
Oropharyngeal and Oral Cancer in Lung Cancer Patients: Do They Present a Worse Prognosis than Isolated Lung Cancer Patients?

 , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
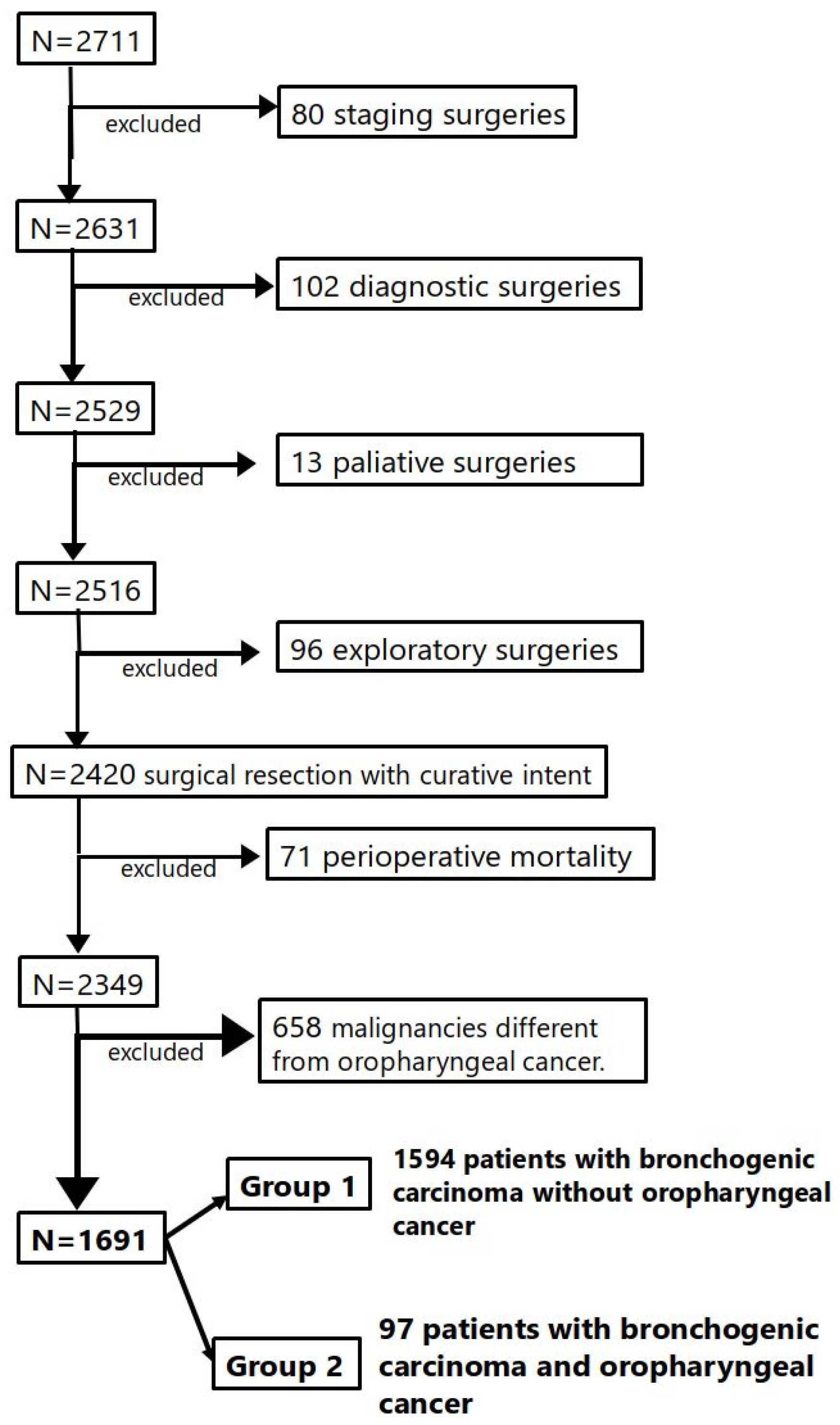
- 1.
