
Human Epidermal Growth Factor Receptor 2-Positive (HER2+) Early Breast Cancer Treatment and Outcomes by Risk of Recurrence: A Retrospective US Electronic Health Records Study

 , , and
, , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
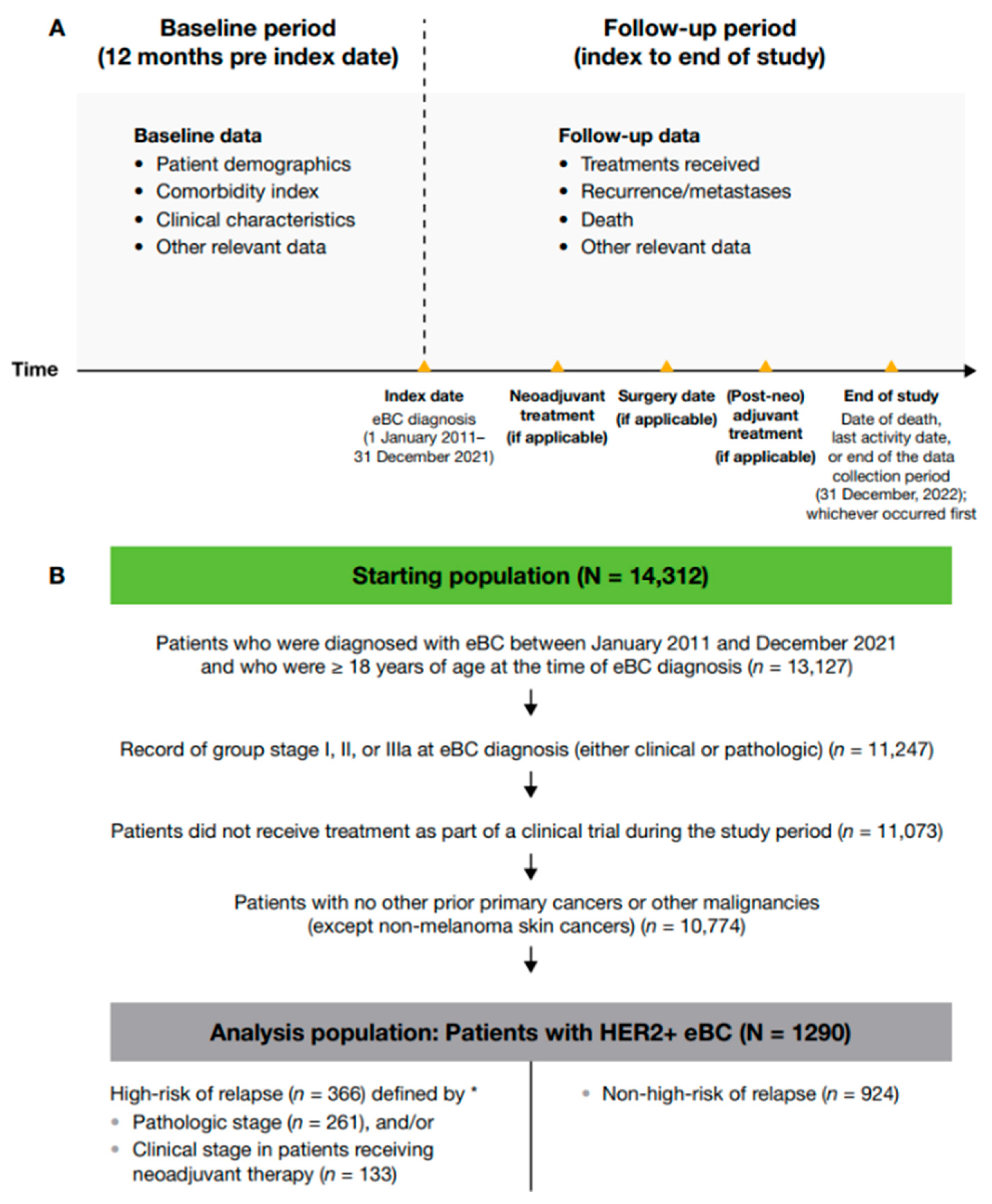
2.2. Study Design
2.3. Study Sample
2.4. Tumor Staging
2.5. Objectives
2.6. Statistical Methods
3. Results
3.1. Patient Population
3.2. Patient Demographics and Baseline Disease Characteristics
3.3. Treatment Patterns in Patients with HER2+ eBC
3.4. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (N = 1290) | High-Risk * (n = 457) | Non-High-Risk (n = 833) | |
|---|---|---|---|
| Age at diagnosis | |||
| Mean (SD) | 57.6 (12.8) | 55.3 (13.3) | 58.9 (12.3) |
| Median [min, max] | 58.0 [23.0, 85.0] | 55.0 [23.0, 84.0] | 59.0 [23.0, 85.0] |
| Sex, n (%) † | |||
| Female | 1281 (99.3) | ≥ 450 (≥ 98) | 827 (99.3) |
| Male | 9 (0.7) | ≤ 5 (≤ 1) | 6 (0.7) |
| Race, n (%) | |||
| White | 817 (63.3) | 282 (61.7) | 535 (64.2) |
| Black | 133 (10.3) | 44 (9.6) | 89 (10.7) |
| Asian | 51 (4.0) | 15 (3.3) | 36 (4.3) |
| Other | 178 (13.8) | 76 (16.6) | 102 (12.2) |
| Missing | 111 (8.6) | 40 (8.8) | 71 (8.5) |
| Ethnicity, n (%) | |||
| Hispanic/Latino | 104 (8.1) | 45 (9.8) | 59 (7.1) |
| Non-Hispanic/Non-Latino | 982 (76.1) | 344 (75.3) | 638 (76.6) |
| Missing | 204 (15.8) | 68 (14.9) | 136 (16.3) |
| BMI at diagnosis, n (%) ‡ | |||
| Normal (18.5–< 25) | 49 (3.8) | 16 (3.5) | 33 (4.0) |
| Overweight (25–< 30) | 55 (4.3) | 17 (3.7) | 38 (4.6) |
| Obese (≥30) | 66 (5.1) | 28 (6.1) | 38 (4.6) |
| Missing | 1119 (86.7) | 396 (86.7) | 723 (86.8) |
| Underweight (< 18.5) | 1 (0.1) | 0 (0.0) | 1 (0.1) |
| Region, n (%) | |||
| South | 500 (38.8) | 180 (39.4) | 320 (38.4) |
| Northeast | 170 (13.2) | 56 (12.3) | 114 (13.7) |
| West | 171 (13.3) | 61 (13.3) | 110 (13.2) |
| Midwest | 165 (12.8) | 55 (12.0) | 110 (13.2) |
| Missing | 284 (22.0) | 105 (23.0) | 179 (21.5) |
| Menopausal status, n (%) | |||
| Premenopausal | 340 (26.4) | 153 (33.5) | 187 (22.4) |
| Postmenopausal | 829 (64.3) | 263 (57.5) | 566 (67.9) |
| Perimenopausal | 33 (2.6) | 14 (3.1) | 19 (2.3) |
| Missing/not applicable/male | 88 (6.8) | 27 (5.9) | 61 (7.3) |
| High-Risk * n = 457 | Non-High-Risk n = 833 | |
|---|---|---|
| Treatment pathway after diagnosis, n (%) | ||
| No treatment | 1 (0.2) | 31 (3.7) |
| Neoadjuvant treatment only | 0 | 0 |
| Neoadjuvant treatment followed by surgery only | 3 (0.7) | 1 (0.1) |
| Surgery only | 41 (9.0) | 162 (19.4) |
| Surgery followed by adjuvant treatment | 161 (35.2) | 547 (65.7) |
| Neoadjuvant treatment followed by surgery and post-neoadjuvant treatment | 251 (54.9) | 92 (11.0) |
| Type of surgery, n (%) | ||
| Unilateral lumpectomy | 170 (37.2) | 455 (54.6) |
| Unilateral mastectomy | 147 (32.2) | 147 (17.6) |
| High-Risk * | Non-High-Risk † | |||||
|---|---|---|---|---|---|---|
| 2011–2013 (n = 20) | 2014–2017 (n = 69) | 2018–2021 (n = 74) | 2011–2013 (n = 10) | 2014–2017 (n = 66) | 2018–2021 (n = 108) | |
| Patients receiving neoadjuvant treatment, n (%) ‡ | ||||||
