CrossRef]
- Vinhas, M.; Leitão, P.M.; Raimundo, B.S.; Gil, N.; Vaz, P.D.; Luis-Ferreira, F. AI Applied to Volatile Organic Compound (VOC) Profiles from Exhaled Breath Air for Early Detection of Lung Cancer. Cancers 2024, 16, 2200. [Google Scholar] [CrossRef]
- Gallos, I.K.; Tryfonopoulos, D.; Shani, G.; Amditis, A.; Haick, H.; Dionysiou, D.D. Advancing Colorectal Cancer Diagnosis with AI-Powered Breathomics: Navigating Challenges and Future Directions. Diagnostics 2023, 13. [Google Scholar] [CrossRef]
- Grasso, A.; Altomare, V.; Fiorini, G.; Zompanti, A.; Pennazza, G.; Santonico, M. Innovative Methodologies for the Early Detection of Breast Cancer: A Review Categorized by Target Biological Samples. Biosensors 2025, 15, 257. [Google Scholar] [CrossRef]
- Kim, M.; Park, J.; Oh, S.; Jeong, B.-H.; Byun, Y.; Shin, S.H.; Im, Y.; Cho, J.H.; Cho, E.-H. Deep learning model integrating cfDNA methylation and fragment size profiles for lung cancer diagnosis. Sci. Rep. 2024, 14, 14797. [Google Scholar] [CrossRef]
- Yan, F.; Jiang, L.; Ye, F.; Ping, J.; Bowley, T.Y.; Ness, S.A.; Li, C.I.; Marchetti, D.; Tang, J.; Guo, Y. Deep neural network based tissue deconvolution of circulating tumor cell RNA. J. Transl. Med. 2023, 21, 783. [Google Scholar] [CrossRef] [PubMed]
- Moser, T.; Kühberger, S.; Lazzeri, I.; Vlachos, G.; Heitzer, E. Bridging biological cfDNA features and machine learning approaches. Trends Genet. 2023, 39, 285–307. [Google Scholar] [CrossRef] [PubMed]
- Medina, J.E.; Annapragada, A.V.; Lof, P.; Short, S.; Bartolomucci, A.L.; Mathios, D.; Koul, S.; Niknafs, N.; Noë, M.; Foda, Z.H.; et al. Early Detection of Ovarian Cancer Using Cell-Free DNA Fragmentomes and Protein Biomarkers. Cancer Discov. 2025, 15, 105–118. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society Recommendations for the Early Detection of Breast Cancer. Available online: https://www.cancer.org/cancer/types/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html (accessed on 11 March 2025).
- NCCN Guidelines Breast Cancer; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2025.
- Li, J.; Guan, X.; Fan, Z.; Ching, L.M.; Li, Y.; Wang, X.; Cao, W.M.; Liu, D.X. Non-Invasive Biomarkers for Early Detection of Breast Cancer. Cancers 2020, 12, 2767. [Google Scholar] [CrossRef]
- Ginsburg, O.; Yip, C.H.; Brooks, A.; Cabanes, A.; Caleffi, M.; Dunstan Yataco, J.A.; Gyawali, B.; McCormack, V.; McLaughlin de Anderson, M.; Mehrotra, R.; et al. Breast cancer early detection: A phased approach to implementation. Cancer 2020, 126 (Suppl. S10), 2379–2393. [Google Scholar] [CrossRef]
- Duque, G.; Manterola, C.; Otzen, T.; Arias, C.; Palacios, D.; Mora, M.; Galindo, B.; Holguín, J.P.; Albarracín, L. Cancer Biomarkers in Liquid Biopsy for Early Detection of Breast Cancer: A Systematic Review. Clin. Med. Insights Oncol. 2022, 16, 11795549221134831. [Google Scholar] [CrossRef]
- Panet, F.; Papakonstantinou, A.; Borrell, M.; Vivancos, J.; Vivancos, A.; Oliveira, M. Use of ctDNA in early breast cancer: Analytical validity and clinical potential. Npj Breast Cancer 2024, 10, 50. [Google Scholar] [CrossRef]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef]
