
Perioperative Chemotherapy for Gastro-Esophageal or Gastric Cancer: Anthracyclin Triplets versus FLOT

 , , ,
, , , 

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
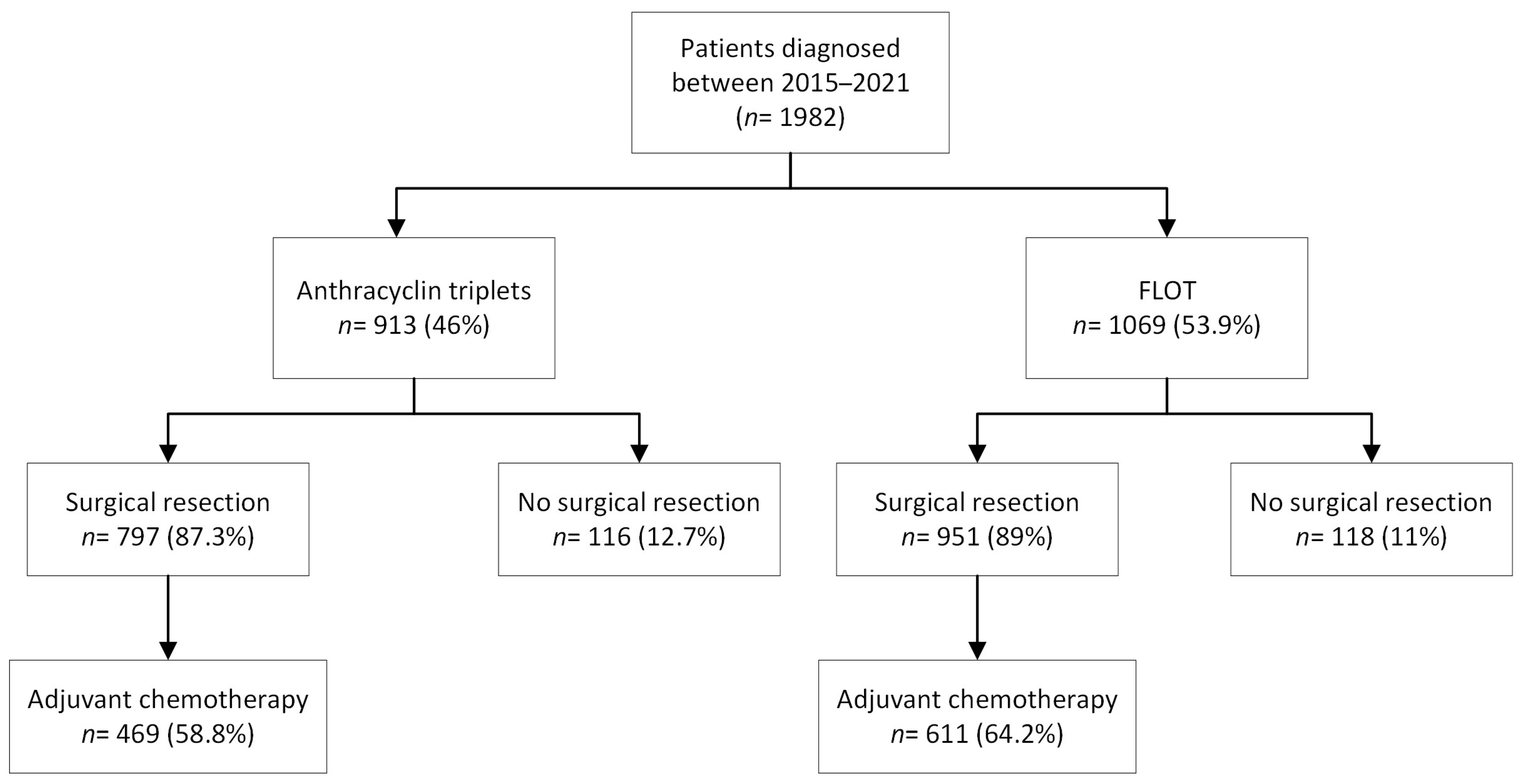
2.1. Study Design and Patients
2.2. Perioperative Chemotherapy
2.3. Pathological Assessment
2.4. Outcomes
2.5. Statistical Analyses
3. Results
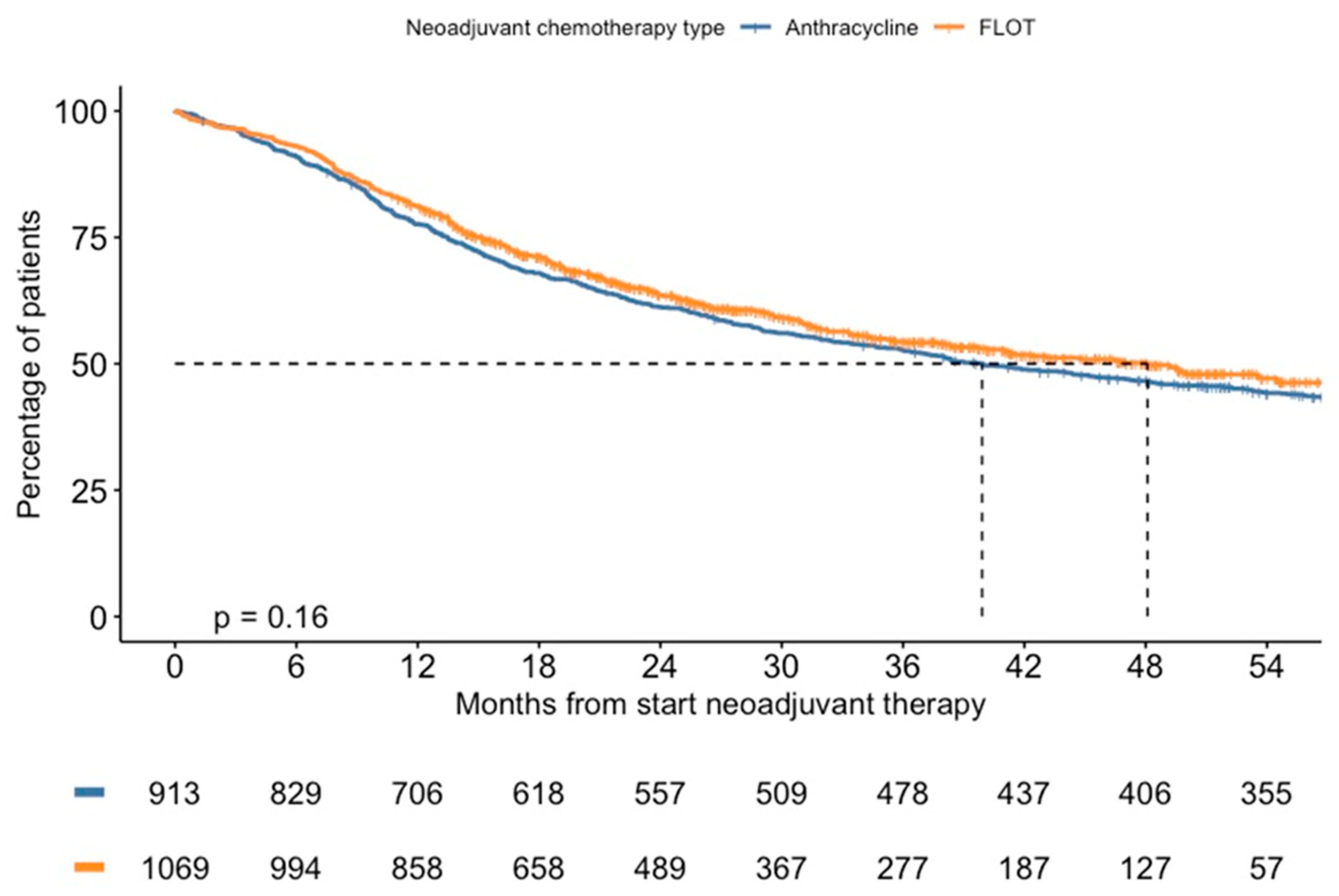
3.1. Survival and Prognostic Factors
3.2. Neoadjuvant Chemotherapy Cycles
3.3. Secondary Outcomes
3.4. Primary Surgical Resection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuijper, S.C.; Pape, M.; Vissers, P.A.; Jeene, P.M.; Kouwenhoven, E.A.; Haj Mohammad, N.; Ruurda, J.P.; Sosef, M.N.; Verhoeven, R.H.; van Laarhoven, H.W. Trends in Best-case, typical and worst-case survival scenarios of patients with non-metastatic esophagogastric cancer between 2006 and 2020: A population-based study. Int. J. Cancer 2023, 153, 33–43. [Google Scholar] [CrossRef] [PubMed]
- van Putten, M.; Nelen, S.D.; Lemmens, V.E.; Stoot, J.H.; Hartgrink, H.H.; Gisbertz, S.S.; Bilgen, E.J.S.; Heisterkamp, J.; A Verhoeven, R.H.; Nieuwenhuijzen, G.A.P. Overall survival before and after centralization of Gastric Cancer Surgery in the Netherlands. Br. J. Surg. 2018, 105, 1807–1815. [Google Scholar] [CrossRef]
- Integraal Kankercentrum Nederland. Slokdarm-en Maagkanker in Nederland. Available online: https://iknl.nl/getmedia/196f17c1-3c86-41b8-ad9d-721ab0ba81d8/slokdarm_maag_def.pdf (accessed on 26 July 2023).