| Anastrozole | 0 | 1 (1.4) | 1 (1.4) | 1 (10.0) | 2 (3.0) | 3 (2.8) |
| Carboplatin | 9 (45.0) | 59 (85.5) | 62 (83.8) | 4 (40.0) | 48 (72.7) | 85 (78.7) |
| Cisplatin | 1 (5.0) | 0 | 0 | 0 | 0 | 0 |
| Cyclophosphamide | 9 (45.0) | 4 (5.8) | 7 (9.5) | 4 (40.0) | 4 (6.1) | 7 (6.5) |
| Docetaxel | 10 (50.0) | 65 (94.2) | 63 (85.1) | 6 (60.0) | 56 (84.8) | 87 (80.6) |
| Doxorubicin | 9 (45.0) | 3 (4.3) | 6 (8.1) | 4 (40.0) | 3 (4.5) | 7 (6.5) |
| Etoposide | 1 (5.0) | 0 | 0 | 0 | 0 | 0 |
| Exemestane | 0 | 0 | 1 (1.4) | 0 | 0 | 0 |
| Fulvestrant | 0 | 1 (1.4) | 1 (1.4) | 0 | 0 | 0 |
| Goserelin | 0 | 0 | 6 (8.1) | 0 | 0 | 1 (0.9) |
| Letrozole | 0 | 1 (1.4) | 1 (1.4) | 0 | 0 | 0 |
| Leuprolide | 0 | 1 (1.4) | 2 (2.7) | 0 | 0 | 3 (2.8) |
| Mesna | 0 | 0 | 1 (1.4) | 0 | 0 | 0 |
| Paclitaxel | 10 (50.0) | 6 (8.7) | 11 (14.9) | 3 (30.0) | 7 (10.6) | 22 (20.4) |
| Paclitaxel protein-bound | 1 (5.0) | 2 (2.9) | 0 | 0 | 1 (1.5) | 1 (0.9) |
| Pertuzumab | 2 (10.0) | 67 (97.1) | 65 (87.8) | 3 (30.0) | 57 (86.4) | 87 (80.6) |
| Pertuzumab, trastuzumab and hyaluronidase-zzxf | 0 | 0 | 5 (6.8) | 0 | 0 | 2 (1.9) |
| Rituximab | 0 | 0 | 1 (1.4) | 0 | 0 | 0 |
| Tamoxifen | 0 | 0 | 0 | 0 | 2 (3.0) | 1 (0.9) |
| Trastuzumab | 16 (80.0) | 69 (100.0) | 44 (59.5) | 8 (80.0) | 62 (93.9) | 55 (50.9) |
| Trastuzumab-anns | 0 | 0 | 22 (29.7) | 0 | 0 | 44 (40.7) |
| Trastuzumab-dkst | 0 | 0 | 1 (1.4) | 0 | 0 | 5 (4.6) |
| Trastuzumab-dttb | 0 | 0 | 0 | 0 | 0 | 1 (0.9) |
| Trastuzumab-qyyp | 0 | 0 | 5 (6.8) | 0 | 0 | 8 (7.4) |
| Trastuzumab and hyaluronidase-oysk | 0 | 0 | 2 (2.7) | 0 | 0 | 0 |
| Tretinoin | 0 | 0 | 0 | 0 | 1 (1.5) | 0 |
| Vincristine | 0 | 0 | 0 | 0 | 1 (1.5) | 0 |
| High-Risk * | Non-High-Risk † | |||||
|---|---|---|---|---|---|---|
| 2011–2013 (n = 90) | 2014–2017 (n = 130) | 2018–2021 (n = 101) | 2011–2013 (n = 192) | 2014–2017 (n = 289) | 2018–2021 (n = 249) | |
| Patients receiving specific (post-neo)adjuvant treatment, n (%) ‡ | ||||||
| Ado-trastuzumab emtansine | 0 | 0 | 21 (20.8) | 0 | 0 | 29 (11.6) |
| Anastrozole | 37 (41.1) | 49 (37.7) | 31 (30.7) | 89 (46.4) | 122 (42.2) | 93 (37.3) |
| Bendamustine | 0 | 0 | 1 (1.0) | 0 | 0 | 0 |
| Bevacizumab | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Bevacizumab-awwb | 0 | 0 | 0 | 1 (0.5) | 0 | 0 |
| Blinatumomab | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Bortezomib | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Capecitabine | 0 | 0 | 1 (1.0) | 1 (0.5) | 0 | 0 |
| Carboplatin | 19 (21.1) | 25 (19.2) | 16 (15.8) | 59 (30.7) | 66 (22.8) | 26 (10.4) |
| Cisplatin | 2 (2.2) | 1 (0.8) | 0 | 0 | 0 | 0 |
| Cyclophosphamide | 10 (11.1) | 20 (15.4) | 6 (5.9) | 22 (11.5) | 21 (7.3) | 7 (2.8) |
| Daratumumab and hyaluronidase-fihj | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Docetaxel | 25 (27.8) | 26 (20.0) | 18 (17.8) | 67 (34.9) | 72 (24.9) | 29 (11.6) |
| Doxorubicin | 8 (8.9) | 14 (10.8) | 5 (5.0) | 13 (6.8) | 15 (5.2) | 4 (1.6) |
| Doxorubicin pegylated liposomal | 0 | 0 | 0 | 1 (0.5) | 0 | 0 |
| Durvalumab | 0 | 1 (0.8) | 0 | 0 | 0 | 0 |
