
Impact of Primary Tumor Location on Demographics, Resectability, Outcomes, and Quality of Life in Finnish Metastatic Colorectal Cancer Patients (Subgroup Analysis of the RAXO Study)

 , , , , , ,
, , , , , ,  , , and add
Show full author list
, , and add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Demographics
3.2. Resectability, Resections, and LAT
3.3. Treatments
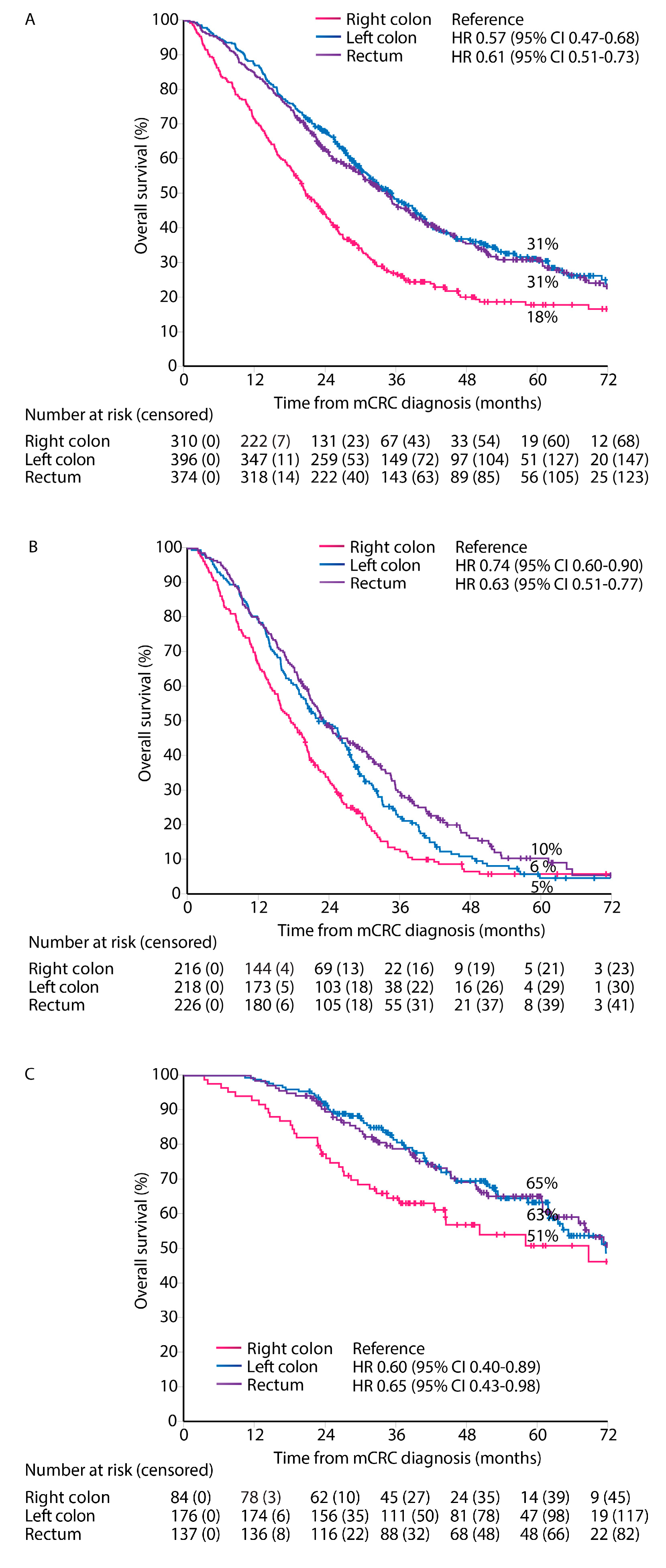
3.4. Overall Survival and Progression-Free Survival
3.5. Multivariable Model for OS
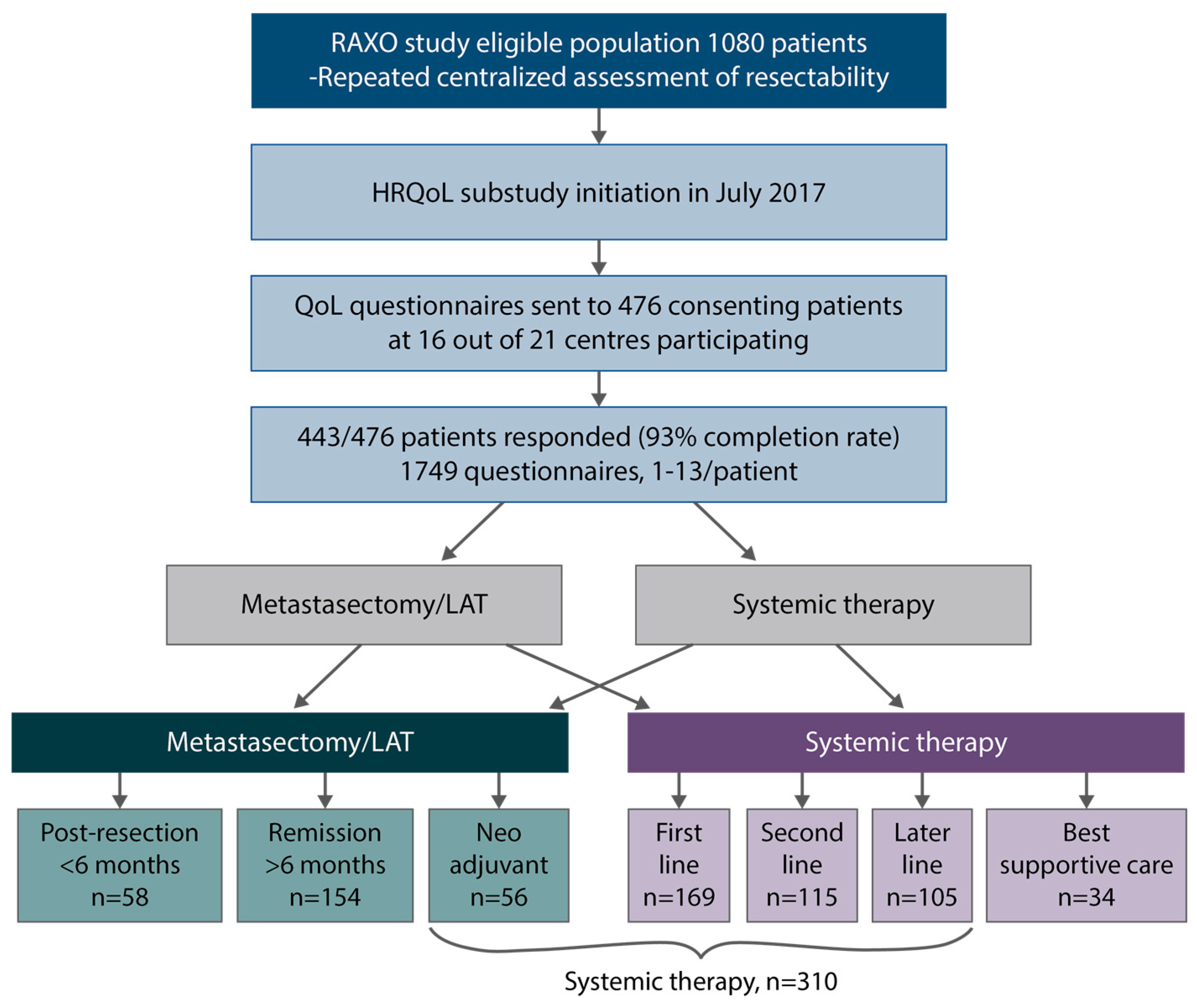
3.6. HRQoL and PTL in Different Treatment Phases
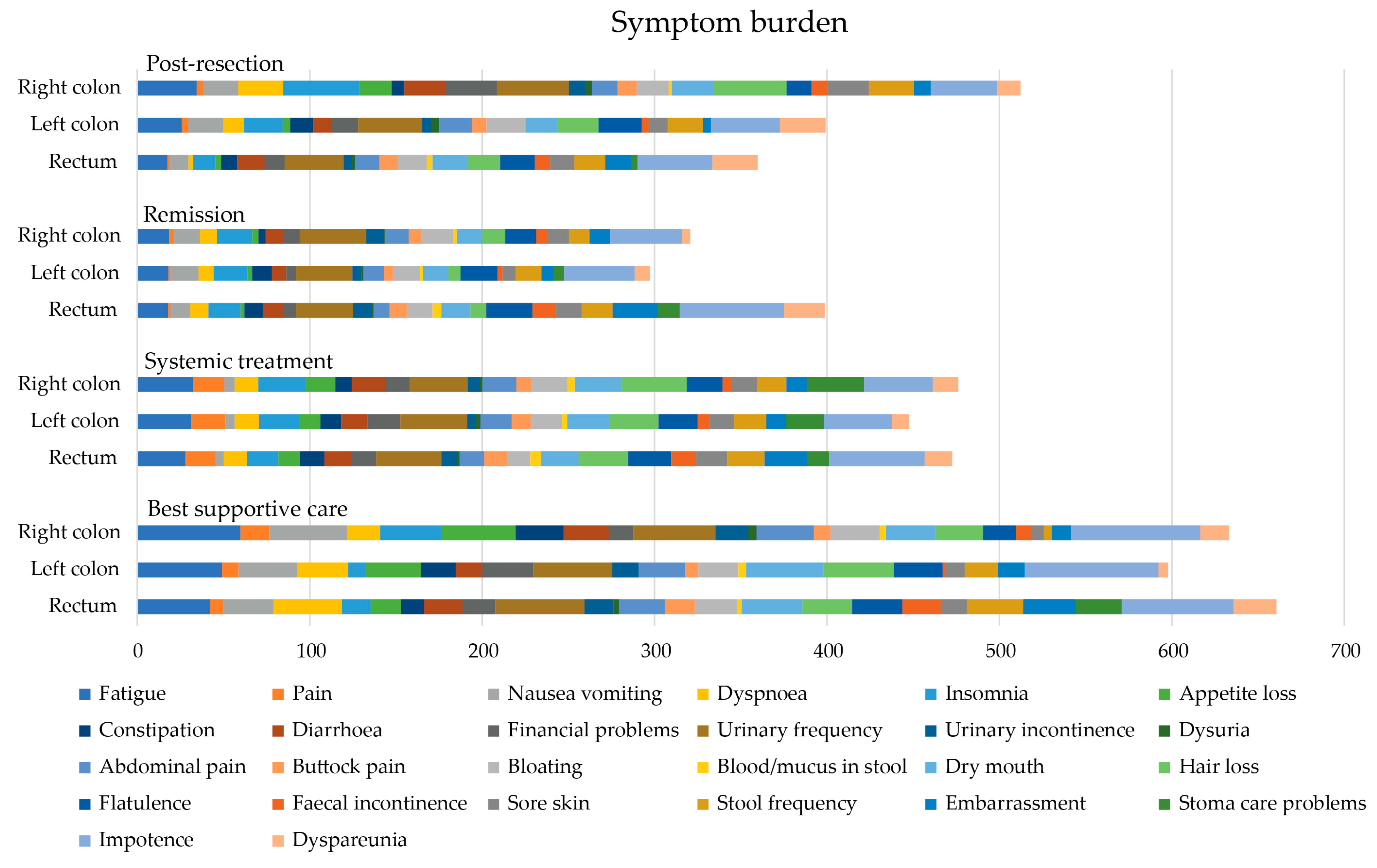
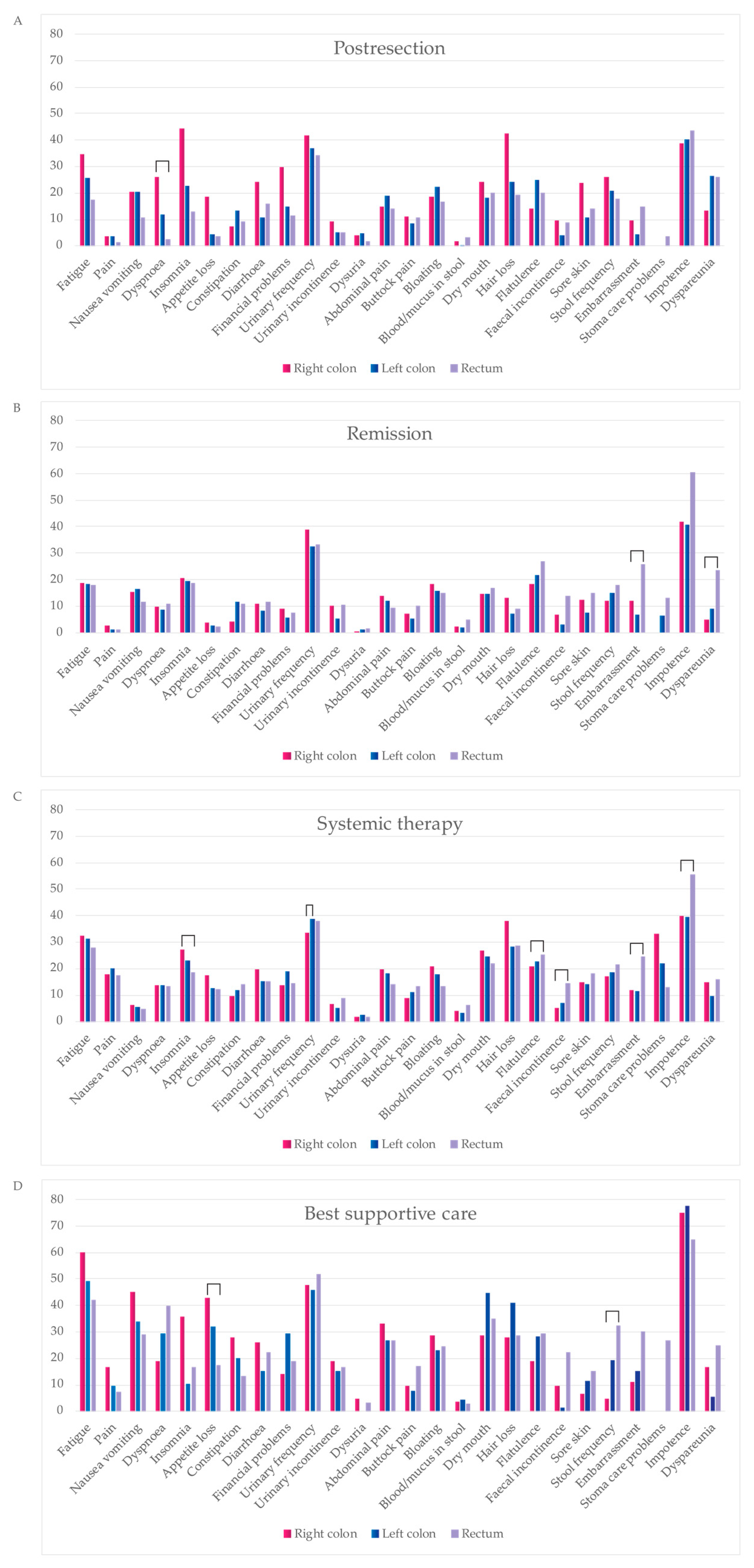
3.7. QLQ-C30 and QLQ-CR29 Symptom Scales
4. Discussion
4.1. Resectability and Resections
4.2. Survival, Prognosis, and Predictive Factors
4.3. Health-Related Quality of Life
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iacopetta, B. Are There Two Sides to Colorectal Cancer? Int. J. Cancer 2002, 101, 403–408. [Google Scholar] [CrossRef]
- Arnold, D.; Lueza, B.; Douillard, J.Y.; Peeters, M.; Lenz, H.J.; Venook, A.; Heinemann, V.; Van Cutsem, E.; Pignon, J.P.; Tabernero, J.; et al. Prognostic and Predictive Value of Primary Tumour Side in Patients with RAS Wild-Type Metastatic Colorectal Cancer Treated with Chemotherapy and EGFR Directed Antibodies in Six Randomized Trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef] [PubMed]
- Venook, A.P.; Niedzwiecki, D.; Innocenti, F.; Fruth, B.; Greene, C.; O’Neil, B.H.; Shaw, J.E.; Atkins, J.N.; Horvath, L.E.; Polite, B.N.; et al. Impact of Primary (1°) Tumor Location on Overall Survival (OS) and Progression-Free Survival (PFS) in Patients (Pts) with Metastatic Colorectal Cancer (MCRC): Analysis of CALGB/SWOG 80405 (Alliance). J. Clin. Oncol. 2016, 34, 3504. [Google Scholar] [CrossRef]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef]
- Flemer, B.; Lynch, D.B.; Brown, J.M.R.; Jeffery, I.B.; Ryan, F.J.; Claesson, M.J.; O’Riordain, M.; Shanahan, F.; O’Toole, P.W. Tumour-Associated and Non-Tumour-Associated Microbiota in Colorectal Cancer. Gut 2017, 66, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Dienstmann, R.; Vermeulen, L.; Guinney, J.; Kopetz, S.; Tejpar, S.; Tabernero, J. Consensus Molecular Subtypes and the Evolution of Precision Medicine in Colorectal Cancer. Nat. Rev. Cancer 2017, 17, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.; Kopetz, S.; Tie, J.; Gibbs, P.; Jiang, Z.-Q.; Lieu, C.H.; Agarwal, A.; Maru, D.M.; Sieber, O.; Desai, J. Impact of BRAF Mutation and Microsatellite Instability on the Pattern of Metastatic Spread and Prognosis in Metastatic Colorectal Cancer. Cancer 2011, 117, 4623–4632. [Google Scholar] [CrossRef] [PubMed]
- Yaeger, R.; Chatila, W.K.; Lipsyc, M.D.; Hechtman, J.F.; Cercek, A.; Sanchez-Vega, F.; Jayakumaran, G.; Middha, S.; Zehir, A.; Donoghue, M.T.A.; et al. Clinical Sequencing Defines the Genomic Landscape of Metastatic Colorectal Cancer. Cancer Cell 2018, 33, 125–136.e3. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, N.P.M.; Van Der Kruijssen, D.E.W.; Hugen, N.; De Hingh, I.H.J.T.; Nagtegaal, I.D.; Verhoeven, R.H.A.; Koopman, M.; De Wilt, J.H.W. The Impact of Primary Tumor Location in Synchronous Metastatic Colorectal Cancer: Differences in Metastatic Sites and Survival. Ann. Surg. Oncol. 2019, 27, 1580–1588. [Google Scholar] [CrossRef]
- Tejpar, S.; Stintzing, S.; Ciardiello, F.; Tabernero, J.; Van Cutsem, E.; Beier, F.; Esser, R.; Lenz, H.J.; Heinemann, V. Prognostic and Predictive Relevance of Primary Tumor Location in Patients with Ras Wild-Type Metastatic Colorectal Cancer Retrospective Analyses of the CRYSTAL and FIRE-3 Trials. JAMA Oncol. 2017, 3, 194–201. [Google Scholar] [CrossRef]
- Loupakis, F.; Yang, D.; Yau, L.; Feng, S.; Cremolini, C.; Zhang, W.; Maus, M.K.H.; Antoniotti, C.; Langer, C.; Scherer, S.J.; et al. Primary Tumor Location as a Prognostic Factor in Metastatic Colorectal Cancer. JNCI J. Natl. Cancer Inst. 2015, 107, 427. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, T.; Taieb, J.; Kuboki, Y.; Pfeiffer, P.; Kumar, A.; Hochster, H.S. Trifluridine/Tipiracil with or without Bevacizumab in Metastatic Colorectal Cancer: Results of a Systematic Review and Meta-Analysis. Ther. Adv. Med. Oncol. 2023, 15, 17588359221146137. [Google Scholar] [CrossRef] [PubMed]
