

Psychosocial Burden of Women Who Are to Undergo Additional Diagnostic Procedures Due to Positive Screening for Cervical Cancer

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Study Population
2.2. Study Design
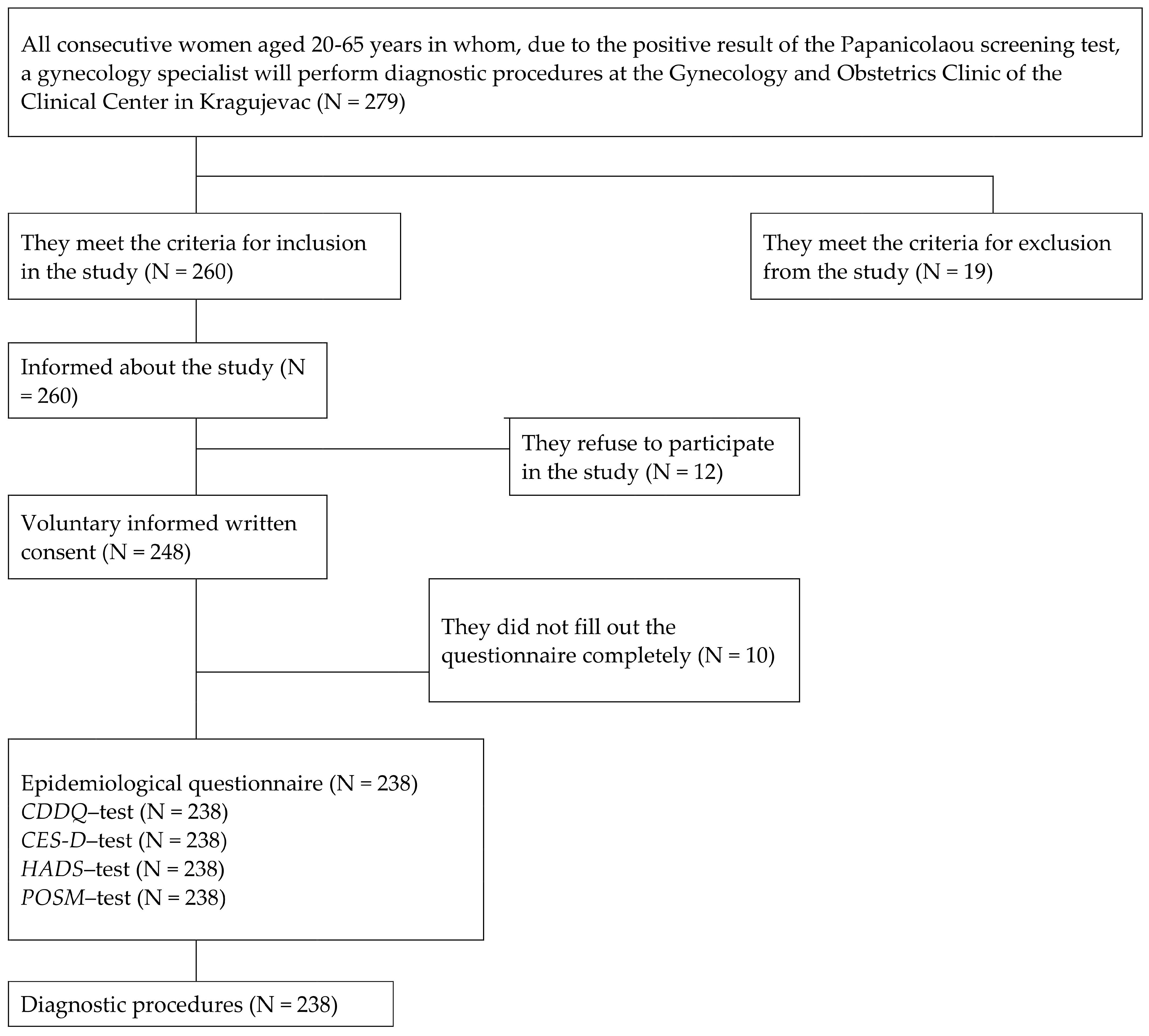
2.3. Study Sample
2.4. Sample Size Calculation
2.5. Data Collection
2.6. Instruments
2.7. Statistical Analyses
2.8. Ethical Considerations
3. Results
4. Discussion
4.1. Implications
4.2. The Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 2 June 2024).
- Singh, G.K.; Azuine, R.E.; Siahpush, M. Global inequalities in cervical cancer incidence and mortality are linked to deprivation, low socioeconomic status, and human development. Int. J. MCH AIDS 2012, 1, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Bolarinwa, O.A.; Holt, N. Barriers to breast and cervical cancer screening uptake among Black, Asian, and Minority Ethnic women in the United Kingdom: Evidence from a mixed-methods systematic review. BMC Health Serv. Res. 2023, 23, 390. [Google Scholar] [CrossRef] [PubMed]
- Ngune, I.; Kalembo, F.; Loessl, B.; Kivuti-Bitok, L.W. Biopsychosocial risk factors and knowledge of cervical cancer among young women: A case study from Kenya to inform HPV prevention in Sub-Saharan Africa. PLoS ONE 2020, 15, e0237745. [Google Scholar] [CrossRef] [PubMed]
