
Antiandrogens as Therapies for COVID-19: A Systematic Review
 , , , , , ,
, , , , , ,  , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
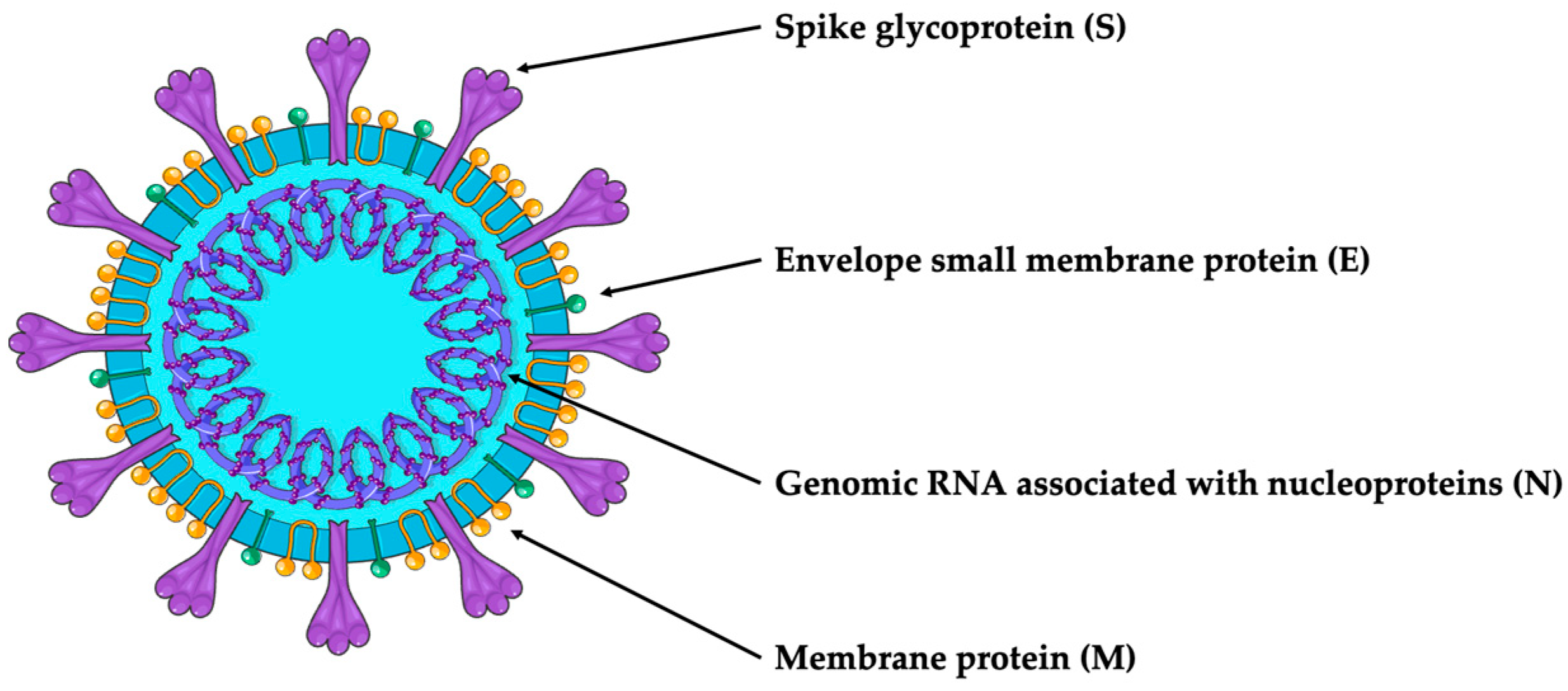
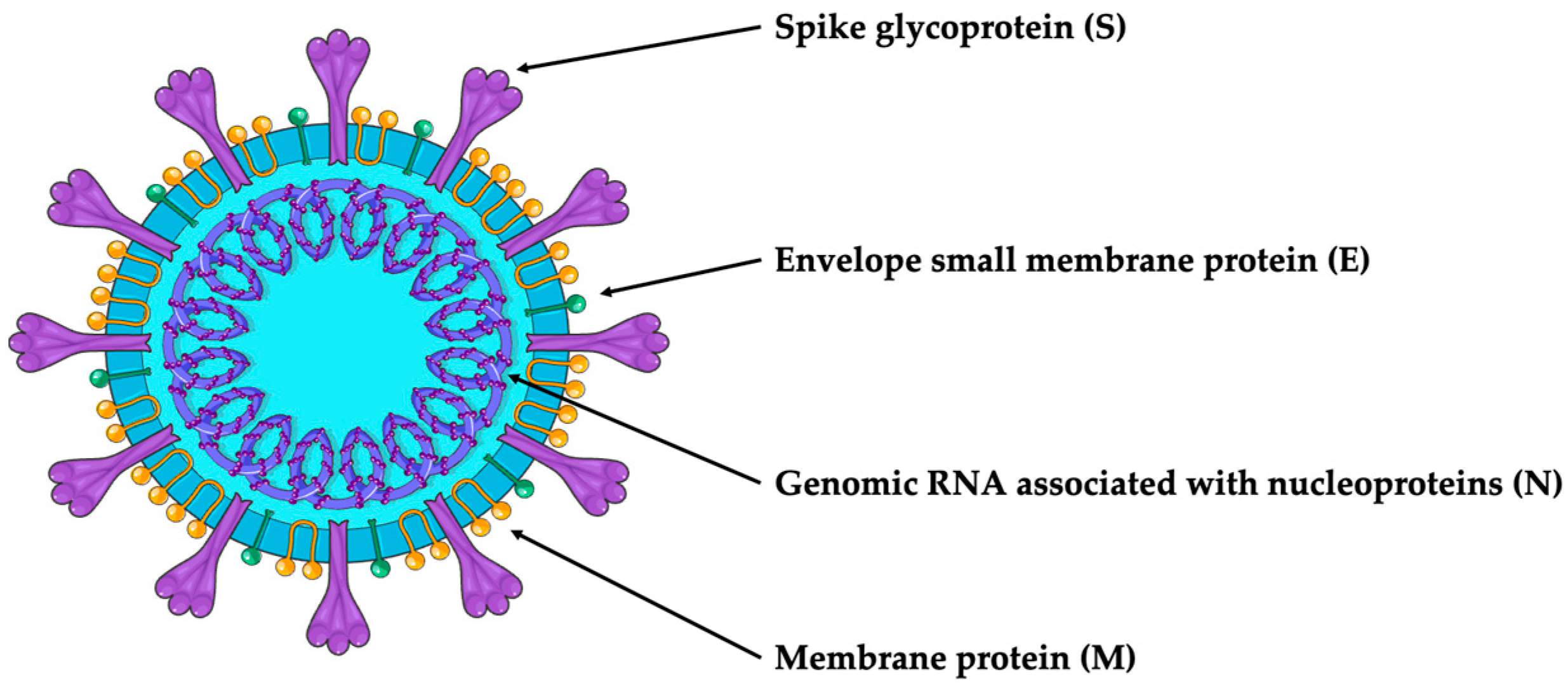
1.1. SARS-CoV-2 Structure
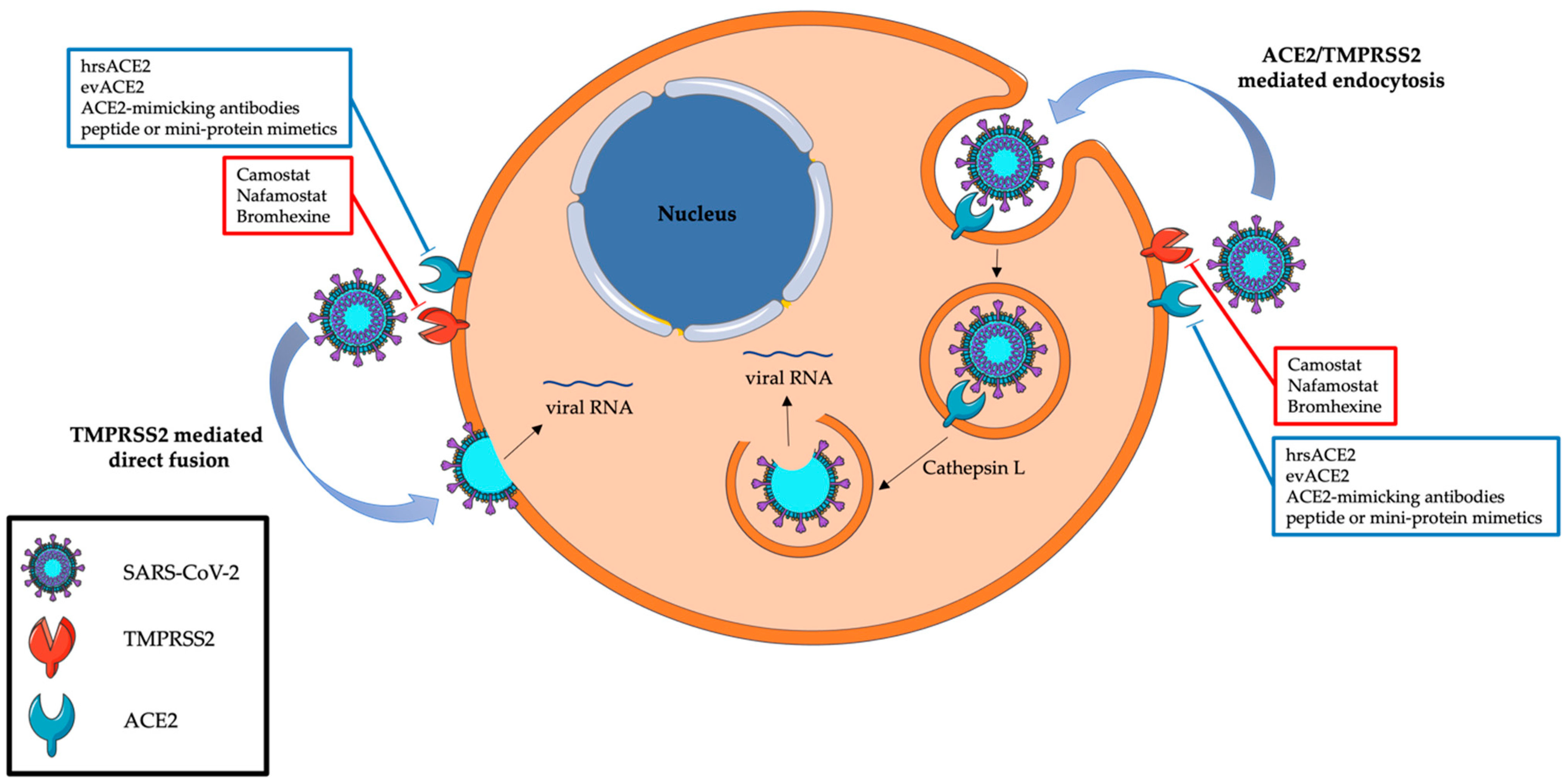
1.2. SARS-CoV-2 Internalization
1.3. TMPRSS2-Targeting Therapies
1.4. ACE2 and Spike Protein-Targeted Therapies
1.5. Androgen Deprivation Therapy
1.6. Other Anti-SARS-CoV-2 Treatments
2. Methods