- Dassen, A.E.; Dikken, J.L.; Bosscha, K.; Wouters, M.W.; Cats, A.; van de Velde, C.J.; Coebergh, J.-W.; Lemmens, V.E.P.P. Gastric cancer: Decreasing incidence but stable survival in the Netherlands. Acta Oncol. 2013, 53, 138–142. [Google Scholar] [CrossRef] [PubMed]
- van der Kaaij, R.T.; Koemans, W.J.; van Putten, M.; Snaebjornsson, P.; Luijten, J.C.; van Dieren, J.M.; Cats, A.; Lemmens, V.E.; Verhoeven, R.H.; van Sandick, J.W. A population-based study on intestinal and diffuse type adenocarcinoma of the oesophagus and stomach in the Netherlands between 1989 and 2015. Eur. J. Cancer 2020, 130, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.K.; Kang, W.K.; Shin, D.B.; Chen, J.; Xiong, J.; Wang, J.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as first-line therapy in patients with advanced gastric cancer: A randomised phase III noninferiority trial. Ann. Oncol. 2009, 20, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.; Saltz, L.; Twelves, C.; Van Cutsem, E.; Hoff, P.; Kang, Y.; Saini, J.P.; Gilberg, F.; Cunningham, D. Efficacy of capecitabine versus 5-fluorouracil in colorectal and gastric cancers: A meta-analysis of individual data from 6171 patients. Ann. Oncol. 2011, 22, 2604–2609. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Starling, N.; Rao, S.; Iveson, T.; Nicolson, M.; Coxon, F.; Middleton, G.; Daniel, F.; Oates, J.; Norman, A.R. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N. Engl. J. Med. 2008, 358, 36–46. [Google Scholar] [CrossRef]
- Okines, A.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v50–v54. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar]
