
Real-World Outcome of Treatment with Single-Agent Ibrutinib in Italian Patients with Chronic Lymphocytic Leukemia: Final Results of the EVIdeNCE Study

 , , ,
, , ,  , ,
, ,  ,
,  ,
,  , , , , , ,
, , , , , ,  add
Show full author list
add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Determination
2.2. Statistical Analysis
3. Results
3.1. Study Population and Baseline Characteristics
3.2. Ibrutinib Starting Dose and Concomitant Medications
3.3. Retention and Discontinuation Rate
3.4. Clinical Response and Survival Outcomes
3.5. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kipps, T.J.; Stevenson, F.K.; Wu, C.J.; Croce, C.M.; Packham, G.; Wierda, W.G.; O’Brien, S.; Gribben, J.; Rai, K. Chronic lymphocytic leukaemia. Nat. Rev. Dis. Prim. 2017, 3, 16096. [Google Scholar] [CrossRef] [PubMed]
- Rozman, C.; Montserrat, E. Chronic lymphocytic leukemia. N. Engl. J. Med. 1995, 333, 1052–1057. [Google Scholar] [CrossRef]
- Hallek, M.; Shanafelt, T.D.; Eichhorst, B. Chronic lymphocytic leukaemia. Lancet 2018, 391, 1524–1537. [Google Scholar] [CrossRef]
- Eyre, T.A. Richter transformation—Is there light at the end of this tunnel? Hematology 2023, 2023, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Pagel, J.M. Current and future treatment strategies in chronic lymphocytic leukemia. J. Hematol. Oncol. 2021, 14, 69. [Google Scholar] [CrossRef]
- Honigberg, L.A.; Smith, A.M.; Sirisawad, M.; Verner, E.; Loury, D.; Chang, B.; Li, S.; Pan, Z.; Thamm, D.H.; Miller, R.A.; et al. The Bruton tyrosine kinase inhibitor PCI-32765 blocks B-cell activation and is efficacious in models of autoimmune disease and B-cell malignancy. Proc. Natl. Acad. Sci. USA 2010, 107, 13075–13080. [Google Scholar] [CrossRef] [PubMed]
- Burger, J.A.; Tedeschi, A.; Barr, P.M.; Robak, T.; Owen, C.; Ghia, P.; Bairey, O.; Hillmen, P.; Bartlett, N.L.; Li, J.; et al. Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2015, 373, 2425–2437. [Google Scholar] [CrossRef]
- Byrd, J.C.; Brown, J.R.; O’Brien, S.; Barrientos, J.C.; Kay, N.E.; Reddy, N.M.; Coutre, S.; Tam, C.S.; Mulligan, S.P.; Jaeger, U.; et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N. Engl. J. Med. 2014, 371, 213–223. [Google Scholar] [CrossRef]
- Moreno, C.; Greil, R.; Demirkan, F.; Tedeschi, A.; Anz, B.; Larratt, L.; Simkovic, M.; Samoilova, O.; Novak, J.; Ben-Yehuda, D.; et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in first-line treatment of chronic lymphocytic leukaemia (iLLUMINATE): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 43–56. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Wang, X.V.; Kay, N.E.; Hanson, C.A.; O’Brien, S.; Barrientos, J.; Jelinek, D.F.; Braggio, E.; Leis, J.F.; Zhang, C.C.; et al. Ibrutinib-Rituximab or Chemoimmunotherapy for Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2019, 381, 432–443. [Google Scholar] [CrossRef]