- Znaor, A.; Ryzhov, A.; Losada, M.L.; Carvalho, A.; Smelov, V.; Barchuk, A.; Valkov, M.; Ten, E.; Andreasyan, D.; Zhizhilashvili, S.; et al. Breast and cervical cancer screening practices in nine countries of Eastern Europe and Central Asia: A population-based survey. J. Cancer Policy 2023, 38, 100436. [Google Scholar] [CrossRef]
- Lemp, J.M.; De Neve, J.-W.; Bussmann, H.; Chen, S.; Manne-Goehler, J.; Theilmann, M.; Marcus, M.-E.; Ebert, C.; Probst, C.; Tsabedze-Sibanyoni, L.; et al. Lifetime Prevalence of Cervical Cancer Screening in 55 Low- and Middle-Income Countries. JAMA 2020, 324, 1532–1542. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; CONCORD Working Group; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef]
- Chargari, C.; Arbyn, M.; Leary, A.; Abu-Rustum, N.; Basu, P.; Bray, F.; Chopra, S.; Nout, R.; Tanderup, K.; Viswanathan, A.; et al. Increasing global accessibility to high-level treatments for cervical cancers. Gynecol. Oncol. 2022, 164, 231–241. [Google Scholar] [CrossRef]
- Abdalla, E.; Troy, R.; Fall, S.; Elhussin, I.; Egiebor-Aiwan, O.; Nganwa, D. Racial differences in 5-year relative survival rates of cervical cancer by stage at diagnosis, between African American (black) and white women, living in the state of Alabama, USA. BMC Cancer 2020, 20, 830. [Google Scholar] [CrossRef]
- Institute for Public Health of Serbia “Dr. Milan Jovanović Batut”, Cancer Screening Office. Cervical Cancer Screening; Institute of Public Health of Serbia “Dr Milan Jovanović Batut”: Belgrade, Serbia, 2013; Available online: http://www.skriningsrbija.rs/srl/skrining-raka-grlica-materice/ (accessed on 2 June 2024).
