

Systematic Review and Meta-Analysis of Particle Beam Therapy versus Photon Radiotherapy for Skull Base Chordoma: TRP-Chordoma 2024

 , , ,
, , ,  , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
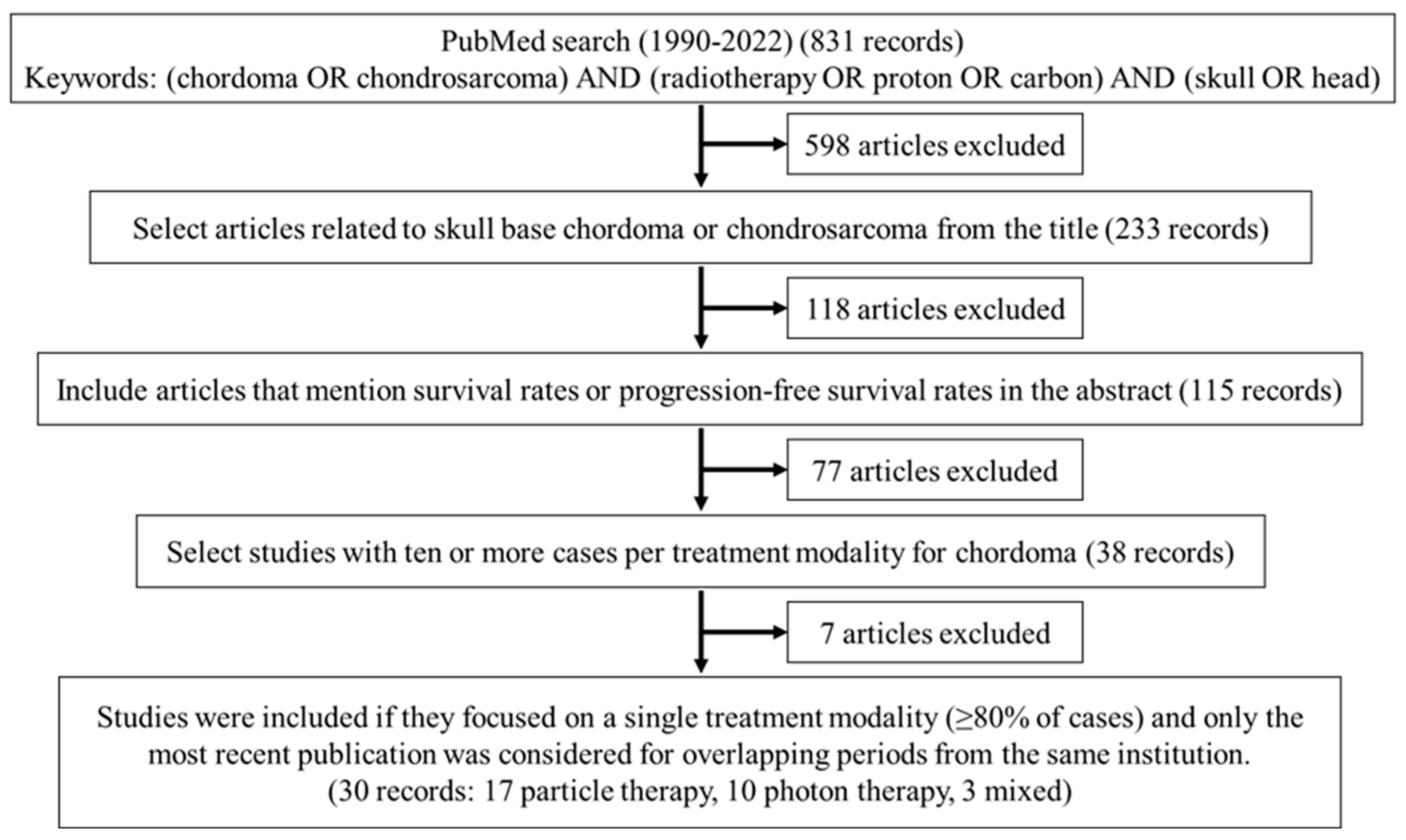
2. Materials and Methods
2.1. Selection Criteria for Meta-Analysis
2.2. Statistical Analysis
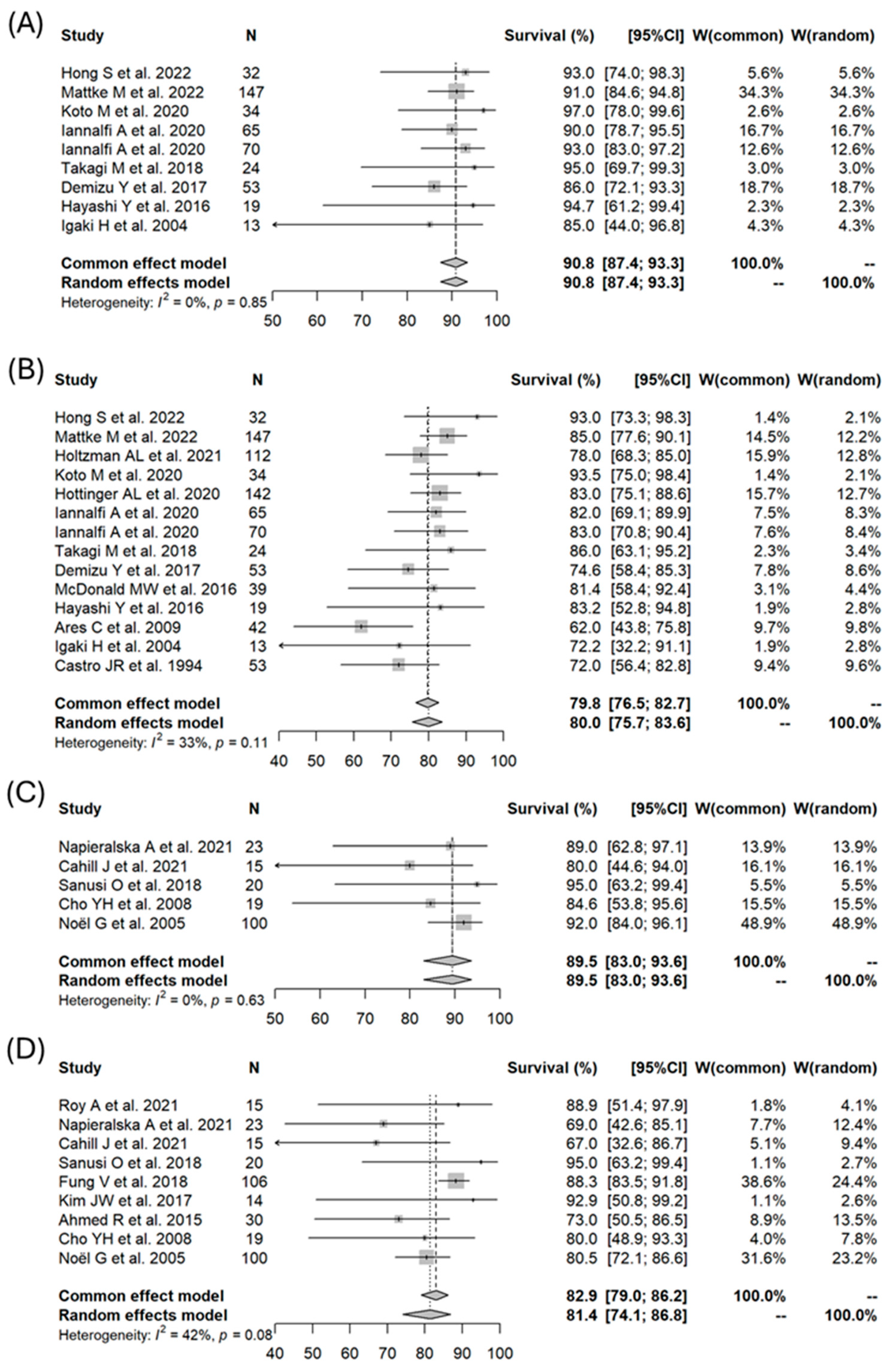
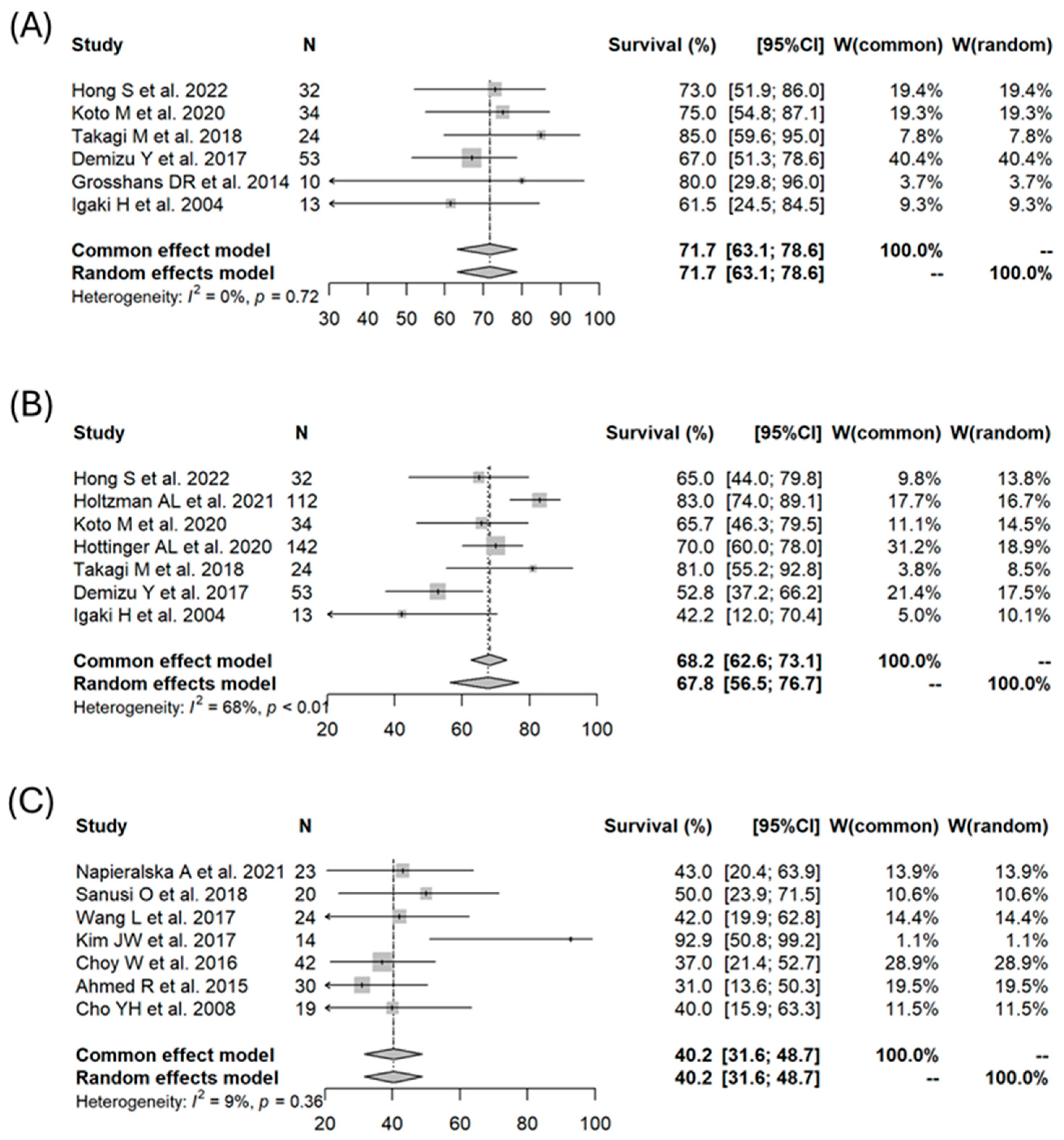
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bakker, S.H.; Jacobs, W.C.H.; Pondaag, W.; Gelderblom, H.; Nout, R.A.; Dijkstra, P.D.S.; Peul, W.C.; Vleggeert-Lankamp, C.L.A. Chordoma: A systematic review of the epidemiology and clinical prognostic factors predicting progression-free and overall survival. Eur. Spine J. 2018, 27, 3043–3058. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Bone Cancer (Version 1.2024). Available online: https://www.nccn.org/professionals/physician_gls/pdf/bone.pdf (accessed on 23 March 2024).
- Barber, S.M.; Sadrameli, S.S.; Lee, J.J.; Fridley, J.S.; Teh, B.S.; Oyelese, A.A.; Telfeian, A.E.; Gokaslan, Z.L. Chordoma-current understanding and modern treatment paradigms. J. Clin. Med. Res. 2021, 10, 1054. [Google Scholar] [CrossRef]
- Chanplakorn, P.; Lertudomphonwanit, T.; Homcharoen, W.; Suwanpramote, P.; Laohacharoensombat, W. Results following surgical resection of recurrent chordoma of the spine: Experience in a single institution. World J. Surg. Oncol. 2020, 18, 228. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Li, M.; Shi, J.; Jing, L.; Zhai, Y.; Zhang, S.; Wang, J.; Zhao, P.; Li, C.; Gui, S.; et al. Mid-term follow-up surgical results in 284 cases of clival chordomas: The risk factors for outcome and tumor recurrence. Neurosurg. Rev. 2022, 45, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Dial, B.L.; Kerr, D.L.; Lazarides, A.L.; Catanzano, A.A.; Green, C.L.; Risoli, T., Jr.; lazer, D.G.; Goodwin, R.C.; Brigman, B.E.; Eward, W.C.; et al. The role of radiotherapy for chordoma patients managed with surgery: Analysis of the National Cancer Database. Spine 2020, 45, E742–E751. [Google Scholar] [CrossRef]
- Hug, E.B.; Pelak, M.; Frank, S.J.; Fossati, P. A review of particle therapy for skull base tumors: Modern considerations and future directions. Int. J. Part. Ther. 2021, 8, 168–178. [Google Scholar] [CrossRef]
- Zhou, J.; Yang, B.; Wang, X.; Jing, Z. Comparison of the effectiveness of radiotherapy with photons and particles for chordoma after surgery: A meta-analysis. World Neurosurg. 2018, 117, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, S.L.; Bilsky, M.H.; Laufer, I. Chordomas of the skull base, mobile spine, and sacrum: An epidemiologic investigation of presentation, treatment, and survival. World Neurosurg. 2018, 113, e618–e627. [Google Scholar] [CrossRef] [PubMed]
