
Early Immune Checkpoint Inhibitor Administration Increases the Risk of Radiation-Induced Pneumonitis in Patients with Stage III Unresectable NSCLC Undergoing Chemoradiotherapy

 , , ,
, , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Meta-Analysis
2.1.1. Search Strategy and Selection Criteria
2.1.2. Data Extraction
2.1.3. Quality Assessment
2.1.4. Statistics Analysis
2.2. Real-World Retrospective Study
2.2.1. Study Design and Patients
2.2.2. Treatment Strategy
2.2.3. Diagnosis and Classification of RP
2.2.4. Statistical Analysis
3. Results
3.1. Results in Meta-Analysis
3.1.1. Search Results
3.1.2. Characteristics and Methodological Quality of the Studies
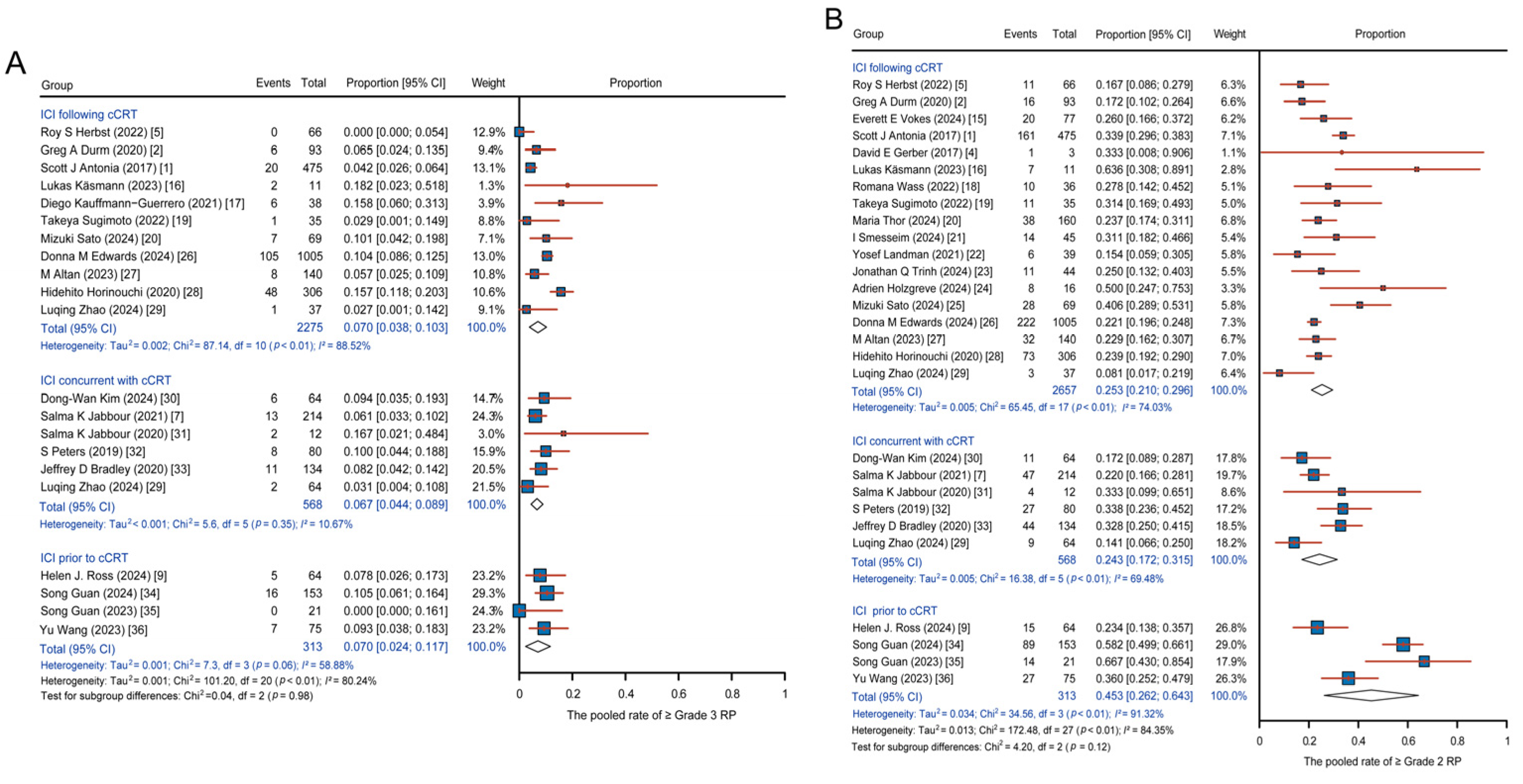
3.1.3. Results of the Statistical Analyses
3.2. Results in Real-World Retrospective Study
3.2.1. Patient Characteristics
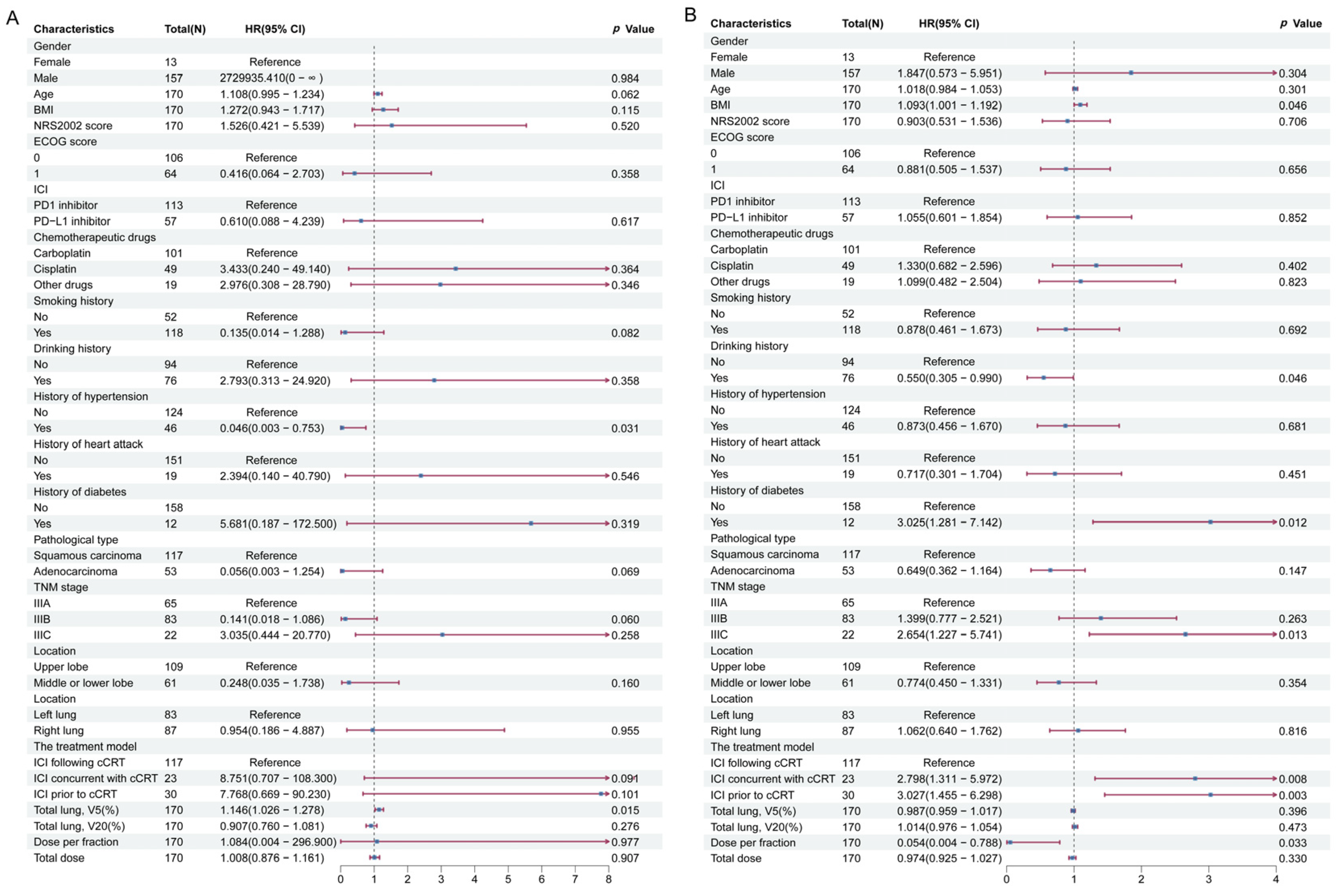
3.2.2. Radiation-Related Pneumonia Outcome
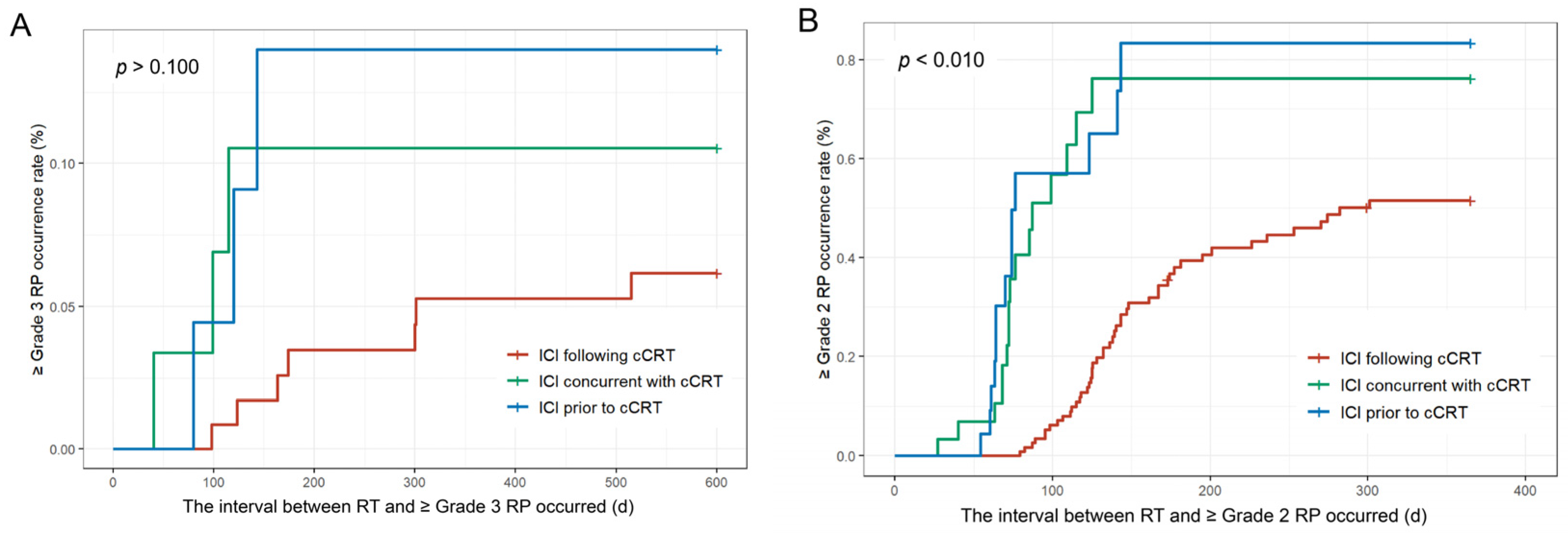
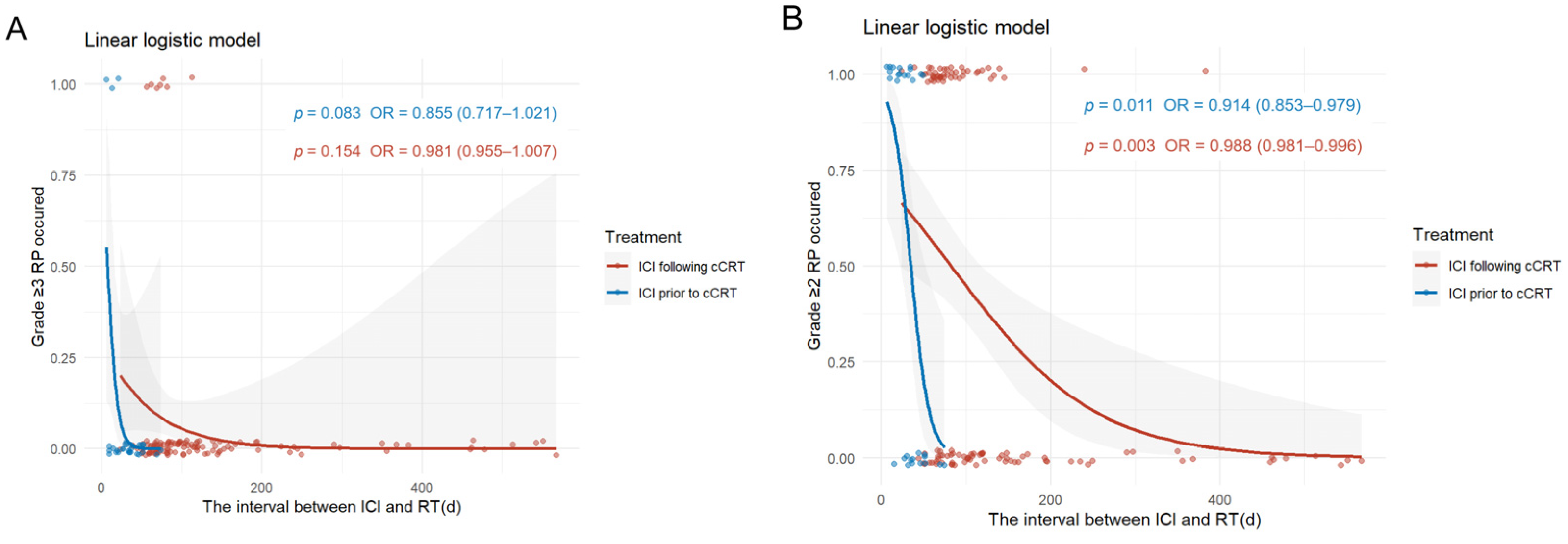
3.2.3. Interval Between ICI and RT Relating to RP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| cCRT | Concurrent chemoradiotherapy |
| CI | Confidence intervals |
| CT | Computed tomography |
| HR | Hazard ratios |
| ICI | Immune checkpoint inhibitors |
| IQR | Interquartile range |
| NSCLC | Non-small cell lung cancer |
| OR | Odds ratios |
| PD-1 | Programmed death 1 |
| PD-L1 | Programmed death-ligand 1 |
| RCTs | Randomized controlled trials |
| RP | Radiation-related pneumonitis |
| RT | Radiotherapy |
| RWSs | Real-world retrospective studies |
| SD | Standard deviation |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) Search strategy in PubMed | |
| # | Query |
| #1 | “Carcinoma, Non-Small-Cell Lung”[Mesh] |
| #2 | ((((((((Non Small Cell Lung) OR Non-Small-Cell Lung) OR Non-Small-Cell Lung Carcinomas) OR Non-Small Cell Lung Cancer) OR Non-Small-Cell Lung Carcinoma) OR Non Small Cell Lung Carcinoma) OR Nonsmall Cell Lung Cancer) OR Non-Small Cell Lung Carcinoma) |
| #3 | #1 OR #2 |
| #4 | “Immunotherapy”[Mesh] |
| #5 | (“Immunotherapy”[Mesh]) OR (Immunotherapies[Title/Abstract]) |
| #6 | “Immune Checkpoint Inhibitors”[Mesh] |
| #7 | ((((((((((((((((((Immune Checkpoint Blockers[Title/Abstract]) OR Immune Checkpoint Inhibitor[Title/Abstract]) OR CTLA-4 Inhibitors[Title/Abstract]) OR CTLA 4 Inhibitors[Title/Abstract]) OR Cytotoxic T-Lymphocyte-Associated Protein 4 Inhibitor[Title/Abstract]) OR Cytotoxic T Lymphocyte Associated Protein 4 Inhibitor[Title/Abstract]) OR CTLA-4 Inhibitor[Title/Abstract]) OR CTLA 4 Inhibitor[Title/Abstract]) OR PD-1 Inhibitor[Title/Abstract]) OR PD 1 Inhibitor[Title/Abstract]) OR Programmed Cell Death Protein 1 Inhibitor[Title/Abstract]) OR Immune Checkpoint Blockade[Title/Abstract]) OR Immune Checkpoint Inhibition[Title/Abstract]) OR PD-L1 Inhibitor[Title/Abstract]) OR PD L1 Inhibitor[Title/Abstract]) OR Programmed Death-Ligand 1 Inhibitors[Title/Abstract]) OR Programmed Death Ligand 1 Inhibitors[Title/Abstract]) OR PD-1-PD-L1 Blockade[Title/Abstract]) OR PD 1 PD L1 Blockade[Title/Abstract] |
| #8 | #5 OR #6 OR #7 |
| #9 | “Chemoradiotherapy”[Mesh] |
| #10 | (((((((((((((Chemoradiotherapies) OR Radiochemotherapy) OR Radiochemotherapies) OR Concurrent Chemoradiotherapy) OR Concurrent Chemoradiotherapies) OR Concomitant Chemoradiotherapy) OR Concomitant Chemoradiotherapies) OR Concomitant Radiochemotherapy) OR Concomitant Radiochemotherapies) OR Concurrent Radiochemotherapy) OR Concurrent Radiochemotherapies) OR Synchronous Chemoradiotherapy) OR Synchronous Chemoradiotherapies) |
| #11 | #9 OR #10 |
| #12 | #3 AND #8 AND #11 |
| (b) Search strategy in Embase | |
| # | Query |
| #1 | ‘non small cell lung cancer’/exp |
| #2 | ‘bronchial non small cell cancer’:ab,ti OR ‘bronchial non small cell carcinoma’:ab,ti OR ‘carcinoma, non-small-cell lung’:ab,ti OR ‘lung cancer, non small cell’:ab,ti OR ‘lung non small cell cancer’:ab,ti OR ‘lung non small cell carcinoma’:ab,ti OR ‘non oat cell lung cancer’:ab,ti OR ‘non small cell bronchial cancer’:ab,ti OR ‘non small cell cancer, lung’:ab,ti OR ‘non small cell lung carcinoma’:ab,ti OR ‘non small cell pulmonary cancer’:ab,ti OR ‘non small cell pulmonary carcinoma’:ab,ti OR ‘non squamous NSCLC’:ab,ti OR ‘non-oat cell lung cancer’:ab,ti OR ‘non-small-cell lung carcinoma’:ab,ti OR ‘nonsmall cell carcinoma of the lung’:ab,ti OR ‘nonsmall cell lung cancer’:ab,ti OR ‘nonsmall cell lung carcinoma’:ab,ti OR ‘pulmonary non small cell cancer’:ab,ti OR ‘pulmonary non small cell carcinoma’:ab,ti OR ‘non small cell lung cancer’:ab,ti |