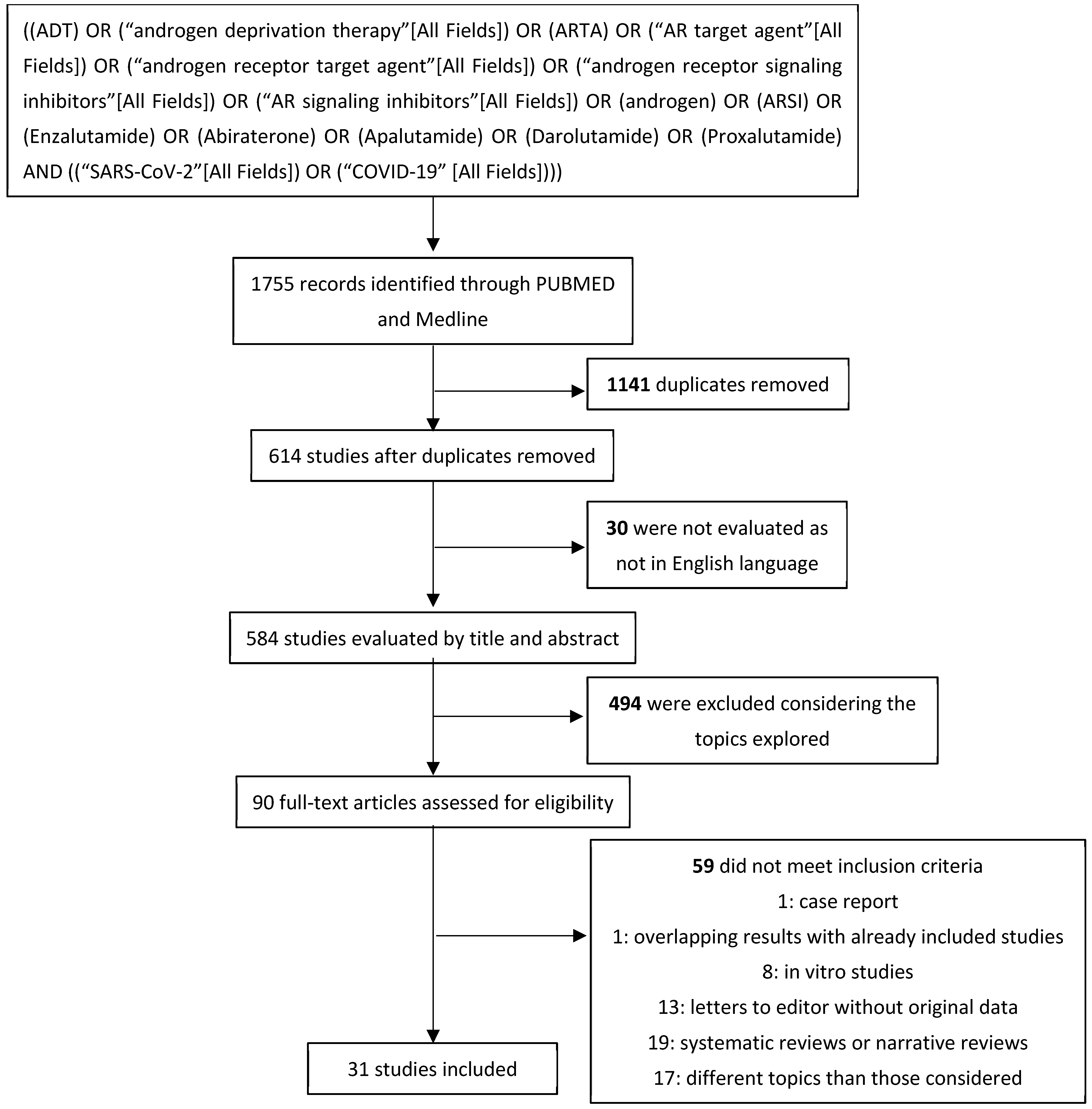
2.1. Literature Search
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Characteristics of Included Studies
3.2. Retrospective Studies
3.3. Prospective Observational Studies
3.4. Randomized Clinical Trials
3.5. 5-ARIs
4. Discussion
4.1. Limits and Controversies
4.2. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Weekly Epidemiological Update on COVID-19—27 April 2023. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---27-april-2023 (accessed on 11 June 2023).
