
Comparative Efficacy of Neoadjuvant Nivolumab Plus Chemotherapy versus Conventional Comparator Treatments in Resectable Non-Small-Cell Lung Cancer: A Systematic Literature Review and Network Meta-Analysis

 , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. SLR and NMA Eligibility
2.2. Target Populations
2.3. Data Preparation
2.4. Quantitative Evidence Synthesis
2.5. Sensitivity Analysis
3. Results
3.1. Evidence Base
3.2. Proportional Hazard Assessment and Model Selection
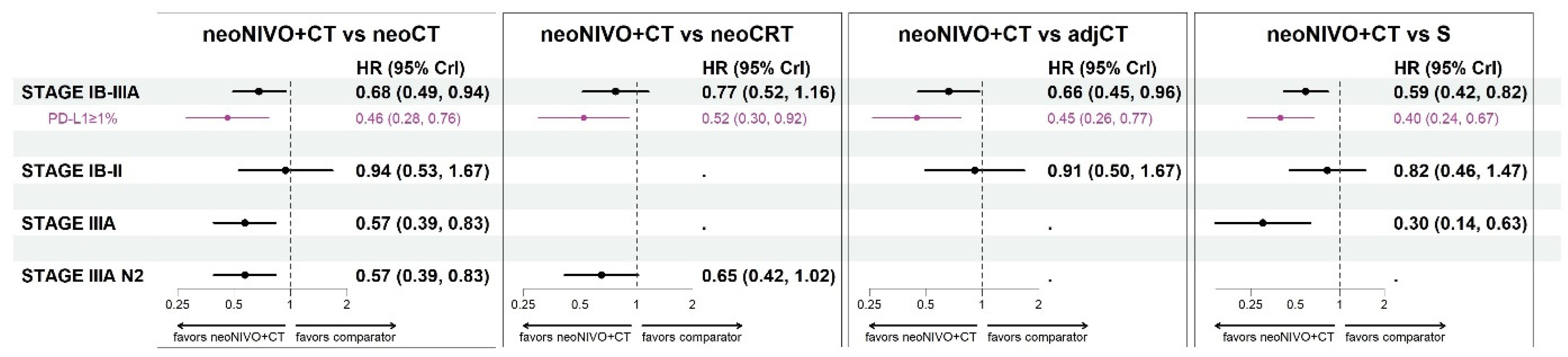
3.3. Relative Efficacy for Event-Free Survival
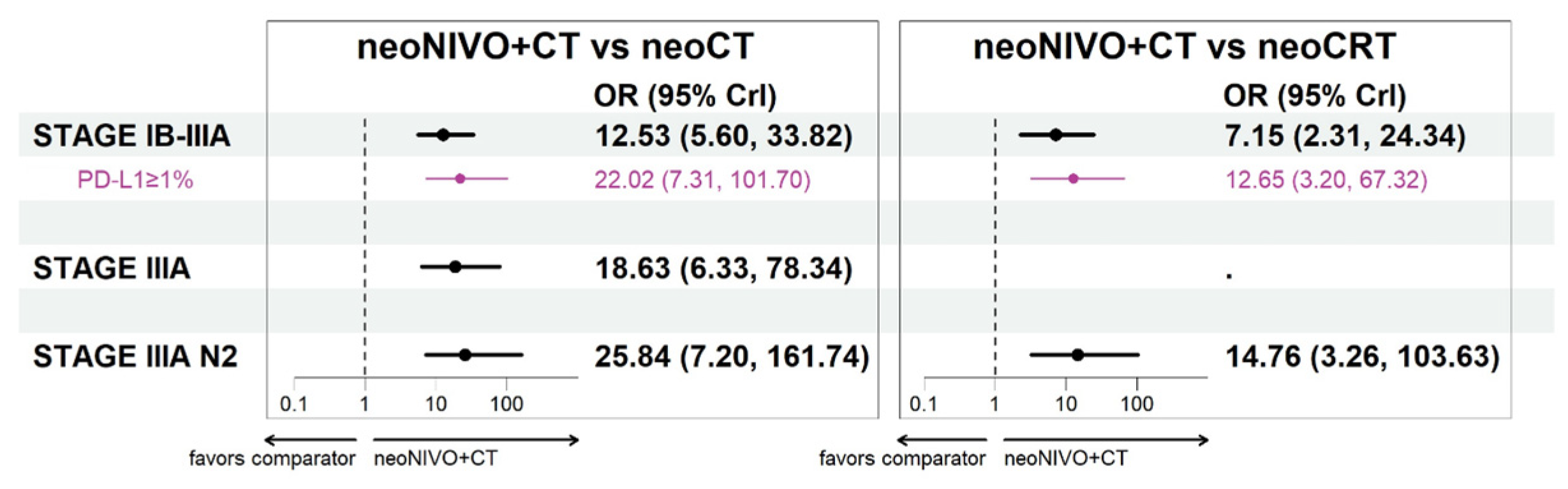
3.4. Relative Efficacy for Pathological Complete Response
3.5. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- NCC Network. NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer; Version 3; NCC: Atlanta, GA, USA, 2023. [Google Scholar]
- Postmus, P.; Kerr, K.; Oudkerk, M.; Senan, S.; Waller, D.; Vansteenkiste, J.; Escriu, C.; Peters, S. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- PDQ Adult Treatment Editorial Board. PDQ Non-Small Cell Lung Cancer Treatment. 2021. Available online: https://www.cancer.gov/types/lung/patient/non-small-cell-lung-treatment-pdq (accessed on 2 December 2021).