- O’Connor, M.; Gallagher, P.; Waller, J.; Martin, C.; O’Leary, J.; Sharp, L.; Irish Cervical Screening Research Consortium (CERVIVA). Adverse psychological outcomes following colposcopy and related procedures: A systematic review. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 24–38. [Google Scholar] [CrossRef]
- Sharp, L.; Cotton, S.; Carsin, A.; Gray, N.; Thornton, A.; Cruickshank, M.; Little, J.; TOMBOLA Group. Factors associated with psychological distress following colposcopy among women with low-grade abnormal cervical cytology: A prospective study within the Trial Of Management of Borderline and Other Low grade Abnormal smears (TOMBOLA). Psychooncology 2013, 22, 368–380. [Google Scholar] [CrossRef]
- Korfage, I.; van Ballegooijen, M.; Wauben, B.; Looman, C.; Habbema, J.; Essink-Bot, M. Having a Pap smear, quality of life before and after cervical screening: A questionnaire study. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Hamdiui, N.; Marchena, E.; Stein, M.L.; van Steenbergen, J.E.; Crutzen, R.; van Keulen, H.M.; Reis, R.; Muijsenbergh, M.E.v.D.; Timen, A. Decision-making, barriers, and facilitators regarding cervical cancer screening participation among Turkish and Moroccan women in the Netherlands: A focus group study. Ethn. Health 2022, 27, 1147–1165. [Google Scholar] [CrossRef] [PubMed]
- Ilic, I.; Babic, G.; Dimitrijevic, A.; Grujicic, S.S.; Ilic, M.D. Depression before and after diagnostic procedures among women with abnormal finding of Papanicolaou screening test. Cancer Med. 2022, 11, 3518–3528. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, A.; Tapper, A.-M.; Leminen, A.; Sintonen, H.; Roine, R.P. Health-related quality of life and perception of anxiety in women with abnormal cervical cytology referred for colposcopy: An observational study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 387–391. [Google Scholar] [CrossRef]
- Aker, S.Ş.; Ağar, E.; Tinelli, A.; Hatirnaz, S.; Ortaç, F. The Impact of HPV Diagnosis and Abnormal Cervical Cytology Results on Sexual Dysfunction and Anxiety. Int. J. Environ. Res. Public Health 2023, 20, 3630. [Google Scholar] [CrossRef]
- Lofters, A.K.; Telner, D.; Kalia, S.; Slater, M. Association Between Adherence to Cancer Screening and Knowledge of Screening Guidelines: Feasibility Study Linking Self-Reported Survey Data with Medical Records. JMIR Cancer 2018, 4, e10529. [Google Scholar] [CrossRef]
- Hui, S.K.; Miller, S.M.; Wen, K.Y.; Fang, Z.; Li, T.; Buzaglo, J.; Hernandez, E. Psychosocial barriers to follow-up adherence after an abnormal cervical cytology test result among low-income, inner-city women. J. Prim. Care Community Health 2014, 5, 234–241. [Google Scholar] [CrossRef]
- Fish, L.J.; Moorman, P.G.; Wordlaw-Stintson, L.; Vidal, A.; Smith, J.S.; Hoyo, C. Factors Associated with Adherence to Follow-up Colposcopy. Am. J. Health Educ. 2013, 44, 293–298. [Google Scholar] [CrossRef]
- Orbell, S.; Hagger, M.; Brown, V.; Tidy, J. Appraisal theory and emotional sequelae of first visit to colposcopy following an abnormal cervical screening result. Br. J. Health Psychol. 2004, 9, 533–555. [Google Scholar] [CrossRef]
- Sharp, L.; Cotton, S.; Cruickshank, M.; Gray, N.; Smart, L.; Whynes, D.; Little, J.; TOMBOLA Group. Impact of post-colposcopy management on women’s long-term worries: Results from the UK population-based TOMBOLA trial. J. Fam. Plan. Reprod. Health Care 2016, 42, 43–51. [Google Scholar] [CrossRef]
- Gray, N.M.; Sharp, L.; Cotton, S.C.; Avis, M.; Philips, Z.; Russell, I.; Walker, L.G.; Whynes, D.; Little, J.; TOMBOLA Group. Developing a questionnaire to measure the psychosocial impact of an abnormal cervical smear result and its subsequent management: The TOMBOLA (Trial of Management of Borderline and Other Low-grade Abnormal smears) trial. Qual. Life Res. 2005, 14, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Shinn, E.; Basen-Engquist, K.; Le, T.; Hansis-Diarte, A.; Bostic, D.; Martinez-Cross, J.; Santos, A.; Follen, M. Distress after an abnormal Pap smear result: Scale development and psychometric validation. Prev. Med. 2004, 39, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Rothnie, K.; Cotton, S.C.; Fielding, S.; Gray, N.M.; Little, J.; Cruickshank, M.E.; Walker, L.G.; Avis, M.; Sharp, L.; TOMBOLA Group. Measuring the psychosocial burden in women with low-grade abnormal cervical cytology in the TOMBOLA trial: Psychometric properties of the Process and Outcome Specific Measure (POSM). Health Qual. Life Outcomes 2014, 12, 154. [Google Scholar] [CrossRef]
- Ilic, I. Assessment of Anxiety and Depression in Women with Positive Papanicolaou Screening Test before and after Diagnostic Procedures. Ph.D. Thesis, University of Kragujevac, Kragujevac, Serbia, 2019. Available online: https://nardus.mpn.gov.rs/handle/123456789/12014?show=full&locale-attribute=sr_RS (accessed on 2 April 2022).
