
Temporal Trends in Treatment and Outcomes of Endometrial Carcinoma in the United States, 2005–2020

 ,
,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Description of the Entire Cohort
3.2. Patient and Tumor Characteristics across Periods Studied
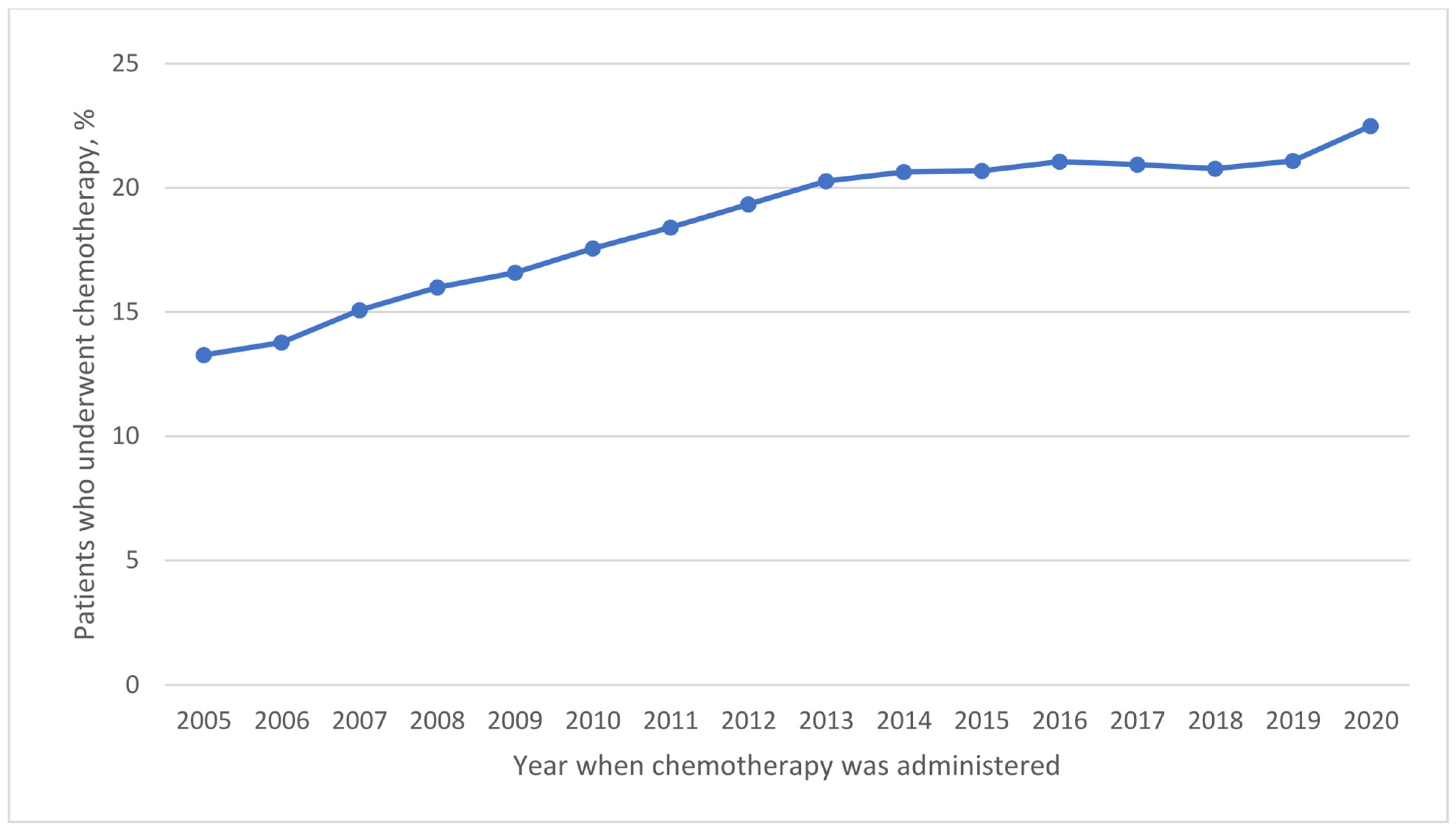
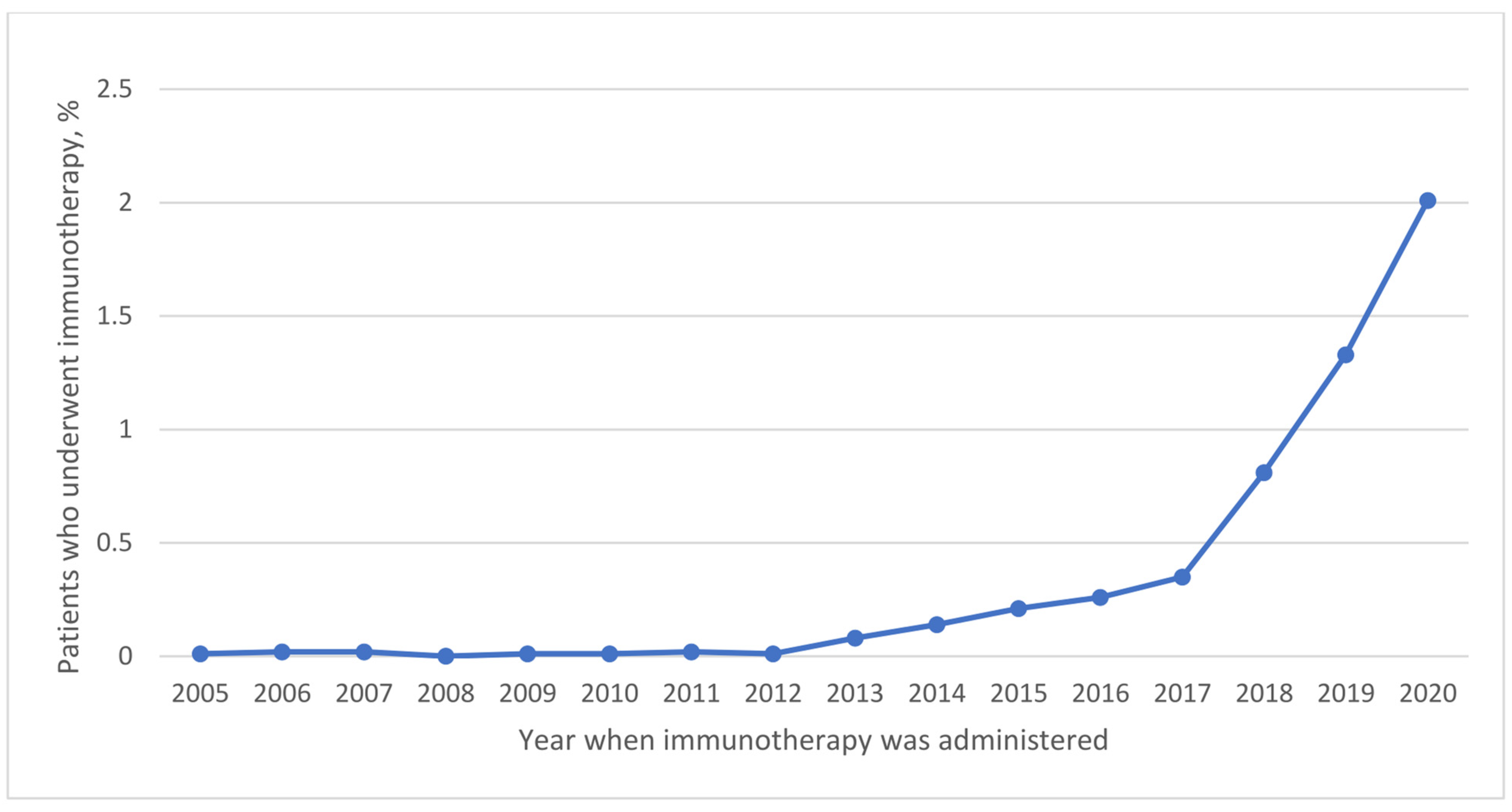
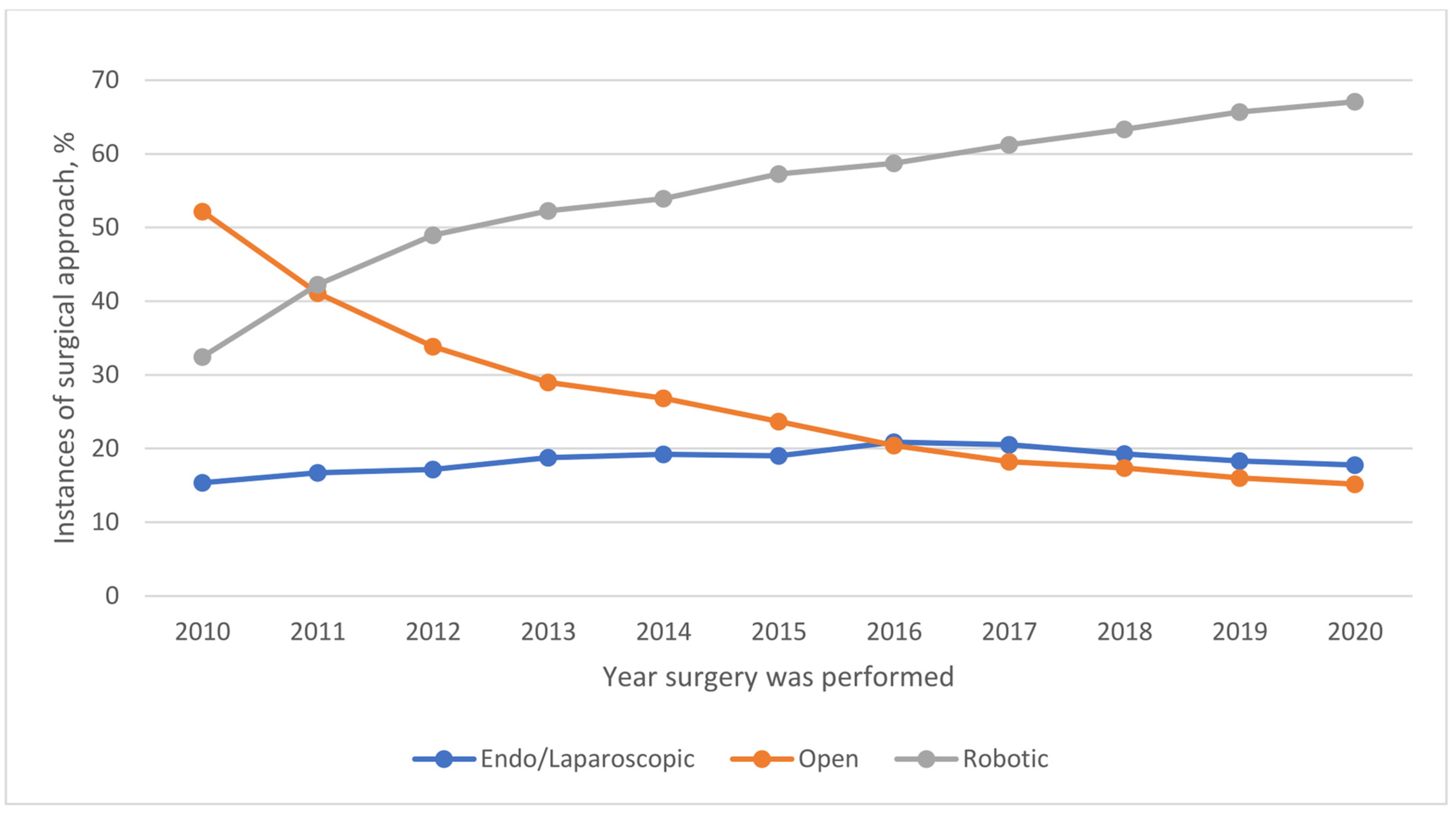
3.3. Temporal Trends in Treatment Approaches
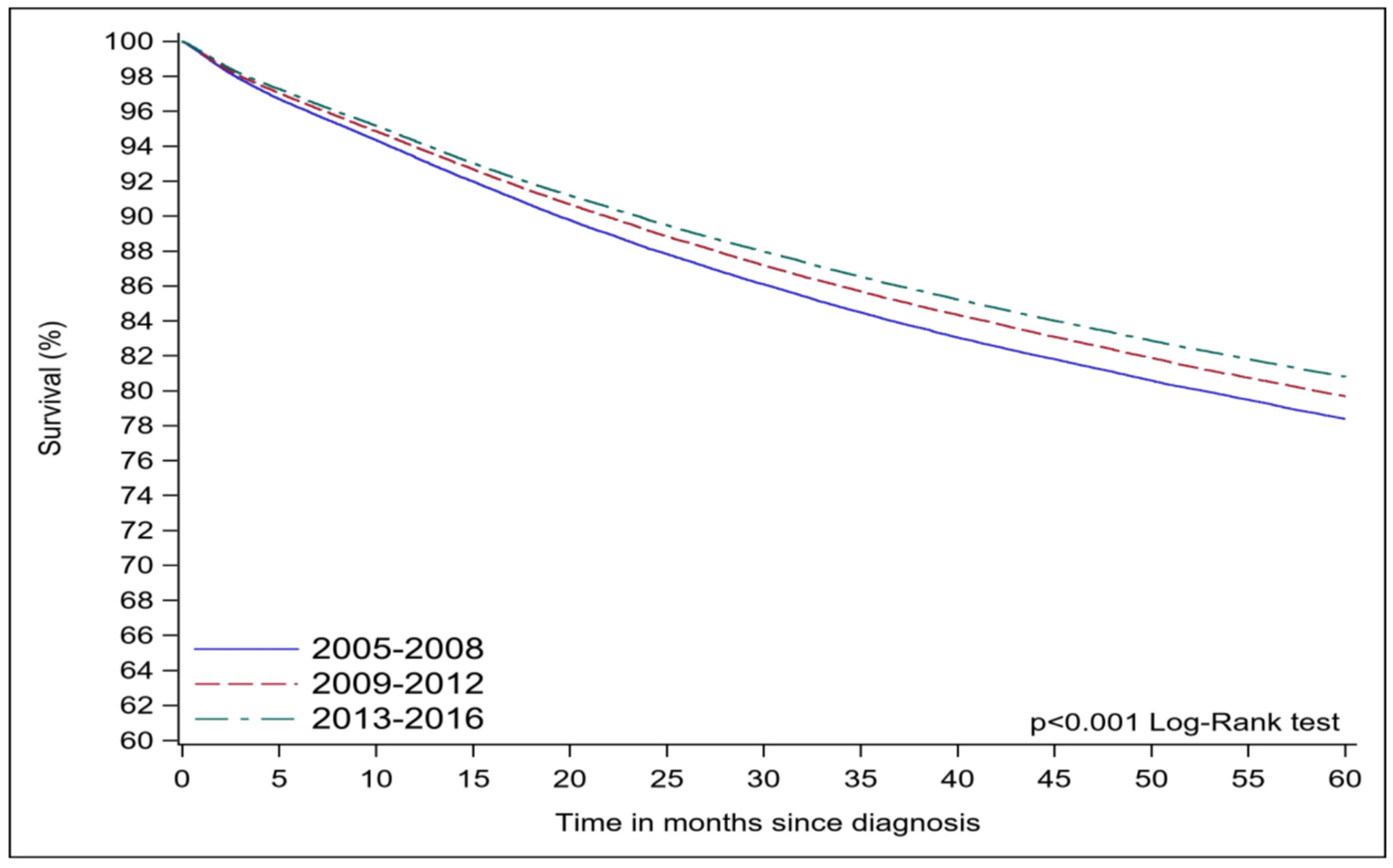
3.4. Temporal Trends in Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020, GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Beavis, A.L.; Cheema, S.; Holschneider, C.H.; Duffy, E.L.; Amneus, M.W. Almost half of women with endometrial cancer or hyperplasia do not know that obesity affects their cancer risk. Gynecol. Oncol. Rep. 2015, 13, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.T. Reproductive factors and the risk of endometrial cancer. Int. J. Gynecol. Cancer. 2014, 24, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, E.M.; Weinstein, L.C.; Hillson, C. Endometrial cancer. Am. Fam. Physician. 2009, 80, 1075–1080. [Google Scholar] [PubMed]
- Uharcek, P.; Mlyncek, M.; Ravinger, J.; Matejka, M. Prognostic factors in women 45 years of age or younger with endometrial cancer. Int. J. Gynecol. Cancer 2008, 18, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Pellerin, G.P.; Finan, M.A. Endometrial cancer in women 45 years of age or younger: A clinicopathological analysis. Am. J. Obstet. Gynecol. 2005, 193, 1640–1644. