
Clinical Benefit from Docetaxel +/− Ramucirumab Is Not Associated with Mutation Status in Metastatic Non-Small-Cell Lung Cancer Patients Who Progressed on Platinum Doublets and Immunotherapy

 , , , ,
, , , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
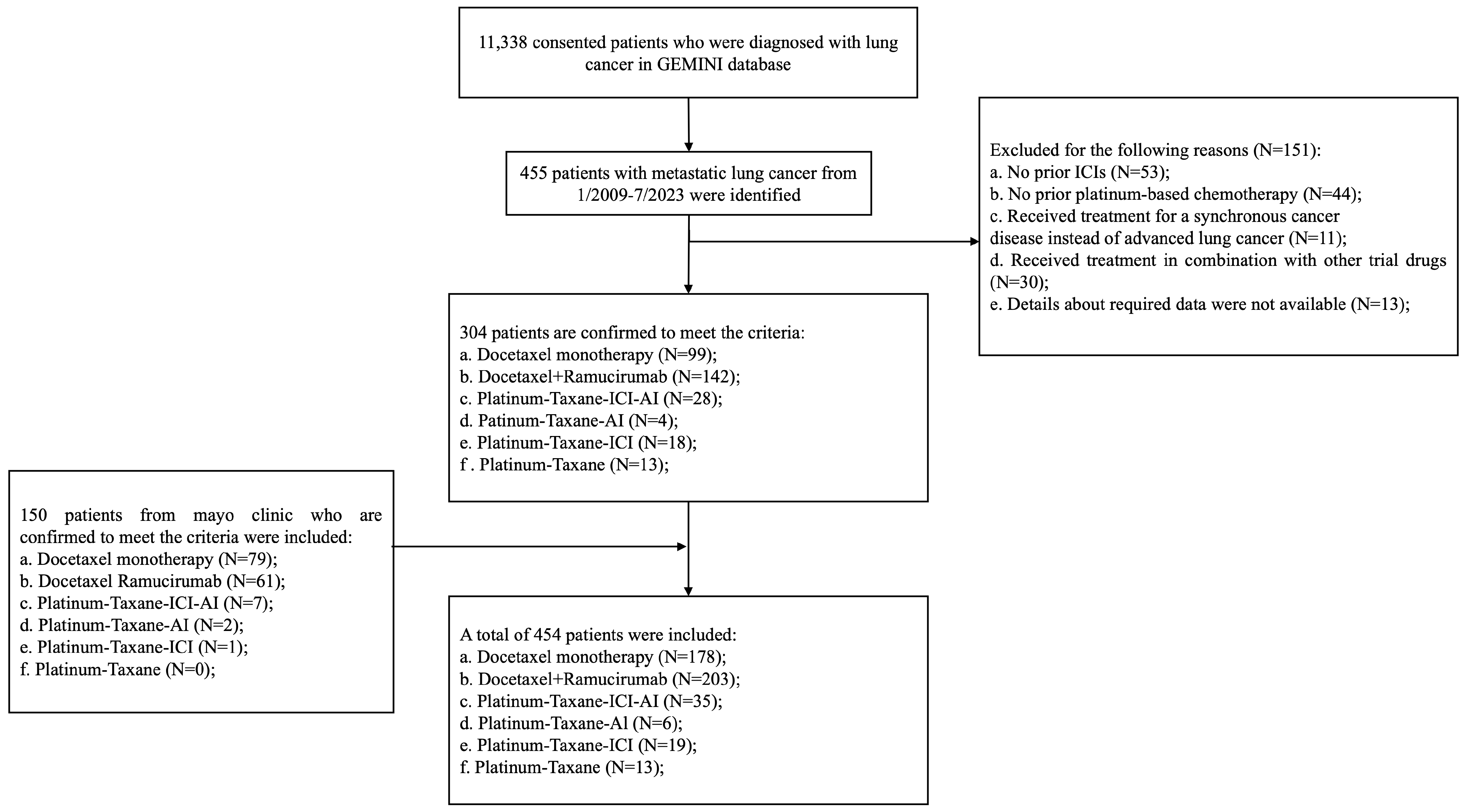
2.1. Study Population and Data Collection
2.2. Clinical Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Neither Genomic Subtype nor PD-L1 Expression Was Associated with Benefit from Docetarel+/Ramucirumab
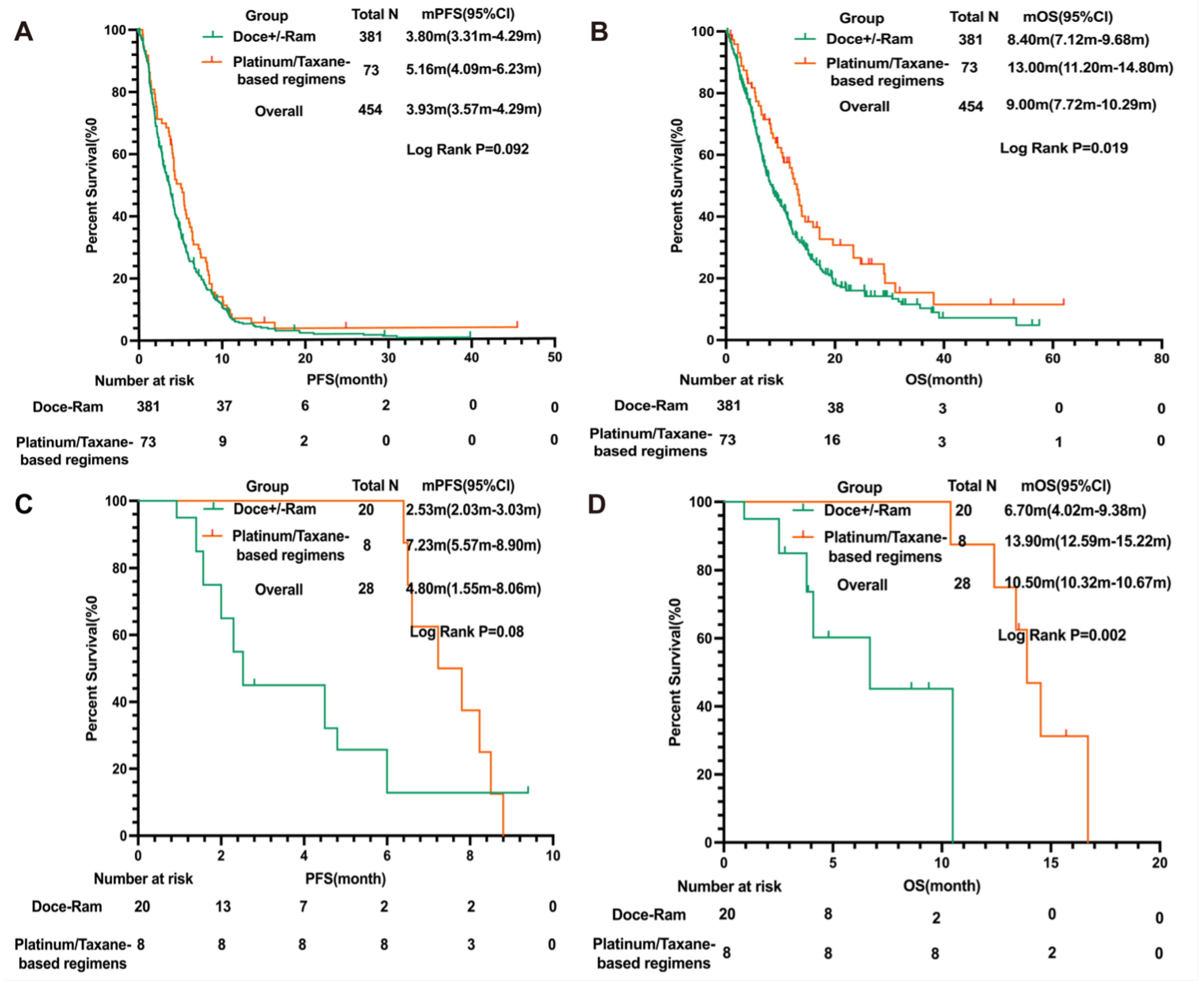
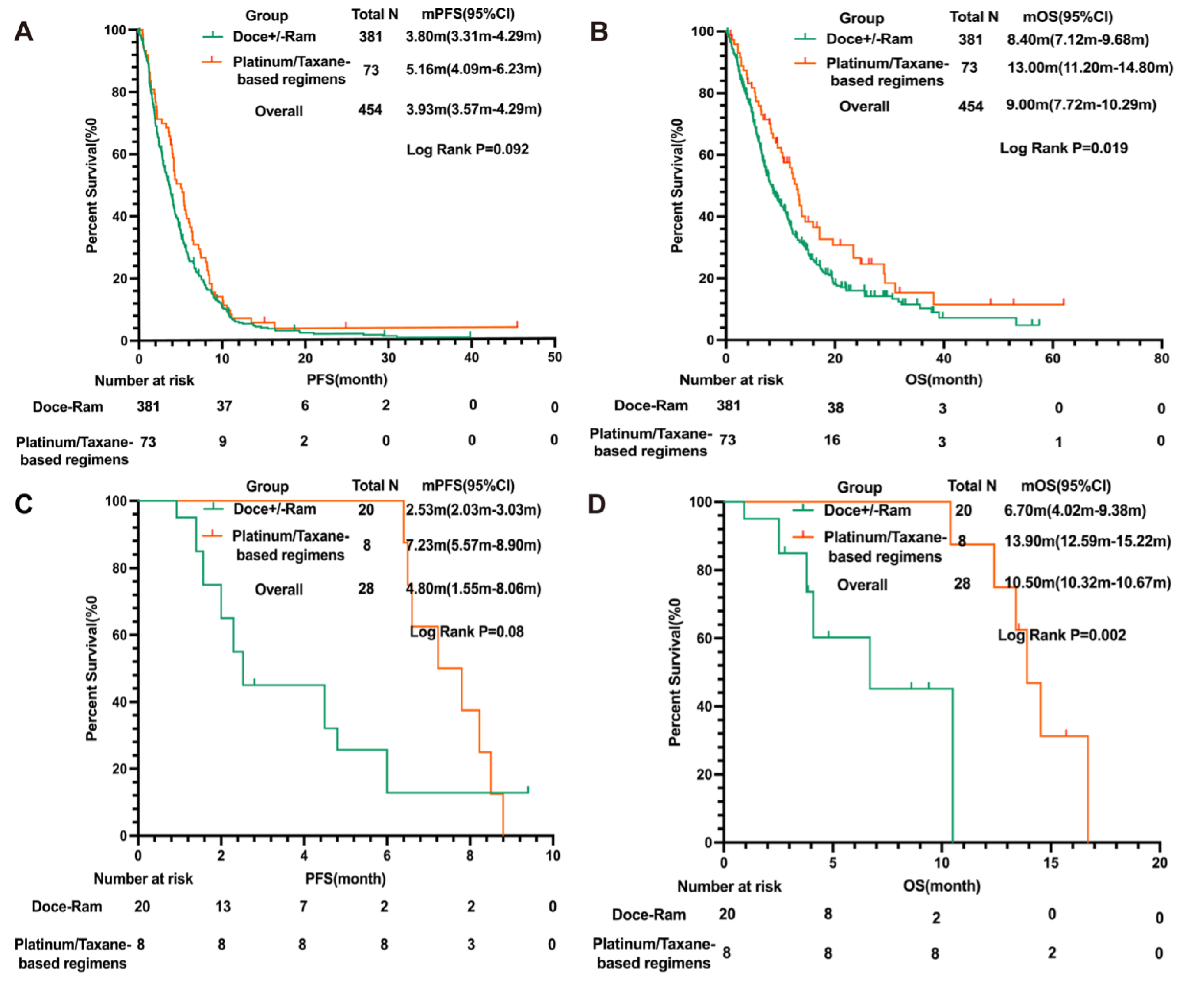
3.3. Platinum/Taxane-Based Regimens Had Superior Efficacy to Docetaxel +/− Ramucirumab
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, K.D.; Goding Sauer, A.; Ortiz, A.P.; Fedewa, S.A.; Pinheiro, P.S.; TortoleroLuna, G.; Martinez-Tyson, D.; Jemal, A.; Siegel, R.L. Cancer Statistics for Hispanics/Latinos, 2018. CA Cancer J. Clin. 2018, 68, 425–445. [Google Scholar] [CrossRef]
- Masters, G.A.; Johnson, D.H.; Temin, S. Systemic Therapy for Stage IV Non-Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Oncol. Pract. 2016, 12, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-SmallCell Lung Cancer with PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Schenker, M.; Lee, K.H.; Provencio, M.; Nishio, M.; Lesniewski-Kmak, K.; Sangha, R.; Ahmed, S.; Raimbourg, J.; Feeney, K.; et al. Nivolumab plus ipilimumab versus chemotherapy as first-line treatment in advanced non-small-cell lung cancer with high tumour mutational burden: Patient-reported outcomes results from the randomised, open-label, phase III CheckMate 227 trial. Eur. J. Cancer 2019, 116, 137–147. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef]
- Garon, E.B.; Ciuleanu, T.E.; Arrieta, O.; Prabhash, K.; Syrigos, K.N.; Goksel, T.; Park, K.; Gorbunova, V.; Kowalyszyn, R.D.; Pikiel, J.; et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): A multicentre, double-blind, randomised phase 3 trial. Lancet 2014, 384, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Mazieres, J.; Kowalski, D.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Laktionov, K.; Hermes, B.; Cicin, I.; Rodríguez-Cid, J.; et al. Health-Related Quality of Life with Carboplatin-Paclitaxel or nab-Paclitaxel with or Without Pembrolizumab in Patients with Metastatic Squamous Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 271280. [Google Scholar] [CrossRef]
- Reck, M.; Wehler, T.; Orlandi, F.; Nogami, N.; Barone, C.; Moro-Sibilot, D.; Shtivelband, M.; González Larriba, J.L.; Rothenstein, J.; Früh, M.; et al. Safety and Patient-Reported Outcomes of Atezolizumab Plus Chemotherapy with or Without Bevacizumab Versus Bevacizumab Plus Chemotherapy in Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 2530–2542. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Mok, T.S.K.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; et al. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): Key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir. Med. 2019, 7, 387401. [Google Scholar] [CrossRef]