- Ilic, I.; Babic, G.; Dimitrijevic, A.; Ilic, M.; Sipetic Grujicic, S. Psychological distress among women with abnormal pap smear results in Serbia: Validity and reliability of the Cervical Dysplasia Distress Questionnaire. PLoS ONE 2019, 14, e0218070. [Google Scholar] [CrossRef]
- Ilic, I.; Babic, G.; Dimitrijevic, A.; Ilic, M.; Sipetic Grujicic, S. Internal consistency and validity of the Hospital Anxiety and Depression Scale (HADS) in women with abnormal Pap smear in Serbia. Women Health 2021, 61, 363–371. [Google Scholar] [CrossRef]
- Ilic, I.; Babic, G.; Dimitrijevic, A.; Ilic, M.; Sipetic Grujicic, S. Reliability and validity of the Center for Epidemiologic Studies Depression (CES-D) scale in Serbian women with abnormal Papanicolaou smear results. Int. J. Gynecol. Cancer 2019, 29, 996–1002. [Google Scholar] [CrossRef]
- Sawadogo, B.; Sheba, G.N.; Rutebemberwa, E.; Sawadogo, M.; Meda, N. Knowledge and beliefs on cervical cancer and practices on cervical cancer screening among women aged 20 to 50 years in Ouagadougou, Burkina Faso, 2012: A cross-sectional study. Pan. Afr. Med. J. 2014, 18, 175. [Google Scholar] [CrossRef]
- Harder, E.; Juul, K.E.; Jensen, S.M.; Thomsen, L.T.; Frederiksen, K.; Kjaer, S.K. Factors associated with non-participation in cervical cancer screening—A nationwide study of nearly half a million women in Denmark. Prev. Med. 2018, 111, 94–100. [Google Scholar] [CrossRef]
- Ministry of Health, Republic of Serbia. National Health Survey, Serbia 2013; Ministry of Health, Republic of Serbia: Belgrade, Serbia, 2014. [Google Scholar]
- O’Connor, M.; O’Leary, E.; Waller, J.; Gallagher, P.; D’Arcy, T.; Flannelly, G.; Martin, C.M.; McRae, J.; Prendiville, W.; Irish Cervical Screening Research Consortium (CERVIVA); et al. Trends in, and predictors of, anxiety and specific worries following colposcopy: A 12-month longitudinal study. Psychooncology 2016, 25, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Rask, M.; Swahnberg, K.; Oscarsson, M. Swedish women’s awareness of human papillomavirus, and health-related quality of life, anxiety, and depression after a notification of an abnormal Pap smear result: A cross-sectional study. Eur. J. Cancer Prev. 2019, 28, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Han, H.R. Potential links between health literacy and cervical cancer screening behaviors: A systematic review. Psychooncology 2016, 25, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Momberg, M.; Botha, M.H.; Van der Merwe, F.H.; Moodley, J. Women’s experiences with cervical cancer screening in a colposcopy referral clinic in Cape Town, South Africa: A qualitative analysis. BMJ Open 2017, 7, e013914. [Google Scholar] [CrossRef]
