
Optimal Treatment Strategy for Oligo-Recurrence Lung Cancer Patients with Driver Mutations

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
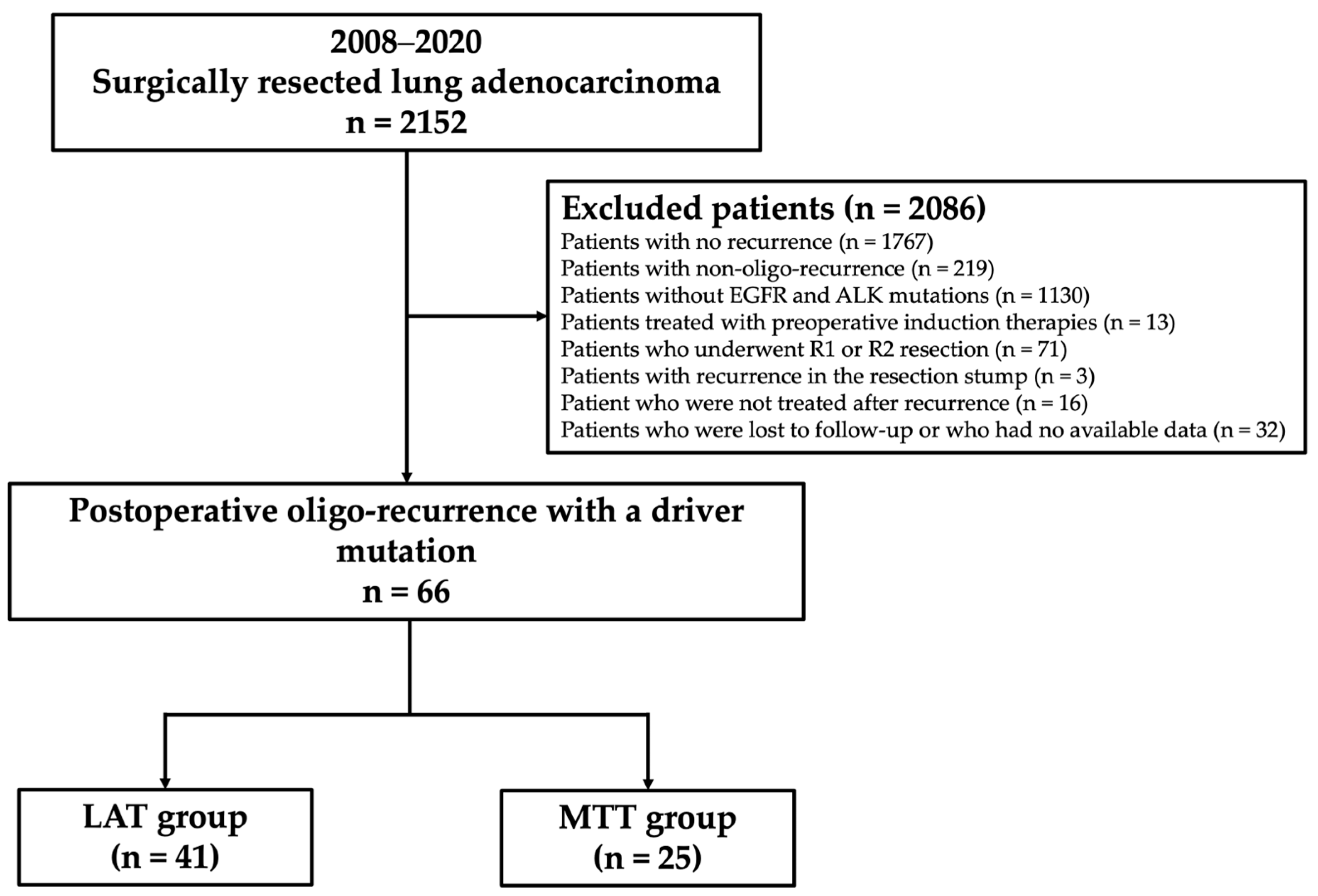
2.1. Study Design and Patient Selection
2.2. Postoperative Surveillance and Definition of Recurrence Patterns and Initial Therapies Post-Recurrence
2.3. Detection of Driver Mutations
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
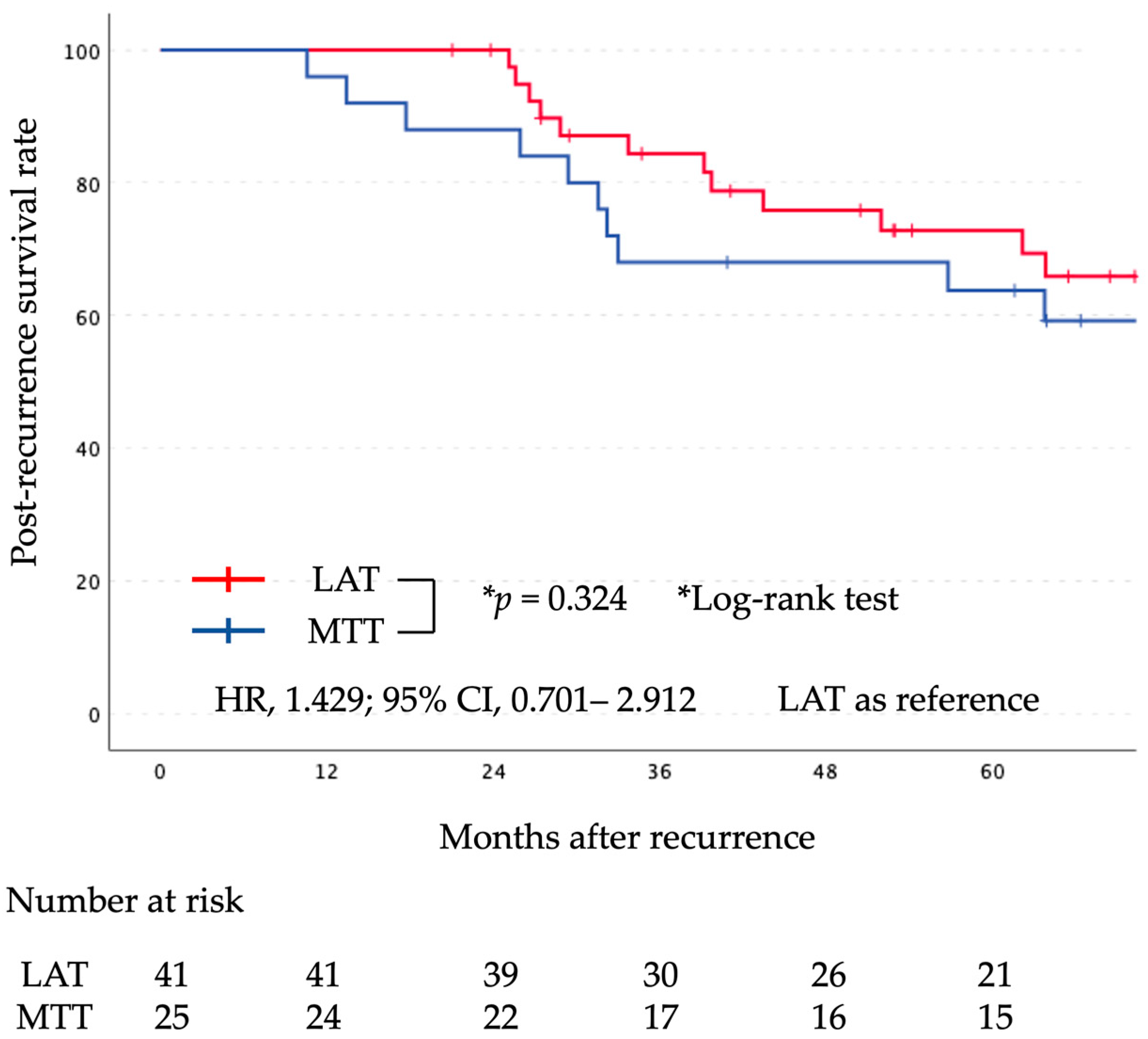
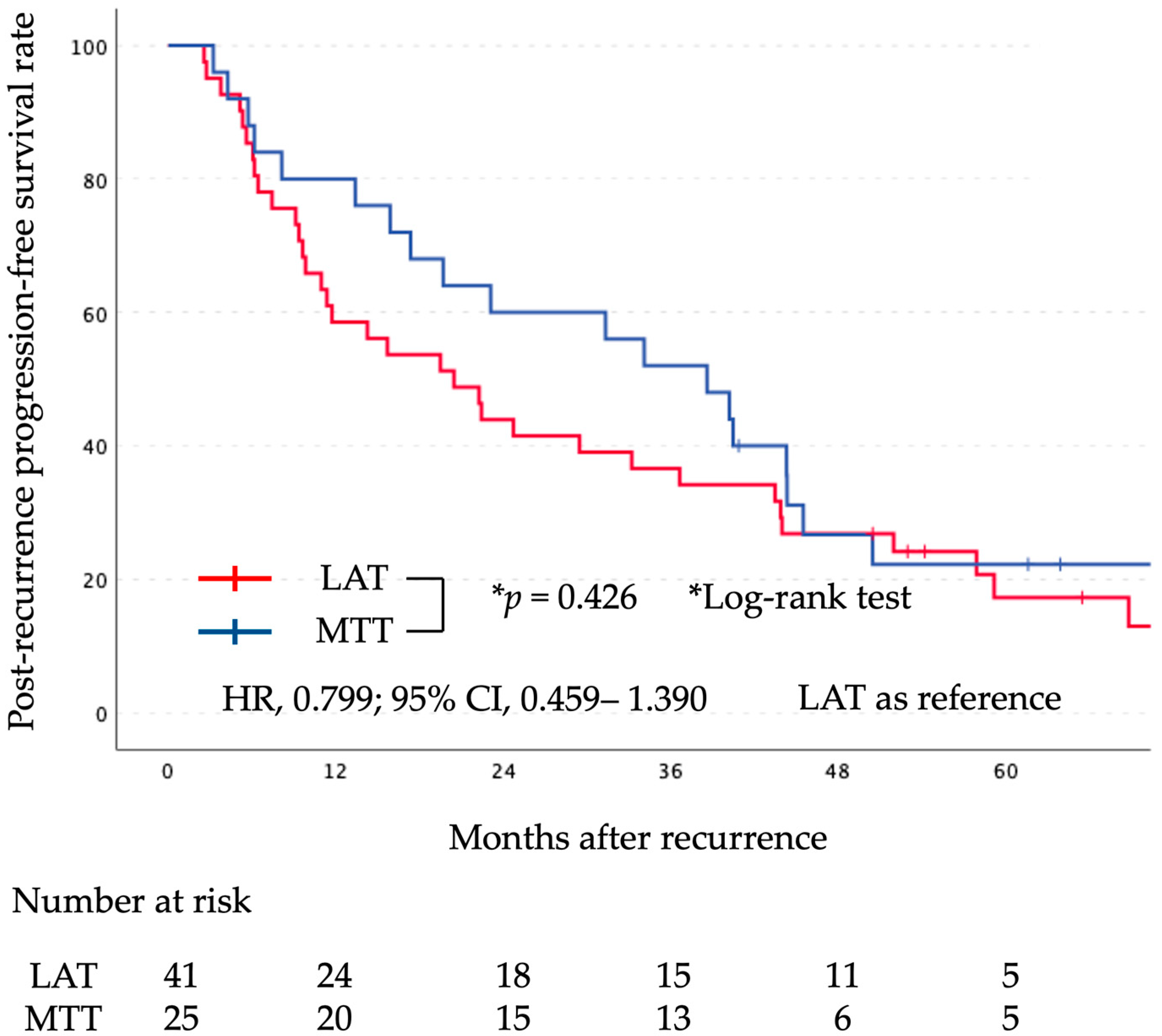
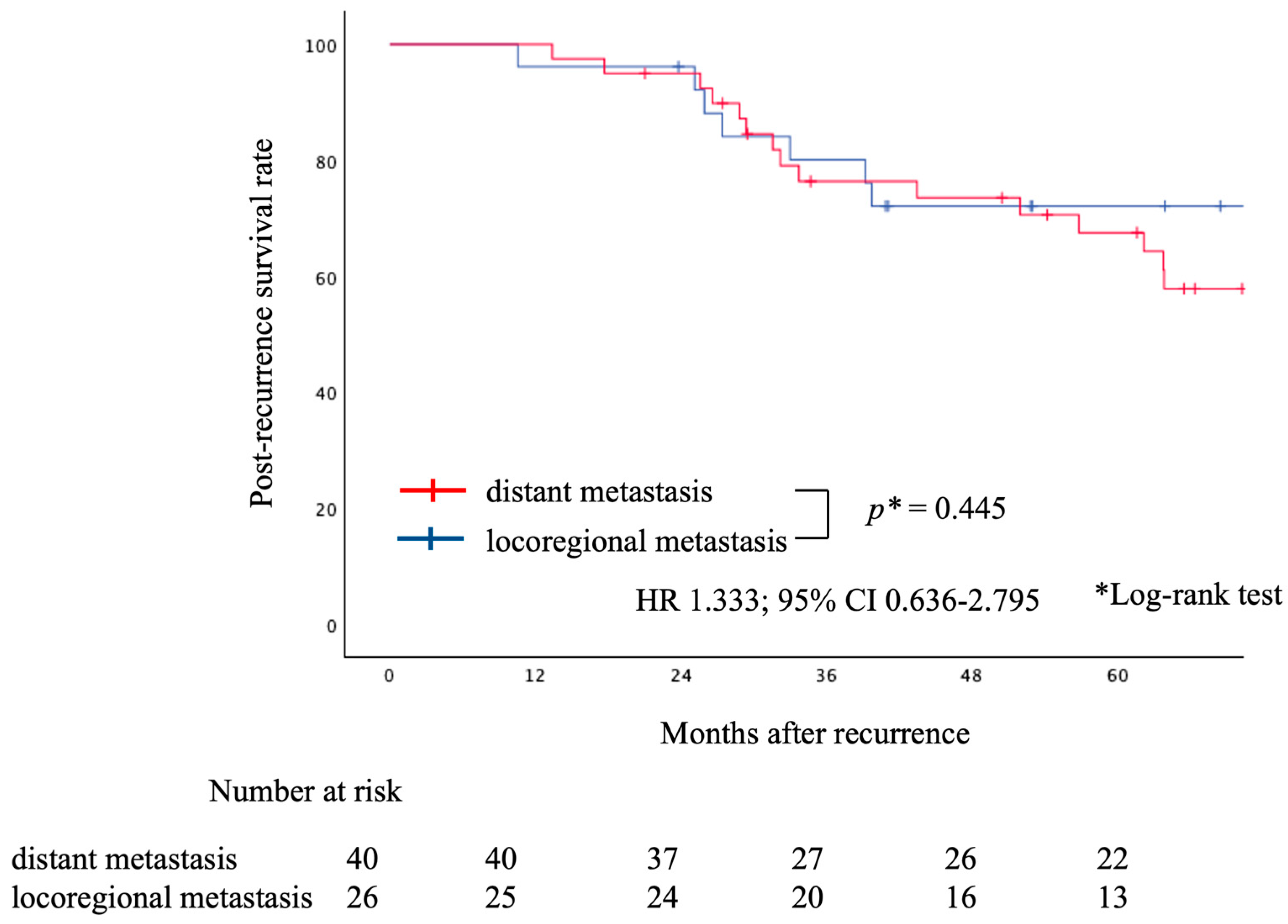
3.2. Prognostic Analyses
4. Discussion
4.1. Primary Findings
4.2. Post-Recurrence Therapies for Oligo-Recurrence Patients with Driver Mutations
4.3. Interpretation of the Study Findings
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lynch, T.J.; Bell, D.W.; Sordella, R. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004, 350, 2129–2139. [Google Scholar] [CrossRef] [PubMed]
- Paez, J.G.; Jänne, P.A.; Lee, J.C. EGFR mutations in lung cancer: Correlation with clinical response to gefitinib therapy. Science 2004, 304, 1497–1500. [Google Scholar] [CrossRef] [PubMed]
- Kwak, E.L.; Bang, Y.J.; Camidge, D.R. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Evans, T.; Gettinger, S. Treatment of stage IV non-small cell lung cancer: Diagnosis and management of lung cancer, diagnosis and management of lung cancer, 3rd ed. American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e341S–e368S. [Google Scholar] [CrossRef]
- Patel, P.R.; Yoo, D.S.; Niibe, Y. A call for the aggressive treatment of oligometastatic and oligo-recurrent non-small cell lung cancer. Pulm. Med. 2012, 2012, 480961. [Google Scholar] [CrossRef]