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.L.; Garside, J.; Hurteau, J.; Nguyen, J.; Kobayashi, M. Treatment Patterns and Outcomes Among Patients With Advanced or Recurrent Endometrial Cancer Initiating First-Line Therapy in the United States. J. Health Econ. Outcomes Res. 2023, 10, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Martins, D.; O’Sullivan, D.E.; Boyne, D.J.; Cheung, W.Y.; Allonby, O.; Habash, M.; Brenner, D.R.; Riemer, J.; McGee, J. Understanding Characteristics, Treatment Patterns, and Clinical Outcomes for Individuals with Advanced or Recurrent Endometrial Cancer in Alberta, Canada: A Retrospective, Population-Based Cohort Study. Curr. Oncol. 2023, 30, 2277–2289. [Google Scholar] [CrossRef]
- Liu, J.; Emond, B.; Maiese, E.M.; Lafeuille, M.H.; Lefebvre, P.; Ghelerter, I.; Wu, C.; Hurteau, J.A.; Thaker, P.H. Real-world utilization and outcomes of systemic therapy among patients with advanced or recurrent endometrial cancer in the United States. Curr. Med. Res. Opin. 2022, 38, 1935–1945. [Google Scholar] [CrossRef]
- Tung, H.-J.; Huang, H.-J.; Lai, C.-H. Adjuvant and post-surgical treatment in endometrial cancer. Best. Pract. Res. Clin. Obstet. Gynaecol. 2022, 78, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial cancer. Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef]
- Crosbie, E.J.; Kitson, S.J.; McAlpine, J.N.; Mukhopadhyay, A.; Powell, M.E.; Singh, N. Endometrial cancer. Lancet 2022, 399, 1412–1428. [Google Scholar] [CrossRef] [PubMed]