- Boeckx, N.; Koukakis, R.; Op De Beeck, K.; Rolfo, C.; Van Camp, G.; Siena, S.; Tabernero, J.; Douillard, J.-Y.; André, T.; Peeters, M. Primary Tumor Sidedness Has an Impact on Prognosis and Treatment Outcome in Metastatic Colorectal Cancer: Results from Two Randomized First-Line Panitumumab Studies. Ann. Oncol. 2017, 28, 1862–1868. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, C.; Amodio, P.M.; Chilelli, M.G.; Santoro, R.; Schirripa, M.; Ranalli, T.V.; Pessina, G.; Giron Berrios, J.R.; Natoni, F.; Virtuoso, A.; et al. Real-Life Experience of the Prognostic Significance of the Primary Tumor Location on the Timing of Colorectal Liver Metastases: A Retrospective Analysis. Cureus 2022, 14, e30607. [Google Scholar] [CrossRef] [PubMed]
- Gasser, E.; Braunwarth, E.; Riedmann, M.; Cardini, B.; Fadinger, N.; Presl, J.; Klieser, E.; Ellmerer, P.; Dupré, A.; Imai, K.; et al. Primary Tumour Location Affects Survival after Resection of Colorectal Liver Metastases: A Two-Institutional Cohort Study with International Validation, Systematic Meta-Analysis and a Clinical Risk Score. PLoS ONE 2019, 14, e0217411. [Google Scholar] [CrossRef]
- Loupakis, F.; Hurwitz, H.I.; Saltz, L.; Arnold, D.; Grothey, A.; Nguyen, Q.L.; Osborne, S.; Talbot, J.; Srock, S.; Lenz, H.J. Impact of Primary Tumour Location on Efficacy of Bevacizumab plus Chemotherapy in Metastatic Colorectal Cancer. Br. J. Cancer 2018, 119, 1451–1455. [Google Scholar] [CrossRef]
- Lapinsky, E.; Man, L.C.; MacKenzie, A.R. Health-Related Quality of Life in Older Adults with Colorectal Cancer. Curr. Oncol. Rep. 2019, 21, 81. [Google Scholar] [CrossRef]
- Wedding, U.; Ködding, D.; Pientka, L.; Steinmetz, H.T.; Schmitz, S. Physicians’ Judgement and Comprehensive Geriatric Assessment (CGA) Select Different Patients as Fit for Chemotherapy. Crit. Rev. Oncol. Hematol. 2007, 64, 1–9. [Google Scholar] [CrossRef]
- Bonnetain, F.; Borg, C.; Adams, R.R.; Ajani, J.A.; Benson, A.; Bleiberg, H.; Chibaudel, B.; Diaz-Rubio, E.; Douillard, J.Y.; Fuchs, C.S.; et al. How Health-Related Quality of Life Assessment Should Be Used in Advanced Colorectal Cancer Clinical Trials. Ann. Oncol. 2017, 28, 2077–2085. [Google Scholar] [CrossRef]
- Hamers, P.A.H.; Vink, G.R.; Elferink, M.A.G.; Stellato, R.K.; Dijksterhuis, W.P.M.; Punt, C.J.A.; Koopman, M.; May, A.M.; Beerepoot, L.V.; Creemers, G.-J.; et al. Quality of Life and Survival of Metastatic Colorectal Cancer Patients Treated with Trifluridine-Tipiracil (QUALITAS). Clin. Color. Cancer 2022, 21, 154–166. [Google Scholar] [CrossRef]
- Lehtomäki, K.; Stedt, H.P.; Osterlund, E.; Muhonen, T.; Soveri, L.-M.; Halonen, P.; Salminen, T.K.; Kononen, J.; Kallio, R.; Ålgars, A.; et al. Health-Related Quality of Life in Metastatic Colorectal Cancer Patients Treated with Curative Resection and/or Local Ablative Therapy or Systemic Therapy in the Finnish RAXO-Study. Cancers 2022, 14, 1713. [Google Scholar] [CrossRef]
- Lehtomäki, K.; Soveri, L.M.; Osterlund, E.; Lamminmäki, A.; Uutela, A.; Heervä, E.; Halonen, P.; Stedt, H.; Aho, S.; Muhonen, T.; et al. Resectability, Resections, Survival Outcomes, and Quality of Life in Older Adult Patients with Metastatic Colorectal Cancer (the RAXO-Study). J. Clin. Med. 2023, 12, 3541. [Google Scholar] [CrossRef] [PubMed]
- Wei, A.C.; Coburn, N.G.; Devitt, K.S.; Serrano, P.E.; Moulton, C.-A.; Cleary, S.P.; Law, C.; Moore, M.J.; Gallinger, S. Survival Following Resection of Intra- and Extra-Hepatic Metastases from Colorectal Cancer: A Phase II Trial. Ann. Surg. Oncol. 2016, 23, 2644–2651. [Google Scholar] [CrossRef] [PubMed]
- Wiering, B.; Oyen, W.J.G.; Adang, E.M.M.; van der Sijp, J.R.M.; Roumen, R.M.; de Jong, K.P.; Ruers, T.J.M.; Krabbe, P.F.M. Long-Term Global Quality of Life in Patients Treated for Colorectal Liver Metastases. Br. J. Surg. 2011, 98, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Langenhoff, B.S.; Krabbe, P.F.M.; Peerenboom, L.; Wobbes, T.; Ruers, T.J.M. Quality of Life after Surgical Treatment of Colorectal Liver Metastases. Br. J. Surg. 2006, 93, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Studer, P.; Horn, T.; Haynes, A.; Candinas, D.; Banz, V.M. Quality of Life after Hepatic Resection. Br. J. Surg. 2018, 105, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Cashin, P.; Mahteme, H.; Syk, I.; Frödin, J.; Glimelius, B.; Graf, W. Quality of Life and Cost Effectiveness in a Randomized Trial of Patients with Colorectal Cancer and Peritoneal Metastases. Eur. J. Surg. Oncol. 2018, 44, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Osterlund, P.; Salminen, T.; Soveri, L.M.; Kallio, R.; Kellokumpu, I.; Lamminmäki, A.; Halonen, P.; Ristamäki, R.; Lantto, E.; Uutela, A.; et al. Repeated Centralized Multidisciplinary Team Assessment of Resectability, Clinical Behavior, and Outcomes in 1086 Finnish Metastatic Colorectal Cancer Patients (RAXO): A Nationwide Prospective Intervention Study. Lancet Reg. Health Eur. 2021, 3, 100049. [Google Scholar] [CrossRef] [PubMed]
