
Chondrosarcoma of the Femur: Is Local Recurrence Influenced by the Presence of an Extraosseous Component?

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
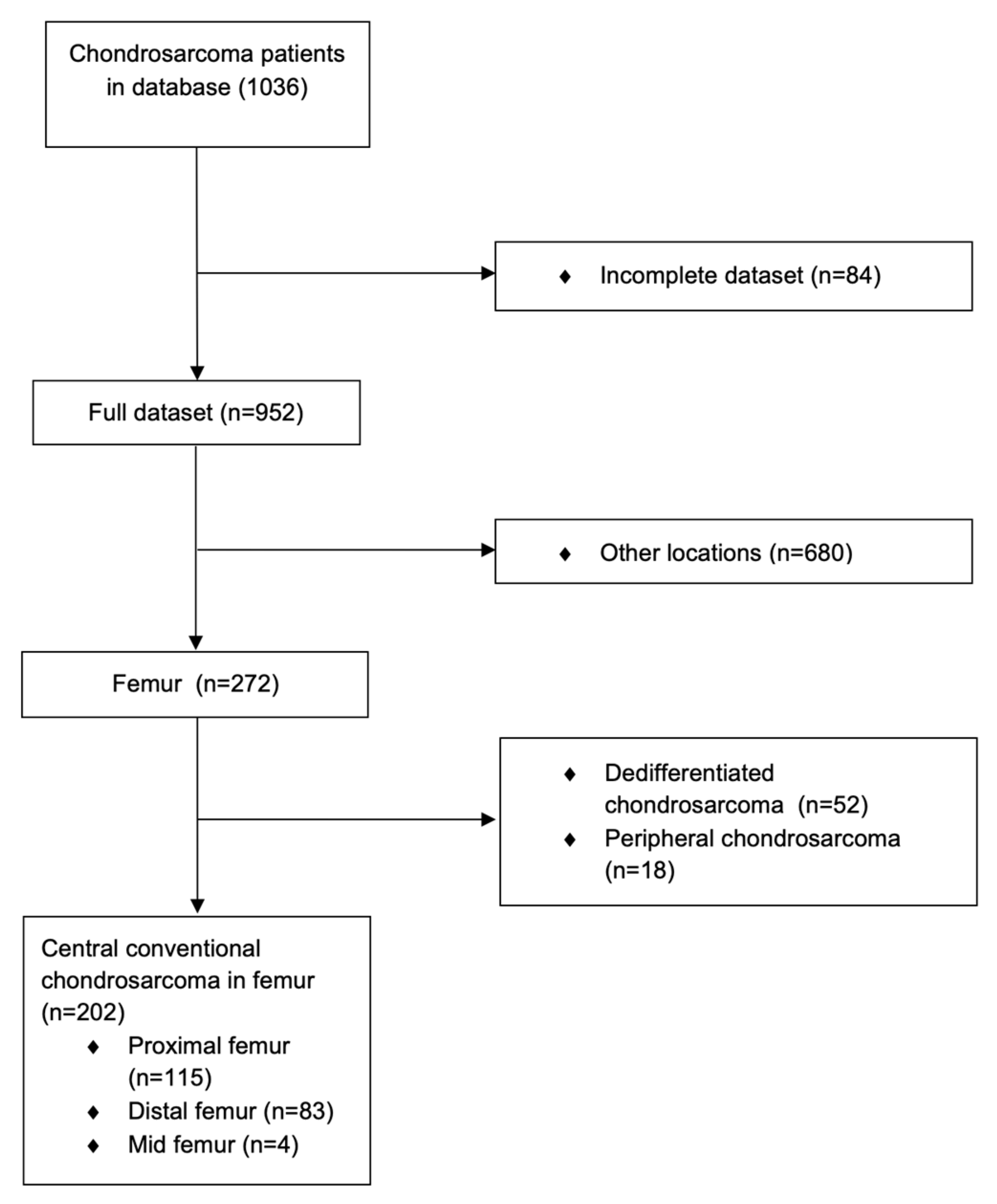
3. Results
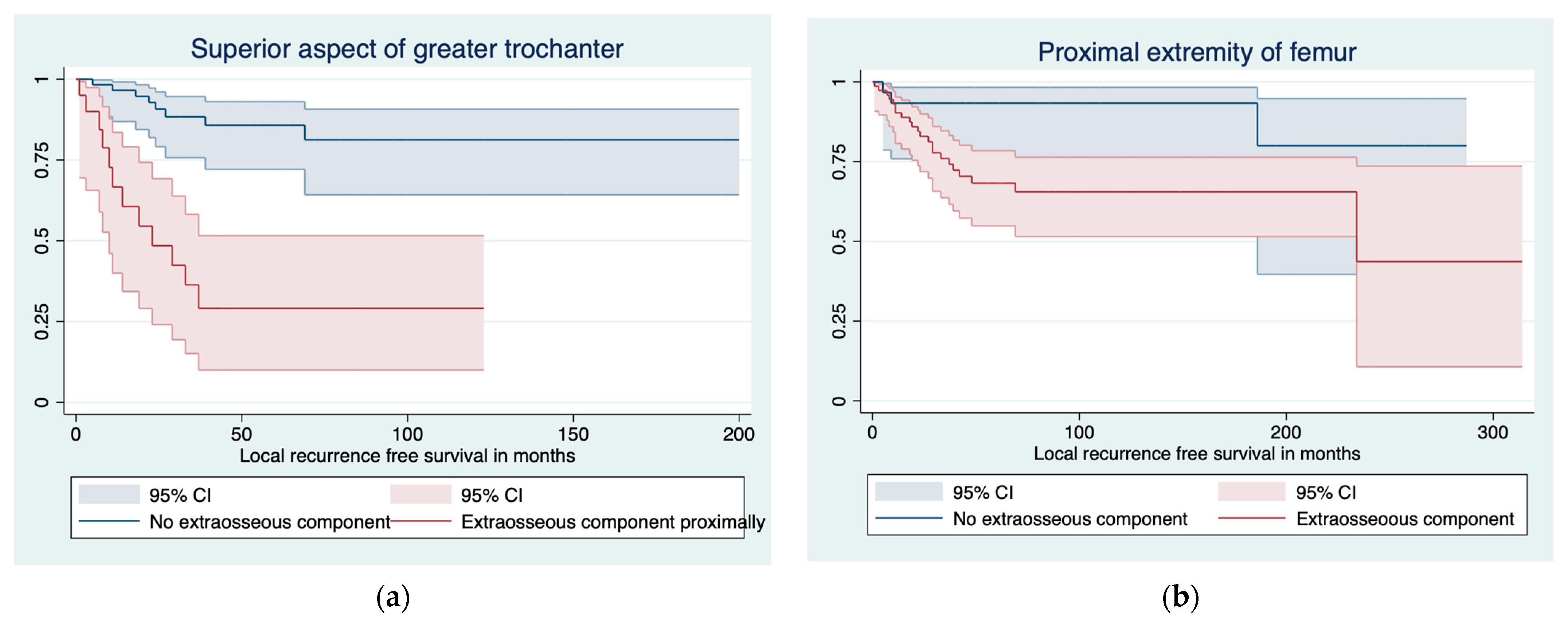
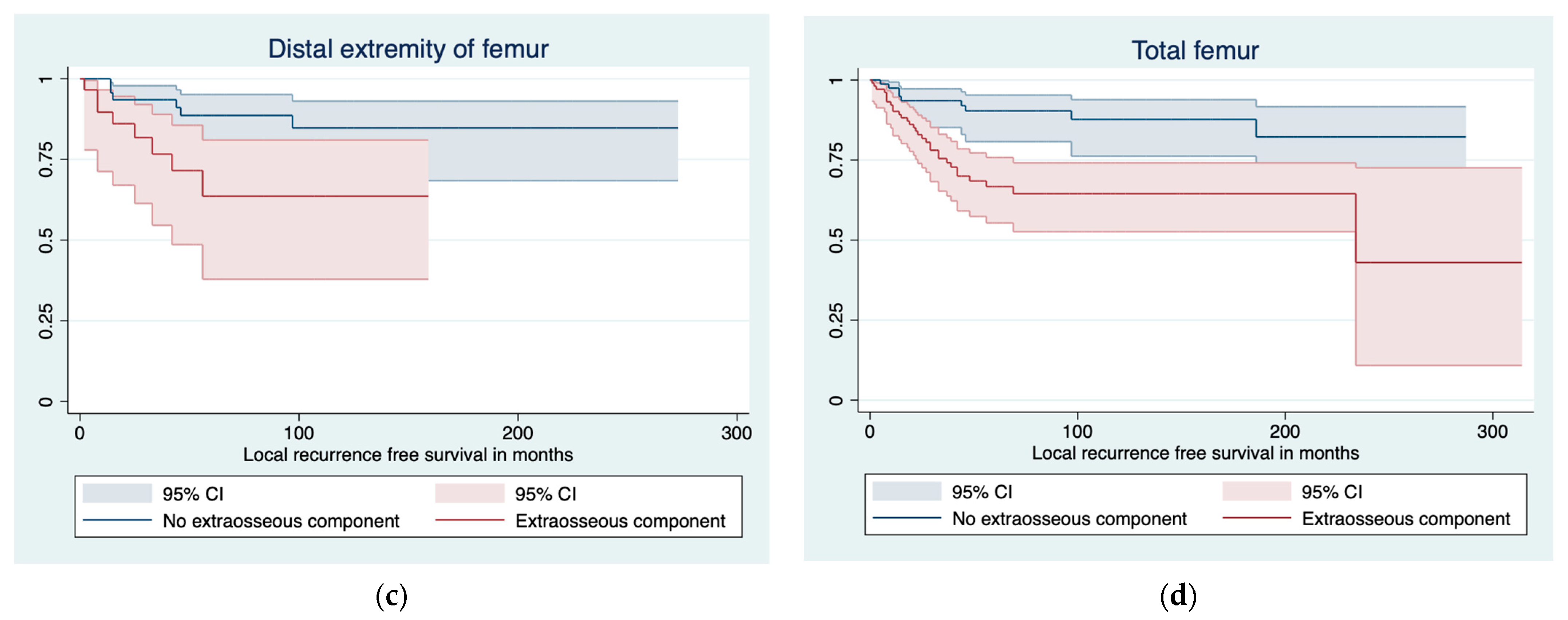
3.1. Predictors of LR and LRFS
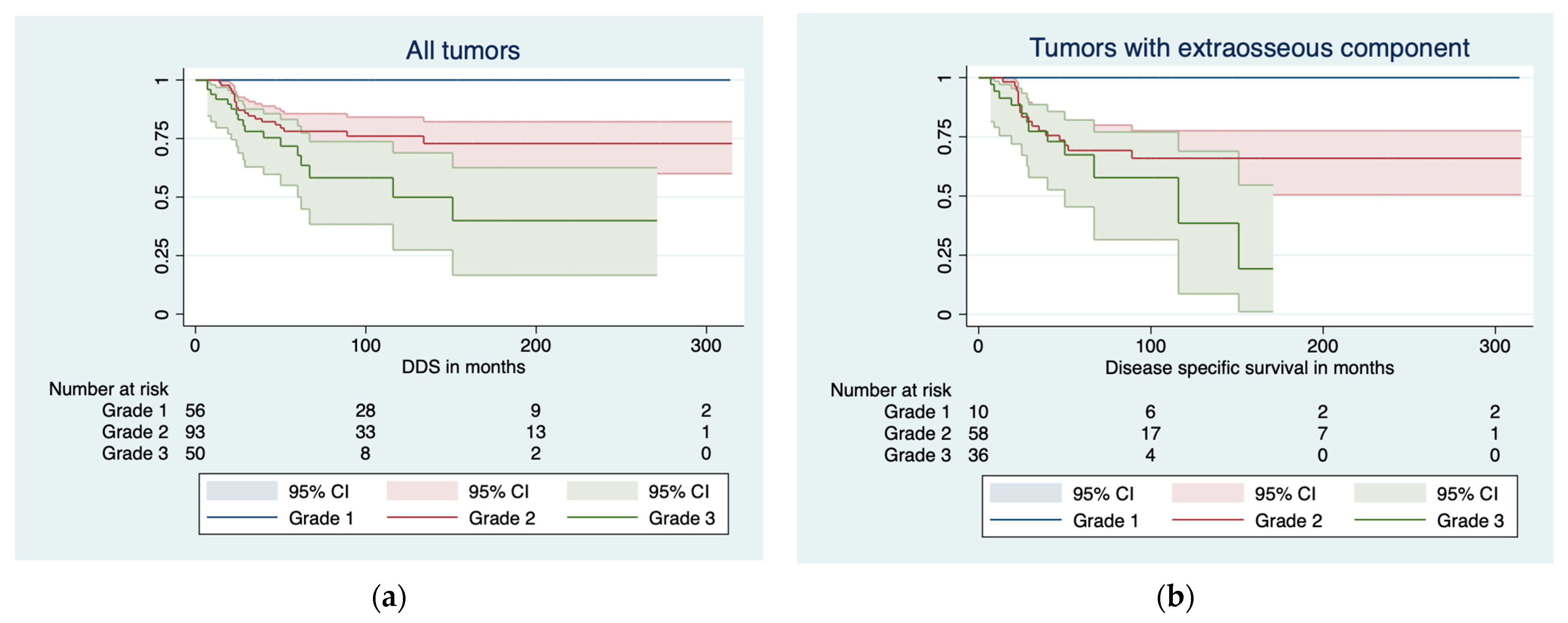
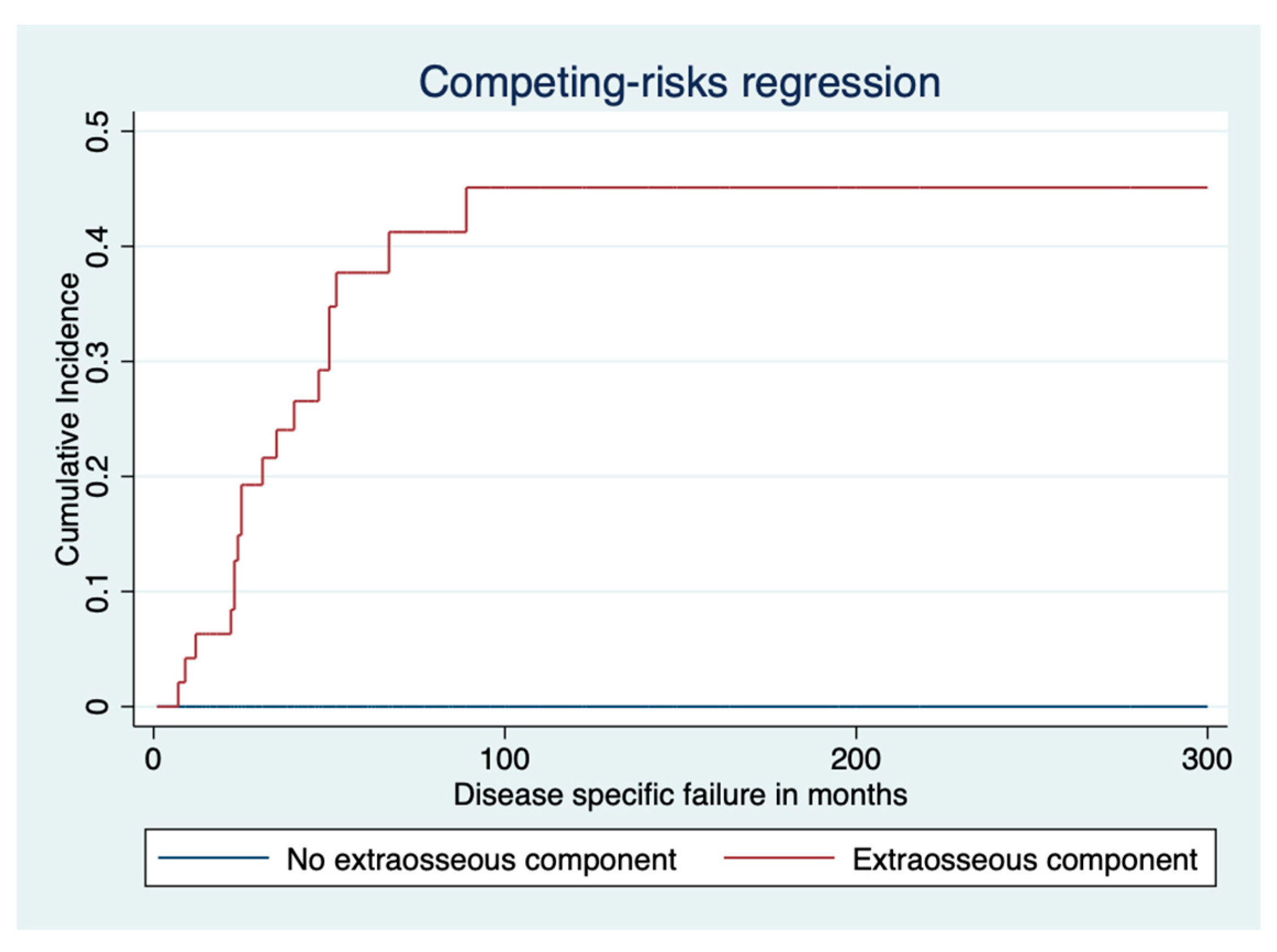
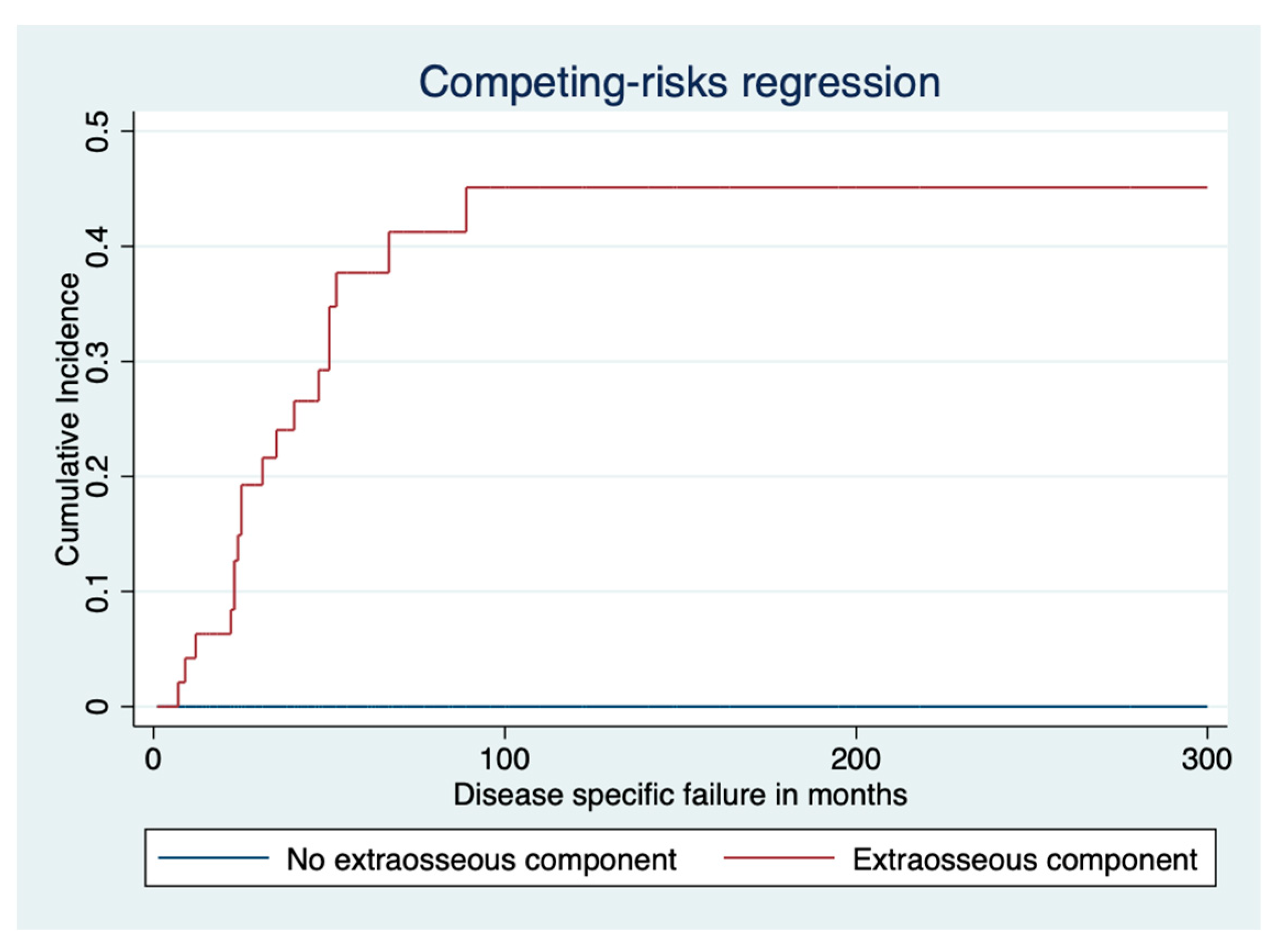
3.2. Disease-Specific Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.-H.; Lee, S.K. Classification of Chondrosarcoma: From Characteristic to Challenging Imaging Findings. Cancers 2023, 15, 1703. [Google Scholar] [CrossRef]
- Venneker, S.; Bovée, J.V.M.G. IDH Mutations in Chondrosarcoma: Case Closed or Not. Cancers 2023, 15, 3603. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, A.; Tudor, M.; Montanari, J.; Commenchail, K.; Savu, D.I.; Lesueur, P.; Chevalier, F. Chondrosarcoma Resistance to Radiation Therapy: Origins and Potential Therapeutic Solutions. Cancers 2023, 15, 1962. [Google Scholar] [CrossRef] [PubMed]
- Gelderblom, H.; Hogendoorn, P.C.; Dijkstra, S.D.; van Rijswijk, C.S.; Krol, A.D.; Taminiau, A.H.; Bovée, J.V. The Clinical Approach Towards Chondrosarcoma. Oncologist 2008, 13, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, M.K.; Evans, S.; Stevenson, J.; Sumathi, V.; Kask, G.; Jeys, L.M.; Parry, M.C. Clinical differences between central and peripheral chondrosarcomas. Bone Jt. J. 2021, 103, 984–990. [Google Scholar] [CrossRef]
- Arshi, A.; Sharin, J.; Park, D.Y.; Park, H.Y.; Bernthal, N.M.; Yazdanshenas, H.; Shamie, A.N. Chondrosarcoma of the ossoeus spiine. J. Bone Jt. Surg. Br. 2005, 87, 1527–1530. [Google Scholar]