- Arciuolo, D.; Travaglino, A.; Raffone, A.; Raimondo, D.; Santoro, A.; Russo, D.; Varricchio, S.; Casadio, P.; Inzani, F.; Seracchioli, R.; et al. TCGA Molecular Prognostic Groups of Endometrial Carcinoma: Current Knowledge and Future Perspectives. Int. J. Mol. Sci. 2022, 23, 11684. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Piedmonte, M.R.; Spirtos, N.M.; Eisenkop, S.M.; Schlaerth, J.B.; Mannel, R.S.; Barakat, R.; Pearl, M.L.; Sharma, S.K. Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study. J. Clin. Oncol. 2012, 30, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, S.L.; Mogensen, O.; Wu, C.; Lund, K.; Iachina, M.; Korsholm, M.; Jensen, P.T. Nationwide Introduction of Minimally Invasive Robotic Surgery for Early-Stage Endometrial Cancer and Its Association with Severe Complications. JAMA Surg. 2019, 154, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Tobias, C.J.; Chen, L.; Melamed, A.; St Clair, C.; Khoury-Collado, F.; Tergas, A.I.; Hou, J.Y.; Hur, C.; Ananth, C.V.; Neugut, A.I.; et al. Association of Neoadjuvant Chemotherapy with Overall Survival in Women with Metastatic Endometrial Cancer. JAMA Network Open. 2020, 3, e2028612. [Google Scholar] [CrossRef] [PubMed]
- Vargo, J.A.; Boisen, M.M.; Comerci, J.T.; Kim, H.; Houser, C.J.; Sukumvanich, P.; Olawaiye, A.B.; Kelley, J.L.; Edwards, R.P.; Huang, M.; et al. Neoadjuvant radiotherapy with or without chemotherapy followed by extrafascial hysterectomy for locally advanced endometrial cancer clinically extending to the cervix or parametria. Gynecol. Oncol. 2014, 135, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.B.; Wu, J.; Chen, L.; Albright, B.B.; Previs, R.A.; Moss, H.A.; Davidson, B.A.; Havrilesky, L.J.; Melamed, A.; Wright, J.D. Neoadjuvant chemotherapy for advanced stage endometrial cancer: A systematic review. Gynecol. Oncol. Rep. 2021, 38, 100887. [Google Scholar] [CrossRef] [PubMed]