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; Van de Velde, C.J.; Balmana, J.; Regula, J.; et al. ESMO Consensus Guidelines for Management of Patients with Colon and Rectal Cancer. A Personalized Approach to Clinical Decision Making. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO Consensus Guidelines for the Management of Patients with Metastatic Colorectal Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Azad, N.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Garrido-Laguna, I.; et al. Rectal Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 1139–1167. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef] [PubMed]
- Osterlund, E.; Ristimäki, A.; Kytölä, S.; Kuopio, T.; Heervä, E.; Muhonen, T.; Halonen, P.; Kallio, R.; Soveri, L.M.; Sundström, J.; et al. KRAS-G12C Mutation in One Real-Life and Three Population-Based Nordic Cohorts of Metastatic Colorectal Cancer. Front. Oncol. 2022, 12, 826073. [Google Scholar] [CrossRef] [PubMed]
- Sintonen, H. The 15D Instrument of Health-Related Quality of Life: Properties and Applications. In Proceedings of the Annals of Medicine; Royal Society of Medicine Press Ltd.: London, UK, 2001; Volume 33, pp. 328–336. [Google Scholar]
- Brooks, R. EuroQol: The Current State of Play. Health Policy N. Y. 1996, 37, 53–72. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Gujral, S.; Conroy, T.; Fleissner, C.; Sezer, O.; King, P.M.; Avery, K.N.L.; Sylvester, P.; Koller, M.; Sprangers, M.A.G.; Blazeby, J.M. Assessing Quality of Life in Patients with Colorectal Cancer: An Update of the EORTC Quality of Life Questionnaire. Eur. J. Cancer 2007, 43, 1564–1573. [Google Scholar] [CrossRef] [PubMed]
- Punt, C.J.A.; Bond, M.J.G.; Bolhuis, K.; Loosveld, O.J.L.; de Groot, J.W.; Droogendijk, H.; Helgason, H.H.; Hendriks, M.P.; Klaase, J.M.; Kazemier, G.; et al. LBA27 First-Line Systemic Treatment in Patients with Initially Unresectable Colorectal Cancer Liver Metastases (CRLM): Overall Survival of the Phase III CAIRO5 Study of the Dutch Colorectal Cancer Group. Ann. Oncol. 2023, 34, S1268. [Google Scholar] [CrossRef]
- Engstrand, J.; Nilsson, H.; Strömberg, C.; Jonas, E.; Freedman, J. Colorectal Cancer Liver Metastases—A Population-Based Study on Incidence, Management and Survival. BMC Cancer 2018, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Sorbye, H.; Dragomir, A.; Sundström, M.; Pfeiffer, P.; Thunberg, U.; Bergfors, M.; Aasebø, K.; Eide, G.E.; Ponten, F.; Qvortrup, C.; et al. High BRAF Mutation Frequency and Marked Survival Differences in Subgroups According to KRAS/BRAF Mutation Status and Tumor Tissue Availability in a Prospective Population-Based Metastatic Colorectal Cancer Cohort. PLoS ONE 2015, 10, e0131046. [Google Scholar] [CrossRef]
- Nunes, L.; Aasebø, K.; Mathot, L.; Ljungström, V.; Edqvist, P.H.; Sundström, M.; Dragomir, A.; Pfeiffer, P.; Ameur, A.; Ponten, F.; et al. Molecular Characterization of a Large Unselected Cohort of Metastatic Colorectal Cancers in Relation to Primary Tumor Location, Rare Metastatic Sites and Prognosis. Acta Oncol. 2020, 59, 417–426. [Google Scholar] [CrossRef]
- Riihimäki, M.; Hemminki, A.; Sundquist, J.; Hemminki, K. Patterns of Metastasis in Colon and Rectal Cancer OPEN. Nat. Publ. Gr. 2016, 6, 29765. [Google Scholar] [CrossRef]
- Uutela, A.; Osterlund, E.; Halonen, P.; Kallio, R.; Ålgars, A.; Salminen, T.; Lamminmäki, A.; Soveri, L.M.; Ristamäki, R.; Lehtomäki, K.; et al. Resectability, Conversion, Metastasectomy and Outcome According to RAS and BRAF Status for Metastatic Colorectal Cancer in the Prospective RAXO Study. Br. J. Cancer 2022, 127, 686. [Google Scholar] [CrossRef] [PubMed]
- Uutela, A.; Nordin, A.; Osterlund, E.; Halonen, P.; Kallio, R.; Soveri, L.M.; Salminen, T.; Ålgars, A.; Ristimäki, A.; Ovissi, A.; et al. Resectability and Resection Rates of Colorectal Liver Metastases According to RAS and BRAF Mutational Status: Prospective Study. Br. J. Surg. 2023, 110, 931. [Google Scholar] [CrossRef] [PubMed]
