
FDG-PET in Chimeric Antigen Receptor T-Cell (CAR T-Cell) Therapy Toxicity: A Systematic Review

 ,
,  ,
,  ,
,  , ,
, ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Literature Search
2.2. Assessment of Methodological Quality
3. Results
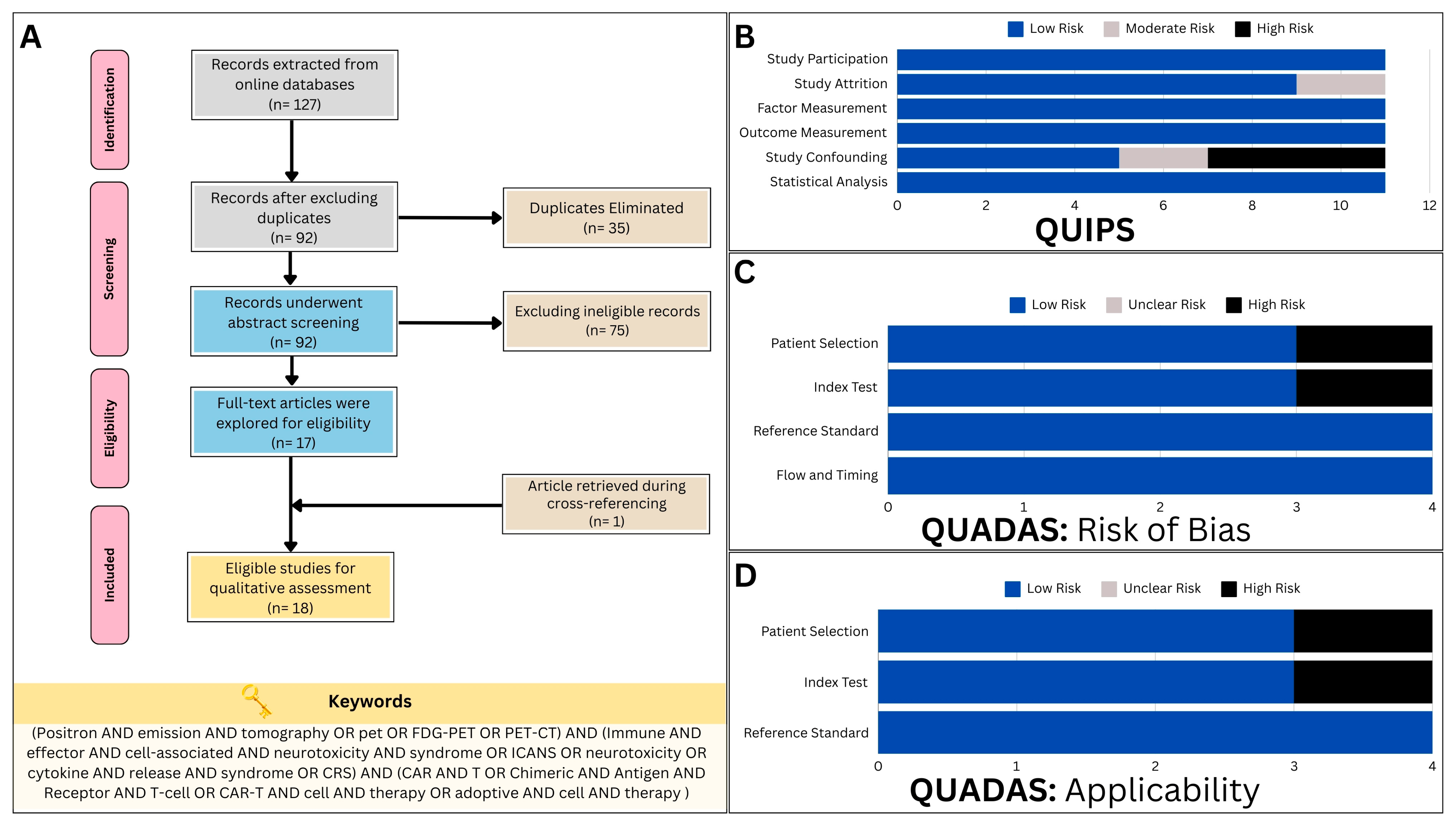
3.1. Search Results
3.2. Assessment of Methodological Quality and Risk of Bias
4. Systematic Review
4.1. Study Characteristics
4.2. Baseline PET for the Prediction of CAR T-Cell Therapy Toxicity
4.2.1. First Clinical Study
4.2.2. Unicentric Studies with Endorsing Evidence
4.2.3. Unicentric Studies with Negative Results
4.2.4. Multicentric Studies
4.2.5. Latest Research Evidence
4.2.6. General Summary
4.3. Diagnostic Utility
4.3.1. First Attempt to Detect Neurotoxicity via Brain [18F]FDG PET
4.3.2. Global Brain Hypometabolism
4.3.3. Frontal Predominant Encephalopathy
4.3.4. Functional Alterations Associated with Neurotoxicity
4.3.5. Irreversible Neurotoxicity
4.3.6. Tracking CAR T-Cell Therapy Toxicity Elsewhere
5. Discussion
5.1. Significance of the Current Review
5.2. Advancement of Preclinical Research
5.2.1. [18F]-Labeled Tracers
5.2.2. Non-[18F]-Labeled Tracers
5.2.3. Interleukin-Focused Imaging Approach
5.3. General Perspectives
5.4. Authors’ Thoughts on Mechanisms and Improvements
5.5. Study Limiations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Juretić, A. Cancer immunotherapy: Mechanism of action. Libr. Oncol. Croat. J. Oncol. 2017, 45, 38–42. [Google Scholar]
- Roy, R.; Singh, S.K.; Misra, S. Advancements in cancer immunotherapies. Vaccines 2022, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Wall, D.; Krueger, J. Chimeric antigen receptor T cell therapy comes to clinical practice. Curr. Oncol. 2020, 27, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.W.; Bhattarai, N. CAR-T Cell Therapy: Mechanism, Management, and Mitigation of Inflammatory Toxicities. Front. Immunol. 2021, 12, 693016. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Laetsch, T.W.; Buechner, J.; Rives, S.; Boyer, M.; Bittencourt, H.; Bader, P.; Verneris, M.R.; Stefanski, H.E.; Myers, G.D. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N. Engl. J. Med. 2018, 378, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Munoz, J.; Goy, A.; Locke, F.L.; Jacobson, C.A.; Hill, B.T.; Timmerman, J.M.; Holmes, H.; Jaglowski, S.; Flinn, I.W. KTE-X19 CAR T-cell therapy in relapsed or refractory mantle-cell lymphoma. N. Engl. J. Med. 2020, 382, 1331–1342. [Google Scholar] [CrossRef]
