
The Emerging Role of Tertiary Lymphoid Structures in Breast Cancer: A Narrative Review

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
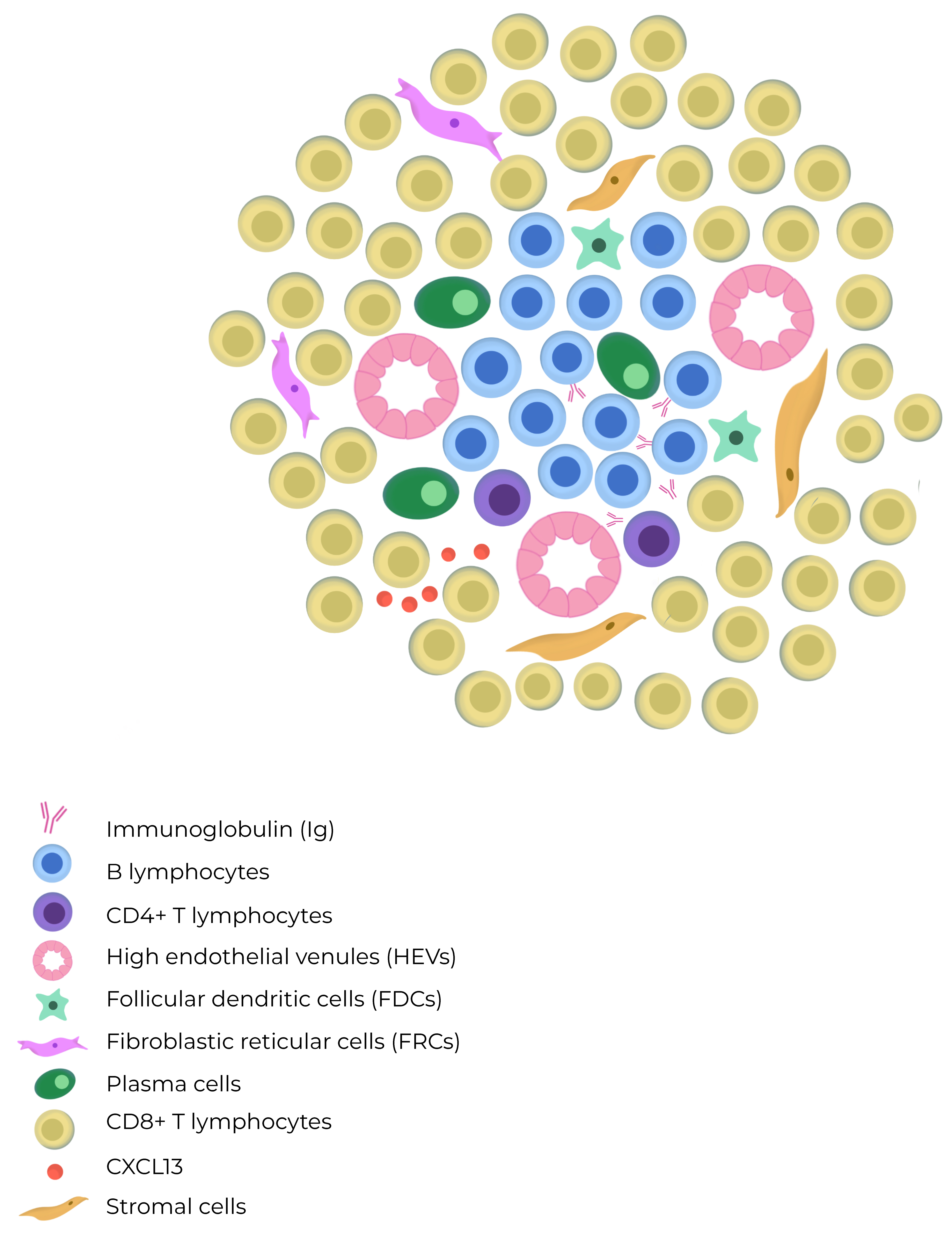
3.1. Organization of TLSs
3.2. Role in Solid Tumors
3.3. TLS in Breast Cancer
3.3.1. HER2-Positive Tumors
3.3.2. HR-Positive Breast Tumors
3.3.3. Triple-Negative Breast Tumors
3.4. Metastatic Breast Cancer
3.5. Diagnosis of TLSs
3.6. Single-Cell scRNA-Seq Evidence on TLSs in Breast Cancer
3.7. TLS as a Predictive Factor for Immunotherapy Response
3.8. TLS Manipulation as Therapeutic Opportunity
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schmid, P.; Cortes, J. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Tsang, J.Y.S. Distinct Tertiary Lymphoid Structure Associations and Their Prognostic Relevance in HER2 Positive and Negative Breast Cancers. Oncologist 2017, 22, 1316–1324. [Google Scholar] [CrossRef]
- Tarantino, P.; Gandini, S. Immunotherapy addition to neoadjuvant chemotherapy for early triple negative breast cancer: A systematic review and meta-analysis of randomized clinical trials. Crit. Rev. Oncol. Hematol. 2021, 159, 103223. [Google Scholar] [CrossRef]
- Luo, S. Chronic Inflammation: A Common Promoter in Tertiary Lymphoid Organ Neogenesis. Front. Immunol. 2019, 10, 2938. [Google Scholar] [CrossRef] [PubMed]
- Wakasu, S.; Tagawa, T. Preventive effect of tertiary lymphoid structures on lymph node metastasis of lung adenocarcinoma. Cancer Immunol. Immunother. 2023, 72, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- Horeweg, N.; Workel, H.H. Tertiary lymphoid structures critical for prognosis in endometrial cancer patients. Nat. Commun. 2022, 13, 1373. [Google Scholar] [CrossRef]
- Di Caro, G.; Bergomas, F. Occurrence of tertiary lymphoid tissue is associated with T-cell infiltration and predicts better prognosis in early-stage colorectal cancers. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 2147–2158. [Google Scholar] [CrossRef]
- Trüb, M.; Zippelius, A. Tertiary Lymphoid Structures as a Predictive Biomarker of Response to Cancer Immunotherapies. Front. Immunol. 2021, 12, 674565. [Google Scholar] [CrossRef]
- Solinas, C.; Garaud, S. Immune Checkpoint Molecules on Tumor-Infiltrating Lymphocytes and Their Association with Tertiary Lymphoid Structures in Human Breast Cancer. Front. Immunol. 2017, 8, 1412. [Google Scholar] [CrossRef]
- Brandum, E.P.; Jørgensen, A.S. Dendritic Cells and CCR7 Expression: An Important Factor for Autoimmune Diseases, Chronic Inflammation, and Cancer. Int. J. Mol. Sci. 2021, 22, 8340. [Google Scholar] [CrossRef]
- Vaghjiani, R.G.; Skitzki, J.J. Tertiary Lymphoid Structures as Mediators of Immunotherapy Response. Cancers 2022, 14, 3748. [Google Scholar] [CrossRef]
- Zhang, N.; Wang, D. Analysis of immune status in gastric adenocarcinoma with different infiltrating patterns and origin sites. Front. Immunol. 2022, 13, 978715. [Google Scholar] [CrossRef]