- Stacchiotti, S.; Sommer, J.; Chordoma Global Consensus Group. Building a global consensus approach to chordoma: A position paper from the medical and patient community. Lancet Oncol. 2015, 16, e71–e83. [Google Scholar] [CrossRef]
- Almefty, K.; Pravdenkova, S.; Colli, B.O.; Al-Mefty, O.; Gokden, M. Chordoma and chondrosarcoma: Similar, but quite different, skull base tumors. Cancer 2007, 110, 2457–2467. [Google Scholar] [CrossRef]
- Bohman, L.E.; Koch, M.; Bailey, R.L.; Alonso-Basanta, M.; Lee, J.Y.K. Skull base chordoma and chondrosarcoma: Influence of clinical and demographic factors on prognosis: A SEER analysis. World Neurosurg. 2014, 82, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Lu, V.M.; O’Connor, K.P.; Mahajan, A.; Carlson, M.L.; Van Gompel, J.J. Carbon ion radiotherapy for skull base chordomas and chondrosarcomas: A systematic review and meta-analysis of local control, survival, and toxicity outcomes. J. Neurooncol. 2020, 147, 503–513. [Google Scholar] [CrossRef]
- Available online: http://prisma-statement.org/prismastatement/checklist.aspx?AspxAutoDetectCookieSupport=1 (accessed on 23 March 2024).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Laack, N.; Mahajan, A.; Choby, G.; O’Brien, E.; Stokken, J.; Janus, J.; Van Gompel, J.J. Analysis of early outcomes of pencil beam proton therapy compared with passive scattering proton therapy for clival chordoma. World Neurosurg. 2023, 171, e644–e653. [Google Scholar] [CrossRef] [PubMed]
- Mattke, M.; Ohlinger, M.; Bougatf, N.; Harrabi, S.; Wolf, R.; Seidensaal, K.; Welzel, T.; Röder, F.; Gerum, S.; Ellerbrock, M.; et al. Proton and carbon ion beam treatment with active raster scanning method in 147 patients with skull base chordoma at the Heidelberg ion beam therapy center: A single-center experience. Strahlenther Onkol. 2023, 199, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Holtzman, A.L.; Rotondo, R.L.; Rutenberg, M.S.; Indelicato, D.J.; De Leo, A.; Rao, D.; Patel, J.; Morris, C.G.; Mendenhall, W.M. Clinical outcomes following dose-escalated proton therapy for skull-base chordoma. Int. J. Part. Ther. 2021, 8, 179–188. [Google Scholar] [CrossRef]
- Koto, M.; Ikawa, H.; Kaneko, T.; Hagiwara, Y.; Hayashi, K.; Tsuji, H. Long-term outcomes of skull base chordoma treated with high-dose carbon-ion radiotherapy. Head Neck 2020, 42, 2607–2613. [Google Scholar] [CrossRef] [PubMed]