- Taylor, M.D.; Nagji, A.S.; Bhamidipati, C.M.; Theodosakis, N.; Kozower, B.D.; Lau, C.L.; Jones, D.R. Tumor recurrence after complete resection for non-small cell lung cancer. Ann. Thorac. Surg. 2012, 93, 1813–1820; discussion 1820–1821. [Google Scholar] [CrossRef] [PubMed]
- Uramoto, H.; Tanaka, F. Recurrence after surgery in patients with NSCLC. Transl. Lung Cancer Res. 2014, 3, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Arriagada, R.; Auperin, A.; Burdett, S.; Higgins, J.P.; Johnson, D.H.; Le Chevalier, T.; Le Pechoux, C.; Parmar, M.K.; Pignon, J.P.; Souhami, R.L.; et al. Adjuvant chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer: Two meta-analyses of individual patient data. Lancet 2010, 375, 1267–1277. [Google Scholar] [CrossRef] [PubMed]
- Butts, C.A.; Ding, K.; Seymour, L.; Twumasi-Ankrah, P.; Graham, B.; Gandara, D.; Johnson, D.H.; Kesler, K.A.; Green, M.; Vincent, M.; et al. Randomized phase III trial of vinorelbine plus cisplatin compared with observation in completely resected stage IB and II non-small-cell lung cancer: Updated survival analysis of JBR-10. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Uprety, D.; Mandrekar, S.J.; Wigle, D.; Roden, A.C.; Adjei, A.A. Neoadjuvant immunotherapy for NSCLC: Current concepts and future approaches. J. Thorac. Oncol. 2020, 15, 1281–1297. [Google Scholar] [CrossRef] [PubMed]
- NSCLC Meta-Analysis Collaborative Group. Preoperative chemotherapy for non-small-cell lung cancer: A systematic review and meta-analysis of individual participant data. Lancet 2014, 383, 1561–1571. [Google Scholar] [CrossRef] [PubMed]
- Albain, K.S.; Swann, R.S.; Rusch, V.W.; Turrisi, A.T., 3rd; Shepherd, F.A.; Smith, C.; Chen, Y.; Livingston, R.B.; Feins, R.H.; Gandara, D.R.; et al. Radiotherapy plus chemotherapy with or without surgical resection for stage III non-small-cell lung cancer: A phase III randomised controlled trial. Lancet 2009, 374, 379–386. [Google Scholar] [CrossRef]
- Spicer, J.D.; Shewale, J.B.; Nelson, D.B.; Mitchell, K.G.; Bott, M.J.; Vallières, E.; Wilshire, C.L.; Vaporciyan, A.A.; Swisher, S.G.; Jones, D.R.; et al. Multimodality Therapy for N2 Non-Small Cell Lung Cancer: An Evolving Paradigm. Ann. Thorac. Surg. 2019, 107, 277–284. [Google Scholar] [CrossRef]
- Zinner, R.; Axelrod, R.; Solomides, C.C.; Cowan, S.; Leiby, B.; Bhatia, A.K.; Sundermeyer, M.L.; Hooper, D.C.; Harshyne, L.; Lu-Yao, G.L. Neoadjuvant nivolumab (N) plus cisplatin (C)/pemetrexed (P) or cisplatin/gemcitabine (G) in resectable NSCLC. J. Clin. Oncol. 2020, 38, 9051. [Google Scholar] [CrossRef]
- Yang, C.-F.J.; McSherry, F.; Mayne, N.R.; Wang, X.; Berry, M.F.; Tong, B.; Harpole, D.H., Jr.; D’Amico, T.A.; Christensen, J.D.; Ready, N.E. Surgical outcomes after neoadjuvant chemotherapy and ipilimumab for non-small cell lung cancer. Ann. Thorac. Surg. 2018, 105, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, J.; Cai, L.; Chen, S.; Jiang, Y. The safety and efficacy of neoadjuvant programmed death 1 inhibitor therapy with surgical resection in stage IIIA non-small cell lung cancer. Ann. Transl. Med. 2021, 9, 486. [Google Scholar] [CrossRef] [PubMed]