| #3 | #1 OR #2 |
| #4 | ‘immune checkpoint inhibitor’/exp |
| #5 | ‘immune checkpoint inhibitor’/exp OR ‘Immune Checkpoint Blockers’:ab,kw,ti OR ‘Immune Checkpoint Inhibitor’:ab,kw,ti OR ‘CTLA-4 Inhibitors’:ab,kw,ti OR ‘CTLA 4 Inhibitors’:ab,kw,ti OR ‘Cytotoxic T-Lymphocyte-Associated Protein 4 Inhibitor’:ab,kw,ti OR ‘Cytotoxic T Lymphocyte Associated Protein 4 Inhibitor’:ab,kw,ti OR ‘CTLA-4 Inhibitor’:ab,kw,ti OR ‘CTLA 4 Inhibitor’:ab,kw,ti OR ‘PD-1 Inhibitor’:ab,kw,ti OR ‘PD 1 Inhibitor’:ab,kw,ti OR ‘Programmed Cell Death Protein 1 Inhibitor’:ab,kw,ti OR ‘Immune Checkpoint Blockade’:ab,kw,ti OR ‘Immune Checkpoint Inhibition’:ab,kw,ti OR ‘PD-L1 Inhibitor’:ab,kw,ti OR ‘PD L1 Inhibitor’:ab,kw,ti OR ‘Programmed Death-Ligand 1 Inhibitors’:ab,kw,ti OR ‘Programmed Death Ligand 1 Inhibitors’:ab,kw,ti OR ‘PD-1-PD-L1 Blockade’:ab,kw,ti OR ‘PD 1 PD L1 Blockade’:ab,kw,ti |
| #6 | ‘checkpoint inhibitor therapy’/exp |
| #7 | ‘check point blocking therapy’:ab,ti OR ‘check point inhibition therapy’:ab,ti OR ‘check point inhibitor therapy’:ab,ti OR ‘check point inhibitor-based therapy’:ab,ti OR ‘check point inhibitorbased therapy’:ab,ti OR ‘check point inhibitors therapy’:ab,ti OR ‘checkpoint blockade antibody therapy’:ab,ti OR ‘checkpoint blockade immune therapy’:ab,ti OR ‘checkpoint blockade immunotherapy’:ab,ti OR ‘checkpoint blockade therapy’:ab,ti OR ‘checkpoint blockage therapy’:ab,ti OR ‘checkpoint blocker immune therapy’:ab,ti OR ‘checkpoint blocker therapy’:ab,ti OR ‘checkpoint blocking antibody therapy’:ab,ti OR ‘checkpoint blocking immunotherapy’:ab,ti OR ‘checkpoint blocking therapy’:ab,ti OR ‘checkpoint immune therapy’:ab,ti OR ‘checkpoint immunotherapy’:ab,ti OR ‘checkpoint inhibition therapy’:ab,ti OR ‘checkpoint inhibitor antibody therapy’:ab,ti OR ‘checkpoint inhibitors therapy’:ab,ti OR ‘checkpoint inhibitory therapy’:ab,ti OR ‘immune checkpoint blockade therapy’:ab,ti OR ‘immune checkpoint blockage therapy’:ab,ti OR ‘immune checkpoint blocker therapy’:ab,ti OR ‘immune checkpoint blocking therapy’:ab,ti OR ‘immune checkpoint inhibition therapy’:ab,ti OR ‘immune checkpoint inhibitor therapy’:ab,ti OR ‘immune checkpoint mAb therapy’:ab,ti OR ‘immune checkpoint therapy’:ab,ti OR ‘immuno-checkpoint therapy’:ab,ti OR ‘immunocheckpoint therapy’:ab,ti OR ‘immunological checkpoint therapy’:ab,ti OR ‘inhibitor checkpoint therapy’:ab,ti OR ‘checkpoint inhibitor therapy’:ab,ti |
| #8 | #5 OR #6 OR #7 |
| #9 | ‘chemoradiotherapy‘/exp |
| #10 | ‘Chemoradiotherapies’:ab,kw,ti OR ‘Radiochemotherapy’:ab,kw,ti OR ‘Radiochemotherapies’:ab,kw,ti OR ‘Concurrent Chemoradiotherapy’:ab,kw,ti OR ‘Concurrent Chemoradiotherapies’:ab,kw,ti OR ‘Concomitant Chemoradiotherapy’:ab,kw,ti OR ‘Concomitant Chemoradiotherapies’:ab,kw,ti OR ‘Concomitant Radiochemotherapy’:ab,kw,ti OR ‘Concomitant Radiochemotherapies’:ab,kw,ti OR ‘Concurrent Radiochemotherapy’:ab,kw,ti OR ‘Concurrent Radiochemotherapies’:ab,kw,ti OR ‘Synchronous Chemoradiotherapy’:ab,kw,ti OR ‘Synchronous Chemoradiotherapies’:ab,kw,ti |
| #11 | #9 OR #10 |
| #12 | #3 AND #8 AND #11 |
| (c) Search strategy in Web of Science | |
| # | Query |
| #1 | TS = (non small cell lung cancer OR Non Small Cell Lung OR Non-Small-Cell Lung OR Non-Small-Cell Lung Carcinomas OR Non-Small Cell Lung Cancer OR Non-Small-Cell Lung Carcinoma OR Non Small Cell Lung Carcinoma OR Nonsmall Cell Lung Cancer OR Non-Small Cell Lung Carcinoma) |
| #2 | TS = (cancer immunotherapy OR immunotherapy, cancer OR tumor immunotherapy OR tumour immunotherapy OR cancer immunotherapy OR checkpoint inhibitor therapy OR check point blocking therapy OR check point inhibition therapy OR check point inhibitor therapy OR check point inhibitor-based therapy OR check point inhibitorbased therapy OR check point inhibitors therapy OR checkpoint blockade antibody therapy OR checkpoint blockade immune therapy OR checkpoint blockade immunotherapy OR checkpoint blockade therapy OR checkpoint blockage therapy OR checkpoint blocker immune therapy OR checkpoint blocker therapy OR checkpoint blocking antibody therapy OR checkpoint blocking immunotherapy OR checkpoint blocking therapy OR checkpoint immune therapy OR checkpoint immunotherapy OR checkpoint inhibition therapy OR checkpoint inhibitor antibody therapy OR checkpoint inhibitors therapy OR checkpoint inhibitory therapy OR immune checkpoint blockade therapy OR immune checkpoint blockage therapy OR immune checkpoint blocker therapy OR immune checkpoint blocking therapy OR immune checkpoint inhibition therapy OR immune checkpoint inhibitor therapy OR immune checkpoint mAb therapy OR immune checkpoint therapy OR immuno-checkpoint therapy OR immunocheckpoint therapy OR immunological checkpoint therapy OR inhibitor checkpoint therapy OR checkpoint inhibitor therapy) |
