

A Preliminary Evaluation of Advanced Oxidation Protein Products (AOPPs) as a Potential Approach to Evaluating Prognosis in Early-Stage Breast Cancer Patients and Its Implication in Tumour Angiogenesis: A 7-Year Single-Centre Study
 , , , ,
, , , , 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
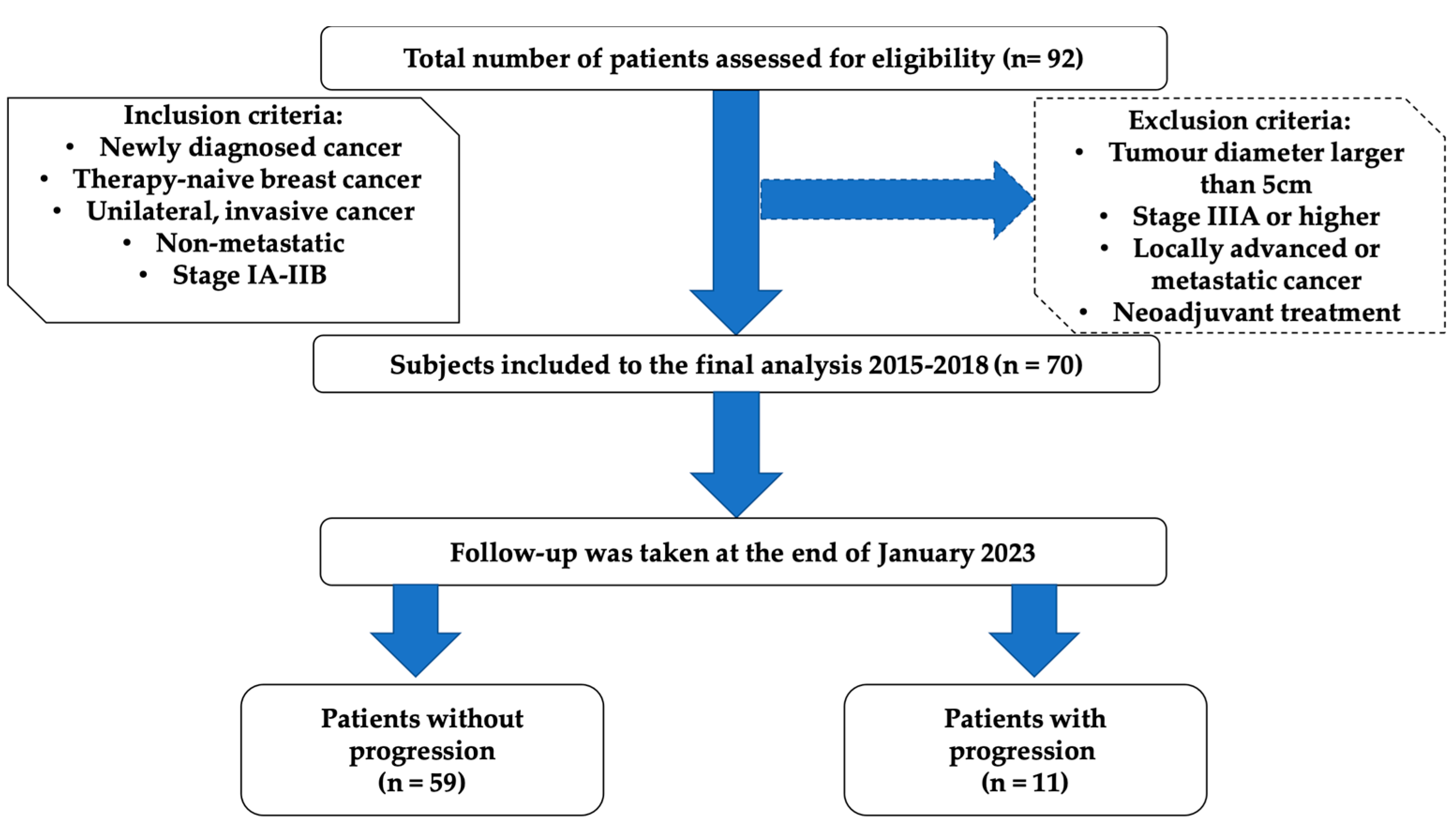
2.1. Patient Samples and Clinical Data
2.2. Adjuvant Therapy
2.3. Patients Follow-Up
2.4. Blood Collection
2.5. Measurements of AOPP
2.6. Measurements of Angiogenic Factors
2.7. Statistical Analysis
3. Results
3.1. Effect of Undergone Procedures, Clinical, and Molecular Characteristics on AOPP Concentration
3.2. The Dependence between AOPP Levels and Angiogenic Biomarkers