- Abramson, J.S.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Wang, M.; Arnason, J.; Mehta, A.; Purev, E.; Maloney, D.G.; Andreadis, C.; et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): A multicentre seamless design study. Article. Lancet 2020, 396, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Sengsayadeth, S.; Savani, B.N.; Oluwole, O.; Dholaria, B. Overview of approved CAR-T therapies, ongoing clinical trials, and its impact on clinical practice. EJHaem 2022, 3, 6–10. [Google Scholar] [CrossRef]
- Munshi, N.C.; Anderson Jr, L.D.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef]
- Berdeja, J.G.; Madduri, D.; Usmani, S.Z.; Jakubowiak, A.; Agha, M.; Cohen, A.D.; Stewart, A.K.; Hari, P.; Htut, M.; Lesokhin, A. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): A phase 1b/2 open-label study. Lancet 2021, 398, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Al-Ibraheem, A.; Mottaghy, F.M.; Juweid, M.E. PET/CT in Hodgkin Lymphoma: An Update. Semin. Nucl. Med. 2023, 53, 303–319. [Google Scholar] [CrossRef] [PubMed]
- Zanoni, L.; Bezzi, D.; Nanni, C.; Paccagnella, A.; Farina, A.; Broccoli, A.; Casadei, B.; Zinzani, P.L.; Fanti, S. PET/CT in Non-Hodgkin Lymphoma: An Update. Semin. Nucl. Med. 2023, 53, 320–351. [Google Scholar] [CrossRef]
- Al-Ibraheem, A.; Abdlkadir, A.S.; Juweid, M.E.; Al-Rabi, K.; Ma’koseh, M.; Abdel-Razeq, H.; Mansour, A. FDG-PET/CT in the monitoring of lymphoma immunotherapy response: Current status and future prospects. Cancers 2023, 15, 1063. [Google Scholar] [CrossRef] [PubMed]
- Linguanti, F.; Abenavoli, E.M.; Berti, V.; Lopci, E. Metabolic imaging in B-cell lymphomas during CAR-T cell therapy. Cancers 2022, 14, 4700. [Google Scholar] [CrossRef] [PubMed]
- Jain, T.; Bar, M.; Kansagra, A.J.; Chong, E.A.; Hashmi, S.K.; Neelapu, S.S.; Byrne, M.; Jacoby, E.; Lazaryan, A.; Jacobson, C.A. Use of chimeric antigen receptor T cell therapy in clinical practice for relapsed/refractory aggressive B cell non-Hodgkin lymphoma: An expert panel opinion from the American Society for Transplantation and Cellular Therapy. Biol. Blood Marrow Transplant. 2019, 25, 2305–2321. [Google Scholar] [CrossRef]
- Ruff, A.; Ballard, H.J.; Pantel, A.R.; Namoglu, E.C.; Hughes, M.E.; Nasta, S.D.; Chong, E.A.; Bagg, A.; Ruella, M.; Farwell, M.D. 18 F-fluorodeoxyglucose positron emission tomography/computed tomography following chimeric antigen receptor T-cell therapy in large B-cell lymphoma. Mol. Imaging Biol. 2021, 23, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Murad, V.; Kohan, A.; Ortega, C.; Prica, A.; Veit-Haibach, P.; Metser, U. Role of FDG PET/CT in Patients With Lymphoma Treated With Chimeric Antigen Receptor T-Cell Therapy: Current Concepts. Am. J. Roentgenol. 