Advanced Imaging for Localized Prostate Cancer


Abstract
Simple Summary
Abstract
1. Introduction
2. Multiparametric Magnetic Resonance Imaging
2.1. Multiparametric MRI (mpMRI)
2.2. Biopsy-Naïve Patients
2.3. Previous Negative Biopsy
2.4. Active Surveillance
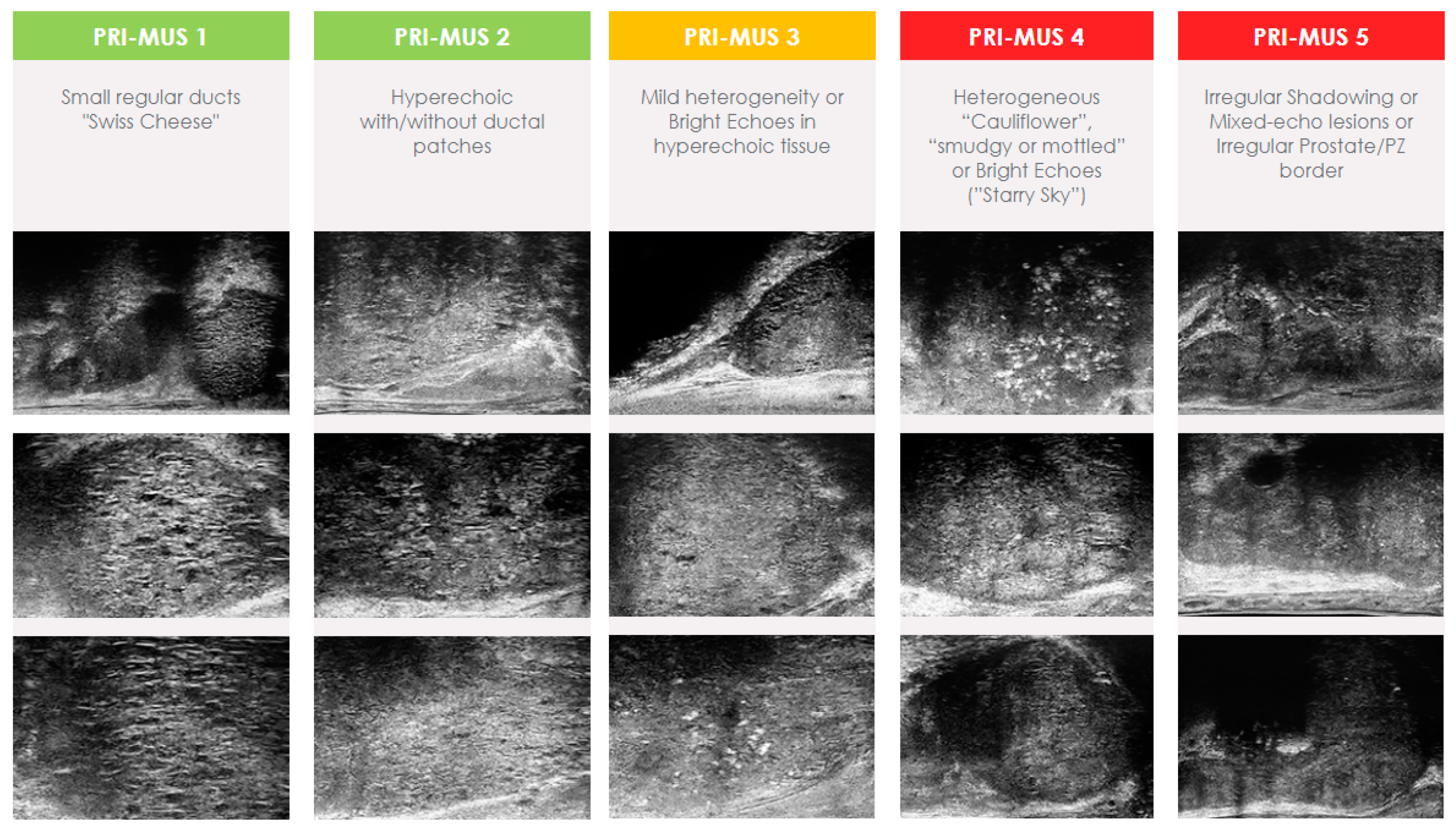
3. Micro-Ultrasound
3.1. Complementary Role with MRI
3.2. Biopsy-Naïve Patients
3.3. Previous Negative Biopsy
3.4. Active Surveillance
4. PSMA PET
4.1. Biopsy-Naïve Patients
4.2. Previous Negative Biopsy
4.3. Active Surveillance
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Tosoian, J.J.; Mamawala, M.; Epstein, J.I.; Landis, P.; Macura, K.J.; Simopoulos, D.N.; Carter, H.B.; Gorin, M.A. Active Surveillance of Grade Group 1 Prostate Cancer: Long-Term Outcomes from a Large Prospective Cohort. Eur. Urol. 2020, 77, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Litwin, M.S.; Tan, H.J. The Diagnosis and Treatment of Prostate Cancer: A Review. JAMA J. Am. Med. Assoc. 2017, 317, 2532–2542. [Google Scholar] [CrossRef] [PubMed]
- Cowan, T.; Baker, E.; McCray, G.; Reeves, F.; Houlihan, K.; Johns-Putra, L. Detection of Clinically Significant Cancer in the Anterior Prostate by Transperineal Biopsy. BJU Int. 2020, 126, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Matoso, A.; Epstein, J.I. Defining Clinically Significant Prostate Cancer on the Basis of Pathological Findings. Histopathology 2019, 74, 135–145. [Google Scholar] [CrossRef]
- Corcoran, N.M.; Hong, M.K.H.; Casey, R.G.; Hurtado-Coll, A.; Peters, J.; Harewood, L.; Goldenberg, S.L.; Hovens, C.M.; Costello, A.J.; Gleave, M.E. Upgrade in Gleason Score between Prostate Biopsies and Pathology Following Radical Prostatectomy Significantly Impacts upon the Risk of Biochemical Recurrence. BJU Int. 2011, 108, E202–E210. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic Accuracy of Multi-Parametric MRI and TRUS Biopsy in Prostate Cancer (PROMIS): A Paired Validating Confirmatory Study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef]
- Dos Santos, D.N.; Horvat, N.; Dias, A.B.; Mota, M.; Filho, G.; Schoen, K.; Ghai, S.; Queiroz, M.; Viana, P. Prostate Cancer Imaging: What We Already Know and What Is on the Horizon. Radiographics 2022, 42, E123–E124. [Google Scholar] [CrossRef]
- EAU Guidelines. Available online: https://uroweb.org/guidelines/prostate-cancer/chapter/diagnostic-evaluation (accessed on 22 August 2023).
