
Multiparametric Approach to the Colorectal Cancer Phenotypes Integrating Morphofunctional Assessment and Computer Tomography
 , , , , , ,
, , , , , ,
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Anthropometric and Morphofunctional Assessment
2.2.1. BIVA
2.2.2. Nutritional Ultrasound
2.2.3. Functional Assessment
2.2.4. CT FocusedOn®
2.3. Assessment of Sarcopenia and Low Muscle Mass
2.4. Statistical Analyses
3. Results
3.1. Body Composition Parameters and Functional Status: BIVA, NU, HGS, and CT
3.2. Comparison with Reference Value of Sarcopenia
3.3. Correlation Analysis between Muscle Measures: CT, BIVA, NU, and Functional Test (HGS)
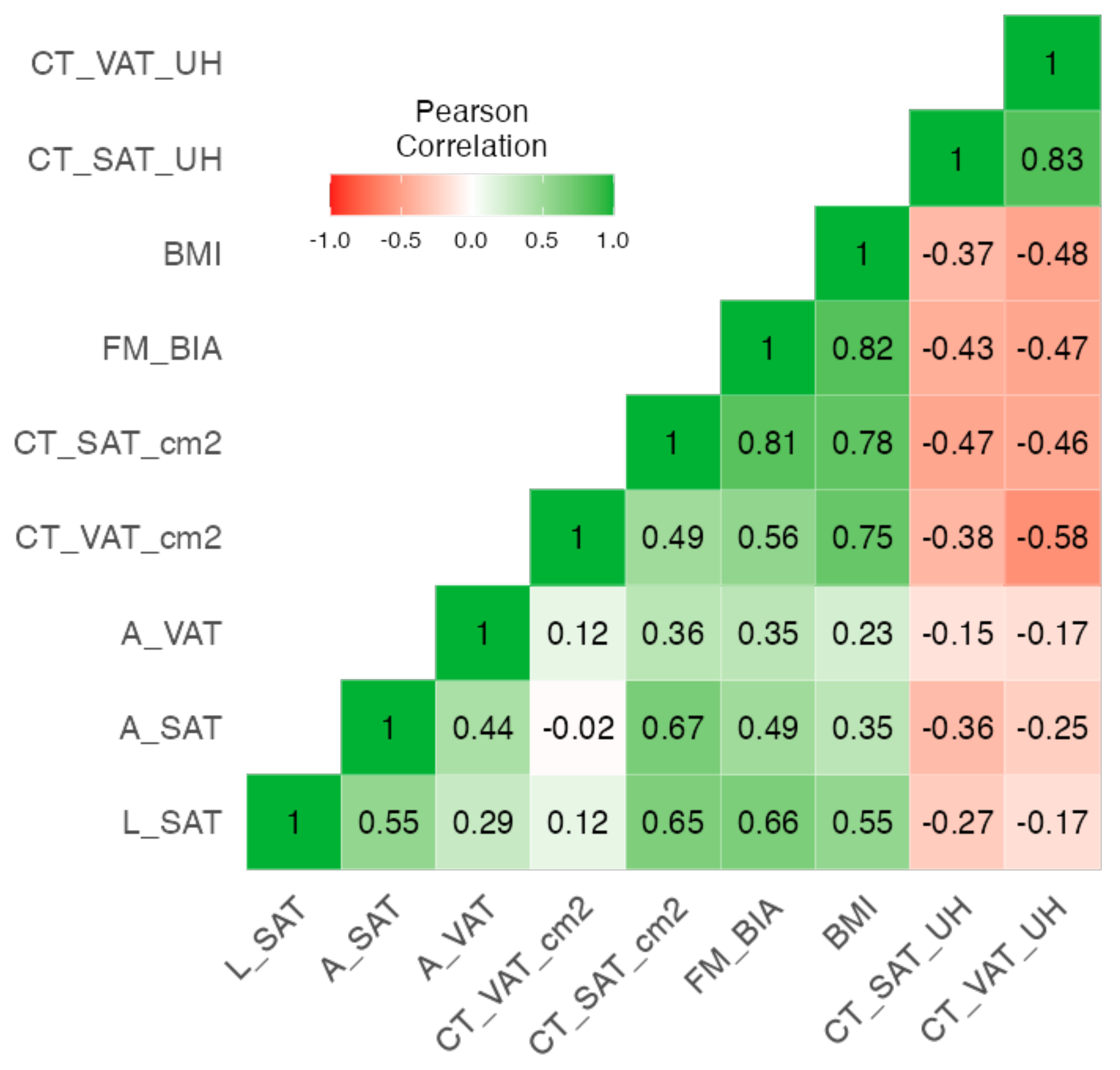
3.4. Correlation Analysis between Adipose Measures: CT, BIVA, and NU
3.5. Regression Model Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aran, V.; Victorino, A.P.; Thuler, L.C.; Ferreira, C.G. Colorectal Cancer: Epidemiology, Disease Mechanisms and Interventions to Reduce Onset and Mortality. Clin. Color. Cancer 2016, 15, 195–203. [Google Scholar]
- Kocarnik, J.M.; Hua, X.; Hardikar, S.; Robinson, J.; Lindor, N.M.; Win, A.K.; Hopper, J.L.; Figueiredo, J.C.; Potter, J.D.; Campbell, P.T.; et al. Long-term weight loss after colorectal cancer diagnosis is associated with lower survival: The Colon Cancer Family Registry. Cancer 2017, 123, 4701–4708. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar]
- Cederholm, T.; Jensen, G.; Correia, M.; Gonzalez, M.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar]
- Miller, J.; Wells, L.; Nwulu, U.; Currow, D.; Johnson, M.J.; Skipworth, R.J.E. Validated screening tools for the assessment of cachexia, sarcopenia, and malnutrition: A systematic review. Am. J. Clin. Nutr. 2018, 108, 1196–1208. [Google Scholar]
- Piccoli, A.; Nigrelli, S.; Caberlotto, A.; Bottazzo, S.; Rossi, B.; Pillon, L.; Maggiore, Q. Bivariate normal values of the bioelectrical impedance vector in adult and elderly populations. Am. J. Clin. Nutr. 1995, 61, 269–270. [Google Scholar] [CrossRef]