- Donati, D.; El Ghoneimy, A.; Bertoni, F.; Di Bella, C.; Mercuri, M. Surgical treatment and outcome of conventional pelvic chondrosarcoma. J. Bone Jt. Surg. 2013, 108, 19–27. [Google Scholar] [CrossRef]
- Mavrogenis, A.F.; Angelini, A.; Drago, G.; Merlino, B.; Ruggieri, P. Survival analysis of patients with chondrosarcomas of the pelvis. Spine 2017, 42, 644–652. [Google Scholar] [CrossRef]
- Fletcher, C.D.M.; Bridge, J.A.; Hogendoorn, P.C.W. Chondrogenic Tumors. In Soft Tissue and Bone Tumors, 4th ed.; IARC Pub-lisher: Lyon, France, 2013. [Google Scholar]
- Riedel, R.F.; Larrier, N.; Dodd, L.; Kirsch, D.; Martinez, S.; Brigman, B.E. The Clinical Management of Chondrosarcoma. Curr. Treat. Options Oncol. 2009, 10, 94–106. [Google Scholar] [CrossRef]
- Healey, J.H.; Lane, J.M. Chondrosarcoma. Clin. Orthop. Relat. Res. 1986, 204, 119–129. [Google Scholar] [CrossRef]
- Laitinen, M.K.; Stevenson, J.D.; Parry, M.C.; Sumathi, V.; Grimer, R.J.; Jeys, L.M. The role of grade in local recurrence and the disease-specific survival in chondrosarcomas. Bone Jt. J. 2018, 100, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Fiorenza, F.; Abudu, A.; Grimer, R.J.; Carter, S.R.; Tillman, R.M.; Ayoub, K.; Mangham, D.C.; Davies, A.M. Risk factors for survival and local control in chondrosarcoma of bone. J. Bone Jt. Surg. 2002, 84, 93–99. [Google Scholar] [CrossRef]