- Woyach, J.A.; Ruppert, A.S.; Heerema, N.A.; Zhao, W.; Booth, A.M.; Ding, W.; Bartlett, N.L.; Brander, D.M.; Barr, P.M.; Rogers, K.A.; et al. Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL. N. Engl. J. Med. 2018, 379, 2517–2528. [Google Scholar] [CrossRef] [PubMed]
- Barr, P.M.; Robak, T.; Owen, C.; Tedeschi, A.; Bairey, O.; Bartlett, N.L.; Burger, J.A.; Hillmen, P.; Coutre, S.; Devereux, S.; et al. Sustained efficacy and detailed clinical follow-up of first-line ibrutinib treatment in older patients with chronic lymphocytic leukemia: Extended phase 3 results from RESONATE-2. Haematologica 2018, 103, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Barr, P.M.; Owen, C.; Robak, T.; Tedeschi, A.; Bairey, O.; Burger, J.A.; Hillmen, P.; Coutre, S.E.; Dearden, C.; Grosicki, S.; et al. Up to 8-year follow-up from RESONATE-2: First-line ibrutinib treatment for patients with chronic lymphocytic leukemia. Blood Adv. 2022, 6, 3440–3450. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Wang, X.V.; Hanson, C.A.; Paietta, E.M.; O’Brien, S.; Barrientos, J.; Jelinek, D.F.; Braggio, E.; Leis, J.F.; Zhang, C.C.; et al. Long-term outcomes for ibrutinib-rituximab and chemoimmunotherapy in CLL: Updated results of the E1912 trial. Blood 2022, 140, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Byrd, J.C.; Hillmen, P.; O’Brien, S.; Barrientos, J.C.; Reddy, N.M.; Coutre, S.; Tam, C.S.; Mulligan, S.P.; Jaeger, U.; Barr, P.M.; et al. Long-term follow-up of the RESONATE phase 3 trial of ibrutinib vs ofatumumab. Blood 2019, 133, 2031–2042. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; Allan, J.N.; Siddiqi, T.; Kipps, T.J.; Jacobs, R.; Opat, S.; Barr, P.M.; Tedeschi, A.; Trentin, L.; Bannerji, R.; et al. Fixed-duration ibrutinib plus venetoclax for first-line treatment of CLL: Primary analysis of the CAPTIVATE FD cohort. Blood 2022, 139, 3278–3289. [Google Scholar] [CrossRef] [PubMed]
- Corrigan-Curay, J.; Sacks, L.; Woodcock, J. Real-World Evidence and Real-World Data for Evaluating Drug Safety and Effectiveness. JAMA 2018, 320, 867–868. [Google Scholar] [CrossRef]
- Forum, U.C. Ibrutinib for relapsed/refractory chronic lymphocytic leukemia: A UK and Ireland analysis of outcomes in 315 patients. Haematologica 2016, 101, 1563–1572. [Google Scholar] [CrossRef]
- Akpinar, S.; Dogu, M.H.; Celik, S.; Ekinci, O.; Hindilerden, I.Y.; Dal, M.S.; Davulcu, E.A.; Tekinalp, A.; Hindilerden, F.; Ozcan, B.G.; et al. The Real-World Experience with Single Agent Ibrutinib in Relapsed/Refractory CLL. Clin. Lymphoma Myeloma Leuk. 2022, 22, 169–173. [Google Scholar] [CrossRef]
- Winqvist, M.; Andersson, P.O.; Asklid, A.; Karlsson, K.; Karlsson, C.; Lauri, B.; Lundin, J.; Mattsson, M.; Norin, S.; Sandstedt, A.; et al. Long-term real-world results of ibrutinib therapy in patients with relapsed or refractory chronic lymphocytic leukemia: 30-month follow up of the Swedish compassionate use cohort. Haematologica 2019, 104, e208–e210. [Google Scholar] [CrossRef]