- Garlini, L.M.; Alves, F.D.; Ceretta, L.B.; Perry, I.S.; Souza, G.C.; Clausell, N.O. Phase angle and mortality: A systematic review. Eur. J. Clin. Nutr. 2019, 73, 495–508. [Google Scholar]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; García-Almeida, J.M.; Bellido-Guerrero, D.; Talluri, A.; Lukaski, H.; Tinahones, F.J. Phase angle and standardized phase angle from bioelectrical impedance measurements as a prognostic factor for mortality at 90 days in patients with COVID-19: A longitudinal cohort study. Clin. Nutr. 2022, 41, 3106–3114. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7886631/ (accessed on 28 October 2021).
- Grundmann, O.; Yoon, S.L.; Williams, J.J. The value of bioelectrical impedance analysis and phase angle in the evaluation of malnutrition and quality of life in cancer patients—A comprehensive review. Eur. J. Clin. Nutr. 2015, 69, 1290–1297. [Google Scholar]
- Paiva, S.I.; Borges, L.R.; Halpern-Silveira, D.; Assunção, M.C.F.; Barros, A.J.D.; Gonzalez, M.C. Standardized phase angle from bioelectrical impedance analysis as prognostic factor for survival in patients with cancer. Support. Care Cancer 2011, 19, 187–192. [Google Scholar]
- Sánchez-Torralvo, F.J.; González-Poveda, I.; García-Olivares, M.; Porras, N.; Gonzalo-Marín, M.; Tapia, M.J.; Mera-Velasco, S.; Toval-Mata, J.A.; Ruiz-López, M.; Carrasco-Campos, J.; et al. Poor Physical Performance Is Associated with Postoperative Complications and Mortality in Preoperative Patients with Colorectal Cancer. Nutrients 2022, 14, 1484. [Google Scholar] [CrossRef] [PubMed]
- Vegas-Aguilar, I.M.; Guirado-Peláez, P.; Fernández-Jiménez, R.; Boughanem, H.; Tinahones, F.J.; Garcia-Almeida, J.M. Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer. Cancers 2023, 15, 847. [Google Scholar] [CrossRef] [PubMed]
- Golder, A.M.; Sin, L.K.E.; Alani, F.; Alasadi, A.; Dolan, R.; Mansouri, D.; Horgan, P.G.; McMillan, D.C.; Roxburgh, C.S. The relationship between the mode of presentation, CT-derived body composition, systemic inflammatory grade and survival in colon cancer. J. Cachexia Sarcopenia Muscle 2022, 13, 2863–2874. [Google Scholar] [CrossRef]
- García-Almeida, J.M.; García-García, C.; Vegas-Aguilar, I.M.; Ballesteros Pomar, M.D.; Cornejo-Pareja, I.M.; Fernández Medina, B.; de Luis Román, D.A.; Bellido Guerrero, D.; Bretón Lesmes, I.; Tinahones Madueño, F.J. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinol. Diabetes Nutr. 2023, 70, 74–84. Available online: https://www.sciencedirect.com/science/article/pii/S2530016422001471 (accessed on 28 October 2021).