- Angelini, A.; Guerra, G.; Mavrogenis, A.F.; Pala, E.; Picci, P.; Ruggieri, P. Clinical outcome of central conventional chondrosarcoma. J. Surg. Oncol. 2012, 106, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, J.D.; Laitinen, M.K.; Parry, M.C.; Sumathi, V.; Grimer, R.J.; Jeys, L.M. The role of surgical margins in chondrosarcoma. Eur. J. Surg. Oncol. 2018, 44, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Andreou, D.; Fehlberg, S.; Pink, D.; Werner, M.; Tunn, P.-U. Survival amnd prognostic factors in chondrosarcoma. Results in 115 patients with long-term follow-up. Acta Orthop. 2011, 82, 749–755. [Google Scholar] [CrossRef]
- Kim, H.; Bindiganavile, S.S.; Han, I. Oncologic outcome after local recurrence of chondrosarcoma: Analysis of prognostic factors. J. Surg. Oncol. 2015, 111, 957–961. [Google Scholar] [CrossRef]
- Kask, G.; Laitinen, M.K.; Stevenson, J.; Evans, S.; Jeys, L.M.; Parry, M.C. Chondrosarcoma of the hands and feet. Bone Jt. J. 2021, 103, 562–568. [Google Scholar] [CrossRef]
- Wellings, E.P.; Mallett, K.E.; Parkes, C.W.; Labott, J.R.; Rose, P.S.; Houdek, M.T. Impact of tumour stage on the surgical outcomes of scapular chondrosarcoma. Int. Orthop. 2022, 46, 1175–1180. [Google Scholar] [CrossRef]
- Banskota, N.; Fang, X.; Yuan, D.; Lei, S.; Zhang, W.; Duan, H. Comparative Study of Proximal Femur Bone Tumor Patients Undergoing Hemiarthroplasty versus Total Hip Arthroplasty: A Meta-Analysis. J. Clin. Med. 2023, 12, 1209. [Google Scholar] [CrossRef]
- ESMO/European Sarcoma Network Working Group. Bone sarcomas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014, 25, 113–123. [Google Scholar] [CrossRef]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. Clin. Orthop. Relat. Res. 1980, 415, 106–120. [Google Scholar] [CrossRef]