- Hong, L.; Aminu, M.; Li, S.; Lu, X.; Petranovic, M.; Saad, M.B.; Chen, P.; Qin, K.; Varghese, S.; Rinsurongkawong, W.; et al. Efficacy and clinicogenomic correlates of response to immune checkpoint inhibitors alone or with chemotherapy in non-small cell lung cancer. Nat. Commun. 2023, 14, 695. [Google Scholar] [CrossRef]
- Negrao, M.V.; Skoulidis, F.; Montesion, M.; Schulze, K.; Bara, I.; Shen, V.; Xu, H.; Hu, S.; Sui, D.; Elamin, Y.Y.; et al. Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer. J. Immunother. Cancer 2021, 9, e002891. [Google Scholar] [CrossRef]
- Le, X.; Puri, S.; Negrao, M.V.; Nilsson, M.B.; Robichaux, J.; Boyle, T.; Hicks, J.K.; Lovinger, K.L.; Roarty, E.; Rinsurongkawong, W.; et al. Landscape of EGFR-Dependent and -Independent Resistance Mechanisms to Osimertinib and Continuation Therapy Beyond Progression in EGFR-Mutant NSCLC. Clin. Cancer Res. 2018, 24, 6195–6203. [Google Scholar] [CrossRef]
- Yoshimura, A.; Yamada, T.; Okuma, Y.; Kitadai, R.; Takeda, T.; Kanematsu, T.; Goto, H.; Yoneda, H.; Harada, T.; Kubota, Y.; et al. Retrospective analysis of docetaxel in combination with ramucirumab for previously treated non-small cell lung cancer patients. Transl. Lung Cancer Res. 2019, 8, 450–460. [Google Scholar] [CrossRef]
- Le, X.; Elamin, Y.Y.; Zhang, J. New Actions on Actionable Mutations in Lung Cancers. Cancers 2023, 15, 2917. [Google Scholar] [CrossRef] [PubMed]
- Langer, C.J. Epidermal growth factor receptor inhibition in mutation-positive non-smallcell lung cancer: Is afatinib better or simply newer? J. Clin. Oncol. 2013, 31, 3303–3306. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Bauer, T.M.; de Marinis, F.; Felip, E.; Goto, Y.; Liu, G.; Mazieres, J.; Kim, D.W.; Mok, T.; Polli, A.; et al. First-Line Lorlatinib or Crizotinib in Advanced ALKPositive Lung Cancer. N. Engl. J. Med. 2020, 383, 2018–2029. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.W.; Ou, S.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef]
- Soria, J.C.; Tan, D.S.W.; Chiari, R.; Wu, Y.L.; Paz-Ares, L.; Wolf, J.; Geater, S.L.; Orlov, S.; Cortinovis, D.; Yu, C.J.; et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): A randomised, open-label, phase 3 study. Lancet 2017, 389, 917–929. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kim, H.R.; Ahn, M.J.; Yang, J.C.; Han, J.Y.; Lee, J.S.; Hochmair, M.J.; Li, J.Y.; Chang, G.C.; Lee, K.H.; et al. Brigatinib versus Crizotinib in ALK-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2027–2039. [Google Scholar] [CrossRef]
- Planchard, D.; Besse, B.; Groen, H.J.M.; Souquet, P.J.; Quoix, E.; Baik, C.S.; Barlesi, F.; Kim, T.M.; Mazieres, J.; Novello, S.; et al. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: An openlabel, multicentre phase 2 trial. Lancet Oncol. 2016, 17, 984–993. [Google Scholar] [CrossRef]