2023, 222, e2330301. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; group, C. The CARE guidelines: Consensus-based clinical case report guideline development. J. Clin. Epidemiol. 2014, 67, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Cheng, Y.; Zhang, K. Adherence of unpublished case reports to the Case Report (CARE) guidelines: A retrospective cross-sectional analysis of 139 case report manuscripts initially submitted to AME medical journals. AME Med. J. 2022, 7. [Google Scholar] [CrossRef]
- Gui, J.; Li, M.; Xu, J.; Zhang, X.; Mei, H.; Lan, X. [(18)F]FDG PET/CT for prognosis and toxicity prediction of diffuse large B-cell lymphoma patients with chimeric antigen receptor T-cell therapy. Eur. J. Nucl. Med. Mol. Imaging 2024. [Google Scholar] [CrossRef] [PubMed]
- Hong, R.M.; Yin, E.T.S.; Wang, L.Q.; Zhao, X.; Zhou, L.H.; Wang, G.F.; Zhang, M.M.; Zhao, H.L.; Wei, G.Q.; Wang, Y.Y.; et al. Tumor Burden Measured by 18F-FDG PET/CT in Predicting Efficacy and Adverse Effects of Chimeric Antigen Receptor T-Cell Therapy in Non-Hodgkin Lymphoma. Front. Oncol. 2021, 11, 9. [Google Scholar] [CrossRef] [PubMed]
- Marchal, E.; Palard-Novello, X.; Lhomme, F.; Meyer, M.E.; Manson, G.; Devillers, A.; Marolleau, J.P.; Houot, R.; Girard, A. Baseline 18F FDG PET features are associated with survival and toxicity in patients treated with CAR T cells for large B cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2024, 51, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Morbelli, S.; Gambella, M.; Raiola, A.M.; Ghiggi, C.; Bauckneht, M.; Raimondo, T.D.; Lapucci, C.; Sambuceti, G.; Inglese, M.; Angelucci, E. Brain FDG-PET findings in chimeric antigen receptor T-cell therapy neurotoxicity for diffuse large B-cell lymphoma. J. Neuroimaging 2023, 33, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Pensato, U.; Amore, G.; Muccioli, L.; Sammali, S.; Rondelli, F.; Rinaldi, R.; D’Angelo, R.; Nicodemo, M.; Mondini, S.; Sambati, L.; et al. CAR t-cell therapy in BOlogNa-NEUrotoxicity TReatment and Assessment in Lymphoma (CARBON-NEUTRAL): Proposed protocol and results from an Italian study. J. Neurol. 2023, 270, 2659–2673. [Google Scholar] [CrossRef]
- Rubin, D.B.; Danish, H.H.; Ali, A.B.; Li, K.; LaRose, S.; Monk, A.D.; Cote, D.J.; Spendley, L.; Kim, A.H.; Robertson, M.S.; et al. Neurological toxicities associated with chimeric antigen receptor T-cell therapy. Brain 2019, 142, 1334–1348. [Google Scholar] [CrossRef]