- Brito-Rocha, T.; Constâncio, V.; Henrique, R.; Jerónimo, C. Shifting the Cancer Screening Paradigm: The Rising Potential of Blood-Based Multi-Cancer Early Detection Tests. Cells 2023, 12, 935. [Google Scholar] [CrossRef]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Giro Benet, J.; Seo, M.; Khine, M.; Guma Padro, J.; Pardo Martnez, A.; Kurdahi, F. Breast cancer detection by analyzing the volatile organic compound (VOC) signature in human urine. Sci. Rep. 2022, 12, 14873. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Cataneo, R.N.; Cruz-Ramos, J.A.; Huston, J.; Ornelas, O.; Pappas, N.; Pathak, S. Prediction of breast cancer risk with volatile biomarkers in breath. Breast Cancer Res. Treat. 2018, 170, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, H.; Li, Y.; Fang, Y.; Guo, Y.; Li, S.; Xu, J.; Jia, Z.; Zou, J.; Liu, G.; et al. A novel non-invasive exhaled breath biopsy for the diagnosis and screening of breast cancer. J. Hematol. Oncol. 2023, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Bevers, T.B.; Larsen, L.H.; Pappas, N.; Pathak, S. Rapid point-of-care breath test predicts breast cancer and abnormal mammograms in symptomatic women. J. Breath. Res. 2024, 18, 046011. [Google Scholar] [CrossRef]
- Yang, Y.; Long, H.; Feng, Y.; Tian, S.; Chen, H.; Zhou, P. A multi-omics method for breast cancer diagnosis based on metabolites in exhaled breath, ultrasound imaging, and basic clinical information. Heliyon 2024, 10, e32115. [Google Scholar] [CrossRef]
- Leemans, M.; Bauer, P.; Cuzuel, V.; Audureau, E.; Fromantin, I. Volatile Organic Compounds Analysis as a Potential Novel Screening Tool for Breast Cancer: A Systematic Review. Biomark. Insights 2022, 17, 11772719221100709. [Google Scholar] [CrossRef]
- Can Lung Cancer Be Found Early? Available online: https://www.cancer.org/cancer/types/lung-cancer/detection-diagnosis-staging/detection.html#:~:text=LDCT%20scans%20can%20help%20find,of%20dying%20from%20lung%20cancer (accessed on 11 March 2025).
- USPSTF. Final Recommendation Statement: Lung Cancer: Screening. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung-cancer-screening#fullrecommendationstart (accessed on 11 March 2025).
- Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; Sicks, J.D. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Sadate, A.; Occean, B.V.; Beregi, J.P.; Hamard, A.; Addala, T.; de Forges, H.; Fabbro-Peray, P.; Frandon, J. Systematic review and meta-analysis on the impact of lung cancer screening by low-dose computed tomography. Eur. J. Cancer 2020, 134, 107–114. [Google Scholar] [CrossRef]
- Field, J.K.; Vulkan, D.; Davies, M.P.A.; Baldwin, D.R.; Brain, K.E.; Devaraj, A.; Eisen, T.; Gosney, J.; Green, B.A.; Holemans, J.A.; et al. Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis. Lancet Reg. Health Eur. 2021, 10, 100179. [Google Scholar] [CrossRef]
- Adamek, M.; Wachuła, E.; Szabłowska-Siwik, S.; Boratyn-Nowicka, A.; Czyżewski, D. Risk factors assessment and risk prediction models in lung cancer screening candidates. Ann. Transl. Med. 2016, 4, 151. [Google Scholar] [CrossRef] [PubMed]
- Hunger, T.; Wanka-Pail, E.; Brix, G.; Griebel, J. Lung Cancer Screening with Low-Dose CT in Smokers: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 1040. [Google Scholar] [CrossRef] [PubMed]
