
Evolving Precision First-Line Systemic Treatment for Patients with Unresectable Non-Small Cell Lung Cancer


Abstract
Simple Summary
Abstract
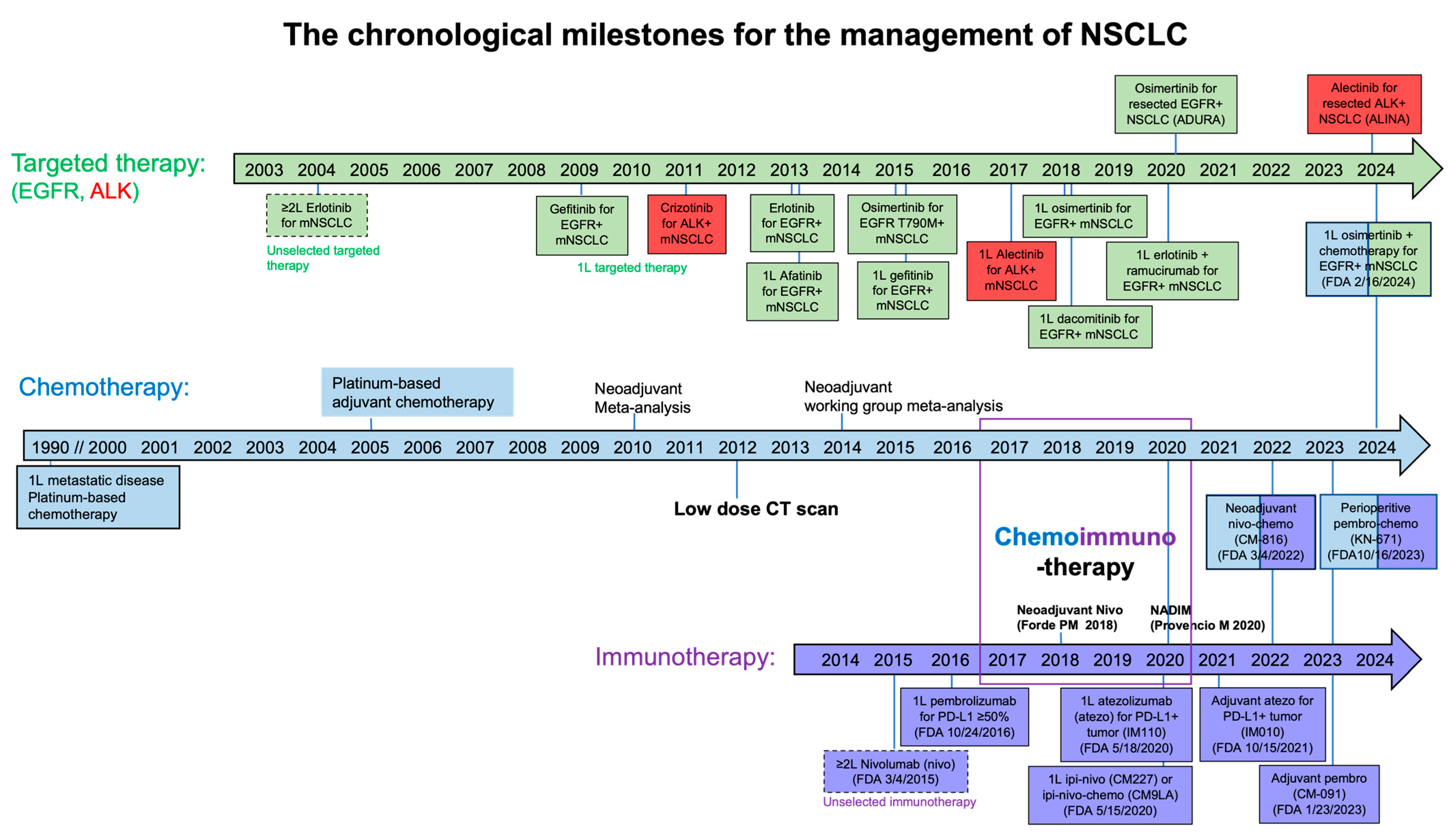
1. Introduction
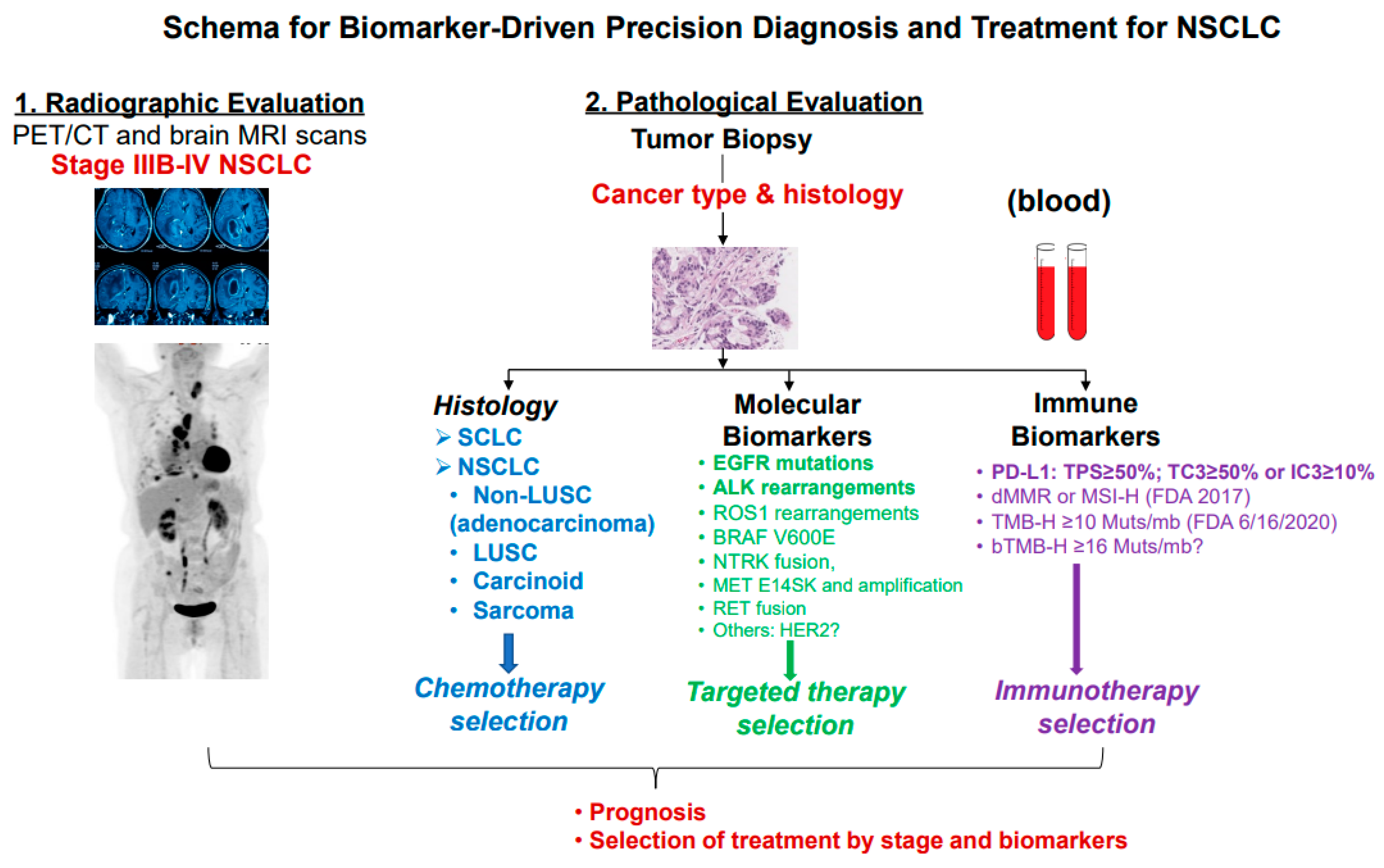
2. Histopathological Diagnosis
3. Molecular Biomarker Testing
4. Immune Biomarkers
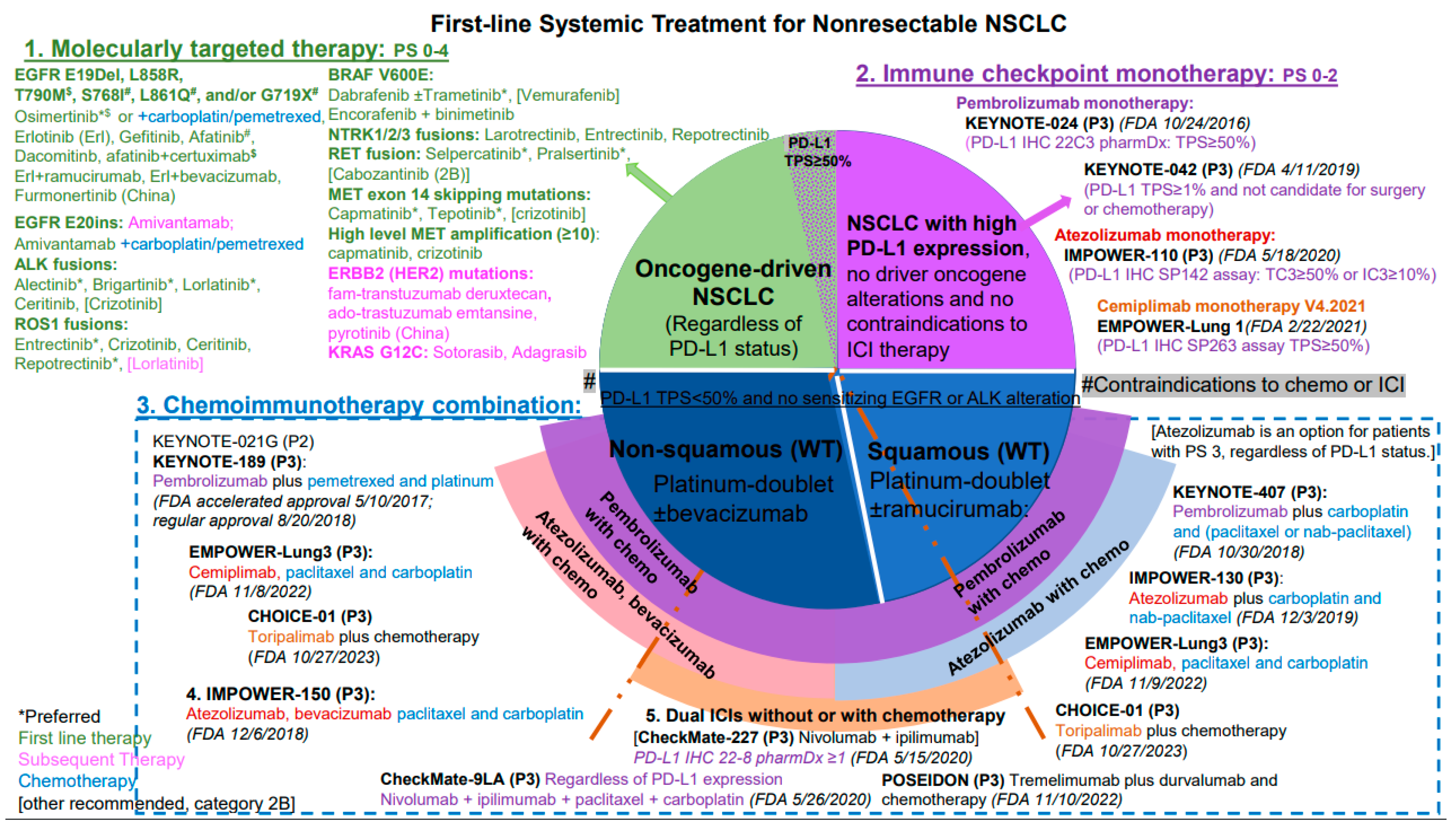
5. Selection of First-Line Systemic Therapy for Patients with Advanced NSCLC
5.1. First-Line Systemic Therapy for Oncogene-Driven NSCLC
5.2. Selection of First-Line Systemic Therapy with PD-1/PD-L1 Inhibitor Monotherapy
5.3. Selection of First-Line Therapy with PD-1/PD-L1 Inhibitor in Combination with Chemotherapy
5.4. First-Line Systemic Therapy with ICIs and Bevacizumab