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Nalla, L.V.; Sharma, M.; Sharma, N.; Singh, A.A.; Malim, F.M.; Ghatage, M.; Mukarram, M.; Pawar, A.; Parihar, N.; et al. Association of COVID-19 with Comorbidities: An Update. ACS Pharmacol. Transl. Sci. 2023, 6, 334–354. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Majidipur, A.; Morin-Dewaele, M.; Gaspar Lopes, J.; Berry, F.; Fouchet, J.; Bartier, S.; Dufros Duval, A.; Soyeux, P.; Huet, E.; Louis, B.; et al. Apalutamide Prevents SARS-CoV-2 Infection in Lung Epithelial Cells and in Human Nasal Epithelial Cells. Int. J. Mol. Sci. 2023, 24, 3288. [Google Scholar] [CrossRef]
- Mousavizadeh, L.; Ghasemi, S. Genotype and phenotype of COVID-19: Their roles in pathogenesis. J. Microbiol. Immunol. Infect. 2021, 54, 159–163. [Google Scholar] [CrossRef]
- Shang, J.; Wan, Y.; Luo, C.; Ye, G.; Geng, Q.; Auerbach, A.; Li, F. Cell entry mechanisms of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 11727–11734. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Kruger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Goulter, A.B.; Goddard, M.J.; Allen, J.C.; Clark, K.L. ACE2 gene expression is up-regulated in the human failing heart. BMC Med. 2004, 2, 19. [Google Scholar] [CrossRef]
- Clarke, N.E.; Turner, A.J. Angiotensin-converting enzyme 2: The first decade. Int. J. Hypertens. 2012, 2012, 307315. [Google Scholar] [CrossRef]
- Hikmet, F.; Mear, L.; Edvinsson, A.; Micke, P.; Uhlen, M.; Lindskog, C. The protein expression profile of ACE2 in human tissues. Mol. Syst. Biol. 2020, 16, e9610. [Google Scholar] [CrossRef] [PubMed]
- Vishvkarma, R.; Rajender, S. Could SARS-CoV-2 affect male fertility? Andrologia 2020, 52, e13712. [Google Scholar] [CrossRef]
- Cheng, J.; Zhou, J.; Fu, S.; Fu, J.; Zhou, B.; Chen, H.; Fu, J.; Wei, C. Prostate adenocarcinoma and COVID-19: The possible impacts of TMPRSS2 expressions in susceptibility to SARS-CoV-2. J. Cell. Mol. Med. 2021, 25, 4157–4165. [Google Scholar] [CrossRef]
- Zang, R.; Gomez Castro, M.F.; McCune, B.T.; Zeng, Q.; Rothlauf, P.W.; Sonnek, N.M.; Liu, Z.; Brulois, K.F.; Wang, X.; Greenberg, H.B.; et al. TMPRSS2 and TMPRSS4 promote SARS-CoV-2 infection of human small intestinal enterocytes. Sci. Immunol. 2020, 5, eabc3582. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.G.K.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.S.; Bals, J.; Hauser, B.M.; et al. SARS-CoV-2 Receptor ACE2 Is an Interferon-Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues. Cell 2020, 181, 1016–1035.e19. [Google Scholar] [CrossRef]
- Chen, L.; Li, X.; Chen, M.; Feng, Y.; Xiong, C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc. Res. 2020, 116, 1097–1100. [Google Scholar] [CrossRef]
- Semaan, L.; Mander, N.; Cher, M.L.; Chinni, S.R. TMPRSS2-ERG fusions confer efficacy of enzalutamide in an in vivo bone tumor growth model. BMC Cancer 2019, 19, 972. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.M.; True, L.; Hawley, S.; Matsumura, M.; Morrissey, C.; Vessella, R.; Nelson, P.S. The androgen-regulated type II serine protease TMPRSS2 is differentially expressed and mislocalized in prostate adenocarcinoma. J. Pathol. 2008, 215, 118–125. [Google Scholar] [CrossRef]
- Lucas, J.M.; Heinlein, C.; Kim, T.; Hernandez, S.A.; Malik, M.S.; True, L.D.; Morrissey, C.; Corey, E.; Montgomery, B.; Mostaghel, E.; et al. The androgen-regulated protease TMPRSS2 activates a proteolytic cascade involving components of the tumor microenvironment and promotes prostate cancer metastasis. Cancer Discov. 2014, 4, 1310–1325. [Google Scholar] [CrossRef]
- Guo, W.; Porter, L.M.; Crozier, T.W.; Coates, M.; Jha, A.; McKie, M.; Nathan, J.A.; Lehner, P.J.; Greenwood, E.J.; McCaughan, F. Topical TMPRSS2 inhibition prevents SARS-CoV-2 infection in differentiated human airway cultures. Life Sci. Alliance 2022, 5, e20210111. [Google Scholar] [CrossRef]
- Shirato, K.; Kawase, M.; Matsuyama, S. Middle East respiratory syndrome coronavirus infection mediated by the transmembrane serine protease TMPRSS2. J. Virol. 2013, 87, 12552–12561. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Hofmann-Winkler, H.; Smith, J.C.; Kruger, N.; Sorensen, L.K.; Sogaard, O.S.; Hasselstrom, J.B.; Winkler, M.; Hempel, T.; Raich, L.; et al. Camostat mesylate inhibits SARS-CoV-2 activation by TMPRSS2-related proteases and its metabolite GBPA exerts antiviral activity. bioRxiv 2020. [Google Scholar] [CrossRef]
- Samuel, R.M.; Majd, H.; Richter, M.N.; Ghazizadeh, Z.; Zekavat, S.M.; Navickas, A.; Ramirez, J.T.; Asgharian, H.; Simoneau, C.R.; Bonser, L.R.; et al. Androgen Signaling Regulates SARS-CoV-2 Receptor Levels and Is Associated with Severe COVID-19 Symptoms in Men. Cell Stem Cell 2020, 27, 876–889.e12. [Google Scholar] [CrossRef]
- Youk, J.; Kim, T.; Evans, K.V.; Jeong, Y.I.; Hur, Y.; Hong, S.P.; Kim, J.H.; Yi, K.; Kim, S.Y.; Na, K.J.; et al. Three-Dimensional Human Alveolar Stem Cell Culture Models Reveal Infection Response to SARS-CoV-2. Cell Stem Cell 2020, 27, 905–919.e10. [Google Scholar] [CrossRef] [PubMed]
- Breining, P.; Frolund, A.L.; Hojen, J.F.; Gunst, J.D.; Staerke, N.B.; Saedder, E.; Cases-Thomas, M.; Little, P.; Nielsen, L.P.; Sogaard, O.S.; et al. Camostat mesylate against SARS-CoV-2 and COVID-19-Rationale, dosing and safety. Basic Clin. Pharmacol. Toxicol. 2021, 128, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Gunst, J.D.; Staerke, N.B.; Pahus, M.H.; Kristensen, L.H.; Bodilsen, J.; Lohse, N.; Dalgaard, L.S.; Bronnum, D.; Frobert, O.; Honge, B.; et al. Efficacy of the TMPRSS2 inhibitor camostat mesilate in patients hospitalized with COVID-19-a double-blind randomized controlled trial. eClinicalMedicine 2021, 35, 100849. [Google Scholar] [CrossRef]
- Kinoshita, T.; Shinoda, M.; Nishizaki, Y.; Shiraki, K.; Hirai, Y.; Kichikawa, Y.; Tsushima, K.; Shinkai, M.; Komura, N.; Yoshida, K.; et al. A multicenter, double-blind, randomized, parallel-group, placebo-controlled study to evaluate the efficacy and safety of camostat mesilate in patients with COVID-19 (CANDLE study). BMC Med. 2022, 20, 342. [Google Scholar] [CrossRef]
- Jeong, H.C.; Chae, Y.J.; Shin, K.H. Predicting the systemic exposure and lung concentration of nafamostat using physiologically-based pharmacokinetic modeling. Transl. Clin. Pharmacol. 2022, 30, 201–211. [Google Scholar] [CrossRef]
- Kettunen, P.; Lesnikova, A.; Rasanen, N.; Ojha, R.; Palmunen, L.; Laakso, M.; Lehtonen, S.; Kuusisto, J.; Pietilainen, O.; Saber, S.H.; et al. SARS-CoV-2 Infection of Human Neurons Is TMPRSS2 Independent, Requires Endosomal Cell Entry, and Can Be Blocked by Inhibitors of Host Phosphoinositol-5 Kinase. J. Virol. 2023, 97, e0014423. [Google Scholar] [CrossRef]