- Al-Batran, S.; Homann, N.; Schmalenberg, H.; Kopp, H.; Haag, G.; Luley, K.; Schmiegel, W.H.; Folprecht, G.; Probst, S.; Prasnikar, N.; et al. Perioperative chemotherapy with docetaxel, oxaliplatin, and fluorouracil/leucovorin (FLOT) versus epirubicin, cisplatin, and fluorouracil or capecitabine (ECF/ECX) for resectable gastric or gastroesophageal junction (GEJ) adenocarcinoma (FLOT4-AIO): A multicenter, randomized phase 3 trial. J. Clin. Oncol. 2017, 35, 4004. [Google Scholar]
- NVMO-Commissie BOM. Perioperatieve chemotherapie met FLOT bij het resectabele lokaal gevorderde adenocarcinoom van de maag of gastro-oesofageale overgang. Med. Oncol. 2019, 22, 25–28. [Google Scholar]
- Pentheroudakis, G. Recent eUpdates to the ESMO Clinical Practice Guidelines on hepatocellular carcinoma, cancer of the pancreas, soft tissue and visceral sarcomas, cancer of the prostate and gastric cancer. Ann. Oncol. 2019, 30, 1395–1397. [Google Scholar] [CrossRef] [PubMed]
- International Union against Cancer (UICC). TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell: Chichester, UK, 2009. [Google Scholar]
- International Union against Cancer (UICC). TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Chichester, UK, 2017. [Google Scholar]
- College of American Pathologists. Protocol for the Examination of Specimens from Patients with Carcinoma of the Esophagus. Available online: https://documents.cap.org/protocols/cp-esophagus-17protocol-4000.pdf (accessed on 23 March 2023).