- Colbeck, E.J.; Ager, A. Tertiary Lymphoid Structures in Cancer: Drivers of Antitumor Immunity, Immunosuppression, or Bystander Sentinels in Disease? Front. Immunol. 2017, 8, 1830. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Zhu, M. Lymphotoxin signalling in tertiary lymphoid structures and immunotherapy. Cell. Mol. Immunol. 2017, 14, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Meylan, M.; Petitprez, F. Tertiary lymphoid structures generate and propagate anti-tumor antibody-producing plasma cells in renal cell cancer. Immunity 2022, 55, 527–541.e5. [Google Scholar] [CrossRef]
- Weiner, L.M.; Surana, R. Monoclonal antibodies: Versatile platforms for cancer immunotherapy. Nat. Rev. Immunol. 2010, 10, 317–327. [Google Scholar] [CrossRef]
- Harris, R.J.; Cheung, A. Tumor-Infiltrating B Lymphocyte Profiling Identifies IgG-Biased, Clonally Expanded Prognostic Phenotypes in Triple-Negative Breast Cancer. Cancer Res. 2021, 81, 4290–4304. [Google Scholar] [CrossRef] [PubMed]
- Calderaro, J.; Petitprez, F. Intra-tumoral tertiary lymphoid structures are associated with a low risk of early recurrence of hepatocellular carcinoma. J. Hepatol. 2019, 70, 58–65. [Google Scholar] [CrossRef]
- Posch, F.; Silina, K. Maturation of tertiary lymphoid structures and recurrence of stage II and III colorectal cancer. Oncoimmunology 2018, 7, e1378844. [Google Scholar] [CrossRef]
- Meshcheryakova, A.; Tamandl, D. B cells and ectopic follicular structures: Novel players in anti-tumor programming with prognostic power for patients with metastatic colorectal cancer. PLoS ONE 2014, 9, e99008. [Google Scholar] [CrossRef]
- Sautès-Fridman, C.; Petitprez, F. Tertiary lymphoid structures in the era of cancer immunotherapy. Nat. Rev. Cancer 2019, 19, 307–325. [Google Scholar] [CrossRef] [PubMed]
- Vanhersecke, L.; Brunet, M.; Guégan, J.P.; Rey, C.; Bougouin, A.; Cousin, S.; Le Moulec, S.; Besse, B.; Loriot, Y.; Larroquette, M.; et al. Mature tertiary lymphoid structures predict immune checkpoint inhibitor efficacy in solid tumors independently of PD-L1 expression. Nat. Cancer 2021, 2, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Huang, X. Tertiary lymphoid structures favor outcome in resected esophageal squamous cell carcinoma. J. Pathol. Clin. Res. 2022, 8, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Liu, X. Prognostic value of tertiary lymphoid structure and tumour infiltrating lymphocytes in oral squamous cell carcinoma. Int. J. Oral. Sci. 2020, 12, 24. [Google Scholar] [CrossRef]
- Germain, C.; Gnjatic, S. Presence of B cells in tertiary lymphoid structures is associated with a protective immunity in patients with lung cancer. Am. J. Respir. Crit. Care Med. 2014, 189, 832–844. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, N.; Gil-Jimenez, A. The Tumor Immune Landscape and Architecture of Tertiary Lymphoid Structures in Urothelial Cancer. Front. Immunol. 2021, 12, 793964. [Google Scholar] [CrossRef]
- Lynch, K.T.; Young, S.J. Heterogeneity in tertiary lymphoid structure B-cells correlates with patient survival in metastatic melanoma. J. Immunother. Cancer. 2021, 9, e002273. [Google Scholar] [CrossRef]