- Hoffmann, M.; Schroeder, S.; Kleine-Weber, H.; Muller, M.A.; Drosten, C.; Pohlmann, S. Nafamostat Mesylate Blocks Activation of SARS-CoV-2: New Treatment Option for COVID-19. Antimicrob. Agents Chemother. 2020, 64, e00754-20. [Google Scholar] [CrossRef]
- Ramani, A.; Muller, L.; Ostermann, P.N.; Gabriel, E.; Abida-Islam, P.; Muller-Schiffmann, A.; Mariappan, A.; Goureau, O.; Gruell, H.; Walker, A.; et al. SARS-CoV-2 targets neurons of 3D human brain organoids. EMBO J. 2020, 39, e106230. [Google Scholar] [CrossRef] [PubMed]
- Lyoo, K.S.; Kim, H.M.; Lee, B.; Che, Y.H.; Kim, S.J.; Song, D.; Hwang, W.; Lee, S.; Park, J.H.; Na, W.; et al. Direct neuronal infection of SARS-CoV-2 reveals cellular and molecular pathology of chemosensory impairment of COVID-19 patients. Emerg. Microbes Infect. 2022, 11, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Seccia, T.M.; Shagjaa, T.; Morpurgo, M.; Caroccia, B.; Sanga, V.; Faoro, S.; Venturini, F.; Iadicicco, G.; Lococo, S.; Mazzitelli, M.; et al. RAndomized Clinical Trial Of NAfamostat Mesylate, A Potent Transmembrane Protease Serine 2 (TMPRSS2) Inhibitor, in Patients with COVID-19 Pneumonia. J. Clin. Med. 2023, 12, 6618. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.W.; Mao, H.J.; Wu, Y.L.; Tanaka, Y.; Zhang, W. TMPRSS2: A potential target for treatment of influenza virus and coronavirus infections. Biochimie 2017, 142, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alegria-Arcos, M.; Barbosa, T.; Sepulveda, F.; Combariza, G.; Gonzalez, J.; Gil, C.; Martinez, A.; Ramirez, D. Network pharmacology reveals multitarget mechanism of action of drugs to be repurposed for COVID-19. Front. Pharmacol. 2022, 13, 952192. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, S.; Nao, N.; Shirato, K.; Kawase, M.; Saito, S.; Takayama, I.; Nagata, N.; Sekizuka, T.; Katoh, H.; Kato, F.; et al. Enhanced isolation of SARS-CoV-2 by TMPRSS2-expressing cells. Proc. Natl. Acad. Sci. USA 2020, 117, 7001–7003. [Google Scholar] [CrossRef] [PubMed]
- Ansarin, K.; Tolouian, R.; Ardalan, M.; Taghizadieh, A.; Varshochi, M.; Teimouri, S.; Vaezi, T.; Valizadeh, H.; Saleh, P.; Safiri, S.; et al. Effect of bromhexine on clinical outcomes and mortality in COVID-19 patients: A randomized clinical trial. Bioimpacts 2020, 10, 209–215. [Google Scholar] [CrossRef]
- Vila Mendez, M.L.; Anton Sanz, C.; Cardenas Garcia, A.D.R.; Bravo Malo, A.; Torres Martinez, F.J.; Martin Moros, J.M.; Real Torrijos, M.; Vendrell Covisa, J.F.J.; Guzman Sierra, O.; Molina Barcena, V.; et al. Efficacy of Bromhexine versus Standard of Care in Reducing Viral Load in Patients with Mild-to-Moderate COVID-19 Disease Attended in Primary Care: A Randomized Open-Label Trial. J. Clin. Med. 2022, 12, 142. [Google Scholar] [CrossRef]
- Tolouian, R.; Mulla, Z.D.; Jamaati, H.; Babamahmoodi, A.; Marjani, M.; Eskandari, R.; Dastan, F. Effect of bromhexine in hospitalized patients with COVID-19. J. Investig. Med. 2023, 71, 691–699. [Google Scholar] [CrossRef]
- Zhang, H.; Lv, P.; Jiang, J.; Liu, Y.; Yan, R.; Shu, S.; Hu, B.; Xiao, H.; Cai, K.; Yuan, S.; et al. Advances in developing ACE2 derivatives against SARS-CoV-2. Lancet Microbe 2023, 4, e369–e378. [Google Scholar] [CrossRef]
- Wang, R.; Zhang, Q.; Ge, J.; Ren, W.; Zhang, R.; Lan, J.; Ju, B.; Su, B.; Yu, F.; Chen, P.; et al. Analysis of SARS-CoV-2 variant mutations reveals neutralization escape mechanisms and the ability to use ACE2 receptors from additional species. Immunity 2021, 54, 1611–1621.e5. [Google Scholar] [CrossRef] [PubMed]
- Cameroni, E.; Bowen, J.E.; Rosen, L.E.; Saliba, C.; Zepeda, S.K.; Culap, K.; Pinto, D.; VanBlargan, L.A.; De Marco, A.; di Iulio, J.; et al. Broadly neutralizing antibodies overcome SARS-CoV-2 Omicron antigenic shift. Nature 2022, 602, 664–670. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration (FDA). Fact Sheet for Health Care Providers. Emergency Use Authorization (EUA) of Bamlanivimab and Etesevimab. Available online: https://www.fda.gov/media/145802/download (accessed on 11 June 2023).
- Cohen, M.S.; Nirula, A.; Mulligan, M.J.; Novak, R.M.; Marovich, M.; Yen, C.; Stemer, A.; Mayer, S.M.; Wohl, D.; Brengle, B.; et al. Effect of Bamlanivimab vs Placebo on Incidence of COVID-19 Among Residents and Staff of Skilled Nursing and Assisted Living Facilities: A Randomized Clinical Trial. JAMA 2021, 326, 46–55. [Google Scholar] [CrossRef]
- A Study of LY3819253 (LY-CoV555) and LY3832479 (LY-CoV016) in Preventing SARS-CoV-2 Infection and COVID-19 in Nursing Home Residents and Staff (BLAZE-2). NCT04497987. Available online: https://trials.lilly.com/en-US/trial/247831 (accessed on 2 October 2023).
- Alwani, M.; Yassin, A.; Al-Zoubi, R.M.; Aboumarzouk, O.M.; Nettleship, J.; Kelly, D.; Al-Qudimat, A.R.; Shabsigh, R. Sex-based differences in severity and mortality in COVID-19. Rev. Med. Virol. 2021, 31, e2223. [Google Scholar] [CrossRef] [PubMed]
- Clift, A.K.; von Ende, A.; Tan, P.S.; Sallis, H.M.; Lindson, N.; Coupland, C.A.C.; Munafo, M.R.; Aveyard, P.; Hippisley-Cox, J.; Hopewell, J.C. Smoking and COVID-19 outcomes: An observational and Mendelian randomisation study using the UK Biobank cohort. Thorax 2022, 77, 65–73. [Google Scholar] [CrossRef]
- Cai, H. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir. Med. 2020, 8, e20. [Google Scholar] [CrossRef] [PubMed]
- Regitz-Zagrosek, V. Sex and gender differences in health. Science & Society Series on Sex and Science. EMBO Rep. 2012, 13, 596–603. [Google Scholar] [CrossRef]
- Bischof, E.; Oertelt-Prigione, S.; Morgan, R.; Klein, S.L.; The Sex and Gender in COVID-19 Clinical Trials Working Group (SGC); Gender and COVID-19 Working Group. Towards Precision Medicine: Inclusion of Sex and Gender Aspects in COVID-19 Clinical Studies-Acting Now before It Is Too Late-A Joint Call for Action. Int. J. Environ. Res. Public Health 2020, 17, 3715. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G.; Tombal, B.; Gillessen, S.; ESMO Guidelines Committee. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1119–1134. [Google Scholar] [CrossRef]
- Leach, D.A.; Mohr, A.; Giotis, E.S.; Cil, E.; Isac, A.M.; Yates, L.L.; Barclay, W.S.; Zwacka, R.M.; Bevan, C.L.; Brooke, G.N. The antiandrogen enzalutamide downregulates TMPRSS2 and reduces cellular entry of SARS-CoV-2 in human lung cells. Nat. Commun. 2021, 12, 4068. [Google Scholar] [CrossRef] [PubMed]
- Welen, K.; Rosendal, E.; Gisslen, M.; Lenman, A.; Freyhult, E.; Fonseca-Rodriguez, O.; Bremell, D.; Stranne, J.; Balkhed, A.O.; Niward, K.; et al. A Phase 2 Trial of the Effect of Antiandrogen Therapy on COVID-19 Outcome: No Evidence of Benefit, Supported by Epidemiology and In Vitro Data. Eur. Urol. 2022, 81, 285–293. [Google Scholar] [CrossRef]