- Heist, R.S.; Seto, T.; Han, J.; Reguart, N.; Garon, E.B.; Groen, H.J.M.; Tan, D.S.W.; Hida, T.; de Jonge, M.; Orlov, S.V.; et al. CMET-22. CAPMATINIB (INC280) IN METΔEX14-MUTATED ADVANCED NON-SMALL CELL LUNG CANCER (NSCLC): EFFICACY DATA FROM THE PHASE 2 GEOMETRY MONO-1 STUDY. Neuro-Oncology 2019, 21, vi56. [Google Scholar] [CrossRef]
- Drilon, A.; Clark, J.W.; Weiss, J.; Ou, S.I.; Camidge, D.R.; Solomon, B.J.; Otterson, G.A.; Villaruz, L.C.; Riely, G.J.; Heist, R.S.; et al. Antitumor activity of crizotinib in lung cancers harboring a MET exon 14 alteration. Nat. Med. 2020, 26, 47–51. [Google Scholar] [CrossRef]
- Gainor, J.F.; Curigliano, G.; Kim, D.W.; Lee, D.H.; Besse, B.; Baik, C.S.; Doebele, R.C.; Cassier, P.A.; Lopes, G.; Tan, D.S.W.; et al. Pralsetinib for RET fusion-positive nonsmall-cell lung cancer (ARROW): A multi-cohort, open-label, phase 1/2 study. Lancet Oncol. 2021, 22, 959–969. [Google Scholar] [CrossRef]
- Drilon, A.; Oxnard, G.R.; Tan, D.S.W.; Loong, H.H.F.; Johnson, M.; Gainor, J.; McCoach, C.E.; Gautschi, O.; Besse, B.; Cho, B.C.; et al. Efficacy of Selpercatinib in RET Fusion-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Drilon, A.; Rekhtman, N.; Arcila, M.; Wang, L.; Ni, A.; Albano, M.; Van Voorthuysen, M.; Somwar, R.; Smith, R.S.; Montecalvo, J.; et al. Cabozantinib in patients with advanced RET-rearranged non-small-cell lung cancer: An open-label, single-centre, phase 2, single-arm trial. Lancet Oncol. 2016, 17, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Drilon, A.; Wang, L.; Hasanovic, A.; Suehara, Y.; Lipson, D.; Stephens, P.; Ross, J.; Miller, V.; Ginsberg, M.; Zakowski, M.F.; et al. Response to Cabozantinib in patients with RET fusion-positive lung adenocarcinomas. Cancer Discov. 2013, 3, 630–635. [Google Scholar] [CrossRef]
- Mazières, J.; Zalcman, G.; Crinò, L.; Biondani, P.; Barlesi, F.; Filleron, T.; Dingemans, A.M.; Léna, H.; Monnet, I.; Rothschild, S.I.; et al. Crizotinib therapy for advanced lung adenocarcinoma and a ROS1 rearrangement: Results from the EUROS1 cohort. J. Clin. Oncol. 2015, 33, 992–999. [Google Scholar] [CrossRef]
- Shaw, A.T.; Ou, S.H.; Bang, Y.J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-rearranged nonsmall-cell lung cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef]
- Kazandjian, D.; Blumenthal, G.M.; Luo, L.; He, K.; Fran, I.; Lemery, S.; Pazdur, R. Benefit-Risk Summary of Crizotinib for the Treatment of Patients with ROS1 AlterationPositive, Metastatic Non-Small Cell Lung Cancer. Oncologist 2016, 21, 974–980. [Google Scholar] [CrossRef]
- Shepherd, F.A.; Domerg, C.; Hainaut, P.; Jänne, P.A.; Pignon, J.P.; Graziano, S.; Douillard, J.Y.; Brambilla, E.; Le Chevalier, T.; Seymour, L.; et al. Pooled analysis of the prognostic and predictive effects of KRAS mutation status and KRAS mutation subtype in early-stage resected non-small-cell lung cancer in four trials of adjuvant chemotherapy. J. Clin. Oncol. 2013, 31, 2173–2181. [Google Scholar] [CrossRef]