| Epirubicin | 1 (1.1) | 4 (3.1) | 0 | 0 | 1 (0.3) | 1 (0.4) |
| Etoposide | 1 (1.1) | 0 | 0 | 0 | 0 | 0 |
| Exemestane | 13 (14.4) | 17 (13.1) | 6 (5.9) | 20 (10.4) | 32 (11.1) | 28 (11.2) |
| Fluorouracil | 0 | 5 (3.8) | 0 | 5 (2.6) | 2 (0.7) | 3 (1.2) |
| Fulvestrant | 0 | 0 | 1 (1.0) | 0 | 1 (0.3) | 0 |
| Gemcitabine | 1 (1.1) | 1 (0.8) | 0 | 1 (0.5) | 1 (0.3) | 1 (0.4) |
| Goserelin | 1 (1.1) | 8 (6.2) | 9 (8.9) | 0 | 3 (1.0) | 5 (2.0) |
| Hydroxyurea | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
| Inotuzumab ozogamicin | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Irinotecan | 0 | 0 | 0 | 0 | 1 (0.3) | 1 (0.4) |
| Lapatinib | 0 | 1 (0.8) | 0 | 0 | 0 | 0 |
| Lenalidomide | 0 | 0 | 1 (1.0) | 0 | 1 (0.3) | 0 |
| Lenvatinib | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Letrozole | 22 (24.4) | 31 (23.8) | 15 (14.9) | 41 (21.4) | 73 (25.3) | 51 (20.5) |
| Leucovorin | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
| Leuprolide | 3 (3.3) | 5 (3.8) | 5 (5.0) | 0 | 2 (0.7) | 5 (2.0) |
| Levoleucovorin | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Mercaptopurine | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Methotrexate | 0 | 1 (0.8) | 1 (1.0) | 1 (0.5) | 2 (0.7) | 1 (0.4) |
| Neratinib | 0 | 5 (3.8) | 12 (11.9) | 0 | 6 (2.1) | 6 (2.4) |
| Niraparib | 0 | 0 | 0 | 1 (0.5) | 0 | 0 |
| Nivolumab | 0 | 1 (0.8) | 0 | 0 | 0 | 0 |
| Olaparib | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
| Oxaliplatin | 0 | 0 | 0 | 0 | 1 (0.3) | 1 (0.4) |
| Paclitaxel | 11 (12.2) | 20 (15.4) | 3 (3.0) | 20 (10.4) | 70 (24.2) | 76 (30.5) |
| Paclitaxel protein-bound | 1 (1.1) | 1 (0.8) | 0 | 0 | 3 (1.0) | 4 (1.6) |
| Pegaspargase | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Pembrolizumab | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
| Pemetrexed | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
| Pertuzumab | 1 (1.1) | 26 (20.0) | 50 (49.5) | 0 | 22 (7.6) | 60 (24.1) |
| Pertuzumab, trastuzumab and hyaluronidase-zzxf | 0 | 0 | 5 (5.0) | 0 | 0 | 2 (0.8) |
| Polatuzumab vedotin-piiq | 0 | 0 | 1 (1.0) | 0 | 0 | 0 |
| Ramucirumab | 0 | 0 | 0 | 0 | 1 (0.3) | 0 |
| Rituximab | 0 | 0 | 1 (1.0) | 0 | 0 | 0 |
| Rituximab and hyaluronidase | 0 | 0 | 1 (1.0) | 0 | 0 | 0 |
| Ruxolitinib | 0 | 0 | 0 | 0 | 0 | 1 (0.4) |
| Tamoxifen | 37 (41.1) | 42 (32.3) | 18 (17.8) | 46 (24.0) | 88 (30.4) | 57 (22.9) |
| Topotecan | 0 | 0 | 0 | 1 (0.5) | 0 | 0 |
| Toremifene | 1 (1.1) | 1 (0.8) | 0 | 2 (1.0) | 0 | 0 |
| Trastuzumab | 60 (66.7) | 113 (86.9) | 54 (53.5) | 110 (57.3) | 211 (73.0) | 120 (48.2) |
| Trastuzumab-anns | 0 | 1 (0.8) | 33 (32.7) | 0 | 0 | 87 (34.9) |
| Trastuzumab-dkst | 0 | 0 | 2 (2.0) | 0 | 0 | 7 (2.8) |
| Trastuzumab-qyyp | 0 | 1 (0.8) | 8 (7.9) | 0 | 0 | 25 (10.0) |
| Tretinoin | 0 | 0 | 0 | 1 (0.5) | 0 | 0 |
| Triptorelin | 0 | 1 (0.8) | 0 | 0 | 0 | 0 |
| Vincristine | 0 | 0 | 1 (1.0) | 0 | 1 (0.3) | 0 |
| Vinorelbine | 0 | 1 (0.8) | 0 | 0 | 0 | 0 |


References
- International Agency for Research on Cancer. Breast Cancer. Available online: https://www.iarc.who.int/cancer-type/breast-cancer (accessed on 2 August 2024).