- Kim, J.; Hwang, S.Y.; Kim, D.; Kim, M.; Baek, K.; Kang, M.; An, S.; Gong, J.; Park, S.; Kandeel, M.; et al. Abiraterone Acetate Attenuates SARS-CoV-2 Replication by Interfering with the Structural Nucleocapsid Protein. Biomol. Ther. 2022, 30, 427–434. [Google Scholar] [CrossRef]
- Koskinen, M.; Carpen, O.; Honkanen, V.; Seppanen, M.R.J.; Miettinen, P.J.; Tuominen, J.A.; Raivio, T. Androgen deprivation and SARS-CoV-2 in men with prostate cancer. Ann. Oncol. 2020, 31, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Gedeborg, R.; Loeb, S.; Styrke, J.; Kiiski-Berggren, R.; Garmo, H.; Stattin, P. Susceptibility to SARS-CoV-2 infection and risk for severe COVID-19 in patients with prostate cancer on androgen deprivation therapy. Int. J. Cancer 2022, 151, 1925–1934. [Google Scholar] [CrossRef] [PubMed]
- Unlu, S.; Shin, J.J.; Par-Young, J.; Simonov, M.; Vinetz, J.; Petrylak, D.P.; Kang, I.; Kim, J.W. Effect of Androgen-Androgen Receptor Directed Therapy on COVID-19 Outcome in Prostate Cancer Patients. Cancer Investig. 2023, 41, 77–83. [Google Scholar] [CrossRef]
- Gu, Y.; Xue, M.; Wang, Q.; Hong, X.; Wang, X.; Zhou, F.; Sun, J.; Wang, G.; Peng, Y. Novel Strategy of Proxalutamide for the Treatment of Prostate Cancer through Coordinated Blockade of Lipogenesis and Androgen Receptor Axis. Int. J. Mol. Sci. 2021, 22, 13222. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Xu, W.; Zhang, W.; Sun, Y.; Yan, H.; Gao, X.; Wang, F.; Zhou, Q.; Hou, J.; Ren, S.; et al. Preclinical profile and phase I clinical trial of a novel androgen receptor antagonist GT0918 in castration-resistant prostate cancer. Eur. J. Cancer 2020, 134, 29–40. [Google Scholar] [CrossRef]
- Cadegiani, F.A.; McCoy, J.; Gustavo Wambier, C.; Vano-Galvan, S.; Shapiro, J.; Tosti, A.; Zimerman, R.A.; Goren, A. Proxalutamide Significantly Accelerates Viral Clearance and Reduces Time to Clinical Remission in Patients with Mild to Moderate COVID-19: Results from a Randomized, Double-Blinded, Placebo-Controlled Trial. Cureus 2021, 13, e13492. [Google Scholar] [CrossRef]
- Loughlin, K.R. The clinical applications of five-alpha reductase inhibitors. Can. J. Urol. 2021, 28, 10584–10588. [Google Scholar]
- Bramson, H.N.; Hermann, D.; Batchelor, K.W.; Lee, F.W.; James, M.K.; Frye, S.V. Unique preclinical characteristics of GG745, a potent dual inhibitor of 5AR. J. Pharmacol. Exp. Ther. 1997, 282, 1496–1502. [Google Scholar]
- Chislett, B.; Chen, D.; Perera, M.L.; Chung, E.; Bolton, D.; Qu, L.G. 5-alpha reductase inhibitors use in prostatic disease and beyond. Transl. Androl. Urol. 2023, 12, 487–496. [Google Scholar] [CrossRef]
- Park, J.J.; Lee, H.Y.; Shim, S.R.; Lee, S.W.; Kim, K.T.; Kim, J.H. Prostate cancer specific mortality after 5alpha-reductase inhibitors medication in benign prostatic hyperplasia patients: Systematic review and meta-analysis. Aging Male 2021, 24, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Knijnik, P.G.; Brum, P.W.; Cachoeira, E.T.; Paludo, A.O.; Gorgen, A.R.H.; Burttet, L.M.; Neyeloff, J.L.; Neto, B.S. The impact of 5-alpha-reductase inhibitors on mortality in a prostate cancer chemoprevention setting: A meta-analysis. World J. Urol. 2021, 39, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Lyon, M.; Li, J.; Cullen, J.; Milinovich, A.; Kattan, M.; Jehi, L.; Sharifi, N.; Klein, E.A. 5alpha-Reductase Inhibitors Are Associated with Reduced Risk of SARS-CoV-2 Infection: A Matched-Pair, Registry-Based Analysis. J. Urol. 2022, 207, 183–189. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Montopoli, M.; Zumerle, S.; Vettor, R.; Rugge, M.; Zorzi, M.; Catapano, C.V.; Carbone, G.M.; Cavalli, A.; Pagano, F.; Ragazzi, E.; et al. Androgen-deprivation therapies for prostate cancer and risk of infection by SARS-CoV-2: A population-based study (N = 4532). Ann. Oncol. 2020, 31, 1040–1045. [Google Scholar] [CrossRef]
- Lee, K.M.; Heberer, K.; Gao, A.; Becker, D.J.; Loeb, S.; Makarov, D.V.; Gulanski, B.; DuVall, S.L.; Aslan, M.; Lee, J.; et al. A Population-Level Analysis of the Protective Effects of Androgen Deprivation Therapy Against COVID-19 Disease Incidence and Severity. Front. Med. 2022, 9, 774773. [Google Scholar] [CrossRef]
- Kwon, D.H.; Vashisht, R.; Borno, H.T.; Aggarwal, R.R.; Small, E.J.; Butte, A.J.; Huang, F.W. Androgen-deprivation therapy and SARS-CoV-2 in men with prostate cancer: Findings from the University of California Health System registry. Ann. Oncol. 2021, 32, 678–679. [Google Scholar] [CrossRef] [PubMed]
- Hunt, C.M.; Efird, J.T.; Redding, T.S.t.; Thompson, A.D., Jr.; Press, A.M.; Williams, C.D.; Hostler, C.J.; Suzuki, A. Medications Associated with Lower Mortality in a SARS-CoV-2 Positive Cohort of 26,508 Veterans. J. Gen. Intern. Med. 2022, 37, 4144–4152. [Google Scholar] [CrossRef]
- Caffo, O.; Zagonel, V.; Baldessari, C.; Berruti, A.; Bortolus, R.; Buti, S.; Ceresoli, G.L.; Donini, M.; Ermacora, P.; Fornarini, G.; et al. On the relationship between androgen-deprivation therapy for prostate cancer and risk of infection by SARS-CoV-2. Ann. Oncol. 2020, 31, 1415–1416. [Google Scholar] [CrossRef]
- Caffo, O.; Gasparro, D.; Di Lorenzo, G.; Volta, A.D.; Guglielmini, P.; Zucali, P.; Bortolus, R.; Cavo, A.; Ceresoli, G.; Chiari, R.; et al. Incidence and outcomes of severe acute respiratory syndrome coronavirus 2 infection in patients with metastatic castration-resistant prostate cancer. Eur. J. Cancer 2020, 140, 140–146. [Google Scholar] [CrossRef]
- Patel, V.G.; Zhong, X.; Liaw, B.; Tremblay, D.; Tsao, C.K.; Galsky, M.D.; Oh, W.K. Does androgen deprivation therapy protect against severe complications from COVID-19? Ann. Oncol. 2020, 31, 1419–1420. [Google Scholar] [CrossRef]
- Jimenez-Alcaide, E.; Garcia-Fuentes, C.; Hernandez, V.; De la Pena, E.; Perez-Fernandez, E.; Castro, A.; Caballero-Perea, B.; Guijarro, A.; Llorente, C. Influence of androgen deprivation therapy on the severity of COVID-19 in prostate cancer patients. Prostate 2021, 81, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.L.; Tucker, M.D.; Bakouny, Z.; Labaki, C.; Hsu, C.Y.; Shyr, Y.; Armstrong, A.J.; Beer, T.M.; Bijjula, R.R.; Bilen, M.A.; et al. Association Between Androgen Deprivation Therapy and Mortality Among Patients With Prostate Cancer and COVID-19. JAMA Netw. Open 2021, 4, e2134330. [Google Scholar] [CrossRef] [PubMed]
- Duarte, M.B.O.; Leal, F.; Argenton, J.L.P.; Carvalheira, J.B.C. Impact of androgen deprivation therapy on mortality of prostate cancer patients with COVID-19: A propensity score-based analysis. Infect. Agent Cancer 2021, 16, 66. [Google Scholar] [CrossRef]