| #3 | TS = (chemoradiotherapy OR Chemoradiotherapies OR Radiochemotherapy OR Radiochemotherapies OR Concurrent Chemoradiotherapy OR Concurrent Chemoradiotherapies OR Concomitant Chemoradiotherapy OR Concomitant Chemoradiotherapies OR Concomitant Radiochemotherapy OR Concomitant Radiochemotherapies OR Concurrent Radiochemotherapy OR Concurrent Radiochemotherapies OR Synchronous Chemoradiotherapy OR Synchronous Chemoradiotherapies) |
| #4 | #1 AND #2 AND #3 |
| (d) Search strategy in ClinicalTrials | |
| Condition/disease | NSCLC, Stage III |
| Other terms | Chemoradiotherapy |
| Intervention/treatment | Immunotherapy |
| (A) The inclusion criteria: |
| (1) Prospective or retrospective studies that conduct clinicopathological examinations of stage III unresectable NSCLC; (2) Treated with concurrent chemoradiotherapy and immunotherapy; (3) Reported the incidence of RP; (4) Published in English. |
| (B) The exclusion criteria: |
| (1) Studies reported only patient survival data (e.g., OS, PFS) without the occurrence of RP; (2) Use of sequential chemoradiotherapy; (3) Use of radiotherapy alone; (4) Immunotherapy not administered; (5) Inclusion of other tumor types (e.g., small-cell lung and esophageal cancers); (6) Inclusion of patients with non-stage III NSCLC; (7) Non-investigational articles (e.g., abstracts, letters, tumor reviews, and systematic reviews); (8) Articles on other topics (e.g., animal and molecular experiments). |
| (A) The inclusion criteria: |
| (1) Pathologically and clinically confirmed diagnosis of stage III unresectable NSCLC per the 9th edition of AJCC staging; (2) Treatment with cCRT and immunotherapy using anti-PD-1/anti-PD-L1; (3) Age ≥18 years; (4) Availability of complete clinical, imaging, and radiotherapy planning data; (5) ECOG PS of ≤1, with no significant dysfunction in cardiac, hepatic, renal, or other major organs; (6) Total radiotherapy dose of ≥40 Gy; (7) Follow-up duration of >6 months. |
| (B) The exclusion criteria: |
| (1) History of prior chest radiotherapy; (2) Severe lung infection; (3) Sequential radiotherapy; (4) Prior surgery; (5) Incomplete clinical data. |
| Author (Year) | Selection | Comparability | Outcome | Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | H | ||
| Lukas Käsmann (2023) [16] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Romana Wass (2022) [18] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Jonathan Q Trinh (2024) [23] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Adrien Holzgreve (2024) [24] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Mizuki Sato (2024) [25] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Donna M Edwards (2024) [26] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Luqing Zhao (2024) [29] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Song Guan (2024) [34] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Song Guan (2023) [35] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
References
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Durm, G.A.; Jabbour, S.K.; Althouse, S.K.; Liu, Z.; Sadiq, A.A.; Zon, R.T.; Jalal, S.I.; Kloecker, G.H.; Williamson, M.J.; Reckamp, K.L.; et al. A phase 2 trial of consolidation pembrolizumab following concurrent chemoradiation for patients with unresectable stage III non-small cell lung cancer: Hoosier Cancer Research Network LUN 14-179. Cancer 2020, 126, 4353–4361. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Chen, M.; Jiang, O.; Pan, Y.; Hu, D.; Lin, Q.; Wu, G.; Cui, J.; Chang, J.; Cheng, Y.; et al. Sugemalimab versus placebo after concurrent or sequential chemoradiotherapy in patients with locally advanced, unresectable, stage III non-small-cell lung cancer in China (GEMSTONE-301): Interim results of a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2022, 23, 209–219. [Google Scholar]
- Gerber, D.E.; Urbanic, J.J.; Langer, C.; Hu, C.; Chang, I.F.; Lu, B.; Movsas, B.; Jeraj, R.; Curran, W.J.; Bradley, J.D. Treatment Design and Rationale for a Randomized Trial of Cisplatin and Etoposide Plus Thoracic Radiotherapy Followed by Nivolumab or Placebo for Locally Advanced Non-Small-Cell Lung Cancer (RTOG 3505). Clin. Lung Cancer 2017, 18, 333–339. [Google Scholar] [CrossRef]