- Deng, M.; Yan, L.; Tong, R.; Zhao, J.; Li, Y.; Yin, Y.; Zhang, Q.; Gao, J.; Wang, Q.; Hou, G.; et al. Ultrasound Assessment of the Rectus Femoris in Patients with Chronic Obstructive Pulmonary Disease Predicts Sarcopenia. Int. J. Chron. Obstruct. Pulmon. Dis. 2022, 17, 2801–2810. [Google Scholar] [CrossRef]
- Sánchez-Torralvo, F.J.; Porras, N.; Ruiz-García, I.; Maldonado-Araque, C.; García-Olivares, M.; Girón, M.V.; Gonzalo-Marín, M.; Olveira, C.; Olveira, G. Usefulness of Muscle Ultrasonography in the Nutritional Assessment of Adult Patients with Cystic Fibrosis. Nutrients 2022, 14, 3377. [Google Scholar] [CrossRef]
- Fernández-Jiménez, R.; Cabrera Cesar, E.; Sánchez García, A.; Espíldora Hernández, F.; Vegas-Aguilar, I.M.; Amaya-Campos, M.D.M.; Cornejo-Pareja, I.; Guirado-Peláez, P.; Simón-Frapolli, V.; Murri, M.; et al. Rectus Femoris Cross-Sectional Area and Phase Angle asPredictors of 12-Month Mortality in Idiopathic Pulmonary Fibrosis Patients. Nutrients 2023, 15, 4473. [Google Scholar] [CrossRef]
- Simón-Frapolli, V.J.; Vegas-Aguilar, I.M.; Fernández-Jiménez, R.; Cornejo-Pareja, I.M.; Sánchez-García, A.M.; Martínez-López, P.; Nuevo-Ortega, P.; Reina-Artacho, C.; Estecha-Foncea, M.A.; Gómez-González, A.M.; et al. Phase angle and rectus femoris cross-sectional area as predictors of severe malnutrition and their relationship with complications in outpatients with post-critical SARS-CoV2 disease. Front. Nutr. 2023, 10, 1218266. [Google Scholar] [CrossRef]
- Nakanishi, R.; Oki, E.; Sasaki, S.; Hirose, K.; Jogo, T.; Edahiro, K.; Korehisa, S.; Taniguchi, D.; Kudo, K.; Kurashige, J.; et al. Sarcopenia is an independent predictor of complications after colorectal cancer surgery. Surg. Today 2018, 48, 151–157. [Google Scholar] [CrossRef]
- Cornejo-Pareja, I.; Soler-Beunza, A.G.; Vegas-Aguilar, I.M.; Fernández-Jiménez, R.; Tinahones, F.J.; García-Almeida, J.M. Predictors of Sarcopenia in Outpatients with Post-Critical SARS-CoV2 Disease. Nutritional Ultrasound of Rectus Femoris Muscle, a Potential Tool. Nutrients 2022, 14, 4988. [Google Scholar] [CrossRef]
- Piccoli, A.; Pastori, G. BIVA software; Department of Medical and Surgical Sciences, University of Padova: Padova, Italy, 2002. [Google Scholar]
- de Luis Roman, D.; García Almeida, J.M.; Bellido Guerrero, D.; Guzmán Rolo, G.; Martín, A.; Primo Martín, D.; García-Delgado, Y.; Guirado-Peláez, P.; Palmas, F.; Tejera Pérez, C.; et al. Ultrasound Cut-Off Values for Rectus Femoris for Detecting Sarcopenia in Patients with Nutritional Risk. Nutrients 2024, 16, 1552. [Google Scholar] [CrossRef] [PubMed]
- Campa, F.; Coratella, G.; Cerullo, G.; Stagi, S.; Paoli, S.; Marini, S.; Grigoletto, A.; Moroni, A.; Petri, C.; Andreoli, A.; et al. New bioelectrical impedance vector references and phase angle centile curves in 4367 adults: The need for an urgent update after 30 years. Clin. Nutr. 2023, 42, 1749–1758. [Google Scholar] [CrossRef] [PubMed]