5.5. First-Line CTLA-4 and PD-1 Antibody Combination
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
List of Abbreviations
| ABCP | atezolizumab + BCP |
| ALK | anaplastic lymphoma kinase |
| BCP | bevacizumab, carboplatin, and paclitaxel |
| BRAF | B-Raf proto-oncogene |
| CI | confidence interval |
| CNV | copy number variations |
| CT | standard-of-care histology-based, platinum-containing chemotherapy doublet |
| CTLA-4 | cytotoxic T-lymphocyte-associated protein 4 |
| ctDNA | circulating tumor DNA |
| D | durvalumab |
| dMMR | defective mismatch repair |
| DoR | duration of response |
| EGFR | epidermal growth factor receptor |
| ERBB2 | v-erb-b2 avian erythroblastic leukemia viral oncogene homolog 2 |
| FDA | Food and Drug Administration |
| FISH | fluorescence in situ hybridization |
| HER | human epidermal growth factor receptor |
| HR | hazard ratio |
| IHC | immunohistochemistry |
| irAEs | immune-related adverse effects |
| KRAS | KRAS proto-oncogene |
| LA | locally advanced |
| LUAD | lung adenocarcinoma |
| LUSC | lung squamous carcinoma |
| M | metastatic |
| MET | MET proto-oncogene |
| MSI | microsatellite instability |
| Mo | month |
| NA | not available |
| NCCN | National Comprehensive Cancer Network |
| NGS | next-generation sequencing |
| HR | hazard ratio |
| NGS | next-generation sequence |
| NSCLC | non-small cell lung cancer |
| NTRK | neurotrophic tyrosine receptor kinase |
| ORR | overall response rate |
| OS | overall survival |
| PCR | polymerase chain reaction |
| PD-1 | programmed death protein 1 |
| PD-L1 | programmed death-ligand 1 |
| PFS | progression-free survival |
| RET | rearranged during transfection |
| ROS1 | ROS proto-oncogene 1 |
| RT-PCR | real-time polymerase chain reaction |
| SNV | single nucleotide variants |
| SoC | standard-of-care |
| T | tremelimumab |
| TKI | tyrosine kinase inhibitor |
| TMB | tumor mutation burden |
| TPS | total proportion score |
| TTF-1 | transcription factor-1 |
| UT | undifferentiated tumor |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Chemotherapy in non-small cell lung cancer: A meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung Cancer Collaborative Group. BMJ 1995, 311, 899–909.