- Dartigeas, C.; Slama, B.; Doyle, M.; Tapprich, C.; Albrecht, C.; Dupuis, S.; Wapenaar, R.; Schmidt-Hieber, C.; Leblond, V. FIRE Study: Real-World Effectiveness and Safety of Ibrutinib in Clinical Practice in Patients with CLL and MCL. Clin. Hematol. Int. 2022, 4, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Ysebaert, L.; Aurran-Schleinitz, T.; Dartigeas, C.; Dilhuydy, M.S.; Feugier, P.; Michallet, A.S.; Tournilhac, O.; Dupuis, J.; Sinet, P.; Albrecht, C.; et al. Real-world results of ibrutinib in relapsed/refractory CLL in France: Early results on a large series of 428 patients. Am. J. Hematol. 2017, 92, E166–E168. [Google Scholar] [CrossRef] [PubMed]
- Abrisqueta, P.; Loscertales, J.; Terol, M.J.; Ramirez Payer, A.; Ortiz, M.; Perez, I.; Cuellar-Garcia, C.; Fernandez de la Mata, M.; Rodriguez, A.; Lario, A.; et al. Real-World Characteristics and Outcome of Patients Treated with Single-Agent Ibrutinib for Chronic Lymphocytic Leukemia in Spain (IBRORS-LLC Study). Clin. Lymphoma Myeloma Leuk. 2021, 21, e985–e999. [Google Scholar] [CrossRef] [PubMed]
- Mato, A.R.; Roeker, L.E.; Allan, J.N.; Pagel, J.M.; Brander, D.M.; Hill, B.T.; Cheson, B.D.; Furman, R.R.; Lamanna, N.; Tam, C.S.; et al. Outcomes of front-line ibrutinib treated CLL patients excluded from landmark clinical trial. Am. J. Hematol. 2018, 93, 1394–1401. [Google Scholar] [CrossRef]
- Dimou, M.; Iliakis, T.; Pardalis, V.; Bitsani, C.; Vassilakopoulos, T.P.; Angelopoulou, M.; Tsaftaridis, P.; Papaioannou, P.; Koudouna, A.; Kalyva, S.; et al. Safety and efficacy analysis of long-term follow up real-world data with ibrutinib monotherapy in 58 patients with CLL treated in a single-center in Greece. Leuk. Lymphoma 2019, 60, 2939–2945. [Google Scholar] [CrossRef]
- Aarup, K.; Rotbain, E.C.; Enggaard, L.; Pedersen, R.S.; Bergmann, O.J.; Thomsen, R.H.; Frederiksen, M.; Frederiksen, H.; Nielsen, T.; Christiansen, I.; et al. Real-world outcomes for 205 patients with chronic lymphocytic leukemia treated with ibrutinib. Eur. J. Haematol. 2020, 105, 646–654. [Google Scholar] [CrossRef]
- Frei, C.R.; Le, H.; McHugh, D.; Ryan, K.; Jones, X.; Galley, S.; Franklin, K.; Baus, C.J.; Tavera, J.; Janania-Martinez, M.; et al. Outcomes in chronic lymphocytic leukemia patients on novel agents in the US Veterans Health Administration System. Leuk. Lymphoma 2021, 62, 1664–1673. [Google Scholar] [CrossRef]
- Khelifi, R.S.; Huang, S.J.; Savage, K.J.; Villa, D.; Scott, D.W.; Ramadan, K.; Connors, J.M.; Sehn, L.H.; Toze, C.L.; Gerrie, A.S. Population-level impact of ibrutinib for chronic lymphocytic leukemia in British Columbia, Canada. Leuk. Lymphoma 2023, 64, 1129–1138. [Google Scholar] [CrossRef]
- Mato, A.R.; Nabhan, C.; Thompson, M.C.; Lamanna, N.; Brander, D.M.; Hill, B.; Howlett, C.; Skarbnik, A.; Cheson, B.D.; Zent, C.; et al. Toxicities and outcomes of 616 ibrutinib-treated patients in the United States: A real-world analysis. Haematologica 2018, 103, 874–879. [Google Scholar] [CrossRef]