- Tfayli, A.; Al Assaad, M.; Fakhri, G.; Akel, R.; Atwi, H.; Ghanem, H.; El Karak, F.; Farhat, F.; Al Rabi, K.; Sfeir, P. Neoadjuvant chemotherapy and Avelumab in early stage resectable nonsmall cell lung cancer. Cancer Med. 2020, 9, 8406–8411. [Google Scholar] [CrossRef] [PubMed]
- Shu, C.A.; Gainor, J.F.; Awad, M.M.; Chiuzan, C.; Grigg, C.M.; Pabani, A.; Garofano, R.F.; Stoopler, M.B.; Cheng, S.K.; White, A. Neoadjuvant atezolizumab and chemotherapy in patients with resectable non-small-cell lung cancer: An open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Shen, D.; Wang, J.; Wu, J.; Chen, S.; Li, J.; Liu, J.; Chen, Q.; Jiang, Y. Neoadjuvant pembrolizumab with chemotherapy for the treatment of stage IIB–IIIB resectable lung squamous cell carcinoma. J. Thorac. Dis. 2021, 13, 1760–1768. [Google Scholar] [CrossRef] [PubMed]
- Provencio, M.; Nadal, E.; Insa, A.; García-Campelo, M.R.; Casal-Rubio, J.; Domine, M.; Majem, M.; Rodriguez-Abreu, D.; Martinez-Marti, A.; Carpeño, J.D.C. Neoadjuvant chemotherapy and nivolumab in resectable non-small-cell lung cancer (NADIM): An open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 1413–1422. [Google Scholar] [CrossRef] [PubMed]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.R.; Brahmer, J.R.; Swanson, S.J.; et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef] [PubMed]
- Duan, H.; Wang, T.; Luo, Z.; Tong, L.; Dong, X.; Zhang, Y.; Afzal, M.Z.; Correale, P.; Liu, H.; Jiang, T. Neoadjuvant programmed cell death protein 1 inhibitors combined with chemotherapy in resectable non-small cell lung cancer: An open-label, multicenter, single-arm study. Transl. Lung Cancer Res. 2021, 10, 1020–1028. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Ades, A.; Caldwell, D.M.; Reken, S.; Welton, N.J.; Sutton, A.J.; Dias, S. Evidence synthesis for decision making 7: A reviewer’s checklist. Med. Decis. Mak. 2013, 33, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Goring, S.; Rogula, B.; Lucherini, S.; Vo, L.; Lozano-Ortega, G.; Besada, M.; Chaudhary, M.; Varol, N.; Lam, P.; Girard, N. P15 Indirect Treatment Comparisons of Time-to-Event Outcomes with Mis-Matched “Time Zero”: Methodology and Application in Resectable Non-Small Cell Lung Cancer. Value Health 2023, 26, S4. [Google Scholar] [CrossRef]
- Bormann, I. DigitizeIt. 2020 [2.5.3]. Available online: https://www.digitizeit.de (accessed on 5 March 2022).
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventionsb; Wiley: Hoboken, NJ, USA, 2019; pp. 205–228. [Google Scholar]
- European Medicines Agency. OPVIDO® (Nivolumab). 2023. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/opdivo (accessed on 1 December 2023).