- Howlader, N.; Forjaz, G.; Mooradian, M.J.; Meza, R.; Kong, C.Y.; Cronin, K.A.; Mariotto, A.B.; Lowy, D.R.; Feuer, E.J. The Effect of Advances in Lung-Cancer Treatment on Population Mortality. N. Engl. J. Med. 2020, 383, 640–649. [Google Scholar] [CrossRef]
- Li, T.; Pan, K.; Ellinwood, A.K.; Cress, R.D. Survival Trends of Metastatic Lung Cancer in California by Age at Diagnosis, Gender, Race/Ethnicity, and Histology, 1990–2014. Clin. Lung Cancer 2021, 22, e602–e611. [Google Scholar] [CrossRef]
- Ma, W.; Gilligan, B.M.; Yuan, J.; Li, T. Current status and perspectives in translational biomarker research for PD-1/PD-L1 immune checkpoint blockade therapy. J. Hematol. Oncol. 2016, 9, 47. [Google Scholar] [CrossRef]
- Li, T.; Kung, H.J.; Mack, P.C.; Gandara, D.R. Genotyping and genomic profiling of non-small-cell lung cancer: Implications for current and future therapies. J. Clin. Oncol. 2013, 31, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Scott, E.C.; Baines, A.C.; Gong, Y.; Moore, R., Jr.; Pamuk, G.E.; Saber, H.; Subedee, A.; Thompson, M.D.; Xiao, W.; Pazdur, R.; et al. Trends in the approval of cancer therapies by the FDA in the twenty-first century. Nat. Rev. Drug Discov. 2023, 22, 625–640. [Google Scholar] [CrossRef] [PubMed]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The three Es of cancer immunoediting. Annu. Rev. Immunol. 2004, 22, 329–360. [Google Scholar] [CrossRef]
- Piljic Burazer, M.; Mladinov, S.; Capkun, V.; Kuret, S.; Glavina Durdov, M. The Utility of Thyroid Transcription Factor 1 (TTF-1), Napsin A, Excision Repair Cross-Complementing 1 (ERCC1), Anaplastic Lymphoma Kinase (ALK) and the Epidermal Growth Factor Receptor (EGFR) Expression in Small Biopsy in Prognosis of Patients with Lung Adenocarcinoma—A Retrograde Single-Center Study from Croatia. Med. Sci. Monit. 2017, 23, 489–497. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Ao, M.H.; Zhang, H.; Sakowski, L.; Sharma, R.; Illei, P.B.; Gabrielson, E.; Askin, F.; Li, Q.K. The utility of a novel triple marker (combination of TTF1, napsin A, and p40) in the subclassification of non-small cell lung cancer. Hum. Pathol. 2014, 45, 926–934. [Google Scholar] [CrossRef]
- Zhang, P.; Han, Y.P.; Huang, L.; Li, Q.; Ma, D.L. Value of napsin A and thyroid transcription factor-1 in the identification of primary lung adenocarcinoma. Oncol. Lett. 2010, 1, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, X.; Yin, J.; Song, X.; Chen, X.; Feng, J.; Gao, H.; Liu, L.; Wei, S. The high diagnostic accuracy of combined test of thyroid transcription factor 1 and Napsin A to distinguish between lung adenocarcinoma and squamous cell carcinoma: A meta-analysis. PLoS ONE 2014, 9, e100837. [Google Scholar] [CrossRef] [PubMed]
- Schilsky, J.B.; Ni, A.; Ahn, L.; Datta, S.; Travis, W.D.; Kris, M.G.; Chaft, J.E.; Rekhtman, N.; Hellmann, M.D. Prognostic impact of TTF-1 expression in patients with stage IV lung adenocarcinomas. Lung Cancer 2017, 108, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Affandi, K.A.; Tizen, N.M.S.; Mustangin, M.; Zin, R. p40 Immunohistochemistry Is an Excellent Marker in Primary Lung Squamous Cell Carcinoma. J. Pathol. Transl. Med. 2018, 52, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Lilo, M.T.; Allison, D.; Wang, Y.; Ao, M.; Gabrielson, E.; Geddes, S.; Zhang, H.; Askin, F.; Li, Q.K. Expression of P40 and P63 in lung cancers using fine needle aspiration cases. Understanding clinical pitfalls and limitations. J. Am. Soc. Cytopathol. 2016, 5, 123–132. [Google Scholar] [CrossRef]
