
Human Papillomavirus Types and Cervical Cancer Screening among Female Sex Workers in Cameroon
 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Populations and Methods
2.1. Study Population, Setting, and Procedure
2.1.1. The Study Type
2.1.2. The Setting
2.1.3. Inclusion and Exclusion Criteria
- Inclusion criteria: The main inclusion criteria were women 30 years and above who self-identify themselves as FSWs.
- Exclusion criteria: Our exclusion criteria included (1) pregnancy, (2) previous total abdominal hysterectomy, and (3) women with already diagnosed invasive cervical cancer.
2.1.4. Data Collection
2.1.5. The Procedure
2.2. Data Analysis
3. Results
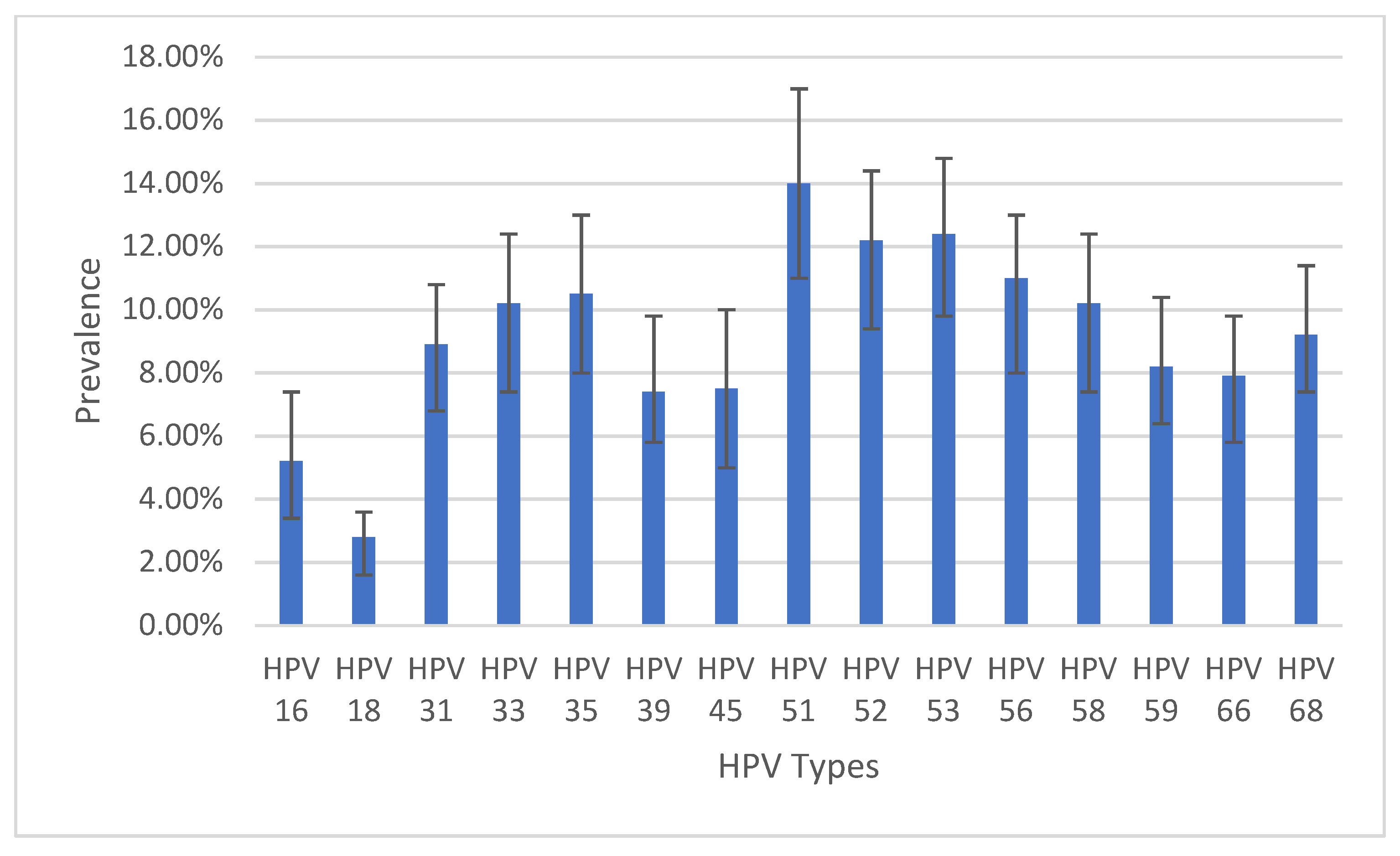
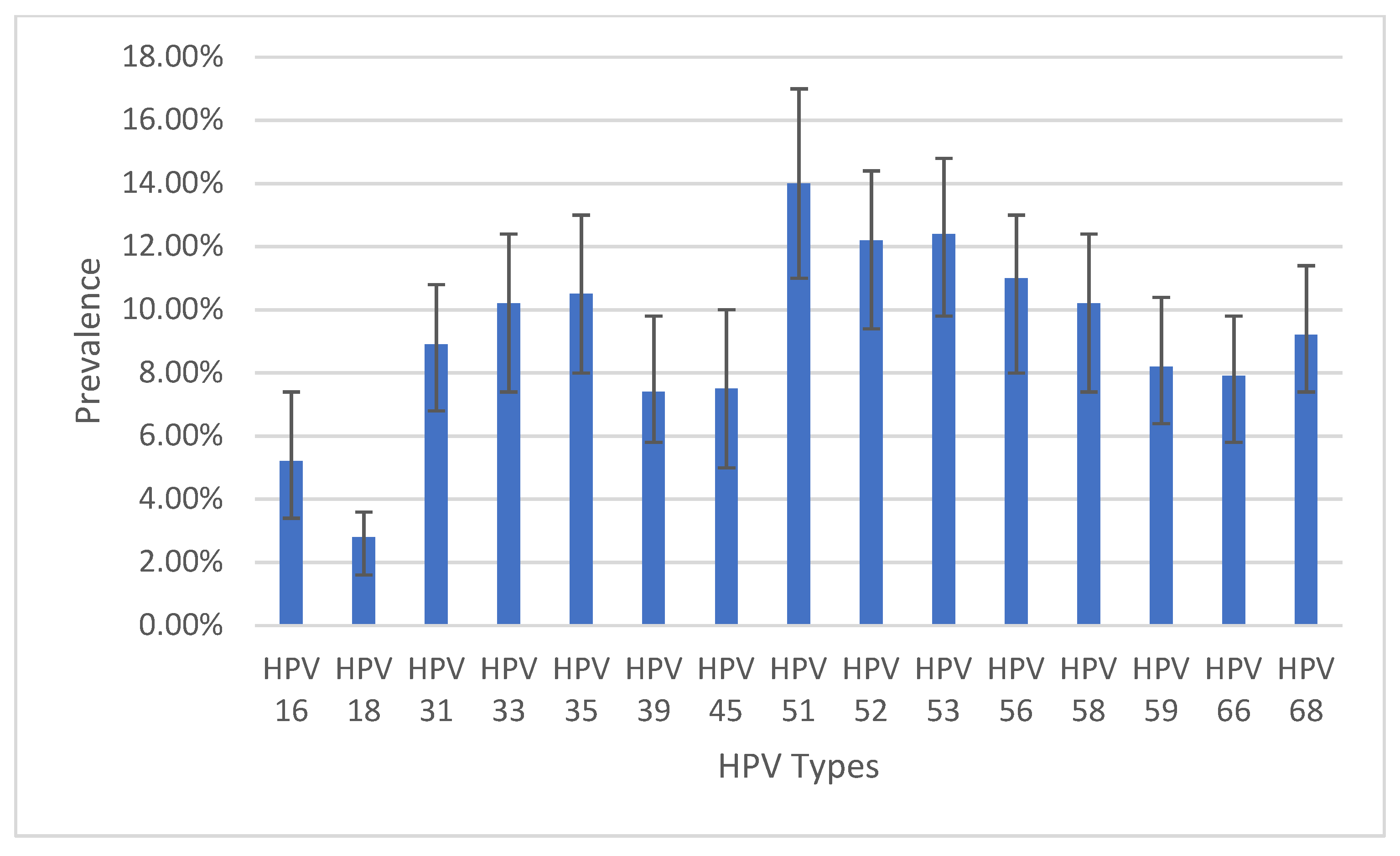
3.1. HPV Genotyping Results
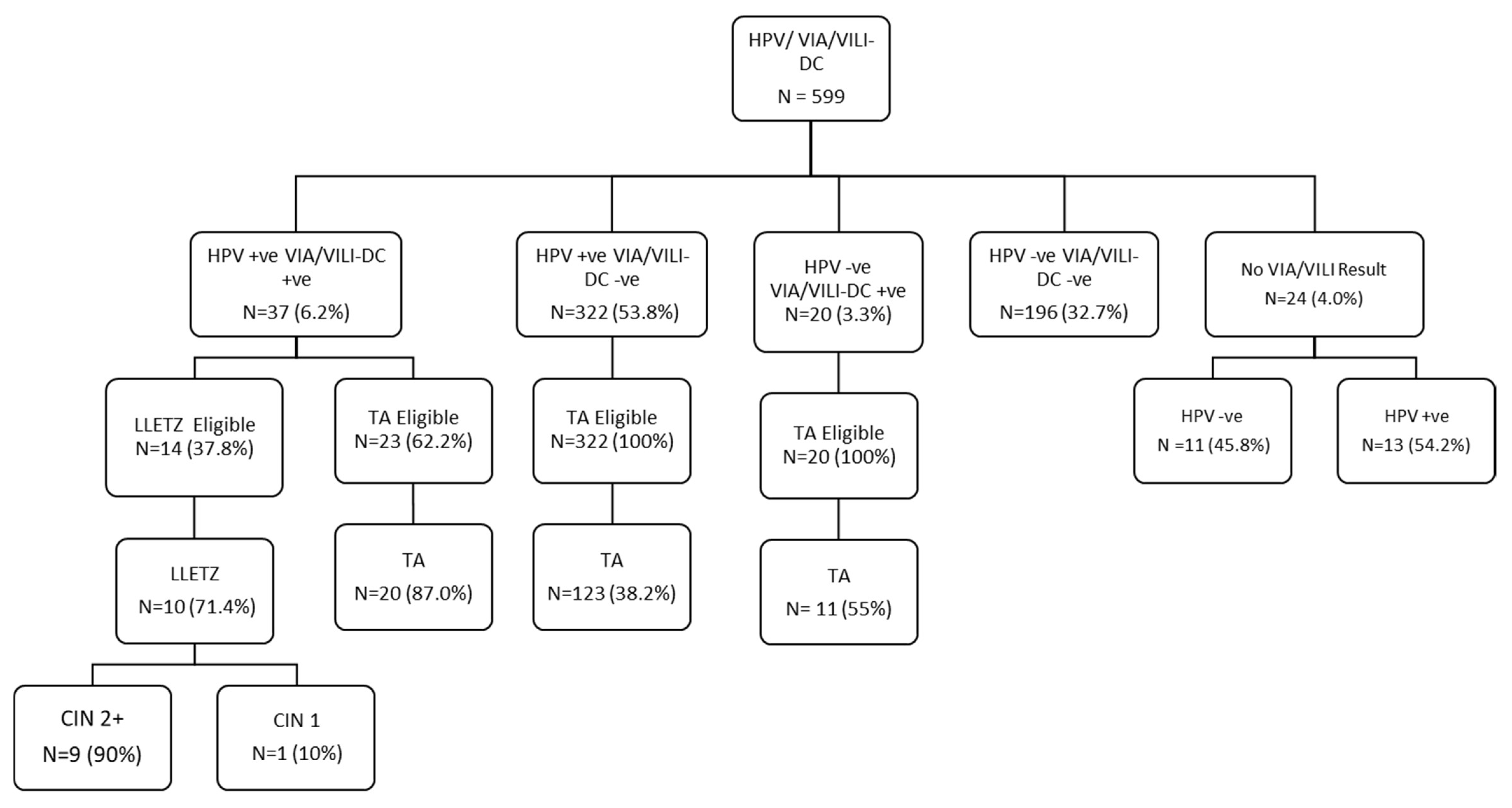
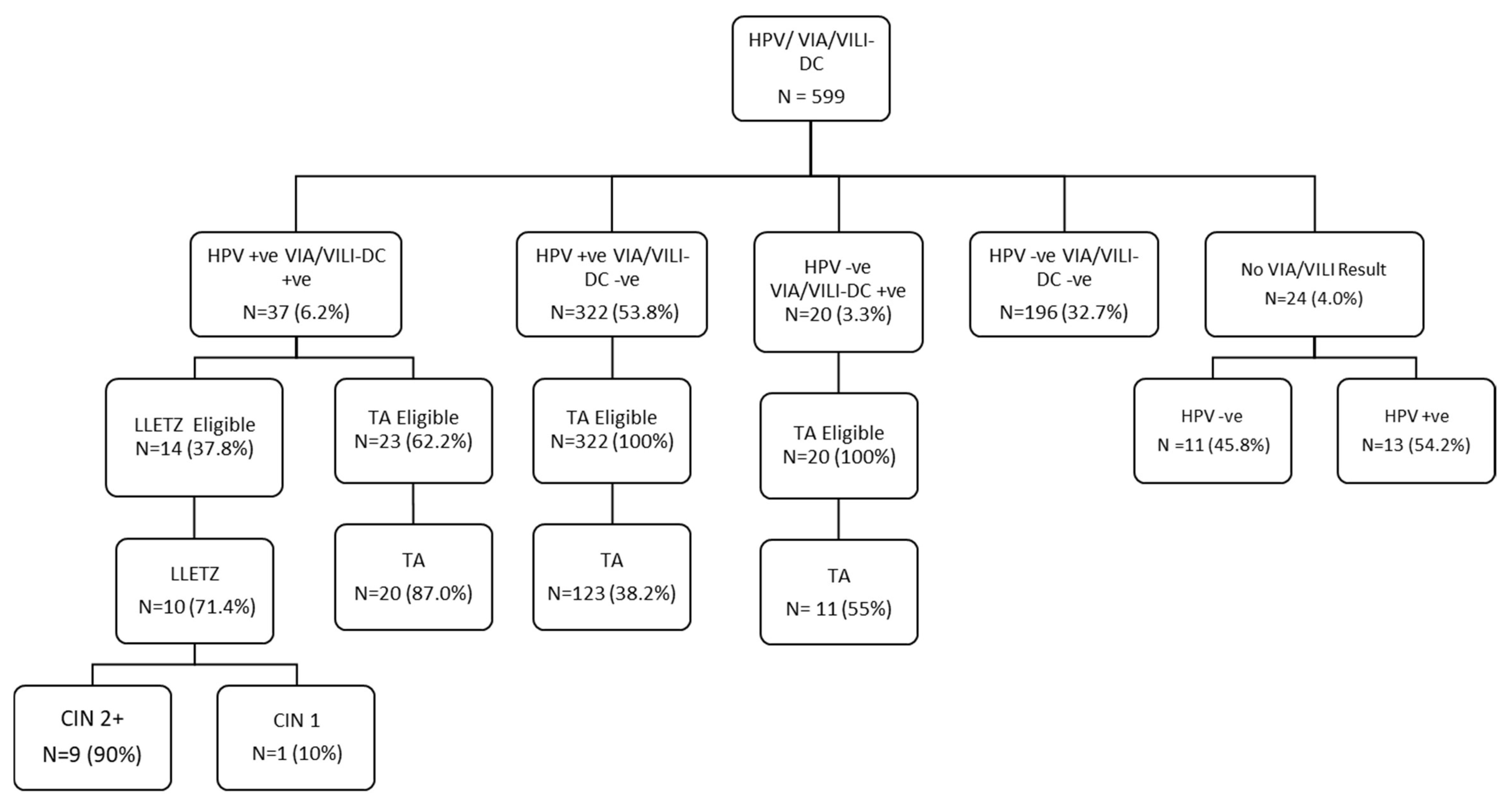
3.2. VIA/VILI-DC Results
3.3. Treatment Uptake
4. Discussion
4.1. Human Papillomavirus Genotyping
4.2. Precancerous Lesions of the Cervix
4.3. Treatment Uptake
4.4. Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Comprehensive Cervical Cancer Control. December 2014, p. 364. Available online: http://www.who.int/reproductivehealth/publications/cancers/cervical-cancer-guide/en/%5Cnwww.who.int (accessed on 26 November 2014).