- Dalla Volta, A.; Valcamonico, F.; Zamboni, S.; Ferrari, V.D.; Grisanti, S.; Simeone, C.; Berruti, A. Is androgen deprivation therapy protective against SARS-CoV-2 infection and related complications in prostate cancer patients? Minerva Urol. Nefrol. 2020, 72, 778–779. [Google Scholar] [CrossRef]
- Klein, E.A.; Li, J.; Milinovich, A.; Schold, J.D.; Sharifi, N.; Kattan, M.W.; Jehi, L. Androgen Deprivation Therapy in Men with Prostate Cancer Does Not Affect Risk of Infection with SARS-CoV-2. J. Urol. 2021, 205, 441–443. [Google Scholar] [CrossRef]
- Di Lorenzo, G.; Buonerba, L.; Ingenito, C.; Crocetto, F.; Buonerba, C.; Libroia, A.; Sciarra, A.; Ragone, G.; Sanseverino, R.; Iaccarino, S.; et al. Clinical Characteristics of Metastatic Prostate Cancer Patients Infected with COVID-19 in South Italy. Oncology 2020, 98, 743–747. [Google Scholar] [CrossRef]
- Ianhez, M.; Ramos, P.M.; Goren, A.; Miot, H.A. Androgen sensitivity in COVID-19 and antiandrogens: Prospective data are still needed. Dermatol. Ther. 2020, 33, e14166. [Google Scholar] [CrossRef]
- Gedeborg, R.; Lindhagen, L.; Loeb, S.; Styrke, J.; Garmo, H.; Stattin, P. Androgen deprivation therapy, comorbidity, cancer stage and mortality from COVID-19 in men with prostate cancer. Scand. J. Urol. 2022, 56, 104–111. [Google Scholar] [CrossRef]
- Kazan, O.; Culpan, M.; Efiloglu, O.; Atis, G.; Yildirim, A. The clinical impact of androgen deprivation therapy on SARS-CoV-2 infection rates and disease severity. Turk. J. Urol. 2021, 47, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Goren, A.; Wambier, C.G.; Herrera, S.; McCoy, J.; Vano-Galvan, S.; Gioia, F.; Comeche, B.; Ron, R.; Serrano-Villar, S.; Ramos, P.M.; et al. Anti-androgens may protect against severe COVID-19 outcomes: Results from a prospective cohort study of 77 hospitalized men. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e13–e15. [Google Scholar] [CrossRef]
- Shah, N.J.; Patel, V.G.; Zhong, X.; Pina, L.; Hawley, J.E.; Lin, E.; Gartrell, B.A.; Febles, V.A.; Wise, D.R.; Qin, Q.; et al. The Impact of Androgen Deprivation Therapy on COVID-19 Illness in Men With Prostate Cancer. JNCI Cancer Spectr. 2022, 6, pkac035. [Google Scholar] [CrossRef]
- Davidsson, S.; Messing Eriksson, A.; Udumyan, R.; Swanholm, P.; Lewin Lundh, M.; Widing, C.; Lindlof, C.; Fridfeldt, J.; Andersson, S.O.; Fall, K. Androgen deprivation therapy in men with prostate cancer is not associated with COVID-2019 infection. Prostate 2023, 83, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Cadegiani, F.A.; Zimerman, R.A.; Fonseca, D.N.; Correia, M.N.; Muller, M.P.; Bet, D.L.; Slaviero, M.R.; Zardo, I.; Benites, P.R.; Barros, R.N.; et al. Final Results of a Randomized, Placebo-Controlled, Two-Arm, Parallel Clinical Trial of Proxalutamide for Hospitalized COVID-19 Patients: A Multiregional, Joint Analysis of the Proxa-Rescue AndroCoV Trial. Cureus 2021, 13, e20691. [Google Scholar] [CrossRef] [PubMed]
- Nickols, N.G.; Mi, Z.; DeMatt, E.; Biswas, K.; Clise, C.E.; Huggins, J.T.; Maraka, S.; Ambrogini, E.; Mirsaeidi, M.S.; Levin, E.R.; et al. Effect of Androgen Suppression on Clinical Outcomes in Hospitalized Men With COVID-19: The HITCH Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e227852. [Google Scholar] [CrossRef]
- McCoy, J.; Cadegiani, F.A.; Wambier, C.G.; Herrera, S.; Vano-Galvan, S.; Mesinkovska, N.A.; Ramos, P.M.; Shapiro, J.; Sinclair, R.; Tosti, A.; et al. 5-alpha-reductase inhibitors are associated with reduced frequency of COVID-19 symptoms in males with androgenetic alopecia. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e243–e246. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, M.; Duga, S.; Azzolini, E.; Fasulo, V.; Buffi, N.; Saita, A.; Lughezzani, G.; Paraboschi, E.M.; Hurle, R.; Nobili, A.; et al. Impact of chronic exposure to 5-alpha reductase inhibitors on the risk of hospitalization for COVID-19: A case-control study in male population from two COVID-19 regional centers of Lombardy, Italy. Minerva Urol. Nephrol. 2022, 74, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Zarehoseinzade, E.; Allami, A.; Ahmadi, M.; Bijani, B.; Mohammadi, N. Finasteride in hospitalized adult males with COVID-19: A risk factor for severity of the disease or an adjunct treatment: A randomized controlled clinical trial. Med. J. Islam. Repub. Iran 2021, 35, 30. [Google Scholar] [CrossRef]
- Cadegiani, F.A.; McCoy, J.; Gustavo Wambier, C.; Goren, A. Early Antiandrogen Therapy With Dutasteride Reduces Viral Shedding, Inflammatory Responses, and Time-to-Remission in Males With COVID-19: A Randomized, Double-Blind, Placebo-Controlled Interventional Trial (EAT-DUTA AndroCoV Trial—Biochemical). Cureus 2021, 13, e13047. [Google Scholar] [CrossRef]
- McCoy, J.; Goren, A.; Cadegiani, F.A.; Vano-Galvan, S.; Kovacevic, M.; Situm, M.; Shapiro, J.; Sinclair, R.; Tosti, A.; Stanimirovic, A.; et al. Proxalutamide Reduces the Rate of Hospitalization for COVID-19 Male Outpatients: A Randomized Double-Blinded Placebo-Controlled Trial. Front. Med. 2021, 8, 668698. [Google Scholar] [CrossRef]
- Frontiers Editorial Office. Retraction: Proxalutamide Reduces the Rate of Hospitalization for COVID-19 Male Outpatients: A Randomized Double-Blinded Placebo-Controlled Trial. Front. Med. 2022, 9, 964099. [Google Scholar] [CrossRef]
- RF Services, Inc. ‘Too Good to Be True’: Doubts Swirl around Trial That Saw 77% Reduction in COVID-19 Mortality. Available online: https://www.science.org/content/article/too-good-be-true-doubts-swirl-around-trial-saw-77-reduction-covid-19-mortality (accessed on 25 June 2023).
- NOTA PÚBLICA: CNS Elucida à Sociedade Brasileira Fatos Sobre Estudo Irregular Com Proxalutamida. 15 de Outubro de 2021. Available online: https://conselho.saude.gov.br/ultimas-noticias-cns/2095-nota-publica-cns-elucida-a-sociedade-brasileira-fatos-sobre-estudo-irregular-com-proxalutamida (accessed on 11 June 2023).
- Goren, A.; Vano-Galvan, S.; Wambier, C.G.; McCoy, J.; Gomez-Zubiaur, A.; Moreno-Arrones, O.M.; Shapiro, J.; Sinclair, R.D.; Gold, M.H.; Kovacevic, M.; et al. A preliminary observation: Male pattern hair loss among hospitalized COVID-19 patients in Spain—A potential clue to the role of androgens in COVID-19 severity. J. Cosmet. Dermatol. 2020, 19, 1545–1547. [Google Scholar] [CrossRef]
- Wambier, C.G.; Goren, A. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is likely to be androgen mediated. J. Am. Acad. Dermatol. 2020, 83, 308–309. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic (accessed on 11 June 2023).