- Nicholson, A.G.; Tsao, M.S.; Beasley, M.B.; Borczuk, A.C.; Brambilla, E.; Cooper, W.A.; Dacic, S.; Jain, D.; Kerr, K.M.; Lantuejoul, S.; et al. The 2021 WHO Classification of Lung Tumors: Impact of Advances Since 2015. J. Thorac. Oncol. 2022, 17, 362–387. [Google Scholar] [CrossRef]
- Vargas, A.J.; Harris, C.C. Biomarker development in the precision medicine era: Lung cancer as a case study. Nat. Rev. Cancer 2016, 16, 525–537. [Google Scholar] [CrossRef] [PubMed]
- Hugo, W.; Zaretsky, J.M.; Sun, L.; Song, C.; Moreno, B.H.; Hu-Lieskovan, S.; Berent-Maoz, B.; Pang, J.; Chmielowski, B.; Cherry, G.; et al. Genomic and Transcriptomic Features of Response to Anti-PD-1 Therapy in Metastatic Melanoma. Cell 2016, 165, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Zaretsky, J.M.; Garcia-Diaz, A.; Shin, D.S.; Escuin-Ordinas, H.; Hugo, W.; Hu-Lieskovan, S.; Torrejon, D.Y.; Abril-Rodriguez, G.; Sandoval, S.; Barthly, L.; et al. Mutations Associated with Acquired Resistance to PD-1 Blockade in Melanoma. N. Engl. J. Med. 2016, 375, 819–829. [Google Scholar] [CrossRef]
- Lindeman, N.I.; Cagle, P.T.; Beasley, M.B.; Chitale, D.A.; Dacic, S.; Giaccone, G.; Jenkins, R.B.; Kwiatkowski, D.J.; Saldivar, J.S.; Squire, J.; et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: Guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2013, 137, 828–860. [Google Scholar] [CrossRef]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef]
- Kalemkerian, G.P.; Narula, N.; Kennedy, E.B.; Biermann, W.A.; Donington, J.; Leighl, N.B.; Lew, M.; Pantelas, J.; Ramalingam, S.S.; Reck, M.; et al. Molecular Testing Guideline for the Selection of Patients With Lung Cancer for Treatment With Targeted Tyrosine Kinase Inhibitors: American Society of Clinical Oncology Endorsement of the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 911–919. [Google Scholar] [CrossRef]
- Muro, K.; Van Cutsem, E.; Narita, Y.; Pentheroudakis, G.; Baba, E.; Li, J.; Ryu, M.H.; Zamaniah, W.I.W.; Yong, W.P.; Yeh, K.H.; et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic gastric cancer: A JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann. Oncol. 2019, 30, 19–33. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Guidelines: Non-Small Cell Lung Cancer V2.2019. Plymouth Meeting: Montgomery, PA, USA, 2018. [Google Scholar]
- Wan, J.C.M.; Massie, C.; Garcia-Corbacho, J.; Mouliere, F.; Brenton, J.D.; Caldas, C.; Pacey, S.; Baird, R.; Rosenfeld, N. Liquid biopsies come of age: Towards implementation of circulating tumour DNA. Nat. Rev. Cancer 2017, 17, 223–238. [Google Scholar] [CrossRef]
- Chung, J.H.; Pavlick, D.; Hartmaier, R.; Schrock, A.B.; Young, L.; Forcier, B.; Ye, P.; Levin, M.K.; Goldberg, M.; Burris, H.; et al. Hybrid capture-based genomic profiling of circulating tumor DNA from patients with estrogen receptor-positive metastatic breast cancer. Ann. Oncol. 2017, 28, 2866–2873. [Google Scholar] [CrossRef]
- Exome Aggregation Consortium. 2017. Available online: http://exac.broadinstitute.org/ (accessed on 30 May 2024).