- Patients who underwent surgery consecutively with the diagnosis of BC in HCSC.
- 2.
- Patients who underwent surgery within the specified period: 1989 to 2024.
- 3.
- Patients with BC with an additional diagnosis of OAOC treated with radical purpose.
- 4.
- Patients who underwent surgical treatment of their BC with curative intention.
- 1.
- Patients with BC who underwent staging surgery.
- 2.
- Patients with BC who underwent diagnostic surgery (biopsy).
- 3.
- Patients with BC undergoing surgery with palliative intent.
- 4.
- Patients with BC who underwent exploratory thoracotomy (unresectable tumor).
- 5.
- Patients with BC who experienced postoperative mortality.
- 6.
- Patients with BC diagnosed with another malignancy that was different from oropharyngeal cancer.
3. Results
- −
- Group 1: 1594 patients with isolated BC.
- −
- Group 2: 97 patients with BC and previous oropharyngeal cancer.
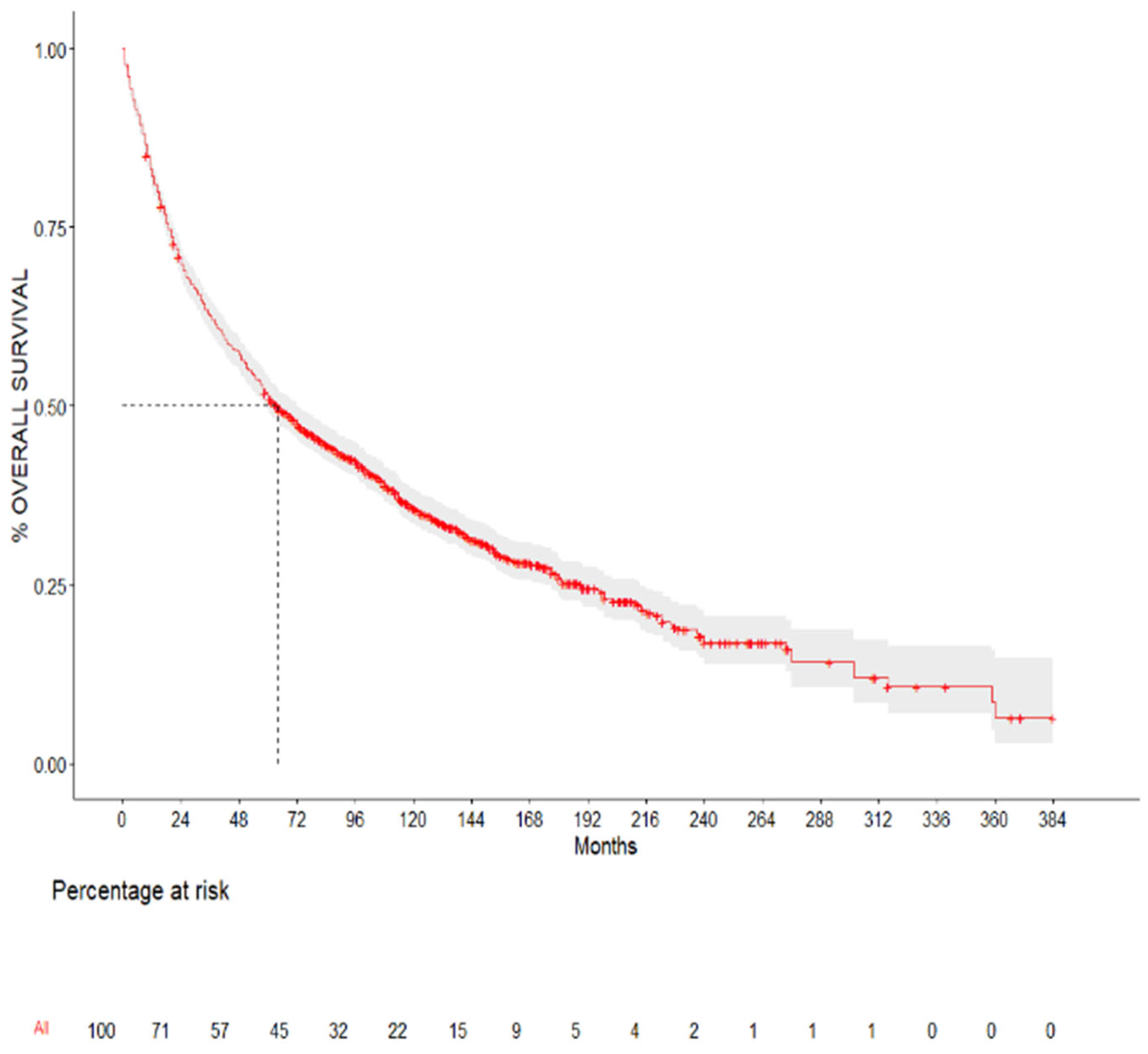
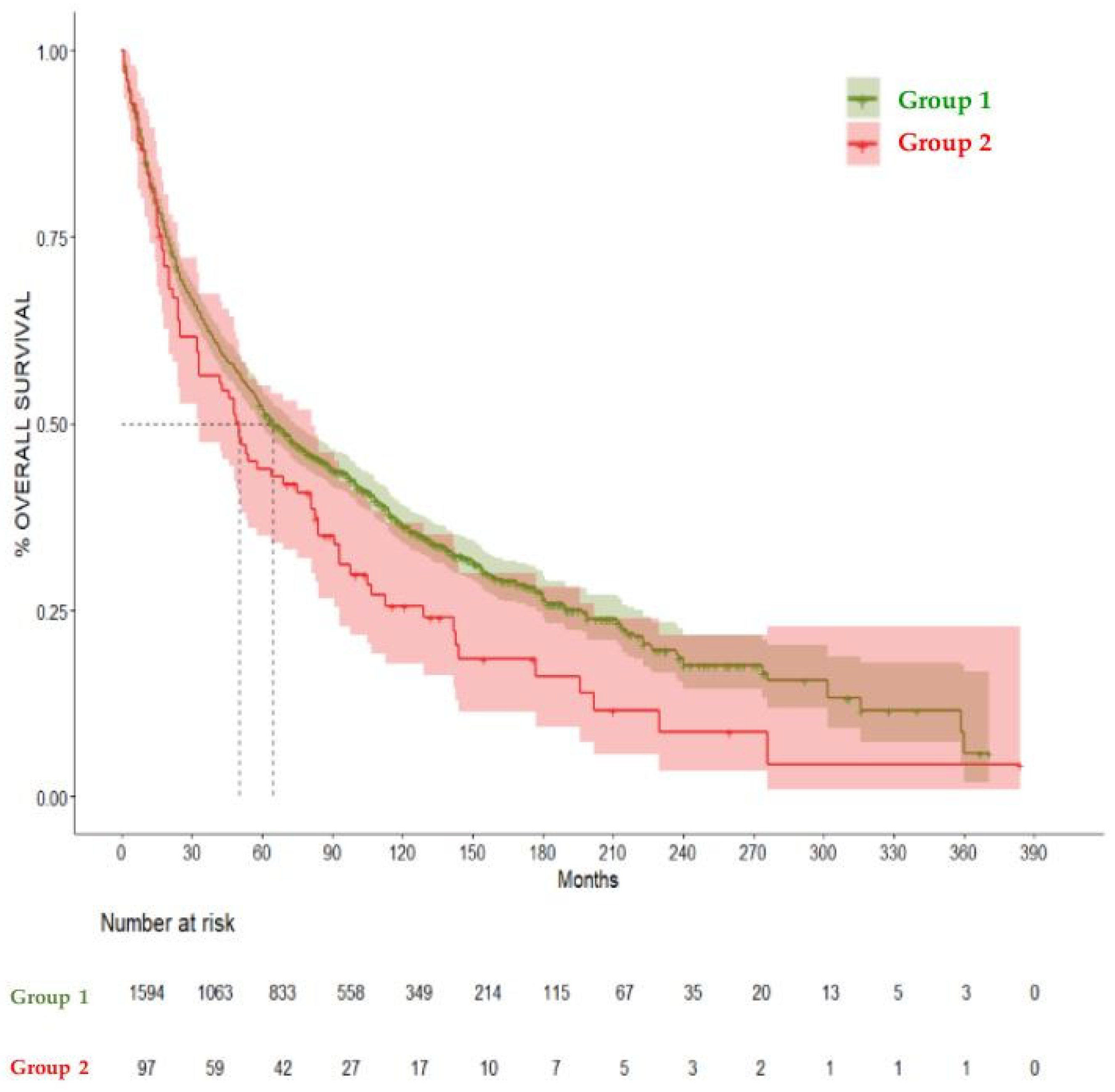
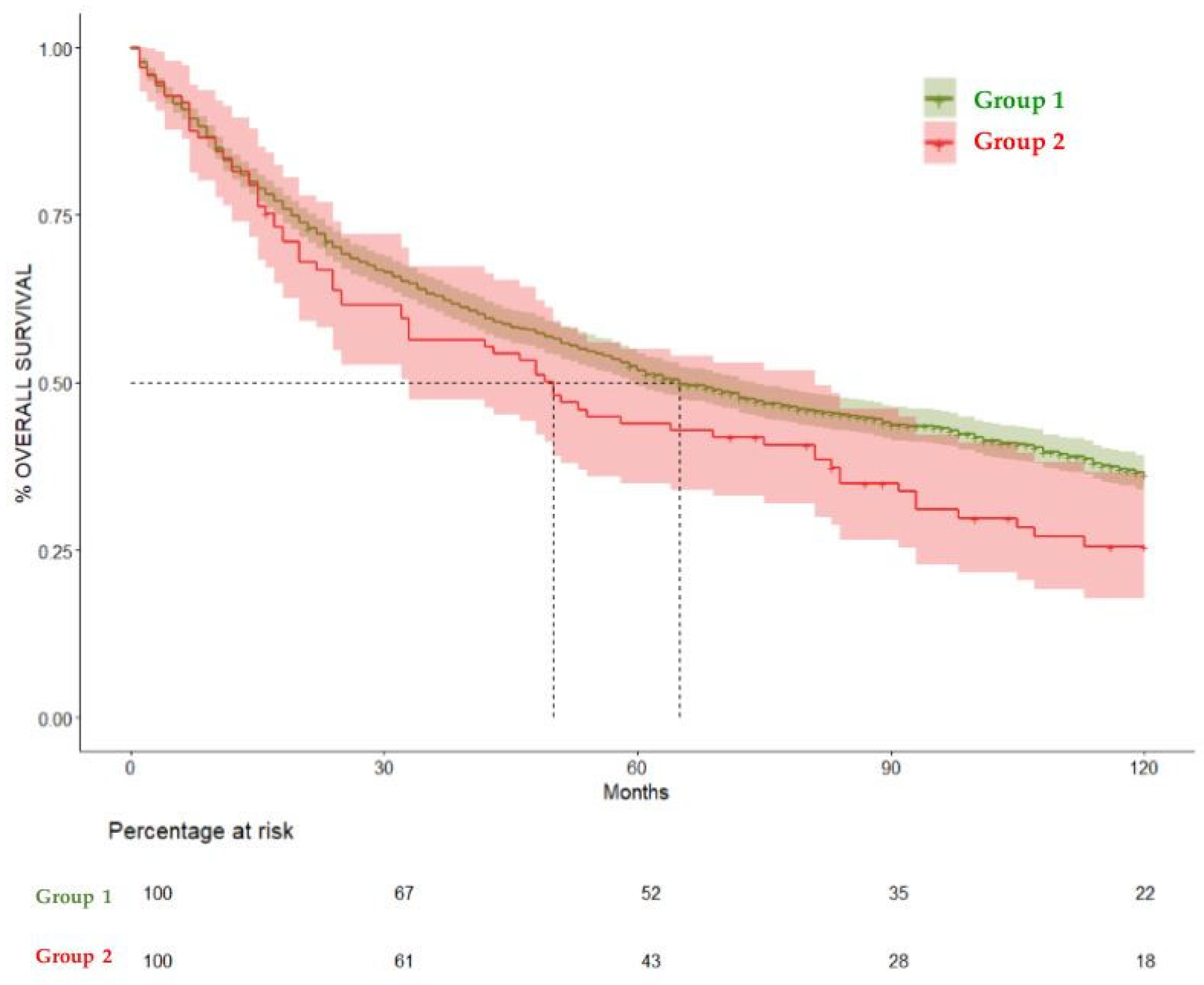
Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 25 February 2021).