- International Agency for Research on Cancer. Breast Cancer Facts & Figures 2024–2025. Available online: https://www.cancer.org/research/cancer-facts-statistics/breast-cancer-facts-figures.html (accessed on 15 January 2025).
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef] [PubMed]
- Morales, S.; Gasol, A.; Sanchez, D.R. HER2-Positive Cancers and Antibody-Based Treatment: State of the Art and Future Developments. Cancers 2021, 13, 5771. [Google Scholar] [CrossRef]
- Cronin, K.A.; Harlan, L.C.; Dodd, K.W.; Abrams, J.S.; Ballard-Barbash, R. Population-Based Estimate of the Prevalence of HER-2 Positive Breast Cancer Tumors for Early Stage Patients in the US. Cancer Investig. 2010, 28, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Unni, N.; Peng, Y. The Changing Paradigm for the Treatment of HER2-Positive Breast Cancer. Cancers 2020, 12, 2081. [Google Scholar] [CrossRef] [PubMed]
- O’Shaughnessy, J.; Gradishar, W.; O’Regan, R.; Gadi, V. Risk of Recurrence in Patients with HER2+ Early-Stage Breast Cancer: Literature Analysis of Patient and Disease Characteristics. Clin. Breast Cancer 2023, 23, 350–362. [Google Scholar] [CrossRef]
- Pernas, S.; Tolaney, S.M. Management of Early-Stage Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer. JCO Oncol. Pract. 2021, 17, 320–330. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Abramson, V.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; et al. NCCN Guidelines® Insights: Breast Cancer, Version 4.2023. J. Natl. Compr. Canc. Netw. 2023, 21, 594–608. [Google Scholar] [CrossRef]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef]
- Harbeck, N. Neoadjuvant and Adjuvant Treatment of Patients with HER2-Positive Early Breast Cancer. Breast 2022, 62 (Suppl. 1), S12–S16. [Google Scholar] [CrossRef]
- Matuschek, C.; Jazmati, D.; Bölke, E.; Tamaskovics, B.; Corradini, S.; Budach, W.; Krug, D.; Mohrmann, S.; Ruckhäberle, E.; Fehm, T.; et al. Post-Neoadjuvant Treatment Strategies in Breast Cancer. Cancers 2022, 14, 1246. [Google Scholar] [CrossRef]
- Perez, E.A.; Romond, E.H.; Suman, V.J.; Jeong, J.-H.; Sledge, G.; Geyer, C.E.; Martino, S.; Rastogi, P.; Gralow, J.; Swain, S.M.; et al. Trastuzumab plus Adjuvant Chemotherapy for Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer: Planned Joint Analysis of Overall Survival from NSABP B-31 and NCCTG N9831. J. Clin. Oncol. 2014, 32, 3744–3752. [Google Scholar] [CrossRef] [PubMed]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 Years’ Follow-up of Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Early Breast Cancer: Final Analysis of the HERceptin Adjuvant (HERA) Trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef]
- Ma, X.; Long, L.; Moon, S.; Adamson, B.J.S.; Baxi, S.S. Comparison of Population Characteristics in Real-World Clinical Oncology Databases in the US: Flatiron Health, SEER, and NPCR. MedRxiv. 2023. Preprint Published Online, Not Peer Reviewed. Available online: https://www.medrxiv.org/content/10.1101/2020.03.16.20037143v3 (accessed on 23 September 2024).