- Wei, J.T.; Barocas, D.; Carlsson, S.; Coakley, F.; Eggener, S.; Etzioni, R.; Fine, S.W.; Han, M.; Konety, B.R.; Miner, M.; et al. Early Detection of Prostate Cancer: AUA/SUO Guideline Part II: Considerations for a Prostate Biopsy. J. Urol. 2023, 210, 54–63. [Google Scholar] [CrossRef]
- Mason, R.J.; Marzouk, K.; Finelli, A.; Saad, F.; So, A.I.; Violette, P.D.; Breau, R.H.; Rendon, R.A. UPDATE—2022 Canadian Urological Association Recommendations on Prostate Cancer Screening and Early Diagnosis: Endorsement of the 2021 Cancer Care Ontario Guidelines on Prostate Multiparametric Magnetic Resonance Imaging. Yosetsu Gakkai Shi/J. Jpn. Weld. Soc. 2022, 16, E184–E196. [Google Scholar] [CrossRef]
- Giganti, F.; Rosenkrantz, A.B.; Villeirs, G.; Panebianco, V.; Stabile, A.; Emberton, M.; Moore, C.M. The Evolution of MRI of the Prostate: The Past, the Present, and the Future. Am. J. Roentgenol. 2019, 213, 384–396. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Demirel, H.C.; Davis, J.W. Multiparametric Magnetic Resonance Imaging: Overview of the Technique, Clinical Applications in Prostate Biopsy and Future Directions. Turk. J. Urol. 2018, 44, 93. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Belue, M.J.; Yilmaz, E.C.; Daryanani, A.; Turkbey, B. Current Status of Biparametric MRI in Prostate Cancer Diagnosis: Literature Analysis. Life 2022, 12, 804. [Google Scholar] [CrossRef] [PubMed]
- Iacob, R.; Stoicescu, E.R.; Cerbu, S.; Manolescu, D.L.; Bardan, R.; Cumpănaş, A. Could Biparametric MRI Replace Multiparametric MRI in the Management of Prostate Cancer? Life 2023, 13, 465. [Google Scholar] [CrossRef]
- Asif, A.; Nathan, A.; Ng, A.; Khetrapal, P.; Chan, V.W.S.; Giganti, F.; Allen, C.; Freeman, A.; Punwani, S.; Lorgelly, P.; et al. Comparing Biparametric to Multiparametric MRI in the Diagnosis of Clinically Significant Prostate Cancer in Biopsy-Naive Men (PRIME): A Prospective, International, Multicentre, Non-Inferiority within-Patient, Diagnostic Yield Trial Protocol. BMJ Open 2023, 13, e070280. [Google Scholar] [CrossRef]
- Zhang, M.; Milot, L.; Khalvati, F.; Sugar, L.; Downes, M.; Baig, S.M.; Klotz, L.; Haider, M.A. Value of Increasing Biopsy Cores per Target with Cognitive MRI-Targeted Transrectal US Prostate Biopsy. Radiology 2019, 291, 83–89. [Google Scholar] [CrossRef]
- Dimitroulis, P.; Rabenalt, R.; Nini, A.; Hiester, A.; Esposito, I.; Schimmöller, L.; Antoch, G.; Albers, P.; Arsov, C. Multiparametric Magnetic Resonance Imaging/Ultrasound Fusion Prostate Biopsy—Are 2 Biopsy Cores per Magnetic Resonance Imaging Lesion Required? J. Urol. 2018, 200, 1030–1034. [Google Scholar] [CrossRef]
- Cetin, S.; Huseyinli, A.; Koparal, M.Y.; Bulut, E.C.; Ucar, M.; Gonul, I.I.; Sozen, S. How Many Cores Should Be Taken from Each Region of Interest When Performing a Targeted Transrectal Prostate Biopsy? Prostate Int. 2023, 11, 122–126. [Google Scholar] [CrossRef]
- Subramanian, N.; Recchimuzzi, D.Z.; Xi, Y.; Diaz De Leon, A.; Chen, H.; Xie, D.; Goldberg, K.; Rofsky, N.M.; Pedrosa, I.; Costa, D.N. Impact of the Number of Cores on the Prostate Cancer Detection Rate in Men Undergoing In-Bore Magnetic Resonance Imaging-Guided Targeted Biopsies. J. Comput. Assist. Tomogr. 2021, 45, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Recchimuzzi, D.Z.; de Leon, A.D.; Pedrosa, I.; Travalini, D.; Latin, H.; Goldberg, K.; Meng, X.; Begovic, J.; Rayan, J.; Roehrborn, C.G.; et al. Direct MRI-Guided In-Bore Targeted Biopsy of the Prostate: A Step-by-Step How To and Lessons Learned. Radiographics 2024, 44, e230142. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.N.; Goldberg, K.; de Leon, A.D.; Lotan, Y.; Xi, Y.; Aziz, M.; Freifeld, Y.; Margulis, V.; Raj, G.; Roehrborn, C.G.; et al. Magnetic Resonance Imaging–Guided In-Bore and Magnetic Resonance Imaging-Transrectal Ultrasound Fusion Targeted Prostate Biopsies: An Adjusted Comparison of Clinically Significant Prostate Cancer Detection Rate. Eur. Urol. Oncol. 2019, 2, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Venderink, W.; van der Leest, M.; van Luijtelaar, A.; van de Ven, W.J.M.; Fütterer, J.J.; Sedelaar, J.P.M.; Huisman, H.J. Retrospective Comparison of Direct In-Bore Magnetic Resonance Imaging (MRI)-Guided Biopsy and Fusion-Guided Biopsy in Patients with MRI Lesions Which Are Likely or Highly Likely to Be Clinically Significant Prostate Cancer. World J. Urol. 2017, 35, 1849–1855. [Google Scholar] [CrossRef]
- Ramos, F.; Korets, R.; Fleishman, A.; Kaul, S.; Johnson, M.; Wei, J.L.; Olumi, A.F.; Tsai, L.L.; Gershman, B. Comparative Effectiveness of Magnetic Resonance Imaging-Ultrasound Fusion Versus In-Bore Magnetic Resonance Imaging-Targeted Prostate Biopsy. Urology 2023, 171, 164–171. [Google Scholar] [CrossRef]
- Arsov, C.; Rabenalt, R.; Blondin, D.; Quentin, M.; Hiester, A.; Godehardt, E.; Gabbert, H.E.; Becker, N.; Antoch, G.; Albers, P.; et al. Prospective Randomized Trial Comparing Magnetic Resonance Imaging (MRI)-Guided In-Bore Biopsy to MRI-Ultrasound Fusion and Transrectal Ultrasound-Guided Prostate Biopsy in Patients with Prior Negative Biopsies. Eur. Urol. 2015, 68, 713–720. [Google Scholar] [CrossRef]
- Lovegrove, C.E.; Miah, S.; El-Shater Bosaily, A.; Bott, S.; Brown, L.; Burns-Cox, N.; Dudderidge, T.; Freeman, A.; Henderson, A.; Hindley, R.; et al. Comparison of Transrectal Ultrasound Biopsy to Transperineal Template Mapping Biopsies Stratified by Multiparametric Magnetic Resonance Imaging Score in the PROMIS Trial. J. Urol. 2020, 203, 100–105. [Google Scholar] [CrossRef]