- Aubrey, J.; Esfandiari, N.; Baracos, V.E.; Buteau, F.A.; Frenette, J.; Putman, C.T.; Mazurak, V.C. Measurement of skeletal muscle radiation attenuation and basis of its biological variation. Acta Physiol. 2014, 210, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Palmas, F.; Ciudin, A.; Guerra, R.; Eiroa, D.; Espinet, C.; Roson, N.; Burgos, R.; Simó, R. Comparison of computed tomography and dual-energy X-ray absorptiometry in the evaluation of body composition in patients with obesity. Front. Endocrinol. 2023, 14, 1161116. [Google Scholar] [CrossRef]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St-Onge, M.-P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef]
- Prado, C.M.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Caan, B.J.; Meyerhardt, J.A.; Kroenke, C.H.; Alexeeff, S.; Xiao, J.; Weltzien, E.; Feliciano, E.C.; Castillo, A.L.; Quesenberry, C.P.; Kwan, M.L.; et al. Explaining the Obesity Paradox: The Association between Body Composition and Colorectal Cancer Survival (C-SCANS Study). Cancer Epidemiol. Biomarkers Prev. 2017, 26, 1008–1015. [Google Scholar] [CrossRef]
- Dolan, R.D.; Almasaudi, A.S.; Dieu, L.B.; Horgan, P.G.; McSorley, S.T.; McMillan, D.C. The relationship between computed tomography-derived body composition, systemic inflammatory response, and survival in patients undergoing surgery for colorectal cancer. J. Cachexia Sarcopenia Muscle 2019, 10, 111–122. [Google Scholar] [CrossRef]
- Martin, D.; Maeder, Y.; Kobayashi, K.; Schneider, M.; Koerfer, J.; Melloul, E.; Halkic, N.; Hübner, M.; Demartines, N.; Becce, F.; et al. Association between CT-Based Preoperative Sarcopenia and Outcomes in Patients That Underwent Liver Resections. Cancers 2022, 14, 261. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Kyle, U.G.; Kondrup, J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: Phase angle and impedance ratio. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 330–339. [Google Scholar] [CrossRef]
- Tewari, N.; Awad, S.; Macdonald, I.A.; Lobo, D.N. A comparison of three methods to assess body composition. Nutrition 2018, 47, 1–5. [Google Scholar] [CrossRef] [PubMed]
- da Silva, B.R.; Orsso, C.E.; Gonzalez, M.C.; Sicchieri, J.M.F.; Mialich, M.S.; Jordao, A.A.; Prado, C.M. Phase angle and cellular health: Inflammation and oxidative damage. Rev. Endocr. Metab. Disord. 2022, 24, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Prior-Sánchez, I.; Herrera-Martínez, A.D.; Zarco-Martín, M.T.; Fernández-Jiménez, R.; Gonzalo-Marín, M.; Muñoz-Garach, A.; Vilchez-López, F.J.; Cayón-Blanco, M.; Villarrubia-Pozo, A.; Muñoz-Jiménez, C.; et al. Prognostic value of bioelectrical impedance analysis in head and neck cancer patients undergoing radiotherapy: A VALOR® study. Front. Nutr. 2024, 11, 1335052. [Google Scholar] [CrossRef] [PubMed]