- Arbour, K.C.; Jordan, E.; Kim, H.R.; Dienstag, J.; Yu, H.A.; Sanchez-Vega, F.; Lito, P.; Berger, M.; Solit, D.B.; Hellmann, M.; et al. Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non-Small Cell Lung Cancer. Clin. Cancer Res. 2018, 24, 334–340. [Google Scholar] [CrossRef]
- Chen, Z.; Cheng, K.; Walton, Z.; Wang, Y.; Ebi, H.; Shimamura, T.; Liu, Y.; Tupper, T.; Ouyang, J.; Li, J.; et al. A murine lung cancer co-clinical trial identifies genetic modifiers of therapeutic response. Nature 2012, 483, 613–617. [Google Scholar] [CrossRef]
- Bonanno, L.; De Paoli, A.; Zulato, E.; Esposito, G.; Calabrese, F.; Favaretto, A.; Santo, A.; Conte, A.D.; Chilosi, M.; Oniga, F.; et al. LKB1 Expression Correlates with Increased Survival in Patients with Advanced Non-Small Cell Lung Cancer Treated with Chemotherapy and Bevacizumab. Clin. Cancer Res. 2017, 23, 3316–3324. [Google Scholar] [CrossRef]
- Thummalapalli, R.; Ricciuti, B.; Bandlamudi, C.; Muldoon, D.; Rizvi, H.; Elkrief, A.; Luo, J.; Alessi, J.V.; Pecci, F.; Lamberti, G.; et al. Clinical and Molecular Features of Long-term Response to Immune Checkpoint Inhibitors in Patients with Advanced NonSmall Cell Lung Cancer. Clin. Cancer Res. 2023, 29, 4408–4418. [Google Scholar] [CrossRef]
- Saad, M.B.; Hong, L.; Aminu, M.; Vokes, N.I.; Chen, P.; Salehjahromi, M.; Qin, K.; Sujit, S.J.; Lu, X.; Young, E.; et al. Predicting benefit from immune checkpoint inhibitors in patients with non-small-cell lung cancer by CT-based ensemble deep learning: A retrospective study. Lancet Digit. Health 2023, 5, e404–e420. [Google Scholar] [CrossRef]
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.M.; Gainor, J.F.; Schrock, A.B.; Hartmaier, R.J.; Trabucco, S.E.; Gay, L.; et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov. 2018, 8, 822–835. [Google Scholar] [CrossRef]
- Nakagawa, K.; Garon, E.B.; Seto, T.; Nishio, M.; Ponce Aix, S.; Paz-Ares, L.; Chiu, C.H.; Park, K.; Novello, S.; Nadal, E.; et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 1655–1669. [Google Scholar] [CrossRef] [PubMed]
- Furuya, N.; Ito, K.; Sakaguchi, T.; Hida, N.; Kakinuma, K.; Morikawa, K.; Inoue, T.; Komase, Y.; Hataji, O.; Mineshita, M. The Impact of EGFR Mutation Status and Brain Metastasis for Non-Small Cell Lung Cancer Treated with Ramucirumab plus Docetaxel. Oncology 2020, 98, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Ellis-Caleo, T.; Neal, J.W. The role of ramucirumab with docetaxel in epidermal growth factor receptor mutant and wild-type non-small cell lung cancer. J. Thorac. Dis. 2021, 13, 4864–4871. [Google Scholar] [CrossRef] [PubMed]
- Sazonova, E.V.; Kopeina, G.S.; Imyanitov, E.N.; Zhivotovsky, B. Platinum drugs and taxanes: Can we overcome resistance? Cell Death Discov. 2021, 7, 155. [Google Scholar] [CrossRef] [PubMed]