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef]
- Gomez, D.R.; Blumenschein, G.R.; Lee, J.J. Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: A multicentre, randomised, controlled, phase 2 study. Lancet Oncol. 2016, 17, 1672–1682. [Google Scholar] [CrossRef]
- Gomez, D.R.; Tang, C.; Zhang, J. Local consolidative therapy vs. maintenance therapy or observation for patients with oligometastatic non–small-cell lung cancer: Long-term results of a multi-institutional, phase II, randomized study. J. Clin. Oncol. 2019, 37, 1558–1565. [Google Scholar] [CrossRef]
- Puneeth Iyengar, P.; Wardak, Z.; Gerber, D.E. Consider elaborating on how post-recurrence treatments were selected: Was it standardized or physician-dependent? Were the cases discussed at a multidisciplinary tumour board? A few comments on factors influencing choices would be informative. JAMA Oncol. 2018, 4, e173501. [Google Scholar] [CrossRef]
- Hishida, T.; Yoshida, J.; Aokage, K. Postoperative oligo-recurrence of non-small-cell lung cancer: Clinical features and survival. Eur. J. Cardiothorac. Surg. 2016, 49, 847–853. [Google Scholar] [CrossRef]
- Travis, W.D.; Asamura, H.; Bankier, A.A. The IASLC lung cancer staging project: Proposals for coding T categories for subsolid nodules and assessment of tumor size in part-solid tumors in the forthcoming eighth edition of the TNM classification of lung cancer. J. Thorac. Oncol. 2016, 11, 1204–1223. [Google Scholar] [CrossRef]