- Moldovan, P.C.; Van den Broeck, T.; Sylvester, R.; Marconi, L.; Bellmunt, J.; van den Bergh, R.C.N.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; Fossati, N.; et al. What Is the Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in Excluding Prostate Cancer at Biopsy? A Systematic Review and Meta-Analysis from the European Association of Urology Prostate Cancer Guidelines Panel. Eur. Urol. 2017, 72, 250–266. [Google Scholar] [CrossRef]
- Caglic, I.; Kovac, V.; Barrett, T. Multiparametric MRI—Local Staging of Prostate Cancer and Beyond. Radiol. Oncol. 2019, 53, 159–170. [Google Scholar] [CrossRef]
- de Rooij, M.; Hamoen, E.H.J.; Witjes, J.A.; Barentsz, J.O.; Rovers, M.M. Accuracy of Magnetic Resonance Imaging for Local Staging of Prostate Cancer: A Diagnostic Meta-Analysis. Eur. Urol. 2016, 70, 233–245. [Google Scholar] [CrossRef]
- Sebesta, E.M.; Anderson, C.B. The Surgical Management of Prostate Cancer. Semin. Oncol. 2017, 44, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Eastham, J.A.; Auffenberg, G.B.; Barocas, D.A.; Chou, R.; Crispino, T.; Davis, J.W.; Eggener, S.; Horwitz, E.M.; Kane, C.J.; Lin, D.W.; et al. Clinically Localized Prostate Cancer: AUA/ASTRO Guideline 2022. J. Urol. 2022, 208, 10–33. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Vesprini, D.; Sethukavalan, P.; Jethava, V.; Zhang, L.; Jain, S.; Yamamoto, T.; Mamedov, A.; Loblaw, A. Long-Term Follow-up of a Large Active Surveillance Cohort of Patients with Prostate Cancer. J. Clin. Oncol. 2015, 33, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of Prostate Systematic and Targeted Biopsy on the Basis of Multiparametric MRI in Biopsy-Naive Patients (MRI-FIRST): A Prospective, Multicentre, Paired Diagnostic Study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Sidana, A.; Watson, M.J.; George, A.K.; Rastinehad, A.R.; Vourganti, S.; Rais-Bahrami, S.; Muthigi, A.; Maruf, M.; Gordetsky, J.B.; Nix, J.W.; et al. Fusion Prostate Biopsy Outperforms 12-Core Systematic Prostate Biopsy in Patients with Prior Negative Systematic Biopsy: A Multi-Institutional Analysis. Urol. Oncol. 2018, 36, 341.e1–341.e7. [Google Scholar] [CrossRef]
- Ouzzane, A.; Renard-Penna, R.; Marliere, F.; Mozer, P.; Olivier, J.; Barkatz, J.; Puech, P.; Villers, A. Magnetic Resonance Imaging Targeted Biopsy Improves Selection of Patients Considered for Active Surveillance for Clinically Low Risk Prostate Cancer Based on Systematic Biopsies. J. Urol. 2015, 194, 350–356. [Google Scholar] [CrossRef]
- Klotz, L.; Loblaw, A.; Sugar, L.; Moussa, M.; Berman, D.M.; Van der Kwast, T.; Vesprini, D.; Milot, L.; Kebabdjian, M.; Fleshner, N.; et al. Active Surveillance Magnetic Resonance Imaging Study (ASIST): Results of a Randomized Multicenter Prospective Trial. Eur. Urol. 2019, 75, 300–309. [Google Scholar] [CrossRef]
- Turkbey, B.; Brown, A.M.; Sankineni, S.; Wood, B.J.; Pinto, P.A.; Choyke, P.L. Multiparametric Prostate Magnetic Resonance Imaging in the Evaluation of Prostate Cancer. CA Cancer J. Clin. 2016, 66, 326–336. [Google Scholar] [CrossRef]
- Mowatt, G.; Scotland, G.; Boachie, C.; Cruickshank, M.; Ford, J.A.; Fraser, C.; Kurban, L.; Lam, T.B.; Padhani, A.R.; Royle, J.; et al. The Diagnostic Accuracy and Cost-Effectiveness of Magnetic Resonance Spectroscopy and Enhanced Magnetic Resonance Imaging Techniques in Aiding the Localisation of Prostate Abnormalities for Biopsy: A Systematic Review and Economic Evaluation. Health Technol. Assess. 2013, 17, 1–281. [Google Scholar] [CrossRef]
- Valerio, M.; Willis, S.; Van Der Meulen, J.; Emberton, M.; Ahmed, H.U. Methodological Considerations in Assessing the Utility of Imaging in Early Prostate Cancer. Curr. Opin. Urol. 2015, 25, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.U.; Kirkham, A.; Arya, M.; Illing, R.; Freeman, A.; Allen, C.; Emberton, M. Is It Time to Consider a Role for MRI before Prostate Biopsy? Nat. Rev. Clin. Oncol. 2009, 6, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/Ultrasound Fusion–Guided Biopsy With Ultrasound-Guided Biopsy for the Diagnosis of Prostate Cancer. JAMA 2015, 313, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Hansen, N.L.; Kesch, C.; Barrett, T.; Koo, B.; Radtke, J.P.; Bonekamp, D.; Schlemmer, H.P.; Warren, A.Y.; Wieczorek, K.; Hohenfellner, M.; et al. Multicentre Evaluation of Targeted and Systematic Biopsies Using Magnetic Resonance and Ultrasound Image-Fusion Guided Transperineal Prostate Biopsy in Patients with a Previous Negative Biopsy. BJU Int. 2017, 120, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. Prostate Cancer, Version 4.2023, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2023, 21, 1067–1096. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, A.; Yerram, N.K.; O’Connor, L.; Brisbane, W.; Sharma, V.; Chuang, R.; Jayadevan, R.; Ahdoot, M.; Daneshvar, M.; Priester, A.; et al. Magnetic Resonance Imaging-Guided Biopsy in Active Surveillance of Prostate Cancer. J. Urol. 2022, 207, 823–831. [Google Scholar] [CrossRef]
- Fusco, F.; Emberton, M.; Arcaniolo, D.; De Nunzio, C.; Manfredi, C.; Creta, M. Prostatic High-Resolution Micro-Ultrasound: An Attractive Step-Forward in the Management of Prostate Cancer Patients. Prostate Cancer Prostatic Dis. 2022, 26, 521–522. [Google Scholar] [CrossRef]