- Benedix, F.; Kube, R.; Meyer, F.; Schmidt, U.; Gastinger, I.; Lippert, H. Comparison of 17,641 Patients with Right- and Left-Sided Colon Cancer: Differences in Epidemiology, Perioperative Course, Histology, and Survival. Dis. Colon Rectum 2010, 53, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Tomasello, G.; Borgonovo, K.; Ghidini, M.; Turati, L.; Dallera, P.; Passalacqua, R.; Sgroi, G.; Barni, S. Prognostic Survival Associated with Left-Sided vs Right-Sided Colon Cancer: A Systematic Review and Meta-Analysis. JAMA Oncol. 2017, 3, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.M.; MacKinlay, A.; Semira, C.; Schieber, C.; Jimeno Yepes, A.J.; Lee, B.; Wong, R.; Hettiarachchige, C.K.H.; Gunn, N.; Tie, J.; et al. Stage-Based Variation in the Effect of Primary Tumor Side on All Stages of Colorectal Cancer Recurrence and Survival. Clin. Color. Cancer 2018, 17, e569–e577. [Google Scholar] [CrossRef] [PubMed]
- Hamfjord, J.; Myklebust, T.Å.; Larsen, I.K.; Kure, E.H.; Glimelius, B.; Guren, T.K.; Tveit, K.M.; Guren, M.G. Survival Trends of Right- and Left-Sided Colon Cancer across Four Decades: A Norwegian Population-Based Study. Cancer Epidemiol. Biomark. Prev. 2022, 31, 342. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, K.; Muro, K.; Watanabe, J.; Shitara, K.; Ohori, H.; Shiozawa, M.; Yasui, H.; Oki, E.; Sato, T.; Naito, T.; et al. Efficacy of Panitumumab in Patients with Left-Sided Disease, MSS/MSI-L, and RAS/BRAF WT: A Biomarker Study of the Phase III PARADIGM Trial. J. Clin. Oncol. 2023, 41, 3508. [Google Scholar] [CrossRef]
- Watanabe, J.; Muro, K.; Shitara, K.; Yamazaki, K.; Shiozawa, M.; Ohori, H.; Takashima, A.; Yokota, M.; Makiyama, A.; Akazawa, N.; et al. Panitumumab vs Bevacizumab Added to Standard First-Line Chemotherapy and Overall Survival Among Patients with RAS Wild-Type, Left-Sided Metastatic Colorectal Cancer: A Randomized Clinical Trial. JAMA 2023, 329, 1271–1282. [Google Scholar] [CrossRef]
- Lee, K.-H.; Chen, W.-S.; Jiang, J.-K.; Yang, S.-H.; Wang, H.-S.; Chang, S.-C.; Lan, Y.-T.; Lin, C.-C.; Lin, H.-H.; Huang, S.-C.; et al. The Efficacy of Anti-EGFR Therapy in Treating Metastatic Colorectal Cancer Differs between the Middle/Low Rectum and the Left-Sided Colon. Br. J. Cancer 2021, 125, 816–825. [Google Scholar] [CrossRef]
- Kodama, H.; Masuishi, T.; Wakabayashi, M.; Nakata, A.; Kumanishi, R.; Nakazawa, T.; Ogata, T.; Matsubara, Y.; Honda, K.; Narita, Y.; et al. Differential Efficacy of Targeted Monoclonal Antibodies in Left-Sided Colon and Rectal Metastatic Cancers. Clin. Color. Cancer 2023, 22, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Schuurhuizen, C.S.E.W.; Braamse, A.M.J.; Konings, I.R.H.M.; Sprangers, M.A.G.; Ket, J.C.F.; Dekker, J.; Verheul, H.M.W. Does Severe Toxicity Affect Global Quality of Life in Patients with Metastatic Colorectal Cancer during Palliative Systemic Treatment? A Systematic Review. Ann. Oncol. 2017, 28, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Bakkerus, L.; Buffart, L.M.; Buffart, T.E.; Meyer, Y.M.; Zonderhuis, B.M.; Haasbeek, C.J.A.; Versteeg, K.S.; Loosveld, O.J.L.; de Groot, J.W.B.; Hendriks, M.P.; et al. Health-Related Quality of Life in Patients with Metastatic Colorectal Cancer Undergoing Systemic Therapy with or Without Maximal Tumor Debulking. J. Natl. Compr. Cancer Netw. 2023, 21, 1059–1066.e5. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Mehnert, A.; Dégi, C.; Reissmann, D.R.; Schotte, D.; Schulte, T. The Relationship between Global and Specific Components of Quality of Life, Assessed with the EORTC QLQ-C30 in a Sample of 2019 Cancer Patients. Eur. J. Cancer Care 2017, 26, e12416. [Google Scholar] [CrossRef]
- Savikko, J.; Vikatmaa, L.; Hiltunen, A.M.; Mallat, N.; Tukiainen, E.; Salonen, S.M.; Nordin, A. Enhanced Recovery Protocol in Laparoscopic Liver Surgery. Surg. Endosc. 2021, 35, 1058. [Google Scholar] [CrossRef]
- Savikko, J.; Ilmakunnas, M.; Mäkisalo, H.; Nordin, A.; Isoniemi, H. Enhanced Recovery Protocol after Liver Resection. Br. J. Surg. 2015, 102, 1526–1532. [Google Scholar] [CrossRef]
- Bai, J.; Yang, M.; Liu, Z.; Efetov, S.; Kayaalp, C.; Dulskas, A.; Shaw, D.; Wang, X. Primary Tumor Resection in Colorectal Cancer Patients with Unresectable Distant Metastases: A Minireview. Front. Oncol. 2023, 13, 1138407. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shitara, K.; Mizusawa, J.; Hamaguchi, T.; Shida, D.; Komori, K.; Ikeda, S.; Ojima, H.; Ike, H.; Shiomi, A.; et al. Primary Tumor Resection Plus Chemotherapy Versus Chemotherapy Alone for Colorectal Cancer Patients with Asymptomatic, Synchronous Unresectable Metastases (JCOG1007, IPACS): A Randomized Clinical Trial. J. Clin. Oncol. 2021, 39, 1098. [Google Scholar] [CrossRef]