- Bitty-Anderson, A.M.; Gbeasor-Komlanvi, F.A.; Bakoubayi, A.W.; Bakoubayi, A.W.; Tchankoni, M.K.; Sadio, A.J.; Salou, M.; Dagnra, C.A.; Ekouevi, D.K.; Coffie, P.A. High burden of self-reported sexually transmitted infections among female sex workers in Togo in 2021. Front. Public Health 2022, 10, 915029. [Google Scholar] [CrossRef] [PubMed]
- Strzelczyk, J.K.; Biernacki, K.; Gaździcka, J.; Chełmecka, E.; Miśkiewicz-Orczyk, K.; Zięba, N.; Strzelczyk, J.; Misiołek, M. The Prevalence of High- and Low-Risk Types of HPV in Patients with Squamous Cell Carcinoma of the Head and Neck, Patients with Chronic Tonsillitis, and Healthy Individuals Living in Poland. Diagnostics 2021, 11, 2180. [Google Scholar] [CrossRef] [PubMed]
- Wright, T.C.; Cox, T.J. Cervical Cancer: Epidemiology and Etiology. In Modern Colposcopy: Textbook and Atlas, 3rd ed.; Mayeaux, E.J., Cox, J.T., Eds.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014; pp. 61–73. [Google Scholar]
- Cox, J.T.; Chelmow, D.P.; Moscicki, A.B. Management of Abnormal Cervical Cancer Screening. In Modern Colposcopy: Textbook and Atlas, 3rd ed.; Mayeaux, E.J., Cox, J.T., Eds.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014; pp. 571–598. [Google Scholar]
- Radzki, D.; Kusiak, A.; Ordyniec-Kwaśnica, I.; Bondarczuk, A. Human papillomavirus and leukoplakia of the oral cavity: A systematic review. Postep Dermatol. I Alergol. 2022, 39, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Visalli, G.; Di Pietro, A.; Currò, M.; Ciarello, M.P.; D’andrea, F.; Nunnari, G.; Pellicanò, G.F.; Facciolà, A. How much does hiv positivity affect the presence of oral hpv? A molecular epidemiology survey. Int. J. Environ. Res. Public Health 2021, 18, 8999. [Google Scholar] [CrossRef]
- Lee, G.; Elit, L.; Ngalla, C.; Manjuh, F.; Bardin, R.; Manga, S. Multiple Anogenital Cancers in a 26-Year-Old Female: A Case Report. SciBase Obstet. Gynecol. 2023, 1, 4–7. [Google Scholar]
- Lien, K.; Mayer, W.; Herrera, R.; Padilla, N.T.; Cai, X.; Lin, V.; Pholcharoenchit, R.; Palefsky, J.; Tugizov, S.M. HIV-1 Proteins gp120 and Tat Promote Epithelial-Mesenchymal Transition and Invasiveness of HPV-Positive and HPV-Negative Neoplastic Genital and Oral Epithelial Cells. Microbiol. Spectr. 2022, 10, e0362222. [Google Scholar] [CrossRef]
- Vieira, G.V.; Somera Dos Santos, F.; Lepique, A.P.; da Fonseca, C.K.; Innocentini, L.M.A.R.; Braz-Silva, P.H.; Quintana, S.M.; Sales, K.U. Proteases and HPV-Induced Carcinogenesis. Cancers 2022, 14, 3038. [Google Scholar] [CrossRef]
- Billong, S.C.; Nguefack-Tsague, G.; Fokam, J.; Emmanuel, F.; Isac, S.; Fodjo, R.A.T.; Ngoufack, M.N.; Kwedi, S.; Moukam, L.V.; Tchetmi, T.; et al. Mapping and size estimates of female sex workers in Cameroon: Toward informed policy for design and implementation in the national HIV program. PLoS ONE 2019, 14, e0212315. [Google Scholar] [CrossRef]
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Khalil, A.I.; Baussano, I.; Shah, A.S.V.; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Andrea, S.; et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob Health 2021, 9, e161–e169. [Google Scholar] [CrossRef]
- Hooi, D.J.; Quint, W.G.V.; Lissenberg-Witte, B.I.; Kenterd, G.; Pinedoe, H.M.; de Koningb, M.N.C.; Meije, C.J.L.M. Human papillomavirus (HPV) types prevalence in cervical samples of female sex-workers on Curaçao. Prev. Med. Rep. 2018, 11, 120–124. [Google Scholar] [CrossRef]
- Zhao, Y.; Bao, H.; Ma, L.; Xie, Y.; Zhang, S.-K.; Qiao, Y.-L.; Qi, X.-R.; Yang, C.-X.; Zhao, F.H. Real-world effectiveness of primary screening with high-risk human papillomavirus testing in the cervical cancer screening programme in China: A nationwide, population-based study. BMC Med. 2021, 19, 164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Guidelines for Screening and Treatment of Precancerous Lesions for Cervical Cancer Prevention. Available online: http://www.guideline.gov/content.aspx?f=rss&id=49521&osrc=12 (accessed on 19 November 2013).
- Zhang, W.; Du, H.; Huang, X.; Liu, Y.; Shi, B.; Zhang, W.; Qu, X.; Wei, L. Evaluation of an isothermal amplification HPV detection assay for primary cervical cancer screening. Infect. Agent. Cancer. 2020, 15, 65. [Google Scholar] [CrossRef] [PubMed]