- Wang, B.; Broomfield, S.; Medina Martín, A.; Albers, P.; Fung, C.; Kinnaird, A. Detection of Clinically Significant Prostate Cancer by Micro-Ultrasound-Informed Systematic Biopsy during MRI/Micro-Ultrasound Fusion Biopsy. Can. Urol. Assoc. J. 2023, 14. [Google Scholar] [CrossRef]
- Schaer, S.; Rakauskas, A.; Dagher, J.; La Rosa, S.; Pensa, J.; Brisbane, W.; Marks, L.; Kinnaird, A.; Abouassaly, R.; Klein, E.; et al. Assessing Cancer Risk in the Anterior Part of the Prostate Using Micro-Ultrasound: Validation of a Novel Distinct Protocol. World J. Urol. 2023, 41, 3325–3331. [Google Scholar] [CrossRef]
- Ghai, S.; Eure, G.; Fradet, V.; Hyndman, M.E.; McGrath, T.; Wodlinger, B.; Pavlovich, C.P. Assessing Cancer Risk on Novel 29 MHz Micro-Ultrasound Images of the Prostate: Creation of the Micro-Ultrasound Protocol for Prostate Risk Identification. J. Urol. 2016, 196, 562–569. [Google Scholar] [CrossRef]
- Rohrbach, D.; Wodlinger, B.; Wen, J.; Mamou, J.; Feleppa, E. High-Frequency Quantitative Ultrasound for Imaging Prostate Cancer Using a Novel Micro-Ultrasound Scanner. Ultrasound Med. Biol. 2018, 44, 1341–1354. [Google Scholar] [CrossRef] [PubMed]
- Tay, K.J.; Gupta, R.T.; Rastinehad, A.R.; Tsivian, E.; Freedland, S.J.; Moul, J.W.; Polascik, T.J. Navigating MRI-TRUS Fusion Biopsy: Optimizing the Process and Avoiding Technical Pitfalls. Expert. Rev. Anticancer. Ther. 2016, 16, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Coker, M.A.; Glaser, Z.A.; Gordetsky, J.B.; Thomas, J.V.; Rais-Bahrami, S. Targets Missed: Predictors of MRI-Targeted Biopsy Failing to Accurately Localize Prostate Cancer Found on Systematic Biopsy. Prostate Cancer Prostatic Dis. 2018, 21, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Andriole, G.; Cash, H.; Cooperberg, M.; Crawford, E.D.; Emberton, M.; Gomez-Sancha, F.; Klein, E.; Lughezzani, G.; Marks, L.; et al. Optimization of Prostate Biopsy—Micro-Ultrasound versus MRI (OPTIMUM): A 3-Arm Randomized Controlled Trial Evaluating the Role of 29 MHz Micro-Ultrasound in Guiding Prostate Biopsy in Men with Clinical Suspicion of Prostate Cancer. Contemp. Clin. Trials 2022, 112, 106618. [Google Scholar] [CrossRef] [PubMed]
- Org, S.; Cash, H.; Hofbauer, S.L.; Shore, N.; Pavlovich, C.P.; Bulang, S.; Schostak, M.; Planken, E.; Jaspars, J.J.; Luger, F.; et al. Prostate Cancer Detection by Novice Micro-Ultrasound Users Enrolled in a Training Program. Soc. Int. Urol. J. 2022, 3, 62–68. [Google Scholar] [CrossRef]
- Albers, P.; Bennett, J.; Evans, M.; Martin, E.S.; Wang, B.; Broomfield, S.; Martín, A.M.; Tu, W.; Fung, C.; Kinnaird, A. Value of Incremental Biopsy Cores for Microultrasound Targeted Prostate Biopsies. Urology 2024, 184, 142–148. [Google Scholar] [CrossRef]
- Albers, P.; Wang, B.; Broomfield, S.; Medina Martín, A.; Fung, C.; Kinnaird, A. Micro-Ultrasound Versus Magnetic Resonance Imaging in Prostate Cancer Active Surveillance. Eur. Urol. Open Sci. 2022, 46, 33–35. [Google Scholar] [CrossRef]
- Kudlackova, S.; Kurfurstova, D.; Kral, M.; Hruska, F.; Vidlar, A.; Student, V. Do Not Underestimate Anterior Prostate Cancer. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2021, 165, 198–202. [Google Scholar] [CrossRef]
- Stamey, T.A.; Donaldson, A.N.; Yemoto, C.E.; Mcneal, J.E.; Sozen, S.; Gill, H. Histological and Clinical Findings in 896 Consecutive Prostates Treated Only with Radical Retropubic Prostatectomy: Epidemiologic Significance of Annual Changes. J. Urol. 1998, 160, 2412–2417. [Google Scholar] [CrossRef]
- McNeal, J.E.; Redwine, E.A.; Freiha, F.S.; Stamey, T.A. Zonal Distribution of Prostatic Adenocarcinoma. Correlation with Histologic Pattern and Direction of Spread. Am. J. Surg. Pathol. 1988, 12, 897–906. [Google Scholar] [CrossRef]
- McNeal, J.E.; Haillot, O. Patterns of Spread of Adenocarcinoma in the Prostate as Related to Cancer Volume. Prostate 2001, 49, 48–57. [Google Scholar] [CrossRef] [PubMed]
- McNeal, J.E. Cancer Volume and Site of Origin of Adenocarcinoma in the Prostate: Relationship to Local and Distant Spread. Hum. Pathol. 1992, 23, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Abouassaly, R.; Klein, E.A.; El-Shefai, A.; Stephenson, A. Impact of Using 29 MHz High-Resolution Micro-Ultrasound in Real-Time Targeting of Transrectal Prostate Biopsies: Initial Experience. World J. Urol. 2020, 38, 1201–1206. [Google Scholar] [CrossRef] [PubMed]
- Lughezzani, G.; Saita, A.; Lazzeri, M.; Paciotti, M.; Maffei, D.; Lista, G.; Hurle, R.; Buffi, N.M.; Guazzoni, G.; Casale, P. Comparison of the Diagnostic Accuracy of Micro-Ultrasound and Magnetic Resonance Imaging/Ultrasound Fusion Targeted Biopsies for the Diagnosis of Clinically Significant Prostate Cancer. Eur. Urol. Oncol. 2019, 2, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Lughezzani, G.; Maffei, D.; Sánchez, A.; Pereira, J.G.; Staerman, F.; Cash, H.; Luger, F.; Lopez, L.; Shore, N.D.; et al. Comparison of Micro-Ultrasound and Multiparametric Magnetic Resonance Imaging for Prostate Cancer: A Multicenter, Prospective Analysis. Can. Urol. Assoc. J. 2020, 15, E11–E16. [Google Scholar] [CrossRef] [PubMed]