- Wang, J.; Hu, Y.; Yang, S.; Wei, G.; Zhao, X.; Wu, W.; Zhang, Y.; Zhang, Y.; Chen, D.; Wu, Z.; et al. Role of Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Predicting the Adverse Effects of Chimeric Antigen Receptor T Cell Therapy in Patients with Non-Hodgkin Lymphoma. Biol. Blood Marrow Transpl. 2019, 25, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Pensato, U.; Amore, G.; D’Angelo, R.; Rinaldi, R.; Nicodemo, M.; Rondelli, F.; Mondini, S.; Santoro, R.; Sammali, S.; Farolfi, A. Frontal predominant encephalopathy with early paligraphia as a distinctive signature of CAR T-cell therapy-related neurotoxicity. J. Neurol. 2022, 269, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Aghajan, Y.; Yu, A.; Jacobson, C.A.; Kim, A.I.; Kean, L.; Robertson, M.; Vaitkevicius, H. Myelopathy Because of CAR-T–Related Neurotoxicity Treated With Siltuximab. Neurol. Clin. Pract. 2021, 11, e944–e946. [Google Scholar] [CrossRef] [PubMed]
- Gust, J.; Finney, O.C.; Li, D.; Brakke, H.M.; Hicks, R.M.; Futrell, R.B.; Gamble, D.N.; Rawlings-Rhea, S.D.; Khalatbari, H.K.; Ishak, G.E. Glial injury in neurotoxicity after pediatric CD19-directed chimeric antigen receptor T cell therapy. Ann. Neurol. 2019, 86, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Luttwak, E.; Beyar-Katz, O.; Hazut Krauthammer, S.; Bar-On, Y.; Amit, O.; Gold, R.; Perry, C.; Avivi, I.; Ram, R. [18F] FDG PET-CT in patients with DLBCL treated with CAR-T cell therapy: A practical approach of reporting pre-and post-treatment studies. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Iacoboni, G.; Simó, M.; Villacampa, G.; Catalá, E.; Carpio, C.; Díaz-Lagares, C.; Vidal-Jordana, Á.; Bobillo, S.; Marín-Niebla, A.; Pérez, A. Prognostic impact of total metabolic tumor volume in large B-cell lymphoma patients receiving CAR T-cell therapy. Ann. Hematol. 2021, 100, 2303–2310. [Google Scholar] [CrossRef] [PubMed]
- Ligero, M.; Simó, M.; Carpio, C.; Iacoboni, G.; Balaguer-Montero, M.; Navarro, V.; Sánchez-Salinas, M.A.; Bobillo, S.; Marín-Niebla, A.; Iraola-Truchuelo, J. PET-based radiomics signature can predict durable responses to CAR T-cell therapy in patients with large B-cell lymphoma. EJHaem 2023, 4, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Voltin, C.-A.; Gödel, P.; Beckmann, L.; Heger, J.-M.; Kobe, C.; Kutsch, N.; Borchmann, P.; Dietlein, M.; Herrmann, K.; Stelljes, M. Outcome prediction in patients with large B-cell lymphoma undergoing chimeric antigen receptor T-cell therapy. HemaSphere 2023, 7, e817. [Google Scholar] [CrossRef] [PubMed]