- Degregorio, G.; Manga, S.; Kiyang, E.; Manjuh, F.; Bradford, L.; Cholli, P.; Wamai, R.; Ogembo, R.; Sando, Z. Implementing a fee-for-service cervical cancer screening and treatment program in Cameroon: Challenges and opportunities. Oncologist 2017, 22, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Manga, S.; Parham, G.; Benjamin, N.; Nulah, K.; Sheldon, L.K.; Welty, E.; Ogembo, G.J.; Bradford, L.; Sando, Z.; Shields, R.; et al. Cervical Cancer Screening in Cameroon. J. Low. Genit. Tract Dis. 2015, 19, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Ramírez, A.; López-Monteon, A.; Ramos-Ligonio, A.; Méndez-Bolaina, E.; Guapillo-Vargas, M.R.B. Prevalence of Trichomonas vaginalis and Human papillomavirus in female sex workers in Central Veracruz, Mexico. Rev. Argent. Microbiol. 2018, 50, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Velazquez-Hernandez, N.; Sanchez-Anguiano, L.F.; Guerra-Infante, F.M.; Aguilar-Durana, M.; Perez-Alamosa, A.R.; Estrada-Martineza, S.; Navarrete-Floresa, J.A.; Sandoval-Carrilloa, A.A.; Antuna-Salcido, E.I.; Hernandez-Tinoco, J.; et al. Human Papillomavirus Infection in Female Sex Workers: A Case-Control Study. J. Clin. Med. Res. 2019, 11, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Adams, A.R.; Nortey, P.A.; Dortey, B.A.; Asmah, R.H.; Wiredu, E.K. Cervical Human Papillomavirus Prevalence, Genotypes, and Associated Risk Factors among Female Sex Workers in Greater Accra, Ghana. J. Oncol. 2019, 2019, 8062176. [Google Scholar] [CrossRef]
- Ferré, V.M.; Ekouevi, D.K.; Gbeasor-Komlanvi, F.A.; Collin, G.; Le Hingrat, Q.; Tchounga, B.; Salou, M.; Descamps, D.; Charpentier, C.; Dagnra, A.C. Prevalence of human papillomavirus, human immunodeficiency virus and other sexually transmitted infections among female sex workers in Togo: A national cross-sectional survey. Clin. Microbiol. Infect. 2019, 25, 1560.e1–1560.e7. [Google Scholar] [CrossRef]
- Montano, S.M.; Hsieh, E.J.; Calderón, M.; Ton, T.G.N.; Quijano, E.; Solari, V.; Zunt, J.R. Human papillomavirus infection in female sex workers in Lima, Peru. Sex Transm. Infect. 2011, 87, 81–82. [Google Scholar] [CrossRef]
- Menon, S.; Van Den Broeck, D.; Rossi, R.; Ogbe, E.; Mabeya, H. Multiple HPV infections in female sex workers in Western Kenya: Implications for prophylactic vaccines within this subpopulation. Infect. Agent. Cancer. 2017, 12, 2. [Google Scholar] [CrossRef]
- Sweet, K.; Bosire, C.; Sanusi, B.; Sherrod, C.J.; Kwatampora, J.; Waweru, W.; Mugo, N.; Kimani, J.; Ting, J.; Clark, J.; et al. Prevalence, incidence, and distribution of human papillomavirus types in female sex workers in Kenya. Int. J. STD AIDS 2020, 31, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Diop-Ndiaye, H.; Beiter, K.; Gheit, T.; Ndoyea, A.S.; Draméa, A.; McKay-Chopinb, S.; Tommasinob, M.; Boyea, C.S.B.; Syllab, B.; Kanea, C.T. Human Papillomavirus infection in Senegalese female sex workers. Papillomavirus Res. 2019, 7, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.; Blas, M.M.; Cabral, A.; Byraiah, G.; Guerra-Giraldez, C.; Sarabia-Vega, V.; Carcamo, C.; Gravitt, P.E.; Halsey, N.A. Human papillomavirus prevalence, cervical abnormalities and risk factors among female sex workers in Lima, Peru. Int. J. STD AIDS 2012, 23, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Farahmand, M.; Moghoofei, M.; Dorost, A.; Abbasi, S.; Monavari, S.H.; Kiani, S.J.; Tavakoli, A. Prevalence and genotype distribution of genital human papillomavirus infection in female sex workers in the world: A systematic review and meta-analysis. BMC Public Health. 2020, 20, 1455. [Google Scholar] [CrossRef]
- Okoye, J.O.; Ofodile, C.A.; Adeleke, O.K.; Obioma, O. Prevalence of high-risk HPV genotypes in sub-Saharan Africa according to HIV status: A 20-year systematic review. Epidemiol. Health 2021, 43, e2021039. [Google Scholar] [CrossRef] [PubMed]
- Nyasenu, Y.T.; Gbeasor-Komlanvi, F.A.; Ehlan, A.; Issa, S.A.R.; Dossim, S.; Kolou, M.; Yambiyo, B.M.; David, M.P.; Salou, M.; Ekouevi, D.K.; et al. Prevalence and distribution of human papillomavirus (hpv) genotypes among hiv infected women in lomé, Togo. PLoS ONE 2019, 14, e0212516. [Google Scholar] [CrossRef] [PubMed]
- Looker, K.J.; Rönn, M.M.; Brock, P.M.; Brisson, M.; Drolet, M.; Mayaud, P.; Boily, M. Evidence of synergistic relationships between HIV and Human Papillomavirus (HPV): Systematic reviews and meta-analyses of longitudinal studies of HPV acquisition and clearance by HIV status, and of HIV acquisition by HPV status. J. Int. AIDS Soc. 2018, 21, e25110. [Google Scholar] [CrossRef]