- Travis, W.D.; Ladanyi, M.; Scagliotti, G. Adenocarcinoma. In WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th ed.; Travis, W.D., Brambilla, E., Burke, A.P., Marx, A., Nicholson, A.G., Eds.; Agency for Research on Cancer: Lyon, France, 2015; pp. 26–37. [Google Scholar]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Ashworth, A.; Rodrigues, G.; Boldt, G. Is there an oligometastatic state in non-small cell lung cancer? A systematic review of the literature. Lung Cancer 2013, 82, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Heeke, S.; Benzaquen, J.; Hofman, V. Critical assessment in routine clinical practice of liquid biopsy for EGFR status testing in non–small-cell lung cancer: A single-laboratory experience (LPCE, Nice, France). Clin. Lung Cancer 2020, 21, 56–65.e8. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, K.; Togashi, Y.; Kamihara, Y. Prospective and clinical validation of ALK immunohistochemistry: Results from the phase I/II study of alectinib for ALK-positive lung cancer (AF-001JP study). Ann. Oncol. 2016, 27, 185–192. [Google Scholar] [CrossRef]
- Matsuguma, H.; Nakahara, R.; Wakamatsu, I. Definitive local therapy for oligo-recurrence in patients with completely resected non-small cell lung cancer. Am. J. Clin. Oncol. 2020, 43, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Niibe, Y.; Hayakawa, K. Oligometastases and oligo-recurrence: The new era of cancer therapy. JPN J. Clin. Oncol. 2010, 40, 107–111. [Google Scholar] [CrossRef]
- Sonoda, D.; Matsuura, Y.; Kondo, Y. A Reasonable Definition of Oligo-Recurrence in Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2022, 23, 82–90. [Google Scholar] [CrossRef]