- Birnbaum, B.; Nussbaum, N.; Seidl-Rathkopf, K.; Agrawal, M.; Estevez, M.; Estola, E.; Haimson, J.; He, L.; Larson, P.; Richardson, P. Model-Assisted Cohort Selection with Bias Analysis for Generating Large-Scale Cohorts from the EHR for Oncology Research. Available online: http://arxiv.org/abs/2001.09765 (accessed on 23 September 2024).
- Loibl, S.; Mano, M.; Untch, M.; Huang, C.-S.; Mamounas, E.; Wolmark, N.; Knott, A.; Siddiqui, A.; Boulet, T.; Nyawira, B.; et al. Phase III Study of Adjuvant Ado-Trastuzumab Emtansine vs Trastuzumab for Residual Invasive HER2-Positive Early Breast Cancer after Neoadjuvant Chemotherapy and HER2-Targeted Therapy: KATHERINE Final IDFS and Updated OS Analysis. Cancer Res. 2024, 84 (Suppl. 9), GS03-12. [Google Scholar] [CrossRef]
- Abraham, J.; Mayden, K.D. Improving Outcomes in HER2-Positive Breast Cancer: Analysis and Application of Evolving Data and Best Practices. J. Adv. Pract. Oncol. 2020, 11, 271–274. [Google Scholar] [CrossRef]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.; Reynolds, K.L.; Smith, B.L.; Alexander, B.; Moy, B.; Isakoff, S.J.; et al. Pathologic Complete Response after Neoadjuvant Chemotherapy and Impact on Breast Cancer Recurrence and Survival: A Comprehensive Meta-Analysis. Clin. Cancer Res. 2020, 26, 2838–2848. [Google Scholar] [CrossRef]
- Amiri-Kordestani, L.; Wedam, S.; Zhang, L.; Tang, S.; Tilley, A.; Ibrahim, A.; Justice, R.; Pazdur, R.; Cortazar, P. First FDA Approval of Neoadjuvant Therapy for Breast Cancer: Pertuzumab for the Treatment of Patients with HER2-Positive Breast Cancer. Clin. Cancer Res. 2014, 20, 5359–5364. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; de la Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and Safety of Neoadjuvant Pertuzumab and Trastuzumab in Women with Locally Advanced, Inflammatory, or Early HER2-Positive Breast Cancer (NeoSphere): A Randomised Multicentre, Open-Label, Phase 2 Trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef] [PubMed]
- von Minckwitz, G.; Huang, C.-S.; Mano, M.; Loibl, S.; Mamounas, E.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef]
- Martin, M.; Holmes, F.A.; Ejlertsen, B.; Delaloge, S.; Moy, B.; Iwata, H.; von Minckwitz, G.; Chia, S.K.L.; Mansi, J.; Barrios, C.H.; et al. Neratinib after Trastuzumab-Based Adjuvant Therapy in HER2-Positive Breast Cancer (ExteNET): 5-Year Analysis of a Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Oncol. 2017, 18, 1688–1700. [Google Scholar] [CrossRef]
- Holmes, F.A.; Moy, B.; Delaloge, S.; Chia, S.K.L.; Ejlertsen, B.; Mansi, J.; Iwata, H.; Gnant, M.; Buyse, M.; Barrios, C.H.; et al. Overall Survival with Neratinib after Trastuzumab-Based Adjuvant Therapy in HER2-Positive Breast Cancer (ExteNET): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Eur. J. Cancer 2023, 184, 48–59. [Google Scholar] [CrossRef]
- Loibl, S. Adjuvant Pertuzumab and Trastuzumab in Patients with Early HER-2 Positive Breast Cancer in APHINITY: 8.4 Years’ Follow-up. ESMO Virtual Plenary. Available online: https://oncologypro.esmo.org/meeting-resources/esmo-virtual-plenary-resources/adjuvant-pertuzumab-and-trastuzumab-in-patients-with-early-her-2-positive-breast-cancer-in-aphinity-8.4-years-follow-up (accessed on 10 February 2025).
- Dang, C.; Ewer, M.S.; Delaloge, S.; Ferrero, J.-M.; Colomer, R.; de la Cruz-Merino, L.; Werner, T.L.; Dadswell, K.; Verrill, M.; Eiger, D.; et al. BERENICE Final Analysis: Cardiac Safety Study of Neoadjuvant Pertuzumab, Trastuzumab, and Chemotherapy Followed by Adjuvant Pertuzumab and Trastuzumab in HER2-Positive Early Breast Cancer. Cancers 2022, 14, 2596. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov NCT04622319. A Phase 3, Multicenter, Randomized, Open-Label, Active-Controlled Study of Trastuzumab Deruxtecan (T-DXd) versus Trastuzumab Emtansine (T-DM1) in Participants with High-Risk HER2-Positive Primary Breast Cancer Who Have Residual Invasive Disease in Breast or Axillary Lymph Nodes Following Neoadjuvant Therapy (DESTINY-Breast05). Available online: https://clinicaltrials.gov/study/NCT04622319 (accessed on 3 January 2025).
- ClinicalTrials.gov NCT05113251. ClinicalTrials.gov NCT05113251. A Phase 3 Open-Label Trial of Neoadjuvant Trastuzumab Deruxtecan (T-DXd) Monotherapy or T-DXd Followed by THP Compared to ddAC-THP in Participants With High-Risk HER2-Positive Early-Stage Breast Cancer (DESTINY-Breast11). Available online: https://clinicaltrials.gov/study/NCT05113251 (accessed on 15 January 2025).