- World Health Organization. Family Planning: A Global Handbook for Providers. 2018 EDITION What’ s New in This Edition? World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Repp, K.K.; Nielson, C.M.; Fu, R.; Schafer, S.; Lazcano-Ponce, E.; Salmero, J.; Quiterio, M.; Villa, L.L.; Giuliano, A.R. Male human papillomavirus prevalence and association with condom use in Brazil, Mexico, and the United States. J. Infect. Dis. 2012, 205, 1287–1293. [Google Scholar] [CrossRef]
- Tounkara, F.K.; Téguété, I.; Guédou, F.A.; Be´hanzin, L.C.; Traore, S.; Aza-Gnandji, M.; Keita, B.; Guenoun, J.; Keita, B.; Guenoun, J.; et al. Human papillomavirus genotype distribution and factors associated among female sex workers in West Africa. PLoS ONE 2020, 15, e0242711. [Google Scholar] [CrossRef]
- Rikhotso, R.R.; Mitchell, E.M.; Wilson, D.T.; Doede, A.; Matume, N.D.; Bessong, P.O. Prevalence, and distribution of selected cervical human papillomavirus types in HIV infected and HIV uninfected women in South Africa, 1989–2021: A narrative review. South. Afr. J. Infect. Dis. 2022, 37, a363. [Google Scholar] [CrossRef]
- Alarcón-Romero, L.d.C.; Organista-Nava, J.; Gómez-Gómez, Y.; Ortiz-Ortiz, J.; Hernández-Sotelo, D.; del Moral-Hernández, O.; Mendoza-Catalán, M.A.; Antaño-Arias, R.; Leyva-Vázquez, M.A.; Sales-Linares, N.; et al. Prevalence and Distribution of Human Papillomavirus Genotypes (1997–2019) and Their Association With Cervical Cancer and Precursor Lesions in Women From Southern Mexico. Cancer Control 2022, 29, 10732748221103331. [Google Scholar] [CrossRef] [PubMed]
- Ogembo, J.G.; Manga, S.; Nulah, K.; Foglabenchi, L.H.; Perlman, S.; Wamai, R.G.; Welty, T.; Welty, E.; Tih, P. Achieving high uptake of human papillomavirus vaccine in Cameroon: Lessons learned in overcoming challenges. Vaccine 2014, 32, 4399–4403. [Google Scholar] [CrossRef] [PubMed]
- DeGregorio, G.A.; Bradford, L.S.; Manga, S.; Manjuh, F.; Bradford, L.; Cholli, P.; Wamai, R.; Ogembo, R.; Sando, Z.; Liu, Y.; et al. Prevalence, predictors, and same-day treatment of positive VIA enhanced by digital cervicography and histopathology results in a cervical cancer prevention program in Cameroon. PLoS ONE 2016, 11, e0157319. [Google Scholar] [CrossRef] [PubMed]
- Namale, G.; Mayanja, Y.; Kamacooko, O.; Bagiire, D.; Ssali, A.; Seeley, J.; Newton, R.; Kamali, A. Visual inspection with acetic acid (VIA) positivity among female sex workers: A cross-sectional study highlighting one-year experiences in early detection of pre-cancerous and cancerous cervical lesions in Kampala, Uganda. Infect. Agent. Cancer 2021, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Kulkarni, V.; Darak, T.; Mahajan, U.; Srivastava, Y.; Gupta, S.; Krishnan, S.; Mandolkar, M.; Bharti, A.C. Cervical cancer screening and treatment of cervical intraepithelial neoplasia in female sex workers using “screen and treat” approach. Int. J. Womens Health 2015, 7, 477–483. [Google Scholar] [CrossRef]
- Padalko, E.; Ali-Risasi, C.; Van Renterghem, L.; Bamelis, M.; De Mey, A.; Sturtewagen, O.; Vastenavond, H.; Broeck, D.V.; Weyers, S.; Praet, M. Evaluation of the clinical significance of human papillomavirus (HPV) 53. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 191, 7–9. [Google Scholar] [CrossRef]
- Devóglio, L.L.; Corrente, J.E.; Borgato, M.H.; Godoy, I. Smoking among female sex workers: Prevalence and associated variables. J. Bras. Pneumol. 2017, 43, 6–13. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | HPV Negative N = 227 (37.9%) 95 %CI: (34.0–41.8%) | HPV Positive N = 372 (62.1%) 95 %CI: (58.2–66.0%) | p Value |
|---|---|---|---|
| Age 30–39 40–49 ≥50 | 124 (36.3) 83 (40.7) 20 (37.7) | 218 (63.7) 121 (59.3) 33 (62.3) | 0.587 |
| Marital Status Married Single Others | 16 (44.4) 174 (36.2) 32 (43.8) | 20 (55.6) 307 (63.8) 41 (56.2) | 0.310 |
| Educational Level 0–7 years 8–14 years 15–17 years ≥18 | 46 (34.8) 98 (40.5) 10 (29.4) 7 (58.3) | 86 (65.2) 144 (59.5) 24 (70.6) 5 (41.7) | 0.228 |
| Site of Screening Bafoussam Yaoundé Douala | 17 (53.1) 97 (45.8) 113 (31.8) | 15 (46.9) 115 (54.2) 242 (68.2) | 0.001 |
| Other Occupation Domestic worker/housewife Trader/farmer Student Others | 191 (37.8) 11 (35.5) 5 (45.5) 12 (54.6) | 314 (62.2) 20 (64.5) 6 (54.5) 10 (45.4) | 0.418 |
| HIV Status Positive Negative | 158 (42.0) 51 (28.3) | 218 (58.0) 129 (71.7) | 0.002 |
| Religion Baptist Catholic Presbyterian Pentecostal Muslims Others | 16 (35.6) 117 (36.6) 36 (40.0) 23 (37.7) 8 (53.3) 17 (38.6) | 29 (64.4) 203 (63.4) 55 (60.4) 38 (62.3) 7 (46.7) 27 (61.4) | 0.852 |
| Duration in Sex work <3 years 3–7 years ≥7 years | 52 (40.3) 99 (34.6) 59 (38.8) | 77 (59.7) 187 (65.4) 93 (61.2) | 0.468 |