- Vaishampayan, U.; Parchment, R.E.; Jasti, B.R.; Hussain, M. Taxanes: An overview of the pharmacokinetics and pharmacodynamics. Urology 1999, 54, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Picard, M. Management of Hypersensitivity Reactions to Taxanes. Immunol. Allergy Clin. N. Am. 2017, 37, 679–693. [Google Scholar] [CrossRef]
- Garcia, M.S.; Sanchez-Pedreño, C.; Albero, M.I.; Rodenas, V. Determination of penicillamine or tiopronin in pharmaceutical preparations by flow injection analysis. J. Pharm. Biomed. Anal. 1993, 11, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Fossella, F.; Pereira, J.R.; von Pawel, J.; Pluzanska, A.; Gorbounova, V.; Kaukel, E.; Mattson, K.V.; Ramlau, R.; Szczesna, A.; Fidias, P.; et al. Randomized, multinational, phase III study of docetaxel plus platinum combinations versus vinorelbine plus cisplatin for advanced non-small-cell lung cancer: The TAX 326 study group. J. Clin. Oncol. 2003, 21, 3016–3024. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.; Crowley, J.; Bunn, P.A., Jr.; Presant, C.A.; Grevstad, P.K.; Moinpour, C.M.; Ramsey, S.D.; Wozniak, A.J.; Weiss, G.R.; Moore, D.F.; et al. Randomized phase III trial of paclitaxel plus carboplatin versus vinorelbine plus cisplatin in the treatment of patients with advanced non–small-cell lung cancer: A Southwest Oncology Group trial. J. Clin. Oncol. 2001, 19, 3210–3218. [Google Scholar] [CrossRef]
- Schiller, J.H.; Harrington, D.; Belani, C.P.; Langer, C.; Sandler, A.; Krook, J.; Zhu, J.; Johnson, D.H. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N. Engl. J. Med. 2002, 346, 92–98. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; De Marinis, F.; Rinaldi, M.; Crinò, L.; Gridelli, C.; Ricci, S.; Matano, E.; Boni, C.; Marangolo, M.; Failla, G.; et al. Phase III randomized trial comparing three platinum-based doublets in advanced non-small-cell lung cancer. J. Clin. Oncol. 2002, 20, 4285–4291. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Clinicopathological Characteristics | Overall (n = 454) | Docetaxel (n = 178) | Docetaxel + Ramucirumab (n = 203) | Platinum-Taxane-AIs-ICIs (n = 35) | Platinum-Taxane-AIs (n = 6) | Platinum-Taxane-ICIs (n = 19) | Platinum-Taxane (n = 13) |
|---|---|---|---|---|---|---|---|
| Age, years | |||||||
| Median | 64 | 65 | 64 | 59 | 56.5 | 64 | 67 |
| Range | 27–90 | 31–90 | 27–82 | 28–74 | 48–71 | 46–76 | 46–76 |
| Gender | |||||||
| Male | 231 (50.88) | 88 (49.44) | 107 (52.71) | 14 (40) | 2 (33.33) | 14 (73.68) | 6 (46.15) |
| Female | 223 (49.12) | 90 (50.56) | 96 (47.29) | 21 (60) | 4 (66.67) | 5 (26.32) | 7 (53.85) |
| Smoking History | |||||||
| Never | 124 (27.31) | 45 (25.28) | 55 (27.09) | 14 (40) | 2 (33.33) | 3 (15.80) | 5 (38.46) |
| Current | 38 (8.37) | 16 (8.99) | 15 (7.39) | 2 (5.71) | 1 (16.67) | 4 (21.05) | 0 (0) |
| Former | 292 (64.32) | 117 (65.73) | 133 (65.52) | 19 (54.29) | 3 (50) | 12 (63.16) | 8 (61.54) |
| ECOG PS | |||||||