- Herbst, R.S.; Majem, M.; Barlesi, F.; Carcereny, E.; Chu, Q.; Monnet, I.; Sanchez-Hernandez, A.; Dakhil, S.; Camidge, D.R.; Winzer, L.; et al. COAST: An Open-Label, Phase II, Multidrug Platform Study of Durvalumab Alone or in Combination With Oleclumab or Monalizumab in Patients With Unresectable, Stage III Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 3383–3393. [Google Scholar] [CrossRef]
- Bradley, J.D.; Nishio, M.; Okamoto, I.; Newton, M.D.; Trani, L.; Shire, N.J.; Gu, Y.; Dennis, P.A.; Lee, K.H. PACIFIC2: Phase 3 study of concurrent durvalumab and platinum-based chemoradiotherapy in patients with unresectable, stage III NSCLC. J. Clin. Oncol. 2019, 37, 15. [Google Scholar] [CrossRef]
- Jabbour, S.K.; Lee, K.H.; Frost, N.; Breder, V.; Kowalski, D.M.; Pollock, T.; Levchenko, E.; Reguart, N.; Martinez-Marti, A.; Houghton, B.; et al. Pembrolizumab Plus Concurrent Chemoradiation Therapy in Patients With Unresectable, Locally Advanced, Stage III Non–Small Cell Lung Cancer. JAMA Oncol. 2021, 7, 1351–1359. [Google Scholar] [CrossRef]
- De Ruysscher, D.; Ramalingam, S.; Urbanic, J.; Gerber, D.E.; Tan, D.S.W.; Cai, J.; Li, A.; Peters, S. CheckMate 73L: A Phase 3 Study Comparing Nivolumab Plus Concurrent Chemoradiotherapy Followed by Nivolumab With or Without Ipilimumab Versus Concurrent Chemoradiotherapy Followed by Durvalumab for Previously Untreated, Locally Advanced Stage III Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2022, 23, e264–e268. [Google Scholar]
- Ross, H.J.; Kozono, D.; Wang, X.F.; Urbanic, J.J.; Williams, T.M.; Nelson, G.D.; Carbone, D.P.; Chung, D.; Robb, R.; Byun, W.Y.; et al. Atezolizumab Before and After Chemoradiation for Unresectable Stage III Non–Small Cell Lung Cancer. JAMA Oncol. 2024, 10, 1212–1219. [Google Scholar] [CrossRef]
- Hwang, W.L.; Pike, L.R.G.; Royce, T.J.; Mahal, B.A.; Loeffler, J.S. Safety of combining radiotherapy with immune-checkpoint inhibition. Nat. Rev. Clin. Oncol. 2018, 15, 477–494. [Google Scholar] [CrossRef]
- Hanania, A.N.; Mainwaring, W.; Ghebre, Y.T.; Hanania, N.A.; Ludwig, M. Radiation-Induced Lung Injury: Assessment and Management. Chest 2019, 156, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) v5.0. 27 November 2017. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 15 May 2025).
- Vokes, E.E.; Mornex, F.; Sezer, A.; Cheng, Y.; Fang, J.; Baz, D.V.; Cil, T.; Adjei, A.A.; Ahn, M.J.; Barlesi, F.; et al. Bintrafusp Alfa with CCRT Followed by Bintrafusp Alfa Versus Placebo With CCRT Followed by Durvalumab in Patients With Unresectable Stage III NSCLC: A Phase 2 Randomized Study. J. Thorac. Oncol. 2024, 19, 285–296. [Google Scholar] [CrossRef]
- Käsmann, L.; Eze, C.; Taugner, J.; Nieto, A.; Hofstetter, K.; Kröninger, S.; Guggenberger, J.; Kenndoff, S.; Flörsch, B.; Tufman, A.; et al. Concurrent/sequential versus sequential immune checkpoint inhibition in inoperable large stage III non-small cell lung cancer patients treated with chemoradiotherapy: A prospective observational study. J. Cancer Res. Clin. Oncol. 2023, 149, 7393–7403. [Google Scholar] [CrossRef]
- Kauffmann-Guerrero, D.; Taugner, J.; Eze, C.; Käsmann, L.; Li, M.; Tufman, A.; Manapov, F. Clinical Management and Outcome of Grade III Pneumonitis after Chemoradioimmunotherapy for Inoperable Stage III Non-Small Cell Lung Cancer-A Prospective Longitudinal Assessment. Diagnostics 2021, 11, 1968. [Google Scholar] [CrossRef]
- Wass, R.; Hochmair, M.; Kaiser, B.; Grambozov, B.; Feurstein, P.; Weiß, G.; Moosbrugger, R.; Sedlmayer, F.; Lamprecht, B.; Studnicka, M.; et al. Durvalumab after Sequential High Dose Chemoradiotherapy versus Standard of Care (SoC) for Stage III NSCLC: A Bi-Centric Trospective Comparison Focusing on Pulmonary Toxicity. Cancers 2022, 14, 3226. [Google Scholar] [CrossRef]
- Sugimoto, T.; Fujimoto, D.; Sato, Y.; Tamiya, M.; Yokoi, T.; Taniguchi, Y.; Hino, A.; Hata, A.; Uchida, J.; Fukuda, Y.; et al. Prospective multicenter cohort study of durvalumab for patients with unresectable stage III non-small cell lung cancer and grade 1 radiation pneumonitis. Lung Cancer 2022, 171, 3–8. [Google Scholar] [CrossRef]
- Thor, M.; Lee, C.; Sun, L.; Patel, P.; Apte, A.; Grkovski, M.; Shepherd, A.F.; Gelblum, D.Y.; Wu, A.J.; Simone, C.B., 2nd; et al. An 18F-FDG PET/CT and Mean Lung Dose Model to Predict Early Radiation Pneumonitis in Stage III Non-Small Cell Lung Cancer Patients Treated with Chemoradiation and Immunotherapy. J. Nucl. Med. 2024, 65, 520–526. [Google Scholar] [CrossRef]
- Smesseim, I.; Mets, O.M.; Daniels, J.M.A.; Bahce, I.; Senan, S. Diagnosis and management of pneumonitis following chemoradiotherapy and immunotherapy in stage III non-small cell lung cancer. Radiother. Oncol. 2024, 194, 110147. [Google Scholar] [CrossRef]