- Hottinger, A.L.; Bojaxhiu, B.; Ahlhelm, F.; Walser, M.; Bachtiary, B.; Zepter, S.; Lomax, T.; Pica, A.; Weber, D.C. Prognostic impact of the “Sekhar Grading System for Cranial Chordomas” in patients treated with pencil beam scanning proton therapy: An institutional analysis. Radiat. Oncol. 2020, 15, 96. [Google Scholar] [CrossRef] [PubMed]
- Iannalfi, A.; D’Ippolito, E.; Riva, G.; Molinelli, S.; Gandini, S.; Viselner, G.; Fiore, M.R.; Vischioni, B.; Vitolo, V.; Bonora, M.; et al. Proton and carbon ion radiotherapy in skull base chordomas: A prospective study based on a dual particle and a patient-customized treatment strategy. Neuro Oncol. 2020, 22, 1348–1358. [Google Scholar] [CrossRef]
- Takagi, M.; Demizu, Y.; Nagano, F.; Terashima, K.; Fujii, O.; Jin, D.; Mima, M.; Niwa, Y.; Katsui, K.; Suga, M.; et al. Treatment outcomes of proton or carbon ion therapy for skull base chordoma: A retrospective study. Radiat Oncol. 2018, 13, 232. [Google Scholar] [CrossRef]
- Demizu, Y.; Mizumoto, M.; Onoe, T.; Nakamura, N.; Kikuchi, Y.; Shibata, T.; Okimoto, T.; Sakurai, H.; Akimoto, T.; Ono, K.; et al. Proton beam therapy for bone sarcomas of the skull base and spine: A retrospective nationwide multicenter study in Japan. Cancer Sci. 2017, 108, 972–977. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.C.; Malyapa, R.; Albertini, F.; Bolsi, A.; Kliebsch, U.; Walser, M.; Pica, A.; Combescure, C.; Lomax, A.J.; Schneider, R. Long term outcomes of patients with skull-base low-grade chondrosarcoma and chordoma patients treated with pencil beam scanning proton therapy. Radiother. Oncol. 2016, 120, 169–174. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.W.; Linton, O.R.; Moore, M.G.; Ting, J.Y.; Cohen-Gadol, A.A.; Shah, M.V. Influence of residual tumor volume and radiation dose coverage in outcomes for clival chordoma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, Y.; Mizumoto, M.; Akutsu, H.; Takano, S.; Matsumura, A.; Okumura, T.; Kawabe, T.; Zenkoh, J.; Sakurai, H.; Tsuboi, K. Hyperfractionated high-dose proton beam radiotherapy for clival chordomas after surgical removal. Br. J. Radiol. 2016, 89, 20151051. [Google Scholar] [CrossRef] [PubMed]
- Grosshans, D.R.; Zhu, X.R.; Melancon, A.; Allen, P.K.; Poenisch, F.; Palmer, M.; McAleer, M.F.; McGovern, S.L.; Gillin, M.; DeMonte, F.; et al. Spot scanning proton therapy for malignancies of the base of skull: Treatment planning, acute toxicities, and preliminary clinical outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 540–546. [Google Scholar] [CrossRef]