- Xu, Y.; Wan, B.; Chen, X.; Zhan, P.; Zhao, Y.; Zhang, T.; Liu, H.; Afzal, M.Z.; Dermime, S.; Hochwald, S.N.; et al. The association of PD-L1 expression with the efficacy of anti- PD-1/PD-L1 immunotherapy and survival of non-small cell lung cancer patients: A meta-analysis of randomized controlled trials. Transl. Lung Cancer Res. 2019, 8, 413–428. [Google Scholar] [CrossRef] [PubMed]
- Rogula, B.; Lozano-Ortega, G.; Johnston, K.M. A method for reconstructing individual patient data from kaplan-meier survival curves that incorporate marked censoring times. MDM Policy Pract. 2022, 7, 23814683221077643. [Google Scholar] [CrossRef]
- Guyot, P.; Ades, A.; Ouwens, M.J.; Welton, N.J. Enhanced secondary analysis of survival data: Reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef]
- Waser, N.; Vo, L.; McKenna, M.; Penrod, J.; Goring, S. Real-world treatment patterns in resectable (stages I–III) non-small-cell lung cancer: A systematic literature review. Future Oncol. 2022, 18, 1519–1530. [Google Scholar] [CrossRef]
- Forde, P.M.; Spicer, J.; Girard, N.; Provencio, M.; Lu, S.; Wang, C.; Awad, M.M.; Mitsudomi, T.; Felip, E.; Swanson, S.J.; et al. Neoadjuvant nivolumab plus platinum-doublet chemotherapy for resectable NSCLC: 3-year update from CheckMate 816. In Proceedings of the European Lung Cancer Congress 2023, Copenhagen, Denmark, 29 March–1 April 2023. [Google Scholar]
- Provencio, M.; Nadal, E.; Gonzáles-Larriba, J.L.; Martinez-Marti, A.; Bernabé, R.; Bosch-Barrera, J.; Casal-Rubio, J.; Calvo, V.; Insa, A.; Ponce, S.; et al. Nivolumab + chemotherapy (CT) vs. CT as neoadjuvant treatment for resectable stage IIIA-B non-small cell lung cancer (NSCLC): NADIM II trial. In Proceedings of the ASCO, Chicago, IL, USA, 3–7 June 2022. [Google Scholar]
- Felip, E.; Rosell, R.; Maestre, J.A.; Rodríguez-Paniagua, J.M.; Morán, T.; Astudillo, J.; Alonso, G.; Borro, J.M.; González-Larriba, J.L.; Torres, A.; et al. Preoperative chemotherapy plus surgery versus surgery plus adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3138–3145. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Pastorino, U.; Vansteenkiste, J.F.; Spaggiari, L.; Facciolo, F.; Orlowski, T.M.; Maiorino, L.; Hetzel, M.; Leschinger, M.; Visseren-Grul, C. Randomized phase III study of surgery alone or surgery plus preoperative cisplatin and gemcitabine in stages IB to IIIA non-small-cell lung cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Pisters, K.M.; Vallieres, E.; Crowley, J.J.; Franklin, W.A.; Bunn, P.A., Jr.; Ginsberg, R.J.; Putnam, J.B., Jr.; Chansky, K.; Gandara, D. Surgery with or without preoperative paclitaxel and carboplatin in early-stage non–small-cell lung cancer: Southwest Oncology Group Trial S9900, an intergroup, randomized, phase III trial. J. Clin. Oncol. 2010, 28, 1843–1849. [Google Scholar] [CrossRef]
- Li, J.; YU, L.C.; Chen, P.; SHI, S.B.; DAI, C.H.; WU, J.R. Randomized controlled trial of neoadjuvant chemotherapy with cisplatin and vinorelbine in patients with stage IIIA non-small cell lung cancer in China. Asia-Pac. J. Clin. Oncol. 2009, 5, 87–94. [Google Scholar] [CrossRef]
- Girard, N.; Mornex, F.; Douillard, J.Y.; Bossard, N.; Quoix, E.; Beckendorf, V.; Grunenwald, D.; Amour, E.; Milleron, B. Is neoadjuvant chemoradiotherapy a feasible strategy for stage IIIA-N2 non-small cell lung cancer? Mature results of the randomized IFCT-0101 phase II trial. Lung Cancer 2010, 69, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Katakami, N.; Tada, H.; Mitsudomi, T.; Kudoh, S.; Senba, H.; Matsui, K.; Saka, H.; Kurata, T.; Nishimura, Y.; Fukuoka, M. A phase 3 study of induction treatment with concurrent chemoradiotherapy versus chemotherapy before surgery in patients with pathologically confirmed N2 stage IIIA nonsmall cell lung cancer (WJTOG9903). Cancer 2012, 118, 6126–6135. [Google Scholar] [CrossRef] [PubMed]