- Cabrita, R.; Lauss, M. Tertiary lymphoid structures improve immunotherapy and survival in melanoma. Nature 2020, 577, 561–565. [Google Scholar] [CrossRef]
- Italiano, A.; Bessede, A. Pembrolizumab in soft-tissue sarcomas with tertiary lymphoid structures: A phase 2 PEMBROSARC trial cohort. Nat. Med. 2022, 28, 1199–1206. [Google Scholar] [CrossRef]
- Gatti-Mays, M.E.; Balko, J.M. Gameiro SR. If we build it they will come: Targeting the immune response to breast cancer. npj Breast Cancer 2019, 5, 37. [Google Scholar] [CrossRef]
- de Jong, V.M.T.; Wang, Y. Prognostic Value of Stromal Tumor-Infiltrating Lymphocytes in Young, Node-Negative, Triple-Negative Breast Cancer Patients Who Did Not Receive (neo)Adjuvant Systemic Therapy. J. Clin. Oncol. 2022, 40, 2361–2374. [Google Scholar] [CrossRef] [PubMed]
- Gu-Trantien, C.; Loi, S. CD4+ follicular helper T cell infiltration predicts breast cancer survival. J. Clin. Investig. 2013, 123, 2873–2892. [Google Scholar] [CrossRef]
- Li, R.; Berglund, A. The 12-CK Score: Global Measurement of Tertiary Lymphoid Structures. Front. Immunol. 2021, 12, 694079. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Liu, J. The Presence of Tertiary Lymphoid Structures Provides New Insight Into the Clinicopathological Features and Prognosis of Patients With Breast Cancer. Front. Immunol. 2022, 13, 868155. [Google Scholar] [CrossRef]
- Kang, W.; Feng, Z. Tertiary Lymphoid Structures in Cancer: The Double-Edged Sword Role in Antitumor Immunity and Potential Therapeutic Induction Strategies. Front. Immunol. 2021, 12, 689270. [Google Scholar] [CrossRef]
- Mauldin, I.S.; Mahmutovic, A. Multiplex Immunofluorescence Histology for Immune Cell Infiltrates in Melanoma-Associated Tertiary Lymphoid Structures. Methods Mol. Biol. 2021, 2265, 573–587. [Google Scholar] [PubMed]
- Mustapha, R.; Ng, K. Insights Into Unveiling a Potential Role of Tertiary Lymphoid Structures in Metastasis. Front. Mol. Biosci. 2021, 8, 661516. [Google Scholar] [CrossRef]
- Jacquelot, N.; Tellier, J.; Nutt, S.; Belz, G. Tertiary lymphoid structures and B lymphocytes in cancer prognosis and response to immunotherapies. Oncoimmunology 2021, 10, 1900508. [Google Scholar]
- Lee, H.J.; Park, I.A. Tertiary lymphoid structures: Prognostic significance and relationship with tumour-infiltrating lymphocytes in triple-negative breast cancer. J. Clin. Pathol. 2016, 69, 422–430. [Google Scholar] [CrossRef]
- Song, I.H.; Heo, S.H. Predictive Value of Tertiary Lymphoid Structures Assessed by High Endothelial Venule Counts in the Neoadjuvant Setting of Triple-Negative Breast Cancer. Cancer Res. Treat. 2017, 49, 399–407. [Google Scholar] [CrossRef]
- Li, K.; Ji, J. Analysis of the Correlation and Prognostic Significance of Tertiary Lymphoid Structures in Breast Cancer: A Radiomics-Clinical Integration Approach. J. Magn. Reson. Imaging 2023. ahead-of-print. [Google Scholar] [CrossRef]
- Noël, G.; Fontsa, M. Functional Th1-oriented T follicular helper cells that infiltrate human breast cancer promote effective adaptive immunity. J. Clin. Investig. 2021, 131, e139905. [Google Scholar] [CrossRef]