- Houdek, M.T.; Watts, C.D.; Wyles, C.C.; Rose, P.S.; Taunton, M.J.; Sim, F.H. Functional and oncologic outcome of cemented endoprosthesis for malignant proximal femoral tumors. J. Surg. Oncol. 2016, 114, 501–506. [Google Scholar] [CrossRef]
- Davies, A.; Patel, A.; Azzopardi, C.; James, S.; Botchu, R.; Jeys, L. The influence of site on the incidence and diagnosis of solitary central cartilage tumours of the femur. A 21st century perspective. J. Clin. Orthop. Trauma 2022, 32, 101953. [Google Scholar] [CrossRef]
- Kurisunkal, V.; Laitinen, M.K.; Kaneuchi, Y.; Kapanci, B.; Stevenson, J.; Parry, M.C.; Reito, A.; Fujiwara, T.; Jeys, L.M. Is 2 mm a wide margin in high-grade conventional chondrosarcomas of the pelvis? Bone Jt. J. 2021, 103, 1150–1154. [Google Scholar] [CrossRef]
- Thorkildsen, J.; Norum, O.J.; Myklebust, T.A.; Zaikova, O. Chondrosarcoma local recurrence in the Cancer Registry of Norway cohort (1990–2013): Patterns and impact. J. Surg. Oncol. 2021, 123, 510–520. [Google Scholar] [CrossRef]
- Fromm, J.; Klein, A.; Baur-Melnyk, A.; Knösel, T.; Lindner, L.; Birkenmaier, C.; Roeder, F.; Jansson, V.; Dürr, H.R. Survival and prognostic factors in conventional central chondrosarcoma. BMC Cancer 2018, 18, 849. [Google Scholar] [CrossRef]
- Frassica, F.J.; Unni, K.K.; Beabout, J.W.; Sim, F.H. Dedifferentiated chondrosarcoma. A report of the clinicopathological features and treatment of seventy-eight cases. J. Bone Jt. Surg. Am 1986, 68, 1197–1205. [Google Scholar] [CrossRef]
- Staals, E.L.; Bacchini, P.; Bertoni, F. Dedifferentiated central chondrosarcoma. Cancer 2006, 106, 2682–2691. [Google Scholar] [CrossRef]