- Kim, H.-S.; Lee, S.; Kim, J.H. Real-world evidence versus randomized controlled trial: Clinical research based on Electronic Medical Records. J. Korean Med. Sci. 2018, 33, e213. [Google Scholar] [CrossRef] [PubMed]
- Giommoni, E.; Lavacchi, D.; Tirino, G.; Fornaro, L.; Iachetta, F.; Pozzo, C.; Satolli, M.A.; Spallanzani, A.; Puzzoni, M.; Stragliotto, S.; et al. Results of the observational prospective RealFLOT study. BMC Cancer 2021, 21, 1086. [Google Scholar] [CrossRef] [PubMed]
- Fukagawa, T. Role of staging laparoscopy for Gastric cancer patients. Ann. Gastroenterol. Surg. 2019, 3, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Tourani, S.S.; Cabalag, C.; Link, E.; Chan, S.T.; Duong, C.P. Laparoscopy and peritoneal cytology: Important prognostic tools to guide treatment selection in gastric adenocarcinoma. ANZ J. Surg. 2013, 85, 69–73. [Google Scholar] [CrossRef]
- Gertsen, E.C.; Brenkman, H.J.; van Hillegersberg, R.; van Sandick, J.W.; van Berge Henegouwen, M.I.; Gisbertz, S.S.; Luyer, M.D.; Nieuwenhuijzen, G.A.; Van Lanschot, J.J.; Lagarde, S.M.; et al. 18F-fludeoxyglucose–positron emission tomography/computed tomography and laparoscopy for staging of locally Advanced gastric cancer. JAMA Surg. 2021, 156, e215340. [Google Scholar] [CrossRef]
- Kapiev, A.; Rabin, I.; Lavy, R.; Chikman, B.; Shapira, Z.; Kais, H.; Poluksht, N.; Amsalam, Y.; Halpern, Z.; Markon, I.; et al. The role of diagnostic laparoscopy in the management of patients with gastric cancer. Isr. Med. Assoc. J. 2010, 12, 726–728. [Google Scholar]
- Convie, L.; Thompson, R.J.; Kennedy, R.; Clements, W.D.B.; Carey, P.D.; Kennedy, J.A. The current role of staging laparoscopy in oesophagogastric cancer. Ann. R. Coll. Surg. Engl. 2015, 97, 146–150. [Google Scholar] [CrossRef]
- Muntean, V.; Oniu, T.; Lungoci, C.; Fabian, O.; Munteanu, D.; Molnar, G.; Bintintan, V. Staging Laparoscopy in digestive cancers. J. Gastrointest. Liver Dis. 2009, 18, 461–467. [Google Scholar]
- Jiménez Fonseca, P.; Carmona-Bayonas, A.; Hernández, R.; Custodio, A.; Cano, J.M.; Lacalle, A.; Echavarria, I.; Macias, I.; Mangas, M.; Via, L.; et al. Lauren subtypes of Advanced Gastric Cancer Influence Survival and response to chemotherapy: Real-world data from the Agamenon National Cancer Registry. Br. J. Cancer 2017, 117, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Galletti, G.; Zhang, C.; Gjyrezi, A.; Cleveland, K.; Zhang, J.; Powell, S.; Thakkar, P.V.; Betel, D.; Shah, M.A.; Giannakakou, P. Microtubule engagement with taxane is altered in Taxane-resistant gastric cancer. Clin. Cancer Res. 2020, 26, 3771–3783. [Google Scholar] [CrossRef]