| Number of clients per day ≤5 6 to 10 11–14 ≥15 Do not want to respond | 126 (35.4) 63 (38.0) 4 (44.4) 10 (47.6) 24 (51.1) | 230 (64.6) 103 (62.0) 5 (55.6) 11 (52.4) 23 (48.9) | 0.247 |
| Income per month XAF < 50,000 XAF ≥ 50,000 Do not want to respond | 34 (31.5) 118 (34.4) 75 (50.7) | 74 (68.5) 225 (65.6) 73 (49.3) | 0.001 |
| Condom use Always Sometimes Depends on the customer’s preference Never Do not want to answer | 138 (36.2) 56 (35.0) 23 (53.5) 1 (50.0) 9 (75.0) | 243 (63.8) 104 (65.0) 20 (46.5) 1 (50.0) 3 (25.0) | 0.009 |
| Alcohol per week 0 to 5 bottles 6 to 10 bottles 11 to 14 bottles ≥15 bottles Do not want to respond | 73 (34.3) 47 (38.2) 21 (43.8) 29 (40.9) 57 (39.6) | 140 (65.7) 76(61.8) 27 (56.2) 42 (59.1) 87 (23.4) | 0.676 |
| Smoking per week 0 to 14 ≥15 Do not want to respond | 10 (41.7) 10 (37.0) 207 (37.8) | 14 (58.3) 17 (63.0) 341 (62.2) | 0.925 |
| Responded to smoking question Do not want to respond Responded | 207 (37.8) 20 (39.2) | 341 (62.2) 31 (60.8) | 0.839 |
| * Other sexual practices Oral sex Anal sex Sexting Group sex Do not want to answer | 22 (34.4) 10 (37.0) 1 (20.0) 16 (30.8) 4 (44.4) | 42 (65.6) 17 (63.0) 4 (80.0) 36 (69.2) 5 (55.6) | 0.539 0.925 0.656 0.268 0.736 |
| Treatment uptake Yes | 0 (0.0) | 141 (100.0) | <0.0001 |
| Predictors | HPV Infection | |||||
|---|---|---|---|---|---|---|
| cOR | 95% CI | p-Value | aOR | 95% CI | p-Value | |
| Age 30–39 40–49 ≥50 | Ref 0.83 0.94 | -- 0.58–1.18 0.52–1.71 | -- 0.302 0.835 | |||
| Marital Status Married Single Others | Ref 1.41 1.03 | -- 0.71–2.80 0.46–2.29 | -- 0.323 0.952 | |||
| Educational Level 0–7 years 8–14 years 15–17 years ≥18 | 2.62 2.06 3.36 Ref | 0.79–8.71 0.64–6.67 0.86–13.14 -- | 0.117 0.229 0.082 -- | |||
| Site of Screening Bafoussam Yaoundé Douala | Ref 1.34 2.43 | -- 0.64–2.83 1.17–5.03 | -- 0.437 0.017 | Ref 1.49 2.18 | -- 0.64–3.46 0.93–5.09 | -- 0.351 0.072 |
| Other Occupation Domestic worker/housewife Trader/farmer Student Others | Ref 1.11 0.73 0.51 | -- 0.52–2.36 0.22–2.42 0.22–1.20 | -- 0.794 0.607 0.121 | |||
| HIV Status Positive Negative | 1.83 Ref | 1.25–2.69 -- | 0.002 -- | 1.65 Ref | 1.11–2.45 -- | 0.014 -- |
| Religion Baptist Catholic Presbyterian Pentecostal Muslim Others | 1.10 1.05 0.93 Ref 0.53 0.96 | 0.49–2.44 0.60–1.85 0.48–1.80 -- 0.17–1.65 0.43–2.14 | 0.821 0.865 0.818 -- 0.274 0.923 | |||
| Duration in Sex work <3 years 3–7 years ≥7 years | Ref 1.28 1.06 | -- 0.83–1.96 0.66–1.72 | -- 0.265 0.799 | |||
| Income per month XAF < 50,000 XAF ≥ 50,000 Do not want to respond | Ref 0.88 0.45 | -- 0.55–1.39 0.27–0.75 | -- 0.576 0.002 | Ref 0.75 0.49 | -- 0.45–1.24 0.27–0.89 | -- 0.261 0.019 |
| Condom use Always Sometimes Depends on the customer’s preference Never Do not want to answer | Ref 1.06 0.49 0.57 0.19 | -- 072–1.55 0.26–0.93 0.04–9.15 0.05–0.71 | -- 0.787 0.029 0.690 0.014 | Ref 1.38 0.50 1.26 0.50 | -- 0.89–2.15 0.25–1.00 0.08–20.90 0.12–2.05 | -- 0.152 0.049 0.874 0.337 |
| Characteristics | VIA/VILI Negative N = 518 90.1% | VIA/VILI Positive N = 57 9.9% | p Value |
|---|---|---|---|
| Age 30–39 40–49 ≥50 | 291 (88.2) 177 (92.2) 50 (94.3) | 39 (11.8) 15 (7.8) 3 (5.7) | 0.186 |
| Marital Status Married Single Others | 33 (91.7) 411 (89.2) 67 (95.7) | 3 (8.3) 50 (10.8) 3 (4.3) | 0.219 |
| Educational Level 0–7 years 8–14 years 15–17 years ≥18 | 119 (91.5) 204 (89.5) 27 (84.4) 10 (90.9) | 11 (8.5) 24 (10.5) 5 (15.6) 1 (9.1) | 0.607 |
| Site of Screening Bafoussam Yaoundé Douala | 27 (90.0) 188 (94.5) 303 (87.6) | 3 (10.0) 11 (5.5) 43 (12.4) | 0.035 |
| Other Occupation Domestic worker/housewife Trader/farmer Student Others | 433 (89.3) 29 (93.5) 9 (100.0) 19 (86.4) | 52 (10.7) 2 (6.5) 0 (0) 3 (5.3) | 0.728 |
| HIV Status Positive Negative | 150 (85.7) 331 (91.7) | 25 (14.3) 30 (8.3) | 0.033 |
| Religion (N = 555) Baptist Catholic Presbyterian Pentecostal Muslim Others | 39 (90.7) 277 (90.8) 80 (90.9) 50 (82.0) 13 (86.7) 39 (90.7) | 4 (9.3) 28 (9.2) 8 (9.1) 11 (18.0) 2 (13.3) 4 (9.3) | 0.441 |
| Duration in Sex work <3 years 3–7 years ≥7 years | 114 (90.5) 243 (88.7) 134 (92.4) | 12 (9.5) 31 (11.3) 11 (7.6) | 0.506 |
| Number of clients per day ≤5 6 to 10 11–14 ≥15 Do not want to respond | 303 (88.6) 147 (91.3) 8 (47.1) 19 (100.0) 41 (91.1) | 39 11.4() 14 (8.7) 9 (51.9) 0 (0) 4 (8.9) | 0.530 |
| Income per month XAF < 50,000 XAF ≥ 50,000 Do not want to respond | 99 (93.4) 293 (88.5) 126 (91.3) | 7 (6.6) 38 (11.5) 12 (8.7) | 0.295 |