- Blanchard, L.; Girard, J.P. High endothelial venules (HEVs) in immunity, inflammation and cancer. Angiogenesis 2021, 24, 719–753. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Jian, C.Z. Potential Role of CXCL13/CXCR5 Signaling in Immune Checkpoint Inhibitor Treatment in Cancer. Cancers 2022, 14, 294. [Google Scholar] [CrossRef]
- Prat, A.; Guarneri, V. Development and validation of the new HER2DX assay for predicting pathological response and survival outcome in early-stage HER2-positive breast cancer. eBioMedicine 2022, 75, 103801. [Google Scholar] [CrossRef]
- Sobottka, B.; Pestalozzi, B. Similar lymphocytic infiltration pattern in primary breast cancer and their corresponding distant metastases. Oncoimmunology 2016, 5, e1153208. [Google Scholar] [CrossRef]
- Yu, B.H.; Li, B.Z. Cytoplasmic FOXP1 expression is correlated with ER and calpain II expression and predicts a poor outcome in breast cancer. Diagn. Pathol. 2018, 13, 36. [Google Scholar] [CrossRef]
- Zhang, N.N.; Qu, F.J. Prognostic impact of tertiary lymphoid structures in breast cancer prognosis: A systematic review and meta-analysis. Cancer Cell Int. 2021, 21, 536. [Google Scholar] [CrossRef]
- Cardoso, F.; Bardia, A. KEYNOTE-756: Randomized, double-blind, phase III study of pembrolizumab vs placebo + neoadjuvant chemotherapy (CT) and adjuvant endocrine therapy (ET) for high-risk, early-stage estrogen receptor–positive human epidermal growth factor receptor 2–negative (ER+/HER2−) breast cancer (BC). Ann. Oncol. 2019, 30 (Suppl. S9), IX7–IX8. [Google Scholar]
- Deng, J.; Wang, E.S. CDK4/6 Inhibition Augments Antitumor Immunity by Enhancing T-cell Activation. Cancer Discov. 2018, 8, 216–233. [Google Scholar] [CrossRef]
- Zhou, L.; Xu, B. Tertiary lymphoid structure signatures are associated with survival and immunotherapy response in muscle-invasive bladder cancer. Oncoimmunology 2021, 10, 1915574. [Google Scholar] [CrossRef]
- Cortes, J.; Cescon, D.W. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Heo, S.H. Presence of tertiary lymphoid structures determines the level of tumor-infiltrating lymphocytes in primary breast cancer and metastasis. Mod. Pathol. 2019, 32, 70–80. [Google Scholar] [CrossRef]
- Alhesa, A.; Awad, H. PD-L1 expression in breast invasive ductal carcinoma with incomplete pathological response to neoadjuvant chemotherapy. Int. J. Immunopathol. Pharmacol. 2022, 36, 3946320221078433. [Google Scholar] [CrossRef] [PubMed]
- Badve; Sunil, S. Determining PD-L1 Status in Patients with Triple-Negative Breast Cancer: Lessons Learned From IMpassion130. J. Natl. Cancer Inst. 2022, 114, 664–675. [Google Scholar] [CrossRef] [PubMed]
- Buisseret, L.; Desmedt, C. Reliability of tumor-infiltrating lymphocyte and tertiary lymphoid structure assessment in human breast cancer. Mod. Pathol. 2017, 30, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Massa, D.; Tosi, A. Multiplexed In Situ Spatial Protein Profiling in the Pursuit of Precision Immuno-Oncology for Patients with Breast Cancer. Cancers 2022, 14, 4885. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Qiao, S. The gene signature of tertiary lymphoid structures within ovarian cancer predicts the prognosis and immunotherapy benefit. Front. Genet. 2023, 13, 1090640. [Google Scholar] [CrossRef] [PubMed]
