
Advanced Diagnostic and Therapeutic Endoscopy for Early Gastric Cancer


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
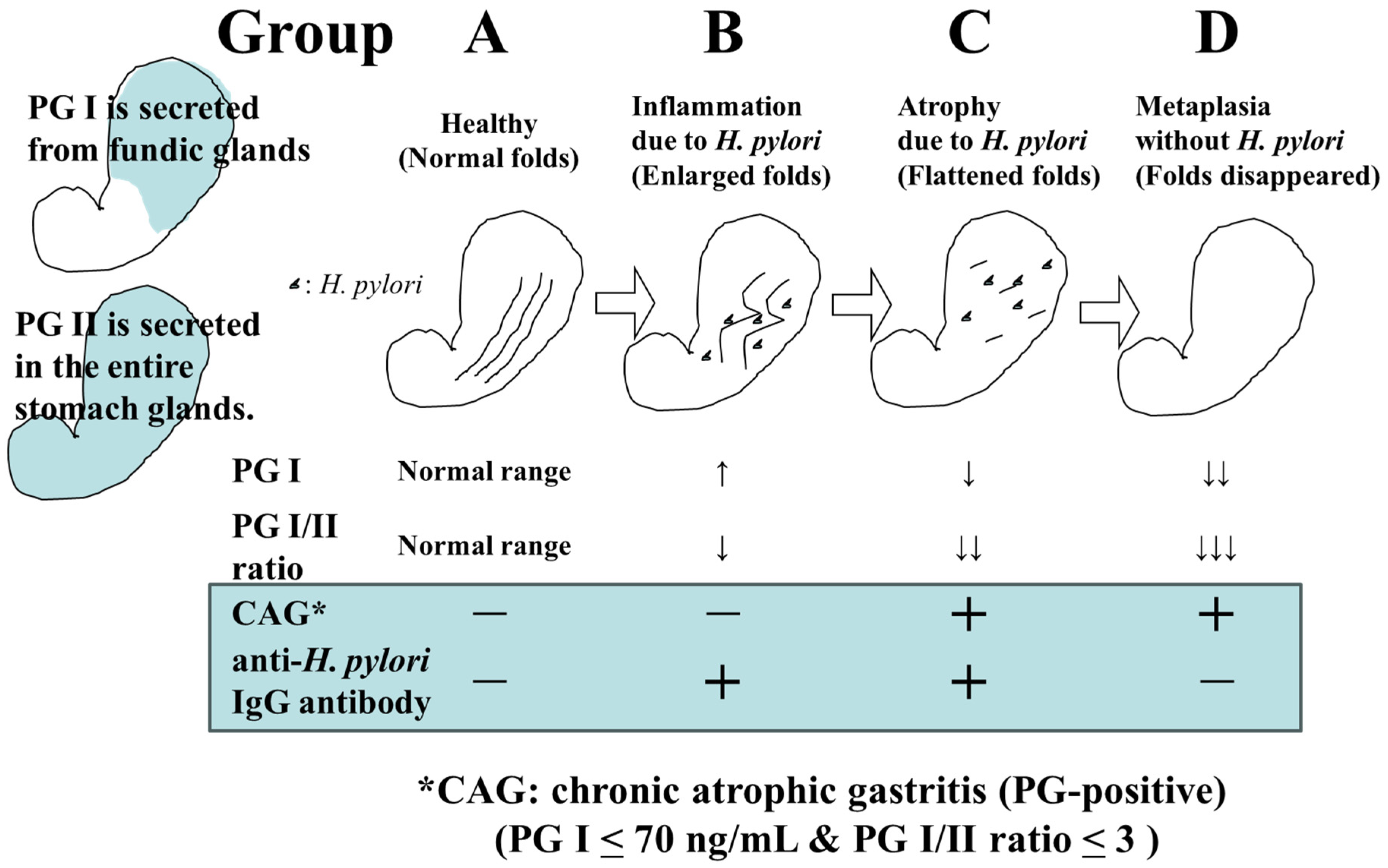
2. The Role of Endoscopy in Gastric Cancer Detection
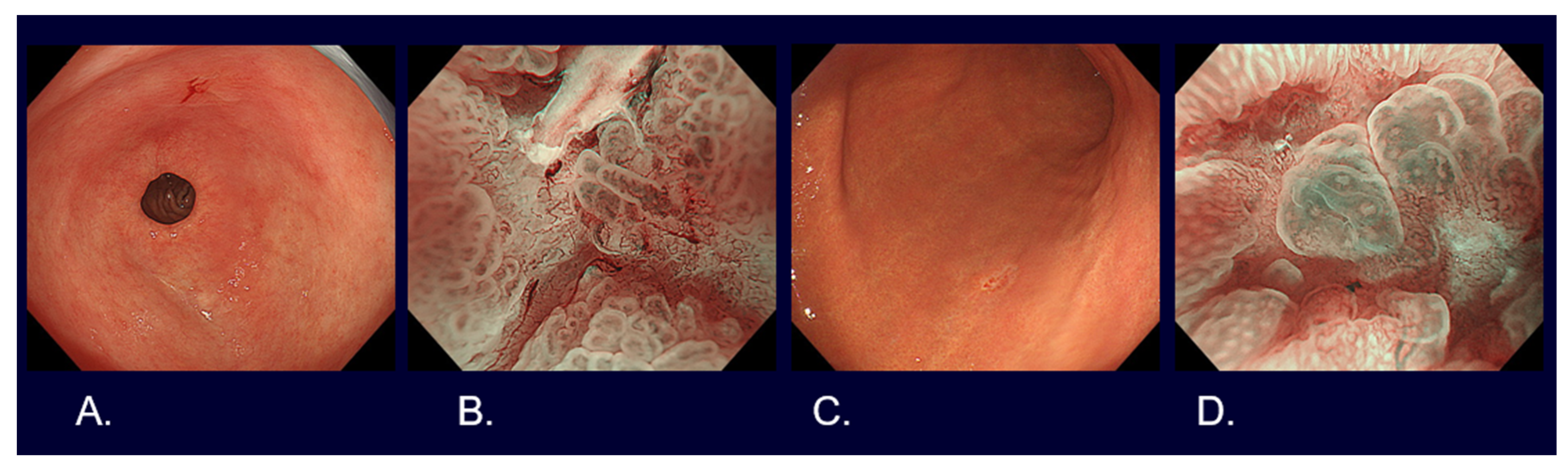
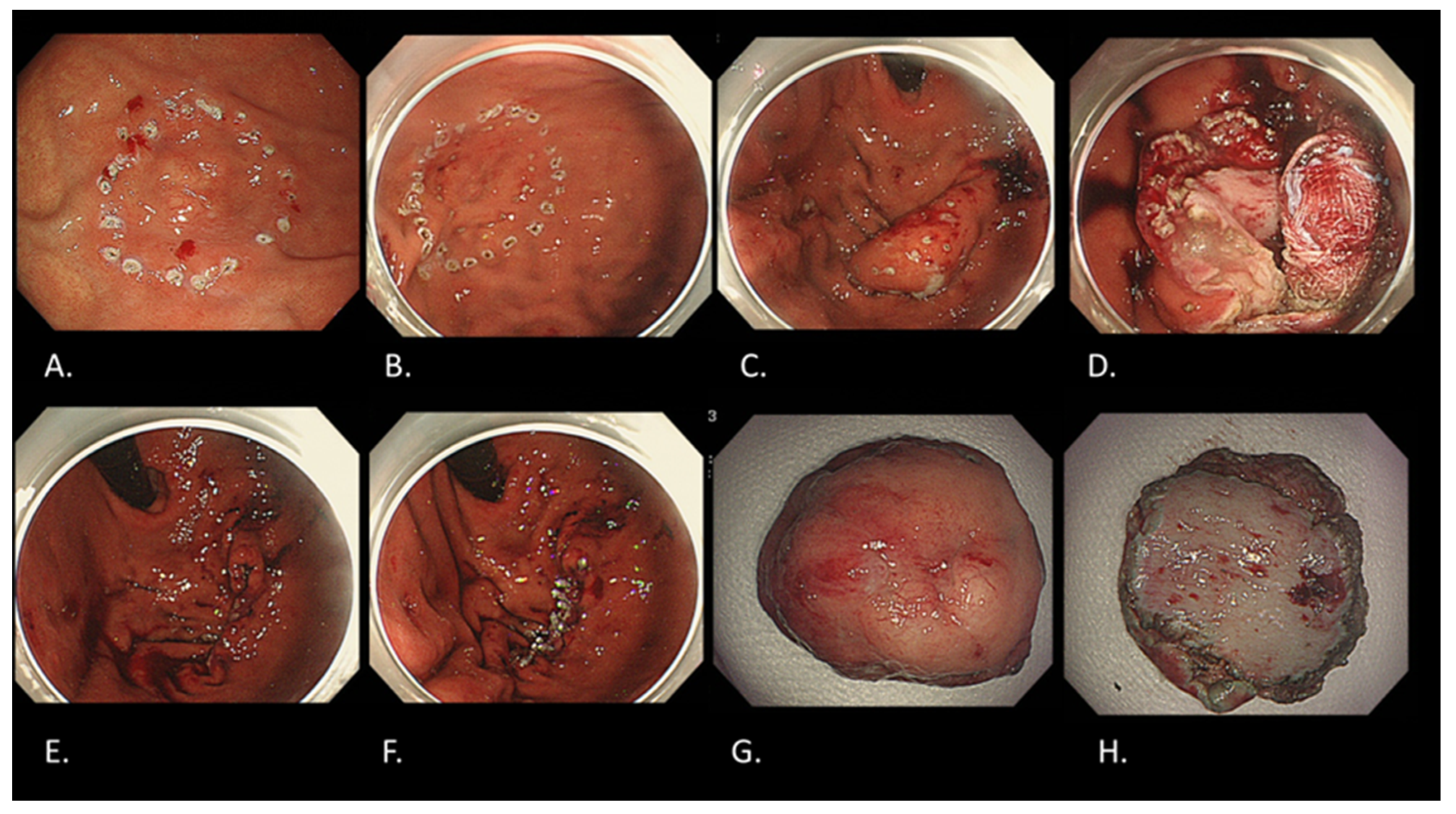
3. Endoscopic Diagnosis of Early Gastric Cancer
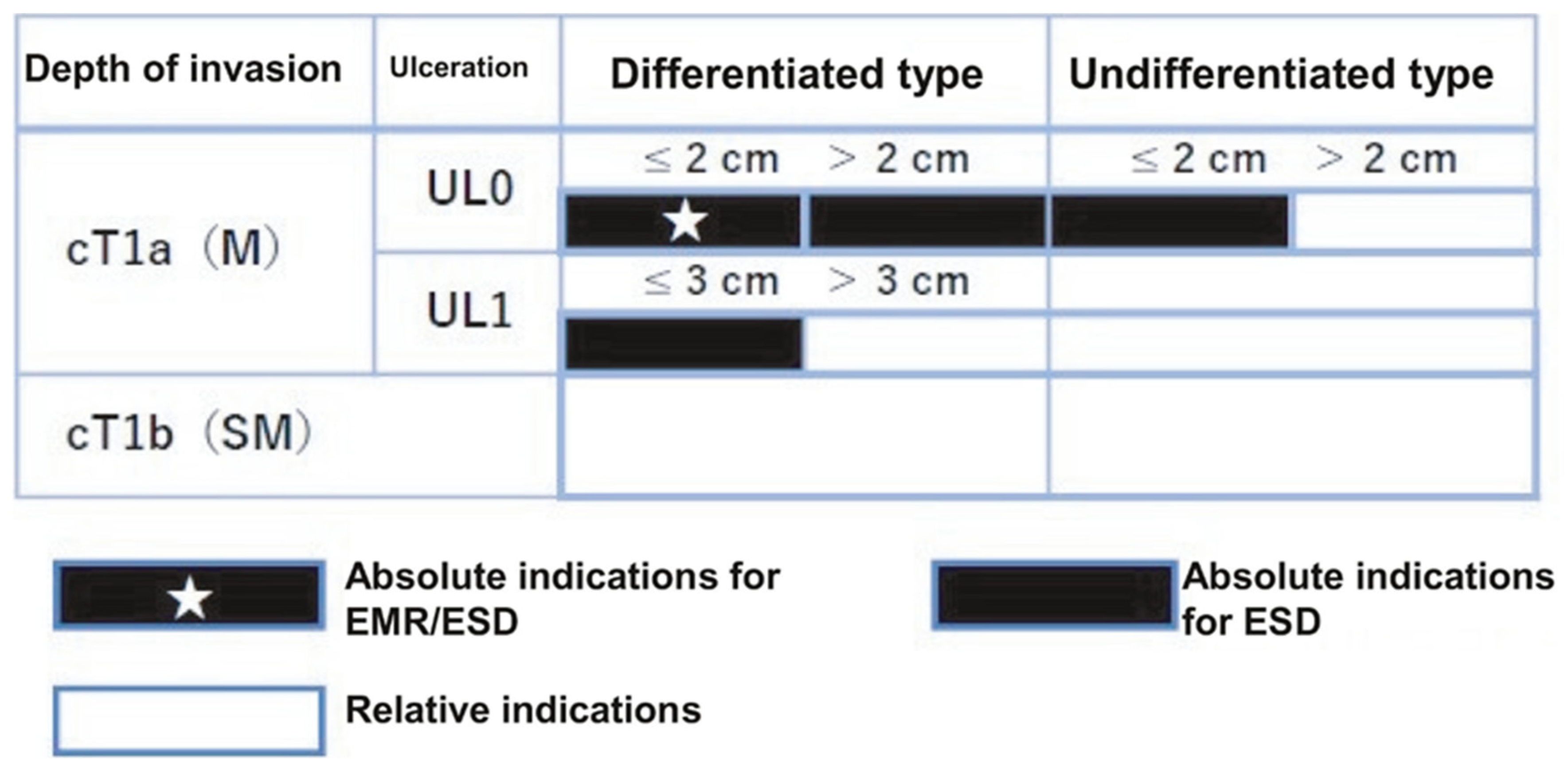
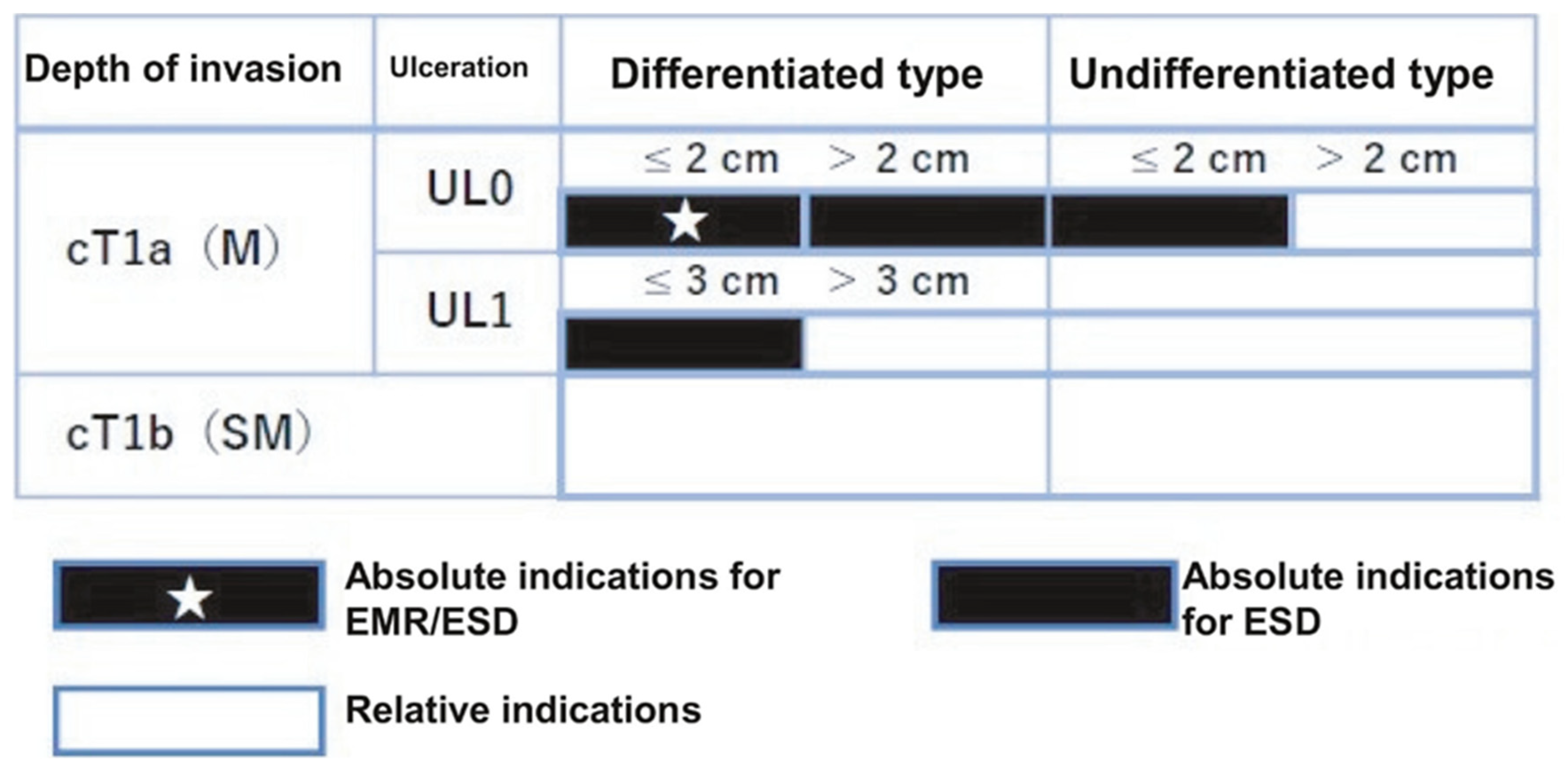
4. Guidelines for Endoscopic Resection for Early Gastric Cancers [14,15]
Indications of Endoscopic Resection for Early Gastric Cancer
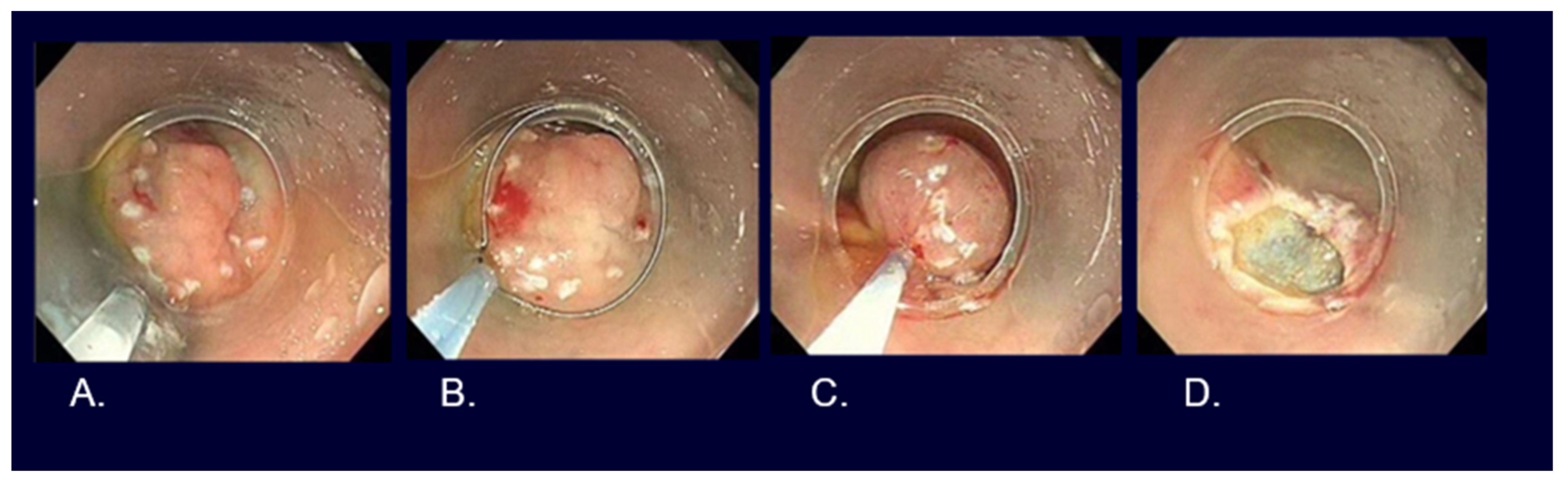
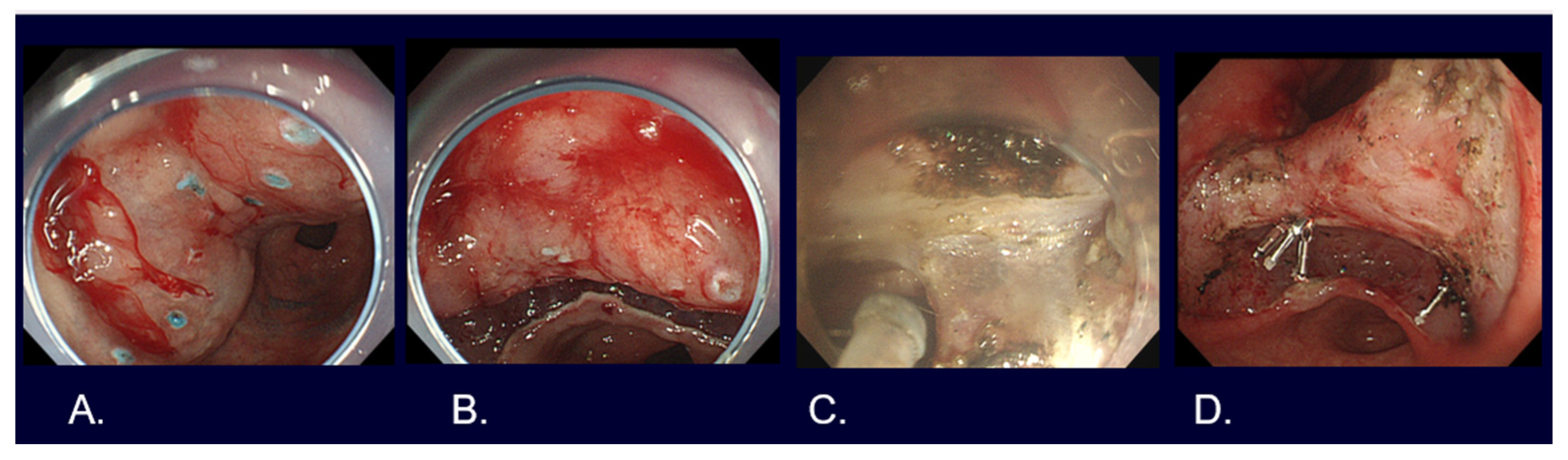
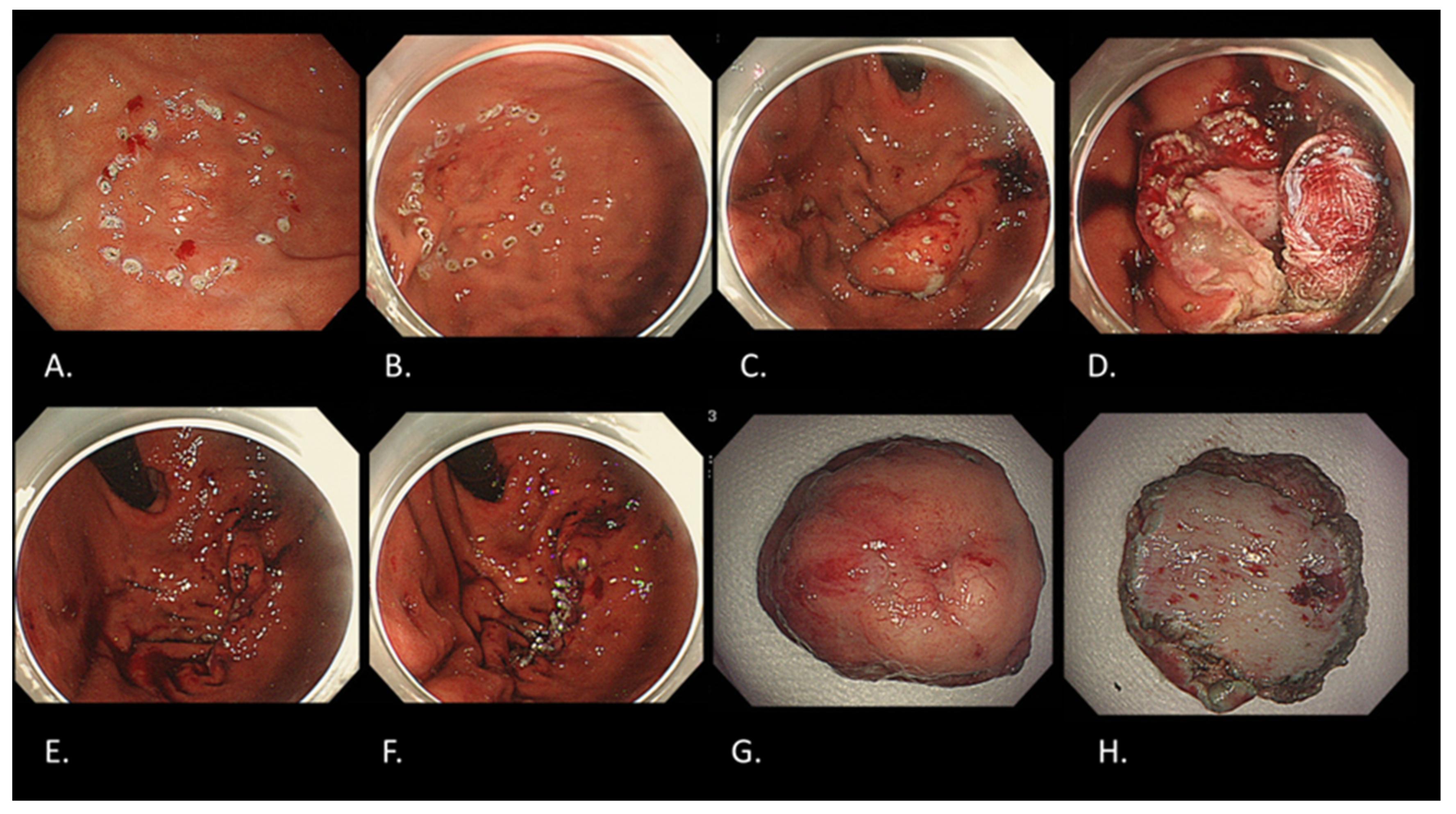
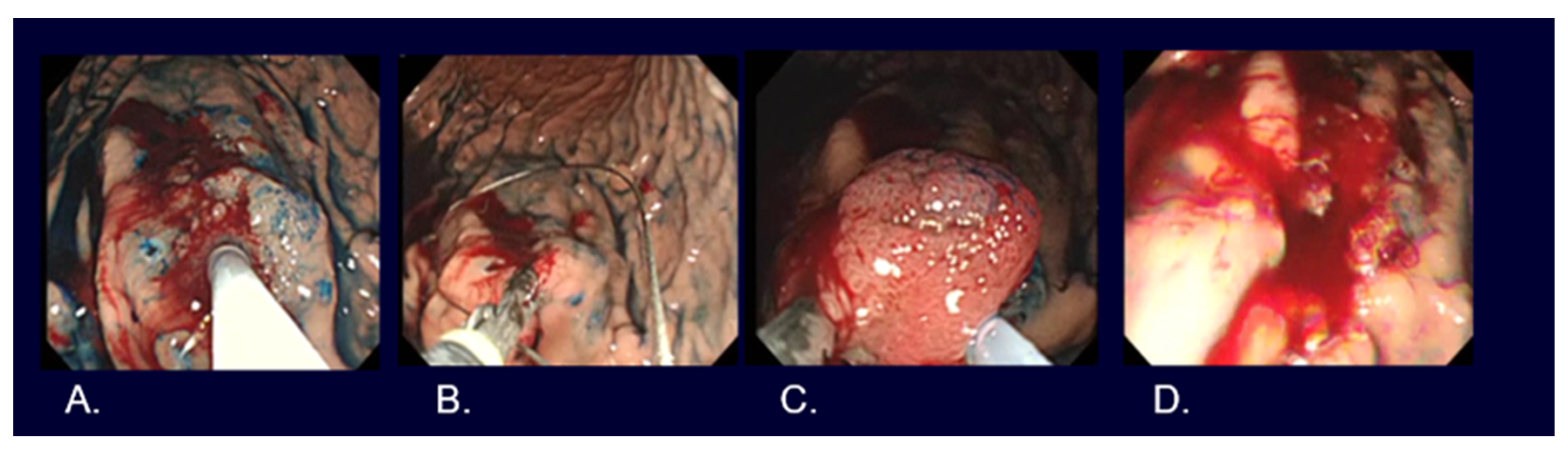
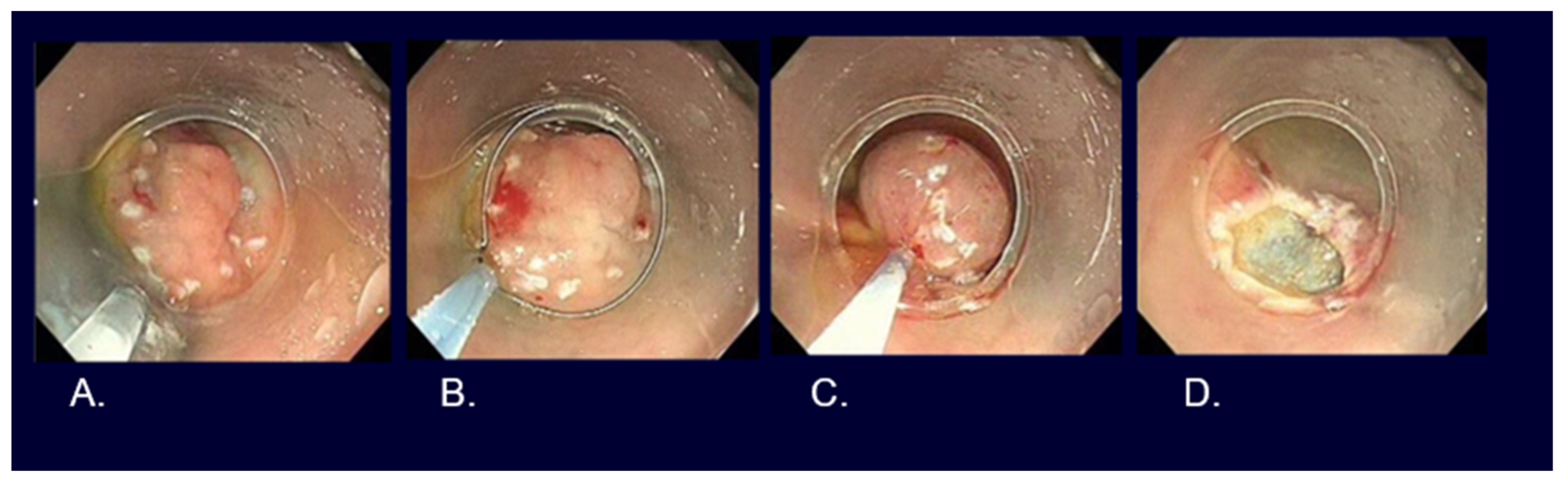
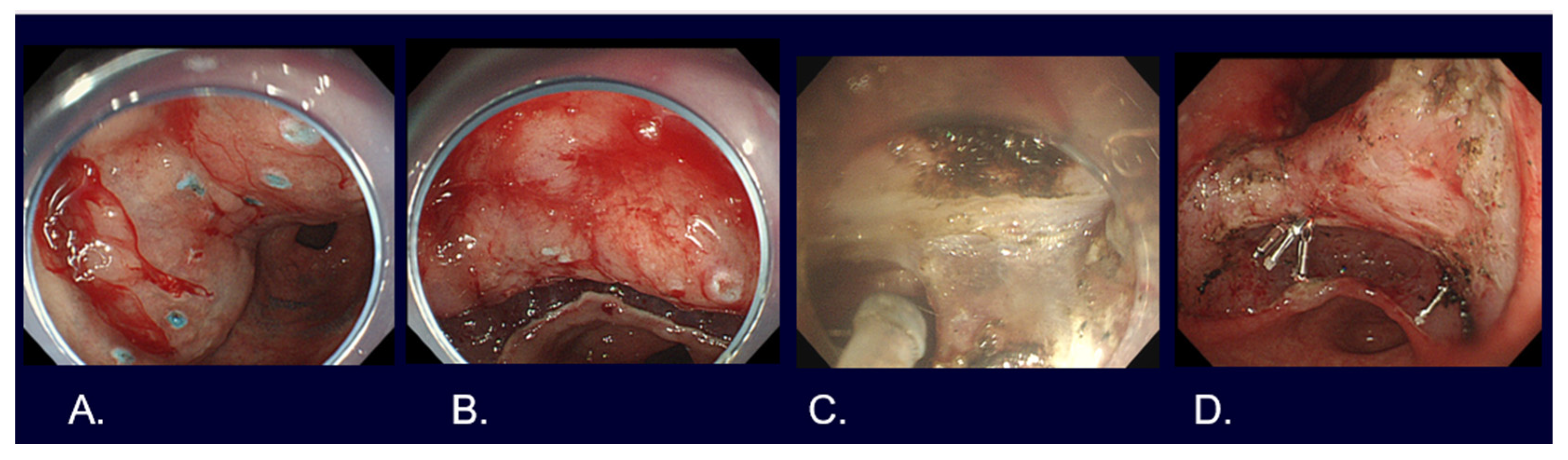
5. Types of Endoscopic Resection for Early Gastric Cancer
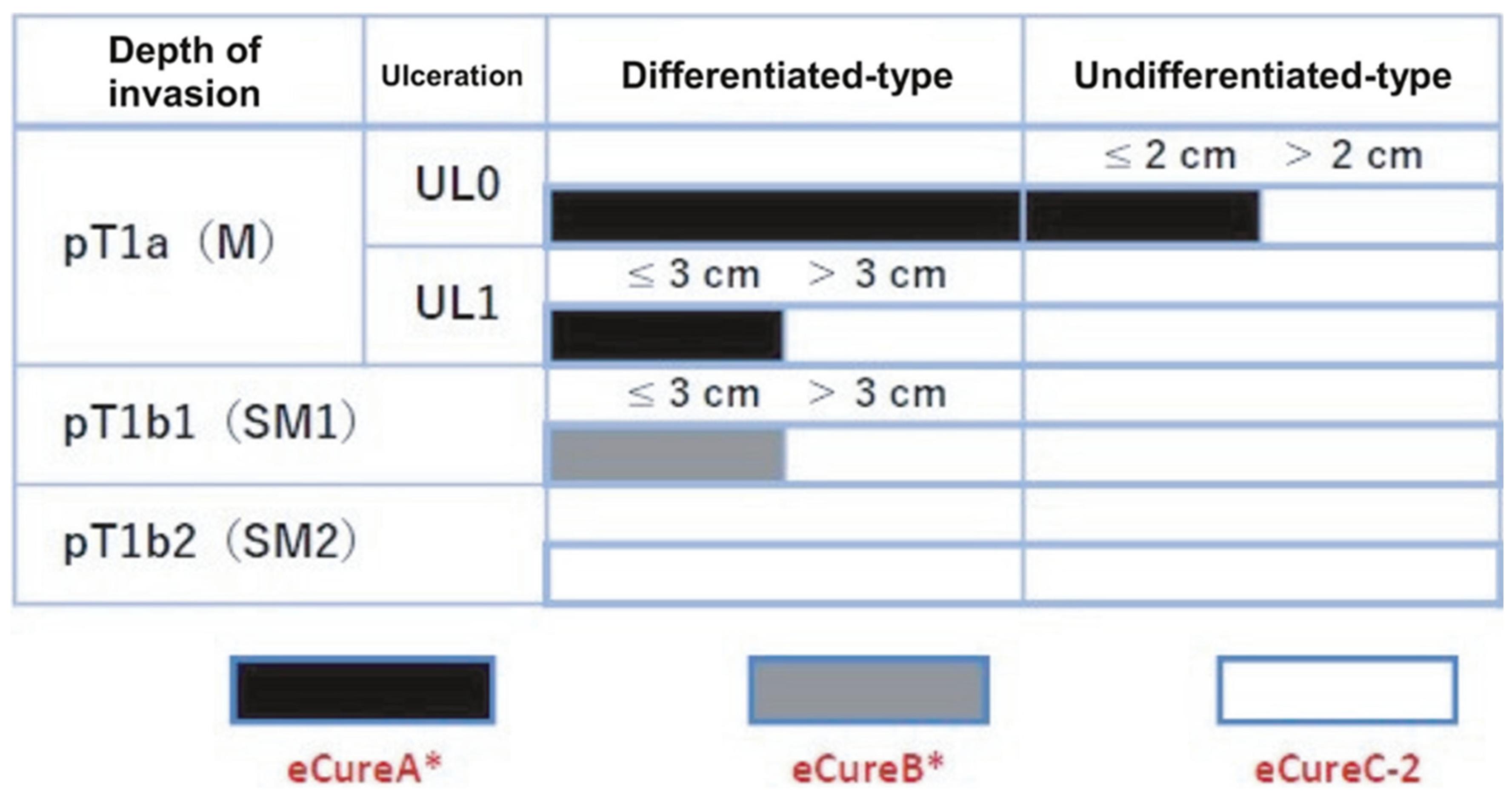
6. Evaluation of Curability after Endoscopic Resection
7. Endoscopic Resection Results for Early-Stage Gastric Cancer
8. Future Perspectives on Endoscopic Diagnosis and Treatment for Early Gastric Cancer
9. Conclusions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kato, M. Endoscopic Submucosal Dissection (ESD) Is Being Accepted as a New Procedure of Endoscopic Treatment of Early Gastric Cancer. Intern. Med. Tokyo Jpn. 2005, 44, 85–86. [Google Scholar] [CrossRef] [PubMed]
- Ono, H.; Kondo, H.; Gotoda, T.; Shirao, K.; Yamaguchi, H.; Saito, D.; Hosokawa, K.; Shimoda, T.; Yoshida, S. Endoscopic Mucosal Resection for Treatment of Early Gastric Cancer. Gut 2001, 48, 225–229. [Google Scholar] [CrossRef]