- Świątkowski, F.; Górnicki, T.; Bułdyś, K.; Chabowski, M. The Quality of Life of Patients with Surgically Treated Colorectal Cancer: A Narrative Review. J. Clin. Med. 2022, 11, 6211. [Google Scholar] [CrossRef]
- Ratjen, I.; Schafmayer, C.; Enderle, J.; di Giuseppe, R.; Waniek, S.; Koch, M.; Burmeister, G.; Nöthlings, U.; Hampe, J.; Schlesinger, S.; et al. Health-Related Quality of Life in Long-Term Survivors of Colorectal Cancer and Its Association with All-Cause Mortality: A German Cohort Study. BMC Cancer 2018, 18, 1156. [Google Scholar] [CrossRef]
- Qaderi, S.M.; van der Heijden, J.A.G.; Verhoeven, R.H.A.; de Wilt, J.H.W.; Custers, J.A.E.; Beets, G.L.; Belt, E.J.T.; Berbée, M.; Beverdam, F.H.; Blankenburgh, R.; et al. Trajectories of Health-Related Quality of Life and Psychological Distress in Patients with Colorectal Cancer: A Population-Based Study. Eur. J. Cancer 2021, 158, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Valeikaite-Tauginiene, G.; Kraujelyte, A.; Poskus, E.; Jotautas, V.; Saladzinskas, Z.; Tamelis, A.; Lizdenis, P.; Dulskas, A.; Samalavicius, N.E.; Strupas, K.; et al. Predictors of Quality of Life Six Years after Curative Colorectal Cancer Surgery: Results of the Prospective Multicenter Study. Medicina 2022, 58, 482. [Google Scholar] [CrossRef] [PubMed]
- Schover, L.R.; van der Kaaij, M.; van Dorst, E.; Creutzberg, C.; Huyghe, E.; Kiserud, C.E. Sexual Dysfunction and Infertility as Late Effects of Cancer Treatment. Eur. J. Cancer Suppl. 2014, 12, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Sadovsky, R.; Basson, R.; Krychman, M.; Morales, A.M.; Schover, L.; Wang, R.; Incrocci, L. Cancer and Sexual Problems. J. Sex. Med. 2010, 7, 349–373. [Google Scholar] [CrossRef] [PubMed]
- Färkkilä, N.; Sintonen, H.; Saarto, T.; Järvinen, H.; Hänninen, J.; Taari, K.; Roine, R.P. Health-Related Quality of Life in Colorectal Cancer. Color. Dis. 2013, 15, e215–e222. [Google Scholar] [CrossRef] [PubMed]
- Hamidou, Z.; Chibaudel, B.; Hebbar, M.; Hug de Larauze, M.; André, T.; Louvet, C.; Brusquant, D.; Garcia-Larnicol, M.-L.; de Gramont, A.; Bonnetain, F. Time to Definitive Health-Related Quality of Life Score Deterioration in Patients with Resectable Metastatic Colorectal Cancer Treated with FOLFOX4 versus Sequential Dose-Dense FOLFOX7 Followed by FOLFIRI: The MIROX Randomized Phase III Trial. PLoS ONE 2016, 11, e0157067. [Google Scholar] [CrossRef] [PubMed]
- Láng, I.; Köhne, C.-H.; Folprecht, G.; Rougier, P.; Curran, D.; Hitre, E.; Sartorius, U.; Griebsch, I.; Van Cutsem, E. Quality of Life Analysis in Patients with KRAS Wild-Type Metastatic Colorectal Cancer Treated First-Line with Cetuximab plus Irinotecan, Fluorouracil and Leucovorin. Eur. J. Cancer 2013, 49, 439–448. [Google Scholar] [CrossRef]
- Quidde, J.; Hegewisch-Becker, S.; Graeven, U.; Lerchenmüller, C.A.; Killing, B.; Depenbusch, R.; Steffens, C.-C.; Lange, T.; Dietrich, G.; Stoehlmacher, J.; et al. Quality of Life Assessment in Patients with Metastatic Colorectal Cancer Receiving Maintenance Therapy after First-Line Induction Treatment: A Preplanned Analysis of the Phase III AIO KRK 0207 Trial. Ann. Oncol. 2016, 27, 2203–2210. [Google Scholar] [CrossRef]
- Bertaut, A.; Touchefeu, Y.; Blanc, J.; Bouché, O.; François, E.; Conroy, T.; Artru, P.; Adenis, A.; Gobbo, J.; Borg, C.; et al. Health-Related Quality of Life Analysis in Metastatic Colorectal Cancer Patients Treated by Second-Line Chemotherapy, Associated with Either Cetuximab or Bevacizumab: The PRODIGE 18 Randomized Phase II Study. Clin. Color. Cancer 2022, 21, e49–e61. [Google Scholar] [CrossRef]
- Flyum, I.R.; Mahic, S.; Grov, E.K.; Joranger, P. Health-Related Quality of Life in Patients with Colorectal Cancer in the Palliative Phase: A Systematic Review and Meta-Analysis. BMC Palliat. Care 2021, 20, 144. [Google Scholar] [CrossRef]
- Färkkilä, N.; Torvinen, S.; Roine, R.P.; Sintonen, H.; Hänninen, J.; Taari, K.; Saarto, T. Health-Related Quality of Life among Breast, Prostate, and Colorectal Cancer Patients with End-Stage Disease. Qual. Life Res. 2014, 23, 1387–1394. [Google Scholar] [CrossRef]
- Luo, X.; Li, J.; Chen, M.; Gong, J.; Xu, Y.; Li, Q. A Literature Review of Post-treatment Survivorship Interventions for Colorectal Cancer Survivors and/or Their Caregivers. Psychooncology 2021, 30, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Jefford, M.; Emery, J.D.; James Martin, A.; De Abreu Lourenco, R.; Lisy, K.; Grunfeld, E.; Mohamed, M.A.; King, D.; Tebbutt, N.C.; Lee, M.; et al. SCORE: A Randomised Controlled Trial Evaluating Shared Care (General Practitioner and Oncologist) Follow-up Compared to Usual Oncologist Follow-up for Survivors of Colorectal Cancer. eClinicalMedicine 2023, 66, 102346. [Google Scholar] [CrossRef] [PubMed]