- Ababneh, H.S.; Ng, A.K.; Abramson, J.S.; Soumerai, J.D.; Takvorian, R.W.; Frigault, M.J.; Patel, C.G. Metabolic parameters predict survival and toxicity in chimeric antigen receptor T-cell therapy-treated relapsed/refractory large B-cell lymphoma. Hematol. Oncol. 2023, 42, e3231. [Google Scholar] [CrossRef]
- Beuchat, I.; Danish, H.H.; Rubin, D.B.; Jacobson, C.; Robertson, M.; Vaitkevicius, H.; Lee, J.W. EEG findings in CAR T-cell-associated neurotoxicity: Clinical and radiological correlations. Neuro-Oncology 2022, 24, 313–325. [Google Scholar] [CrossRef]
- Derlin, T.; Schultze-Florey, C.; Werner, R.A.; Möhn, N.; Skripuletz, T.; David, S.; Beutel, G.; Eder, M.; Ross, T.L.; Bengel, F.M.; et al. 18F-FDG PET/CT of off-target lymphoid organs in CD19-targeting chimeric antigen receptor T-cell therapy for relapsed or refractory diffuse large B-cell lymphoma. Ann. Nucl. Med. 2021, 35, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; de Jong, D.; Das, J.P.; Widemon, R.S.; Braumuller, B.; Paily, J.; Deng, A.; Liou, C.; Roa, T.; Huang, A. Imaging the Side Effects of CAR T Cell Therapy: A Primer for the Practicing Radiologist. Acad. Radiol. 2023, 30, 2712–2727. [Google Scholar] [CrossRef]
- Sakemura, R.; Cox, M.J.; Bansal, A.; Roman, C.M.; Hefazi, M.; Vernon, C.J.; Glynn, D.L.; Pandey, M.K.; DeGrado, T.R.; Siegler, E.L.; et al. Dynamic Imaging of Chimeric Antigen Receptor T Cells with 18F Tetrafluoroborate Positron Emission Tomography/Computed Tomography. Jove-J. Vis. Exp. 2022, 180, e62334. [Google Scholar] [CrossRef] [PubMed]
- Weist, M.R.; Starr, R.; Aguilar, B.; Chea, J.; Miles, J.K.; Poku, E.; Gerdts, E.; Yang, X.; Priceman, S.J.; Forman, S.J.; et al. PET of Adoptively Transferred Chimeric Antigen Receptor T Cells with 89Zr-Oxine. J. Nucl. Med. 2018, 59, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Leland, P.; Kumar, D.; Nimmagadda, S.; Bauer, S.R.; Puri, R.K.; Joshi, B.H. Characterization of chimeric antigen receptor modified T cells expressing scFv-IL-13Rα2 after radiolabeling with 89Zirconium oxine for PET imaging. J. Transl. Med. 2023, 21, 14. [Google Scholar] [CrossRef] [PubMed]
- Brudno, J.N.; Kochenderfer, J.N. Recent advances in CAR T-cell toxicity: Mechanisms, manifestations and management. Blood Rev. 2019, 34, 45–55. [Google Scholar] [CrossRef]
- Neill, L.; Rees, J.; Roddie, C. Neurotoxicity—CAR T-cell therapy: What the neurologist needs to know. Pract. Neurol. 2020, 20, 285–293. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| CARE Item 1 | Aghajan 2021 [33] | Gust 2019 [34] | Huang 2023 [42] |