- Hamashima, C. Systematic Review Group and Guideline Development Group for Gastric Cancer Screening Guidelines Update Version of the Japanese Guidelines for Gastric Cancer Screening. Jpn. J. Clin. Oncol. 2018, 48, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Mabe, K.; Inoue, K.; Kamada, T.; Kato, K.; Kato, M.; Haruma, K. Endoscopic Screening for Gastric Cancer in Japan: Current Status and Future Perspectives. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2022, 34, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Miki, K. Gastric Cancer Screening by Combined Assay for Serum Anti-Helicobacter Pylori IgG Antibody and Serum Pepsinogen Levels-“ABC Method”. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2011, 87, 405–414. [Google Scholar] [CrossRef]
- Yoshida, T.; Kato, J.; Inoue, I.; Yoshimura, N.; Deguchi, H.; Mukoubayashi, C.; Oka, M.; Watanabe, M.; Enomoto, S.; Niwa, T.; et al. Cancer Development Based on Chronic Active Gastritis and Resulting Gastric Atrophy as Assessed by Serum Levels of Pepsinogen and Helicobacter Pylori Antibody Titer. Int. J. Cancer 2014, 134, 1445–1457. [Google Scholar] [CrossRef]
- Watanabe, M.; Kato, J.; Inoue, I.; Yoshimura, N.; Yoshida, T.; Mukoubayashi, C.; Deguchi, H.; Enomoto, S.; Ueda, K.; Maekita, T.; et al. Development of Gastric Cancer in Nonatrophic Stomach with Highly Active Inflammation Identified by Serum Levels of Pepsinogen and Helicobacter Pylori Antibody Together with Endoscopic Rugal Hyperplastic Gastritis. Int. J. Cancer 2012, 131, 2632–2642. [Google Scholar] [CrossRef]