- Jentschke, M.; Lehmann, R.; Drews, N.; Hansel, A.; Schmitz, M.; Hillemanns, P. Psychological distress in cervical cancer screening: Results from a German online survey. Arch. Gynecol. Obstet. 2020, 302, 699–705. [Google Scholar] [CrossRef]
- Kola, S.; Walsh, J.C. Determinants of pre-procedural state anxiety and negative affect in first-time colposcopy patients: Implications for intervention. Eur. J. Cancer Care 2012, 21, 469–476. [Google Scholar] [CrossRef]
- Drolet, M.; Brisson, M.; Maunsell, E.; Franco, E.L.; Coutlée, F.; Ferenczy, A.; Fisher, W.; Mansi, J.A. The psychosocial impact of an abnormal cervical smear result. Psychooncology 2012, 21, 1071–1081. [Google Scholar] [CrossRef]
- Wang, X.; Wang, S.; Yang, D.; Chu, Y.; Hao, Y.; Dai, H. Associations among resilience, hope, social support, stress, and anxiety severity in Chinese women with abnormal cervical cancer screening results. Heliyon 2022, 8, e12539. [Google Scholar] [CrossRef]
- Vasic, P. Childbirth postponement and age-related infertility in Serbia. Facta Univ. Ser. Philos. Sociol. Psychol. Hist. 2021, 20, 97–111. [Google Scholar] [CrossRef]
- Scherer-Quenzer, A.C.; Herbert, S.-L.; Schlaiss, T.; Wöckel, A.; Diessner, J.; Grunz, J.-P.; Findeis, J.; Kiesel, M. Assessment of psychological distress in patients with cervical dysplasia according to age, education, information acquisition and information level. Arch. Gynecol. Obstet. 2024, 1–9. [Google Scholar] [CrossRef]
- Sansoni, M.; Tagai, E.K.; Lapitan, E.; Wen, K.-Y.; Xu, J.; Belfiglio, A.; Hudson, S.V.; Kohler, R.E.; Hernandez, E.; Miller, S.M. Development of a text message-based intervention for follow-up colposcopy among predominately underserved Black and Hispanic/Latinx women. Cancer Causes Control 2022, 33, 861–873. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Mean ± SD, Min–Max |
|---|---|
| Age (years) | 46.2 ± 10.5, 23–65 |
| Total number of years of schooling | 11.7 ± 2.6, 4–20 |
| Menarche age | 13.3 ± 1.7, 9–18 |
| Age of menopause | 49.4 ± 4.2, 38–58 |
| Duration of menopause | 6.7 ± 5.6, 1–25 |
| Age at first pregnancy | 23.7 ± 4.3, 16–41 |
| Body mass index | 24.3 ± 4.2, 15.4–38.9 |
| POSM subscales | Mean ± SD (Range), Min–Max |
| 43.56 ± 11.94 (1–100), 15.87–72.22 |
| 45.62 ± 14.04 (1–100), 16.67–87.50 |
| Variables | β (95%CI) | p |
|---|---|---|
| Age | 0.032 (−0.767; 1.415) | 0.559 |
| Place of residence (Urban) | −0.025 (−3.521; 2.197) | 0.649 |
| Educational level (Faculty) | −0.025 (−3.793; 2.366) | 0.649 |
| Occupation (Professional) | −0.128 (−2.116; −0.201) | 0.018 * |
| Marital status (With partner) | 0.083 (−0.694; 5.713) | 0.124 |
| Pregnancy (Ever) | −0.033 (−4.970; 2.605) | 0.540 |
| Children (Yes) | −0.007 (−3.724; 3.235) | 0.890 |
| Menopause (Yes) | −0.006 (−2.733; 2.445) | 0.913 |
| Oral contraceptive use (Ever) | −0.132 (−7.774; 0.876) | 0.014 * |