- Husson, O.; de Rooij, B.H.; Kieffer, J.; Oerlemans, S.; Mols, F.; Aaronson, N.K.; van der Graaf, W.T.A.; van de Poll-Franse, L.V. The EORTC QLQ-C30 Summary Score as Prognostic Factor for Survival of Patients with Cancer in the “Real-World”: Results from the Population-Based PROFILES Registry. Oncologist 2020, 25, e722. [Google Scholar] [CrossRef] [PubMed]
- Pate, A.; Lowery, J.; Kilbourn, K.; Blatchford, P.J.; McNulty, M.; Risendal, B. Quality of Life and the Negative Impact of Comorbidities in Long-Term Colorectal Cancer Survivors: A Population-Based Comparison. J. Cancer Surviv. 2020, 14, 653–659. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Right Colon | Left Colon | Rectum | p-Value * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1080 | 100% | 310 | 29% | 396 | 37% | 374 | 35% | |||
| Median age (range) | 66 (21–90) | 68 (21–90) | 66 (33–86) | 66 (29–89) | 0.017 | |||||
| Age groups | ≤70 years | 711 | 66% | 190 | 61% | 277 | 70% | 244 | 65% | 0.053 |
| >70 years | 369 | 34% | 120 | 39% | 119 | 30% | 130 | 35% | ||
| Sex | Male | 654 | 61% | 163 | 53% | 246 | 62% | 245 | 66% | 0.002 |
| Female | 426 | 39% | 147 | 47% | 150 | 38% | 129 | 34% | ||
| ECOG performance | 0 | 294 | 27% | 79 | 25% | 120 | 30% | 95 | 25% | 0.388 |
| status | 1 | 598 | 55% | 172 | 55% | 216 | 55% | 210 | 56% | |
| 2–3 | 188 | 17% | 59 | 19% | 60 | 15% | 69 | 18% | ||
| Primary resection | Right colectomy | 42 | 4% | 227 | 73% | 0 | 0% | 0 | 0% | |
| (Sub)Total colectomy | 55 | 5% | 16 | 5% | 24 | 6% | 2 | 1% | ||
| Left colectomy, Sigma, Hartmann | 202 | 19% | 0 | 0% | 266 | 67% | 17 | 5% | ||
| Anterior resection | 283 | 26% | 0 | 0% | 30 | 8% | 172 | 46% | ||
| Abdominoperineal resection | 252 | 23% | 0 | 0% | 0 | 0% | 55 | 15% | ||
| Other | 19 | 2% | 12 | 4% | 4 | 1% | 3 | 1% | ||
| Never surgery | 227 | 21% | 55 | 18% | 72 | 18% | 125 | 33% | ||
| Histology | Adenocarcinoma | 963 | 89% | 248 | 80% | 369 | 93% | 346 | 93% | <0.001 |
| Mucinous adenocarcinoma | 107 | 10% | 56 | 18% | 25 | 6% | 26 | 7% | ||
| Signet cell carcinoma | 6 | 1% | 3 | 1% | 1 | 0.3% | 2 | 1% | ||
| MINEN | 4 | 0.4% | 3 | 1% | 1 | 0.3% | 0 | 0% | ||
| Tumor grade | Low | 717 | 81% | 185 | 71% | 295 | 87% | 237 | 83% | <0.001 |
| High | 168 | 19% | 75 | 29% | 43 | 13% | 50 | 17% | ||
| Not available | 195 | - | 50 | - | 58 | - | 87 | - | - | |
| Presentation of | Synchronous | 732 | 68% | 222 | 72% | 268 | 68% | 242 | 65% | 0.157 |
| metastases | Metachronous | 348 | 32% | 88 | 28% | 128 | 32% | 132 | 35% | |
| Number of | 1 | 582 | 54% | 161 | 52% | 225 | 57% | 196 | 52% | 0.122 |
| metastatic sites | 2 | 317 | 29% | 84 | 27% | 116 | 29% | 117 | 31% | |
| 3+ | 181 | 17% | 65 | 21% | 55 | 14% | 61 | 16% | ||
| Metastatic sites | Liver | 809 | 75% | 219 | 71% | 322 | 81% | 268 | 72% | 0.001 |
| Lung | 331 | 31% | 69 | 22% | 97 | 24% | 165 | 44% | <0.001 | |
| Lymph nodes | 272 | 25% | 95 | 31% | 72 | 18% | 105 | 28% | <0.001 | |
| Peritoneum | 170 | 16% | 85 | 27% | 64 | 16% | 21 | 6% | <0.001 | |
| Local relapse | 67 | 6% | 21 | 7% | 19 | 5% | 27 | 7% | 0.336 | |
| Ovarian | 26 | 2% | 15 | 5% | 7 | 2% | 4 | 1% | 0.003 | |
| Bone | 26 | 2% | 8 | 3% | 6 | 2% | 12 | 3% | 0.301 | |
| Adrenal | 15 | 1% | 3 | 1% | 6 | 2% | 6 | 2% | 0.750 | |
| Brain | 3 | 0% | 1 | 0% | 2 | 1% | 0 | 0% | 0.406 | |
| Other | 89 | 8% | 32 | 10% | 34 | 9% | 23 | 6% | 0.135 | |
| Smoking status | Former or never | 662 | 86% | 199 | 88% | 252 | 90% | 211 | 81% | 0.006 |
| Current | 106 | 14% | 28 | 12% | 28 | 10% | 50 | 19% | ||
| Not available | 312 | - | 83 | - | 116 | - | 113 | - | - | |
| Mutation status | RAS & BRAF wt | 354 | 35% | 56 | 19% | 165 | 44% | 133 | 38% | <0.001 |
| RAS mt | 553 | 55% | 163 | 56% | 190 | 51% | 200 | 58% | ||
| BRAF-V600E mt | 99 | 10% | 70 | 24% | 16 | 4% | 13 | 4% | ||
| (K)RAS wt | 59 | - | 16 | - | 21 | - | 22 | - | - | |
| Not tested | 15 | - | 5 | - | 4 | - | 6 | - | - | |
| MMR-status | pMMR | 410 | 97% | 107 | 92% | 165 | 97% | 138 | 100% | 0.002 |
| dMMR | 14 | 3% | 9 | 8% | 5 | 3% | 0 | 0% | ||
| Not available | 656 | - | 194 | - | 226 | - | 236 | - | - | |
| All Patients | Right Colon | Left Colon | Rectum | p-Value * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1080 | 100% | 310 | 29% | 396 | 37% | 374 | 35% | |||
| Upfront resectability | Upfront resectable | 309 | 29% | 79 | 26% | 127 | 32% | 103 | 28% | 0.008 |