- El Beaino, M.; Hoda, S.T.; Eldeib, A.J.; Masrouha, K. Dedifferentiated Chondrosarcoma: Diagnostic Controversies and Emerging Therapeutic Targets. Curr. Oncol. Rep. 2023, 25, 1117–1126. [Google Scholar] [CrossRef]
- Grimer, R.J.; Gosheger, G.; Taminiau, A.; Biau, D.; Matejovsky, Z.; Kollender, Y.; San-Julian, M.; Gherlinzoni, F.; Ferrari, C. Dedifferentiated chondrosarcoma: Prognostic factors and outcome from a European group. Eur. J. Cancer 2007, 43, 2060–2065. [Google Scholar]
- Bickels, J.; Meller, I.; Henshaw, R.M.; Malawer, M.M. Reconstruction of Hip Stability after Proximal and Total Femur Resections. Clin. Orthop. Relat. Res. 2000, 375, 218–230. [Google Scholar] [CrossRef]
- Elbuluk, A.M.; Coxe, F.R.; Schimizzi, G.V.; Ranawat, A.S.; Bostrom, M.P.; Sierra, R.J.; Sculco, P.K. Abductor Deficiency-Induced Recurrent Instability after Total Hip Arthroplasty. JBJS Rev. 2020, 8, e0164. [Google Scholar] [CrossRef]
- Henderson, E.R.; Keeney, B.J.; Pala, E.; Funovics, P.T.; Eward, W.C.; Groundland, J.S.; Ehrlichman, L.K.; Puchner, S.S.E.; Brigman, B.E.; Ready, J.E.; et al. The stability of the hip after the use of a proximal femoral endoprosthesis for oncological indications: Analysis of variables relating to the patient and the surgical technique. Bone Jt. J. 2017, 99, 531–537. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Grade 1 | Grade 2 | Grade 3 |
|---|---|---|---|---|
| Eligible cases | 202 | 57 (28%) | 94 (46%) | 51 (26%) |
| Site | ||||
| Proximal extremity | 115 (57%) | 20 (17%) | 60 (52%) | 35 (30%) |
| Distal extremity | 83 (41%) | 36 (43%) | 32 (38%) | 15 (19%) |
| Corpus | 4 (1.9%) | 1 (25%) | 2 (50%) | 1 (25%) |