- Lughezzani, G.; Maffei, D.; Saita, A.; Paciotti, M.; Diana, P.; Buffi, N.M.; Colombo, P.; Elefante, G.M.; Hurle, R.; Lazzeri, M.; et al. Diagnostic Accuracy of Microultrasound in Patients with a Suspicion of Prostate Cancer at Magnetic Resonance Imaging: A Single-Institutional Prospective Study. Eur. Urol. Focus. 2021, 7, 1019–1026. [Google Scholar] [CrossRef]
- Maffei, D.; Fasulo, V.; Avolio, P.P.; Saitta, C.; Paciotti, M.; De Carne, F.; Colombo, P.; Pasini, L.; De Zorzi, S.Z.; Saita, A.; et al. Diagnostic Performance of MicroUltrasound at MRI-Guided Confirmatory Biopsy in Patients under Active Surveillance for Low-Risk Prostate Cancer. Prostate 2023, 83, 886–895. [Google Scholar] [CrossRef]
- Chessa, F.; Schiavina, R.; Amelio, E.; Gaudiano, C.; Giusti, D.; Bianchi, L.; Pultrone, C.; Marcelli, E.; Distefano, C.; Lodigiani, L.; et al. Diagnostic Accuracy of the Novel 29 MHz Micro-Ultrasound “ExactVuTM” for the Detection of Clinically Significant Prostate Cancer: A Prospective Single Institutional Study. A Step Forward in the Diagnosis of Prostate Cancer. Arch. Ital. Urol. Androl. 2021, 93, 132–138. [Google Scholar] [CrossRef]
- Cornud, F.; Lefevre, A.; Flam, T.; Dumonceau, O.; Galiano, M.; Soyer, P.; Camparo, P.; Barral, M. MRI-Directed High-Frequency (29MhZ) TRUS-Guided Biopsies: Initial Results of a Single-Center Study. Eur. Radiol. 2020, 30, 4838–4846. [Google Scholar] [CrossRef]
- Eure, G.; Fanney, D.; Lin, J.; Wodlinger, B.; Ghai, S. Comparison of Conventional Transrectal Ultrasound, Magnetic Resonance Imaging, and Micro-Ultrasound for Visualizing Prostate Cancer in an Active Surveillance Population: A Feasibility Study. Can. Urol. Assoc. J. 2019, 13, E70–E77. [Google Scholar] [CrossRef]
- Staerman, F. The Utility of 29 MHz Resolution Micro-Ultrasound and mpMRI in the Management of Gleason 6 Prostate Cancer with Active Surveillance. Eur. Urol. Suppl. 2019, 18, e3502. [Google Scholar] [CrossRef]
- García Garzón, J.R.; de Arcocha Torres, M.; Delgado-Bolton, R.; Ceci, F.; Alvarez Ruiz, S.; Orcajo Rincón, J.; Caresia Aróztegui, A.P.; García Velloso, M.J.; García Vicente, A.M. 68Ga-PSMA PET/CT in Prostate Cancer. Rev. Esp. Med. Nucl. Imagen Mol. 2018, 37, 130–138. [Google Scholar] [CrossRef]
- Farolfi, A.; Calderoni, L.; Mattana, F.; Mei, R.; Telo, S.; Fanti, S.; Castellucci, P. Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer. J. Nucl. Med. 2021, 62, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Malan, N.; Vangu, M.D.T. Normal Variants, Pitfalls, and Artifacts in Ga-68 Prostate Specific Membrane Antigen (PSMA) PET/CT Imaging. Front. Nucl. Med. 2022, 2, 825512. [Google Scholar] [CrossRef] [PubMed]
- Piron, S.; Verhoeven, J.; Vanhove, C.; De Vos, F. Recent Advancements in 18F-Labeled PSMA Targeting PET Radiopharmaceuticals. Nucl. Med. Biol. 2022, 106–107, 29–51. [Google Scholar] [CrossRef]
- Veit-Haibach, P.; Ahlström, H.; Boellaard, R.; Delgado Bolton, R.C.; Hesse, S.; Hope, T.; Huellner, M.W.; Iagaru, A.; Johnson, G.B.; Kjaer, A.; et al. International EANM-SNMMI-ISMRM Consensus Recommendation for PET/MRI in Oncology. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 3513–3537. [Google Scholar] [CrossRef]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N.; et al. F-18 Labelled PSMA-1007: Biodistribution, Radiation Dosimetry and Histopathological Validation of Tumor Lesions in Prostate Cancer Patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef]
- Dietlein, M.; Kobe, C.; Kuhnert, G.; Stockter, S.; Fischer, T.; Schomäcker, K.; Schmidt, M.; Dietlein, F.; Zlatopolskiy, B.D.; Krapf, P.; et al. Comparison of [(18)F]DCFPyL and [ (68)Ga]Ga-PSMA-HBED-CC for PSMA-PET Imaging in Patients with Relapsed Prostate Cancer. Mol. Imaging Biol. 2015, 17, 575–584. [Google Scholar] [CrossRef]
- Jetty, S.; Loftus, J.R.; Patel, A.; Gupta, A.; Puri, S.; Dogra, V. Prostate Cancer—PET Imaging Update. Cancers 2023, 15, 796. [Google Scholar] [CrossRef]
- Alshamrani, A.F.A. Diagnostic Accuracy of Molecular Imaging Techniques for Detecting Prostate Cancer: A Systematic Review. Diagnostics 2024, 14, 1315. [Google Scholar] [CrossRef]
- Zhang, H.; Qi, L.; Cai, Y.; Gao, X. Gastrin-Releasing Peptide Receptor (GRPR) as a Novel Biomarker and Therapeutic Target in Prostate Cancer. Ann. Med. 2024, 56, 2320301. [Google Scholar] [CrossRef] [PubMed]
- Challapalli, A.; Barwick, T.D.; Dubash, S.R.; Inglese, M.; Grech-Sollars, M.; Kozlowski, K.; Tam, H.; Patel, N.H.; Winkler, M.; Flohr, P.; et al. Bench to Bedside Development of [18F]Fluoromethyl-(1,2-2H4)Choline ([18F]D4-FCH). Molecules 2023, 28, 8018. [Google Scholar] [CrossRef] [PubMed]
- Okudaira, H.; Shikano, N.; Nishii, R.; Miyagi, T.; Yoshimoto, M.; Kobayashi, M.; Ohe, K.; Nakanishi, T.; Tamai, I.; Namiki, M.; et al. Putative Transport Mechanism and Intracellular Fate of Trans-1-Amino-3-18F-Fluorocyclobutanecarboxylic Acid in Human Prostate Cancer. J. Nucl. Med. 2011, 52, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Savir-Baruch, B.; Schuster, D.M. Prostate Cancer Imaging with 18F-Fluciclovine. PET Clin. 2022, 17, 607–620. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.S.; Sakellis, C.G.; Hyun, H.; Jacene, H.A. Extraprostatic Uptake of 18F-Fluciclovine: Differentiation of Nonprostatic Neoplasms from Metastatic Prostate Cancer. Am. J. Roentgenol. 2020, 214, 641–648. [Google Scholar] [CrossRef]
- Beer, M.; Montani, M.; Gerhardt, J.; Wild, P.J.; Hany, T.F.; Hermanns, T.; Müntener, M.; Kristiansen, G. Profiling Gastrin-Releasing Peptide Receptor in Prostate Tissues: Clinical Implications and Molecular Correlates. Prostate 2012, 72, 318–325. [Google Scholar] [CrossRef]