- Yagi, K.; Nakamura, A.; Sekine, A. Characteristic Endoscopic and Magnified Endoscopic Findings in the Normal Stomach without Helicobacter Pylori Infection. J. Gastroenterol. Hepatol. 2002, 17, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Nishibayashi, H.; Kanayama, S.; Kiyohara, T.; Yamamoto, K.; Miyazaki, Y.; Yasunaga, Y.; Shinomura, Y.; Takeshita, T.; Takeuchi, T.; Morimoto, K.; et al. Helicobacter Pylori-Induced Enlarged-Fold Gastritis Is Associated with Increased Mutagenicity of Gastric Juice, Increased Oxidative DNA Damage, and an Increased Risk of Gastric Carcinoma. J. Gastroenterol. Hepatol. 2003, 18, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Kamada, T.; Tanaka, A.; Yamanaka, Y.; Manabe, N.; Kusunoki, H.; Miyamoto, M.; Tanaka, S.; Hata, J.; Chayama, K.; Haruma, K. Nodular Gastritis with Helicobacter pylori Infection Is Strongly Associated with Diffuse-Type Gastric Cancer in Young Patients. Dig. Endosc. 2007, 19, 180–184. [Google Scholar] [CrossRef]
- Muto, M.; Yao, K.; Kaise, M.; Kato, M.; Uedo, N.; Yagi, K.; Tajiri, H. Magnifying Endoscopy Simple Diagnostic Algorithm for Early Gastric Cancer (MESDA-G). Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2016, 28, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Yao, K.; Anagnostopoulos, G.K.; Ragunath, K. Magnifying Endoscopy for Diagnosing and Delineating Early Gastric Cancer. Endoscopy 2009, 41, 462–467. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2023, 26, 1–25. [Google Scholar] [CrossRef]