- Niibe, Y.; Nishimura, T.; Inoue, T. Oligo-recurrence predicts favorable prognosis of brain-only oligometastases in patients with non-small cell lung cancer treated with stereotactic radiosurgery or stereotactic radiotherapy: A multiinstitutional study of 61 subjects. BMC Cancer 2016, 16, 659. [Google Scholar] [CrossRef]
- Niibe, Y.; Yamamoto, T.; Onishi, H. Pulmonary oligometastases treated be stereotactic body radiation therapy. Anticancer Res. 2020, 40, 393–399. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Kosaka, T.; Endoh, H. Mutations of the epidermal growth factor receptor gene predict prolonged survival after gefitinib treatment in patients with non-small-cell lung cancer with postoperative recurrence. J. Clin. Oncol. 2005, 23, 2513–2520. [Google Scholar] [CrossRef]
- Matsuura, Y.; Ninomiya, H.; Ichinose, J. Prognostic impact and distinctive characteristics of surgically resected anaplastic lymphoma kinase-rearranged lung adenocarcinoma. JTCS 2022, 163, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Moriya, T.; Hamaji, M.; Yoshizawa, A. Epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors as a first-line treatment for postoperative recurrent and EGFR- mutated non-small-cell lung cancer. Interact. Cardiovasc. Thorac. Surg. 2022, 34, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.S.; Bai, Y.F.; Verma, V. Randomized Trial of First-Line Tyrosine Kinase Inhibitor With ir Without Radiotherapy for Synchronous Oligometastic EGFR-Mutated Non-Small Cell Lung Cancer. J. Natl. Cancer Inst. 2023, 115, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Tahsin, M.K.; Emily, A.V.; Saumil, G. Osimertinib. Surgery, and radiation therapy in treating patients with stage IIIB or IV non-small cell lung cancer with EGFR mutations (NORTHSTAR). Ann. Surg. Oncol. 2022, 29, 4688–4689. [Google Scholar] [CrossRef]