- Rakaee, M.; Adib, E. Artificial intelligence in digital pathology approach identifies the predictive impact of tertiary lymphoid structures with immune-checkpoints therapy in NSCLC, Meeting Abstract|2022 ASCO Annual Meeting. J. Clin. Oncol. 2022, 40 (Suppl. S16), 9065. [Google Scholar] [CrossRef]
- Domblides, C.; Rochefort, J. Tumor-Associated Tertiary Lymphoid Structures: From Basic and Clinical Knowledge to Therapeutic Manipulation. Front. Immunol. 2021, 12, 698604. [Google Scholar] [CrossRef]
- Engelhard, V.H.; Rodriguez, A.B. Immune Cell Infiltration and Tertiary Lymphoid Structures as Determinants of Antitumor Immunity. J. Immunol. 2018, 200, 432–442. [Google Scholar] [CrossRef]
- Tallón de Lara, P.; Castañón, H. CD39+PD-1+CD8+ T cells mediate metastatic dormancy in breast cancer. Nat. Commun. 2021, 12, 769. [Google Scholar] [CrossRef] [PubMed]
- Wortman, J.C.; He, T.F. Spatial distribution of B cells and lymphocyte clusters as a predictor of triple-negative breast cancer outcome. Npj Breast Cancer. 2021, 7, 84. [Google Scholar] [CrossRef] [PubMed]
- Sofopoulos, M.; Fortis, S.P. The prognostic significance of peritumoral tertiary lymphoid structures in breast cancer. Cancer Immunol. Immunother. 2019, 68, 1733–1745. [Google Scholar] [CrossRef] [PubMed]
- De Silva, P.; Garaud, S. FOXP1 negatively regulates tumor infiltrating lymphocyte migration in human breast cancer. eBioMedicine 2019, 39, 226–238. [Google Scholar] [CrossRef]
- Wang, Q. Single-cell transcriptome sequencing of B-cell heterogeneity and tertiary lymphoid structure predicts breast cancer prognosis and neoadjuvant therapy efficacy. Clin. Transl. Med. 2023, 13, e1346. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, Z.X. Integrated analysis of single-cell and bulk RNA sequencing data reveals a pan-cancer stemness signature predicting immunotherapy response. Genome Med. 2022, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Clubb, J.H.A.; Kudling, T.V. Adenovirus Encoding Tumor Necrosis Factor Alpha and Interleukin 2 Induces a Tertiary Lymphoid Structure Signature in Immune Checkpoint Inhibitor Refractory Head and Neck Cancer. Front. Immunol. 2022, 13, 794251. [Google Scholar] [CrossRef] [PubMed]
- Zhong, K.; Xu, Y.; Cheng, Y.; Wen, Y.; Cai, L.; He, G.; Huang, H.; Fu, S.; Zhong, X.; Zheng, Y.; et al. Case report: Primary hepatocellular carcinoma with portal vein tumor thrombus characterized by active tumor immune microenvironment achieving a complete response following treatment of combined immunotherapy. Front. Immunol. 2022, 13, 999763. [Google Scholar] [CrossRef]
- Wang, L.; Gong, S. Genomic properties and clinical outcomes associated with tertiary lymphoid structures in patients with breast cancer. Sci. Rep. 2023, 13, 13542. [Google Scholar] [CrossRef]
- Fridman, W.H.; Sibéril, S. Activation of B cells in Tertiary Lymphoid Structures in cancer: Anti-tumor or anti-self? Semin. Immunol. 2023, 65, 101703. [Google Scholar] [CrossRef] [PubMed]