| 0–1 | 349 (76.87) | 132 (74.16) | 162 (79.80) | 26 (74.29) | 6 (100) | 13 (68.42) | 10 (76.92) |
| 2–3 | 105 (23.13) | 46 (25.84) | 41 (21.20) | 9 (25.71) | 0 (0) | 6 (31.58) | 3 (23.08) |
| Clinical Stage | |||||||
| IIIB | 5 (1.10) | 2 (1.12) | 0 (0) | 1 (2.86) | 0 (0) | 1 (5.26) | 1 (7.69) |
| IVA | 71 (15.64) | 32 (17.98) | 28 (13.79) | 2 (5.71) | 0 (0) | 6 (31.58) | 3 (23.08) |
| IVB | 378 (83.26) | 144 (80.90) | 175 (86.21) | 32 (91.43) | 6 (100) | 12 (63.16) | 9 (69.23) |
| Race | |||||||
| White or Caucasian | 374 (82.38) | 151 (84.83) | 162 (79.80) | 29 (82.86) | 4 (60.0) | 16 (84.21) | 12 (92.31) |
| Asian | 34 (7.27) | 12 (6.74) | 15 (0.49) | 3 (8.57) | 1 (20.0) | 2 (10.53) | 1 (7.69) |
| Black or African American | 34 (7.49) | 11 (6.18) | 20 (9.85) | 1 (2.86) | 1 (20.0) | 1 (5.26) | 0 (0) |
| Hispanic or Latino | 12 (2.64) | 4 (2.25) | 6 (2.96) | 2 (5.71) | 0 (0) | 0 (0) | 0 (0) |
| Histology | |||||||
| ADC | 371 (81.72) | 145 (81.46) | 171 (84.24) | 34 (97.14) | 5 (83.33) | 6 (31.58) | 10 (76.92) |
| SQC | 64 (14.10) | 26 (14.61) | 24 (11.82) | 0 (0) | 0 (0) | 11 (57.89) | 3 (23.08) |
| Adenosquamous | 5 (1.10) | 3 (1.69) | 2 (0.99) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Carcinoid tumor | 1 (0.22) | 1 (0.56) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Large cell neuroendocrine carcinoma | 8 (1.76) | 2 (1.12) | 4 (2.25) | 0 (0) | 1 (16.67) | 1 (5.26) | 0 (0) |
| NSCLC—nonspecific subtype | 5 (1.10) | 1 (0.56) | 2 (0.99) | 1 (2.86) | 0 (0) | 1 (5.26) | 0 (0) |
| Recurrent NSCLC | |||||||
| Yes | 63 (13.88) | 32 (17.98) | 26 (12.81) | 3 (8.57) | 1 (16.67) | 1 (5.26) | 0 (0) |
| No | 391 (86.12) | 146 (82.02) | 177 (87.19) | 32 (91.43) | 5 (83.33) | 18 (94.74) | 13 (100.00) |
| Line of Treatment | |||||||
| 2 | 188 (41.41) | 65 (36.52) | 92 (45.32) | 14 (40.00) | 3 (50.00) | 8 (42.11) | 6 (46.15) |
| 3 | 144 (31.72) | 63 (35.39) | 63 (31.03) | 8 (22.86) | 1 (16.67) | 6 (31.58) | 3 (23.08) |
| 4 | 68 (14.98) | 29 (16.29) | 24 (11.82) | 6 (17.14) | 1 (16.67) | 5 (26.32) | 3 (23.08) |
| 5–10 | 54 (11.89) | 21 (11.80) | 24 (11.82) | 7 (20.00) | 1 (16.67) | 0 (0) | 1 (7.69) |
| Metastasis at Baseline | |||||||
| Brain | 175 (39.95) | 69 (38.76) | 85 (41.87) | 14 (40.00) | 3 (50) | 5 (26.32) | 2 (15.38) |
| Liver | 105 (23.97) | 38 ( (21.35) | 52 (25.62) | 11 (31.43) | 2 (33.33) | 3 (15.79) | 4 (30.77) |
| Bone | 241 (55.02) | 103 (57.87) | 114 (56.16) | 16 (45.71) | 5 (83.33) | 5 (26.32) | 6 (46.15) |
| Adrenal | 69 (15.75) | 35 (19.66) | 29 (14.29) | 5 (14.29) | 1 (16.67) | 2 (10.53) | 0 (0) |
| TX duration | 1.80 (0.70–32.9) | 1.60 (0.70–20.23) | 1.90 (0.70–32.90) | 5.30 (0.70–33.47) | 3.50 (0.70–8.30) | 3.40 (0.63–14.07) | 1.60 (0.63–5.10) |
| Reason for Treatment Discontinuation | |||||||
| Disease progression/death | 338 (77.17) | 143 (80.33) | 156 (76.85) | 27 (77.14) | 5 (83.33) | 14 (73.68) | 4 (30.77) |
| Toxicity | 59 (13.47) | 20 (11.24) | 28 (13.79) | 4 (11.43) | 1 (16.67) | 1 (5.26) | 5 (38.46) |