- Landman, Y.; Jacobi, O.; Kurman, N.; Yariv, O.; Peretz, I.; Rotem, O.; Dudnik, E.; Zer, A.; Allen, A.M. Durvalumab after concurrent chemotherapy and high-dose radiotherapy for locally advanced non-small cell lung cancer. OncoImmunology 2021, 10, 1959979. [Google Scholar] [CrossRef] [PubMed]
- Trinh, J.Q.; Xiong, Y.; Smith, L.M.; Abughanimeh, O.; Marr, A.S.; Ganti, A.K. Durvalumab Outcomes in Stage III Non-small Cell Lung Cancer: A Single-institution Study. Anticancer Res. 2024, 44, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Holzgreve, A.; Taugner, J.; Käsmann, L.; Müller, P.; Tufman, A.; Reinmuth, N.; Li, M.; Winkelmann, M.; Unterrainer, L.M.; Nieto, A.E.; et al. Metabolic patterns on [(18)F]FDG PET/CT in patients with unresectable stage III NSCLC undergoing chemoradiotherapy ± durvalumab maintenance treatment. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 2466–2476. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Odagiri, K.; Tabuchi, Y.; Okamoto, H.; Shimokawa, T.; Nakamura, Y.; Hata, M. Patterns and Incidence of Pneumonitis and Initial Treatment Outcomes with Durvalumab Consolidation Therapy after Radical Chemoradiotherapy for Stage III Non-Small Cell Lung Cancer. Cancers 2024, 16, 1162. [Google Scholar] [CrossRef]
- Edwards, D.M.; Sankar, K.; Alseri, A.; Jiang, R.; Schipper, M.; Miller, S.; Dess, K.; Strohbehn, G.W.; Elliott, D.A.; Moghanaki, D.; et al. Pneumonitis After Chemoradiotherapy and Adjuvant Durvalumab in Stage III Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2024, 118, 963–970. [Google Scholar] [CrossRef]
- Altan, M.; Soto, F.; Xu, T.; Wilson, N.; Franco-Vega, M.C.; Simbaqueba Clavijo, C.A.; Shannon, V.R.; Faiz, S.A.; Gandhi, S.; Lin, S.H.; et al. Pneumonitis After Concurrent Chemoradiation and Immune Checkpoint Inhibition in Patients with Locally Advanced Non-small Cell Lung Cancer. Clin. Oncol. 2023, 35, 630–639. [Google Scholar] [CrossRef]
- Horinouchi, H.; Atagi, S.; Oizumi, S.; Ohashi, K.; Kato, T.; Kozuki, T.; Seike, M.; Sone, T.; Sobue, T.; Tokito, T.; et al. Real-world outcomes of chemoradiotherapy for unresectable Stage III non-small cell lung cancer: The SOLUTION study. Cancer Med. 2020, 9, 6597–6608. [Google Scholar] [CrossRef]
- Zhao, L.; Zhao, Z.; Yan, X.; Wu, F.; Sun, N.; Guo, R.; Yu, S.; Hu, X.; Feng, J. Comparison of Efficacy and Safety of First-Line Treatment Options for Unresectable Stage III Non-Small Cell Lung Cancer: A Retrospective Analysis. Int. J. Clin. Pract. 2024, 2024, 8585035. [Google Scholar] [CrossRef]
- Kim, D.W.; Chul Cho, B.; Pachipala, K.; Kim, S.W.; Wang, C.L.; Chang, G.C.; Ahn, M.J.; Alvarez, R.; Chiu, C.H.; Trigo, J.; et al. Durvalumab in combination with chemoradiotherapy for patients with unresectable stage III non-small-cell lung cancer: Results from the phase 1 CLOVER study. Lung Cancer 2024, 190, 107530. [Google Scholar] [CrossRef]
- Jabbour, S.K.; Berman, A.T.; Decker, R.H.; Lin, Y.; Feigenberg, S.J.; Gettinger, S.N.; Aggarwal, C.; Langer, C.J.; Simone, C.B., 2nd; Bradley, J.D.; et al. Phase 1 Trial of Pembrolizumab Administered Concurrently With Chemoradiotherapy for Locally Advanced Non-Small Cell Lung Cancer: A Nonrandomized Controlled Trial. JAMA Oncol. 2020, 6, 848–855. [Google Scholar] [CrossRef]
- Peters, S.; Felip, E.; Dafni, U.; Belka, C.; Guckenberger, M.; Irigoyen, A.; Nadal, E.; Becker, A.; Vees, H.; Pless, M.; et al. Safety evaluation of nivolumab added concurrently to radiotherapy in a standard first line chemo-radiotherapy regimen in stage III non-small cell lung cancer-The ETOP NICOLAS trial. Lung Cancer 2019, 133, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-term results of NRG oncology RTOG 0617: Standard-versus high-dose chemoradiotherapy with or without cetuximab for unresectable stage III non-small-cell lung cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Guan, S.; Sun, J.; Wang, Y.; Han, S.; Chen, C.; Yue, D.; Huang, Y.; Ren, K.; Wang, J.; Wang, J.; et al. Chemoradiotherapy versus surgery after neoadjuvant chemoimmunotherapy in patients with stage III NSCLC: A real-world multicenter retrospective study. Cancer Immunol. Immunother. 2024, 73, 120. [Google Scholar] [CrossRef]