|---|---|---|---|
| Title | 0 | 0 | 0 |
| Keywords | 0 | 1 | 1 |
| Abstract | 1 | 1 | 1 |
| Introduction | 1 | 1 | 1 |
| Patient information | 1 | 1 | 1 |
| Clinical findings | 1 | 1 | 1 |
| Timeline | 0 | 1 | 0 |
| Diagnostic assessment | 1 | 1 | 1 |
| Therapeutic intervention | 1 | 1 | 0 |
| Follow-up and outcome | 1 | 0 | 0 |
| Discussion | 0 | 0 | 0 |
| Patient perspective | 0 | 0 | 0 |
| Informed consent | 1 | 1 | 0 |
| Numerical score | 8 | 9 | 6 |
| Quality score | Intermediate quality | Intermediate quality | Intermediate quality |
| First Author (Year, Country) | Patients (M 1, F 2) | Age in Years | Cancer Type | Article Type (Design) | Institutional Experience | Patients Evaluated via PET | Explored Domain |
|---|---|---|---|---|---|---|---|
| Ababneh (2023, USA 3) [39] | 59 (33 M, 26 F) | 66 | LBCL 4 (r/r 5) | Original (R 6) | Monocentric | 59 Patients | Predictive |
| Beuchat (2022, USA) [40] | 91 (52 M, 29F) | 61 | NHL 7 | Original (R) | Monocentric | 8 Patients | Diagnostic |
| Derlin (2021, DE 8) [41] | 10 (6 M, 4 F) | 59 | DLBCL 9 (r/r) | Original (R) | Monocentric | 10 Patients | Predictive |
| Gui (2024, CN 10) [25] | 38 (23M, 15 F) | 55 | DLBCL 9 (r/r) | Original (R) | Monocentric | 38 Patients | Predictive |
| Hong (2021, CN) [26] | 41 (17 M, 24 F) | 44 | NHL (r/r) | Original (R) | Monocentric | 44 Patients | Predictive |
| Marchal (2024, FR 11) [27] | 56 (36 M, 20 F) | 60 | LBCL | Original (R) | Multicentric | 56 Patients | Predictive |
| Morbelli (2023, IT 12) [28] | 21 (10 M, 11 F) | 56 | DLBCL (rf 13) | Original (R) | Monocentric | 21 Patients | Predictive |
| Pensato (2023, IT) [29] | 46 (33 M, 13 F) | 56 | NHL | Original (P 14) | Monocentric | 6 Patients | Diagnostic |
| Rubin (2019, USA) [30] | 100 (61 M, 39 F) | 64 | HM 15 and Sarcoma | Original (P) | Monocentric | 6 Patients | Diagnostic |
| Wang (2019, CN) [31] | 19 (12 M, 7 F) | 43 | NHL | Original (R) | Monocentric | 19 Patients | Predictive |
| Pensato (2022, IT) [32] | 4 (1 M, 3 F) | 66 | DLBCL | Original (R) | Monocentric | 4 Patients | Diagnostic |
| Gust (2019, USA) [34] | 43 (21 M, 22 F) | 12 | B-ALL 16 | Original (P) | Monocentric | 1 Patient | Diagnostic |
| Cohen (2021, IL 17) [35] | 48 (25 M, 23F) | 68 | DLBCL (r/r) | Original (R) | Monocentric | 48 Patients | Predictive |
| Iacoboni (2021, ES 18) [36] | 35 (26 M, 9F) | 58 | LBCL (r/r) | Original (R) | Monocentric | 35 Patients | Predictive |