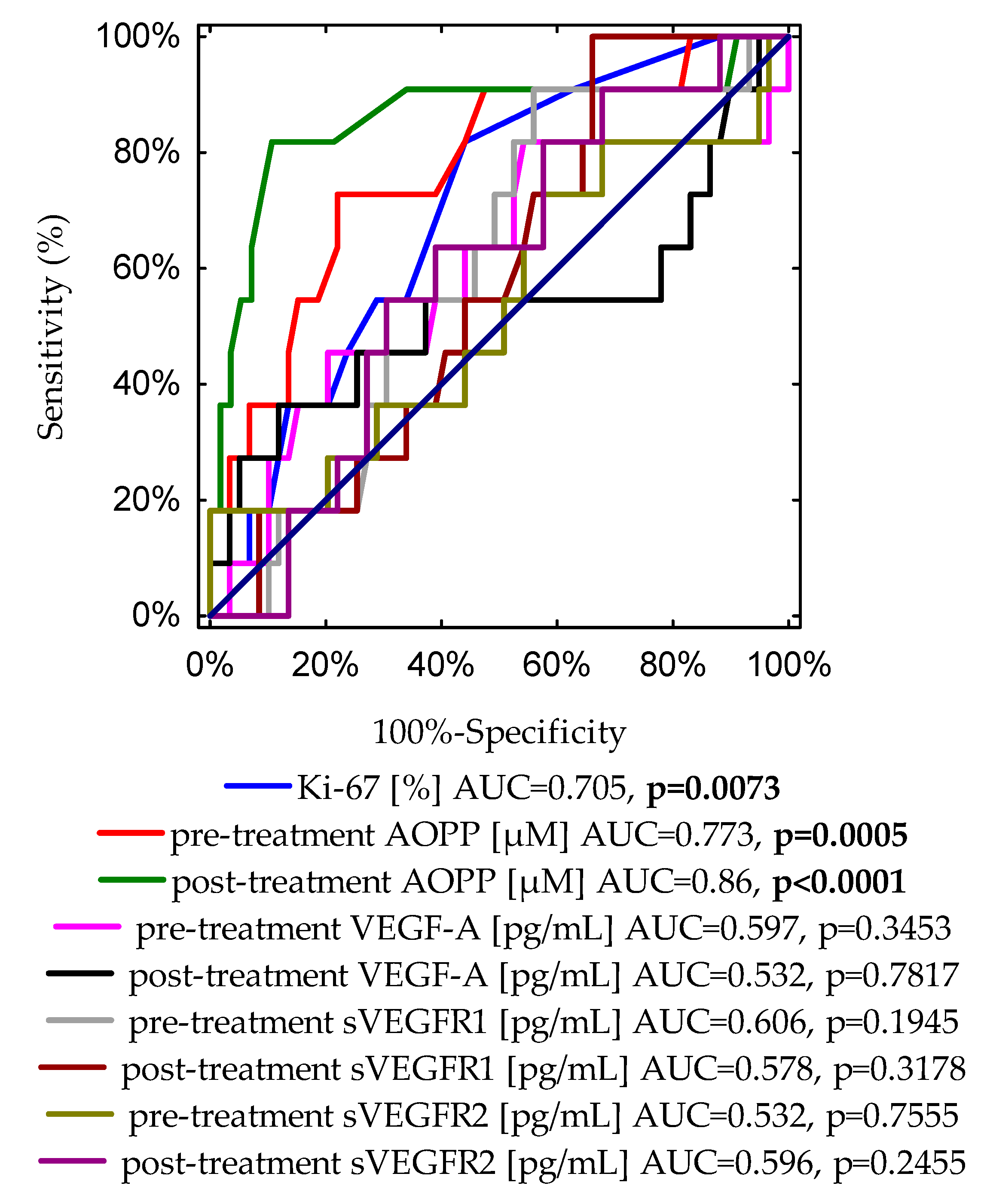
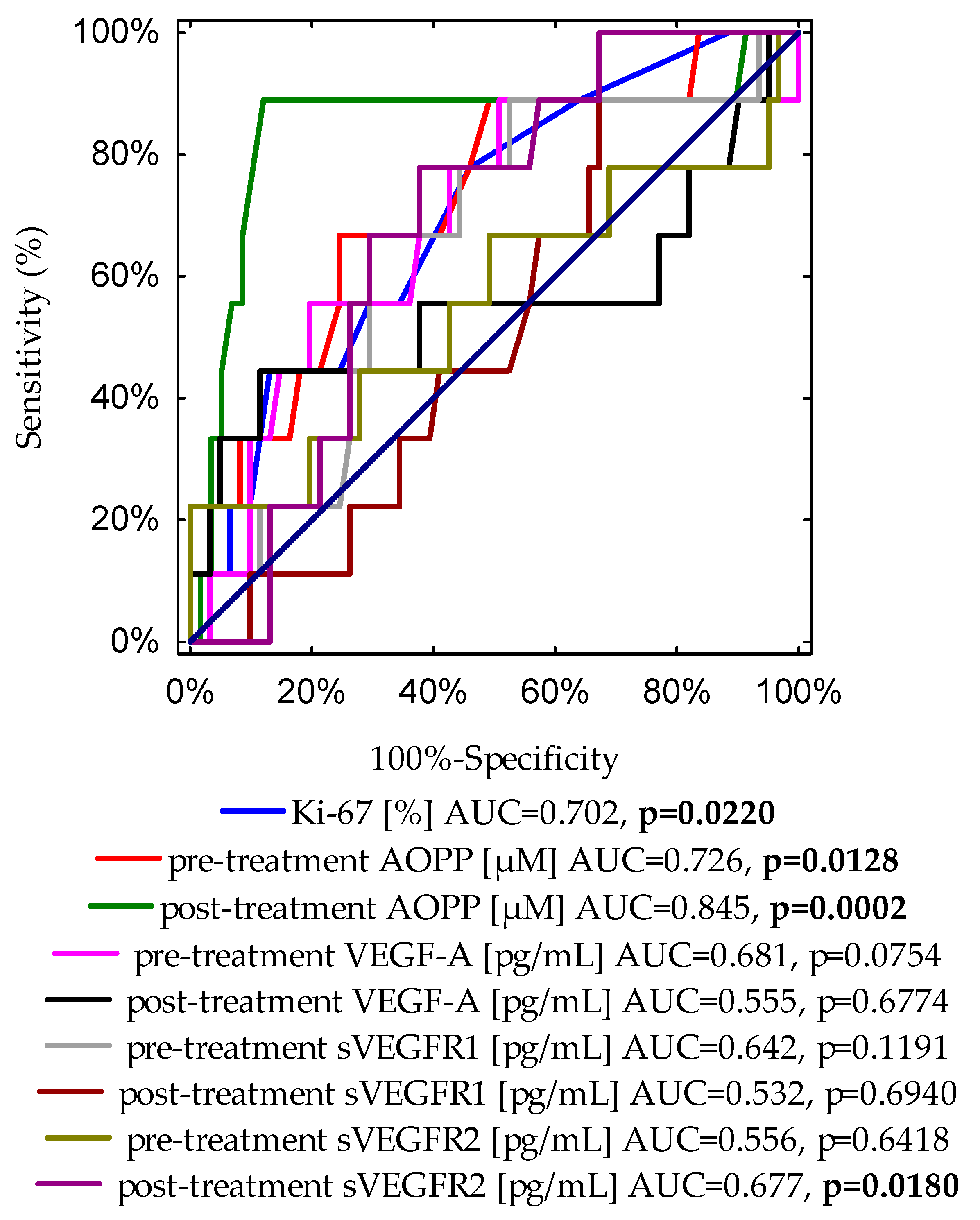
3.3. The Receiver Operating Characteristic (ROC) for Identifying Markers of Disease Progression
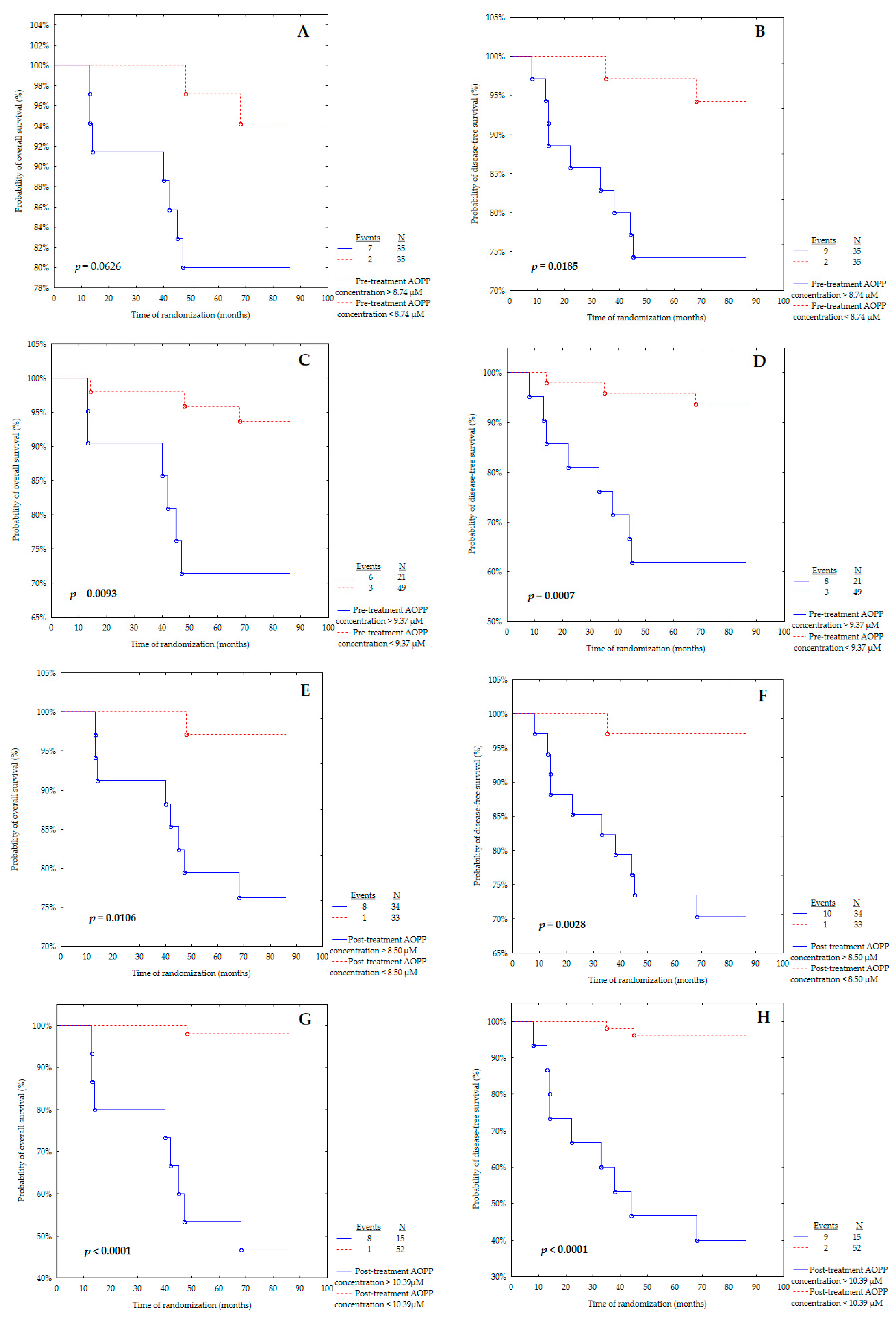
3.4. Survival Analysis Regarding Pre- and Post-Treatment AOPP Concentrations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Jafari, S.H.; Saadatpour, Z.; Salmaninejad, A.; Momeni, F.; Mokhtari, M.; Nahand, J.S.; Rahmati, M.; Mirzaei, H.; Kianmehr, M. Breast Cancer Diagnosis: Imaging Techniques and Biochemical Markers. J. Cell Physiol. 2018, 233, 5200–5213. [Google Scholar] [CrossRef]
- National Cancer Institute Female Breast Cancer: Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/breast.html (accessed on 18 March 2023).