- Sugizaki, C.S.A.; Queiroz, N.P.; Silva, D.M.; Freitas, A.T.V.S.; Costa, N.A.; Peixoto, M.R.G. Comparison of Bioelectrical Impedance Vector Analysis (BIVA) to 7-point Subjective Global Assessment for the diagnosis of malnutrition. J. Bras. Nefrol. 2022, 44, 171–178. [Google Scholar] [CrossRef]
- Castillo-Martínez, L.; Colín-Ramírez, E.; Orea-Tejeda, A.; González Islas, D.G.; Rodríguez García, W.D.; Santillán Díaz, C.; Gutiérrez Rodríguez, A.E.; Vázquez Durán, M.; Keirns Davies, C. Cachexia assessed by bioimpedance vector analysis as a prognostic indicator in chronic stable heart failure patients. Nutrition 2012, 28, 886–891. [Google Scholar] [CrossRef]
- Espinosa-Cuevas, Á.; Ch-Durán, L.-X.; Carsi, X.A.; González-Ortiz, A.; Ramos-Acevedo, S.; López-Cisneros, S.; Correa Rotter, R.; Miranda Alatriste, P.V. Agreement between vector analysis and body composition measurements by four types of bioelectrical impedance technology in hemodialysis patients. Nutr. Hosp. 2022, 39, 1047–1057. [Google Scholar]
- Lee, C.M.; Kang, J. Prognostic impact of myosteatosis in patients with colorectal cancer: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1270–1282. [Google Scholar] [CrossRef]
- Mortellaro, S.; Triggiani, S.; Mascaretti, F.; Galloni, M.; Garrone, O.; Carrafiello, G.; Ghidini, M. Quantitative and Qualitative Radiological Assessment of Sarcopenia and Cachexia in Cancer Patients: A Systematic Review. J. Pers. Med. 2024, 14, 243. [Google Scholar] [CrossRef]
- Ji, W.; Liu, X.; Zhang, Y.; Zhao, Y.; He, Y.; Cui, J.; Li, W. Development of Formulas for Calculating L3 Skeletal Muscle Mass Index and Visceral Fat Area Based on Anthropometric Parameters. Front. Nutr. 2022, 9, 910771. [Google Scholar] [CrossRef]
- Tolonen, A.; Pakarinen, T.; Sassi, A.; Kyttä, J.; Cancino, W.; Rinta-Kiikka, I.; Pertuz, S.; Arponen, O. Methodology, clinical applications, and future directions of body composition analysis using computed tomography (CT) images: A review. Eur. J. Radiol. 2021, 145, 109943. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Male | Female | p-Value | |
|---|---|---|---|---|
| N = 267 | N = 165 | N = 102 | ||
| Age (years) | 68.2 ± 10.9 | 68.3 ± 11.4 | 68.1 ± 9.97 | 0.87 |
| Gender | 165 (61.8%) | 102 (38.2%) | ||
| BMI (kg/m2) | 26.8 ± 4.93 | 26.5 ± 4.30 | 27.3 ± 5.80 | 0.28 |
| Malnutrition GLIM criteria Type of cancer | 99 (37.1%) | 61 (22.8%) | 38 (14.2%) | 0.96 |
| Colon | 215 (80.5%) | 131 (49.1%) | 84 (31.5%) | |
| Rectum | 52(19.5%) | 34 (12.7%) | 18 (6.7%) | |
| Stage | ||||
| Unknown at valuation | 15 (5.6%) | 8 (3.0%) | 7 (2.6%) | 0.57 |
| I | 62 (23.2%) | 37 (13.9%) | 25 (9.4%) | |
| II | 84 (31.5%) | 56 (21.0%) | 28 (10.5%) | |
| III | 91 (34.1%) | 54 (20.2%) | 37 (13.9%) | |
| IV | 15 (5.6%) | 10 (3.7%) | 5 (1.9%) | |
| Type of surgery | 0.57 | |||
| Open | 13 (4.9%) | 9 (3.4%) | 4 (1.5%) | |