- Boisen, M.M.; Vargo, J.A.; Beriwal, S.; Sukumvanich, P.; Olawaiye, A.B.; Kelley, J.L.; Edwards, R.P.; Huang, M.; Courtney-Brooks, M.; Comerci, J.T. Surgical Outcomes of Patients Undergoing Extrafascial Hysterectomy After Neoadjuvant Radiotherapy With or Without Chemotherapy for Locally Advanced Endometrial Cancer Clinically Extending to the Cervix or Parametria. Int. J. Gynecol. Cancer. 2017, 27, 1149–1154. [Google Scholar] [CrossRef]
- Aravantinou-Fatorou, A.; Andrikopoulou, A.; Liontos, M.; Fiste, O.; Georgakopoulou, V.E.; Dimopoulos, M.A.; Gavriatopoulou, M.; Zagouri, F. Pembrolizumab in endometrial cancer: Where we stand now. Oncol. Lett. 2021, 22, 821. [Google Scholar] [CrossRef] [PubMed]
- Hopewood, P. Using the NCDB to explore trends in cancer. Bull. Am. Coll. Surg. 2017, 102, 78–80. [Google Scholar]
- Raval, M.V.; Bilimoria, K.Y.; Stewart, A.K.; Bentrem, D.J.; Ko, C.Y. Using the NCDB for cancer care improvement: An introduction to available quality assessment tools. J. Surg. Oncol. 2009, 99, 488–490. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Fritz, A.P.C.; Jack, A.; Shanmugaratnam, K.; Sobin, L.; Parkin, D.M.; Whelan, S. (Eds.) International Classification of Diseases for Oncology (ICD-O), 3rd ed.; World Health Organization (WHO): Geneva, Switzerland, 2019. Available online: https://www.who.int/publications/i/item/international-classification-of-diseases-for-oncology (accessed on 19 August 2023).