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant Trastuzumab in HER2-Positive Breast Cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [PubMed]
- van Ramshorst, M.S.; van der Voort, A.; van Werkhoven, E.D.; Mandjes, I.A.; Kemper, I.; Dezentjé, V.O.; Oving, I.M.; Honkoop, A.H.; Tick, L.W.; van de Wouw, A.J.; et al. Neoadjuvant Chemotherapy with or without Anthracyclines in the Presence of Dual HER2 Blockade for HER2-Positive Breast Cancer (TRAIN-2): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2018, 19, 1630–1640. [Google Scholar] [CrossRef] [PubMed]
- Garutti, M.; Cucciniello, L.; Arpino, G.; Fabi, A.; Livi, L.; Munzone, E.; Staropoli, N.; Zamagni, C.; Zambelli, A.; Puglisi, F. Risk-Based Therapeutic Strategies for HER2-Positive Early Breast Cancer: A Consensus Paper. Clin. Breast Cancer 2023, 23, e458–e469. [Google Scholar] [CrossRef]




| Overall (N = 1290) | High-Risk * (n = 366) | Non-High-Risk (n = 924) | |
|---|---|---|---|
| Age at diagnosis | |||
| Mean (SD) | 57.6 (12.8) | 55.5 (13.5) | 58.5 (12.4) |
| Median [min, max] | 58.0 [23.0, 85.0] | 56.0 [23.0, 84.0] | 59.0 [23.0, 85.0] |
| Sex, n (%) † | |||
| Female | 1281 (99.3) | ≥ 360 (≥98) | 918 (99.4) |
| Male | 9 (0.7) | ≤ 5 (≤ 1) | 6 (0.6) |
| Race, n (%) | |||
| White | 817 (63.3) | 223 (60.9) | 594 (64.3) |
| Black | 133 (10.3) | 38 (10.4) | 95 (10.3) |
| Asian | 51 (3.9) | 13 (3.6) | 38 (4.1) |
| Other | 178 (13.8) | 59 (16.1) | 119 (12.9) |
| Missing | 111 (8.6) | 33 (9.0) | 78 (8.4) |
| Ethnicity, n (%) | |||
| Hispanic/Latino | 104 (8.1) | 33 (9.0) | 71 (7.7) |
| Non-Hispanic/Non-Latino | 982 (76.1) | 281 (76.8) | 701 (75.9) |
| Missing | 204 (15.8) | 52 (14.2) | 152 (16.5) |
| BMI at diagnosis, n (%) ‡ | |||
| Normal (18.5–< 25) | 49 (3.8) | 13 (3.6) | 36 (3.9) |
| Overweight (25–< 30) | 55 (4.3) | 17 (4.6) | 38 (4.1) |
| Obese (≥ 30) | 66 (5.1) | 23 (6.3) | 43 (4.7) |
| Missing | 1119 (86.7) | 313 (85.5) | 806 (87.2) |
| Underweight (< 18.5) | 1 (0.1) | 0 (0) | 1 (0.1) |
| Region, n (%) | |||
| South | 500 (38.8) | 138 (37.7) | 362 (39.2) |
| Northeast | 170 (13.2) | 48 (13.1) | 122 (13.2) |
| West | 171 (13.3) | 49 (13.4) | 122 (13.2) |
| Midwest | 165 (12.8) | 43 (11.7) | 122 (13.2) |
| Missing | 284 (22.0) | 88 (24.0) | 196 (21.2) |
| Menopausal status, n (%) | |||
| Premenopausal | 340 (26.4) | 120 (32.8) | 220 (23.8) |
| Postmenopausal | 829 (64.3) | 212 (57.9) | 617 (66.8) |
| Perimenopausal | 33 (2.6) | 10 (2.7) | 23 (2.5) |
| Missing/not applicable/male | 88 (6.8) | 24 (6.6) | 64 (6.9) |
| Months of follow up | |||
| Mean (SD) | 61.5 (35.8) | 63.0 (36.5) | 61.0 (35.5) |
| Median (IQR) | 58.0 (31.9, 87.8) | 58.2 (31.1, 94.7) | 57.8 (32.4, 85.1) |
| High-Risk * n = 366 | Non-High-Risk n = 924 | |
|---|---|---|
| Treatment pathway after diagnosis, n (%) | ||
| No treatment | 1 (0.3) | 34 (3.7) |
| Neoadjuvant treatment only | 0 | 0 |
| Neoadjuvant treatment followed by surgery only | 3 (0.8) | 1 (0.1) |
| Surgery only | 41 (11.2) | 159 (17.2) |
| Surgery followed by adjuvant treatment | 161 (44.0) | 547 (59.2) |
| Neoadjuvant treatment followed by surgery and post-neoadjuvant treatment | 160 (43.7) | 183 (19.8) |
| Type of surgery, n (%) | ||
| Unilateral lumpectomy | 127 (34.7) | 498 (53.9) |
| Unilateral mastectomy | 128 (35.0) | 166 (18.0) |
| High-Risk * n = 366 | Non-High-Risk n = 924 | |||
|---|---|---|---|---|
| Received Neoadjuvant Therapy | Did Not Receive Neoadjuvant Therapy | Received Neoadjuvant Therapy | Did Not Receive Neoadjuvant Therapy | |
| Overall, n | 163 | 203 | 184 | 740 |
| ER status, n (%) | ||||