- Janssens, A.; Berneman, Z.N.; Offner, F.; Snauwaert, S.; Mineur, P.; Vanstraelen, G.; Meers, S.; Spoormans, I.; Bron, D.; Vande Broek, I.; et al. Effectiveness and Safety of Ibrutinib for Chronic Lymphocytic Leukemia in Routine Clinical Practice: 3-Year Follow-up of the Belgian Ibrutinib Real-World Data (BiRD) Study. Clin. Hematol. Int. 2022, 4, 133–143. [Google Scholar] [CrossRef]
- Narezkina, A.; Akhter, N.; Lu, X.; Emond, B.; Panjabi, S.; Forbes, S.P.; Hilts, A.; Liu, S.; Lafeuille, M.H.; Lefebvre, P.; et al. Real-World Persistence and Time to Next Treatment With Ibrutinib in Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Including Patients at High Risk for Atrial Fibrillation or Stroke. Clin. Lymphoma Myeloma Leuk. 2022, 22, e959–e971. [Google Scholar] [CrossRef]
- Hillmen, P.; Xie, J.; Yong, A.S.M.; Waweru, C.; Sorof, T.A.; Goyal, R.K.; Davis, K.L. Real-world treatment patterns, adverse events and clinical outcomes in patients with chronic lymphocytic leukaemia treated with ibrutinib in the UK. EJHaem 2021, 2, 219–227. [Google Scholar] [CrossRef]
- Maddocks, K.J.; Ruppert, A.S.; Lozanski, G.; Heerema, N.A.; Zhao, W.; Abruzzo, L.; Lozanski, A.; Davis, M.; Gordon, A.; Smith, L.L.; et al. Etiology of Ibrutinib Therapy Discontinuation and Outcomes in Patients with Chronic Lymphocytic Leukemia. JAMA Oncol. 2015, 1, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Gocer, M.; Kurtoglu, E. Safety and efficacy analysis of ibrutinib in 32 patients with CLL and various B-cell lymphomas: Real-world data from a single-center study in Turkey. Blood Res. 2020, 55, 206–212. [Google Scholar] [CrossRef]
- Molica, S.; Scalzulli, P.R.; Scarfo, L.; Guarini, A.; Murru, R.; Sportoletti, P.; Frigeri, F.; Albano, F.; Di Renzo, N.; Sanna, A.; et al. The Use of Ibrutinib in Italian CLL Patients Treated in a Real-World Setting (EVIDENCE): A Preliminary Report. Blood 2021, 138, 4684. [Google Scholar] [CrossRef]
- Hallek, M.; Cheson, B.D.; Catovsky, D.; Caligaris-Cappio, F.; Dighiero, G.; Dohner, H.; Hillmen, P.; Keating, M.; Montserrat, E.; Chiorazzi, N.; et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 2018, 131, 2745–2760. [Google Scholar] [CrossRef] [PubMed]
- Rigolin, G.M.; Olimpieri, P.P.; Summa, V.; Celant, S.; Scarfo, L.; Tognolo, L.; Ballardini, M.P.; Urso, A.; Sessa, M.; Gambara, S.; et al. Outcomes in patients with chronic lymphocytic leukemia and TP53 aberration who received first-line ibrutinib: A nationwide registry study from the Italian Medicines Agency. Blood Cancer J. 2023, 13, 99. [Google Scholar] [CrossRef] [PubMed]
- Munir, T.; Brown, J.R.; O’Brien, S.; Barrientos, J.C.; Barr, P.M.; Reddy, N.M.; Coutre, S.; Tam, C.S.; Mulligan, S.P.; Jaeger, U.; et al. Final analysis from RESONATE: Up to six years of follow-up on ibrutinib in patients with previously treated chronic lymphocytic leukemia or small lymphocytic lymphoma. Am. J. Hematol. 2019, 94, 1353–1363. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, S.P.; Opat, S.; Marlton, P.; Kuss, B.; Gerungan, P.; Puig, A.; McGeachie, M.; Tam, C.S. Ibrutinib use, treatment duration, and concomitant medications in Australian patients with relapsed or refractory chronic lymphocytic leukaemia. Br. J. Haematol. 2022, 198, 790–793. [Google Scholar] [CrossRef]