- Emile, S.H.; Horesh, N.; Freund, M.R.; Garoufalia, Z.; Gefen, R.; Silva-Alvarenga, E.; Maron, D.J.; DaSilva, G.; Wexner, S.D. Trends in the Characteristics, Treatment, and Outcomes of Rectal Adenocarcinoma in the US from 2004 to 2019, A National Cancer Database Analysis. JAMA Oncol. 2023, 9, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Gaber, C.; Meza, R.; Ruterbusch, J.J.; Cote, M.L. Endometrial Cancer Trends by Race and Histology in the USA: Projecting the Number of New Cases from 2015 to 2040. J. Racial Ethn. Health Disparities 2017, 4, 895–903. [Google Scholar] [CrossRef]
- American Society of Clinical Oncology. Uterine Cancer: Statistics. 2023. Available online: https://www.cancer.net/cancer-types/uterine-cancer/statistics (accessed on 19 August 2023).
- Lu, K.H.; Broaddus, R.R. Endometrial Cancer. N. Engl. J. Med. 2020, 383, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.L.; Bourn, S.; Skoufalos, A.; Beck, E.H.; Castillo, D.J. An Innovative Approach to Health Care Delivery for Patients with Chronic Conditions. Popul. Health Manag. 2017, 20, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Randall, M.E.; Filiaci, V.L.; Muss, H.; Spirtos, N.M.; Mannel, R.S.; Fowler, J.; Thigpen, J.T.; Benda, J.A. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2006, 24, 36–44. [Google Scholar] [CrossRef]
- OSUCCC Immunotherapy Drug Shows Promise in Advanced Endometrial Cancer. 2023. Available online: https://cancer.osu.edu/news/immunotherapy-drug-shows-promise-in-advanced-endometrial-cancer (accessed on 22 August 2023).
- Hamoud, B.H.; Sima, R.M.; Vacaroiu, I.A.; Georgescu, M.T.; Bobirca, A.; Gaube, A.; Bobirca, F.; Georgescu, D.E. The Evolving Landscape of Immunotherapy in Uterine Cancer: A Comprehensive Review. Life 2023, 13, 1502. [Google Scholar] [CrossRef]
- Eskander, R.N.; Sill, M.W.; Beffa, L.; Moore, R.G.; Hope, J.M.; Musa, F.B.; Mannel, R.; Shahin, M.S.; Cantuaria, G.H.; Girda, E.; et al. Pembrolizumab plus Chemotherapy in Advanced Endometrial Cancer. N. Engl. J. Med. 2023, 388, 2159–2170. [Google Scholar] [CrossRef]
- Mirza, M.R.; Chase, D.M.; Slomovitz, B.M.; dePont Christensen, R.; Novák, Z.; Black, D.; Gilbert, L.; Sharma, S.; Valabrega, G.; Landrum, L.M.; et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N. Engl. J. Med. 2023, 388, 2145–2158. [Google Scholar] [CrossRef]
- Pickett, C.M.; Seeratan, D.D.; Mol, B.W.J.; Nieboer, T.E.; Johnson, N.; Bonestroo, T.; Aarts, J.W. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst. Rev. 2023, 8, Cd003677. [Google Scholar]
- Wang, J.; Li, X.; Wu, H.; Zhang, Y.; Wang, F. A Meta-Analysis of Robotic Surgery in Endometrial Cancer: Comparison with Laparoscopy and Laparotomy. Dis. Markers 2020, 2020, 2503753. [Google Scholar] [CrossRef]
- Pedra Nobre, S.; Mueller, J.J.; Gardner, G.J.; Long Roche, K.; Brown, C.L.; Soslow, R.A.; Alektiar, K.M.; Sonoda, Y.; Broach, V.A.; Jewell, E.L.; et al. Comparison of minimally invasive versus open surgery in the treatment of endometrial carcinosarcoma. Int. J. Gynecol. Cancer. 2020, 30, 1162–1168. [Google Scholar] [CrossRef]
- Ind, T.; Laios, A.; Hacking, M.; Nobbenhuis, M. A comparison of operative outcomes between standard and robotic laparoscopic surgery for endometrial cancer: A systematic review and meta-analysis. Int. J. Med. Robot. 2017, 13, e1851. [Google Scholar] [CrossRef]
- Mäenpää, M.M.; Nieminen, K.; Tomás, E.I.; Laurila, M.; Luukkaala, T.H.; Mäenpää, J.U. Robotic-assisted vs traditional laparoscopic surgery for endometrial cancer: A randomized controlled trial. Am. J. Obstet. Gynecol. 2016, 215, e581–e588. [Google Scholar] [CrossRef]