- Gao, X.; Tang, Y.; Chen, M.; Li, J.; Yin, H.; Gan, Y.; Zu, X.; Cai, Y.; Hu, S. A Prospective Comparative Study of [68Ga]Ga-RM26 and [68Ga]Ga-PSMA-617 PET/CT Imaging in Suspicious Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 2177–2187. [Google Scholar] [CrossRef]
- Schollhammer, R.; De Clermont Gallerande, H.; Yacoub, M.; Quintyn Ranty, M.L.; Barthe, N.; Vimont, D.; Hindié, E.; Fernandez, P.; Morgat, C. Comparison of the Radiolabeled PSMA-Inhibitor 111In-PSMA-617 and the Radiolabeled GRP-R Antagonist 111In-RM2 in Primary Prostate Cancer Samples. EJNMMI Res. 2019, 9, 52. [Google Scholar] [CrossRef]
- Rowe, S.P.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A. PSMA-RADS Version 1.0: A Step Towards Standardizing the Interpretation and Reporting of PSMA–Targeted PET Imaging Studies. Eur. Urol. 2018, 73, 485–487. [Google Scholar] [CrossRef]
- Emmett, L.; Buteau, J.; Papa, N.; Moon, D.; Thompson, J.; Roberts, M.J.; Rasiah, K.; Pattison, D.A.; Yaxley, J.; Thomas, P.; et al. The Additive Diagnostic Value of Prostate-Specific Membrane Antigen Positron Emission Tomography Computed Tomography to Multiparametric Magnetic Resonance Imaging Triage in the Diagnosis of Prostate Cancer (PRIMARY): A Prospective Multicentre Study. Eur. Urol. 2021, 80, 682–689. [Google Scholar] [CrossRef]
- Uprimny, C.; Kroiss, A.S.; Decristoforo, C.; Fritz, J.; von Guggenberg, E.; Kendler, D.; Scarpa, L.; di Santo, G.; Roig, L.G.; Maffey-Steffan, J.; et al. 68Ga-PSMA-11 PET/CT in Primary Staging of Prostate Cancer: PSA and Gleason Score Predict the Intensity of Tracer Accumulation in the Primary Tumour. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Demirci, E.; Kabasakal, L.; Şahin, O.E.; Akgün, E.; Gültekin, M.H.; Doǧanca, T.; Tuna, M.B.; Öbek, C.; Kiliç, M.; Esen, T.; et al. Can SUVmax Values of Ga-68-PSMA PET/CT Scan Predict the Clinically Significant Prostate Cancer? Nucl. Med. Commun. 2019, 40, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Seifert, R.; Emmett, L.; Rowe, S.P.; Herrmann, K.; Hadaschik, B.; Calais, J.; Giesel, F.L.; Reiter, R.; Maurer, T.; Heck, M.; et al. Second Version of the Prostate Cancer Molecular Imaging Standardized Evaluation Framework Including Response Evaluation for Clinical Trials (PROMISE V2). Eur. Urol. 2023, 83, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Yechiel, Y.; Orr, Y.; Gurevich, K.; Gill, R.; Keidar, Z. Advanced PSMA-PET/CT Imaging Parameters in Newly Diagnosed Prostate Cancer Patients for Predicting Metastatic Disease. Cancers 2023, 15, 1020. [Google Scholar] [CrossRef]
- Kase, A.M.; Tan, W.; Copland, J.A.; Cai, H.; Parent, E.E.; Madan, R.A. The Continuum of Metastatic Prostate Cancer: Interpreting PSMA PET Findings in Recurrent Prostate Cancer. Cancers 2022, 14, 1361. [Google Scholar] [CrossRef]
- Mütevelizade, G.; Sezgin, C.; Gümüşer, G.; Sayit, E. Unexpected Metastatic Localizations of Prostate Cancer Determined by 68Ga PSMA PET/CT: Series of Four Cases. Mol. Imaging Radionucl. Ther. 2022, 31, 223–226. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Mier, W.; Haufe, S.; Debus, N.; Eder, M.; Eisenhut, M.; Schäfer, M.; et al. Diagnostic Performance of 68Ga-PSMA-11 (HBED-CC) PET/CT in Patients with Recurrent Prostate Cancer: Evaluation in 1007 Patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1258–1268. [Google Scholar] [CrossRef]
- Liu, F.Y.; Sheng, T.W.; Tseng, J.R.; Yu, K.J.; Tsui, K.H.; Pang, S.T.; Wang, L.J.; Lin, G. Prostate-Specific Membrane Antigen (PSMA) Fusion Imaging in Prostate Cancer: PET-CT vs PET-MRI. Br. J. Radiol. 2022, 95, 20210728. [Google Scholar] [CrossRef]
- Chow, K.M.; So, W.Z.; Lee, H.J.; Lee, A.; Yap, D.W.T.; Takwoingi, Y.; Tay, K.J.; Tuan, J.; Thang, S.P.; Lam, W.; et al. Head-to-Head Comparison of the Diagnostic Accuracy of Prostate-Specific Membrane Antigen Positron Emission Tomography and Conventional Imaging Modalities for Initial Staging of Intermediate- to High-Risk Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. 2023, 84, 36–48. [Google Scholar] [CrossRef]
- Huo, H.; Shen, S.; He, D.; Liu, B.; Yang, F. Head-to-Head Comparison of 68Ga-PSMA-11 PET/CT and 68Ga-PSMA-11 PET/MRI in the Detection of Biochemical Recurrence of Prostate Cancer: Summary of Head-to-Head Comparison Studies. Prostate Cancer Prostatic Dis. 2022, 26, 16–24. [Google Scholar] [CrossRef]
- Santiago Almeida, L.; Etchebehere, E.C.S.d.C.; García Megías, I.; Calapaquí Terán, A.K.; Hadaschik, B.; Colletti, P.M.; Herrmann, K.; Giammarile, F.; Delgado Bolton, R.C. PSMA Radioligand Therapy in Prostate Cancer Where Are We and Where Are We Heading? Clin. Nucl. Med. 2024, 49, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.J.; Castellano, D.; Herrmann, K.; de Bono, J.S.; Shore, N.D.; Chi, K.N.; Crosby, M.; Piulats, J.M.; Fléchon, A.; Wei, X.X.; et al. 177Lu-PSMA-617 versus a Change of Androgen Receptor Pathway Inhibitor Therapy for Taxane-Naive Patients with Progressive Metastatic Castration-Resistant Prostate Cancer (PSMAfore): A Phase 3, Randomised, Controlled Trial. Lancet 2024, 404, 1227–1239. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.; Pepe, L.; Tamburo, M.; Marletta, G.; Pennisi, M.; Fraggetta, F. Targeted Prostate Biopsy: 68Ga-PSMA PET/CT vs. MpMRI in the Diagnosis of Prostate Cancer. Arch. Ital. Urol. Androl. 2022, 94, 274–277. [Google Scholar] [CrossRef]