- Wang, R.; Zhu, Y.; Liu, X.; Liao, X.; He, J.; Niu, L. The Clinicopathological Features and Survival Outcomes of Patients with Different Metastatic Sites in Stage IV Breast Cancer. BMC Cancer 2019, 19, 1091. [Google Scholar] [CrossRef]
- Madu, C.O.; Wang, S.; Madu, C.O.; Lu, Y. Angiogenesis in Breast Cancer Progression, Diagnosis, and Treatment. J. Cancer 2020, 11, 4474–4494. [Google Scholar] [CrossRef]
- Ayoub, N.M.; Jaradat, S.K.; Al-Shami, K.M.; Alkhalifa, A.E. Targeting Angiogenesis in Breast Cancer: Current Evidence and Future Perspectives of Novel Anti-Angiogenic Approaches. Front. Pharmacol. 2022, 13, 838133. [Google Scholar] [CrossRef]
- Mdkhana, B.; Goel, S.; Saleh, M.A.; Siddiqui, R.; Khan, N.A.; Elmoselhi, A.B. Role of Oxidative Stress in Angiogenesis and the Therapeutic Potential of Antioxidants in Breast Cancer. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 4677–4692. [Google Scholar]
- Lugano, R.; Ramachandran, M.; Dimberg, A. Tumor Angiogenesis: Causes, Consequences, Challenges and Opportunities. Cell Mol. Life Sci. 2020, 77, 1745–1770. [Google Scholar] [CrossRef]
- Yang, F.; Jin, C.; Jiang, Y.J.; Li, J.; Di, Y.; Fu, D.L. Potential Role of Soluble VEGFR-1 in Antiangiogenesis Therapy for Cancer. Expert Rev. Anticancer. Ther. 2011, 11, 541–549. [Google Scholar] [CrossRef]
- Bando, H.; Weich, H.A.; Brokelmann, M.; Horiguchi, S.; Funata, N.; Ogawa, T.; Toi, M. Association between Intratumoral Free and Total VEGF, Soluble VEGFR-1, VEGFR-2 and Prognosis in Breast Cancer. Br. J. Cancer 2005, 92, 553–561. [Google Scholar] [CrossRef]
- Cao, J.; Yang, R.; Smith, T.E.; Evans, S.; McCollum, G.W.; Pomerantz, S.C.; Petley, T.; Harris, I.R.; Penn, J.S. Human Umbilical Tissue-Derived Cells Secrete Soluble VEGFR1 and Inhibit Choroidal Neovascularization. Mol. Ther. Methods Clin. Dev. 2019, 14, 37–46. [Google Scholar] [CrossRef]
- Thielemann, A.; Baszczuk, A.; Kopczyński, Z.; Kopczyński, P.; Grodecka-Gazdecka, S. Clinical Usefulness of Assessing VEGF and Soluble Receptors SVEGFR-1 and SVEGFR-2 in Women with Breast Cancer. Ann. Agric. Environ. Med. 2013, 20, 293–297. [Google Scholar]
- Gurer-Orhan, H.; Ince, E.; Konyar, D.; Saso, L.; Suzen, S. The Role of Oxidative Stress Modulators in Breast Cancer. Curr. Med. Chem. 2017, 25, 4084–4101. [Google Scholar] [CrossRef]
- Schetter, A.J.; Heegaard, N.H.H.; Harris, C.C. Inflammation and Cancer: Interweaving MicroRNA, Free Radical, Cytokine and P53 Pathways. Carcinogenesis 2009, 31, 37–49. [Google Scholar] [CrossRef]
- Sawicka, E.; Kratz, E.M.; Szymańska, B.; Guzik, A.; Wesołowski, A.; Kowal, P.; Pawlik-Sobecka, L.; Piwowar, A. Preliminary Study on Selected Markers of Oxidative Stress, Inflammation and Angiogenesis in Patients with Bladder Cancer. Pathol. Oncol. Res. 2020, 26, 821–831. [Google Scholar] [CrossRef] [PubMed]
- Komosinska-Vassev, K.; Olczyk, P.; Winsz-Szczotka, K.; Kuznik-Trocha, K.; Klimek, K.; Olczyk, K. Age- and Gender-Related Alteration in Plasma Advanced Oxidation Protein Products (AOPP) and Glycosaminoglycan (GAG) Concentrations in Physiological Ageing. Clin. Chem. Lab. Med. 2012, 50, 557–563. [Google Scholar] [CrossRef]
- Bagyura, Z.; Takács, A.; Kiss, L.; Dósa, E.; Vadas, R.; Nguyen, T.D.; Dinya, E.; Soós, P.; Szelid, Z.; Láng, O.; et al. Level of Advanced Oxidation Protein Products Is Associated with Subclinical Atherosclerosis. BMC Cardiovasc. Disord. 2022, 22, 5. [Google Scholar] [CrossRef]
- Baskol, G.; Gumus, K.; Oner, A.; Arda, H.; Karakucuk, S. The Role of Advanced Oxidation Protein Products and Total Thiols in Diabetic Retinopathy. Eur. J. Ophthalmol. 2018, 18, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.T.; Wang, S.S.; Zhang, M.; Huang, L.P.; Tian, J.W.; Yu, Y.H.; Wang, Z.J.; Zhong, M. Advanced Oxidation Protein Products Enhances Soluble Fms-like Tyrosine Kinase 1 Expression in Trophoblasts: A Possible Link between Oxidative Stress and Preeclampsia. Placenta 2013, 34, 949–952. [Google Scholar] [CrossRef]
- Wybranowski, T.; Napiórkowska, M.; Bosek, M.; Pyskir, J.; Ziomkowska, B.; Cyrankiewicz, M.; Pyskir, M.; Pilaczyńska-Cemel, M.; Rogańska, M.; Kruszewski, S.; et al. Study of Albumin Oxidation in COVID-19 Pneumonia Patients: Possible Mechanisms and Consequences. Int. J. Mol. Sci. 2022, 23, 10103. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Zhang, Y.; Chen, J.; Mei, C.; Xiong, F.; Shi, W.; Zhou, W.; Liu, X.; Sun, S.; Tian, J.; et al. Association between Serum Advanced Oxidation Protein Products and Mortality Risk in Maintenance Hemodialysis Patients. J. Transl. Med. 2021, 19, 284. [Google Scholar] [CrossRef]
- Liu, J.; Wen, S.; Lin, Y.; Yang, X.; Liu, Z.; Quan, S.; Song, Y. Advanced Oxidation Protein Products Change Biological Behaviors of Rat Endometrial Epithelial Cells by Activating ERK/P38 Signaling Pathways. Biol. Open 2020, 9, bio048876. [Google Scholar] [CrossRef]
- Xian, L.-W.; Li, T.-P.; Wei, Y.-E.; Wu, S.-P.; Ma, L. Relation of Advanced Oxidation Protein Products with VEGF and TGF-Β1 in Colon Cancer Cells Exposed to Intermittent Hypoxia. Nan Fang Yi Ke Da Xue Xue Bao 2011, 31, 619–623. [Google Scholar] [PubMed]
- Zhou, L.L.; Cao, W.; Xie, C.; Tian, J.; Zhou, Z.; Zhou, Q.; Zhu, P.; Li, A.; Liu, Y.; Miyata, T.; et al. The Receptor of Advanced Glycation End Products Plays a Central Role in Advanced Oxidation Protein Products-Induced Podocyte Apoptosis. Kidney Int. 2012, 82, 759–770. [Google Scholar] [CrossRef]
- Lou, A.; Wang, L.; Lai, W.; Zhu, D.; Wu, W.; Wang, Z.; Cai, Z.; Yang, M.; Yang, M. Advanced Oxidation Protein Products Induce Inflammatory Responses and Invasive Behaviour in Fibroblast-like Synoviocytes via the RAGE-NF-ΚB Pathway. Bone Joint Res. 2021, 10, 259–268. [Google Scholar] [CrossRef]