| Other treatment plans available | 7 (1.60) | 2 (1.12) | 3 (1.48) | 0 (0) | 0 (0) | 1 (5.26) | 2 (15.38) |
| Ongoing treatment | 5 (1.14) | 2 (1.12) | 1 (0.49) | 1 (2.86) | 0 (0) | 2 (10.53) | 1 (7.69) |
| Loss to follow-up | 9 (2.05) | 2 (1.12) | 6 (2.96) | 1 (2.86) | 0 (0) | 0 (0) | 0 (0) |
| TX completed | 20 (4.57) | 9 (5.06) | 9 (4.43) | 2 (5.71) | 0 (0) | 1 (5.26) | 1 (7.69) |
| Genomic Mutations | Docetaxel Monotherapy (n = 178) (%) | Docetaxel + Ramucirumab (n = 203) (%) | Overall (n = 381) (%) |
|---|---|---|---|
| Unknown | 15 (8.43) | 13 (6.40) | 28 (7.35) |
| TP53 alterations | |||
| Positive TP53 alterations | 69 (38.76) | 98 (48.28) | 167 (43.83) |
| Negative TP53 alterations | 94 (52.81) | 92 (45.32) | 186 (48.82) |
| KRAS alterations | |||
| Positive KRAS alterations | 48 (26.97) | 78 (38.42) | 127 (33.33) |
| G12A | 3 (1.69) | 1 (0.49) | 4 (1.05) |
| G12C | 18 (10.11) | 22 (10.84) | 40 (10.50) |
| G12D | 9 (5.06) | 22 (10.84) | 31 (8.14) |
| G12F | 1 (0.56) | 1 (0.49) | 2 (0.52) |
| G12V | 8 (4.49) | 17 (8.37) | 25 (6.56) |
| G13C | 1 (0.56) | 3 (1.48) | 5 (1.31) |
| G13D | 1 (0.56) | 2 (0.99) | 3 (0.79) |
| G12V+G13D | 1 (0.56) | 0 (0) | 1 (0.26) |
| Q61L | 0 (0) | 2 (0.99) | 2 (0.52) |
| Q61K | 1 (0.56) | 0 (0) | 1 (0.26) |
| Q61H | 2 (1.12) | 1 (0.49) | 3 (0.79) |
| Other KRAS alterations | 3 (1.69) | 7 (3.45) | 10 (2.62) |
| Negative KRAS alterations | 115 (64.61) | 112 (55.17) | 226 (59.32) |
| EGFR alterations | |||
| Positive EGFR alterations | 29 (16.29) | 36 (17.73) | 65 (17.06) |
| EGFR Del19/EGFR L858R(+/−T790M) | 14 (7.87) | 20 (9.85) | 34 (8.92) |
| EGFR Exon20 ins | 6 (3.37) | 5 (2.46) | 11 (2.89) |
| Other atypical EGFR mutations | 2 (1.12) | 0 (0) | 2 (0.52) |
| Nonactionable EGFR alterations | 7 (3.93) | 11 (5.42) | 18 (4.72) |
| Negative EGFR alterations | 134 (75.28) | 154 (75.86) | 288 (75.59) |
| STK11 alterations | |||
| Positive STK11 alterations | 16 (8.99) | 16 (7.88) | 32 (8.40) |
| Negative STK11 alterations | 147 (82.58) | 174 (85.71) | 321 (84.25) |
| ERBB2 (HER2) alterations | |||
| Positive ERBB2 (HER2) alterations | 11 (6.18) | 15 (7.39) | 26 (6.82) |
| Negative ERBB2 (HER2) alterations | 152 (85.39) | 175 (86.21) | 327 (85.83) |
| MET alterations | |||
| Positive MET alterations | 16 (8.99) | 8 (3.94) | 24 (6.30) |
| MET amplification | 8 (4.49) | 7 (3.45) | 15 (3.94) |
| MET exon14 skipping mutation | 2 (1.12) | 0 (0) | 2 (0.52) |
| Other MET alterations | 6 (3.37) | 1 (0.49) | 7 (1.84) |
| Negative MET alterations | 147 (82.58) | 182 (89.66) | 329 (86.35) |
| PIK3CA alterations | |||
| Positive PIK3CA alterations | 8 (4.49) | 11 (5.42) | 19 (4.99) |
| Negative PIK3CA alterations | 155 (87.08) | 179 (88.18) | 334 (87.66) |
| BRAF alterations | |||
| Positive BRAF alterations | 10 (5.62) | 8 (3.94) | 18 (4.72) |
| BRAF V600E | 2 (1.12) | 4 (1.97) | 6 (1.57) |