| by central assessment | Borderline resectable | 179 | 17% | 44 | 14% | 80 | 20% | 55 | 15% | |
| Non-resectable | 592 | 55% | 187 | 60% | 189 | 48% | 216 | 58% | ||
| Final resectability | Upfront resectable | 309 | 29% | 79 | 26% | 127 | 32% | 103 | 28% | <0.001 |
| status | Converted resectable | 137 | 13% | 25 | 8% | 69 | 17% | 43 | 12% | |
| Unconvertable | 51 | 5% | 19 | 6% | 18 | 5% | 14 | 4% | ||
| Nonresectable mets | 583 | 54% | 187 | 60% | 182 | 46% | 214 | 57% | ||
| Treatment groups | R0–1 resection | 326 | 30% | 73 | 24% | 142 | 36% | 111 | 30% | 0.001 |
| R2-resection or LAT | 71 | 7% | 11 | 4% | 34 | 9% | 26 | 7% | ||
| Systemic only | 660 | 61% | 216 | 70% | 218 | 55% | 226 | 60% | ||
| Best supportive care | 23 | 2% | 10 | 3% | 2 | 1% | 11 | 3% | - | |
| Metastasectomies | All patients | 399 | 37% | 86 | 28% | 176 | 44% | 137 | 37% | <0.001 |
| and/or LAT | Single site metastases | 309/582 | 53% | 64/161 | 40% | 141/225 | 63% | 104/196 | 53% | <0.001 |
| Multiple metastatic sites | 90/498 | 18% | 22/149 | 15% | 35/171 | 21% | 33/178 | 19% | 0.409 | |
| Liver procedure | 316 | 29% | 57 | 18% | 151 | 38% | 108 | 29% | <0.001 | |
| Baseline liver mets | 310/809 | 38% | 57/218 | 26% | 147/321 | 46% | 106/270 | 39% | <0.001 | |
| Baseline liver only | 266/699 | 38% | 47/195 | 24% | 134/269 | 50% | 85/235 | 36% | <0.001 | |
| Lung procedures | 81 | 8% | 10 | 3% | 30 | 8% | 41 | 11% | 0.001 | |
| Baseline lung mets | 46/330 | 14% | 6/68 | 9% | 12/97 | 12% | 28/165 | 17% | 0.229 | |
| Baseline lung only | 27/66 | 41% | 4/10 | 40% | 6/12 | 50% | 17/44 | 39% | 0.776 | |
| Cytoreductive surgery | 48 | 4% | 22 | 7% | 21 | 5% | 5 | 1% | 0.001 | |
| Baseline peritoneal mets | 34/172 | 20% | 17/87 | 20% | 15/64 | 23% | 2/21 | 10% | 0.276 | |
| Baseline peritoneal only | 11/43 | 26% | 8/27 | 30% | 2/13 | 15% | 1/3 | 33% | 0.307 | |
| Local relapse resected | 41 | 4% | 11 | 4% | 16 | 4% | 14 | 4% | 0.942 | |
| Distant lymphadenectomy | 15 | 1% | 6 | 2% | 5 | 1% | 4 | 1% | 0.606 | |
| Gynecologic resection | 17 | 2% | 7 | 2% | 9 | 2% | 1 | 0% | 0.043 | |
| Urologic resection | 10 | 1% | 3 | 1% | 4 | 1% | 3 | 1% | 0.952 | |
| Subcutaneous resection | 10 | 1% | 7 | 2% | 2 | 1% | 1 | 0% | 0.014 | |
| Total | Right Colon | Left Colon | Rectum | p-Value * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1080 | 100% | 310 | 29% | 396 | 37% | 374 | 35% | |||
| Type of treatment | Systemic therapy only | 660 | 61% | 216 | 70% | 218 | 55% | 226 | 60% | <0.001 |
| Metastasectomy and/or LAT | 397 | 37% | 84 | 27% | 176 | 44% | 137 | 37% | ||
| Best supportive care | 23 | 2% | 10 | 3% | 2 | 1% | 11 | 3% | ||
| Chemotherapy | Given in any line or intent | 1052 | 100% | 299 | 100% | 391 | 100% | 362 | 100% | - |
| Number of lines | 1 | 408 | 39% | 124 | 41% | 146 | 37% | 138 | 38% | 0.484 |
| 2 | 269 | 26% | 81 | 27% | 96 | 25% | 92 | 25% | ||
| ≥3 | 375 | 36% | 94 | 31% | 149 | 38% | 132 | 36% | ||
| First-line chemotherapy | Fluoropyrimidine | 1042 | 99% | 295 | 99% | 389 | 99% | 358 | 99% | 0.504 |
| Oxaliplatin | 649 | 62% | 199 | 67% | 239 | 61% | 211 | 58% | 0.090 | |
| Irinotecan | 273 | 26% | 61 | 20% | 116 | 30% | 96 | 27% | 0.022 | |
| Bevacizumab | 614 | 58% | 198 | 66% | 213 | 54% | 203 | 56% | 0.005 | |
| EGFR-inhibitor | 148 | 14% | 15 | 5% | 72 | 18% | 61 | 17% | <0.001 | |
| Best response in first line | PR/CR/NED | 641 | 62% | 159 | 54% | 257 | 67% | 225 | 64% | <0.001 |
| SD | 292 | 28% | 88 | 30% | 106 | 27% | 98 | 28% | ||
| PD | 99 | 10% | 46 | 16% | 23 | 6% | 30 | 8% | ||
| Not available | 20 | - | 6 | - | 5 | - | 9 | - | - | |
| Chemotherapy all lines | Fluoropyrimidine | 1045 | 99% | 296 | 99% | 390 | 100% | 359 | 99% | 0.437 |
| Oxaliplatin | 836 | 79% | 241 | 81% | 315 | 81% | 280 | 77% | 0.468 | |
| Irinotecan | 763 | 73% | 206 | 69% | 295 | 75% | 262 | 72% | 0.161 | |
| VEGF-inhibitor | 756 | 72% | 227 | 76% | 273 | 70% | 256 | 71% | 0.176 | |
| EGFR-inhibitor | 313 | 30% | 46 | 15% | 147 | 38% | 120 | 33% | <0.001 | |
| Univariable | Multivariable | |||||||
|---|---|---|---|---|---|---|---|---|
| N | HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age continuous (years) | 1080 | 1.02 | 1.01–1.02 | <0.001 | 1.00 | 0.99–1.00 | 0.287 | |
| Primary tumor location | Right colon | 310 | 1 | 1 | ||||
| Left colon | 396 | 0.57 | 0.47–0.68 | <0.001 | 0.77 | 0.63–0.93 | 0.007 | |
| Rectum | 374 | 0.61 | 0.51–0.73 | <0.001 | 0.64 | 0–53–0.78 | <0.001 | |
| Number of metastatic | 1 | 582 | 1 | 1 | ||||
| sites | 2 | 317 | 1.86 | 1.58–2.19 | <0.001 | 1.31 | 1.11–1.56 | 0.002 |