- Huntington, S.F.; De Nigris, E.; Puckett, J.; Kamal-Bahl, S.; Farooqui, M.Z.H.; Ryland, K.E.; Sarpong, E.; Yang, X.; Doshi, J. Real-World Treatment Patterns and Outcomes after Ibrutinib Discontinuation Among Elderly Medicare Beneficiaries with Chronic Lymphocytic Leukemia: An Observational Study. Blood 2022, 140, 7939–7940. [Google Scholar] [CrossRef]
- Hardy-Abeloos, C.; Pinotti, R.; Gabrilove, J. Ibrutinib dose modifications in the management of CLL. J. Hematol. Oncol. 2020, 13, 66. [Google Scholar] [CrossRef]
- Gerhardt, A.; Dorfel, S.; Schulz, H.; Schlag, R.; Vornholz, L.; Nejad-Asgari, S.; Welslau, M. Outcomes with ibrutinib in patients with chronic lymphocytic leukaemia: Results from the German multicentre REALITY study. Eur. J. Haematol. 2024. [Google Scholar] [CrossRef]
- Roeker, L.E.; DerSarkissian, M.; Ryan, K.; Chen, Y.; Duh, M.S.; Wahlstrom, S.K.; Hakre, S.; Yu, L.; Guo, H.; Mato, A.R. Real-world comparative effectiveness of acalabrutinib and ibrutinib in patients with chronic lymphocytic leukemia. Blood Adv. 2023, 7, 4291–4301. [Google Scholar] [CrossRef]
- Lampson, B.L.; Yu, L.; Glynn, R.J.; Barrientos, J.C.; Jacobsen, E.D.; Banerji, V.; Jones, J.A.; Walewska, R.; Savage, K.J.; Michaud, G.F.; et al. Ventricular arrhythmias and sudden death in patients taking ibrutinib. Blood 2017, 129, 2581–2584. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.A.; Achenbach, S.J.; Call, T.G.; Rabe, K.G.; Ding, W.; Leis, J.F.; Kenderian, S.S.; Chanan-Khan, A.A.; Koehler, A.B.; Schwager, S.M.; et al. The impact of dose modification and temporary interruption of ibrutinib on outcomes of chronic lymphocytic leukemia patients in routine clinical practice. Cancer Med. 2020, 9, 3390–3399. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, O.S.; Attwood, K.; Lund, I.; Hare, R.; Hernandez-Ilizaliturri, F.J.; Torka, P. Dose reductions in ibrutinib therapy are not associated with inferior outcomes in patients with chronic lymphocytic leukemia (CLL). Leuk. Lymphoma 2019, 60, 1650–1655. [Google Scholar] [CrossRef]
- Rogers, K.A.; Lu, X.; Emond, B.; Ding, Z.; Lefebvre, P.; Lafeuille, M.-H.; Mavani, H.; Qureshi, Z.P.; Ghosh, N. Real-world (RW) dosing patterns and outcomes among chronic lymphocytic leukemia (CLL) patients (pts) with or without an ibrutinib (IBR) dose adjustment (DA) in first-line (1L). J. Clin. Oncol. 2023, 41, 7537. [Google Scholar] [CrossRef]
- Shadman, M.; Karve, S.; Patel, S.; Rava, A.; Sun, H.; Howarth, A.; Tomicki, S.; Srivastava, B.P.; Stephens, D.M. Impact of Ibrutinib Dose Reduction on Duration of Therapy in Patients with Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. In Proceedings of the 65th American Society of Hematology (ASH) Annual Meeting and Exposition, San Diego, CA, USA, 9 December 2023. [Google Scholar]