- Lopci, E.; Saita, A.; Lazzeri, M.; Lughezzani, G.; Colombo, P.; Buffi, N.M.; Hurle, R.; Marzo, K.; Peschechera, R.; Benetti, A.; et al. 68Ga-PSMA Positron Emission Tomography/Computerized Tomography for Primary Diagnosis of Prostate Cancer in Men with Contraindications to or Negative Multiparametric Magnetic Resonance Imaging: A Prospective Observational Study. J. Urol. 2018, 200, 95–103. [Google Scholar] [CrossRef]
- Pepe, P.; Pepe, L.; Tamburo, M.; Marletta, G.; Savoca, F.; Pennisi, M.; Fraggetta, F. 68Ga-PSMA PET/CT Evaluation in Men Enrolled in Prostate Cancer Active Surveillance. Arch. Ital. Urol. Androl. 2023, 95, 31–34. [Google Scholar] [CrossRef]
- Krausewitz, P.; Bundschuh, R.A.; Gaertner, F.C.; Essler, M.; Attenberger, U.; Luetkens, J.; Kristiansen, G.; Muders, M.; Ohlmann, C.H.; Hauser, S.; et al. DEPROMP Trial: The Additive Value of PSMA-PET/CT-Guided Biopsy for Prostate Cancer Management in Biopsy Naïve Men-Study Protocol for a Randomized Trial. Trials 2023, 24, 167. [Google Scholar] [CrossRef]
- Lopci, E.; Lazzeri, M.; Colombo, P.; Casale, P.; Buffi, N.M.; Saita, A.; Peschechera, R.; Hurle, R.; Marzo, K.; Leonardi, L.; et al. Diagnostic Performance and Clinical Impact of PSMA PET/CT versus MpMRI in Patients with a High Suspicion of Prostate Cancer and Previously Negative Biopsy: A Prospective Trial (PROSPET-BX). Urol. Int. 2023, 107, 433–439. [Google Scholar] [CrossRef]
- Gondoputro, W.; Doan, P.; Katelaris, A.; Scheltema, M.J.; Geboers, B.; Agrawal, S.; Liu, Z.; Yaxley, J.; Savdie, R.; Rasiah, K.; et al. 68Ga-PSMA-PET/CT in Addition to MpMRI in Men Undergoing Biopsy during Active Surveillance for Low- to Intermediate-Risk Prostate Cancer: Study Protocol for a Prospective Cross-Sectional Study. Transl. Androl. Urol. 2023, 12, 1598–1606. [Google Scholar] [CrossRef]
- Krausewitz, P.; Gaertner, F.C.; Essler, M.; Attenberger, U.; Luetkens, J.; Kristiansen, G.; Ohlmann, C.H.; Hauser, S.; Ellinger, J.; Ritter, M. DEPROMP-Study: PSMA-PET/CT Prior to Prostate Biopsy: Enhancing Prostate Cancer Detection and Personalized Management. Eur. Urol. 2024, 85, S471. [Google Scholar] [CrossRef]
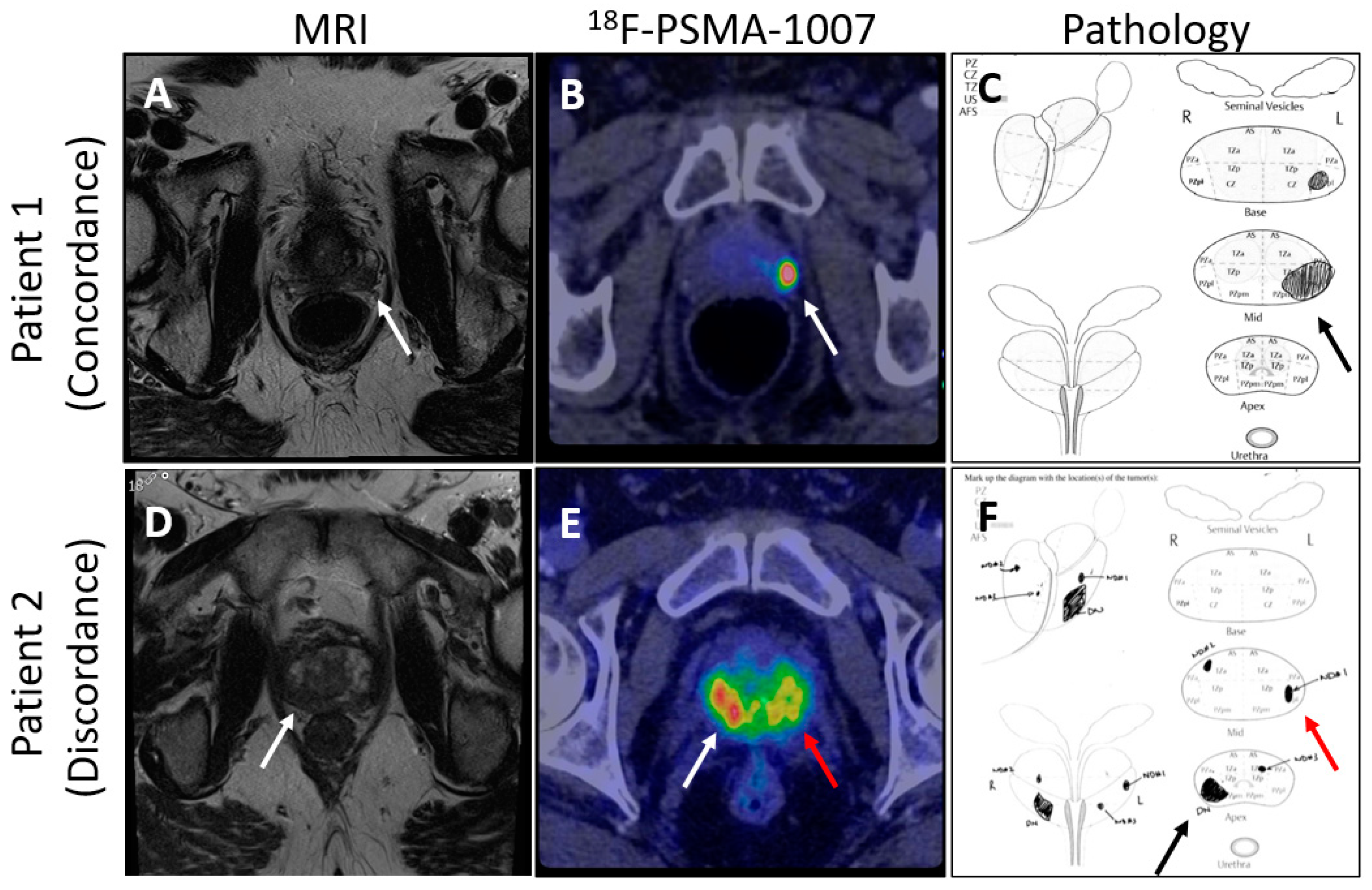
- Mookerji, N.; Pfanner, T.; Hui, A.; Huang, G.; Albers, P.; Mittal, R.; Broomfield, S.; Dean, L.; St Martin, B.; Jacobsen, N.-E.; et al. Fluorine-18 Prostate-Specific Membrane Antigen–1007 PET/CT vs Multiparametric MRI for Locoregional Staging of Prostate Cancer. JAMA Oncol. 2024, 10, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liu, T.; Zhang, Z.; Zhang, N.; Du, P.; Yang, Y.; Liu, Y.; Yu, W.; Li, N.; Gorin, M.A.; et al. 68Ga-PSMA PET/CT Combined with PET/Ultrasound-Guided Prostate Biopsy Can Diagnose Clinically Significant Prostate Cancer in Men with Previous Negative Biopsy Results. J. Nucl. Med. 2020, 61, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Lopci, E.; Lazzeri, M.; Disconzi, L.; Colombo, P.; Saita, A.; Peschechera, R.; Fasulo, V.; Maffei, D.; Zanca, R.; Casale, P.; et al. Interim Analyses from the PROSPET-BX Trial: [G8Ga]PSMA PET/CT vs. MpMRI in Patients with Suspicion of Prostate Cancer and Previous Negative Biopsy. J. Clin. Oncol. 2024, 42, 282. [Google Scholar] [CrossRef]
- Jain, A.; Nassour, A.J.; Dean, T.; Patterson, I.; Tarlinton, L.; Kim, L.; Woo, H. Expanding the Role of PSMA PET in Active Surveillance. BMC Urol. 2023, 23, 77. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study | Design | Population | Key Findings |
|---|---|---|---|
| Ahmed et al. (2017)—PROMIS [7] | Paired-cohort confirmatory test comparing MP-MRI against TRUS-biopsy with template biopsy as reference | Biopsy-naïve | Multiparametric MRI (mpMRI) had a sensitivity of 93% for detecting clinically significant prostate cancer (Gleason score ≥ 3 + 4), compared to 48% with standard TRUS-guided biopsy. The negative predictive value of mpMRI was 89%. Additionally, using mpMRI could have spared 27% of men from undergoing a biopsy. |
| Kasivisvanathan et al. (2018)—PRECISION [35] | Randomized non-inferiority trial comparing MRI-targeted biopsies against standard 12-core biopsy | Biopsy-naïve | In the mpMRI-targeted biopsy group, 38% of men were diagnosed with clinically significant prostate cancer (Gleason score ≥ 3 + 4) compared to 26% in the standard TRUS-guided biopsy group. The number of men diagnosed with clinically insignificant prostate cancer (Gleason score ≤ 3 + 3) was lower in the mpMRI group (9%) compared to the TRUS group (22%). The study also showed that 28% of men could avoid a biopsy entirely if the mpMRI did not show any suspicious lesions. |
| Rouvière et al. (2019)—MRI First [36] | Paired diagnostic study comparing mpMRI-targeted biopsies against standard biopsy | Biopsy-naïve | mpMRI followed by targeted biopsy detected 51% of clinically significant prostate cancers (Gleason score ≥ 3 + 4) compared to 37% detected by systematic biopsy alone. The study also noted that 23% of men could avoid a biopsy if the mpMRI showed no suspicious lesions, and the approach led to fewer diagnoses of clinically insignificant cancers (4% with MRI-targeted biopsy vs. 12% with systematic biopsy). |