- Guan, S.; Ren, K.; Zhang, X.; Yan, M.; Li, X.; Zhao, L. Concurrent chemoradiotherapy versus radiotherapy alone after induction chemoimmunotherapy for stage III NSCLC patients who did not undergo surgery: A single institution retrospective study. Radiat. Oncol. 2023, 18, 122. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, T.; Wang, J.; Zhou, Z.; Liu, W.; Xiao, Z.; Deng, L.; Feng, Q.; Wang, X.; Lv, J.; et al. Induction Immune Checkpoint Inhibitors and Chemotherapy Before Definitive Chemoradiation Therapy for Patients With Bulky Unresectable Stage III Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2023, 116, 590–600. [Google Scholar] [CrossRef]
- Eifert, G.H.; Craill, L.; Carey, E.; O’Connor, C. Affect modification through evaluative conditioning with music. Behav. Res. Ther. 1988, 26, 321–330. [Google Scholar] [CrossRef]
- Horita, N.; Yamamoto, S.; Mizuki, Y.; Kawagoe, T.; Mihara, T.; Yamashiro, T. Minimal Clinically Important Difference (MCID) of Effect Sizes other than Mean Difference. J. Clin. Quest 2024, 1, 116–127. [Google Scholar] [CrossRef]
- Frank, A.J.; Dagogo-Jack, I.; Dobre, I.A.; Tait, S.; Schumacher, L.; Fintelmann, F.J.; Fingerman, L.M.; Keane, F.K.; Montesi, S.B. Management of Lung Cancer in the Patient with Interstitial Lung Disease. Oncologist 2023, 28, e314. [Google Scholar] [CrossRef]
- Eom, J.S.; Song, W.J.; Yoo, H.; Jeong, B.H.; Lee, H.Y.; Koh, W.J.; Jeon, K.; Park, H.Y. Chronic obstructive pulmonary disease severity is associated with severe pneumonia. Ann. Thorac. Med. 2015, 10, 105–111. [Google Scholar]
- Ewig, S.; Birkner, N.; Strauss, R.; Schaefer, E.; Pauletzki, J.; Bischoff, H.; Schraeder, P.; Welte, T.; Hoeffken, G. New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality. Thorax 2009, 64, 1062–1069. [Google Scholar] [CrossRef]
- Collins, G.S.; Ogundimu, E.O.; Altman, D.G. Sample size considerations for the external validation of a multivariable prognostic model: A resampling study. Stat. Med. 2016, 35, 214–226. [Google Scholar] [CrossRef]
- Faivre-Finn, C.; Spigel, D.R.; Senan, S.; Langer, C.J.; Raben, D.; Perez, B.; Özgüroğlu, M.; Daniel, D.; Villegas, A.; Vicente, D.; et al. Efficacy and safety evaluation based on time from completion of radiotherapy to randomization with durvalumab or placebo in pts from PACIFIC. Eur. Soc. Med. Oncol. 2018, 29, viii488. [Google Scholar] [CrossRef]
- Wegner, R.E.; Abel, S.; Hasan, S.; Hasan, S.; White, R.J.; Finley, G.; Monga, D.; Colonias, A.; Verma, V. Time from stereotactic body radiotherapy to immunotherapy as a predictor for outcome in metastatic non small cell lung cancer. J. Clin. Oncol. 2019, 37, 15. [Google Scholar] [CrossRef]
- Massaro, M.; Franceschini, D.; Spoto, R.; Dominici, L.; Franzese, C.; Baldaccini, D.; Marini, B.; di Cristina, L.; Marzo, M.A.; Lo Faro, L.; et al. Locally Advanced Non-Small Cell Lung Cancer: Clinical Outcome, Toxicity and Predictive Factors in Patients Treated with Hypofractionated Sequential or Exclusive Radiotherapy. Curr. Oncol. 2022, 29, 4893–4901. [Google Scholar] [CrossRef]
- Zhu, Z.F.; Fan, M.; Wu, K.L.; Zhao, K.L.; Yang, H.J.; Chen, G.Y.; Jiang, G.L.; Wang, L.J.; Zhao, S.; Fu, X.L. A phase II trial of accelerated hypofractionated three-dimensional conformal radiation therapy in locally advanced non-small cell lung cancer. Radiother. Oncol. 2011, 98, 304–308. [Google Scholar] [CrossRef]
- Mouw, K.W.; Konstantinopoulos, P.A. From checkpoint to checkpoint: DNA damage ATR/Chk1 checkpoint signalling elicits PD-L1 immune checkpoint activation. Br. J. Cancer 2018, 118, 933–935. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhou, J.; Verma, V.; Liu, X.; Wu, M.; Yu, J.; Chen, D. Crossed Pathways for Radiation-Induced and Immunotherapy-Related Lung Injury. Front. Immunol. 2021, 12, 774807. [Google Scholar] [CrossRef]
- Wu, F.; Zhang, Z.; Wang, M.; Ma, Y.; Verma, V.; Xiao, C.; Zhong, T.; Chen, X.; Wu, M.; Yu, J.; et al. Cellular Atlas of Senescent Lineages in Radiation- or Immunotherapy-Induced Lung Injury by Single-Cell RNA-Sequencing Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2023, 116, 1175–1189. [Google Scholar] [CrossRef]
- Zhao, M.; Hou, W.; Pu, D.; Li, Z.; Tu, L.; Ow, C.J.L.; Tian, J.; Li, W. Impact of Pulmonary microbiota on lung cancer treatment-related pneumonia. J. Cancer 2024, 15, 4503–4512. [Google Scholar] [CrossRef]
- Milla, C.E.; Zirbes, J. Pulmonary complications of endocrine and metabolic disorders. Paediatr. Respir. Rev. 2012, 13, 23–28. [Google Scholar] [CrossRef]
- Zhou, C.; Yu, J. Chinese expert consensus on diagnosis and treatment of radiation pneumonitis. Precis. Radiat. Oncol. 2022, 6, 262–271. [Google Scholar] [CrossRef]