- O’Malley, D.M.; Smith, B.; Fowler, J.M. The role of robotic surgery in endometrial cancer. J. Surg. Oncol. 2015, 112, 761–768. [Google Scholar] [CrossRef]
- Dolly, D.; Mihai, A.; Rimel, B.J.; Fogg, L.; Rotmensch, J.; Guirguis, A.; Yordan, E.; Dewdney, S. A Delay from Diagnosis to Treatment Is Associated with a Decreased Overall Survival for Patients with Endometrial Cancer. Front. Oncol. 2016, 6, 31. [Google Scholar] [CrossRef]
- Strohl, A.E.; Feinglass, J.M.; Shahabi, S.; Simon, M.A. Surgical wait time: A new health indicator in women with endometrial cancer. Gynecol. Oncol. 2016, 141, 511–515. [Google Scholar] [CrossRef]
- Elit, L.M.; O’Leary, E.M.; Pond, G.R.; Seow, H.Y. Impact of wait times on survival for women with uterine cancer. J. Clin. Oncol. 2014, 32, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Bensenhaver, J.; Winchester, D.P. Surgical leadership and standardization of multidisciplinary breast cancer care: The evolution of the National Accreditation Program for Breast Centers. Surg. Oncol. Clin. N. Am. 2014, 23, 609–616. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (%) | ||||
|---|---|---|---|---|---|
| 2005–2008 (n = 106,955) | 2009–2012 (n = 131,786) | 2013–2016 (n = 158,942) | 2017–2020 (n = 172,134) | p-Value | |
| Age, Mean (SD) | 62.3 (12.2) | 62.4 (11.7) | 62.6 (11.4) | 63.3 (11.4) | <0.001 |
| Age Category | <0.001 | ||||
| <50 | 14,302 (13.4) | 15,782 (12.0) | 17,710 (11.1) | 18,390 (10.7) | |
| ≥50 | 92,653 (86.6) | 116,004 (88.0) | 141,232 (88.9) | 153,744 (89.3) | |
| Race and Ethnicity | <0.001 | ||||
| Hispanic | 5142 (4.8) | 7423 (5.6) | 10,406 (6.6) | 13,108 (7.6) | |
| Non-Hispanic Black | 7836 (7.3) | 11,345 (8.6) | 15,222 (9.6) | 18,398 (10.7) | |
| Non-Hispanic White | 80,178 (75.0) | 101,613 (77.1) | 122,224 (76.9) | 128,043 (74.4) | |
| Other non-Hispanic | 13,799 (13.0) | 11,405 (8.7) | 11,090 (7.0) | 12,585 (7.3) | |
| Charlson Comorbidity Index Score | <0.001 | ||||
| 0 | 80,062 (74.9) | 96,650 (73.3) | 116,458 (73.3) | 125,700 (73.0) | |
| 1 | 21,285 (19.9) | 27,654 (21.0) | 32,128 (20.2) | 30,998 (18.0) | |
| 2 | 4290 (4.0) | 5750 (4.4) | 7287 (4.6) | 8811 (5.1) | |
| 3 | 1318 (1.2) | 1732 (1.3) | 3069 (1.9) | 6625 (3.9) | |
| Residency | <0.001 | ||||
| Metropolitan | 86,502 (80.9) | 107,147 (81.3) | 129,746 (81.6) | 141,874 (82.4) | |
| Rural | 1823 (1.7) | 2193 (1.7) | 2595 (1.6) | 2643 (1.5) | |
| Urban | 14,009 (13.1) | 17,258 (13.1) | 21,207 (13.3) | 22,872 (13.3) | |
| Insurance Status | <0.001 | ||||
| Medicare | 41,625 (38.9) | 51,538 (39.1) | 65,073 (40.9) | 76,950 (44.7) | |
| Medicaid | 4461 (4.2) | 6718 (5.1) | 10,331 (6.5) | 12,394 (7.2) | |
| Other | 2799 (2.6) | 3522 (2.7) | 4013 (2.5) | 3492 (2.0) | |
| Private | 54,589 (51.0) | 64,780 (49.2) | 74,836 (47.1) | 74,892 (43.5) | |
| Uninsured | 3481 (3.3) | 5228 (4.0) | 4689 (3.0) | 4406 (2.6) | |
| Facility Location | <0.001 | ||||
| New England | 7151 (6.9) | 7970 (6.3) | 9909 (6.4) | 10,005 (6.0) | |
| Middle Atlantic | 18,286 (17.7) | 22,767 (17.8) | 26,762 (17.4) | 27,866 (16.8) | |
| South Atlantic | 19,823 (19.2) | 24,954 (19.6) | 29,777 (19.4) | 33,464 (20.1) | |
| East North Central | 20,228 (19.6) | 23,425 (18.4) | 27,037 (17.6) | 28,762 (17.3) | |
| East South Central | 6290 (6.1) | 7684 (6.0) | 9320 (6.1) | 10,029 (6.0) | |
| West North Central | 8869 (8.6) | 11,245 (8.8) | 13,309 (8.7) | 13,598 (8.2) | |