- Li, Y.; Xu, C.; Wang, B.; Xu, F.; Ma, F.; Qu, Y.; Jiang, D.; Li, K.; Feng, J.; Tian, S.; et al. Proteomic characterization of gastric cancer response to chemotherapy and targeted therapy reveals potential therapeutic strategies. Nat. Commun. 2022, 13, 5723. [Google Scholar] [CrossRef] [PubMed]
- Seidlitz, T.; Chen, Y.-T.; Uhlemann, H.; Schölch, S.; Kochall, S.; Merker, S.R.; Klimova, A.; Hennig, A.; Schweitzer, C.; Pape, K.; et al. Mouse models of human gastric cancer subtypes with stomach-specific CREERT2-mediated pathway alterations. Gastroenterology 2019, 157, 1599–1614. [Google Scholar] [CrossRef] [PubMed]
- Homann, N.; Pauligk, C.; Luley, K.; Werner Kraus, T.; Bruch, H.-P.; Atmaca, A.; Noack, F.; Altmannsberger, H.M.; Jäger, E.; Al-Batran, S.E. Pathological complete remission in patients with oesophagogastric cancer receiving preoperative 5-fluorouracil, Oxaliplatin and Docetaxel. Int. J. Cancer 2011, 130, 1706–1713. [Google Scholar] [CrossRef]
- Schulz, C.; Kullmann, F.; Kunzmann, V.; Fuchs, M.; Geissler, M.; Vehling-Kaiser, U.; Stauder, H.; Wein, A.; Al-Batran, S.E.; Kubin, T.; et al. Neoflot: Multicenter phase II study of perioperative chemotherapy in resectable adenocarcinoma of the gastroesophageal junction or gastric adenocarcinoma-very good response predominantly in patients with intestinal type tumors. Int. J. Cancer 2015, 137, 678–685. [Google Scholar] [CrossRef]
- Sisic, L.; Crnovrsanin, N.; Nienhueser, H.; Jung, J.-O.; Schiefer, S.; Haag, G.M.; Bruckner, T.; Schneider, M.; Müller-Stich, B.P.; Büchler, M.W.; et al. Perioperative chemotherapy with 5-fu, leucovorin, Oxaliplatin, and Docetaxel (FLOT) for esophagogastric adenocarcinoma: Ten years real-life experience from a surgical perspective. Langenbeck’s Arch. Surg. 2023, 408, 81. [Google Scholar] [CrossRef]
- Glatz, T.; Verst, R.; Kuvendjiska, J.; Bronsert, P.; Becker, H.; Hoeppner, J.; Kulemann, B. Pattern of recurrence and patient survival after perioperative chemotherapy with 5-fu, leucovorin, Oxaliplatin and Docetaxel (FLOT) for locally advanced esophagogastric adenocarcinoma in patients treated outside clinical trials. J. Clin. Med. 2020, 9, 2654. [Google Scholar] [CrossRef]
- Yildiz, F.; Eraslan, E.; Ilhan, A.; Demir, H.; Demir, N.; Erdur, E.; Yildirim, O.A.; Kanmaz, H.; Aslan, F.; Tufan, G.; et al. Perioperative docetaxel, oxaliplatin, fluorouracil, and leucovorin (FLOT) in patients with gastric or esophagogastric junction adenocarcinoma: Real-life experience. Int. J. Hematol. Oncol. 2020, 30, 1–7. [Google Scholar] [CrossRef]