| Ligero (2023, ES) [37] | 93 (63 M, 30 F) | 59 | LBCL (r/r) | Original (R) | Monocentric | 93 Patients | Predictive |
| Voltin (2022, DE) [38] | 47 (29 M, 18 F) | 61 | LBCL (r/r) | Original (R) | Multicentric | 47 Patients | Predictive |
| Aghajan (2021, USA) [33] | 1 M | 30 | PMBCL 19 | Case report | NA 20 | 1 Patient | Diagnostic |
| Huang (2023, USA) [42] | 1 F | 47 | B-ALL | Review article | NA | 1 Patient | Diagnostic |
| Studies Reporting Unpredictability | Studies Reporting Predictability | ||
|---|---|---|---|
| First Author, Year | Examined PET Parameters | First Author, Year | Examined PET Parameters |
| Iacoboni, 2021 [36] | Baseline (SUVmax 1, TMTV 2) | Wang, 2019 [31] | Baseline (SUVmax, TMTV *, TLG *) |
| Cohen, 2021 [35] | Baseline (SUVmax, TMTV, TLG 3) | Derlin, 2021 [41] | Baseline (SUVmax *, TMTV, TLG) |
| Voltin, 2022 [38] | Baseline (SUVmax, TMTV) | Hong, 2021 [26] | Baseline (SUVmean 4*, TMTV *, TLG *) |
| Ligero, 2023 [37] | AI 5 radiomics | Marchal, 2024 [27] | Baseline (SUVmean; liver * and spleen *) |
| Morbelli, 2023 [28] | Baseline (TMTV *, TLG *) | ||
| Ababneh, 2023 [39] | Baseline (SUVmax *, TMTV *, TLG *) | ||
| Gui, 2024 [25] | Baseline (SUVmax *, TMTV, TLG *) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Ibraheem, A.; Abdlkadir, A.S.; Lopci, E.; Allouzi, S.; Paez, D.; Alkuwari, M.; Makoseh, M.; Novruzov, F.; Usmani, S.; Al-Rabi, K.; et al. FDG-PET in Chimeric Antigen Receptor T-Cell (CAR T-Cell) Therapy Toxicity: A Systematic Review. Cancers 2024, 16, 1728. https://doi.org/10.3390/cancers16091728
Al-Ibraheem A, Abdlkadir AS, Lopci E, Allouzi S, Paez D, Alkuwari M, Makoseh M, Novruzov F, Usmani S, Al-Rabi K, et al. FDG-PET in Chimeric Antigen Receptor T-Cell (CAR T-Cell) Therapy Toxicity: A Systematic Review. Cancers. 2024; 16(9):1728. https://doi.org/10.3390/cancers16091728
Chicago/Turabian StyleAl-Ibraheem, Akram, Ahmed Saad Abdlkadir, Egesta Lopci, Sudqi Allouzi, Diana Paez, Maryam Alkuwari, Mohammad Makoseh, Fuad Novruzov, Sharjeel Usmani, Kamal Al-Rabi, and et al. 2024. "FDG-PET in Chimeric Antigen Receptor T-Cell (CAR T-Cell) Therapy Toxicity: A Systematic Review" Cancers 16, no. 9: 1728. https://doi.org/10.3390/cancers16091728
APA StyleAl-Ibraheem, A., Abdlkadir, A. S., Lopci, E., Allouzi, S., Paez, D., Alkuwari, M., Makoseh, M., Novruzov, F., Usmani, S., Al-Rabi, K., & Mansour, A. (2024). FDG-PET in Chimeric Antigen Receptor T-Cell (CAR T-Cell) Therapy Toxicity: A Systematic Review. Cancers, 16(9), 1728. https://doi.org/10.3390/cancers16091728