| Other BRAF alterations | 8 (4.49) | 4 (1.97) | 12 (3.15) |
| Negative KRAS alterations | 153 (85.96) | 182 (89.66) | 335 (87.93) |
| ALK alterations | |||
| Positive ALK alterations | 7 (3.93) | 4 (1.97) | 11 (2.89) |
| ALK-EML4 fusion | 1 (0.56) | 3 (1.48) | 4 (1.05) |
| Other ALK alterations | 6 (3.37) | 1 (0.49) | 7 (1.84) |
| Negative PIK3CA alterations | 156 (87.64) | 186 (91.63) | 342 (89.76) |
| NTRK alterations | |||
| Positive NTRK alterations | 3 (1.69) | 4 (1.97) | 7 (1.84) |
| NTRK1/2/3 gene fusion positive | 0 (0) | 1 (0.49) | 1 (0.26) |
| Other NTRK alterations | 3 (1.69) | 3 (1.48) | 6 (1.57) |
| Negative NTRK alterations | 160 (89.89) | 186 (91.63) | 346 (90.81) |
| ROS1 alterations | |||
| Positive ROS1 alterations | 5 (2.81) | 1 (0.49) | 6 (1.57) |
| ROS1 translocation | 2 (1.12) | 1 (0.49) | 3 (0.79) |
| Other ROS1 alterations | 3 (1.69) | 0 (0) | 3 (0.79) |
| Negative ROS1 alterations | 158 (88.76) | 189 (93.10) | 347 (91.08) |
| RET alterations | |||
| Positive MET alterations | 2 (1.12) | 3 (1.48) | 5 (1.31) |
| RET rearrangement | 0 (0) | 1 (0.49) | 1 (0.26) |
| Other RET alterations | 2 (1.12) | 2 (0.99) | 4 (1.05) |
| Negative MET alterations | 161 (90.45) | 187 (92.12) | 348 (91.34) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, K.; Wang, K.; Li, S.; Hong, L.; Padmakumar, P.; Waree, R.; Hubert, S.M.; Le, X.; Vokes, N.; Rai, K.; et al. Clinical Benefit from Docetaxel +/− Ramucirumab Is Not Associated with Mutation Status in Metastatic Non-Small-Cell Lung Cancer Patients Who Progressed on Platinum Doublets and Immunotherapy. Cancers 2024, 16, 935. https://doi.org/10.3390/cancers16050935
Qin K, Wang K, Li S, Hong L, Padmakumar P, Waree R, Hubert SM, Le X, Vokes N, Rai K, et al. Clinical Benefit from Docetaxel +/− Ramucirumab Is Not Associated with Mutation Status in Metastatic Non-Small-Cell Lung Cancer Patients Who Progressed on Platinum Doublets and Immunotherapy. Cancers. 2024; 16(5):935. https://doi.org/10.3390/cancers16050935
Chicago/Turabian StyleQin, Kang, Kaiwen Wang, Shenduo Li, Lingzhi Hong, Priyadharshini Padmakumar, Rinsurongkawong Waree, Shawna M. Hubert, Xiuning Le, Natalie Vokes, Kunal Rai, and et al. 2024. "Clinical Benefit from Docetaxel +/− Ramucirumab Is Not Associated with Mutation Status in Metastatic Non-Small-Cell Lung Cancer Patients Who Progressed on Platinum Doublets and Immunotherapy" Cancers 16, no. 5: 935. https://doi.org/10.3390/cancers16050935
APA StyleQin, K., Wang, K., Li, S., Hong, L., Padmakumar, P., Waree, R., Hubert, S. M., Le, X., Vokes, N., Rai, K., Vaporciyan, A., Gibbons, D. L., Heymach, J. V., Lee, J. J., Woodman, S. E., Chung, C., Jaffray, D. A., Altan, M., Lou, Y., & Zhang, J. (2024). Clinical Benefit from Docetaxel +/− Ramucirumab Is Not Associated with Mutation Status in Metastatic Non-Small-Cell Lung Cancer Patients Who Progressed on Platinum Doublets and Immunotherapy. Cancers, 16(5), 935. https://doi.org/10.3390/cancers16050935