- Moore, J.L.; Kumar, S.; Santaolalla, A.; Patel, P.H.; Kapiris, M.; Van Hemelrijck, M.; Maisey, N.; Hill, M.; Lagergren, J.; Gossage, J.A.; et al. Effect of peri-operative chemotherapy regimen on survival in the treatment of locally advanced oesophago-gastric adenocarcinoma—A comparison of the FLOT and ‘magic’ regimens. Eur. J. Cancer 2022, 163, 180–188. [Google Scholar] [CrossRef]
- Busweiler, L.A.; Wijnhoven, B.P.; van Berge Henegouwen, M.I.; Henneman, D.; van Grieken, N.C.; Wouters, M.W.; van Hillegersberg, R.; van Sandick, J.W.; Bosscha, K.; Cats, A.; et al. Early outcomes from the Dutch upper gastrointestinal cancer audit. Br. J. Surg. 2016, 103, 1855–1863. [Google Scholar] [CrossRef]
- Marano, L.; Verre, L.; Carbone, L.; Poto, G.E.; Fusario, D.; Venezia, D.F.; Calomino, N.; Kaźmierczak-Siedlecka, K.; Polom, K.; Marrelli, D.; et al. Current trends in volume and surgical outcomes in Gastric Cancer. J. Clin. Med. 2023, 12, 2708. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | All Patients (n = 1982, %) | Anthracyclin Triplets (n= 913, %) | FLOT | p-Value |
|---|---|---|---|---|
| (n = 1069, %) | ||||
| Sex | ||||
| Male | 1330 (67.1) | 597 (65.4) | 733 (68.6) | 0.13 a |
| Age (median [IQR]) | 67 (59–73) | 66 (59–72) | 67 (59–73) | 0.02 b |
| Tumor type | ||||
| Adenocarcinoma | 1665 (84.0) | 753 (82.5) | 912 (85.3) | |
| Signet ring cells | 296 (14.9) | 151 (16.5) | 145 (13.6) | |
| Other | 21 (1.1) | 9 (1.0) | 12 (1.1) | 0.18 a |
| Tumor location | ||||
| Gastric cancer (non-cardia) | 1365 (68.9) | 677 (74.2) | 688 (64.4) | |
| GEJ/cardia | 558 (28.2) | 219 (24.0) | 339 (31.7) | |
| Distal esophagus | 59 (3.0) | 17 (1.9) | 42 (3.9) | <0.001 a |
| Differentiation grade | ||||
| Well differentiated (G1) | 35 (1.8) | 18 (2.0) | 17 (1.6) | |
| Moderately differentiated (G2) | 544 (27.4) | 228 (25.0) | 316 (29.6) | |
| Poorly differentiated (G3) | 1029 (51.9) | 476 (52.1) | 553 (51.7) | |
| Undifferentiated (G4) | 13 (0.7) | 8 (0.9) | 5 (0.5) | |
| Grade cannot be assessed (Gx) | 361 (18.2) | 183 (20.0) | 178 (16.7) | 0.07 a |
| Lauren classification | ||||
| Intestinal | 889 (44.9) | 360 (39.4) | 529 (49.5) | |
| Diffuse | 744 (37.5) | 363 (39.8) | 381 (35.6) | |
| Mixed | 85 (4.3) | 35 (3.8) | 50 (4.7) | |
| Unknown | 264 (13.3) | 155 (17.0) | 109 (10.2) | <0.001 a |
| Clinical T-stage | ||||
| cT2 | 573 (28.9) | 330 (36.1) | 243 (22.7) | |
| cT3 | 1052 (53.1) | 390 (42.7) | 662 (61.9) | |
| cT4a | 131 (6.6) | 46 (5.0) | 85 (8.0) | |
| cTx | 226 (11.4) | 147 (16.1) | 79 (7.4) | <0.001 a |