- Ghosh, N.; Wang, R.; Ding, Z.; He, J.; Bokun, A.; Mavani, H.; Qureshi, Z.; Rogers, K.A. Comparative Effectiveness of Ibrutinib Flexible Dosing Treatment Strategies on Time to Next Treatment in a Largely Community-Based Claims Database: A Target Trial Emulation Study. In Proceedings of the 65th American Society of Hematology (ASH) Annual Meeting and Exposition, San Diego, CA, USA, 9 December 2023. [Google Scholar]
- Uminski, K.; Brown, K.; Bucher, O.; Hibbert, I.; Dhaliwal, D.H.; Johnston, J.B.; Geirnaert, M.; Dawe, D.E.; Banerji, V. Descriptive analysis of dosing and outcomes for patients with ibrutinib-treated relapsed or refractory chronic lymphocytic leukemia in a Canadian centre. Curr. Oncol. 2019, 26, e610–e617. [Google Scholar] [CrossRef]
- Tedeschi, A.; Ahn, I.E.; Fraser, G.A.M.; Greil, R.; Munir, T.; Kay, N.E.; Flinn, I.W.; Lee, S.; Saifan, C.; Kearbey, J.; et al. Ibrutinib (Ibr) dose modification for management of early cardiac adverse events in patients with chronic lymphocytic leukemia: Pooled analysis of 7 clinical trials. Hematol. Oncol. 2023, 41, 461–463. [Google Scholar] [CrossRef]
- Ghia, P.; Wierda, W.G.; Barr, P.M.; Kipps, T.J.; Siddiqi, T.; Allan, J.N.; Hunter, Z.; Zhou, C.; Szoke, A.; Dean, J.P.; et al. Relapse after First-Line Fixed Duration Ibrutinib + Venetoclax: High Response Rates to Ibrutinib Retreatment and Absence of BTK Mutations in Patients with Chronic Lymphocytic Leukemia (CLL)/Small Lymphocytic Lymphoma (SLL) with up to 5 Years of Follow-up in the Phase 2 Captivate Study. Blood 2023, 142, 633. [Google Scholar] [CrossRef]
- Moreno, C.; Solman, I.G.; Tam, C.S.; Grigg, A.; Scarfò, L.; Kipps, T.J.; Srinivasan, S.; Mali, R.S.; Zhou, C.; Dean, J.P.; et al. Immune restoration with ibrutinib plus venetoclax in first-line chronic lymphocytic leukemia: The phase 2 CAPTIVATE study. Blood Adv. 2023, 7, 5294–5303. [Google Scholar] [CrossRef] [PubMed]
- Niemann, C.U.; Munir, T.; Moreno, C.; Owen, C.; Follows, G.A.; Benjamini, O.; Janssens, A.; Levin, M.D.; Robak, T.; Simkovic, M.; et al. Fixed-duration ibrutinib-venetoclax versus chlorambucil-obinutuzumab in previously untreated chronic lymphocytic leukaemia (GLOW): 4-year follow-up from a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2023, 24, 1423–1433. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Baseline Characteristics | Overall (n = 309) n (%) | 1L (n = 118) n ^ (%) | 2L (n = 127) n ^ (%) | ≥3L (n = 64) n ^ (%) | p-Value ¶ |
|---|---|---|---|---|---|
| Age at ibrutinib initiation | |||||
| <65 | 71 (23.0) | 18 (15.3) | 38 (29.9) | 15 (23.4) | 0.088 |
| 65–69 | 52 (16.8) | 24 (20.3) | 17 (13.4) | 11 (17.2) | |
| ≥70 | 186 (60.2) | 76 (64.4) | 72 (56.7) | 38 (59.4) | |
| Median (IQR) | 71 (65–77) | 72 (67–77) | 71 (63–74) | 71 (65–78) | |
| Male sex | 195 (63.1) | 74 (62.7) | 78 (61.4) | 43 (67.2) | 0.733 |
| ECOG-PS | |||||
| 0–1 | 238 (90.2) | 82 (89.1) | 109 (92.4) | 47 (87.0) | 0.508 |
| ≥2 | 26 (9.8) | 10 (10.9) | 9 (7.6) | 7 (13.0) | |