- Ono, H.; Yao, K.; Fujishiro, M.; Oda, I.; Uedo, N.; Nimura, S.; Yahagi, N.; Iishi, H.; Oka, M.; Ajioka, Y.; et al. Guidelines for Endoscopic Submucosal Dissection and Endoscopic Mucosal Resection for Early Gastric Cancer (Second Edition). Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2021, 33, 4–20. [Google Scholar] [CrossRef]
- Nakayoshi, T.; Tajiri, H.; Matsuda, K.; Kaise, M.; Ikegami, M.; Sasaki, H. Magnifying Endoscopy Combined with Narrow Band Imaging System for Early Gastric Cancer: Correlation of Vascular Pattern with Histopathology (Including Video). Endoscopy 2004, 36, 1080–1084. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, Y.; Hirasawa, T.; Ishizuka, N.; Hatamori, H.; Ikenoyama, Y.; Tokura, J.; Ishioka, M.; Tokai, Y.; Namikawa, K.; Yoshimizu, S.; et al. Diagnostic Performance in Gastric Cancer Is Higher Using Endocytoscopy with Narrow-Band Imaging than Using Magnifying Endoscopy with Narrow-Band Imaging. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2021, 24, 417–427. [Google Scholar] [CrossRef]
- Choi, J.; Kim, S.G.; Im, J.P.; Kim, J.S.; Jung, H.C.; Song, I.S. Is Endoscopic Ultrasonography Indispensable in Patients with Early Gastric Cancer Prior to Endoscopic Resection? Surg. Endosc. 2010, 24, 3177–3185. [Google Scholar] [CrossRef]
- Asada-Hirayama, I.; Kodashima, S.; Sakaguchi, Y.; Ono, S.; Niimi, K.; Mochizuki, S.; Tsuji, Y.; Minatsuki, C.; Shichijo, S.; Matsuzaka, K.; et al. Magnifying Endoscopy with Narrow-Band Imaging Is More Accurate for Determination of Horizontal Extent of Early Gastric Cancers than Chromoendoscopy. Endosc. Int. Open 2016, 4, E690–E698. [Google Scholar] [CrossRef]