- Deraniyagala, R.L.; Yeung, D.; Mendenhall, W.M.; Li, Z.; Morris, C.G.; Mendenhall, N.P.; Okunieff, P.; Malyapa, R.S. Proton therapy for skull base chordomas: An outcome study from the University of Florida Proton Therapy Institute. J. Neurol. Surg. B Skull Base 2014, 75, 53–57. [Google Scholar] [CrossRef]
- Ares, C.; Hug, E.B.; Lomax, A.J.; Bolsi, A.; Timmermann, B.; Rutz, H.P.; Schuller, J.C.; Pedroni, E.; Goitein, G. Effectiveness and safety of spot scanning proton radiation therapy for chordomas and chondrosarcomas of the skull base: First long-term report. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.C.; Rutz, H.P.; Pedroni, E.S.; Bolsi, A.; Timmermann, B.; Verwey, J.; Lomax, A.J.; Goitein, G. Results of spot-scanning proton radiation therapy for chordoma and chondrosarcoma of the skull base: The Paul Scherrer Institut Experience. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 401–409. [Google Scholar] [CrossRef]
- Igaki, H.; Tokuuye, K.; Okumura, T.; Sugahara, S.; Kagei, K.; Hata, M.; Ohara, K.; Hashimoto, T.; Tsuboi, K.; Takano, S.; et al. Clinical results of proton beam therapy for skull base chordoma. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1120–1126. [Google Scholar] [CrossRef]
- Castro, J.R.; Linstadt, D.E.; Bahary, J.P.; Petti, P.L.; Daftari, I.; Collier, J.M.; Gutin, P.H.; Gauger, G.; Phillips, T.L. Experience in charged particle irradiation of tumors of the skull base: 1977–1992. Int. J. Radiat. Oncol. Biol. Phys. 1994, 29, 647–655. [Google Scholar] [CrossRef]
- Roy, A.; Warade, A.; Jha, A.K.; Misra, B.K. Skull base chordoma: Long-term observation and evaluation of prognostic factors after surgical resection. Neurol. India 2021, 69, 1608–1612. [Google Scholar] [CrossRef] [PubMed]
- Napieralska, A.; Blamek, S. Intracranial chordoma: Radiosurgery, hypofractionated stereotactic radiotherapy and treatment outcomes. Rep. Pract. Oncol. Radiother. 2021, 26, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Cahill, J.; Ibrahim, R.; Mezey, G.; Yianni, J.; Bhattacharyya, D.; Walton, L.; Grainger, A.; Radatz, M.W.R. Gamma knife stereotactic radiosurgery for the treatment of chordomas and chondrosarcomas. Acta Neurochir. 2021, 163, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Hafez, R.F.A.; Fahmy, O.M.; Hassan, H.T. Gamma knife surgery efficacy in controlling postoperative residual clival chordoma growth. Clin. Neurol. Neurosurg. 2019, 178, 51–55. [Google Scholar] [CrossRef]
- Sanusi, O.; Arnaout, O.; Rahme, R.J.; Horbinski, C.; Chandler, J.P. Surgical resection and adjuvant radiation therapy in the treatment of skull base chordomas. World Neurosurg 2018, 115, e13–e21. [Google Scholar] [CrossRef] [PubMed]