- Fucà, G.; Galli, G.; Poggi, M.; Lo Russo, G.; Proto, C.; Imbimbo, M.; Ferrara, R.; Zilembo, N.; Ganzinelli, M.; Sica, A.; et al. Modulation of peripheral blood immune cells by early use of steroids and its association with clinical outcomes in patients with metastatic non-small cell lung cancer treated with immune checkpoint inhibitors. ESMO Open 2019, 4, e000457. [Google Scholar] [CrossRef] [PubMed]
- Elkrief, A.; Derosa, L.; Kroemer, G.; Zitvogel, L.; Routy, B. The negative impact of antibiotics on outcomes in cancer patients treated with immunotherapy: A new independent prognostic factor? Ann. Oncol. 2019, 30, 1572–1579. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R. Mapping of global, regional and national incidence, mortality and mortality-to-incidence ratio of lung cancer in 2020 and 2050. Int. J. Clin. Oncol. 2022, 27, 665–675. [Google Scholar] [CrossRef]
- Liu, T.; Li, S.; Ding, S.; Qiu, J.; Ren, C.; Chen, J.; Wang, H.; Wang, X.; Li, G.; He, Z.; et al. Comparison of post-chemoradiotherapy pneumonitis between Asian and non-Asian patients with locally advanced non-small cell lung cancer: A systematic review and meta-analysis. eClinicalMedicine 2023, 64, 102246. [Google Scholar] [CrossRef]

| Study | Author (Year) | Phase | Study Period | Country | Type of Study | Group | Treatment | Evaluated Patients (n) | ≥Grade 2 RP (n) | ≥Grade 3 RP (n) |
|---|---|---|---|---|---|---|---|---|---|---|
| COAST (NCT03822351) | Roy S Herbst (2022) [5] | II | 2018–2020 | Multicenter | Prospective | ICI following cCRT | Durvalumab following cCRT | 66 | 11 | 0 |
| HCRN LUN 14-179 * | Greg A Durm (2020) [2] | II | 2015–2019 | USA | Prospective | ICI following cCRT | Pembrolizumab following cCRT | 93 | 16 | 6 |
| NCT03840902 | Everett E Vokes (2024) [15] | II | 2019–2021 | Multicenter | Prospective | ICI following cCRT | Durvalumab following cCRT | 77 | 20 | - |
| PACIFIC (NCT02125461) | Scott J Antonia (2017) [1] | III | 2014–2016 | Multicenter | Prospective | ICI following cCRT | Durvalumab following cCRT | 475 | 161 | 20 |
| RTOG 3505 (NCT02768558) | David E Gerber (2017) [4] | III | 2016–2020 | USA | Prospective | ICI following cCRT | Nivolumab following cCRT | 3 | 1 | - |
| RWS | Lukas Käsmann (2023) [16] | 2016–2020 | Germany | Prospective | ICI following cCRT | Nivolumab following cCRT | 11 | 7 | 2 | |
| RWS | Diego Kauffmann-Guerrero (2021) [17] | NA | Germany | Prospective | ICI following cCRT | ICI following cCRT | 38 | - | 6 | |
| RWS | Romana Wass (2022) [18] | NA | Austria | Prospective | ICI following cCRT | Durvalumab following cCRT | 36 | 10 | - | |
| RWS | Takeya Sugimoto (2022) [19] | 2019–2019 | Japan | Prospective | ICI following cCRT | Durvalumab following cCRT | 35 | 11 | 1 | |
| RWS | Maria Thor (2024) [20] | 2017–2021 | USA | Retrospective | ICI following cCRT | Durvalumab following cCRT | 160 | 38 | - | |
| RWS | I Smesseim (2024) [21] | 2018–2021 | Netherlands | Retrospective | ICI following cCRT | Durvalumab following cCRT | 45 | 14 | - | |
| RWS | Yosef Landman (2021) [22] | 2018–2020 | Israel | Retrospective | ICI following cCRT | Durvalumab following cCRT | 39 | 6 | - | |
| RWS | Jonathan Q Trinh (2024) [23] | 2012–2022 | USA | Retrospective | ICI following cCRT | Durvalumab following cCRT | 44 | 11 | - | |
| RWS | Adrien Holzgreve (2024) [24] | NA | Germany | Retrospective | ICI following cCRT | Durvalumab following cCRT | 16 | 8 | - | |
| RWS | Mizuki Sato (2024) [25] | 2013–2022 | Japan | Retrospective | ICI following cCRT | Durvalumab following cCRT | 69 | 28 | 7 | |
| RWS | Donna M Edwards (2024) [26] | 2015–2021 | USA | Retrospective | ICI following cCRT | Durvalumab following cCRT | 1005 | 222 | 105 | |
| RWS | M Altan (2023) [27] | 2018–2021 | USA | Retrospective | ICI following cCRT | Durvalumab following cCRT | 140 | 32 | 8 | |
| RWS | Hidehito Horinouchi (2020) [28] | 2013–2015 | Japan | Retrospective | ICI following cCRT | Durvalumab following cCRT | 306 | 73 | 48 | |
| RWS | Luqing Zhao (2024) [29] | 2013–2023 | China | Retrospective | ICI following cCRT | ICI following cCRT | 37 | 3 | 1 | |
| CLOVER study (NCT03509012) | Dong-Wan Kim (2024) [30] | I | 2018–2020 | Multicenter | Prospective | ICI concurrent with cCRT | Durvalumab concurrent with cCRT | 64 | 11 | 6 |
| KEYNOTE-799 (NCT03631784) | Salma K Jabbour (2021) [7] | II | 2018–2020 | Multicenter | Prospective | ICI concurrent with cCRT | Pembrolizumab concurrent with cCRT | 214 | 47 | 13 |
| NCT02621398 | Salma K Jabbour (2020) [31] | I | 2016–2018 | USA | Prospective | ICI concurrent with cCRT | Pembrolizumab concurrent with cCRT | 12 | 4 | 2 |
| NICOLAS (NCT02434081) | S Peters (2019) [32] | III | 2016–2018 | Multicenter | Prospective | ICI concurrent with cCRT | Nivolumab concurrent with cCRT | 80 | 27 | 8 |