- Twitchell, D.K.; Christensen, M.B.; Hackett, G.; Morgentaler, A.; Saad, F.; Pastuszak, A.W. Examining Male Predominance of Severe COVID-19 Outcomes: A Systematic Review. Androg. Clin. Res. Ther. 2022, 3, 41–53. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Chakladar, J.; Shende, N.; Li, W.T.; Rajasekaran, M.; Chang, E.Y.; Ongkeko, W.M. Smoking-Mediated Upregulation of the Androgen Pathway Leads to Increased SARS-CoV-2 Susceptibility. Int. J. Mol. Sci. 2020, 21, 3627. [Google Scholar] [CrossRef]
- Patanavanich, R.; Glantz, S.A. Smoking Is Associated With COVID-19 Progression: A Meta-analysis. Nicotine Tob. Res. 2020, 22, 1653–1656. [Google Scholar] [CrossRef]
- Baristaite, G.; Gurwitz, D. Estradiol reduces ACE2 and TMPRSS2 mRNA levels in A549 human lung epithelial cells. Drug Dev. Res. 2022, 83, 961–966. [Google Scholar] [CrossRef]
- Amodio, G.; Capogrosso, P.; Pontillo, M.; Tassara, M.; Boeri, L.; Carenzi, C.; Cignoli, D.; Ferrara, A.M.; Ramirez, G.A.; Tresoldi, C.; et al. Combined plasma levels of IL-10 and testosterone, but not soluble HLA-G5, predict the risk of death in COVID-19 patients. Andrology 2023, 11, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Zhong, J.; Jiang, Y.; Zhang, J. Associations between COVID-19 infection and sex steroid hormones. Front. Endocrinol. 2022, 13, 940675. [Google Scholar] [CrossRef]
- Infante, M.; Pieri, M.; Lupisella, S.; D’Amore, L.; Bernardini, S.; Fabbri, A.; Iannetta, M.; Andreoni, M.; Morello, M. Low testosterone levels and high estradiol to testosterone ratio are associated with hyperinflammatory state and mortality in hospitalized men with COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5889–5903. [Google Scholar] [CrossRef]
- Rastrelli, G.; Di Stasi, V.; Inglese, F.; Beccaria, M.; Garuti, M.; Di Costanzo, D.; Spreafico, F.; Greco, G.F.; Cervi, G.; Pecoriello, A.; et al. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology 2021, 9, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Salonia, A.; Corona, G.; Giwercman, A.; Maggi, M.; Minhas, S.; Nappi, R.E.; Sofikitis, N.; Vignozzi, L. SARS-CoV-2, testosterone and frailty in males (PROTEGGIMI): A multidimensional research project. Andrology 2021, 9, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Xie, W.; Li, D.; Shi, L.; Ye, G.; Mao, Y.; Xiong, Y.; Sun, H.; Zheng, F.; Chen, Z.; et al. Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients. J. Med. Virol. 2021, 93, 456–462. [Google Scholar] [CrossRef]
- Fan, C.; Lu, W.; Li, K.; Ding, Y.; Wang, J. ACE2 Expression in Kidney and Testis May Cause Kidney and Testis Infection in COVID-19 Patients. Front. Med. 2020, 7, 563893. [Google Scholar] [CrossRef]
- Wang, Z.; Xu, X. scRNA-seq Profiling of Human Testes Reveals the Presence of the ACE2 Receptor, A Target for SARS-CoV-2 Infection in Spermatogonia, Leydig and Sertoli Cells. Cells 2020, 9, 920. [Google Scholar] [CrossRef]
- Karimi, A.; Nowroozi, A.; Alilou, S.; Amini, E. Effects of Androgen Deprivation Therapy on COVID-19 in Patients with Prostate Cancer: A Systematic Review and Meta-Analysis. Urol. J. 2021, 18, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.B.; Li, W.L.; Sun, M.; Duan, X.; Wang, Y.T.; Zhang, L.X.; Xin, Z.H.; Yun, Z.F.; Fan, B.; Li, X.C. Impacts of androgen deprivation therapy on the risks and outcomes of SARS-CoV-2 infection in patients with prostate cancer. Asian J. Androl. 2023, 25, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.K.; Park, J.J.; Yang, W.J.; Doo, S.W.; Kim, J.H. Relationship Between Androgen Deprivation Therapy for Prostate Cancer and Risk of SARS-CoV-2 Infection: A Systematic Review and Meta-Analysis. J. Korean Med. Sci. 2022, 37, e237. [Google Scholar] [CrossRef]
- Sari Motlagh, R.; Abufaraj, M.; Karakiewicz, P.I.; Rajwa, P.; Mori, K.; Mun, D.H.; Shariat, S.F. Association between SARS-CoV-2 infection and disease severity among prostate cancer patients on androgen deprivation therapy: A systematic review and meta-analysis. World J. Urol. 2022, 40, 907–914. [Google Scholar] [CrossRef]
- O’Callaghan, M.E.; Jay, A.; Kichenadasse, G.; Moretti, K.L. Androgen deprivation therapy in unlikely to be effective for treatment of COVID-19. Ann. Oncol. 2020, 31, 1780–1782. [Google Scholar] [CrossRef] [PubMed]
- Epistolio, S.; Ramelli, G.; Ottaviano, M.; Crupi, E.; Marandino, L.; Biggiogero, M.; Maida, P.A.; Ruinelli, L.; Vogl, U.; Mangan, D.; et al. P1245 Polymorphic Variants of HSD3B1 Gene Confer Different Outcome in Specific Subgroups of Patients Infected With SARS-CoV-2. Front. Med. 2021, 8, 793728. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Drug | Molecular Mechanism | PC Treatment Setting |
|---|---|---|
| Leuprolide | LHRH analogues: lead to eventual down-regulation of LHRH receptors, thus suppressing LH and FSH production and, subsequently, testosterone synthesis after an initial flare-up | nmHSPC mHSPC nmCRPC mCRPC |
| Triptorelin | ||
| Goserelin | ||
| Degarelix | LHRH-antagonists: by binding to LHRH receptors, lead to a rapid decrease in FSH and LH production and then testosterone synthesis | |
| Bicalutamide | Androgen receptor inhibitor | nmHSPC mHSPC nmCRPC mCRPC |
| Flutamide | ||
| Nilutamide | ||
| Enzalutamide | Androgen receptor inhibitor | nmCRPC (PSA-DT < 10 months) mHSPC mCRPC |
| Abiraterone | Selective, irreversible CYP17inhibitor. Interference with androgen biosynthesis. Partial AR antagonist | High-risk LA-PC |
| mHSPC mCRPC | ||
| Apalutamide | Androgen receptor inhibitor | nmCRPC (PSA-DT < 10 months) mHSPC |
| Darolutamide | Androgen receptor inhibitor | nmCRPC (PSA-DT < 10 months) |
| Proxalutamide | Third-generation AR receptor inhibitor | Currently under investigation |
| Finasteride | 5-alpha-reductase inhibitors: impair the conversion of testosterone into dihydrotestosterone | Male alopecia, benign prostate hyperplasia |
| Dutasteride |
| Authors | Year * | Country | Design | Sample Size | Time of Data Collection | Outcomes 1 Ep | Drug | Quality-Bias Assessment | Statistical Evaluations |
|---|---|---|---|---|---|---|---|---|---|
| Retrospective studies | |||||||||
| Montopoli et al. [72] | 2020 | Italy | Retrospective cohort | 4532 men, 118 PC pts | Last update on April 2020 | ADT impact on COVID-19 clinical outcomes | ADT (NOS) | Fair | Positive association |
| Lee et al. [73] | 2020 | USA | Retrospective cohort | 25,006 SARS-CoV-2 pts, 95 under ADT | February–July 2020 | ADT impact on COVID-19 clinical outcomes | ADT (NOS) | Good | Positive association |
| Koskinen et al. [57] | 2020 | Finland | Retrospective cohort | 352 PC pts, 134 under ADT | March–May 2020 | ADT impact on COVID-19 clinical outcomes | History of orchiectomy, GnRH ag./antag. Ars, abiraterone | Fair | No association |
| Kwon et al. [74] | 2020 | USA | Retrospective cohort | 5211 PC pts, 799 under ADT | February–December 2020 | ADT impact on COVID-19 clinical outcomes | GnRH ag./antag. | Good | No association |
| Hunt et al. [75] | 2020 | USA | Retrospective cohort | 26,508 pts (23,659 men) | March to September 2020 | 30-day mortality from first SARS-CoV-2-positive test | Concomitant therapies (including ADT) | Good | Positive trend |