- McRonald, F.E.; Yadegarfar, G.; Baldwin, D.R.; Devaraj, A.; Brain, K.E.; Eisen, T.; Holemans, J.A.; Ledson, M.; Screaton, N.; Rintoul, R.C.; et al. The UK Lung Screen (UKLS): Demographic profile of first 88,897 approaches provides recommendations for population screening. Cancer Prev. Res. 2014, 7, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Lifford, K.J.; Carter, B.; McRonald, F.; Yadegarfar, G.; Baldwin, D.R.; Weller, D.; Hansell, D.M.; Duffy, S.W.; Field, J.K.; et al. Barriers to uptake among high-risk individuals declining participation in lung cancer screening: A mixed methods analysis of the UK Lung Cancer Screening (UKLS) trial. BMJ Open 2015, 5, e008254. [Google Scholar] [CrossRef]
- Quaife, S.L.; Marlow, L.A.V.; McEwen, A.; Janes, S.M.; Wardle, J. Attitudes towards lung cancer screening in socioeconomically deprived and heavy smoking communities: Informing screening communication. Health Expect. 2017, 20, 563–573. [Google Scholar] [CrossRef]
- Quaife, S.L.; Waller, J.; Dickson, J.L.; Brain, K.E.; Kurtidu, C.; McCabe, J.; Hackshaw, A.; Duffy, S.W.; Janes, S.M. Psychological Targets for Lung Cancer Screening Uptake: A Prospective Longitudinal Cohort Study. J. Thorac. Oncol. 2021, 16, 2016–2028. [Google Scholar] [CrossRef]
- O’Dowd, E.L.; Lee, R.W.; Akram, A.R.; Bartlett, E.C.; Bradley, S.H.; Brain, K.; Callister, M.E.J.; Chen, Y.; Devaraj, A.; Eccles, S.R.; et al. Defining the road map to a UK national lung cancer screening programme. Lancet Oncol. 2023, 24, e207–e218. [Google Scholar] [CrossRef]
- Rampariag, R.; Chernyavskiy, I.; Al-Ajam, M.; Tsay, J.J. Controversies and challenges in lung cancer screening. Semin. Oncol. 2022, 49, 191–197. [Google Scholar] [CrossRef]
- Chabon, J.J.; Hamilton, E.G.; Kurtz, D.M.; Esfahani, M.S.; Moding, E.J.; Stehr, H.; Schroers-Martin, J.; Nabet, B.Y.; Chen, B.; Chaudhuri, A.A.; et al. Integrating genomic features for non-invasive early lung cancer detection. Nature 2020, 580, 245–251. [Google Scholar] [CrossRef]
- Liu, M.C.; Klein, E.; Hubbell, E.; Maddala, T.; Aravanis, A.M.; Beausang, J.F.; Filippova, D.; Gross, S.; Jamshidi, A.; Kurtzman, K.; et al. Plasma cell-free DNA (cfDNA) assays for early multi-cancer detection: The circulating cell-free genome atlas (CCGA) study. Ann. Oncol. 2018, 29, viii14. [Google Scholar] [CrossRef]
- Bhamani, A.; Creamer, A.; Verghese, P.; Prendecki, R.; Horst, C.; Tisi, S.; Hall, H.; Khaw, C.R.; Mullin, M.; McCabe, J.; et al. Low-dose CT for lung cancer screening in a high-risk population (SUMMIT): A prospective, longitudinal cohort study. Lancet Oncol. 2025, 26, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Nadauld, L.D.; McDonnell, C.H., 3rd; Beer, T.M.; Liu, M.C.; Klein, E.A.; Hudnut, A.; Whittington, R.A.; Taylor, B.; Oxnard, G.R.; Lipson, J.; et al. The PATHFINDER Study: Assessment of the Implementation of an Investigational Multi-Cancer Early Detection Test into Clinical Practice. Cancers 2021, 13, 3501. [Google Scholar] [CrossRef] [PubMed]
- Tsou, P.H.; Lin, Z.L.; Pan, Y.C.; Yang, H.C.; Chang, C.J.; Liang, S.K.; Wen, Y.F.; Chang, C.H.; Chang, L.Y.; Yu, K.L.; et al. Exploring Volatile Organic Compounds in Breath for High-Accuracy Prediction of Lung Cancer. Cancers 2021, 13, 1431. [Google Scholar] [CrossRef] [PubMed]
- Gasparri, R.; Santonico, M.; Valentini, C.; Sedda, G.; Borri, A.; Petrella, F.; Maisonneuve, P.; Pennazza, G.; D’Amico, A.; Di Natale, C.; et al. Volatile signature for the early diagnosis of lung cancer. J. Breath. Res. 2016, 10, 016007. [Google Scholar] [CrossRef]