- Pless, M.; Stupp, R.; Ris, H.B.; Stahel, R.A.; Weder, W.; Thierstein, S.; Gerard, M.A.; Xyrafas, A.; Früh, M.; Cathomas, R.; et al. Induction chemoradiation in stage IIIA/N2 non-small-cell lung cancer: A phase 3 randomised trial. Lancet 2015, 386, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Luo, Q.; Jian, H.; Zhou, Z.; Cheng, B.; Lu, S.; Liao, M. Long-term results of a randomized controlled trial evaluating preoperative chemotherapy in resectable non-small cell lung cancer. OncoTargets Ther. 2013, 6, 645–650. [Google Scholar]
- Depierre, A.; Milleron, B.; Moro-Sibilot, D.; Chevret, S.; Quoix, E.; Lebeau, B.; Braun, D.; Breton, J.-L.; Lemarié, E.; Gouva, S. Preoperative chemotherapy followed by surgery compared with primary surgery in resectable stage I (except T1N0), II, and IIIa non-small-cell lung cancer. J. Clin. Oncol. 2002, 20, 247–253. [Google Scholar] [PubMed]
- Gilligan, D.; Nicolson, M.; Smith, I.; Groen, H.; Dalesio, O.; Goldstraw, P.; Hatton, M.; Hopwood, P.; Manegold, C.; Schramel, F. Preoperative chemotherapy in patients with resectable non-small cell lung cancer: Results of the MRC LU22/NVALT 2/EORTC 08012 multicentre randomised trial and update of systematic review. Lancet 2007, 369, 1929–1937. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Tsuchiya, R.; Mori, T.; Tada, H.; Ichinose, Y.; Koike, T.; Kato, H.; Lung Cancer Surgical Study Group of the Japan Clinical Oncology Group. A randomized trial comparing induction chemotherapy followed by surgery with surgery alone for patients with stage IIIA N2 non-small cell lung cancer (JCOG 9209). J. Thorac. Cardiovasc. Surg. 2003, 125, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Gómez-Codina, J.; Camps, C.; Javier Sánchez, J.; Maestre, J.; Padilla, J.; Cantó, A.; Abad, A.; Roig, J. Preresectional chemotherapy in stage IIIA non-small-cell lung cancer: A 7-year assessment of a randomized controlled trial. Lung Cancer 1999, 26, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Gómez-Codina, J.; Camps, C.; Maestre, J.; Padille, J.; Cantó, A.; Mate, J.L.; Li, S.; Roig, J.; Olazábal, A.; et al. A randomized trial comparing preoperative chemotherapy plus surgery with surgery alone in patients with non-small-cell lung cancer. N. Engl. J. Med. 1994, 330, 153–158. [Google Scholar] [CrossRef]
- Winton, T.; Livingston, R.; Johnson, D.; Rigas, J.; Johnston, M.; Butts, C.; Cormier, Y.; Goss, G.; Inculet, R.; Vallieres, E.; et al. Vinorelbine plus cisplatin vs. observation in resected non-small-cell lung cancer. N. Engl. J. Med. 2005, 352, 2589–2597. [Google Scholar] [CrossRef]
- Douillard, J.-Y.; Rosell, R.; De Lena, M.; Carpagnano, F.; Ramlau, R.; Gonzáles-Larriba, J.L.; Grodzki, T.; Pereira, J.R.; Le Groumellec, A.; Lorusso, V. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB–IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association [ANITA]): A randomised controlled trial. Lancet Oncol. 2006, 7, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Ou, W.; Sun, H.-b.; Ye, X.; Zhang, B.-b.; Yang, H.; Fang, Q.; Li, P.; Wang, S.-y. Adjuvant carboplatin-based chemotherapy in resected stage IIIA-N2 non-small cell lung cancer. J. Thorac. Oncol. 2010, 5, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Strauss, G.M.; Herndon, J.E.; II, M.A.M.; Johnstone, D.W.; Johnson, E.A.; Harpole, D.H.; Gillenwater, H.H.; Watson, D.M.; Sugarbaker, D.J.; Schilsky, R.L. Adjuvant paclitaxel plus carboplatin compared with observation in stage IB non-small-cell lung cancer: CALGB 9633 with the Cancer and Leukemia Group B, Radiation Therapy Oncology Group, and North Central Cancer Treatment Group Study Groups. J. Clin. Oncol. 2008, 26, 5043–5051. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.; Harris, G.; Patel, A.; Adachi, I.; Edmonds, L.; Song, F. Preoperative versus postoperative chemotherapy in patients with resectable non-small cell lung cancer: Systematic review and indirect comparison meta-analysis of randomized trials. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2009, 4, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Booth, C.M.; Shepherd, F.A.; Peng, Y.; Darling, G.; Li, G.; Kong, W.; Biagi, J.J.; Mackillop, W.J. Time to adjuvant chemotherapy and survival in non-small cell lung cancer: A population-based study. Cancer 2013, 119, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Kehl, K.L.; Zahrieh, D.; Yang, P.; Hillman, S.L.; Tan, A.D.; Sands, J.M.; Oxnard, G.R.; Gillaspie, E.A.; Wigle, D.; Malik, S.; et al. Rates of Guideline-Concordant Surgery and Adjuvant Chemotherapy Among Patients with Early-Stage Lung Cancer in the US ALCHEMIST Study (Alliance A151216). JAMA Oncol. 2022, 8, 717–728. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Tsuboi, M.; Brunelli, A. Surgical perspective on neoadjuvant immunotherapy in non-small cell lung cancer. Ann. Thorac. Surg. 2022, 114, 1505–1515. [Google Scholar] [CrossRef]
- Topalian, S.L.; Taube, J.M.; Pardoll, D.M. Neoadjuvant checkpoint blockade for cancer immunotherapy. Science 2020, 367, eaax0182. [Google Scholar] [CrossRef] [PubMed]
- Sittenfeld, S.; Pham, Y.; Reddy, C.; Obi, E.; Kruse, M.; Al-Hilli, Z.; Cherian, S.; Shah, C.; Tendulkar, R. Ten Year Outcomes of Locoregional and Distant Recurrence for T1-2N1 Breast Cancer with or without Post-Mastectomy Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, E7. [Google Scholar] [CrossRef]
- Pang, L.-L.; Gan, J.-D.; Huang, Y.-H.; Liao, J.; Lv, Y.; Ali, W.A.-S.; Zhang, L.; Fang, W.-F. Investigation of the optimal platinum-based regimen in the postoperative adjuvant chemotherapy setting for early-stage resected non-small lung cancer: A Bayesian network meta-analysis. BMJ Open 2022, 12, e057098. [Google Scholar] [CrossRef]
- Pignon, J.P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE Collaborative Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 3552–3559. [Google Scholar] [CrossRef] [PubMed]
- Phillippo, D.M.; Dias, S.; Ades, A.E.; Belger, M.; Brnabic, A.; Schacht, A.; Saure, D.; Kadziola, Z.; Welton, N.J. Multilevel network meta-regression for population-adjusted treatment comparisons. J. R. Stat. Soc. Ser. A 2020, 183, 1189–1210. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, M.D.; Chaft, J.E.; William, W.N., Jr.; Rusch, V.; Pisters, K.M.; Kalhor, N.; Pataer, A.; Travis, W.D.; Swisher, S.G.; Kris, M.G. Pathological response after neoadjuvant chemotherapy in resectable non-small-cell lung cancers: Proposal for the use of major pathological response as a surrogate endpoint. Lancet. Oncol. 2014, 15, e42–e50. [Google Scholar] [CrossRef] [PubMed]
- Nadler, E.; Vasudevan, A.; Wentworth, C.; Robert, N.; Penrod, J.R.; Fiore, J.; Vo, L. Real-world relationship of early end points to survival end points in patients with resectable non-small-cell lung cancer. Future Oncol. 2023, 19, 1785–1800. [Google Scholar] [CrossRef] [PubMed]
- Pataer, A.; Kalhor, N.; Correa, A.M.; Raso, M.G.; Erasmus, J.J.; Kim, E.S.; Behrens, C.; Lee, J.J.; Roth, J.A.; Stewart, D.J.; et al. Histopathologic response criteria predict survival of patients with resected lung cancer after neoadjuvant chemotherapy. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2012, 7, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Rosner, S.; Liu, C.; Forde, P.M.; Hu, C. Association of Pathologic Complete Response and Long-Term Survival Outcomes Among Patients Treated with Neoadjuvant Chemotherapy or Chemoradiotherapy for NSCLC: A Meta-Analysis. JTO Clin. Res. Rep. 2022, 3, 100384. [Google Scholar] [CrossRef] [PubMed]