| Abortion history (Yes) | 0.029 (−2.222; 3.711) | 0.622 |
| Tobacco use (Ever) | 0.016 (−2.183; 2.930) | 0.774 |
| Alcohol use (Ever) | 0.112 (0.118; 6.817) | 0.038 * |
| Body Mass Index (≥25 kg/m2) | 0.069 (−0.894; 4.271) | 0.199 |
| Family history of cervical cancer (Yes) | 0.015 (−3.625; 4.856) | 0.775 |
| Consequences of the screening procedure (Papanicolaou test) | ||
| Pain | 0.022 (−3.439; 5.274) | 0.679 |
| Bleeding | 0.052 (−1.767; 5.183) | 0.334 |
| Discharge | 0.011 (0.150; 6.468) | 0.040 * |
| Psychological distress by CDDQ scale | 0.243 (3.189; 7.902) | <0.001 *,** |
| CDDQ subscales | ||
| Tension and discomfort | 0.157 (1.005; 5.102) | 0.004 * |
| Embarrassment | 0.151 (0.591; 3.304) | 0.005 * |
| Sexual and reproductive consequences | 0.198 (1.813; 5.854) | <0.001 *,** |
| Health consequences | 0.171 (0.903; 3.761) | 0.001 *,** |
| HADS—Anxiety score (8–21 points) | 0.298 (0.552; 1.123) | <0.001 *,** |
| HADS—Depression score (8–21 points) | 0.285 (0.552; 1.102) | <0.001 *,** |
| CES-D-High burden of depressive symptoms (≥16 points) | 0.284 (0.232; 0.491) | <0.001 *,** |
| CESD subscales | ||
| Somatic complaints | 0.347 (0.029; 0.068) | <0.001 *,** |
| Positive affect | 0.076 (−0.109; 0.667) | 0.159 |
| Depressed affect | 0.226 (0.332; 0.891) | <0.001 *,** |
| Interpersonal relationship | 0.146 (0.410; 2.528) | 0.007 * |
| Knowledge of the meaning of the term dysplasia/precancerous | −0.205 (−7.524; −2.456) | <0.001 *,** |
| Mode of obtaining notification of abnormal Papanicolaou result | −0.014 (−1.064; 0.815) | 0.795 |
| Variables | β (95%CI) | p |
|---|---|---|
| Age | 0.032 (−0.894; 1.673) | 0.551 |
| Place of residence (Urban) | 0.049 (−1.803; 4.918) | 0.363 |
| Educational level (Faculty) | −0.054 (−5.476; 1.763) | 0.314 |
| Occupation (Professional) | 0.044 (−0.667; 1.603) | 0.418 |
| Marital status (With partner) | 0.028 (−2.801; 4.761) | 0.610 |
| Pregnancy (Ever) | −0.051 (−6.592; 2.315) | 0.346 |
| Children (Yes) | −0.027 (−5.115; 3.070) | 0.623 |
| Menopause (Yes) | −0.005 (−3.192; 2.900) | 0.925 |
| Oral contraceptive use (Ever) | 0.026 (−3.103; 5.082) | 0.635 |
| Abortion history (Yes) | −0.119 (−7.381; −0.181) | 0.040 * |
| Tobacco use (Ever) | −0.035 (−3.892; 2.030) | 0.524 |
| Alcohol use (Ever) | −0.029 (−5.005; 2.841) | 0.588 |
| Body Mass Index (≥25 kg/m2) | 0.052 (−1.567; 4.517) | 0.341 |
| Family history of cervical cancer (Yes) | 0.092 (−0.649; 9.290) | 0.088 |
| Consequences of the screening procedure (Papanicolaou test) | ||
| Pain | 0.023 (−4.024; 6.277) | 0.673 |
| Bleeding | 0.073 (−1.262; 6.904) | 0.175 |
| Discharge | −0.053 (−5.601; 1.868) | 0.326 |
| Psychological distress by CDDQ scale | −0.273 (−10.077; −4.578) | <0.001 *,** |
| CDDQ subscales | ||
| Tension and discomfort | −0.172 (−6.361; −1.554) | 0.001 *,** |