- Tada, M.; Murakami, A.; Karita, M.; Yanai, H.; Okita, K. Endoscopic Resection of Early Gastric Cancer. Endoscopy 1993, 25, 445–450. [Google Scholar] [CrossRef]
- Inoue, H.; Takeshita, K.; Hori, H.; Muraoka, Y.; Yoneshima, H.; Endo, M. Endoscopic Mucosal Resection with a Cap-Fitted Panendoscope for Esophagus, Stomach, and Colon Mucosal Lesions. Gastrointest. Endosc. 1993, 39, 58–62. [Google Scholar] [CrossRef]
- Lian, J.; Chen, S.; Zhang, Y.; Qiu, F. A Meta-Analysis of Endoscopic Submucosal Dissection and EMR for Early Gastric Cancer. Gastrointest. Endosc. 2012, 76, 763–770. [Google Scholar] [CrossRef]
- Watanabe, K.; Ogata, S.; Kawazoe, S.; Watanabe, K.; Koyama, T.; Kajiwara, T.; Shimoda, Y.; Takase, Y.; Irie, K.; Mizuguchi, M.; et al. Clinical Outcomes of EMR for Gastric Tumors: Historical Pilot Evaluation between Endoscopic Submucosal Dissection and Conventional Mucosal Resection. Gastrointest. Endosc. 2006, 63, 776–782. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Chiang, T.-H.; Chou, C.-K.; Tu, Y.-K.; Liao, W.-C.; Wu, M.-S.; Graham, D.Y. Association Between Helicobacter Pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-Analysis. Gastroenterology 2016, 150, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Takizawa, K.; Hirasawa, T.; Takeuchi, Y.; Ishido, K.; Hoteya, S.; Yano, T.; Tanaka, S.; Endo, M.; Nakagawa, M.; et al. Short-Term Outcomes of Multicenter Prospective Cohort Study of Gastric Endoscopic Resection: “Real-World Evidence” in Japan. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2019, 31, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Minami, S.; Gotoda, T.; Ono, H.; Oda, I.; Hamanaka, H. Complete Endoscopic Closure of Gastric Perforation Induced by Endoscopic Resection of Early Gastric Cancer Using Endoclips Can Prevent Surgery (with Video). Gastrointest. Endosc. 2006, 63, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Hatta, W.; Tsuji, Y.; Yoshio, T.; Kakushima, N.; Hoteya, S.; Doyama, H.; Nagami, Y.; Hikichi, T.; Kobayashi, M.; Morita, Y.; et al. Prediction Model of Bleeding after Endoscopic Submucosal Dissection for Early Gastric Cancer: BEST-J Score. Gut 2021, 70, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, Y.; Tsuji, Y.; Hirasawa, K.; Takimoto, K.; Wada, T.; Mochizuki, S.; Ohata, K.; Sakaguchi, Y.; Niimi, K.; Ono, S.; et al. Endoscopic Tissue Shielding to Prevent Bleeding after Endoscopic Submucosal Dissection: A Prospective Multicenter Randomized Controlled Trial. Endoscopy 2019, 51, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Akimoto, T.; Goto, O.; Sasaki, M.; Mizutani, M.; Tsutsumi, K.; Kiguchi, Y.; Takatori, Y.; Nakayama, A.; Kato, M.; Fujimoto, A.; et al. Endoscopic Hand Suturing for Mucosal Defect Closure after Gastric Endoscopic Submucosal Dissection May Reduce the Risk of Postoperative Bleeding in Patients Receiving Antithrombotic Therapy. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2022, 34, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Ono, H.; Hirasawa, T.; Takeuchi, Y.; Ishido, K.; Hoteya, S.; Yano, T.; Tanaka, S.; Toya, Y.; Nakagawa, M.; et al. Long-Term Survival After Endoscopic Resection For Gastric Cancer: Real-World Evidence From a Multicenter Prospective Cohort. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2023, 21, 307–318. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive Molecular Characterization of Gastric Adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, E.K.; Kim, Y.H.; Kim, J.-H.; Bae, Y.S.; Lee, Y.C.; Cheong, J.-H.; Noh, S.H.; Kim, H. Epstein-Barr Virus Positivity, Not Mismatch Repair-Deficiency, Is a Favorable Risk Factor for Lymph Node Metastasis in Submucosa-Invasive Early Gastric Cancer. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2016, 19, 1041–1051. [Google Scholar] [CrossRef] [PubMed]
- Ueyama, H.; Yao, T.; Nakashima, Y.; Hirakawa, K.; Oshiro, Y.; Hirahashi, M.; Iwashita, A.; Watanabe, S. Gastric Adenocarcinoma of Fundic Gland Type (Chief Cell Predominant Type): Proposal for a New Entity of Gastric Adenocarcinoma. Am. J. Surg. Pathol. 2010, 34, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Hiki, N.; Yamamoto, Y.; Fukunaga, T.; Yamaguchi, T.; Nunobe, S.; Tokunaga, M.; Miki, A.; Ohyama, S.; Seto, Y. Laparoscopic and Endoscopic Cooperative Surgery for Gastrointestinal Stromal Tumor Dissection. Surg. Endosc. 2008, 22, 1729–1735. [Google Scholar] [CrossRef]