| Caffo et al. [76] | 2020 | Italy | Retrospective cohort | 1949 mCRPC pts | 2020, NOS | SARS-CoV-2 diffusion among PC patients | ADT for mCRPC | Fair | Negative trend |
| Caffo et al. [77] | 2020 | Italy | Retrospective cohort | 1443 mCRPC | February–June 2020 | Death rate and possible impact of the PC therapy/history on mortality | ADT for mCRPC | Good | No association |
| Patel et al. [78] | 2020 | USA | Retrospective cohort | 58 PC pts, 22 under ADT | March–June 2020 | ADT impact on COVID-19 clinical outcomes | GnRH ag./antag. (within 3 months) or [testosterone] < 50 ng/dL within 6 months | Fair | Positive trend |
| Alcaide et al. [79] | 2021 | Spain | Retrospective cohort | 1349 PC pts, 156 under ADT | March–May 2020 | ADT impact on COVID-19 clinical outcomes | ADT (NOS) | Good | No association |
| Schmidt et al. [80] | 2021 | USA | Retrospective cohort | 1106 PC pts | March–February 2021 | 30-day mortality | ADT for at least 6 months | Good | No association |
| Duarte et al. [81] | 2021 | Brazil | Retrospective cohort | 199 PC pts, 156 under ADT | 2020 to April 2021 | Mortality | ADT (NOS) | Good | No association |
| Welen et al. [55] | 2021 | Sweden | Retrospective cohort | 7894 PC pts, 4 GPs. GP3, n = 214 (ADT plus abiraterone/enzalutamide) | February 2020 to May 2021 | ADT impact on COVID-19 clinical outcomes | ADT, abiraterone, enzalutamide | Good | Negative association for GP3 |
| Gedeborg et al. [58] | 2022 | Sweden | Retrospective cohort | 1695 SARS-CoV-2 PC pts, 596 under ADT | February–December 2020 | ADT impact on COVID-19 clinical outcomes | Bicalutamide, Flutamide, GnRH ag., abiraterone, enzalutamide | Good | Negative association |
| Unlu et al. [59] | 2022 | USA | Retrospective cohort | 146 PC pts, 25 under ADT | March–October 2020 | ADT impact on COVID-19 clinical outcomes | GnRH ag./antag., AR antag., enzalutamide, abiraterone | Good | Positive trend |
| Dalla Volta et al. [82] | 2022 | Italy | Retrospective cohort | 83 PC pts under ADT | February–April 2020 | ADT impact on COVID-19 clinical outcomes | ADT (NOS) | Fair | No association |
| Prospective observational studies | |||||||||
| Klein et al. [83] | 2020 | USA | Prospective registry cohort study | 1779 PC pts, 304 under ADT | March–June 2020 | SARS-CoV-2 infection rate, disease severity | ADT (NOS) | Good | No association |
| Di Lorenzo et al. [84] | 2020 | Italy | Prospective obs. cohort | 72 PC pts | March 2020 | ADT impact on COVID-19 clinical outcomes | LHRH ag./antag. abiraterone, enzalutamide, apalutamide | Fair | Positive trend |
| Ianhez et al. [85] | 2020 | Brazil | Snowball sampling population survey | 554 healthy and 17 COVID-19 volunteers under AR | Not reported | ADT impact on COVID-19 clinical outcomes | ADT for PC, 5-ARIs, bicalutamide, spironolactone and cyproaterone | Fair | No association |
| Gedeborg et al. [86] | 2021 | Sweden | Population-based nested case—control cohort | 474 SARS-CoV-2 PC pts | March–December 2020 | ADT impact on COVID-19 clinical outcomes | Bicalutamide, flutamide, GnRH ag., abiraterone, enzalutamide | Good | Negative association |
| Kazan et al. [87] | 2021 | Turkey | Obs. prospective cohort | 365 PC pts, 138 under ADT | August–June 2021 | ADT impact on COVID-19 clinical outcomes | ADT (NOS) | Good | No association |
| Goren et al. [88] | 2021 | Spain | Prospective cohort | 77 pts, 12 under Ars | March–May 2020 | ICU admission rate | Antiandrogens for at least 6 months | Fair | Positive association |
| Shah et al. [89] | 2022 | USA | Multi institutional obs. study | 465 PC pts, 148 receiving ADT | March 2020 | Overall survival | ADT (NOS) | Good | No association |
| Davidsson et al. [90] | 2023 | Sweden | Prospective cohort | 655 PC pts, 224 undergoing ADT; 240 patients with BPH | April–early 2021 | COVID-19 outcomes and positive SARS-CoV-2 antibody serology | ADT, bicalutamide, abiraterone, enzalutamide | Good | No association |
| Randomized clinical trials | |||||||||
| Welen et al. [55] | 2021 | Sweden | RCT | 42 COVID-19 pts | July–November 2020 | Time to mechanical ventilation (or death)/hospital discharge | Enzalutamide | Good | No association |
| Cadegiani et al. [62] | 2021 | Brazil | RCT | 236 volunteers: 171 (proxalutamide arm); 65 (placebo arm) | 2021 (NOS) | Percentage of negative pts negative for SARS-CoV-2 on day 7 | Proxalutamide | Poor | Positive association |
| Cadegiani et al. [91] | 2021 | Brazil | Joint analysis of RCT | 778 volunteers; 423 in the proxalutamide arm | 2021 (NOS) | 14-day and 28-day recovery | Proxalutamide vs. placebo in addition to SOC | Poor | Positive association |
| Nickols et al. [92] | 2022 | USA | RCT | 96 pts: 62 experimental vs. 34 placebo group | July–April 2021 | Mortality, need for hospitalization, need for mechanical ventilation on day 15 | Degarelix 240 mg s.c. vs. saline placebo | Good | No association |
| 5-ARIs | |||||||||
| McCoy et al. [93] | 2020 | Brazil | Retrospective cohort | 300 SARS-CoV-2 pts, 48 under dutasteride | June–July 2020 | COVID-19 severity among men under 5-ARIs | Dutasteride for at least 6 months | Fair | Positive association |
| Lyon et al. [68] | 2021 | USA | Retrospective cohort | 1888 people, 944 5-ARI users | March–February 2021 | SARS-CoV-2-positivity rate | 5-ARIs (finasteride and dutasteride) | Good | Positive association |
| Lazzeri et al. [94] | 2022 | Italy | Obs. case–control cohort | 943 pts, 43 under 5-ARIs | March–April 2020 | Impact of 5-ARIs on COVID-19 clinical outcomes | 5-ARIs (finasteride, dutasteride) for at least 6 months | Fair | Positive association (for men aged >55) |
| Zarehoseinzade et al. [95] | 2021 | Iran | Partial double blinded RCT | 80 hospitalized men ≥ 50 yo | May–June 2020 | Mortality rate and hospital stay | Finasteride | Good | No association |
| Cadegiani et al. [96] | 2021 | Brazil | RCT | 138 SARS-CoV-2 volunteers | June–October 2020 | COVID-19-severity outcomes | Dutasteride | Good | Positive association |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cani, M.; Epistolio, S.; Dazio, G.; Modesti, M.; Salfi, G.; Pedrani, M.; Isella, L.; Gillessen, S.; Vogl, U.M.; Tortola, L.; et al. Antiandrogens as Therapies for COVID-19: A Systematic Review. Cancers 2024, 16, 298. https://doi.org/10.3390/cancers16020298
Cani M, Epistolio S, Dazio G, Modesti M, Salfi G, Pedrani M, Isella L, Gillessen S, Vogl UM, Tortola L, et al. Antiandrogens as Therapies for COVID-19: A Systematic Review. Cancers. 2024; 16(2):298. https://doi.org/10.3390/cancers16020298
Chicago/Turabian StyleCani, Massimiliano, Samantha Epistolio, Giulia Dazio, Mikol Modesti, Giuseppe Salfi, Martino Pedrani, Luca Isella, Silke Gillessen, Ursula Maria Vogl, Luigi Tortola, and et al. 2024. "Antiandrogens as Therapies for COVID-19: A Systematic Review" Cancers 16, no. 2: 298. https://doi.org/10.3390/cancers16020298
APA StyleCani, M., Epistolio, S., Dazio, G., Modesti, M., Salfi, G., Pedrani, M., Isella, L., Gillessen, S., Vogl, U. M., Tortola, L., Treglia, G., Buttigliero, C., Frattini, M., & Pereira Mestre, R. (2024). Antiandrogens as Therapies for COVID-19: A Systematic Review. Cancers, 16(2), 298. https://doi.org/10.3390/cancers16020298