- Waser, N.; Quintana, M.; Schweikert, B.; Chaft, J.; Berry, L.; Adam, A.; Vo, L.; Penrod, J.; Fiore, J.; Berry, D.; et al. Pathologic response in resectable non-small cell lung cancer: A systematic literature review and meta-analysis. J. Natl. Cancer Inst. Cancer Spectr. 2024, 8, pkae021. [Google Scholar]
- William, W.N., Jr.; Pataer, A.; Kalhor, N.; Correa, A.M.; Rice, D.C.; Wistuba, I.I.; Heymach, J.; Lee, J.J.; Kim, E.S.; Munden, R.; et al. Computed tomography RECIST assessment of histopathologic response and prediction of survival in patients with resectable non-small-cell lung cancer after neoadjuvant chemotherapy. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2013, 8, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Mainguene, J.; Basse, C.; Girard, P.; Beaucaire-Danel, S.; Cao, K.; Brian, E.; Grigoroiu, M.; Gossot, D.; Luporsi, M.; Perrot, L.; et al. Surgical or medical strategy for locally-advanced, stage IIIA/B-N2 non-small cell lung cancer: Reproducibility of decision-making at a multidisciplinary tumor board. Lung Cancer 2022, 163, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Felip, E.; Altorki, N.; Zhou, C.; Csőszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB–IIIA non-small-cell lung cancer (IMpower010): A randomised, multicentre, open-label, phase 3 trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef]
- Heymach, J.; Harpole, D.; Mitsudomi, T. AEGEAN: A phase 3 trial of neoadjuvant durvalumab+ chemotherapy followed by adjuvant durvalumab in patients with resectable NSCLC. Zentralbl. Chir. 2023, 148, S87. [Google Scholar] [CrossRef]
- O’Brien, M.; Paz-Ares, L.; Marreaud, S.; Dafni, U.; Oselin, K.; Havel, L.; Esteban, E.; Isla, D.; Martinez-Marti, A.; Faehling, M. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB–IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): An interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022, 23, 1274–1286. [Google Scholar] [CrossRef] [PubMed]
- Wakelee, H.A.; Liberman, M.; Kato, T.; Tsuboi, M.; Lee, S.-H.; He, J.; Gao, S.; Chen, K.-N.; Dooms, C.A.; Majem, M. KEYNOTE-671: Randomized, double-blind, phase 3 study of pembrolizumab or placebo plus platinum-based chemotherapy followed by resection and pembrolizumab or placebo for early stage NSCLC. J. Clin. Oncol. 2023, 41, LBA100. [Google Scholar] [CrossRef]
- Provencio, M.; Nadal, E.; González-Larriba, J.L.; Martínez-Martí, A.; Bernabé, R.; Bosch-Barrera, J.; Casal-Rubio, J.; Calvo, V.; Insa, A.; Ponce, S.; et al. Perioperative Nivolumab and Chemotherapy in Stage III Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 504–513. [Google Scholar] [CrossRef]
- Clinicaltrials.gov. A Study of Neoadjuvant Chemotherapy Plus Nivolumab Versus Neoadjuvant Chemotherapy Plus Placebo, Followed by Surgical Removal and Adjuvant Treatment with Nivolumab or Placebo for Participants with Surgically Removable Early Stage Non-small Cell Lung Cancer. 2023. Available online: https://www.clinicaltrials.gov/study/NCT04025879 (accessed on 1 February 2024).
- Woods, B.S.; Hawkins, N.; Scott, D.A. Network meta-analysis on the log-hazard scale, combining count and hazard ratio statistics accounting for multi-arm trials: A tutorial. BMC Med. Res. Methodol. 2010, 10, 54. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author Year) * | N | Arms (n) | Phase | Blinding | Median FU (yrs) | Region | Post-Surgical Treatment Permitted | |
|---|---|---|---|---|---|---|---|---|
| adjCT | adjRT | |||||||
| Base case studies | ||||||||
| CM816 (Forde 2022) [20,32] | 358 | neoCT (179), neoNIVO + CT (179) | 3 | Open-label | 3.5 | International | Yes (investigator discretion) | Yes (investigator discretion) |
| NADIM II (Provencio 2022) [33] | 86 | neoCT (29), periNIVO + neoCT ◆ (57) | 2 | Open-label | - | Spain | No | No |
| NATCH (Felip 2010) [34] | 619 | S (210), neoCT (199), adjCT (210) | 3 | Open-label | 4.2 | Europe | No | Yes (if pN2) |