| Clinical N-stage | ||||
| cN0 | 1009 (50.9) | 480 (52.6) | 529 (49.5) | |
| cN1 | 575 (29) | 249 (27.3) | 326 (30.5) | |
| cN2 | 308 (15.5) | 146 (16.0) | 162 (15.2) | |
| cN3 | 28 (1.4) | 9 (1.0) | 19 (1.8) | |
| cNx | 62 (3.1) | 29 (3.2) | 33 (3.1) | 0.17 a |
| WHO performance status | ||||
| 0 | 940 (47.4) | 403 (44.1) | 537 (50.2) | |
| 1 | 667 (33.7) | 293 (32.1) | 374 (35.0) | |
| 2–4 | 67 (3.4) | 28 (3.1) | 39 (3.6) | |
| Unknown | 308 (15.5) | 189 (20.7) | 119 (11.1) | <0.001 a |
| Number of comorbidities | ||||
| 0 | 1032 (52.1) | 477 (52.2) | 555 (51.9) | |
| 1–2 | 784 (39.6) | 347 (38.0) | 437 (40.9) | |
| >2 | 80 (4.0) | 33 (3.6) | 47 (4.4) | |
| Unknown | 86 (4.3) | 56 (6.1) | 30 (2.8) | 0.002 a |
| Diagnostic staging laparoscopy | 1196 (60.3) | 403 (44.1) | 793 (74.2) | <0.001 a |
| Univariate Analysis HR (95% CI) | p-Value | Multivariate Analysis HR (95% CI) | p-Value | |
|---|---|---|---|---|
| Sex | ||||
| Male | 1 [reference] | |||
| Female | 0.97 (0.85–1.11) | 0.64 | ||
| Age | 1.01 (1.01–1.02) | <0.0001 | 1.02 (1.01–1.03) | <0.0001 |
| Tumor type | ||||
| Adenocarcinoma | 1 [reference] | |||
| Signet ring cells | 1.08 (0.91–1.29) | 0.36 | ||
| Other/unknown | 1.73 (0.99–2.98) | 0.05 | ||
| Tumor location | ||||
| Gastric cancer (non-cardia) | 1 [reference] | |||
| GEJ/cardia | 1.01 (0.88–1.16) | 0.93 | ||
| Distal esophagus | 1.31 (0.92–1.87) | 0.13 | ||
| Differentiation grade | ||||
| G1–G2 | 1 [reference] | |||
| G3–G4 | 1.61 (1.38–1.88) | <0.0001 | 1.31 (1.09–1.56) | 0.004 |
| Unknown/missing | 1.79 (1.48–2.17) | <0.0001 | 1.48 (1.20–1.83) | 0.0002 |
| Lauren classification | ||||
| Intestinal | 1 [reference] | |||
| Diffuse | 1.72 (1.50–1.98) | <0.0001 | 1.73 (1.47–2.05) | <0.0001 |
| Mixed | 1.35 (0.99–1.85) | 0.06 | 1.34 (0.97–1.84) | 0.08 |
| Unknown | 1.35 (1.11–1.64) | 0.003 | 1.19 (0.97–1.46) | 0.09 |
| cT-category | ||||
| cT2 | 1 [reference] | |||
| cT3 | 1.23 (1.07–1.43) | 0.005 | 1.27 (1.09–1.49) | 0.002 |
| cT4a | 1.44 (1.11–1.87) | 0.006 | 1.38 (1.06–1.80) | 0.02 |
| cTx | 0.88 (0.70–1.10) | 0.25 | 0.89 (0.71–1.11) | 0.29 |
| cN-category | ||||
| cN0 | 1 [reference] | |||
| cN+ | 1.36 (1.19–1.54) | <0.0001 | 1.39 (1.22–1.59) | <0.0001 |
| cNx | 1.51 (1.08–2.09) | 0.02 | 1.57 (1.12–2.19) | 0.009 |
| WHO performance status | ||||
| 0–1 | 1 [reference] | |||
| 2–4 | 1.71 (1.27–2.30) | 0.0004 | 1.70 (1.26–2.30) | 0.0005 |
| Unknown | 1.12 (0.95–1.33) | 0.16 | 1.12 (0.94–1.32) | 0.2 |
| Number of comorbidities | ||||
| 0 | 1 [reference] | |||
| 1–2 | 0.94 (0.82–1.07) | 0.36 | ||