- Nasiri, F.; Kazemi, M. CAR-T cell therapy in triple-negative breast cancer: Hunting the invisible devil. Front. Immunol. 2022, 13, 1018786. [Google Scholar] [CrossRef] [PubMed]
- Johansson-Percival, A.; Ganss, R. Therapeutic Induction of Tertiary Lymphoid Structures in Cancer Through Stromal Remodeling. Front. Immunol. 2021, 12, 674375. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author | Year | Tumor Model | Sample Size | Tipo | Recognition of TLS | Findings |
|---|---|---|---|---|---|---|
| Rutao Li [23] | 2022 | Esophagus | 185 primary ESCC treated by surgical resection | Retrospective | IHC for CD45+, CD20+ B, CD4+ CD8+ T cells, CD11c+ DC | Better DFS (p = 0.0130) and OS (p = 0.0164). |
| Nana Zhang [12] | 2020 | Gastric adenocarcinoma | 180 gastric adenocarcinoma samples (surgery) | Retrospective | IHC staining and MECA-79 + (HEV) | Better OS (p = 0.007) |
| Qunxing Li [24] | 2020 | Oral Squamous cell carcinoma | 168 | Retrospective | Multiplex IHC (CD3+ T cells, CD20+ B cell, PNAd+ HEV DC-LAMP + (LAMP3) | Independent prognostic factor for 5-year OS rate (HR = 3.78) and RFS rate (HR = 3.29) |
| Sho Wakasu [5] | 2022 | Lung adeno carcinoma | 218 | Retrospective | The overlap of T-cell zone and B-cell zone | Better OS [HR] = 0.17, (p = 0.0220) and DFS (HR = 0.54, p = 0.0436). |
| Nanda Horeweg [6] | 2022 | Endometrial adenocarcinoma | 411 (All included patients from the PORTEC-3 study) | Retrospective | scRNA-seq of B-cells to establish the presence of cycling/germinal center B-cells and antibody-secreting B-cells | Better RFS, independent of clinicopathological and molecular factors |
| Di Caro et al. [7] | 2014 | Colorectal | 351 stage II and III colorectal cancer without any sign of metastatic disease | Retrospective | IHC (CD3, CD20, PNAd, Lyve-1, CD21, α-smooth muscle actin and CXCL13 and CCL21 | Better RFS (relapse; p = 0.03) |
| Posch et al. [19] | 2018 | Colo rectal | 109 patients with stage II/III nmCRC | Retrospective | NR | Better RR of recurrence. (HR for low TLS = 3.99, 95% CI: 1.30–12.20, p = 0.015 |
| Meshcheryakova et al. [20] | 2014 | Colo rectal | 65 metastatic colorectal cancer in the liver | Retrospective | IHQ (CD45, CD20, AID, IgM, CD138, and CD68) | Better RFS (p < 0.001) |
| Julien Calderaro [18] | 2019 | HCC | 273 patients with HCC treated by surgical resection | Retrospective | Pathological review NR | Lower risk of early relapse (<2 years after surgery, hazard ratio 0.46, p = 0.005). |
| Germain C. [25] | 2014 | Lung Cancer | 74 untreated patients with early-stage NSCLC | Retrospective | Immunohistochemistry. Characterization of CD20 B-cell subsets by flow cytometry. | Better OS Better DSS |
| Van Dijk [26] | 2021 | Urothelial cancer | 31 cystectomy specimens obtained from NABUCCO | Retrospective | Multiplex immunofluorescence (CD3, CD8, FoxP3, CD68, CD20, PanCK, DAPI) | Better RFS (p = 0.0097) |
| Lynch et al. [27] | 2021 | Melanoma (metastases) | 64 patients | Retrospective | Multiplex immunofluorescence. | Better OS (HR 0.51, p = 0.04) |