| RTOG 0617 (NCT00533949) | Jeffrey D Bradley (2020) [33] | III | 2007–2013 | Multicenter | Prospective | ICI concurrent with cCRT | Cetuximab concurrent with cCRT | 134 | 44 | 11 |
| RWS | Luqing Zhao (2024) [29] | 2013–2023 | China | Retrospective | ICI concurrent with cCRT | ICI concurrent with cCRT | 64 | 9 | 2 | |
| AFT-16 (NCT03102242) | Helen J. Ross (2024) [9] | II | 2017–2019 | USA | Prospective | ICI prior to cCRT | Atezolizumab prior to cCRT | 64 | 15 | 5 |
| RWS | Song Guan (2024) [34] | 2018–2022 | China | Retrospective | ICI prior to cCRT | ICI prior to cCRT | 153 | 89 | 16 | |
| RWS | Song Guan (2023) [35] | 2018–2021 | China | Retrospective | ICI prior to cCRT | ICI prior to cCRT | 21 | 14 | 0 | |
| RWS | Yu Wang (2023) [36] | 2018–2020 | China | Retrospective | ICI prior to cCRT | ICI prior to cCRT | 75 | 27 | 7 |
| Characteristics | Total (n = 170) | ICI Following cCRT (n = 117) | ICI Concurrent with cCRT (n = 23) | ICI Prior to cCRT (n = 30) | p Value |
|---|---|---|---|---|---|
| Gender (n) | 0.746 | ||||
| Female | 13 | 10 | 1 | 2 | |
| Male | 157 | 107 | 22 | 28 | |
| Age (median, IQR) (y) | 61.0 (55.0, 68.0) | 61.0 (55.5, 67.0) | 62.0 (57.0, 69.0) | 62.0 (53.8, 69.0) | 0.810 |
| BMI (mean ± SD) (kg/m2) | 24.53 ± 3.04 | 24.48 ± 3.01 | 24.57 ± 2.80 | 24.69 ± 3.40 | 0.946 |
| Systolic pressure (median, IQR) (mmHg) | 125 (120, 134) | 125 (121, 133.5) | 130 (122, 135) | 124 (115, 135) | 0.352 |
| Diastolic pressure (median, IQR) (mmHg) | 77 (73.75, 84) | 77 (73, 84) | 78 (74, 87) | 76 (72.75, 86.5) | 0.913 |
| NRS2002 score (median, IQR) | 1 (1, 2) | 1 (1, 2) | 1 (1, 2) | 1 (1, 2) | 0.352 |
| ECOG PS (n) | 0.148 | ||||
| 0 | 106 | 77 | 15 | 14 | |
| 1 | 64 | 40 | 8 | 16 | |
| ICI (n) | <0.001 | ||||
| PD1 inhibitors | 113 | 68 | 15 | 30 | |
| PD-L1 inhibitors | 57 | 49 | 8 | 0 | |
| Smoking history (n) | 0.868 | ||||
| No | 52 | 37 | 6 | 9 | |
| Yes | 118 | 80 | 17 | 21 | |
| Drinking history (n) | 0.673 | ||||
| No | 94 | 65 | 11 | 18 | |
| Yes | 76 | 52 | 12 | 12 | |
| History of hypertension (n) | 0.515 | ||||
| No | 124 | 83 | 19 | 22 | |
| Yes | 46 | 34 | 4 | 8 | |
| History of heart attack (n) | 0.250 | ||||
| No | 151 | 101 | 22 | 28 | |
| Yes | 19 | 16 | 1 | 2 | |
| History of diabetes (n) | 0.626 | ||||
| No | 158 | 108 | 21 | 29 | |
| Yes | 12 | 9 | 2 | 1 | |
| Pathological type (n) | 0.009 | ||||
| Squamous carcinoma | 117 | 72 | 20 | 25 | |
| Adenocarcinoma | 53 | 45 | 3 | 5 | |
| TNM stage (n) | 0.381 | ||||
| IIIA | 65 | 40 | 9 | 16 | |
| IIIB | 83 | 62 | 11 | 10 | |
| IIIC | 22 | 15 | 3 | 4 | |
| Location (n) | 0.627 | ||||
| Upper lobe | 109 | 76 | 16 | 17 | |
| Middle and lower lobe | 61 | 41 | 7 | 13 | |
| Location, left or right lungs (n) | 0.335 | ||||
| Left lung | 83 | 53 | 12 | 18 | |
| Right lung | 87 | 64 | 11 | 12 | |
| ≥Grade 2 RP (n) | 0.207 | ||||
| No | 94 | 70 | 10 | 14 | |
| Yes | 76 | 47 | 13 | 16 | |
| ≥Grade 3 RP (n) | 0.445 | ||||
| No | 157 | 110 | 20 | 27 | |
| Yes | 13 | 7 | 3 | 3 | |
| Dose per fraction (median, IQR) (Gy) | 2 (2, 2) | 2 (2, 2) | 2 (2, 2) | 2 (2, 2) | 0.444 |
| Total dose (median, IQR) (Gy) | 60 (56, 60) | 60 (56, 60) | 60 (60, 60) | 60 (54, 60) | 0.290 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, Y.; Mo, Y.; Li, P.; Liang, X.; Yu, J.; Chen, D. Early Immune Checkpoint Inhibitor Administration Increases the Risk of Radiation-Induced Pneumonitis in Patients with Stage III Unresectable NSCLC Undergoing Chemoradiotherapy. Cancers 2025, 17, 1711. https://doi.org/10.3390/cancers17101711
Qin Y, Mo Y, Li P, Liang X, Yu J, Chen D. Early Immune Checkpoint Inhibitor Administration Increases the Risk of Radiation-Induced Pneumonitis in Patients with Stage III Unresectable NSCLC Undergoing Chemoradiotherapy. Cancers. 2025; 17(10):1711. https://doi.org/10.3390/cancers17101711
Chicago/Turabian StyleQin, Yiwei, You Mo, Pengwei Li, Xinyi Liang, Jinming Yu, and Dawei Chen. 2025. "Early Immune Checkpoint Inhibitor Administration Increases the Risk of Radiation-Induced Pneumonitis in Patients with Stage III Unresectable NSCLC Undergoing Chemoradiotherapy" Cancers 17, no. 10: 1711. https://doi.org/10.3390/cancers17101711
APA StyleQin, Y., Mo, Y., Li, P., Liang, X., Yu, J., & Chen, D. (2025). Early Immune Checkpoint Inhibitor Administration Increases the Risk of Radiation-Induced Pneumonitis in Patients with Stage III Unresectable NSCLC Undergoing Chemoradiotherapy. Cancers, 17(10), 1711. https://doi.org/10.3390/cancers17101711