- Guo, Z.J.; Niu, H.X.; Hou, F.F.; Zhang, L.; Fu, N.; Nagai, R.; Lu, X.; Chen, B.H.; Shan, Y.X.; Tian, J.W.; et al. Advanced Oxidation Protein Products Activate Vascular Endothelial Cells via a RAGE-Mediated Signaling Pathway. Antioxid. Redox Signal 2008, 10, 1699–1712. [Google Scholar] [CrossRef]
- Kim, Y.-W.; Byzova, T.V. Oxidative Stress in Angiogenesis and Vascular Disease. Blood 2014, 123, 625–631. [Google Scholar] [CrossRef]
- Huang, Q.; Ji, M.; Li, F.; Li, Y.; Zhou, X.; Hsueh, C.; Zhou, L. Diagnostic and Prognostic Value of Plasma Cell-Free DNA Com- bined with VEGF-C in Laryngeal Squamous Cell Carcinoma. Mol. Cell Probes 2023, 67, 101895. [Google Scholar] [CrossRef] [PubMed]
- Dao, J.; Conway, P.J.; Subramani, B.; Meyyappan, D.; Russell, S.; Mahadevan, D. Using CfDNA and CtDNA as Oncologic Markers: A Path to Clinical Validation. Int. J. Mol. Sci. 2023, 24, 13219. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.; Su, L.; Qian, C. Circulating Tumor DNA: A Promising Biomarker in the Liquid Biopsy of Cancer. Oncotarget 2016, 7, 48832. [Google Scholar] [CrossRef]
- Thierry, A.R.; El Messaoudi, S.; Gahan, P.B.; Anker, P.; Stroun, M. Origins, Structures, and Functions of Circulating DNA in Oncology. Cancer Metastasis Rev. 2016, 35, 347. [Google Scholar] [CrossRef]
- Tumburu, L.; Ghosh-Choudhary, S.; Seifuddin, F.T.; Barbu, E.A.; Yang, S.; Ahmad, M.M.; Wilkins, L.H.W.; Tunc, I.; Sivakumar, I.; Nichols, J.S.; et al. Circulating Mitochondrial DNA Is a Proinflammatory DAMP in Sickle Cell Disease. Blood 2021, 137, 3116. [Google Scholar] [CrossRef]
- Dawson, S.-J.; Tsui, D.W.Y.; Murtaza, M.; Biggs, H.; Rueda, O.M.; Chin, S.-F.; Dunning, M.J.; Gale, D.; Forshew, T.; Mahler-Araujo, B.; et al. Analysis of Circulating Tumor DNA to Monitor Metastatic Breast Cancer. N. Engl. J. Med. 2013, 368, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Gu, J.; Liu, R.; Xu, F.; Qian, H.; He, Q.; Meng, W. Release of Mitochondrial DNA Correlates with Peak Inflammatory Cytokines in Patients with Acute Myocardial Infarction. Anatol. J. Cardiol. 2017, 17, 224–228. [Google Scholar]
- Alekseeva, L.; Mironova, N. Role of Cell-Free DNA and Deoxyribonucleases in Tumor Progression. Int. J. Mol. Sci. 2021, 22, 12246. [Google Scholar] [CrossRef] [PubMed]
- Korabecna, M.; Zinkova, A.; Brynychova, I.; Chylikova, B.; Prikryl, P.; Sedova, L.; Neuzil, P.; Seda, O. Cell-Free DNA in Plasma as an Essential Immune System Regulator. Sci. Rep. 2020, 10, 17478. [Google Scholar] [CrossRef] [PubMed]
- Krychtiuk, K.A.; Wurm, R.; Ruhittel, S.; Lenz, M.; Huber, K.; Wojta, J.; Heinz, G.; Hülsmann, M.; Speidl, W.S. Release of Mitochondrial DNA Is Associated with Mortality in Severe Acute Heart Failure. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 419–428. [Google Scholar] [CrossRef]
- Gaál Kovalčíková, A.; Janovičová, L.; Hodosy, J.; Bábíčková, J.; Vavrincová-Yaghi, D.; Vavrinec, P.; Boor, P.; Podracká, L.; Šebeková, K.; Celec, P.; et al. Extracellular DNA Concentrations in Various Aetiologies of Acute Kidney Injury. Sci. Rep. 2022, 12, 16812. [Google Scholar] [CrossRef]
- Barbalata, T.; Scarlatescu, A.I.; Sanda, G.M.; Toma, L.; Stancu, C.S.; Dorobantu, M.; Micheu, M.M.; Sima, A.V.; Niculescu, L.S. Mitochondrial DNA Together with MiR-142-3p in Plasma Can Predict Unfavorable Outcomes in Patients after Acute Myocardial Infarction. Int. J. Mol. Sci. 2022, 23, 9947. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, Q.; Yuan, K.; Yuan, J. MtDNA in the Pathogenesis of Cardiovascular Diseases. Dis. Markers 2021, 2021, 7157109. [Google Scholar] [CrossRef]
- Demkow, U. Molecular Mechanisms of Neutrophil Extracellular Trap (NETs) Degradation. Int. J. Mol. Sci. 2023, 24, 4896. [Google Scholar] [CrossRef]
- Papayannopoulos, V. Neutrophil Extracellular Traps in Immunity and Disease. Nat. Rev. Immunol. 2017, 18, 134–147. [Google Scholar] [CrossRef]
- Arnhold, J. The Dual Role of Myeloperoxidase in Immune Response. Int. J. Mol. Sci. 2020, 21, 8057. [Google Scholar] [CrossRef]
- Rizo-Téllez, S.A.; Sekheri, M.; Filep, J.G. Myeloperoxidase: Regulation of Neutrophil Function and Target for Therapy. Antioxidants 2022, 11, 2302. [Google Scholar] [CrossRef]
- Descamps-Latscha, B.; Witko-Sarsat, V. Importance of Oxidatively Modified Proteins in Chronic Renal Failure. Kidney Int. Suppl. 2001, 78, S108–S113. [Google Scholar] [CrossRef]
- Capeillère-Blandin, C.; Gausson, V.; Descamps-Latscha, B.; Witko-Sarsat, V. Biochemical and Spectrophotometric Significance of Advanced Oxidized Protein Products. Biochim. Biophys. Acta Mol. Basis Dis. 2004, 1689, 91–102. [Google Scholar] [CrossRef]
- Yue, Q.; Song, Y.; Liu, Z.; Zhang, L.; Yang, L.; Li, J. Receptor for Advanced Glycation End Products (RAGE): A Pivotal Hub in Immune Diseases. Molecules 2022, 27, 4922. [Google Scholar] [CrossRef] [PubMed]
- Fink, K.; Boratyński, J. The Role of Metalloproteinases in Modification of Extracellular Matrix in Invasive Tumor Growth, Metastasis and Angiogenesis. Adv. Hyg. Exp. Med. 2012, 66, 609–628. [Google Scholar] [CrossRef] [PubMed]
- Witko-Sarsat, V.; Friedlander, M.; Capeillere-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced Oxidation Protein Products as a Novel Marker of Oxidative Stress in Uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef]
- Hanasand, M.; Omdal, R.; Norheim, K.B.; Gøransson, L.G.; Brede, C.; Jonsson, G. Improved Detection of Advanced Oxidation Protein Products in Plasma. Clin. Chim. Acta 2012, 413, 901–906. [Google Scholar] [CrossRef]
- Zarychta, E.; Rhone, P.; Bielawski, K.; Rosc, D.; Szot, K.; Zdunska, M.; Ruszkowska-Ciastek, B. Elevated Plasma Levels of Tissue Factor as a Valuable Diagnostic Biomarker with Relevant Efficacy for Prediction of Breast Cancer Morbidity. J. Physiol. Pharmacol. 2018, 69, 921–931. [Google Scholar]
- American Cancer Society. About Breast Cancer. Available online: https://www.cancer.org/content/dam/CRC/PDF/Public/8577.00.pdf (accessed on 30 April 2023).