| West South Central | 6841 (6.6) | 9012 (7.1) | 11,762 (7.6) | 13,383 (8.1) | |
| Mountain | 4286 (4.2) | 5398 (4.2) | 6357 (4.1) | 6834 (4.1) | |
| Pacific | 11,613 (11.2) | 15,130 (11.9) | 19,637 (12.8) | 22,349 (13.4) | |
| Facility Type | <0.001 | ||||
| Community Cancer Program | 4766 (4.6) | 4990 (3.9) | 5313 (3.5) | 5807 (3.5) | |
| Comprehensive Community Cancer Program | 37,507 (36.3) | 45,759 (35.9) | 54,589 (35.5) | 59,463 (35.8) | |
| Academic/Research Program | 38,484 (37.2) | 49,240 (38.6) | 61,759 (40.1) | 65,865 (39.6) | |
| Integrated Network Cancer Program | 22,630 (21.9) | 27,596 (21.6) | 32,209 (20.9) | 35,155 (21.1) | |
| TNM stage | <0.001 | ||||
| 0 | 1119 (1.0) | 1190 (0.9) | 1033 (0.6) | 187 (0.1) | |
| 1 | 69,345 (64.8) | 92,059 (69.9) | 110,698 (69.6) | 116,606 (67.7) | |
| 2 | 8025 (7.5) | 6994 (5.3) | 7081 (4.5) | 6857 (4.0) | |
| 3 | 12,471 (11.7) | 14,435 (10.9) | 17,594 (11.1) | 18,935 (11.0) | |
| 4 | 5533 (5.2) | 7099 (5.4) | 9415 (5.9) | 12,178 (7.1) | |
| Unknown | 10,462 (9.8) | 10,009 (7.6) | 13,121 (8.3) | 17,371 (10.1) | |
| Grade | <0.001 | ||||
| Well differentiated | 43,603 (40.8) | 51,106 (38.8) | 56,288 (35.4) | 75,931 (44.1.) | |
| Moderately differentiated | 31,057 (29.0) | 34,175 (25.9) | 32,684 (20.6) | 38,801 (22.5) | |
| Poorly differentiated | 20,215 (18.9) | 23,110 (17.5) | 24,249 (15.3) | 28,882 (16.8) | |
| Undifferentiated | 2375 (2.2) | 3913 (3.0) | 5871 (3.7) | 1944 (1.1) | |
| Unknown | 9705 (9.1) | 19,482 (14.8) | 39,850 (25.1) | 26,576 (15.4) | |
| Lymphovascular Invasion | <0.001 | ||||
| No | NA | 67,069 (50.9) | 107,541 (67.7) | 113,151 (65.7) | |
| Yes | NA | 16,787 (12.8) | 27,509 (17.3) | 32,478 (18.9) | |
| Unknown | NA | 47,930 (36.3) | 23,892 (15.0) | 26,505 (15.4) | |
| Type of Histology | <0.001 | ||||
| Type I | 91,881 (85.9) | 109,614 (83.2) | 129,405 (81.4) | 138,804 (80.6) | |
| Type II | 7937 (7.4) | 10,450 (7.9) | 15,502 (9.8) | 19,883 (11.6) | |
| Others | 7137 (6.7) | 11,722 (8.9) | 14,035 (8.8) | 13,447 (7.8) | |
| No. of Lymph Nodes Examined, Median (IQR) | 6 (0–16) | 6 (0–16) | 4 (0–14) | 3 (0–8) | <0.001 |
| No. of Positive Lymph Nodes, Median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0 (0–1) | <0.001 |
| Factor | 2005–2008 | 2009–2012 | 2013–2016 | 2017–2020 | p-Value |
|---|---|---|---|---|---|
| Chemotherapy | <0.001 | ||||
| No | 88,193 (82.5) | 105,895 (80.4) | 124,495 (78.3) | 134,004 (77.9) | |
| Yes | 15,080 (14.1) | 23,293 (17.7) | 32,449 (20.4) | 36,255 (21.1) | |
| Immunotherapy | <0.001 | ||||
| No | 104,577 (97.8) | 131,003 (99.4) | 158,314 (99.6) | 169,846 (98.7) | |
| Yes | 15 (0.01) | 17 (0.01) | 278 (0.2) | 1901 (1.1) | |
| Sequencing of Systemic Therapy | <0.001 | ||||
| Adjuvant | 10,865 (10.2) | 21,023 (16.0) | 28,243 (17.8) | 30,138 (17.5) | |
| Intraoperative | 5 (0.00) | 26 (0.02) | 27 (0.02) | 49 (0.03) | |
| Neoadjuvant | 518 (0.5) | 966 (0.7) | 1713 (1.1) | 2307 (1.3) | |
| Neoadjuvant and Adjuvant | 156 (0.2) | 457 (0.4) | 1067 (0.7) | 1883 (1.1) | |
| No Treatment | 68,355 (63.9) | 107,182 (81.3) | 126,500 (79.6) | 136,444 (79.3) | |
| Unknown | 27,056 (25.3) | 2132 (1.6) | 1392 (0.9) | 1313 (0.8) | |
| Sequencing of Radiotherapy | <0.001 | ||||
| Adjuvant | 24,605 (23.0) | 28,567 (21.7) | 37,668 (23.7) | 44,548 (25.9) | |
| Intraoperative | 9 (0.01) | 10 (0.01) | 12 (0.01) | 6 (0.0) | |
| Neoadjuvant | 542 (0.5) | 534 (0.4) | 719 (0.5) | 839 (0.5) | |
| Neoadjuvant and Adjuvant | 53 (0.1) | 59 (0.04) | 82 (0.1) | 104 (0.1) | |