| Laparoscopic | 254 (95.1%) | 156 (58.4%) | 98 (36.7%) | |
| Outcomes | ||||
| Days of admission | 7.32 ± 6.43 | 8.02 ± 7.48 | 6.19 ± 3.99 | 0.02 * |
| Éxitus | 23 (8.6%) | 17 (6.4%) | 6 (2.2%) | 0.21 |
| Immediate Complication | 65 (24.3%) | 43 (15.7%) | 23 (8.6%) | 0.59 |
| Male (n = 165) | Female (n = 102) | p-Value | |
|---|---|---|---|
| BIVA Raw Bioelectrical data | |||
| Rz | 439 ± 77.1 | 483 ± 89.1 | <0.001 |
| Xc | 43.9 ± 10.7 | 43.9 ± 10.5 | 0.955 |
| Phase angle (°) | 5.71 ± 1.15 | 5.20 ± 0.927 | <0.001 |
| BCM (kg) | 34.4 ± 6.68 | 25.9 ± 5.06 | <0.001 |
| Validate BIVA equation | |||
| FFM (kg) | 59.8 ± 9.07 | 45.4 ± 7.29 | <0.001 |
| FFMI (kg/m2) | 20.6 ± 2.81 | 18.0 ± 2.34 | <0.001 |
| FM (kg) | 18.8 ± 9.12 | 20.9 ± 9.24 | 0.080 |
| FM (%) | 24.4 ± 11.3 | 30.3 ± 10.9 | <0.001 |
| ASMM (kg) | 22.8 ± 3.48 | 17.2 ± 3.14 | <0.001 |
| ASMMI (kg/m2) | 7.89 ± 1.06 | 6.83 ± 1.16 | <0.001 |
| Nutritional Ultrasound (NU) | |||
| Rectus femoris cross-sectional area (RF-CSA) (cm2) | 4.35 ± 1.45 | 3.22 ± 1.03 | <0.001 |
| RF-X axis (cm) | 3.82 ± 0.508 | 3.74 ± 3.06 | 0.731 |
| RF-Y axis (cm) | 1.36 ± 0.348 | 1.24 ± 1.04 | 0.174 |
| Leg Subcutaneous adipose tissue (L-SAT) (cm) | 0.594 ± 0.293 | 1.49 ± 1.90 | <0.001 |
| Abdominal Subcutaneous adipose tissue (A-SAT) (cm) | 1.31 ± 0.643 | 2.19 ± 0.899 | <0.001 |
| Preperitoneal adipose tissue (A-VAT) (cm) | 0.685 ± 0.295 | 0.939 ± 0.418 | 0.001 |
| Functional test | |||
| Handgrip strength (kg) | 32.7 ± 9.06 | 19.1 ± 6.64 | <0.001 |
| Male N = 165 | Female N = 102 | p-Value | ||
|---|---|---|---|---|
| Muscle area (SMA) | mean ± SD | 130 ± 23.7 | 92.4 ±15.8 | <0.001 |
| Muscle (%) | mean ± SD | 18.0 ± 4.31 | 14.3 ± 4.21 | <0.001 |
| Muscle (HU) | mean ± SD | 41.0 ± 9.31 | 38.1 ± 9.86 | 0.015 |
| SMI-CT | mean ± SD | 44.8 ± 7.47 | 36.8 ± 5.60 | <0.001 |
| IMAT area | mean ± SD | 15.7 ± 11.4 | 17.3 ± 10.6 | 0.256 |
| IMAT (%) | mean ± SD | 2.65 ± 4.28 | 2.48 ± 1.27 | 0.703 |
| IMAT (HU) | mean ± SD | −64.4 ± 6.33 | −65.8 ± 6.74 | 0.095 |
| CT-VAT area | mean ± SD | 200 ± 117 | 143 ± 83.3 | <0.001 |
| CT-VAT (%) | mean ± SD | 31.0 ± 37.9 | 19.4 ± 8.76 | 0.003 |
| CT-VAT (UH) | mean ± SD | −93.8 ± 8.58 | −93.3 ± 9.18 | 0.650 |
| CT-SAT area | mean ± SD | 156 ± 70.4 | 232 ± 124 | <0.001 |
| CT-SAT (%) | mean ± SD | 26.3 ± 41.3 | 31.8 ± 10.5 | 0.190 |
| CT-SAT (HU) | mean ± SD | −96.6 ± 11.5 | −99.8 ± 11.3 | 0.027 |
| Reference Value | Total | n = 267 |
|---|---|---|
| Sarcopenia CT | ||
| SMI (kg/m2) | ||
| Low SMI (Martin) | Total | 117 (43.8%) |
| Male | n (%) | 75 (28.1%) |
| Female | n (%) | 42 (15.7%) |
| Low SMI (Prado) | Total | 133 (49.8%) |
| Male | n (%) | 109 (40.8%) |
| Female | n (%) | 24 (9%) |
| Sarcopenia (EWGSOP2 criteria) | n (%) | 9 (3.7%) |
| Handgrip strength | ||
| Low HGS | Total | 60 (27.5%) |
| Male | n (%) | 39 (15.3%) |
| Female | n (%) | 31 (12.2%) |
| ASMMI (kg) | ||