- Abd El-Khalik, S.R.; Hafez, Y.M.; Elkholy, R.A. The Role of Circulating Soluble Fms-like Tyrosine Kinase-1 in Patients with Diabetic Foot Ulcer: A Possible Mechanism of Pathogenesis via a Novel Link between Oxidative Stress, Inflammation and Angiogenesis. Microvasc. Res. 2020, 130, 103987. [Google Scholar] [CrossRef]
- Kundaktepe, B.P.; Sozer, V.; Durmus, S.; Kocael, P.C.; Kundaktepe, F.O.; Papila, C.; Gelisgen, R.; Uzun, H. The Evaluation of Oxidative Stress Parameters in Breast and Colon Cancer. Medicine 2021, 100, e25104. [Google Scholar] [CrossRef]
- Kilic, N.; Yavuz Taslipinar, M.; Guney, Y.; Tekin, E.; Onuk, E. An Investigation into the Serum Thioredoxin, Superoxide Dismutase, Malondialdehyde, and Advanced Oxidation Protein Products in Patients with Breast Cancer. Ann. Surg. Oncol. 2014, 21, 4139–4143. [Google Scholar] [CrossRef]
- Salehi, S.S.; Mirmiranpour, H.; Rabizadeh, S.; Esteghamati, A.; Tomasello, G.; Alibakhshi, A.; Najafi, N.; Rajab, A.; Nakhjavani, M. Improvement in Redox Homeostasis after Cytoreductive Surgery in Colorectal Adenocarcinoma. Oxid. Med. Cell. Longev. 2021, 2021, 8864905. [Google Scholar] [CrossRef]
- Koike, A.; Robles, B.E.F.; da Silva Bonacini, A.G.; de Alcantara, C.C.; Reiche, E.M.V.; Dichi, I.; Maes, M.; Cecchini, R.; Simão, A.N.C. Thiol Groups as a Biomarker for the Diagnosis and Prognosis of Prostate Cancer. Sci. Rep. 2020, 10, 9093. [Google Scholar] [CrossRef]
- Otsmane, A.; Kacimi, G.; Adane, S.; Cherbal, F.; Aouichat Bouguerra, S. Clinico-Epidemiological Profile and Redox Imbalance of Lung Cancer Patients in Algeria. J. Med. Life 2018, 11, 210–217. [Google Scholar] [CrossRef]
- Kosova, F.; Çetin, B.; Akinci, M.; Aslan, S.; Ari, Z.; Sepici, A.; Altan, N.; Çetin, A. Advanced Oxidation Protein Products, Ferrous Oxidation in Xylenol Orange, and Malondialdehyde Levels in Thyroid Cancer. Ann. Surg. Oncol. 2007, 14, 2616–2620. [Google Scholar] [CrossRef] [PubMed]
- Brogowska, K.K.; Zajkowska, M.; Mroczko, B. Vascular Endothelial Growth Factor Ligands and Receptors in Breast Cancer. J. Clin. Med. 2023, 12, 2412. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.J.; Nan, G.X. Oxidative Stress-Induced Angiogenesis. J. Clin. Neurosci. 2019, 63, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Suvakov, S.; Jerotic, D.; Damjanovic, T.; Milic, N.; Pekmezovic, T.; Djukic, T.; Jelic-Ivanovic, Z.; Savic Radojevic, A.; Pljesa-Ercegovac, M.; Matic, M.; et al. Markers of Oxidative Stress and Endothelial Dysfunction Predict Haemodialysis Patients Survival. Am. J. Nephrol. 2019, 50, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Chiang, F.F.; Chao, T.H.; Huang, S.C.; Cheng, C.H.; Tseng, Y.Y.; Huang, Y.C. Cysteine Regulates Oxidative Stress and Glutathione-Related Antioxidative Capacity before and after Colorectal Tumor Resection. Int. J. Mol. Sci. 2022, 23, 9581. [Google Scholar] [CrossRef] [PubMed]
- Ek, R.O.; Yildiz, Y.; Cecen, S.; Yenisey, C.; Kavak, T. Effects of Tamoxifen on Myocardial Ischemia-Reperfusion Injury Model in Ovariectomized Rats. Mol. Cell. Biochem. 2008, 308, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.B.; Romero, W.G.; Carvalho, A.L.R.D.A.; Souza, G.A.A.; Claudio, E.R.G.; Abreu, G.R. Effects of Treatment with Chemotherapy and/or Tamoxifen on the Biomarkers of Cardiac Injury and Oxidative Stress in Women with Breast Cancer. Medicine 2017, 96, e8723. [Google Scholar] [CrossRef] [PubMed]
- Baranova, A.; Krasnoselskyi, M.; Starikov, V.; Kartashov, S.; Zhulkevych, I.; Vlasenko, V.; Oleshko, K.; Bilodid, O.; Sadchikova, M.; Vinnyk, Y. Triple-Negative Breast Cancer: Current Treatment Strategies and Factors of Negative Prognosis. J. Med. Life 2022, 2022, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ma, L. Efficacy of Chemotherapy for Lymph Node-Positive Luminal A Subtype Breast Cancer Patients: An Updated Meta-Analysis. World J. Surg. Oncol. 2020, 18, 316. [Google Scholar] [CrossRef]
- Hennigs, A.; Riedel, F.; Gondos, A.; Sinn, P.; Schirmacher, P.; Marmé, F.; Jäger, D.; Kauczor, H.U.; Stieber, A.; Lindel, K.; et al. Prognosis of Breast Cancer Molecular Subtypes in Routine Clinical Care: A Large Prospective Cohort Study. BMC Cancer 2016, 16, 734. [Google Scholar] [CrossRef]
- Abdou, Y.; Gupta, M.; Asaoka, M.; Attwood, K.; Mateusz, O.; Gandhi, S.; Takabe, K. Left Sided Breast Cancer Is Associated with Aggressive Biology and Worse Outcomes than Right Sided Breast Cancer. Sci. Rep. 2022, 12, 13377. [Google Scholar] [CrossRef]
- Nelson, D.R.; Brown, J.; Morikawa, A.; Method, M. Breast Cancer-Specific Mortality in Early Breast Cancer as Defined by High-Risk Clinical and Pathologic Characteristics. PLoS ONE 2022, 17, e0264637. [Google Scholar] [CrossRef]
- Zhou, F.L.; Zhang, W.G.; Wei, Y.C.; Meng, S.; Bai, G.G.; Wang, B.Y.; Yang, H.Y.; Tian, W.; Meng, X.; Zhang, H.; et al. Involvement of Oxidative Stress in the Relapse of Acute Myeloid Leukemia. J. Biol. Chem. 2010, 285, 15010–15015. [Google Scholar] [CrossRef]
- Delrieu, L.; Touillaud, M.; Pérol, O.; Morelle, M.; Martin, A.; Friedenreich, C.M.; Mury, P.; Dufresne, A.; Bachelot, T.; Heudel, P.E.; et al. Impact of Physical Activity on Oxidative Stress Markers in Patients with Metastatic Breast Cancer. Oxid. Med. Cell. Longev. 2021, 2021, 6694594. [Google Scholar] [CrossRef]