- Goto, O.; Takeuchi, H.; Kawakubo, H.; Sasaki, M.; Matsuda, T.; Matsuda, S.; Kigasawa, Y.; Kadota, Y.; Fujimoto, A.; Ochiai, Y.; et al. First Case of Non-Exposed Endoscopic Wall-Inversion Surgery with Sentinel Node Basin Dissection for Early Gastric Cancer. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2015, 18, 434–439. [Google Scholar] [CrossRef]
- Takeuchi, H.; Goto, O.; Yahagi, N.; Kitagawa, Y. Function-Preserving Gastrectomy Based on the Sentinel Node Concept in Early Gastric Cancer. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2017, 20, 53–59. [Google Scholar] [CrossRef]
- Hirasawa, T.; Ikenoyama, Y.; Ishioka, M.; Namikawa, K.; Horiuchi, Y.; Nakashima, H.; Fujisaki, J. Current Status and Future Perspective of Artificial Intelligence Applications in Endoscopic Diagnosis and Management of Gastric Cancer. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2021, 33, 263–272. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujishiro, M. Advanced Diagnostic and Therapeutic Endoscopy for Early Gastric Cancer. Cancers 2024, 16, 1039. https://doi.org/10.3390/cancers16051039
Fujishiro M. Advanced Diagnostic and Therapeutic Endoscopy for Early Gastric Cancer. Cancers. 2024; 16(5):1039. https://doi.org/10.3390/cancers16051039
Chicago/Turabian StyleFujishiro, Mitsuhiro. 2024. "Advanced Diagnostic and Therapeutic Endoscopy for Early Gastric Cancer" Cancers 16, no. 5: 1039. https://doi.org/10.3390/cancers16051039
APA StyleFujishiro, M. (2024). Advanced Diagnostic and Therapeutic Endoscopy for Early Gastric Cancer. Cancers, 16(5), 1039. https://doi.org/10.3390/cancers16051039