| Low ASMMI | Total | 27 (11.2%) |
| Male | n (%) | 22 (9.1%) |
| Female | n (%) | 5 (2.1%) |
| SAT-CT cm2 | Total | n = 267 |
|---|---|---|
| Hight fat mass CT (Caan) | Total | 77 (28.8%) |
| Male | n (%) | 41 (15.4%) |
| Female | n (%) | 36 (13.5%) |
| Muscle Quality (UH) | ||
| Myoesteatosis CT (Dolan) | Total | 65 (24.3%) |
| Male | n (%) | 29 (10.9%) |
| Female | n (%) | 36 (13.5%) |
| 95% Confidence Interval | ||||||
|---|---|---|---|---|---|---|
| Predictor | Estimate | SE | Lower | Upper | t | p |
| Intercept | 23.211 | 23.7882 | −23.681 | 70.102 | 0.976 | 0.330 |
| Gender: | ||||||
| Male Female | 14.821 | 2.6860 | 9.526 | 20.116 | 5.518 | <0.001 |
| Age | −0.332 | 0.0919 | −0.513 | −0.151 | −3.618 | <0.001 |
| Weight | 0.547 | 0.0811 | 0.387 | 0.707 | 6.743 | <0.001 |
| Hight | 9.834 | 14.6346 | −19.014 | 38.682 | 0.672 | 0.502 |
| RF_CSA | 2.298 | 0.8618 | 0.600 | 3.997 | 2.667 | 0.008 |
| HGS | 0.524 | 0.1428 | 0.242 | 0.805 | 3.668 | <0.001 |
| BCM | 0.808 | 0.1944 | 0.425 | 1.191 | 4.155 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guirado-Peláez, P.; Fernández-Jiménez, R.; Sánchez-Torralvo, F.J.; Mucarzel Suárez-Arana, F.; Palmas-Candia, F.X.; Vegas-Aguilar, I.; Amaya-Campos, M.d.M.; Martínez Tamés, G.; Soria-Utrilla, V.; Tinahones-Madueño, F.; et al. Multiparametric Approach to the Colorectal Cancer Phenotypes Integrating Morphofunctional Assessment and Computer Tomography. Cancers 2024, 16, 3493. https://doi.org/10.3390/cancers16203493
Guirado-Peláez P, Fernández-Jiménez R, Sánchez-Torralvo FJ, Mucarzel Suárez-Arana F, Palmas-Candia FX, Vegas-Aguilar I, Amaya-Campos MdM, Martínez Tamés G, Soria-Utrilla V, Tinahones-Madueño F, et al. Multiparametric Approach to the Colorectal Cancer Phenotypes Integrating Morphofunctional Assessment and Computer Tomography. Cancers. 2024; 16(20):3493. https://doi.org/10.3390/cancers16203493
Chicago/Turabian StyleGuirado-Peláez, Patricia, Rocío Fernández-Jiménez, Francisco José Sánchez-Torralvo, Fernanda Mucarzel Suárez-Arana, Fiorella Ximena Palmas-Candia, Isabel Vegas-Aguilar, María del Mar Amaya-Campos, Gema Martínez Tamés, Virginia Soria-Utrilla, Francisco Tinahones-Madueño, and et al. 2024. "Multiparametric Approach to the Colorectal Cancer Phenotypes Integrating Morphofunctional Assessment and Computer Tomography" Cancers 16, no. 20: 3493. https://doi.org/10.3390/cancers16203493
APA StyleGuirado-Peláez, P., Fernández-Jiménez, R., Sánchez-Torralvo, F. J., Mucarzel Suárez-Arana, F., Palmas-Candia, F. X., Vegas-Aguilar, I., Amaya-Campos, M. d. M., Martínez Tamés, G., Soria-Utrilla, V., Tinahones-Madueño, F., García-Almeida, J. M., Burgos-Peláez, R., & Olveira, G. (2024). Multiparametric Approach to the Colorectal Cancer Phenotypes Integrating Morphofunctional Assessment and Computer Tomography. Cancers, 16(20), 3493. https://doi.org/10.3390/cancers16203493