- Taichi, M.; Hirotsugu, K.; Hideyuki, H. Phase II Study of Multidisciplinary Therapy using Pembrolizumab for Patients with Synchronous Oligometastatic Stage IV Non-Small Cell Lung Cancer (TRAP OLIGO study) (WJOG11118L). BMC Cancer 2021, 21, 1121. [Google Scholar] [CrossRef]
- Sonoda, D.; Kondo, Y.; Maruyama, R. Examination of the effectiveness of local therapy for oligo-recurrence of EGFR-mutated NSCLC. Thorac. Cancer 2023, 14, 766–772. [Google Scholar] [CrossRef]
- Dingemans, A.C.; Hendriks, L.E.L.; Berghmans, T. Definition of synchronous oligometastatic non-small cell lung cancer-A consensus report. J. Thorac. Oncol. 2019, 14, 2109–2119. [Google Scholar] [CrossRef]
- Guckenberger, M.; Lievens, Y.; Bouma, A.B. Characterisation and classification of oligometastatic disease. Lancet Oncol. 2020, 21, e18–e28. [Google Scholar] [CrossRef]
- Levy, A.; Hendriks, L.E.L.; Berghmans, T. EORTC Lung Cancer Group survey on the definition of NSCLC synchronous oligometastatic disease. Eur. J. Cancer 2019, 122, 109–114. [Google Scholar] [CrossRef]
- Presley, C.J.; Tang, D.; Soulos, P.R. Association of broad-based genomic sequencing with survival among patients with advanced non-small cell lung cancer in the community oncology setting. JAMA 2018, 320, 469–477. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Initial LAT (n = 41) | Initial MTT (n = 25) | p-Value * |
|---|---|---|---|
| Age, years | |||