- World Health Organization Fact Sheets Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 30 March 2025).
- Chuang, S.C.; Scelo, G.; Tonita, J.M.; Tamaro, S.; Jonasson, J.G.; Kliewer, E.V.; Hemminki, K.; Weiderpass, E.; Pukkala, E.; Tracey, E.; et al. Risk of second primary cancer among patients with head and neck cancers: A pooled analysis of 13 cancer registries. Int. J. Cancer 2008, 123, 2390–2396. [Google Scholar] [CrossRef] [PubMed]
- Donin, N.M.; Kwan, L.; Lenis, A.T.; Drakaki, A.; Chamie, K. Second primary lung cancer in United States cancer survivors, 1992–2008. Cancer Causes Control 2019, 30, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Takatsu, F.; Suzawa, K.; Okazaki, M.; Shien, K.; Yamamoto, H.; Watanabe, M.; Hayama, M.; Ueno, T.; Sugimoto, R.; Maki, Y.; et al. Clinical Features of Patients With Second Primary Lung Cancer After Head and Neck Cancer. Ann. Thorac. Surg. 2022, 117, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Louiea, A.V.; Damhuis, R.A.; Haasbeeka, C.J.; Warner, A.; Rodind, D.; Slotmana, B.J. Treatment and survival of second primary early-stage lung cancer, following treatment of head and neck cancer in the Netherlands. Lung Cancer 2016, 94, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Worldwide Cancer Data|World Cancer Research Fund. Available online: https://www.wcrf.org/preventing-cancer/cancer-statistics/worldwide-cancer-data/#global-cancer-incidence-both-sexes (accessed on 30 March 2025).
- Lung Cancer Statistics|World Cancer Research Fund. Available online: https://www.wcrf.org/dietandcancer/cancer-trends/lung-cancer-statistics (accessed on 30 March 2025).
- Oliver, A.L. Lung Cancer: Epidemiology and Screening. Surg. Clin. N. Am. 2022, 102, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Mouth and Oral Cancer Statistics|World Cancer Research Fund. Available online: https://www.wcrf.org/preventing-cancer/cancer-statistics/mouth-and-oral-cancer-statistics/ (accessed on 30 March 2025).
- Vogt, A.; Schmid, S.; Heinimann, K.; Frick, H.; Herrmann, C.; Cerny, T.; Omlin, A. Multiple primary tumours: Challenges and approaches, a review. ESMO Open 2017, 2, e000172. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Li, X.; Wang, M.; Shen, J.; Sisti, G.; He, Z.; Huang, J.; Li, Y.M.; Wu, A. on behalf of Multidisciplinary Oncology Research Collaborative Group (MORCG). Second primary malignancies among cancer patients. Ann. Transl. Med. 2020, 8, 638. [Google Scholar] [CrossRef] [PubMed]
- Rosso, S.; De Angelis, R.; Ciccolallo, L.; Carrani, E.; Soerjomataram, I.; Grande, E.; Zigon, G.; Brenner, H. The EUROCARE Working Group. Multiple tumours in survival estimates. Eur. J. Cancer 2009, 45, 1080–1094. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zeng, M.; Ju, X.; Lin, A.; Zhou, C.; Shen, J. Correlation between second and first primary cancer: Systematic review and meta-analysis of 9 million cancer patients. Br. J. Surg. 2024, 111, znad377. [Google Scholar] [CrossRef] [PubMed]
- RECurtis New Malignancies Among Cancer Survivors: SEERCancer Registries; U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Washington, DC, USA, 2006; pp. 1973–2000.