- Ben Mahmoud, L.; Mdhaffar, M.; Ghozzi, H.; Ammar, M.; Hakim, A.; Atheymen, R.; Sahnoun, Z.; Elloumi, M.; Zeghal, K. Oxidative Stress in Tunisian Patients with Acute Lymphoblastic Leukemia and Its Involvement in Leukemic Relapse. J. Pediatr. Hematol. Oncol. 2017, 39, e124–e130. [Google Scholar] [CrossRef] [PubMed]
- Kaneda, H.; Taguchi, J.; Ogasawara, K.; Aizawa, T.; Ohno, M. Increased Level of Advanced Oxidation Protein Products in Patients with Coronary Artery Disease. Atherosclerosis 2002, 162, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Han, T.; Nie, C.; Jia, X.; Liu, Y.; Zhu, Z.; Gao, Y. Biomarkers of Oxidation Stress, Inflammation, Necrosis and Apoptosis Are Associated with Hepatitis B-Related Acute-on-Chronic Liver Failure. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Elkabany, Z.A.; El-Farrash, R.A.; Shinkar, D.M.; Ismail, E.A.; Nada, A.S.; Farag, A.S.; Elsayed, M.A.; Salama, D.H.; Macken, E.L.; Gaballah, S.A. Oxidative Stress Markers in Neonatal Respiratory Distress Syndrome: Advanced Oxidation Protein Products and 8-Hydroxy-2-Deoxyguanosine in Relation to Disease Severity. Pediatr. Res. 2020, 87, 74–80. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic and Clinical Data | Overall (n = 70) | Patients without Progression (n = 59) | Patients with Progression (n = 11) |
|---|---|---|---|
| n (%) | |||
| Age (according to median) | |||
| <54 years | 32 (45.7%) | 26 (44.1%) | 6 (54.5%) |
| ≥54 years | 38 (54.3%) | 33 (55.9%) | 5 (45.5%) |
| Menopausal status | |||
| Pre-menopausal | 25 (35.7%) | 19 (32.2%) | 6 (54.5%) |
| Post-menopausal | 45 (64.3%) | 40 (67.8%) | 5 (45.5%) |
| BMI (kg/m2) | |||
| Normal (18.5 ≤ 24.99) | 34 (48.6%) | 26 (44.1%) | 8 (72.7%) |
| Overweight (25 ≤ 29.99) | 22 (31.4%) | 21 (35.6%) | 1 (9.1%) |
| Obese (>30) | 14 (20%) | 12 (20.3%) | 2 (18.2%) |
| Parity status | |||
| 0 | 6 (8.6%) | 3 (5.1%) | 3 (27.3%) |
| 1–2 | 49 (70%) | 44 74.6%) | 5 (45.5%) |
| 3 and more | 15 (21.4%) | 12 (20.3%) | 3 (27.3%) |
| Localization of tumour | |||
| Right breast | 35 (50%) | 29 (49.2%) | 6 (54.5%) |
| Left breast | 35 (50%) | 30 (50.8%) | 5 (45.5%) |
| Diameter of the tumour | |||
| T1 < 2 cm | 45 (64.3%) | 45 (76.3%) | 0 (0%) |
| 2 cm < T2 < 5 cm | 25 (35.7%) | 14 (23.7%) | 11 (100%) |
| Lymph node status | |||
| N0 | 51 (72.9%) | 45 (76.3%) | 6 (54.5%) |
| N1 | 19 (27.1%) | 14 (23.7%) | 5 (45.5%) |
| Histological type | |||
| IDC | 59 (72.9%) | 49 (83.1%) | 10 (90.9%) |
| ILC | 11 (27.1%) | 10 (16.9%) | 1 (9.1%) |
| Grade according to Elston-Ellis | |||
| 1 + 2 | 53 (75.7%) | 45 (76.3%) | 8 (72.7%) |
| 3 | 17 (24.3%) | 14 (23.7%) | 3 (27.3%) |
| Molecular type | |||
| Luminal A (HR+/HER2−/Ki-67 < 20%) | 41 (58.6%) | 38 (64.4%) | 3 (27.3%) |
| Luminal B (HR+/HER2−/Ki-67 ≥ 20%) | 14 (20%) | 9 (15.3%) | 5 (45.5%) |
| Luminal B HER2+ (HR+ HER2+) | 7 (10%) | 6 (8.6%) | 1 (9.1%) |
| Triple negative (HR-/HER2-) | 8 (11.4%) | 6 (8.6%) | 2 (18.2%) |
| Staging | |||
| I | 31 (44.3%) | 30 (50.8%) | 1 (9.1%) |
| II | 39 (55.7%) | 29 (49.2%) | 10 (90.9%) |
| Progesterone receptor (PR) | |||
| Negative | 16 (22.9%) | 13 (22%) | 3 (27.3%) |
| Positive | 54 (77.1%) | 46 (78%) | 8 (72.7%) |
| Oestrogen receptor (ER) | |||
| Negative | 11 (27.1%) | 9 (15.3%) | 2 (18.2%) |
| Positive | 59 (72.9%) | 50 (84.7%) | 9 (81.8%) |
| E-cadherin | |||
| Negative | 5 (7.1%) | 5 (8.5%) | 0 (0%) |
| Positive | 65 (92.9%) | 54 (91.5%) | 11 (100%) |
| Ki-67 | 5 (45.5%) | ||
| <20% | 43 (61.4%) | 38 (64.6%) | 6 (54.5%) |
| ≥20% | 27 (38.6%) | 21 (35.6%) | |
| Comorbidities | |||
| Heart attack | 3 (4.3%) | 3 (5.1%) | 0 (0%) |
| Hypertension | 17 (24.3%) | 16 (27.1%) | 1 (9.1%) |
| Diabetes | 1 (1.4%) | 1 (1.7%) | 0 (0%) |
| Feature/ Number of Patients (%) | Pre-Treatment AOPP Concentration [µM] n = 70 | Post-Treatment AOPP Concentration [µM] n = 67 # | Pre-Treatment vs. Post-Treatment AOPPs n = 67 # p-Value |
|---|---|---|---|
| Surgery | p = 0.5737 | p = 0.8831 | |
| BCS + Radiotherapy n = 58/55 (82.9%/82.1%) | 8.69 (1.17) | 8.40 (2.44) | 0.3260 |
| Mastectomy n = 12/12 (17.1%/17.9%) | 8.89 (0.78) | 8.52 (2.72) | 0.6745 |
| Chemotherapy | p = 0.3471 | p = 0.0283 | |
| Anthracycline n = 25/24 (35.7%/35.8%) | 8.84 (1.07) | 8.59 (2.29) | 0.6074 |
| Non-anthracycline n = 10/9 (14.3%/13.4%) | 9.06 (0.86) | 10.24 * (1.25) | 0.0996 |
| No n = 35/34 (50%/50.7%) | 8.54 (1.19) | 7.82 (2.63) | 0.0778 |
| Endocrine therapy | p = 0.9639 | p = 0.3461 | |
| Tamoxifen n = 35/34 (50%/50.7%) | 8.70 (1.06) | 8.08 ** (2.94) | 0.1910 |
| Inhibitor aromatase n = 13/13 (18.6%/19.4%) | 8.68 (1.35) | 8.17 (2.09) | 0.2273 |
| Tamoxifen and inhibitor aromatase n = 8/8 (11.4%/11.9%) | 9.00 (1.10) | 8.36 (1.66) | 0.1577 |
| Other type n = 2/2 (2.9%/3%) | 8.54 (0.95) | 8.50 (0.45) | 0.9745 |
| No n = 12/10 (17.1%/14.9%) | 8.70 (1.16) | 9.93 (1.46) | 0.0254 |
| Brachytherapy | p = 0.6461 | p = 0.5656 | |
| Yes n = 36/36 (51.4%/53.7%) | 8.67 (1.23) | 8.58 (2.44) | 0.8275 |
| No n = 34/31 (48.6%/46.3%) | 8.79 (0.97) | 8.23 (2.53) | 0.1815 |