| Embarrassment | 0.003 (−1.574; 1.654) | 0.961 |
| Sexual and reproductive consequences | −0.220 (−7.373; −2.641) | <0.001 *,** |
| Health consequences | −0.379 (−7.664; −4.505) | <0.001 *,** |
| HADS—Anxiety score (8–21 points) | −0.199 (−1.003; −0.314) | <0.001 *,** |
| HADS—Depression score (8–21 points) | −0.136 (−0.808; −0.102) | 0.012 * |
| CES-D-High burden of depressive symptoms (≥16 points) | −0.137 (−0.363; −0.048) | 0.011 * |
| CESD subscales | ||
| Somatic complaints | −0.088 (−0.706; 0.066) | 0.101 |
| Positive affect | −0.102 (−0.896; 0.016) | 0.058 |
| Depressed affect | −0.127 (−0.738; −0.068) | 0.018 * |
| Interpersonal relationship | −0.003 (−1.301; 1.218) | 0.949 |
| Knowledge of the meaning of the term dysplasia/precancerous | 0.087 (−0.546; 5.523) | 0.108 |
| Mode of obtaining notification of abnormal Papanicolaou result | 0.051 (−0.573; 1.636) | 0.344 |
| Worry | Satisfaction with Information/Support | |||
|---|---|---|---|---|
| Variables † | β (95%CI) | p | β (95%CI) | p |
| Oral contraceptive use (Ever) | −0.174 (−8.857; −2.514) | <0.001 *,** | ||
| Alcohol use (Ever) | 0.188 (2.863; 8.949) | <0.001 *,** | ||
| Psychological distress by CDDQ scale | −0.210 (−8.859; −2.494) | 0.001 *,** | ||
| HADS—Anxiety score (8–21 points) | 0.189 (0.227; 0.838) | 0.001 *,** | ||
| CES-D—High burden of depressive symptoms (≥16 points) | 0.191 (0.103; 0.383) | 0.001 *,** | ||
| Knowledge of the meaning of the term dysplasia/precancerous | −0.187 (−6.916; −2.198) | <0.001 *,** | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilic, I.; Babic, G.; Dimitrijevic, A.; Sipetic Grujicic, S.; Jakovljevic, V.; Ilic, M. Psychosocial Burden of Women Who Are to Undergo Additional Diagnostic Procedures Due to Positive Screening for Cervical Cancer. Cancers 2024, 16, 3541. https://doi.org/10.3390/cancers16203541
Ilic I, Babic G, Dimitrijevic A, Sipetic Grujicic S, Jakovljevic V, Ilic M. Psychosocial Burden of Women Who Are to Undergo Additional Diagnostic Procedures Due to Positive Screening for Cervical Cancer. Cancers. 2024; 16(20):3541. https://doi.org/10.3390/cancers16203541
Chicago/Turabian StyleIlic, Irena, Goran Babic, Aleksandra Dimitrijevic, Sandra Sipetic Grujicic, Vladimir Jakovljevic, and Milena Ilic. 2024. "Psychosocial Burden of Women Who Are to Undergo Additional Diagnostic Procedures Due to Positive Screening for Cervical Cancer" Cancers 16, no. 20: 3541. https://doi.org/10.3390/cancers16203541
APA StyleIlic, I., Babic, G., Dimitrijevic, A., Sipetic Grujicic, S., Jakovljevic, V., & Ilic, M. (2024). Psychosocial Burden of Women Who Are to Undergo Additional Diagnostic Procedures Due to Positive Screening for Cervical Cancer. Cancers, 16(20), 3541. https://doi.org/10.3390/cancers16203541