- Boakye, E.A.; Buchanan, P.; Hinyard, L.; Osazuwa-Peters, N.; Simpson, M.C.; Schootman, M.; Piccirillo, J.F. Trends in the risk and burden of second primary malignancy among survivors of smoking-related cancers in the United States. Int. J. Cancer 2019, 145, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Singnurkar, A.; Swaminath, A.; Metser, U.; Langer, D.L.; Darling, G.E.; Pond, G.R. The impact of synchronous malignancies on survival in patients with early stage curable non-small-cell lung cancer. Cancer Treat. Res. Commun. 2020, 25, 100246. [Google Scholar] [CrossRef] [PubMed]
- Tanjak, P.; Suktitipat, B.; Vorasan, N.; Juengwiwattanakitti, P.; Thiengtrong, B.; Songjang, C.; Therasakvichya, S.; Laiteerapong, S.; Chinswangwatanakul, V. Risks and cancer associations of metachronous and synchronous multiple primary cancers: A 25-year retrospective study. BMC Cancer 2021, 21, 1045. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Massa, S.; Mazul, A.L.; Kallogjeri, D.; Yaeger, L.; Jackson, R.S.; Zevallos, J.; Pipkorn, P. The association of smoking and outcomes in HPV-positive oropharyngeal cancer: A systematic review. Am. J. Otolaryngol. 2020, 41, 102592. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; Gibson, T.; Sampson, J.; Albanes, D.; Andreotti, G.; Freeman, L.B.; de Gonzalez, A.B.; Caporaso, N.; Curtis, R.E.; Elena, J.; et al. Cigarette Smoking Prior to First Cancer and Risk of Second Smoking-Associated Cancers Among Survivors of Bladder, Kidney, Head and Neck, and Stage I Lung Cancers. J. Clin. Oncol. 2014, 32, 3989–3995. [Google Scholar] [CrossRef] [PubMed]
- Duchateau, C.S.; Stokkel, M.P. Second primary tumors involving non-small cell lung cancer: Prevalence and its influence on survival. Chest 2005, 127, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Zhong, W.Z.; Niu, F.Y.; Zhao, N.; Yang, J.J.; Yan, H.H.; Wu, Y.-L. Multiple primary malignancies involving lung cancer. BMC Cancer 2015, 15, 696. [Google Scholar] [CrossRef] [PubMed]
- Provencio, M.; Romero, N.; Tabernero, J.; Vera, R.; Baz, D.V.; Arraiza, A.; Camps, C.; Felip, E.; Garrido, P.; Gaspar, B.; et al. Future care for long-term cancer survivors: Towards a new model. Clin. Transl. Oncol. 2022, 24, 350–362. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.S.; Chen, M.F.; Huang, Y.K.; Liu, H.P.; Tsai, Y.H. Clinical outcome in lung cancer with a second malignancy: The time sequence matters. Medicine 2016, 95, e5203. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Hyun, N.; Leach, C.R.; Yabroff, K.R.; Jema, A. Association of First Primary Cancer With Risk of Subsequent Primary Cancer Among Survivors of Adult-Onset Cancers in the United States. JAMA 2020, 324, 2521–2535. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 1691) | Group 1 (N = 1594) | Group 2 (N = 97) | p Value | ||
|---|---|---|---|---|---|
| Mean Age (SD) | 64.4 (9.78) | 64.55 (9.91) | 66.23 (7.23) | 0.16 | |
| Gender (%) | Male | 1339 (79.2%) | 1248 (78.3%) | 91 (93.8%) | 0.001 |
| Female | 352 (20.8%) | 346 (21.7%) | 6 (6.2%) | ||