| Cabrita et al. [28] | 2020 | Melanoma | 177 | Retrospective | IHC Anti-CD20 AntiCXCR5 and Anti-CXCL13 | Better 5 year OS (p = 0.006) |
| Italiano et al. [29] | 2022 | Sarcomas | 30 samples | Multicohort phase 2 study of pembrolizumab combined with low-dose cyclophosphamide | NR | Better 6-month NPR (non-progression rate) NPR = 40% ORR 30% |
| Maxime Meylan [15] | 2022 | Renal cell cancer | Primary tumors (n = 130) from three cohorts of treatment-naïve patients with ccRCC | Retrospective | Visium 10X spatial transcriptomics technique that allowed both quantification and localization of B cell-specific gene expression. | Better PFS and response to ICI |
| Author | Breast Cancer Subtype | Type | N | Year of Publication | Recognition of TLS | Findings |
|---|---|---|---|---|---|---|
| Lee et al. [39] | TNBC localized | Retrospective | 769 | 2016 | IHC for MECA-79 and CD31 | Better DFS Better OS |
| Xia Liu [2] | HER2 + and negative breast cancer | Retrospective | 248 | 2017 | IHC CD3, CD20, and CD23 | Better DFS (log-rank = 4.054, p = 0.044) |
| Song [40] | TNBC localized | Retrospective | 108 TNBC patients treated with neoadjuvant chemotherapy | 2017 | IHC for MECA79, CD3, CD8, and CD20 and Nanostring analysis of CXCL13 | Better pCR Better DFS |
| Bin Wang [34] | BC | Systematic Review and Meta-Analysis (PRISMA) criteria | 15 studies with a total of 3898 patients | 2022 | NR | Better DFS (HR = 0.61, p < 0.05) OS (HR = 1.66, p< 0.001) |
| Kezhen Li [41] | Localized breast cancer | Retrospective | 242 patients with localized primary BC (confirmed by surgery) | 2023 | NR | Better 3-year DFS |
| Noel et al. [42] | TNBC (27) & HER2+ (21) | Retrospective | 48 | 2021 | IHC CD3/CD20 | Better DFS (p value = 0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narvaez, D.; Nadal, J.; Nervo, A.; Costanzo, M.V.; Paletta, C.; Petracci, F.E.; Rivero, S.; Ostinelli, A.; Freile, B.; Enrico, D.; et al. The Emerging Role of Tertiary Lymphoid Structures in Breast Cancer: A Narrative Review. Cancers 2024, 16, 396. https://doi.org/10.3390/cancers16020396
Narvaez D, Nadal J, Nervo A, Costanzo MV, Paletta C, Petracci FE, Rivero S, Ostinelli A, Freile B, Enrico D, et al. The Emerging Role of Tertiary Lymphoid Structures in Breast Cancer: A Narrative Review. Cancers. 2024; 16(2):396. https://doi.org/10.3390/cancers16020396
Chicago/Turabian StyleNarvaez, Dana, Jorge Nadal, Adrian Nervo, María Victoria Costanzo, Claudio Paletta, Fernando E. Petracci, Sergio Rivero, Alexis Ostinelli, Berenice Freile, Diego Enrico, and et al. 2024. "The Emerging Role of Tertiary Lymphoid Structures in Breast Cancer: A Narrative Review" Cancers 16, no. 2: 396. https://doi.org/10.3390/cancers16020396
APA StyleNarvaez, D., Nadal, J., Nervo, A., Costanzo, M. V., Paletta, C., Petracci, F. E., Rivero, S., Ostinelli, A., Freile, B., Enrico, D., Pombo, M. T., Amat, M., Aguirre, E. D., Chacon, M., & Waisberg, F. (2024). The Emerging Role of Tertiary Lymphoid Structures in Breast Cancer: A Narrative Review. Cancers, 16(2), 396. https://doi.org/10.3390/cancers16020396