| No Treatment | 77,347 (72.3) | 98,349 (74.6) | 116,348 (73.2) | 123,856 (71.9) | |
| Unknown | 4399 (4.1) | 4267 (3.2) | 4113 (2.6) | 2781 (1.6) | |
| Type of Surgery | <0.001 | ||||
| Local tumor destruction/excision | 1078 (1.0) | 1281 (1.0) | 1567 (1.0) | 1574 (0.9) | |
| Total hysterectomy | 1310 (1.2) | 1663 (1.3) | 1680 (1.1) | 1635 (1.0) | |
| Radical hysterectomy | 84,013 (78.6) | 104,289 (79.1) | 127,842 (80.4) | 140,365 (81.5) | |
| Hysterectomy and Pelvic exenteration | 12,602 (11.8) | 14,820 (11.3) | 15,441 (9.7) | 13,460 (7.8) | |
| Total | 106,955 | 131,786 | 158,942 | 172,134 | |
| Approach of Surgery | <0.001 | ||||
| Endo or Laparoscopic | NA | 14,049 (16.4) | 26,004 (19.5) | 26,794 (19.0) | |
| Open | NA | 35,989 (42.1) | 33,079 (24.8) | 23,587 (16.7) | |
| Robotic | NA | 35,437 (41.5) | 74,207 (55.7) | 90,632 (64.3) | |
| Total | NA | 85,475 | 133,290 | 141,013 | |
| Conversion | <0.001 | ||||
| No | NA | 83,002 (63.0) | 129,793 (81.7) | 137,928 (80.1) | |
| Yes | NA | 2473 (1.9) | 3497 (2.2) | 3085 (1.8) | |
| Total | NA | 85,475 | 133,290 | 141,013 | |
| 30 d Mortality | <0.001 | ||||
| No | 97,776 (91.4) | 120,608 (91.5) | 144,893 (91.2) | 118,189 (68.7) | |
| Yes | 657 (0.6) | 683 (0.5) | 583 (0.4) | 373 (0.2) | |
| Total | 98,433 | 121,291 | 145,476 | 118,562 | |
| 90 d Mortality | <0.001 | ||||
| No | 96,710 (90.4) | 119,404 (90.6) | 143,357 (90.2) | 116,361 (67.6) | |
| Yes | 1467 (1.4) | 1555 (1.2) | 1488 (0.9) | 990 (0.6) | |
| Total | 98,177 | 120,959 | 144,845 | 117,351 | |
| 30 d Readmission | <0.001 | ||||
| No readmission | 96,933 (90.6) | 124,553 (94.5) | 152,322 (95.8) | 166,099 (96.5) | |
| Planned readmission | 1693 (1.6) | 1583 (1.2) | 1520 (1.0) | 1235 (0.7) | |
| Unplanned readmission | 3533 (3.3) | 3439 (2.6) | 3354 (2.1) | 2986 (1.7) | |
| Total | 102,159 | 129,575 | 157,196 | 170,320 | |
| Hospital Stay, Median (IQR) | 3 (2–4) | 2 (1–3) | 1 (1–2) | 1 (0–1) | <0.001 |
| Time from Diagnosis to First Surgery, Median (IQR) | 24 (1–40) | 27 (5–42) | 28 (10–44) | 30 (13–47) | <0.001 |
| Time from Diagnosis to Final Surgery, Median (IQR) | 26 (10–41) | 28 (12–43) | 30 (15–46) | 32 (16–48) | <0.001 |
| Time from Diagnosis to First Treatment, Median (IQR) | 24 (3–40) | 27 (6–42) | 28 (10–44) | 29 (13–46) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adekanmbi, V.; Guo, F.; Hsu, C.D.; Gao, D.; Polychronopoulou, E.; Sokale, I.; Kuo, Y.-F.; Berenson, A.B. Temporal Trends in Treatment and Outcomes of Endometrial Carcinoma in the United States, 2005–2020. Cancers 2024, 16, 1282. https://doi.org/10.3390/cancers16071282
Adekanmbi V, Guo F, Hsu CD, Gao D, Polychronopoulou E, Sokale I, Kuo Y-F, Berenson AB. Temporal Trends in Treatment and Outcomes of Endometrial Carcinoma in the United States, 2005–2020. Cancers. 2024; 16(7):1282. https://doi.org/10.3390/cancers16071282
Chicago/Turabian StyleAdekanmbi, Victor, Fangjian Guo, Christine D. Hsu, Daoqi Gao, Efstathia Polychronopoulou, Itunu Sokale, Yong-Fang Kuo, and Abbey B. Berenson. 2024. "Temporal Trends in Treatment and Outcomes of Endometrial Carcinoma in the United States, 2005–2020" Cancers 16, no. 7: 1282. https://doi.org/10.3390/cancers16071282
APA StyleAdekanmbi, V., Guo, F., Hsu, C. D., Gao, D., Polychronopoulou, E., Sokale, I., Kuo, Y.-F., & Berenson, A. B. (2024). Temporal Trends in Treatment and Outcomes of Endometrial Carcinoma in the United States, 2005–2020. Cancers, 16(7), 1282. https://doi.org/10.3390/cancers16071282