| Unknown | 45 | 26 | 9 | 10 | |
| CIRS score | |||||
| <6 | 174 (71.9) | 62 (66.7) | 76 (77.6) | 36 (70.6) | 0.240 |
| ≥6 | 68 (28.1) | 31 (33.3) | 22 (22.4) | 15 (29.4) | |
| Unknown | 67 | 25 | 29 | 13 | |
| History of significant CVD * | 103 (33.3) | 45 (38.1) | 37 (29.1) | 21 (32.8) | 0.326 |
| Rai Staging System at ibrutinib initiation | |||||
| Stage 0 | 12 (4.1) | 3 (2.7) | 6 (4.9) | 3 (5.3) | 0.464 |
| Stage I-II | 128 (43.8) | 55 (49.1) | 53 (43.1) | 20 (35.1) | |
| Stage III-IV | 152 (52.0) | 54 (48.2) | 64 (52.0) | 34 (59.6) | |
| Unknown | 17 | 6 | 4 | 7 | |
| Mutational status ¥ | |||||
| Unmutated IGHV | 94/135 (69.6) | 38/56 (67.9) | 39/58 (67.2) | 17/21 (81.0) | 0.469 |
| TP53 mutation | 52/164 (31.7) | 25/68 (36.8) | 15/65 (23.1) | 12/31 (38.7) | 0.154 |
| Any cytogenetic alterations | 181/266 (68.0) | 67/102 (65.7) | 77/113 (68.1) | 37/51 (72.5) | 0.692 |
| Del11q | 47/266 (17.7) | 12/102 (11.8) | 25/113 (22.1) | 10/51 (19.6) | 0.128 |
| Del17p | 56/266 (21.1) | 28/102 (27.5) | 19/113 (16.8) | 9/51 (17.6) | 0.129 |
| Del17p or TP53 mutation | 69/138 (50.0) | 32/60 (53.3) | 23/55 (41.8) | 14/23 (60.9) | 0.243 |
| Event Type Description | 1L (n = 118) n (%) | 2L (n = 127) n (%) | ≥3L (n = 64) n (%) | Overall (n = 309) |
|---|---|---|---|---|
| At least one temporary treatment interruption * | 47 (39.8) | 41 (32.3) | 19 (29.7) | 107 (34.6) |
| Treatment permanent discontinuation ^ | 29 (24.6) | 38 (29.9) | 25 (39.1) | 92 (29.8) |
| Reason for discontinuation ¶ | ||||
| AEs | 15 (12.7) | 15 (11.8) | 14 (21.9) | 44 (14.2) |
| Death | 5 (4.2) | 7 (5.5) | 6 (9.4) | 18 (5.8) |
| Disease progression | 3 (2.5) | 9 (7.1) | 3 (4.7) | 15 (4.9) |
| Second malignancy | 1 (0.8) | 5 (3.9) | 2 (3.1) | 8 (2.6) |
| Clinician’s choice | 5 (4.2) | 6 (4.7) | 0 (0.0) | 11 (3.6) |
| Other reason(s) | 2 (1.7) | 4 (3.1) | 1 (1.6) | 7 (2.3) |
| Time (months) to ibrutinib treatment discontinuation ˜, median (IQR) | 5.7 (3.6–11.7) | 11.3 (5.1–16.7) | 7.2 (4.3–14.1) | 6.9 (4.3–15.2) |
| Patients with subsequent CLL therapy | 11 (9.3) | 11 (8.7) | 7 (10.9) | 29 (9.4) |
| Efficacy Outcomes | 1L (n = 118) n (%) | 2L (n = 127) n (%) | ≥3L (n = 64) n (%) | Overall (n = 309) |
|---|---|---|---|---|
| Best response | ||||
| ORR ^ | 84 (80.8) | 79 (75.2) | 39 (68.4) | 202 (75.9) |
| CR * | 29 (27.8) | 17 (16.2) | 3 (5.3) | 49 (18.4) |
| PR | 53 (51.0) | 56 (53.3) | 29 (50.9) | 138 (51.9) |
| PR-L | 2 (1.9) | 6 (5.7) | 7 (12.3) | 15 (5.6) |
| SD | 17 (16.3) | 19 (18.1) | 17 (29.8) | 53 (19.9) |
| DP | 3 (2.9) | 7 (6.7) | 1 (1.8) | 11 (4.1) |
| Unknown | 14 | 22 | 7 | 43 |
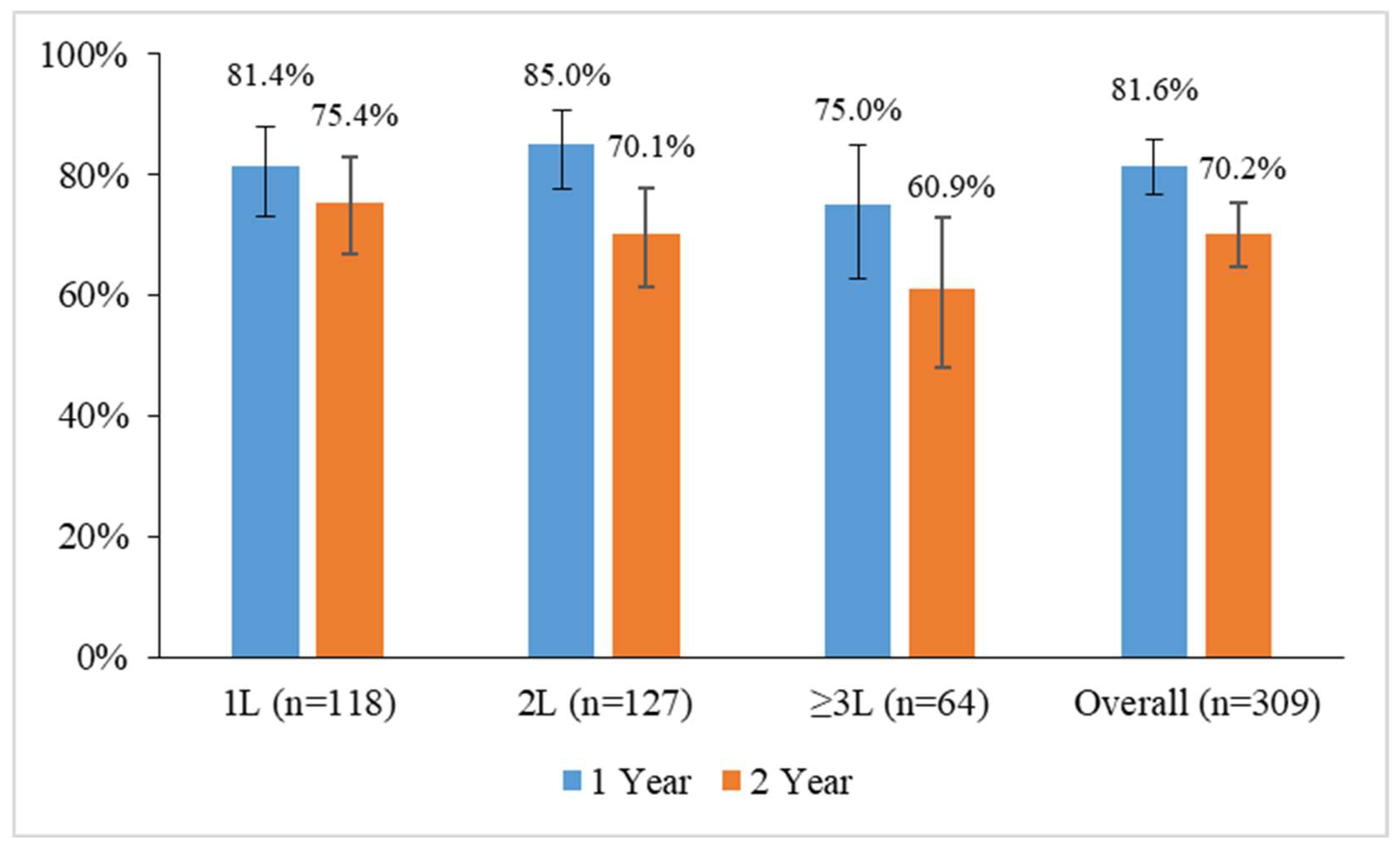
| 2-year PFS, % | 85.4 | 80.0 | 70.1 | 79.3 |
| 2-year OS, % | 91.7 | 86.2 | 80.8 | 85.6 |
| 1L (n = 118) n (%) | 2L (n = 127) n (%) | ≥3L (n = 64) n (%) | Overall (n = 309) | |
|---|---|---|---|---|
| Any grade ^ | ||||
| Any AE | 88 (74.6) | 93 (73.2) | 52 (81.3) | 233 (75.4) |
| Infection (including COVID-19) | 35 (29.7) | 37 (29.1) | 23 (35.9) | 95 (30.7) |