| Male sex | 110 (55%) | 27 (25%) | 50 (46%) | 33 (30%) |
| Proximal extremity | 65 (57%) | 10 (15%) | 33 (51%) | 22 (34%) |
| Distal extremity | 43 (52%) | 17 (40%) | 16 (37%) | 10 (23%) |
| Corpus | 2 (50%) | - | 1 (100%) | 1 (100%) |
| Age at surgery, median (range) | 55 (8–95) | 46 (10–85) | 59 (8–95) | 59 (23–88) |
| Proximal extremity | 59 (8–95) | 50 (10–85) | 60 (8–85) | 62 (25–87) |
| Distal extremity | 51 (16–90) | 44 (16–85) | 57 (28–90) | 54 (23–88) |
| Corpus | 53 (28–81) | 28 | 64 (47–81) | 55 |
| Mean tumor size, cm (range) | 12 (1.5–46) | 7.8 (1.5–46) | 12 (3.0–30) | 16 (4–40) |
| Proximal extremity | 13 (2.0–40) | 7.3 (2.0–17) | 13 (3.5–30) | 17 (6.0–40) |
| Distal extremity | 9.3 (1.5–60) | 8.0 (1.5–46) | 10 (3.0–25) | 11 (4.0–40) |
| Corpus | 13 (6.0–19) | 6.0 | 17 (16–19) | 13 |
| Extraosseous component | 105 (52%) | 10 (10%) | 58 (55%) | 37 (35%) |
| Proximal extremity | 77 (67%) | 6 (8%%) | 42 (55%) | 28 (37%) |
| Distal extremity | 28 (38%) | 4 (14%) | 16 (57%) | 8 (29%) |
| Corpus | 1 (25%) | - | - | 1 (100%) |
| Extraosseous component in cranial part of proximal extremity of femur | 28 (24%) | 1 (5%) | 17 (28%) | 10 (29%) |
| Median follow-up, months (range) | 90 (0–315) | 114 (0–314) | 92 (0–315) | 58 (0–271) |
| Proximal extremity | 84 (0–315) | 117 (13–314) | 93 (0–315) | 50 (0–182) |
| Distal extremity | 100 (0–273) | 114 (0–264) | 93 (8–273) | 78 (7–271) |
| Corpus | 55 (10–104) | 78 | 57 (10–104) | 29 |
| Pathologic fracture | 20 (10%) | 1 (1.8%) | 12 (14%) | 7 (14%) |
| Proximal extremity | 13 (11%) | - | 10 (17%) | 3 (8.6%) |
| Distal extremity | 6 (8.0%) | 1 (2.9%) | 2 (7.4%) | 3 (21%) |