- Kort, S.; Brusse-Keizer, M.; Schouwink, H.; Citgez, E.; de Jongh, F.H.; van Putten, J.W.G.; van den Borne, B.; Kastelijn, E.A.; Stolz, D.; Schuurbiers, M.; et al. Diagnosing Non-Small Cell Lung Cancer by Exhaled Breath Profiling Using an Electronic Nose: A Multicenter Validation Study. Chest 2023, 163, 697–706. [Google Scholar] [CrossRef]
- Janssens, E.; van Meerbeeck, J.P.; Lamote, K. Volatile organic compounds in human matrices as lung cancer biomarkers: A systematic review. Crit. Rev. Oncol. Hematol. 2020, 153, 103037. [Google Scholar] [CrossRef]
- Keogh, R.J.; Riches, J.C. The Use of Breath Analysis in the Management of Lung Cancer: Is It Ready for Primetime? Curr. Oncol. 2022, 29, 7355–7378. [Google Scholar] [CrossRef]
- Vadala, R.; Pattnaik, B.; Bangaru, S.; Rai, D.; Tak, J.; Kashyap, S.; Verma, U.; Yadav, G.; Dhaliwal, R.S.; Mittal, S.; et al. A review on electronic nose for diagnosis and monitoring treatment response in lung cancer. J. Breath. Res. 2023, 17, 024002. [Google Scholar] [CrossRef]
- Chaudhary, V.; Taha, B.A.; Lucky; Rustagi, S.; Khosla, A.; Papakonstantinou, P.; Bhalla, N. Nose-on-Chip Nanobiosensors for Early Detection of Lung Cancer Breath Biomarkers. ACS Sens. 2024, 9, 4469–4494. [Google Scholar] [CrossRef]
- Su, Z.; Yu, X.; He, Y.; Sha, T.; Guo, H.; Tao, Y.; Liao, L.; Zhang, Y.; Lu, G.; Lu, G.; et al. Inconsistencies in predictive models based on exhaled volatile organic compounds for distinguishing between benign pulmonary nodules and lung cancer: A systematic review. BMC Pulm. Med. 2024, 24, 551. [Google Scholar] [CrossRef]
- Fan, X.; Zhong, R.; Liang, H.; Zhong, Q.; Huang, H.; He, J.; Chen, Y.; Wang, Z.; Xie, S.; Jiang, Y.; et al. Exhaled VOC detection in lung cancer screening: A comprehensive meta-analysis. BMC Cancer 2024, 24, 775. [Google Scholar] [CrossRef] [PubMed]
- Buszewski, B.; Ligor, T.; Jezierski, T.; Wenda-Piesik, A.; Walczak, M.; Rudnicka, J. Identification of volatile lung cancer markers by gas chromatography-mass spectrometry: Comparison with discrimination by canines. Anal. Bioanal. Chem. 2012, 404, 141–146. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, M.; Jezierski, T.; Broffman, M.; Hubbard, A.; Turner, K.; Janecki, T. Diagnostic accuracy of canine scent detection in early- and late-stage lung and breast cancers. Integr. Cancer Ther. 2006, 5, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Biehl, W.; Hattesohl, A.; Jörres, R.A.; Duell, T.; Althöhn, U.; Koczulla, A.R.; Schmetzer, H. VOC pattern recognition of lung cancer: A comparative evaluation of different dog- and eNose-based strategies using different sampling materials. Acta Oncologica 2019, 58, 1216–1224. [Google Scholar] [CrossRef]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Survival Rates for Pancreatic Cancer. Available online: https://www.cancer.org/cancer/types/pancreatic-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 12 March 2025).
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Can Pancreatic Cancer Be Found Early? Available online: https://www.cancer.org/cancer/types/pancreatic-cancer/detection-diagnosis-staging/detection.html (accessed on 12 March 2025).