| Feature | Number of Patients (%) | Pre-Treatment AOPP Concentration [μM] n = 70 | Post-Treatment AOPP Concentration [μM] n = 67 # | Pre-Treatment vs. Post-Treatment AOPPs n = 67 # p-Value |
|---|---|---|---|---|
| Tumour localisation | p = 0.0056 | p = 0.5014 | ||
| Left breast | 35/33 (50%/49.3%) | 9.09 (1.09) | 8.63 (2.19) | 0.1685 |
| Right breast | 35/34 (50%/50.7%) | 8.36 (1.02) | 8.22 (2.74) | 0.7493 |
| Molecular subtypes | p < 0.0001 | p < 0.0001 | ||
| Luminal A | 41/40 (58.6%/59.7%) | 8.23 (0.79) | 7.27 *** (2.18) | 0.0102 |
| Luminal B HER2- | 14/14 (20%/20.9%) | 10.05 * (0.86) | 10.20 (2.29) | 0.7808 |
| Luminal B HER2+ and Non-Luminal HER2+ | 7/7 (10%/10.4%) | 9.24 ** (1.03) | 9.75 (0.98) | 0.4711 |
| Triple negative | 8/6 (11.4%/9%) | 8.50 (1.01) | 10.32 (1.39) | 0.0190 |
| Tumour diameter | p = 0.0288 | p = 0.0006 | ||
| T1 2 cm | 45/43 (64.3%/64.2%) | 8.51 (1.03) | 7.68 (2.06) | 0.0174 |
| 2 cm < T2 < 5 cm | 25/24 (35.7%/35.8%) | 9.11 (1.16) | 9.76 (2.61) | 0.1671 |
| Nodal status | p = 0.8878 | p = 0.5610 | ||
| N0 | 51/48 (72.9%/71.6%) | 8.74 (1.13) | 8.53 (2.33) | 0.5414 |
| N1 | 19/19 (27.1%/28.4%) | 8.69 (1.09) | 8.14 (2.84) | 0.3264 |
| Stage of disease | p = 0.1465 | p = 0.2139 | ||
| IA | 31/29 (44.3%/43.3%) | 8.51 (1.11) | 7.99 (1.91) | 0.2416 |
| IIA + IIB | 39/38 (55.7%/56.7%) | 8.90 (1.09) | 8.75 (2.80) | 0.6761 |
| Elston and Ellis grade | p = 0.2782 | p = 0.0890 | ||
| G1 + G2 | 53/51 (75.7%/76.1%) | 8.64 (1.20) | 8.13 (2.50) | 0.1016 |
| G3 | 17/16 (24.3%/23.9%) | 8.98 (0.72) | 9.34 (2.17) | 0.4938 |
| Histological type | p = 0.0115 | p = 0.1471 | ||
| IDC | 59/56 (84.3%/83.6%) | 8.87 (1.12) | 8.62 (2.45) | 0.4067 |
| ILC | 11/11 (15.7%/16.4%) | 7.96 (0.65) | 7.43 (2.46) | 0.4581 |
| Feature | Number of Patients (%) | Pre-Treatment AOPP Concentration [μM] n = 70 | Post-Treatment AOPP Concentration [μM] n = 67 # | Pre-Treatment vs. Post-Treatment AOPPs n = 67 # p-Value |
|---|---|---|---|---|
| Expression of Ki-67 | p = 0.0001 | p = 0.0041 | ||
| <20% | 43/42 (61.4%/62.7%) | 8.35 (0.89) | 7.79 (2.64) | 0.1748 |
| ≥20% | 27/25 (38.6%/37.3%) | 9.36 (1.17) | 9.56 (1.63) | 0.7258 |
| Expression of HER2 | p = 0.2022 | p = 0.1688 | ||
| Positive | 7/6 (10%/9%) | 9.24 (1.03) | 9.75 (0.98) | 0.1918 |
| Negative | 63/61 (90%/91%) | 8.67 (1.11) | 8.29 (2.54) | 0.4711 |
| Hormone receptor status | ||||
| ER+ | 59/58 (84.3%/86.6%) | p = 0.6436 8.70 (1.12) | p = 0.0200 8.15 (2.50) | 0.0617 |
| ER- | 11/9 (15.7%/13.4% | 8.87 (1.06) | 10.19 (1.29) | 0.0360 |
| PR+ | 54/53 (77.1%/79.1%) | p = 0.2128 8.64 (1.15) | p = 0.0187 8.06 (2.59) | 0.0739 |
| PR- | 16/14 (22.9%/20.9%) | 9.03 (0.91) | 9.79 (1.29) | 0.0995 |
| E-cadherin status | p = 0.0862 | p = 0.2403 | ||
| Positive | 65/62 (92.9%/92.5%) | 8.79 (1.11) | 8.52 (2.44) | 0.3643 |
| Negative | 5/5 (7.1%/7.5%) | 7.91 (0.74) | 7.17 (2.80) | 0.5055 |
| Parameter [units] | AOPP Low (<7.87 μM) n = 12 | AOPP Moderate (7.87–9.45 μM) n = 41 | AOPP High (>9.45 μM) n = 17 | p-Value |
|---|---|---|---|---|
| VEGF-A concentration [pg/mL] | 36.78 | 64.87 | 74.12 | 0.0051 |
| sVEGFR1 concentration [pg/mL] | 80.82 | 30.29 | 24.45 | 0.0685 |
| sVEGFR2 concentration [pg/mL] | 8468.45 | 9778.25 | 9182.05 | 0.8836 |
| Parameters [Concentration] | AOPP | |||
|---|---|---|---|---|
| Pre-Treatment | Post-Treatment | |||
| r | p | r | p | |
| Pre-treatment AOPPs [μM] | --- | --- | 0.4103 | 0.0006 |
| Post-treatment AOPPs [μM] | 0.4103 | 0.0006 | --- | --- |
| Pre-treatment VEGF-A [pg/mL] | 0.2415 | 0.0440 | −0.0668 | 0.5914 |
| Post-treatment VEGF-A [pg/mL] | 0.1253 | 0.3013 | 0.1574 | 0.2033 |
| Pre-treatment sVEGFR1 [pg/mL] | −0.1061 | 0.3822 | −0.2317 | 0.0592 |
| Post-treatment sVEGFR1 [pg/mL] | −0.0498 | 0.6822 | −0.1085 | 0.3821 |
| Pre-treatment sVEGFR2 [pg/mL] | −0.0369 | 0.7615 | 0.0128 | 0.9184 |
| Post-treatment sVEGFR2 [pg/mL] | −0.1770 | 0.1426 | −0.3330 | 0.0059 |
| ROC Data | Pre-Treatment AOPP Concentration | Pre-Treatment VEGF-A Concentration | Pre-Treatment sVEGFR1 Concentration | Pre-Treatment sVEGFR2 Concentration |
|---|---|---|---|---|
| AUC | 0.773 | 0.597 | 0.606 | 0.532 |
| Youden index | 0.51 | 0.28 | 0.35 | 0.18 |
| Cut-off point | 9.37 | 74.12 | 37.81 | 4626.99 |
| Sensitivity (%) | 78 | 81.8 | 90.9 | 18.2 |
| Specificity (%) | 72.7 | 45.8 | 44.1 | 100.0 |
| Positive predictive Value (%) | 38.1 | 22.0 | 23.3 | 100.0 |
| Negative predictive Value (%) | 93.9 | 93.1 | 96.3 | 86.8 |
| Accuracy (%) | 77.1 | 51.4 | 51.4 | 87.1 |
| p-Value | 0.0005 | 0.3453 | 0.1945 | 0.7555 |
| ROC Data | Post-Treatment AOPP Concentration | Post-Treatment VEGF-A Concentration | Post-Treatment sVEGFR1 Concentration | Post-Treatment sVEGFR2 Concentration |
|---|---|---|---|---|
| AUC | 0.86 | 0.532 | 0.578 | 0.596 |
| Youden index | 0.71 | 0.24 | 0.34 | 0.25 |
| Cut-off point | 10.39 | 39.92 | 386.5 | 7230.0 |
| Sensitivity (%) | 81.8 | 36.4 | 100.0 | 63.6 |
| Specificity (%) | 89.3 | 88.1 | 33.9 | 61.0 |
| Positive predictive Value (%) | 60.0 | 36.4 | 22.0 | 23.3 |
| Negative predictive Value (%) | 96.2 | 88.1 | 100.0 | 90.0 |
| Accuracy (%) | 88.1 | 80.0 | 44.3 | 61.4 |
| p-Value | <0.0001 | 0.7817 | 0.3178 | 0.2455 |