| Sidana et al. (2018) [37] | Retrospective multicentre analysis comparing targeted and systematic biopsies | Prior negative biopsies | Targeted prostate biopsy detected clinically significant cancer in 26.3% of patients, whereas 12-core systematic biopsy detected it in 18.8% of patients, with systematic biopsy diagnosing only an additional 4.4%. |
| Ouzzane et al. (2015) [38] | Prospective multicenter study comparing systematic biopsies to mpMRI targeted biopsy | Active surveillance | mpMRI-targeted biopsies found that 10% of men deemed eligible for active surveillance with positive mpMRI were found to have clinically significant prostate cancer on targeted biopsy specimens. |
| Klotz et al. (2019)—ASIST [39] | Randomized trial comparing systematic biopsy with systematic and mpMRI targeted biopsy | Active surveillance | mpMRI-targeted biopsy did not significantly improve the clinically significant prostate cancer detection rate (mpMRI-targeted 21.2% vs. systematic 22.8% ≥ GG2). |
| Study | Design | Population | Key Findings |
|---|---|---|---|
| Klotz et al. (2020) [66] | Multicenter, prospective registry comparing mpMRI and microUS | 1040 patients, 352 with prior biopsy, with 286 prior negative | microUS found to have higher sensitivity compared to mpMRI (94% vs. 90%, p = 0.03) and NPV (85% vs. 77%, p = 0.04) for the detection of clinically significant prostate cancer (≥GG2) |
| Lughezzani et al. (2021) [67] | Single-institution cohort study | 320 patients, with 200 biopsy-naïve | microUS found to have a sensitivity of 89.7% and NPV of 81.5% for the detection of csPCa, with a higher sensitivity and NPV for patients undergoing repeat biopsy |
| Albers et al. (2022) [58] | Single-institution cohort study comparing microUS and mpMRI | Active surveillance | microUS found to have a sensitivity of 97% and NPV of 97% with an mpMRI sensitivity of 85% and NPV of 91% for the detection of csPCa |
| Maffei et al. (2023) [68] | Single-institution cohort study comparing microUS and mpMRI | Active surveillance—confirmatory biopsy | microUS found to have 94.1% sensitivity and NPV of 88.9% with an mpMRI sensitivity of 100% and NPV of 100% for the detection of csPCa |
| Klotz et al.—OPTIMUM [55] | Three-arm multicentered randomized controlled trial, comparing mpMRI/microUS, microUS only, and mpMRI/US fusion biopsy | Biopsy-naïve | Trial ongoing, planned enrollment of 1200 men with interim analysis planned at 600 patients. NCT05220501 |
| Kinnaird et al.—MUSIC-AS | Multicenter paired diagnostic trial comparing mpMRI and microUS | Active surveillance | Trial ongoing, planned enrollment of 210 men. NCT05558241 |
| Study | Design | Population | Key Findings |
|---|---|---|---|
| Pepe et al. (2022) [105] | Single-institution cohort study comparing 68Ga-PSMA-11/CT and mpMRI | Mix of biopsy-naïve and repeat biopsy | PSMA PET/CT-targeted biopsy had a sensitivity of 95.4% compared to MRI with 81.8% for the detection of csPCa. PSMA PET had an NPV of 96.5% compared with 87.5% for MRI. |
| Lopci et al. (2018) [106] | Single-institution prospective observational study assessing 68Ga-PSMA | Prior negative biopsy | Of the 45 men enrolled, 25 had positive PSMA PET/CT scans, with csPCa found in 7 men. |
| Pepe et al. (2023) [107] | Single-institution cohort study comparing 68Ga-PSMA-11 PET/CT and mpMRI | Active surveillance | Only three men found to have csPCa, with MRI detecting 66% and PSMA PET/CT also 66%. |
| Emmett et al. (2021)—PRIMARY [91] | Prospective, multicentered, paired diagnostic trial of 68Ga-PSMA-11 PET/CT and mpMRI | Biopsy-naïve | Combination of PSMA PET/CT + MRI improved NPV from 72% for MRI alone to 91% (p < 0.001) for the detection of csPCa. The sensitivity with the addition of PSMA PET/CT improved from 83% to 97% (p < 0.001), with an associated reduction in specificity from 53% to 40% (p = 0.011). |
| Krausewitz et al.—DEPROMP [108] | Prospective trial assessing the benefit of adding 68Ga-PSMA-11 PET/CT to standard-of-care mpMRI-guided prostate biopsy | Biopsy-naïve | Trial ongoing, with planned recruitment of 230 men. Interim analysis found the addition of PSMA-PET/CT to MRI results increased csPCa detection by 3% and PSMA-PET/CT was non-inferior to mpMRI for the detection of csPCa when used alone. |
| Lughezzani et al.—PROSPET-BX [109] | Prospective trial assessing the benefit of adding 68Ga-PSMA-11PET/CT to standard-of-care mpMRI-guided prostate biopsy | Prior negative biopsy | Trial ongoing, with planned recruitment of 128 men. (NCT05297162) Interim analysis found the addition of PSMA PET/CT to MRI results detected 90% of csPCa. |
| Thompson et al. [110] | Prospective multicentered trial assessing 68Ga-PSMA-11 PET/CT in addition to mpMRI | Active surveillance | Trial ongoing, with planned recruitment of 225 men. (ACTRN12622000188730) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albers, P.; Kinnaird, A. Advanced Imaging for Localized Prostate Cancer. Cancers 2024, 16, 3490. https://doi.org/10.3390/cancers16203490
Albers P, Kinnaird A. Advanced Imaging for Localized Prostate Cancer. Cancers. 2024; 16(20):3490. https://doi.org/10.3390/cancers16203490
Chicago/Turabian StyleAlbers, Patrick, and Adam Kinnaird. 2024. "Advanced Imaging for Localized Prostate Cancer" Cancers 16, no. 20: 3490. https://doi.org/10.3390/cancers16203490
APA StyleAlbers, P., & Kinnaird, A. (2024). Advanced Imaging for Localized Prostate Cancer. Cancers, 16(20), 3490. https://doi.org/10.3390/cancers16203490