- Sawhney, M.S.; Calderwood, A.H.; Thosani, N.C.; Rebbeck, T.R.; Wani, S.; Canto, M.I.; Fishman, D.S.; Golan, T.; Hidalgo, M.; Kwon, R.S.; et al. ASGE guideline on screening for pancreatic cancer in individuals with genetic susceptibility: Summary and recommendations. Gastrointest. Endosc. 2022, 95, 817–826. [Google Scholar] [CrossRef]
- Laish, I.; Schechter, M.; Dancour, A.; Lieberman, S.; Levi, Z.; Goldberg, Y.; Kedar, I.; Hasnis, E.; Half, E.; Levi, G.R.; et al. The benefit of pancreatic cancer surveillance in carriers of germline BRCA1/2 pathogenic variants. Cancer 2024, 130, 256–266. [Google Scholar] [CrossRef]
- Katona, B.W.; Lubinski, J.; Pal, T.; Huzarski, T.; Foulkes, W.D.; Moller, P.; Eisen, A.; Randall Armel, S.; Neuhausen, S.L.; Raj, R.; et al. The incidence of pancreatic cancer in women with a BRCA1 or BRCA2 mutation. Cancer 2025, 131, e35666. [Google Scholar] [CrossRef]
- Wang, K.; Wang, X.; Pan, Q.; Zhao, B. Liquid biopsy techniques and pancreatic cancer: Diagnosis, monitoring, and evaluation. Mol. Cancer 2023, 22, 167. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Zhu, Z.; Roy, S.; Jun, E.; Han, H.; Munoz, R.M.; Nishiwada, S.; Sharma, G.; Cridebring, D.; Zenhausern, F.; et al. An Exosome-based Transcriptomic Signature for Noninvasive, Early Detection of Patients with Pancreatic Ductal Adenocarcinoma: A Multicenter Cohort Study. Gastroenterology 2022, 163, 1252–1266.e1252. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Li, T.; Lin, C.; Zhao, B.; Li, Z.; Zhao, Y.; Wang, W. The systematic role of pancreatic cancer exosomes: Distant communication, liquid biopsy and future therapy. Cancer Cell Int. 2024, 24, 264. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Hu, X.; Liu, T. Development of liquid biopsy in detection and screening of pancreatic cancer. Front. Oncol. 2024, 14, 1415260. [Google Scholar] [CrossRef]
- Martinez-Moral, M.P.; Tena, M.T.; Martin-Carnicero, A.; Martinez, A. Highly sensitive serum volatolomic biomarkers for pancreatic cancer diagnosis. Clin. Chim. Acta 2024, 557, 117895. [Google Scholar] [CrossRef]
- Daulton, E.; Wicaksono, A.N.; Tiele, A.; Kocher, H.M.; Debernardi, S.; Crnogorac-Jurcevic, T.; Covington, J.A. Volatile organic compounds (VOCs) for the non-invasive detection of pancreatic cancer from urine. Talanta 2021, 221, 121604. [Google Scholar] [CrossRef]
- Nissinen, S.I.; Roine, A.; Hokkinen, L.; Karjalainen, M.; Venalainen, M.; Helminen, H.; Niemi, R.; Lehtimaki, T.; Rantanen, T.; Oksala, N. Detection of Pancreatic Cancer by Urine Volatile Organic Compound Analysis. Anticancer Res. 2019, 39, 73–79. [Google Scholar] [CrossRef]
- Markar, S.R.; Brodie, B.; Chin, S.T.; Romano, A.; Spalding, D.; Hanna, G.B. Profile of exhaled-breath volatile organic compounds to diagnose pancreatic cancer. Br. J. Surg. 2018, 105, 1493–1500. [Google Scholar] [CrossRef]
- Princivalle, A.; Monasta, L.; Butturini, G.; Bassi, C.; Perbellini, L. Pancreatic ductal adenocarcinoma can be detected by analysis of volatile organic compounds (VOCs) in alveolar air. BMC Cancer 2018, 18, 529. [Google Scholar] [CrossRef]
- Arasaradnam, R.P.; Wicaksono, A.; O’Brien, H.; Kocher, H.M.; Covington, J.A.; Crnogorac-Jurcevic, T. Noninvasive Diagnosis of Pancreatic Cancer Through Detection of Volatile Organic Compounds in Urine. Gastroenterology 2018, 154, 485–487.e481. [Google Scholar] [CrossRef]
- All Cancer Sites Combined: Recent Trends in SEER Age-Adjusted Incidence Rates, 2000–2021. Available online: https://seer.cancer.gov/statistics-network/explorer/. (accessed on 12 March 2025).