| Pre-Treatment AOPP Concentration (μM) | Post-Treatment AOPP Concentration (μM) | |
|---|---|---|
| Medians | 8.74 | 8.50 |
| ROC cut-off points | 9.37 | 10.39 |
| Univariate | ||||||
|---|---|---|---|---|---|---|
| DFS | OS | |||||
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Pre-treatment AOPP concentration | ||||||
| Low vs. High | 0.19 | (0.04–0.89) | 0.0346 | 0.25 | (0.05–1.21) | 0.0847 |
| Post-treatment AOPP concentration | ||||||
| Low vs. High | 0.08 | (0.01–0.66) | 0.0185 | 0.11 | (0.01–0.86) | 0.0358 |
| Pre-treatment VEGF-A concentration | ||||||
| Low vs. High | 1.89 | (0.55–6.46) | 0.3101 | 3.85 | (0.80–18.56) | 0.0924 |
| Post-treatment VEGF-A concentration | ||||||
| Low vs. High | 1.21 | (0.37–3.96) | 0.7552 | 1.28 | (0.34–4.78) | 0.7122 |
| Pre-treatment sVEGFR1 concentration | ||||||
| Low vs. High | 1.89 | (0.55–6.46) | 0.3102 | 3.86 | (0.80–18.60) | 0.0921 |
| Post-treatment sVEGFR1 concentration | ||||||
| Low vs. High | 1.26 | (0.38–4.13) | 0.7015 | 0.83 | (0.22–3.11) | 0.7873 |
| Pre-treatment sVEGFR2 concentration | ||||||
| Low vs. High | 0.85 | (0.26–2.79) | 0.7905 | 1.29 | (0.35–4.80) | 0.7057 |
| Post-treatment sVEGFR2 concentration | ||||||
| Low vs. High | 1.87 | (0.55–6.39) | 0.3181 | 3.76 | (0.78–18.09) | 0.0988 |
| Multivariate | ||||||
|---|---|---|---|---|---|---|
| DFS | OS | |||||
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Pre-treatment AOPP concentration | ||||||
| Low vs. High | 0.16 | (0.03–0.82) | 0.028 | 0.2 | (0.04–1.10) | 0.065 |
| Post-treatment AOPP concentration | ||||||
| Low vs. High | 0.08 | (0.01–0.66) | 0.019 | 0.09 | (0.01–0.81) | 0.031 |
| Pre-treatment VEGF-A concentration | ||||||
| Low vs. High | 1.45 | (0.39–5.31) | 0.578 | 2.81 | (0.54–14.70) | 0.22 |
| Post-treatment VEGF-A concentration | ||||||
| Low vs. High | 0.48 | (0.07–3.26) | 0.45 | 0.63 | (0.07–5.37) | 0.67 |
| Pre-treatment sVEGFR1 concentration | ||||||
| Low vs. High | 1.51 | (0.41–5.59) | 0.537 | 2.89 | (0.56–15.04) | 0.207 |
| Post-treatment sVEGFR1 concentration | ||||||
| Low vs. High | 0.91 | (0.25–3.38) | 0.893 | 0.66 | (0.16–2.77) | 0.568 |
| Pre-treatment sVEGFR2 concentration | ||||||
| Low vs. High | 0.38 | (0.08–1.90) | 0.239 | 0.6 | (0.11–3.42) | 0.568 |
| Post-treatment sVEGFR2 concentration | ||||||
| Low vs. High | 2.74 | (0.73–10.18) | 0.133 | 7.35 | (1.16–46.77) | 0.035 |
| Model 1 | Model 2 | Model 3 | Model 4 | ||
|---|---|---|---|---|---|
| Pre-treatment AOPP concentration | Beta p-value | 0.3695 0.0018 | 0.4041 0.0007 | 0.4912 <0.0001 | 0.3663 0.0196 |
| Post-treatment AOPP concentration | Beta p-value | 0.4737 <0.0001 | 0.4880 <0.0001 | 0.5805 <0.0001 | 0.4490 0.0015 |
| Pre-treatment VEGF-A concentration | Beta p-value | 0.0482 0.7090 | 0.0934 0.4809 | 0.0990 0.4640 | 0.1416 0.2820 |
| Post-treatment VEGF-A concentration | Beta p-value | −0.0002 0.9986 | 0.0498 0.7076 | 0.0563 0.6744 | 0.0422 0.7304 |
| Pre-treatment sVEGFR1 concentration | Beta p-value | −0.2009 0.1029 | −0.2184 0.0774 | −0.2862 0.0198 | −0.2234 0.0593 |
| Post-treatment sVEGFR1 concentration | Beta p-value | −0.1003 0.4106 | −0.1328 0.2872 | −0.1839 0.1413 | −0.1222 0.3127 |
| Pre-treatment sVEGFR2 concentration | Beta p-value | 0.0267 0.8426 | 0.0037 0.9783 | 0.0547 0.6890 | 0.1032 0.4371 |
| Post-treatment sVEGFR2 concentration | Beta p-value | −0.0978 0.4269 | −0.1279 0.3059 | −0.1177 0.3465 | −0.0570 0.6405 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Napiórkowska-Mastalerz, M.; Wybranowski, T.; Bosek, M.; Kruszewski, S.; Rhone, P.; Ruszkowska-Ciastek, B. A Preliminary Evaluation of Advanced Oxidation Protein Products (AOPPs) as a Potential Approach to Evaluating Prognosis in Early-Stage Breast Cancer Patients and Its Implication in Tumour Angiogenesis: A 7-Year Single-Centre Study. Cancers 2024, 16, 1068. https://doi.org/10.3390/cancers16051068
Napiórkowska-Mastalerz M, Wybranowski T, Bosek M, Kruszewski S, Rhone P, Ruszkowska-Ciastek B. A Preliminary Evaluation of Advanced Oxidation Protein Products (AOPPs) as a Potential Approach to Evaluating Prognosis in Early-Stage Breast Cancer Patients and Its Implication in Tumour Angiogenesis: A 7-Year Single-Centre Study. Cancers. 2024; 16(5):1068. https://doi.org/10.3390/cancers16051068
Chicago/Turabian StyleNapiórkowska-Mastalerz, Marta, Tomasz Wybranowski, Maciej Bosek, Stefan Kruszewski, Piotr Rhone, and Barbara Ruszkowska-Ciastek. 2024. "A Preliminary Evaluation of Advanced Oxidation Protein Products (AOPPs) as a Potential Approach to Evaluating Prognosis in Early-Stage Breast Cancer Patients and Its Implication in Tumour Angiogenesis: A 7-Year Single-Centre Study" Cancers 16, no. 5: 1068. https://doi.org/10.3390/cancers16051068
APA StyleNapiórkowska-Mastalerz, M., Wybranowski, T., Bosek, M., Kruszewski, S., Rhone, P., & Ruszkowska-Ciastek, B. (2024). A Preliminary Evaluation of Advanced Oxidation Protein Products (AOPPs) as a Potential Approach to Evaluating Prognosis in Early-Stage Breast Cancer Patients and Its Implication in Tumour Angiogenesis: A 7-Year Single-Centre Study. Cancers, 16(5), 1068. https://doi.org/10.3390/cancers16051068