| Bleeding | 16 (13.6) | 13 (10.2) | 11 (17.2) | 40 (12.9) |
| Fatigue | 9 (7.6) | 14 (11.0) | 8 (12.5) | 31 (10.0) |
| Neutropenia | 9 (7.6) | 16 (12.6) | 5 (7.8) | 30 (9.7) |
| Diarrhea | 12 (10.2) | 10 (7.9) | 6 (9.4) | 28 (9.1) |
| Atrial fibrillation | 8 (6.8) | 11 (8.7) | 6 (9.4) | 25 (8.1) |
| Pyrexia | 7 (5.9) | 10 (7.9) | 7 (10.9) | 24 (7.8) |
| Arthralgia | 8 (6.8) | 10 (7.9) | 2 (3.1) | 20 (6.5) |
| Rash | 9 (7.6) | 8 (6.3) | 3 (4.7) | 20 (6.5) |
| Anemia | 11 (9.3) | 5 (3.9) | 3 (4.7) | 19 (6.1) |
| Hematoma | 7 (5.9) | 8 (6.3) | 3 (4.7) | 18 (5.8) |
| Muscle spasms | 7 (5.9) | 4 (3.1) | 3 (4.7) | 14 (4.5) |
| Hypertension | 3 (2.5) | 4 (3.1) | 6 (9.4) | 13 (4.2) |
| Back pain | 5 (4.2) | 4 (3.1) | 2 (3.1) | 11 (3.6) |
| Thrombocytopenia | 1 (0.8) | 7 (5.5) | 3 (4.7) | 11 (3.6) |
| Grade 3–4 ˜ | ||||
| Any AE | 33 (28.0) | 44 (34.6) | 20 (31.3) | 107 (34.6) |
| Neutropenia | 9 (7.6) | 12 (9.4) | 5 (7.8) | 26 (8.4) |
| Infection | 9 (7.6) | 7 (5.5) | 6 (9.4) | 20 (6.5) |
| Atrial fibrillation | 3 (2.5) | 5 (3.9) | 4 (6.3) | 12 (3.9) |
| Anemia | 5 (4.2) | 1 (0.8) | 2 (3.1) | 8 (2.6) |
| Hypertension | 0 (0.0) | 2 (1.6) | 3 (4.7) | 5 (1.6) |
| Arthralgia | 2 (1.7) | 3 (2.4) | 0 (0.0) | 5 (1.6) |
| Lymphocytosis | 2 (1.7) | 2 (1.6) | 1 (1.6) | 5 (1.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauro, F.R.; Scalzulli, P.R.; Scarfò, L.; Minoia, C.; Murru, R.; Sportoletti, P.; Frigeri, F.; Albano, F.; Di Renzo, N.; Sanna, A.; et al. Real-World Outcome of Treatment with Single-Agent Ibrutinib in Italian Patients with Chronic Lymphocytic Leukemia: Final Results of the EVIdeNCE Study. Cancers 2024, 16, 1228. https://doi.org/10.3390/cancers16061228
Mauro FR, Scalzulli PR, Scarfò L, Minoia C, Murru R, Sportoletti P, Frigeri F, Albano F, Di Renzo N, Sanna A, et al. Real-World Outcome of Treatment with Single-Agent Ibrutinib in Italian Patients with Chronic Lymphocytic Leukemia: Final Results of the EVIdeNCE Study. Cancers. 2024; 16(6):1228. https://doi.org/10.3390/cancers16061228
Chicago/Turabian StyleMauro, Francesca Romana, Potito Rosario Scalzulli, Lydia Scarfò, Carla Minoia, Roberta Murru, Paolo Sportoletti, Ferdinando Frigeri, Francesco Albano, Nicola Di Renzo, Alessandro Sanna, and et al. 2024. "Real-World Outcome of Treatment with Single-Agent Ibrutinib in Italian Patients with Chronic Lymphocytic Leukemia: Final Results of the EVIdeNCE Study" Cancers 16, no. 6: 1228. https://doi.org/10.3390/cancers16061228
APA StyleMauro, F. R., Scalzulli, P. R., Scarfò, L., Minoia, C., Murru, R., Sportoletti, P., Frigeri, F., Albano, F., Di Renzo, N., Sanna, A., Laurenti, L., Massaia, M., Cassin, R., Coscia, M., Patti, C., Pennese, E., Tafuri, A., Chiarenza, A., Galieni, P., ... Molica, S. (2024). Real-World Outcome of Treatment with Single-Agent Ibrutinib in Italian Patients with Chronic Lymphocytic Leukemia: Final Results of the EVIdeNCE Study. Cancers, 16(6), 1228. https://doi.org/10.3390/cancers16061228