| median (IQR) | 66 (61–73) | 65 (56–75) | 0.431 |
| Sex, | |||
| male, n (%) | 16 (39) | 11 (44) | 0.690 |
| Smoking status, | |||
| pack-years, median (IQR) | 2 (0–550) | 5 (0–197) | 0.951 |
| Pathological stage **, | |||
| I/II/III, n (%) | 18 (44)/8 (20)/15 (37) | 3 (12)/8 (32)/14 (56) | 0.026 |
| Tumor size, mm, | |||
| median (IQR) | 28 (23–36) | 28 (20–43) | 0.776 |
| Driver mutation, | |||
| EGFR/ALK, n (%) | 58 (88)/8 (12) | 21 (84)/4 (16) | 0.451 |
| Histological differentiation, well/moderate/poor, n (%) | 2 (5)/32 (78)/7 (17) | 4 (16)/18 (72)/3 (12) | 0.293 |
| Lymphatic invasion, n (%) | 24 (59) | 16 (64) | 0.659 |
| Vascular invasion, n (%) | 30 (73) | 20 (80) | 0.530 |
| Visceral pleural invasion, n (%) | 23 (56) | 14 (56) | 0.994 |
| Intrapulmonary metastasis, n (%) | 7 (17) | 7 (28) | 0.292 |
| Initial recurrence site, | |||
| locoregional/distant/both, n (%) | 18 (43)/21 (51)/2 (5) | 8 (32)/15 (60)/2 (8) | 0.598 |
| Number of recurrence lesions, n (%) | |||
| 1 | 32 (78) | 5 (20) | |
| 2 | 7 (17) | 14 (56) | |
| 3 | 2 (5) | 6 (24) | <0.001 |
| Time from recurrence to treatment, months, median (IQR) | 1 (0–2) | 1 (0–6) | 0.658 |
| Time from recurrence to initiation of MTT, months, median (IQR) | 33 (12–53) | 1 (1–7) | <0.001 |
| Initial Recurrence Site ** | Initial LAT (n = 41) | Initial MTT (n = 25) | p-Value * |
|---|---|---|---|
| Locoregional recurrence, n | 20 | 10 | 0.487 |
| Regional lymph node stations | 12 | 6 | |
| Ipsilateral lung | 8 | 4 | |
| Distant recurrence, n | 23 | 17 | 0.337 |
| Brain | 15 | 2 | |
| Contralateral lung | 3 | 7 | |
| Liver | 1 | 4 | |
| Bone | 7 | 3 | |