- Fung, V.; Calugaru, V.; Bolle, S.; Mammar, H.; Alapetite, C.; Maingon, P.; De Marzi, L.; Froelich, S.; Habrand, J.L.; Dendale, R.; et al. Proton beam therapy for skull base chordomas in 106 patients: A dose adaptive radiation protocol. Radiother. Oncol. 2018, 128, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tian, K.; Ma, J.; Wang, K.; Jia, G.; Wu, Z.; Zhang, L.; Zhang, J. Effect comparisons among treatment measures on progression-free survival in patients with skull base chordomas: A retrospective study of 234 post-surgical cases. Acta Neurochir. 2017, 159, 1803–1813. [Google Scholar] [CrossRef]
- Kim, J.W.; Suh, C.O.; Hong, C.K.; Kim, E.H.; Lee, I.J.; Cho, J.; Lee, K.S. Maximum surgical resection and adjuvant intensity-modulated radiotherapy with simultaneous integrated boost for skull base chordoma. Acta Neurochir. 2017, 159, 1825–1834. [Google Scholar] [CrossRef] [PubMed]
- Choy, W.; Terterov, S.; Ung, N.; Kaprealian, T.; Trang, A.; DeSalles, A.; Chung, L.K.; Martin, N.; Selch, M.; Bergsneider, M.; et al. Adjuvant stereotactic radiosurgery and radiation therapy for the treatment of intracranial chordomas. J. Neurol. Surg. B Skull. Base 2016, 77, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, R.; Sheybani, A.; Menezes, A.H.; Buatti, J.M.; Hitchon, P.W. Disease outcomes for skull base and spinal chordomas: A single center experience. Clin. Neurol. Neurosurg 2015, 130, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.H.; Kim, J.H.; Khang, S.K.; Lee, J.K.; Kim, C.J. Chordomas and chondrosarcomas of the skull base: Comparative analysis of clinical results in 30 patients. Neurosurg. Rev. 2008, 31, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Noël, G.; Feuvret, L.; Calugaru, V.; Dhermain, F.; Mammar, H.; Haie-Méder, C.; Ponvert, D.; Hasboun, D.; Ferrand, R.; Nauraye, C.; et al. Chordomas of the base of the skull and upper cervical spine. One hundred patients irradiated by a 3D conformal technique combining photon and proton beams. Acta Oncol. 2005, 44, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Terahara, A.; Niemierko, A.; Goitein, M.; Finkelstein, D.; Hug, E.; Liebsch, N.; O’Farrell, D.; Lyons, S.; Munzenrider, J. Analysis of the relationship between tumor dose inhomogeneity and local control in patients with skull base chordoma. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Sprave, T.; Verma, V.; Sterzing, F.; Bruckner, T.; Hees, K.; Land, B.; Jäkel, O.; Herfarth, K.; Debus, J.; Uhl, M. Cost-effectiveness of carbon ion radiation therapy for skull base chordoma utilizing long-term (10-year) outcome data. Anticancer Res. 2018, 38, 4853–4858. [Google Scholar] [CrossRef] [PubMed]