| Corpus | 1 (25%) | - | - | 1 (100%) |
| Metastasis | 39 (19%) | - | 21 (22%) | 18 (35%) |
| Proximal extremity | 26 (23%) | - | 14 (23%) | 12 (34%) |
| Distal extremity | 12 (14%) | - | 7 (22%) | 5 (33%) |
| Corpus | 1 | - | - | 1 |
| Median time to metastasis in months (range) | 22 (0–189) | - | 26 (0–189) | 16 (4–41) |
| Proximal extremity | 19 (0–73) | - | 20 (0–73) | 18 (6–41) |
| Distal extremity | 27 (0–189) | - | 38 (0–189) | 11 (4–16) |
| Corpus | 21 | - | - | 21 |
| Local recurrence | 47 (23%) | 7 (12%) | 25 (27%) | 15 (29%) |
| Proximal extremity | 31 (27%) | 2 (10%) | 20 (33%) | 9 (26%) |
| Distal extremity | 15 (18%) | 5 (11%) | 5 (16%) | 5 (33%) |
| Corpus | 1 (25%) | - | - | 1 (100%) |
| Median time to LR in months (range) | 33 (0–234) | 54 (14–186) | 39 (0–234) | 12 (1–22) |
| Proximal extremity | 36 (0–234) | 113 (39–186) | 40 (0–234) | 13 (1–22) |
| Distal extremity | 28 (2–97) | 35 (14–97) | 38 (15–56) | 8 (2–18) |
| Corpus | 21 | - | - | 21 |
| Dead for disease | 37 (18%) | - | 20 (21%) | 17 (33%) |
| Proximal extremity | 25 (22%) | - | 14 (23%) | 11 (31%) |
| Distal extremity | 11 (13%) | - | 6 (19%) | 5 (33%) |
| Corpus | 1 (25%) | - | - | 1 (100%) |
| Total | Grade 1 | Grade 2 | Grade 3 | |
|---|---|---|---|---|
| Curettage | ||||
| Proximal extremity | 9 (8%) [5, 45%] | 9 (45%) [2, 22%] | - | - |
| Distal extremity | 18 (22%) [2, 11%] | 16 (44%) [4, 25%] | 2 (6%) [1, 50%] | - |
| Corpus | - | - | - | - |
| Resection | ||||
| Proximal extremity | 96 (85%) [29, 30%] | 11 (55%) [0] | 58 (97%) [20, 34%] | 27 (82%) [9, 33%] |