- Jacobs, I.; Stabile, I.; Bridges, J.; Kemsley, P.; Reynolds, C.; Grudzinskas, J.; Oram, D. Multimodal approach to screening for ovarian cancer. Lancet 1988, 1, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Yamada, Y.; Sado, T.; Sakata, M.; Yoshida, S.; Kawaguchi, R.; Kanayama, S.; Shigetomi, H.; Haruta, S.; Tsuji, Y.; et al. A randomized study of screening for ovarian cancer: A multicenter study in Japan. Int. J. Gynecol. Cancer 2008, 18, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Menon, U.; Gentry-Maharaj, A.; Burnell, M.; Singh, N.; Ryan, A.; Karpinskyj, C.; Carlino, G.; Taylor, J.; Massingham, S.K.; Raikou, M.; et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomised controlled trial. Lancet 2021, 397, 2182–2193. [Google Scholar] [CrossRef] [PubMed]
- Buys, S.S.; Partridge, E.; Black, A.; Johnson, C.C.; Lamerato, L.; Isaacs, C.; Reding, D.J.; Greenlee, R.T.; Yokochi, L.A.; Kessel, B.; et al. Effect of screening on ovarian cancer mortality: The Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA 2011, 305, 2295–2303. [Google Scholar] [CrossRef]
- Nagarkar, R.; Gopichand, M.; Pal, S.K.; Gupta, A.; Saquib, N.M.; Sagar, G.; Rao, K.V.S.; Siddiqui, Z.; Longkumer, I. The High Sensitivity of the Multi-Cancer Detection Test ONCOVERYX-F Offers a Promising Platform for Ovarian Cancer Screening. Int. J. Womens Health 2024, 16, 1–7. [Google Scholar] [CrossRef]
- Margoni, A.; Gargalionis, A.N.; Papavassiliou, A.G. CA-125:CA72-4 ratio—Towards a promising cost-effective tool in ovarian cancer diagnosis and monitoring of post-menopausal women under hormone treatment. J. Ovarian Res. 2024, 17, 164. [Google Scholar] [CrossRef]
- Davenport, C.; Rai, N.; Sharma, P.; Deeks, J.J.; Berhane, S.; Mallett, S.; Saha, P.; Champaneria, R.; Bayliss, S.E.; Snell, K.I.; et al. Menopausal status, ultrasound and biomarker tests in combination for the diagnosis of ovarian cancer in symptomatic women. Cochrane Database Syst. Rev. 2022, 7, CD011964. [Google Scholar] [CrossRef]
- Sideris, M.; Menon, U.; Manchanda, R. Screening and prevention of ovarian cancer. Med. J. Aust. 2024, 220, 264–274. [Google Scholar] [CrossRef]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Screening for Ovarian Cancer: US Preventive Services Task Force Recommendation Statement. Jama 2018, 319, 588–594. [Google Scholar] [CrossRef]
- Eleje, G.U.; Eke, A.C.; Ezebialu, I.U.; Ikechebelu, J.I.; Ugwu, E.O.; Okonkwo, O.O. Risk-reducing bilateral salpingo-oophorectomy in women with BRCA1 or BRCA2 mutations. Cochrane Database Syst. Rev. 2018, 8, CD012464. [Google Scholar] [CrossRef]
- Hong, M.K.; Ding, D.C. Early Diagnosis of Ovarian Cancer: A Comprehensive Review of the Advances, Challenges, and Future Directions. Diagnostics 2025, 15, 406. [Google Scholar] [CrossRef] [PubMed]
- Raspagliesi, F.; Bogani, G.; Benedetti, S.; Grassi, S.; Ferla, S.; Buratti, S. Detection of Ovarian Cancer through Exhaled Breath by Electronic Nose: A Prospective Study. Cancers 2020, 12, 2408. [Google Scholar] [CrossRef] [PubMed]
- Horvath, G.; Jarverud, G.A.; Jarverud, S.; Horvath, I. Human ovarian carcinomas detected by specific odor. Integr. Cancer Ther. 2008, 7, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Horvath, G.; Andersson, H.; Nemes, S. Cancer odor in the blood of ovarian cancer patients: A retrospective study of detection by dogs during treatment, 3 and 6 months afterward. BMC Cancer 2013, 13, 396. [Google Scholar] [CrossRef]
- Kybert, N.; Prigge, K.; Otto, C.; Ramirez, L.; Joffe, E.; Tanyi, J.; Piltz-Seymour, J.; Johnson, A.T.C.; Preti, G. Exploring ovarian cancer screening using a combined sensor approach: A pilot study. AIP Adv. 2020, 10, 035213. [Google Scholar] [CrossRef]
- Klein, E.A.; Richards, D.; Cohn, A.; Tummala, M.; Lapham, R.; Cosgrove, D.; Chung, G.; Clement, J.; Gao, J.; Hunkapiller, N.; et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Ann. Oncol. 2021, 32, 1167–1177. [Google Scholar] [CrossRef]
- Budnik, B.; Amirkhani, H.; Forouzanfar, M.H.; Afshin, A. Novel proteomics-based plasma test for early detection of multiple cancers in the general population. BMJ Oncol. 2024, 3, e000073. [Google Scholar] [CrossRef]