| CHEST (Scagliotti 2012) [35] | 270 | neoCT (129), S (141) | 3 | - | 2.6–3.3 ‡ | Europe | No ** | No ** |
| SWOG S9900 (Pisters 2010) [36] | 337 | neoCT (169), S (168) | 3 | Open-label | 5.3 | US and Canada | No ** | No ** |
| Li 2009 [37] | 56 † | neoCT (28), S (28) | 3 | Open-label | 3.2 | China | Yes, all patients | Yes, R1 or R2 |
| IFCT 0101 (Girard 2010) [38] | 46 † | neoCT (14), neoCRT ◆◆ (17), neoCRT ◆◆ (15) | 2 | Open-label | 2.6 | France | Yes, R2 *** | Yes, R1 or R2 *** |
| WJTOG 9903 (Katakami 2012) [39] | 60 † | neoCT (29), neoCRT ◆◆ (31) | 3 | - | 5.1 | Japan | No | Unclear |
| SAKK 16/00 (Pless 2015) [40] | 232 | neoCT (115), neoCRT ◆◆ (117) | 3 | Open-label | 4.4 | Europe | Unclear | Yes, R1 or R2 |
| Studies added to the sensitivity analyses (3rd and 2nd generation chemotherapies) | ||||||||
| Chen 2013 [41] | 337 | neoCT (169), S (168) | - | Open-label | 4.5 | China | Yes, all patients | Yes, if pN2 |
| IFCT 0001 (Depierre 2002) [42] | 355 | neoCT (179), S (176) | 3 | - | 6.7 | France | Yes, responders in S arm | Yes, R1 or R2 of pT3 or pN2 |
| MRC LU22 (Gilligan 2007) [43] | 519 | neoCT (258), S (261) | 3 | - | - | Europe | Possible, if deemed inoperable at time of surgery or on progression | |
| JCOG 9209 (Nagai 2003) [44] | 62 † | neoCT (31), S (31) | 3 | Open-label | 6.2 | Japan | No | Yes, R1 or R2 |
| Rosell 1994 [45,46] | 60 | neoCT (30), S (30) | - | Open-label | 5.0 | Spain | Unclear | Yes, all patients |
| Studies added to the sensitivity analyses (completely resected patients) | ||||||||
| JBR10 (Winton 2005) [8,47] | 482 | S (240), adjCT (242) | 3 | Open-label | 9.3 | Canada, US | Unclear in S arm | Unclear |
| ANITA (Douillard 2006) [48] | 840 | S (433), adjCT (407) | 3 | Open-label | 6.3 | International | Unclear in S arm | Yes (investigator discretion) |
| Ou 2010 [49] | 150 | adjCT (79), S (71) | - | - | 2.4 | China | Unclear in S arm | No |
| CALGB 9633 (Strauss 2008) [50] | 344 | adjCT (173), S (171) | - | Open-label | 6.2 | US | Unclear in S arm | Unclear |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girard, N.; Besada, M.; Rogula, B.; Lucherini, S.; Vo, L.; Chaudhary, M.A.; Goring, S.; Lozano-Ortega, G.; Tran, M.; Varol, N.; et al. Comparative Efficacy of Neoadjuvant Nivolumab Plus Chemotherapy versus Conventional Comparator Treatments in Resectable Non-Small-Cell Lung Cancer: A Systematic Literature Review and Network Meta-Analysis. Cancers 2024, 16, 2492. https://doi.org/10.3390/cancers16132492
Girard N, Besada M, Rogula B, Lucherini S, Vo L, Chaudhary MA, Goring S, Lozano-Ortega G, Tran M, Varol N, et al. Comparative Efficacy of Neoadjuvant Nivolumab Plus Chemotherapy versus Conventional Comparator Treatments in Resectable Non-Small-Cell Lung Cancer: A Systematic Literature Review and Network Meta-Analysis. Cancers. 2024; 16(13):2492. https://doi.org/10.3390/cancers16132492
Chicago/Turabian StyleGirard, Nicolas, Mariam Besada, Basia Rogula, Stefano Lucherini, Lien Vo, Mohammad A. Chaudhary, Sarah Goring, Greta Lozano-Ortega, Mia Tran, Nebibe Varol, and et al. 2024. "Comparative Efficacy of Neoadjuvant Nivolumab Plus Chemotherapy versus Conventional Comparator Treatments in Resectable Non-Small-Cell Lung Cancer: A Systematic Literature Review and Network Meta-Analysis" Cancers 16, no. 13: 2492. https://doi.org/10.3390/cancers16132492
APA StyleGirard, N., Besada, M., Rogula, B., Lucherini, S., Vo, L., Chaudhary, M. A., Goring, S., Lozano-Ortega, G., Tran, M., Varol, N., Waser, N., Yu, W. W., Lee, J. M., & Spicer, J. (2024). Comparative Efficacy of Neoadjuvant Nivolumab Plus Chemotherapy versus Conventional Comparator Treatments in Resectable Non-Small-Cell Lung Cancer: A Systematic Literature Review and Network Meta-Analysis. Cancers, 16(13), 2492. https://doi.org/10.3390/cancers16132492