| Distal extremity | 58 (70%) [8, 32%] | 20 (56%) [1, 5%] | 27 (84%) [4, 15%] | 11 (73%) [3, 27%] |
| Corpus | 4 (100%) [1] | 1 (100%) [0] | 2 (100%) [0] | 1 (100%) [1, 100%] |
| Amputation | ||||
| Proximal extremity | 6 (5%) [0] | - | 2 (3%) [0] | 4 (12%) [0] |
| Distal extremity | 7 (8%) [2, 35%] | - | 3 (9%) [0] | 4 (27%) [2, 50%] |
| Corpus | - | - | - | - |
| Hindquarter | ||||
| Proximal extremity | 2 (2%) [0] | - | - | 2 (6%) [0] |
| Distal extremity | - | - | - | - |
| Corpus | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laitinen, M.K.; Parry, M.C.; Morris, G.V.; Grimer, R.J.; Sumathi, V.; Stevenson, J.D.; Jeys, L.M. Chondrosarcoma of the Femur: Is Local Recurrence Influenced by the Presence of an Extraosseous Component? Cancers 2024, 16, 363. https://doi.org/10.3390/cancers16020363
Laitinen MK, Parry MC, Morris GV, Grimer RJ, Sumathi V, Stevenson JD, Jeys LM. Chondrosarcoma of the Femur: Is Local Recurrence Influenced by the Presence of an Extraosseous Component? Cancers. 2024; 16(2):363. https://doi.org/10.3390/cancers16020363
Chicago/Turabian StyleLaitinen, Minna K., Michael C. Parry, Guy V. Morris, Robert J. Grimer, Vaiyapuri Sumathi, Jonathan D. Stevenson, and Lee M. Jeys. 2024. "Chondrosarcoma of the Femur: Is Local Recurrence Influenced by the Presence of an Extraosseous Component?" Cancers 16, no. 2: 363. https://doi.org/10.3390/cancers16020363
APA StyleLaitinen, M. K., Parry, M. C., Morris, G. V., Grimer, R. J., Sumathi, V., Stevenson, J. D., & Jeys, L. M. (2024). Chondrosarcoma of the Femur: Is Local Recurrence Influenced by the Presence of an Extraosseous Component? Cancers, 16(2), 363. https://doi.org/10.3390/cancers16020363