| Lung cancer staging | I | 838 (51.2%) | 781 (50.6%) | 57 (61.3%) | 0.14 |
| II | 345 (21.1%) | 336 (21.7%) | 9 (9.7%) | ||
| III | 415 (25.3%) | 389 (25.2%) | 26 (28.0%) | ||
| IV | 40 (2.4%) | 39 (2.5%) | 1 (1.1%) | ||
| Smoking habit (%) | No | 320 (19.9%) | 314 (20.8%) | 6 (6.2%) | <0.001 |
| 20 PY | 120 (7.5%) | 117 (7.7%) | 3 (3.1%) | ||
| 40 PY | 624 (38.8%) | 589 (39.0%) | 35 (36.1%) | ||
| Ex-smoker | 544 (33.8%) | 491 (32.5%) | 53 (54.6%) | ||
| Mean follow-up [IQR] | 63 [19–111] | 63.5 [19–111.75] | 49 [16–93] | 0.4 | |
| Exitus (%) | 1139 (67.4%) | 1061 (66.6%) | 78 (80.4%) | 0.02 |
| Months | N at Risk | N Event | Survival | Lower 95% CI | Upper 95% CI |
|---|---|---|---|---|---|
| 12 | 1407 | 146 | 82.1% | 80.3% | 84% |
| 24 | 1194 | 208 | 69.8% | 67.7% | 72% |
| 60 | 875 | 69 | 51.4% | 49% | 53.8% |
| 120 | 366 | 34 | 35.7% | 33.4% | 38.3% |
| Months | %Survival Group 1 (95% CI) | %Survival Group 2 (95% CI) | p Value |
|---|---|---|---|
| 12 | 82.2% (80.3–84.1) | 81.44% (74.06–89.6) | 0.1 |
| 24 | 70.2% (68–72.5) | 63.76% (54.85–74.1) | 0.1 |
| 60 | 51.8% (49.4–54.3) | 43.9% (35.02–55) | 0.141 |
| 120 | 36.4% (33.9–39) | 25.54% (17.78–36.7) | 0.0466 |
| Months | DFS Group 1 (95% CI) | DFS Group 2 (95% CI) | p Value |
|---|---|---|---|
| 12 | 77.2% (75.1–79.4%) | 73.7% (65.2–83.3%) | 0.06 |
| 24 | 66.6% (64.2–69.1%) | 62% (52.6–73%) | |
| 60 | 54.8% (52.2–57.4%) | 47.5% (37.8–59.6%) | |
| 120 | 46.5% (43.8–49.4%) | 37.7% (28–50.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noushzady, F.F.; Álvarez, S.H.; Gastardi, J.C.; Vara-Ameigeiras, E.M.; Amorós, C.M.; Serrano-García, I.; Trancho, F.H.; Sarceda, J.R.J.; Martínez, A.M.G. Oropharyngeal and Oral Cancer in Lung Cancer Patients: Do They Present a Worse Prognosis than Isolated Lung Cancer Patients? Cancers 2025, 17, 1850. https://doi.org/10.3390/cancers17111850
Noushzady FF, Álvarez SH, Gastardi JC, Vara-Ameigeiras EM, Amorós CM, Serrano-García I, Trancho FH, Sarceda JRJ, Martínez AMG. Oropharyngeal and Oral Cancer in Lung Cancer Patients: Do They Present a Worse Prognosis than Isolated Lung Cancer Patients? Cancers. 2025; 17(11):1850. https://doi.org/10.3390/cancers17111850
Chicago/Turabian StyleNoushzady, Farzin Falahat, Sonia Herrero Álvarez, Joaquín Calatayud Gastardi, Elena María Vara-Ameigeiras, Carlota Mazo Amorós, Irene Serrano-García, Florentino Hernando Trancho, José Ramón Jarabo Sarceda, and Ana Maria Gómez Martínez. 2025. "Oropharyngeal and Oral Cancer in Lung Cancer Patients: Do They Present a Worse Prognosis than Isolated Lung Cancer Patients?" Cancers 17, no. 11: 1850. https://doi.org/10.3390/cancers17111850
APA StyleNoushzady, F. F., Álvarez, S. H., Gastardi, J. C., Vara-Ameigeiras, E. M., Amorós, C. M., Serrano-García, I., Trancho, F. H., Sarceda, J. R. J., & Martínez, A. M. G. (2025). Oropharyngeal and Oral Cancer in Lung Cancer Patients: Do They Present a Worse Prognosis than Isolated Lung Cancer Patients? Cancers, 17(11), 1850. https://doi.org/10.3390/cancers17111850