- Austin, A.M.; Douglass, M.J.J.; Nguyen, G.T.; Dalfsen, R.; Le, H.; Gorayski, P.; Tee, H.; Penniment, M.; Penfold, S.N. Cost-effectiveness of proton therapy in treating base of skull chordoma. Australas. Phys. Eng. Sci. Med. 2019, 42, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Sher, D.J.; Tishler, R.B.; Pham, N.L.; Punglia, R.S. Cost-effectiveness analysis of intensity modulated radiation therapy versus proton therapy for oropharyngeal squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Q.; Roelofs, E.; Ramaekers, B.L.T.; Eekers, D.; van Soest, J.; Lustberg, T.; Hendriks, T.; Hoebers, F.; van der Laan, H.P.; Korevaar, E.W.; et al. Development and evaluation of an online three-level proton vs photon decision support prototype for head and neck cancer-comparison of dose, toxicity and cost-effectiveness. Radiother. Oncol. 2016, 118, 281–285. [Google Scholar] [CrossRef]
- Schulz-Ertner, D.; Karger, C.P.; Feuerhake, A.; Nikoghosyan, A.; Combs, S.E.; Jäkel, O.; Edler, L.; Scholz, M.; Debus, J. Effectiveness of carbon ion radiotherapy in the treatment of skull-base chordomas. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Mizumoto, M.; Oshiro, Y.; Kino, H.; Akutsu, H.; Nakai, K.; Sumiya, T.; Ishikawa, E.; Maruo, K.; Sakurai, H. Risk factors for radiation necrosis and local recurrence after proton beam therapy for skull base chordoma or chondrosarcoma. Cancers 2023, 15, 5687. [Google Scholar] [CrossRef]
- McDonald, M.W.; Linton, O.R.; Calley, C.S.J. Dose-volume relationships associated with temporal lobe radiation necrosis after skull base proton beam therapy. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 261–267. [Google Scholar] [CrossRef]
- Torres, M.A.; Chang, E.L.; Mahajan, A.; Lege, D.G.; Riley, B.A.; Zhang, X.; Lii, M.; Kornguth, D.G.; Pelloski, C.E.; Woo, S.Y. Optimal treatment planning for skull base chordoma: Photons, protons, or a combination of both? Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Basler, L.; Poel, R.; Schröder, C.; Bolsi, A.; Lomax, A.; Tanadini-Lang, S.; Guckenberger, M.; Weber, D.C. Dosimetric analysis of local failures in skull-base chordoma and chondrosarcoma following pencil beam scanning proton therapy. Radiat. Oncol. 2020, 15, 266. [Google Scholar] [CrossRef] [PubMed]