| Adrenal gland | 0 | 2 | |
| Initial therapy post-recurrence, n (%) | |||
| Surgical resection | 15 (37) | ||
| Cerebral stereotactic radiosurgery | 14 (34) | ||
| Other radiotherapies | 14 (34) | ||
| EGFR-MTTs | 21 (84) | ||
| ALK-MTTs | 4 (16) | ||
| Subsequent administration of LATs, n (%) | 6 (24) | ||
| Subsequent administration of MTTs, n (%) | 23 (56) | ||
| Number of MTTs used, median (range) | 1 (0–4) | 1 (1–3) | 0.249 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tachibana, T.; Matsuura, Y.; Ninomiya, H.; Ichinose, J.; Nakao, M.; Okumura, S.; Nishio, M.; Ikeda, N.; Mun, M. Optimal Treatment Strategy for Oligo-Recurrence Lung Cancer Patients with Driver Mutations. Cancers 2024, 16, 464. https://doi.org/10.3390/cancers16020464
Tachibana T, Matsuura Y, Ninomiya H, Ichinose J, Nakao M, Okumura S, Nishio M, Ikeda N, Mun M. Optimal Treatment Strategy for Oligo-Recurrence Lung Cancer Patients with Driver Mutations. Cancers. 2024; 16(2):464. https://doi.org/10.3390/cancers16020464
Chicago/Turabian StyleTachibana, Taimei, Yosuke Matsuura, Hironori Ninomiya, Junji Ichinose, Masayuki Nakao, Sakae Okumura, Makoto Nishio, Norihiko Ikeda, and Mingyon Mun. 2024. "Optimal Treatment Strategy for Oligo-Recurrence Lung Cancer Patients with Driver Mutations" Cancers 16, no. 2: 464. https://doi.org/10.3390/cancers16020464
APA StyleTachibana, T., Matsuura, Y., Ninomiya, H., Ichinose, J., Nakao, M., Okumura, S., Nishio, M., Ikeda, N., & Mun, M. (2024). Optimal Treatment Strategy for Oligo-Recurrence Lung Cancer Patients with Driver Mutations. Cancers, 16(2), 464. https://doi.org/10.3390/cancers16020464