| Positive | 103 (63.2) | 151 (74.4) | 124 (67.4) | 527 (71.2) |
| Negative | 60 (36.8) | 51 (25.1) | 60 (32.6) | 213 (28.8) |
| Missing | - | 1 (0.5) | - | - |
| PR status, n (%) | ||||
| Positive | 77 (47.2) | 117 (57.6) | 104 (56.5) | 379 (51.2) |
| Negative | 85 (52.1) | 85 (41.9) | 80 (43.5) | 356 (48.1) |
| Missing, equivocal, or unknown | 1 (0.6) | 1 (0.5) | - | 5 (0.7) |
| HR status, n (%) † | ||||
| Positive | 109 (66.9) | 156 (76.8) | 123 (71.7) | 534 (73.4) |
| Negative | 54 (33.1) | 46 (23.2) | 52 (28.3) | 197 (26.6) |
| Missing, equivocal, or unknown | - | 1 (0.5) | - | - |
| High-Risk * n = 366 | Non-High-Risk n = 924 | |||
|---|---|---|---|---|
| Received (Post-Neo)Adjuvant Therapy | Did Not Receive (Post-Neo)Adjuvant Therapy | Received (Post-Neo)Adjuvant Therapy | Did Not Receive (Post-Neo)Adjuvant Therapy | |
| Overall, n | 321 | 45 | 730 | 194 |
| ER status, n (%) | ||||
| Positive | 233 (72.6) | 21 (46.7) | 551 (75.5) | 100 (51.5) |
| Negative | 87 (27.1) | 24 (53.3) | 179 (24.5) | 94 (48.5) |
| Missing | 1 (0.3) | - | - | - |
| PR status, n (%) | ||||
| Positive | 178 (55.5) | 16 (35.6) | 415 (56.8) | 68 (35.1) |
| Negative | 141 (43.9) | 29 (64.4) | 313 (42.9) | 123 (63.4) |
| Missing, equivocal, or unknown | 2 (0.6) | - | 2 (0.3) | 3 (1.5) |
| HR status, n (%) † | ||||
| Positive | 241 (75.1) | 24 (53.3) | 569 (78.0) | 106 (54.6) |
| Negative | 79 (24.6) | 21 (46.7) | 161 (22.0) | 88 (45.4) |
| Missing, equivocal, or unknown | 1 (0.3) | - | - | - |
| Pathologic group stage, n (%) | ||||
| I | 37 (11.5) | 3 (6.7) | 418 (57.3) | 111 (57.2) |
| II | 129 (40.2) | 22 (48.9) | 124 (17.0) | 37 (19.1) |
| III | 43 (13.4) | 14 (31.1) | 2 (0.3) | 5 (2.6) |
| pCR | 69 (21.5) | - | 124 (17.0) | 25 (12.9) |
| Unknown | 43 (13.4) | 6 (13.3) | 62 (8.5) | 16 (8.2) |
| High-Risk * n = 366 | Non-High-Risk † n = 924 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2011–2013 | 2014–2017 | 2018–2021 | 2011–2013 | 2014–2017 | 2018–2021 | |||||||||||||
| HR+ n = 80 | HR− n = 29 | Total N = 109 | HR+ n = 113 | HR− n = 33 | Total N = 146 | HR+ n = 72 | HR− n = 38 | Total N = 110 | HR+ n = 182 | HR− n = 59 | Total ‡ N = 241 | HR+ n = 271 | HR− n = 98 | Total N = 369 | HR+ n = 222 | HR− n = 92 | Total N = 314 | |
| Neoadjuvant therapy, n (%) | 14 (17.5) | 6 (20.7) | 20 (18.3) | 48 (42.5) | 21 (63.6) | 69 (47.3) | 47 (65.3) | 27 (71.1) | 74 (67.3) | 9 (4.9) | 1 (1.7) | 10 (4.1) | 44 (16.2) | 22 (22.4) | 66 (17.9) | 79 (35.6) | 29 (31.5) | 108 (34.4) |
| CT | 14 (17.5) | 6 (20.7) | 20 (18.3) | 47 (41.6) | 21 (63.6) | 68 (46.6) | 45 (62.5) | 27 (71.1) | 72 (65.5) | 8 (4.4) | 1 (1.7) | 9 (3.7) | 42 (15.5) | 22 (22.4) | 64 (17.3) | 77 (34.7) | 29 (31.5) | 106 (33.8) |
| Platinum-based CT | 6 (7.5) | 3 (10.3) | 9 (8.3) | 41 (36.3) | 18 (54.5) | 59 (40.4) | 39 (54.2) | 23 (60.5) | 62 (56.4) | 4 (2.2) | 0 | 4 (1.7) | 35 (12.9) | 13 (13.3) | 48 (13.0) | 62 (27.9) | 23 (25.0) | 85 (27.1) |
| Taxane | 14 (17.5) | 6 (20.7) | 20 (18.3) | 47 (41.6) | 21 (63.6) | 68 (46.6) | 45 (62.5) | 27 (71.1) | 72 (65.5) | 7 (3.8) | 1 (1.7) | 8 (3.3) | 41 (15.1) | 21 (21.4) | 62 (16.8) | 77 (34.7) | 29 (31.5) | 106 (33.8) |
| Other CT | 6 (7.5) | 4 (13.8) | 10 (9.2) | 3 (2.7) | 1 (3.0) | 4 (2.7) | 3 (4.2) | 4 (10.5) | 7 (6.4) | 4 (2.2) | 0 | 4 (1.7) | 2 (0.7) | 4 (4.1) | 6 (1.6) | 3 (1.4) | 4 (4.3) | 7 (2.2) |
| ET | 0 | 0 | 0 | 3 (2.7) | 1 (3.0) | 4 (2.7) | 8 (11.1) | 3 (7.9) | 11 (10.0) | 1 (0.5) | 0 | 1 (0.4) | 2 (0.7) | 0 | 2 (0.5) | 5 (2.3) | 2 (2.2) | 7 (2.2) |
| HER2 directed § | 12 (15.0) | 4 (13.8) | 16 (14.7) | 48 (42.5) | 21 (63.6) | 69 (47.3) | 45 (62.5) | 26 (68.4) | 71 (64.5) | 7 (3.8) | 1 (1.7) | 8 (3.3) | 41 (15.1) | 21 (21.4) | 62 (16.8) | 77 (34.7) | 29 (31.5) | 106 (33.8) |