- Moreno, A.C.; Frank, S.J.; Garden, A.S.; Rosenthal, D.I.; Fuller, C.D.; Gunn, G.B.; Reddy, J.P.; Morrison, W.H.; Williamson, T.D.; Holliday, E.B.; et al. Intensity modulated proton therapy (IMPT): The future of IMRT for head and neck cancer. Oral. Oncol. 2019, 88, 66–74. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Author | Year | Modality | n | Age (Median) | Male (%) | Tumor Volume (Median, cc) | GTR Rate(%) | Total Dose (Median, Gy (RBE)) | 3y OS (%) | 5y OS (%) | 5y PFS (%) | Brain Necrosis (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hong [16] | 2022 | Proton | 32 | 44 | 46.9 | 100.0 | 74 | 93 | 93 | 65 | 13 | |
| Mattke [17] | 2022 | Particle | 147 | 51 | 57.8 | 40.4 | 0.0 | 91 | 85 | 14 | ||
| Holtzman [18] | 2021 | Proton | 112 | 52 | 68.8 | 97.3 | 73.8 | 78 | 83 | 4 | ||
| Koto [19] | 2020 | Carbon | 34 | 52 | 52.9 | 18.7 | 0.0 | 60.8 | 97 | 93.5 | 65.7 | 50 |
| Hottinger [20] | 2020 | Proton | 142 | 42 | 53.5 | 26.3 | 96.5 | 74 | 83 | 70 | ||
| Iannalfi [21] | 2020 | Carbon | 65 | 58 | 64.6 | 13 | 0.0 | 70.4 | 90 | 82 | 30 | |
| Iannalfi [21] | 2020 | Proton | 70 | 53 | 57.1 | 3.5 | 27.1 | 74 | 93 | 83 | 30 | |
| Takagi [22] | 2018 | Particle | 24 | 56 | 41.7 | 17 | 0.0 | 65 | 95 | 86 | 81 | 8 |
| Demizu [23] | 2017 | Proton | 53 | 56 | 70 | 86 | 74.6 | 52.8 | ||||
| Weber [24] | 2016 | Proton | 151 | 43 | 57.0 | 35.4 | 100.0 | 74 | ||||
| McDonald [25] | 2016 | Proton | 39 | 52 | 53.8 | 24.5 | 12.8 | 77.4 | 81.4 | 18 | ||
| Hayashi [26] | 2016 | Proton | 19 | 52 | 42.1 | 19 | 42.1 | 78.4 | 94.7 | 83.2 | 16 | |
| Grosshans [27] | 2014 | Proton | 10 | 43 | 100.0 | 69.8 | 20 | |||||
| Deraniyagala [28] | 2014 | Proton | 33 | 78.8 | 93.9 | 74 | ||||||
| Ares [29] | 2009 | Proton | 42 | 42.9 | 73.5 | 62 | 17 | |||||
| Weber [30] | 2005 | Proton | 18 | 39 | 16.4 | 74 | ||||||
| Igaki [31] | 2004 | Proton | 13 | 61 | 38.5 | 32.9 | 0.0 | 72 | 85 | 72.2 | 42.2 | 15 |
| Castro [32] | 1994 | Particle | 53 | 44 | 43.4 | 100.0 | 72 | 93 | 72 | |||
| Roy [33] | 2021 | GKRS | 15 | 16 | 88.9 | |||||||
| Napieralska [34] | 2021 | SRS/SRT | 23 | 53 | 52.2 | 17 | 21.7 | 52 | 89 | 69 | 43 | |
| Cahill [35] | 2021 | GKRS | 15 | 58 | 66.7 | 13 | 73.3 | 20 | 80 | 67 | 0 | |
| Hafez [36] | 2019 | GKRS | 12 | 46 | 41.7 | 2.7 | 0.0 | 16 | 0 | |||
| Sanusi [37] | 2018 | GKRS | 20 | 47 | 55.0 | 23.07 | 14.8 | 95 | 95 | 50 | 0 | |
| Fung [38] | 2018 | Combined | 106 | 56.6 | 25 | 4.8 | 73.8 | 88.3 | 4 | |||
| Wang [39] | 2017 | GKRS | 24 | 35 | 50.0 | 15.8 | 0.0 | 30.5 | 42 | |||
| Kim [40] | 2017 | IMRT | 14 | 39 | 21.4 | 78.6 | 67 | 92.9 | 92.9 | 0 | ||
| Choy [41] | 2016 | SRS/SRT | 42 | 53 | 57.1 | 27.18 | 92.9 | 17.8 | 37 | |||
| Ahmed [42] | 2015 | RT | 30 | 40 | 50.0 | 81 | 73 | 31 | ||||