- Milner, D.A.; Lennerz, J.K. Technology and Future of Multi-Cancer Early Detection. Life 2024, 14, 833. [Google Scholar] [CrossRef]
- Lennon, A.M.; Buchanan, A.H.; Kinde, I.; Warren, A.; Honushefsky, A.; Cohain, A.T.; Ledbetter, D.H.; Sanfilippo, F.; Sheridan, K.; Rosica, D.; et al. Feasibility of blood testing combined with PET-CT to screen for cancer and guide intervention. Science 2020, 369, eabb9601. [Google Scholar] [CrossRef]

{kind=link}
| Study Name [References] | Cancer Type | Technology | Sample Size | Key Results |
|---|---|---|---|---|
| Schrag et al. [31] PATHFINDER | Multicancer | Liquid biopsy (Galleri methylation assay) | 6621 | Specificity: 99.1% Overall sensitivity: 66.3% Lower sensitivity for early stages |
| Cohen et al. [88] CancerSEEK | Multicancer | Liquid biopsy (ctDNA + protein markers) | 1005 | Specificity: ~99% Sensitivity across cancers: ~60–98%; |
| Liu et al. [93] | Breast cancer | VOC breath (HPPI-TOF-MS) | 5047 | Sensitivity across breast cancer stages: 85–97% High diagnostic accuracy |
| Kort et al. [117] | Lung cancer | VOC breath (Electronic nose) | 575 | Specificity: 49% Sensitivity: 95% Negative predictive value: 94% |
| Arasaradnam et al. [144] | Pancreatic cancer | VOC urine (Ion mobility spectrometry) | 162 | Specificity: 83% Sensitivity: 91% |
| Medina et al. [81] DELFI-Pro | Ovarian cancer | Liquid biopsy (cfDNA fragmentomics + protein markers) | 591 | Specificity: >99% Sensitivity: 72% (stage I), 69% (stage II), 87% (stage III), 100% (stage IV) |
| Half et al. [72] The Rainbow Study | Multicancer | VOC breath (Canine detection + AI) | 1386 | Specificity and sensitivity across cancers: 94%; ~82% for cancers that the system was not trained to detect |
| Cancer Detection Parameter | Liquid Biopsy Alone | Canine VOC Detection Alone | Integrated Approach |
|---|---|---|---|
| Early-stage Detection | Limited sensitivity for early-stage disease (24.2%) compared to later-stage (95.3%) | High sensitivity for early-stage cancers (94.8%) | Combined approach to capturing tumors missed by either method alone |
| Multi-cancer Detection | Effective for some cancer types, but variable performance across others | Can detect trained cancer types with high sensitivity (93.9%) and even untrained cancer types (81.8%) | Complementary detection across a wider range of cancer types |
| Specificity | High specificity (98.4–99.5%) | High specificity (94.3%) | Combined specificity could reduce false positives |
| Sample Requirements | Blood samples for cfDNA, ctDNA analysis | Breath, urine, or other bodily emissions | Multiple sample types enable cross-validation of results |
| Diagnostic Information | Provides genetic/molecular tumor profile for potential treatment guidance | Indicates presence of cancer but limited molecular details | Complete picture: detection plus molecular characterization |
| Integration with AI | AI algorithms enhance detection of subtle molecular patterns | Machine learning improves canine detection accuracy | AI platform integrating both data sources for superior pattern recognition |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madar, S.; Amor, R.E.; Furman-Assaf, S.; Friedman, E. Innovative Approaches to Early Detection of Cancer-Transforming Screening for Breast, Lung, and Hard-to-Screen Cancers. Cancers 2025, 17, 1867. https://doi.org/10.3390/cancers17111867
Madar S, Amor RE, Furman-Assaf S, Friedman E. Innovative Approaches to Early Detection of Cancer-Transforming Screening for Breast, Lung, and Hard-to-Screen Cancers. Cancers. 2025; 17(11):1867. https://doi.org/10.3390/cancers17111867
Chicago/Turabian StyleMadar, Shlomi, Reef Einoch Amor, Sharon Furman-Assaf, and Eitan Friedman. 2025. "Innovative Approaches to Early Detection of Cancer-Transforming Screening for Breast, Lung, and Hard-to-Screen Cancers" Cancers 17, no. 11: 1867. https://doi.org/10.3390/cancers17111867
APA StyleMadar, S., Amor, R. E., Furman-Assaf, S., & Friedman, E. (2025). Innovative Approaches to Early Detection of Cancer-Transforming Screening for Breast, Lung, and Hard-to-Screen Cancers. Cancers, 17(11), 1867. https://doi.org/10.3390/cancers17111867