| 3–5 | 181 | 2.62 | 2.16–3.17 | <0.001 | 1.78 | 1.46–2.17 | <0.001 | |
| ECOG Performance status | 0 | 294 | 1 | 1 | ||||
| 1 | 598 | 1.77 | 1.47–2.13 | <0.001 | 1.48 | 1.23–1.79 | <0.001 | |
| 2–3 | 188 | 3.72 | 2.98–4.65 | <0.001 | 2.56 | 2.03–3.23 | <0.001 | |
| Type of treatment | Systemic therapy only | 660 | 1 | 1 | ||||
| Metastasectomy and/or LAT | 397 | 0.19 | 0.16–0.23 | <0.001 | 0.24 | 0.20–0.29 | <0.001 | |
| Best supportive care | 23 | 10.52 | 6.86–16.12 | <0.001 | 11.02 | 6.89–17.63 | <0.001 | |
| Mutation groups | RAS & BRAF wt | 354 | 1 | 1 | ||||
| RAS mt | 553 | 1.46 | 1.23–1.73 | <0.001 | 1.41 | 1.19–1.68 | <0.001 | |
| BRAF-V600E mt | 99 | 3.13 | 2.42–4.04 | <0.001 | 2.03 | 1.54–2.69 | <0.001 | |
| (K)RAS wt | 59 | 2.96 | 2.19–4.00 | <0.001 | 2.37 | 1.74–3.24 | <0.001 | |
| Not tested | 15 | 2.48 | 1.38–4.44 | 0.002 | 2.56 | 1.40–4.68 | 0.002 | |
| MMR–status | pMMR | 410 | 1 | 1 | ||||
| dMMR | 14 | 1.06 | 0.55–2.07 | 0.857 | 0.69 | 0.35–1.36 | 0.287 | |
| Not tested | 656 | 1.35 | 1.16–1.57 | <0.001 | 0.98 | 0.83–1.15 | 0.768 | |
| 15D | EQ-5D | VAS | GHS | Symptom Burden * | Functioning Scale Sum | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ∆ | p Value | ∆ | p Value | ∆ | p Value | ∆ | p Value | ∆ | p Value | ∆ | p Value | |
| Right colon vs. Left colon | ||||||||||||
| Post-resection | 0.009 | 0.794 | −0.074 | 0.312 | −3.6 | 0.565 | −1.0 | 0.943 | 104 | 0.263 | −29 | 0.494 |
| Remission | 0.010 | 0.499 | 0.000 | 0.752 | −3.0 | 0.303 | 0.4 | 0.853 | 23 | 0.753 | 0 | 0.848 |
| Systemic therapy | 0.001 | 0.533 | 0.001 | 0.570 | −1.7 | 0.273 | −3.6 | 0.232 | −9 | 0.794 | −31 | 0.190 |
| Best supportive care | −0.069 | 0.237 | −0.108 | 0.197 | 0.8 | 0.877 | −12.2 | 0.197 | 60 | 0.400 | −82 | 0.255 |
| Right colon vs. Rectum | ||||||||||||
| Post-resection | −0.053 | 0.169 | −0.140 | 0.069 | −10.5 | 0.044 | −5.4 | 0.627 | 142 | 0.140 | −104 | 0.077 |
| Remission | 0.020 | 0.512 | −0.010 | 0.519 | −2.2 | 0.638 | 0.8 | 0.768 | −59 | 0.217 | 19 | 0.798 |
| Systemic therapy | 0.000 | 0.642 | −0.010 | 0.689 | 0.1 | 0.993 | −2.0 | 0.564 | −49 | 0.172 | −52 | 0.023 |
| Best supportive care | 0.007 | 0.837 | 0.013 | 0.902 | −2.2 | 0.930 | −9.4 | 0.299 | −38 | 0.837 | −125 | 0.142 |
| Left colon vs. Rectum | ||||||||||||
| Post-resection | −0.062 | 0.012 | −0.066 | 0.050 | −6.9 | 0.157 | −4.5 | 0.370 | 38 | 0.455 | −75 | 0.024 |
| Remission | 0.010 | 0.904 | −0.010 | 0.688 | 0.8 | 0.628 | 0.3 | 0.741 | −82 | 0.072 | 19 | 0.603 |
| Systemic therapy | 0.010 | 0.823 | −0.000 | 0.733 | 1.7 | 0.346 | 1.6 | 0.433 | −40 | 0.259 | −21 | 0.310 |
| Best supportive care | 0.076 | 0.217 | 0.121 | 0.462 | −3.0 | 0.531 | 2.8 | 0.742 | −98 | 0.538 | 143 | 0.810 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aho, S.; Osterlund, E.; Ristimäki, A.; Nieminen, L.; Sundström, J.; Mäkinen, M.J.; Kuopio, T.; Kytölä, S.; Ålgars, A.; Ristamäki, R.; et al. Impact of Primary Tumor Location on Demographics, Resectability, Outcomes, and Quality of Life in Finnish Metastatic Colorectal Cancer Patients (Subgroup Analysis of the RAXO Study). Cancers 2024, 16, 1052. https://doi.org/10.3390/cancers16051052
Aho S, Osterlund E, Ristimäki A, Nieminen L, Sundström J, Mäkinen MJ, Kuopio T, Kytölä S, Ålgars A, Ristamäki R, et al. Impact of Primary Tumor Location on Demographics, Resectability, Outcomes, and Quality of Life in Finnish Metastatic Colorectal Cancer Patients (Subgroup Analysis of the RAXO Study). Cancers. 2024; 16(5):1052. https://doi.org/10.3390/cancers16051052
Chicago/Turabian StyleAho, Sonja, Emerik Osterlund, Ari Ristimäki, Lasse Nieminen, Jari Sundström, Markus J. Mäkinen, Teijo Kuopio, Soili Kytölä, Annika Ålgars, Raija Ristamäki, and et al. 2024. "Impact of Primary Tumor Location on Demographics, Resectability, Outcomes, and Quality of Life in Finnish Metastatic Colorectal Cancer Patients (Subgroup Analysis of the RAXO Study)" Cancers 16, no. 5: 1052. https://doi.org/10.3390/cancers16051052
APA StyleAho, S., Osterlund, E., Ristimäki, A., Nieminen, L., Sundström, J., Mäkinen, M. J., Kuopio, T., Kytölä, S., Ålgars, A., Ristamäki, R., Heervä, E., Kallio, R., Halonen, P., Soveri, L.-M., Nordin, A., Uutela, A., Salminen, T., Stedt, H., Lamminmäki, A., ... Osterlund, P. (2024). Impact of Primary Tumor Location on Demographics, Resectability, Outcomes, and Quality of Life in Finnish Metastatic Colorectal Cancer Patients (Subgroup Analysis of the RAXO Study). Cancers, 16(5), 1052. https://doi.org/10.3390/cancers16051052