| Cho [43] | 2008 | RT | 19 | 37 | 21.1 | 73.7 | 60.2 | 84.6 | 80 | 40 | ||
| Noel [44] | 2005 | Combined | 100 | 53 | 60.0 | 23 | 67 | 92 | 80.5 | 1 | ||
| Terahara [45] | 1999 | Combined | 115 | 45 | 57.4 | 46 | 68.9 | 88.9 |
| Factors | Coefficient | SE | Lower CL | Upper CL | Z Value | p Value |
|---|---|---|---|---|---|---|
| 3-year OS | ||||||
| Modality | 0.269 | 0.331 | −0.379 | 0.918 | 0.814 | 0.416 |
| Male ratio | −0.010 | 0.020 | −0.049 | 0.029 | −0.509 | 0.611 |
| Age | 0.025 | 0.041 | −0.056 | 0.106 | 0.609 | 0.543 |
| 5-year OS | ||||||
| Modality | 0.300 | 0.187 | −0.066 | 0.666 | 1.605 | 0.108 |
| Male ratio | 0.009 | 0.011 | −0.012 | 0.030 | 0.819 | 0.413 |
| Age | 0.004 | 0.017 | −0.030 | 0.039 | 0.251 | 0.802 |
| 3-year PFS | ||||||
| Modality | 0.441 | 2.713 | −4.876 | 5.758 | 0.163 | 0.871 |
| Male ratio | −0.007 | 0.076 | −0.156 | 0.143 | −0.086 | 0.932 |
| Age | 0.007 | 0.068 | −0.126 | 0.140 | 0.105 | 0.916 |
| 5-year PFS | ||||||
| Modality | 0.944 | 0.216 | 0.521 | 1.367 | 4.372 | <0.0001 |
| Male ratio | −0.011 | 0.010 | −0.031 | 0.009 | −1.066 | 0.287 |
| Age | 0.008 | 0.016 | −0.023 | 0.039 | 0.508 | 0.612 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, T.; Mizumoto, M.; Oshiro, Y.; Shimizu, S.; Li, Y.; Nakamura, M.; Hosaka, S.; Nakai, K.; Iizumi, T.; Inaba, M.; et al. Systematic Review and Meta-Analysis of Particle Beam Therapy versus Photon Radiotherapy for Skull Base Chordoma: TRP-Chordoma 2024. Cancers 2024, 16, 2569. https://doi.org/10.3390/cancers16142569
Saito T, Mizumoto M, Oshiro Y, Shimizu S, Li Y, Nakamura M, Hosaka S, Nakai K, Iizumi T, Inaba M, et al. Systematic Review and Meta-Analysis of Particle Beam Therapy versus Photon Radiotherapy for Skull Base Chordoma: TRP-Chordoma 2024. Cancers. 2024; 16(14):2569. https://doi.org/10.3390/cancers16142569
Chicago/Turabian StyleSaito, Takashi, Masashi Mizumoto, Yoshiko Oshiro, Shosei Shimizu, Yinuo Li, Masatoshi Nakamura, Sho Hosaka, Kei Nakai, Takashi Iizumi, Masako Inaba, and et al. 2024. "Systematic Review and Meta-Analysis of Particle Beam Therapy versus Photon Radiotherapy for Skull Base Chordoma: TRP-Chordoma 2024" Cancers 16, no. 14: 2569. https://doi.org/10.3390/cancers16142569
APA StyleSaito, T., Mizumoto, M., Oshiro, Y., Shimizu, S., Li, Y., Nakamura, M., Hosaka, S., Nakai, K., Iizumi, T., Inaba, M., Fukushima, H., Suzuki, R., Maruo, K., & Sakurai, H. (2024). Systematic Review and Meta-Analysis of Particle Beam Therapy versus Photon Radiotherapy for Skull Base Chordoma: TRP-Chordoma 2024. Cancers, 16(14), 2569. https://doi.org/10.3390/cancers16142569