| >2 | 1.22 (0.90–1.65) | 0.21 | ||
| Unknown | 1.12 (0.84–1.49) | 0.45 | ||
| Diagnostic laparoscopy | ||||
| No | 1 [reference] | |||
| Yes | 1.14 (1.00–1.30) | 0.04 | 1.03 (0.90–1.19) | 0.65 |
| Anthracyclin Triplets (n = 797, %) | FLOT (n = 951, %) | Adjusted or FLOT (95% CI) | Multivariable Adjusted p-Value | |
|---|---|---|---|---|
| Completed neoadjuvant chemotherapy | 667 (73.1) | 829 (77.6) | 1.32 (1.05–1.66) | 0.02 |
| Resection after neoadjuvant treatment | 797 (87.3) | 951 (89.0) | 1.34 (0.98–1.82) | 0.07 |
| Radical resection (R0) | 698 (87.6) | 832 (87.5) | 1.24 (0.88–1.73) | 0.22 |
| Pathological complete response | 62 (7.8) | 93 (9.8) | 1.58 (1.08–2.32) | 0.02 |
| ypT0-1 | 156 (19.6) | 227 (23.9) | 1.86 (1.43–2.42) | <0.0001 |
| ypN0 | 344 (43.2) | 448 (47.1) | 1.50 (1.20–1.88) | 0.0003 |
| 30-day mortality 90-day mortality | 20 (2.5) 32 (4.0) | 8 (0.8) 23 (2.4) | 0.32 (0.12–0.81) 0.56 (0.30–1.04) | 0.02 0.07 |
| Adjuvant therapy | 468 (58.9) | 611 (64.3) | 1.37 (1.10–1.71) | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geerts, J.F.M.; van der Zijden, C.J.; van der Sluis, P.C.; Spaander, M.C.W.; Nieuwenhuijzen, G.A.P.; Rosman, C.; van Laarhoven, H.W.M.; Verhoeven, R.H.A.; Wijnhoven, B.P.L.; Lagarde, S.M.; et al. Perioperative Chemotherapy for Gastro-Esophageal or Gastric Cancer: Anthracyclin Triplets versus FLOT. Cancers 2024, 16, 1291. https://doi.org/10.3390/cancers16071291
Geerts JFM, van der Zijden CJ, van der Sluis PC, Spaander MCW, Nieuwenhuijzen GAP, Rosman C, van Laarhoven HWM, Verhoeven RHA, Wijnhoven BPL, Lagarde SM, et al. Perioperative Chemotherapy for Gastro-Esophageal or Gastric Cancer: Anthracyclin Triplets versus FLOT. Cancers. 2024; 16(7):1291. https://doi.org/10.3390/cancers16071291
Chicago/Turabian StyleGeerts, Julie F. M., Charlène J. van der Zijden, Pieter C. van der Sluis, Manon C. W. Spaander, Grard A. P. Nieuwenhuijzen, Camiel Rosman, Hanneke W. M. van Laarhoven, Rob H. A. Verhoeven, Bas P. L. Wijnhoven, Sjoerd M. Lagarde, and et al. 2024. "Perioperative Chemotherapy for Gastro-Esophageal or Gastric Cancer: Anthracyclin Triplets versus FLOT" Cancers 16, no. 7: 1291. https://doi.org/10.3390/cancers16071291
APA StyleGeerts, J. F. M., van der Zijden, C. J., van der Sluis, P. C., Spaander, M. C. W., Nieuwenhuijzen, G. A. P., Rosman, C., van Laarhoven, H. W. M., Verhoeven, R. H. A., Wijnhoven, B. P. L., Lagarde, S. M., & Mostert, B. (2024). Perioperative Chemotherapy for Gastro-Esophageal or Gastric Cancer: Anthracyclin Triplets versus FLOT. Cancers, 16(7), 1291. https://doi.org/10.3390/cancers16071291