| (Post-neo)adjuvant therapy, n (%) | 73 (91.3) | 16 (55.2) | 89 (81.7) | 101 (89.4) | 29 (87.9) | 130 (89.0) | 67 (93.1) | 34 (89.5) | 101 (91.8) | 157 (86.3) | 35 (59.3) | 192 (79.7) | 227 (83.8) | 62 (63.3) | 289 (78.3) | 185 (83.3) | 64 (69.6) | 249 (79.3) |
| CT | 29 (36.3) | 7 (24.1) | 36 (33.0) | 40 (35.4) | 9 (27.3) | 49 (33.6) | 19 (26.4) | 6 (15.8) | 25 (22.7) | 60 (33.0) | 30 (50.8) | 90 (37.3) | 104 (38.4) | 36 (36.7) | 140 (37.9) | 78 (35.1) | 30 (32.6) | 108 (34.4) |
| Platinum-based CT | 17 (21.3) | 4 (13.8) | 21 (19.3) | 23 (20.4) | 2 (6.1) | 25 (17.1) | 13 (18.1) | 3(7.9) | 16 (14.5) | 38 (20.9) | 21 (35.6) | 59 (24.5) | 49 (18.1) | 17 (17.3) | 66 (17.9) | 16 (7.2) | 11 (12.0) | 27 (8.6) |
| Taxane | 29 (36.3) | 6 (20.7) | 35 (32.1) | 38 (33.6) | 5 (15.2) | 43 (29.5) | 15 (20.8) | 6(15.8) | 21 (19.1) | 56 (30.8) | 29 (49.2) | 85 (35.3) | 102 (37.6) | 36 (36.7) | 138 (37.4) | 74 (33.3) | 29 (31.5) | 103 (32.8) |
| Other CT | 9 (11.3) | 3 (10.3) | 12 (11.0) | 15 (13.3) | 7 (21.2) | 22 (15.1) | 4 (5.6) | 2(5.3) | 6 (5.5) | 16 (8.8) | 7 (11.9) | 23 (9.5) | 15 (5.5) | 9 (9.2) | 24 (6.5) | 8 (3.6) | 1 (1.1) | 9 (2.9) |
| ET | 55 (68.8) | 2 (6.9) | 57 (52.3) | 76 (67.3) | 4 (12.1) | 80 (54.8) | 45 (62.5) | 1 (2.6) | 46 (41.8) | 120 (65.9) | 2 (3.4) | 122 (50.6) | 172 (63.5) | 4 (4.1) | 176 (47.7) | 137 (61.7) | 1 (1.1) | 138 (43.9) |
| HER2 directed ‡ | 45 (56.3) | 15 (51.7) | 60 (55.0) | 85 (75.2) | 28 (84.8) | 113 (77.4) | 61 (84.7) | 34 (89.5) | 95 (86.4) | 77 (42.3) | 33 (55.9) | 110 (45.6) | 157 (57.9) | 54 (55.1) | 211 (57.2) | 153 (68.9) | 63 (68.5) | 216 (68.8) |
| High-Risk * n = 366 | Non-High-Risk n = 924 | |
|---|---|---|
| Time between/duration of treatment, days (IQR) | ||
| Median time from diagnosis to neoadjuvant therapy | 29 (23–43) | 34 (27–44) |
| Median duration of neoadjuvant therapy | 145 (132–163) | 141 (126–155) |
| Median time between diagnosis and surgery | 76 (26–180) | 36 (15–151) |
| Median time between surgery and (post-neo)adjuvant therapy | 31 (17–71) | 44 (24–84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahtani, R.; Collin, S.M.; Tan, Z.; Shah, C.H.; Adeyemi, B.; Davies, S.; John, E.; Vidal, G. Human Epidermal Growth Factor Receptor 2-Positive (HER2+) Early Breast Cancer Treatment and Outcomes by Risk of Recurrence: A Retrospective US Electronic Health Records Study. Cancers 2025, 17, 1848. https://doi.org/10.3390/cancers17111848
Mahtani R, Collin SM, Tan Z, Shah CH, Adeyemi B, Davies S, John E, Vidal G. Human Epidermal Growth Factor Receptor 2-Positive (HER2+) Early Breast Cancer Treatment and Outcomes by Risk of Recurrence: A Retrospective US Electronic Health Records Study. Cancers. 2025; 17(11):1848. https://doi.org/10.3390/cancers17111848
Chicago/Turabian StyleMahtani, Reshma, Simon M. Collin, Ziyu Tan, Chintal H. Shah, Basirat Adeyemi, Sophie Davies, Ellie John, and Gregory Vidal. 2025. "Human Epidermal Growth Factor Receptor 2-Positive (HER2+) Early Breast Cancer Treatment and Outcomes by Risk of Recurrence: A Retrospective US Electronic Health Records Study" Cancers 17, no. 11: 1848. https://doi.org/10.3390/cancers17111848
APA StyleMahtani, R., Collin, S. M., Tan, Z., Shah, C. H., Adeyemi, B., Davies, S., John, E., & Vidal, G. (2025). Human Epidermal Growth Factor Receptor 2-Positive (HER2+) Early Breast Cancer Treatment and Outcomes by Risk of Recurrence: A Retrospective US Electronic Health Records Study. Cancers, 17(11), 1848. https://doi.org/10.3390/cancers17111848