| Condom use Always Sometimes Depends on the customer’s preference Never Do not want to answer | 330 (90.2) 142 (92.2) 34 (82.9) 2 (100.0) 10 (90.9) | 36 (9.8) 12 (7.8) 7 (17.1) 0 (0) 1 (9.1) | 0.449 |
| Alcohol per week 0 to 5 6 to 10 11 to 14 ≥15 Do not want to respond | 192 (92.3) 111 (92.5) 40 (83.3) 53 (85.5) 122 (89.0) | 16 (7.7) 9 (7.5) 8 (16.7) 9 (14.5) 15 (11.0) | 0.198 |
| Smoking per week 0 to 14 ≥15 Do not want to respond | 20 (95.2) 23 (92.0) 475 (89.8) | 1 (4.8) 2 (8.0) 54 (10.2)) | 0.922 |
| Responded to smoking question Do not want to respond Responded | 475 (89.8) 43 (93.5) | 54 (10.2) 3 (6.5) | 0.607 |
| * Other sexual practices Oral sex Anal sex Sexting Group sex Do not want to answer | 55 (91.7) 23 (88.5) 5 (100.0) 44 (89.8) 7 (77.8) | 5 (8.3) 3 (11.5) 0 (0.0) 5 (10.2) 2 (22.2) | 0.665 0.735 1.000 1.000 0.222 |
| Not Treated N 240 (63.3) | Treated N = 139 (36.7) | p Value | |
|---|---|---|---|
| VIA/VILI Positive Negative | 30 (52.6) 210 (65.2) | 27 (47.4) 112 (34.8) | 0.069 |
| Age 30–39 40–49 ≥50 | 151 (66.8) 68 (57.1) 21 (61.8) | 75 (33.2) 51 (42.9) 13 (38.2) | 0.204 |
| Educational Level 0–7 years 8–14 years 15–17 years ≥18 | 62 (70.5) 90 (62.5) 17 (68.0) 3 (50.0) | 26 (29.5) 54 (37.5) 8 (32.0) 3 (50.0) | 0.507 |
| HIV Status Positive Negative | 74 (56.1) 150 (67.6) | 58 (43.9) 72 (32.4) | 0.030 |
| Site of Screening Bafoussam Yaoundé Douala | 12 (85.7) 84 (75.7) 144 (57.4) | 2 (14.3) 30 (26.3) 107 (42.6) | 0.002 |
| Number of clients per day ≤5 6 to 10 11–14 ≥15 Do not want to respond | 137 (58.6) 72 (67.9) 3 (60.0) 8 (88.9) 20 (80.0) | 97 (41.4) 34 (32.1) 2 (40.0) 1 (11.1) 5 (20.0) | 0.060 |
| Income per month XAF < 50,000 XAF ≥ 50,000 Do not want to respond | 49 (64.0) 138 (57.5) 54 (73.0) | 27 (36.0) 92 (40.0) 20 (27.0) | 0.130 |
| Alcohol per week 0 to 5 6 to 10 11 to 14 ≥15 Do not want to respond | 86 (60.6) 55 (69.6) 22 (68.8) 26 (66.7) 51 (58.2) | 56 (39.4) 24 (30.4) 10 (31.2) 13 (33.3) 36 (25.9) | 0.519 |
| Smoking per week 0 to 14 ≥15 Do not want to respond | 6 (50.0) 11 (68.8) 223 (63.5) | 6 (50.0) 5 (31.2) 128 (36.5) | 0.569 |
| Responded to smoking question Do not want to respond Responded | 223 (63.5) 17 (60.7) | 128 (36.5) 11 (39.3) | 0.766 |
| Predictors | Treatment Uptake | |||||
|---|---|---|---|---|---|---|
| cOR | 95% CI | p-Value | aOR | 95% CI | p-Value | |
| Age 30–39 40–49 ≥50 | Ref 1.51 1.25 | Ref 0.96–2.38 0.59–2.63 | -- 0.077 0.562 | |||
| Marital Status Married Single Others | Ref 0.984 0.75 | Ref 0.35–2.01 0.25–2.22 | -- 0.688 0.604 | |||
| Educational Level 0–7 years 8–14 years 15–17 years ≥18 | 0.42 0.60 0.47 Ref | 0.08–2.22 0.12–3.08 0.08–2.87 -- | 0.306 0.540 0.414 -- | |||
| Site of Screening Bafoussam Yaoundé Douala | Ref 2.14 4.46 | -- 0.45–10.13 0.98–20.33 | -- 0.337 0.054 | Ref 1.64 3.30 | -- 0.33–8.08 0.69–15.68 | -- 0.547 0.134 |
| HIV Status Positive Negative | 1.63 Ref | 1.05–2.55 -- | 0.030 -- | 1.53 -- | 0.97–2.40 -- | 0.065 -- |
| Duration in Sex work <3 years 3–7 years ≥7 years | Ref 1.14 1.06 | -- 0.66–1.98 0.56–1.99 | -- 0.348 0.771 | |||
| Income per month XAF < 50,000 XAF ≥ 50,000 Do not want to respond | Ref 1.19 0.66 | -- 0.69–2.03 0.33–1.32 | -- 0.538 0.240 | |||
| Condom use Always Sometimes Depends on the customer’s preference Never Do not want to answer | Ref 0.79 1.38 <0.001 0.54 | -- 0.48–1.27 0.50–3.20 <0.001–>999.9 0.06–5.29 | -- 0.314 0.457 0.987 0.599 | |||
| VIA/VILI Positive Negative | 1.69 Ref | 0.96–2.98 -- | 0.071 -- | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manga, S.M.; Ye, Y.; Nulah, K.L.; Manjuh, F.; Fokom-Domgue, J.; Scarinci, I.; Tita, A.N. Human Papillomavirus Types and Cervical Cancer Screening among Female Sex Workers in Cameroon. Cancers 2024, 16, 243. https://doi.org/10.3390/cancers16020243
Manga SM, Ye Y, Nulah KL, Manjuh F, Fokom-Domgue J, Scarinci I, Tita AN. Human Papillomavirus Types and Cervical Cancer Screening among Female Sex Workers in Cameroon. Cancers. 2024; 16(2):243. https://doi.org/10.3390/cancers16020243
Chicago/Turabian StyleManga, Simon M., Yuanfan Ye, Kathleen L. Nulah, Florence Manjuh, Joel Fokom-Domgue, Isabel Scarinci, and Alan N. Tita. 2024. "Human Papillomavirus Types and Cervical Cancer Screening among Female Sex Workers in Cameroon" Cancers 16, no. 2: 243. https://doi.org/10.3390/cancers16020243
APA StyleManga, S. M., Ye, Y., Nulah, K. L., Manjuh, F., Fokom-Domgue, J., Scarinci, I., & Tita, A. N. (2024). Human Papillomavirus Types and Cervical Cancer Screening among Female Sex Workers in Cameroon. Cancers, 16(2), 243. https://doi.org/10.3390/cancers16020243