- Schwaederle, M.; Zhao, M.; Lee, J.J.; Eggermont, A.M.; Schilsky, R.L.; Mendelsohn, J.; Lazar, V.; Kurzrock, R. Impact of Precision Medicine in Diverse Cancers: A Meta-Analysis of Phase II Clinical Trials. J. Clin. Oncol. 2015, 33, 3817–3825. [Google Scholar] [CrossRef]
- Doroshow, D.B.; Bhalla, S.; Beasley, M.B.; Sholl, L.M.; Kerr, K.M.; Gnjatic, S.; Wistuba, I.I.; Rimm, D.L.; Tsao, M.S.; Hirsch, F.R. PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nat. Rev. Clin. Oncol. 2021, 18, 345–362. [Google Scholar] [CrossRef]
- Marcus, L.; Fashoyin-Aje, L.A.; Donoghue, M.; Yuan, M.; Rodriguez, L.; Gallagher, P.S.; Philip, R.; Ghosh, S.; Theoret, M.R.; Beaver, J.A.; et al. FDA Approval Summary: Pembrolizumab for the Treatment of Tumor Mutational Burden-High Solid Tumors. Clin. Cancer Res. 2021, 27, 4685–4689. [Google Scholar] [CrossRef]
- Riely, G.J.; Wood, D.E.; Ettinger, D.S.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; et al. Non-Small Cell Lung Cancer, Version 4.2024. J. Natl. Compr. Canc Netw. 2024, 22, 249–274. [Google Scholar] [CrossRef]
- An, H.J.; Chon, H.J.; Kim, C. Peripheral Blood-Based Biomarkers for Immune Checkpoint Inhibitors. Int. J. Mol. Sci. 2021, 22, 9414. [Google Scholar] [CrossRef]
- Ma, W.; Wei, S.; Long, S.; Tian, E.C.; McLaughlin, B.; Jaimes, M.; Montoya, D.J.; Viswanath, V.R.; Chien, J.; Zhang, Q.; et al. Dynamic evaluation of blood immune cells predictive of response to immune checkpoint inhibitors in NSCLC by multicolor spectrum flow cytometry. Front. Immunol. 2023, 14, 1206631. [Google Scholar] [CrossRef]
- Wang, X.; Chen, D.; Ma, Y.; Mo, D.; Yan, F. Variation of peripheral blood-based biomarkers for response of anti-PD-1 immunotherapy in non-small-cell lung cancer. Clin. Transl. Oncol. 2024. [Google Scholar] [CrossRef]
- Gray, S.; Ottensmeier, C.H. Advancing Understanding of Non-Small Cell Lung Cancer with Multiplexed Antibody-Based Spatial Imaging Technologies. Cancers 2023, 15, 4797. [Google Scholar] [CrossRef]
- Gainor, J.F.; Shaw, A.T.; Sequist, L.V.; Fu, X.; Azzoli, C.G.; Piotrowska, Z.; Huynh, T.G.; Zhao, L.; Fulton, L.; Schultz, K.R.; et al. EGFR Mutations and ALK Rearrangements Are Associated with Low Response Rates to PD-1 Pathway Blockade in Non-Small Cell Lung Cancer: A Retrospective Analysis. Clin. Cancer Res. 2016, 22, 4585–4593. [Google Scholar] [CrossRef]
- Oxnard, G.R.; Yang, J.C.; Yu, H.; Kim, S.W.; Saka, H.; Horn, L.; Goto, K.; Ohe, Y.; Mann, H.; Thress, K.S.; et al. TATTON: A multi-arm, phase Ib trial of osimertinib combined with selumetinib, savolitinib, or durvalumab in EGFR-mutant lung cancer. Ann. Oncol. 2020, 31, 507–516. [Google Scholar] [CrossRef]
- Gavralidis, A.; Gainor, J.F. Immunotherapy in EGFR-Mutant and ALK-Positive Lung Cancer: Implications for Oncogene-Driven Lung Cancer. Cancer J. 2020, 26, 517–524. [Google Scholar] [CrossRef]
- Shepherd, F.A.; Rodrigues Pereira, J.; Ciuleanu, T.; Tan, E.H.; Hirsh, V.; Thongprasert, S.; Campos, D.; Maoleekoonpiroj, S.; Smylie, M.; Martins, R.; et al. Erlotinib in previously treated non-small-cell lung cancer. N. Engl. J. Med. 2005, 353, 123–132. [Google Scholar] [CrossRef]
- Yu, H.A.; Riely, G.J. Second-generation epidermal growth factor receptor tyrosine kinase inhibitors in lung cancers. J. Natl. Compr. Cancer Netw. 2013, 11, 161–169. [Google Scholar] [CrossRef]
- Karachaliou, N.; Fernandez-Bruno, M.; Bracht, J.W.P.; Rosell, R. EGFR first- and second-generation TKIs-there is still place for them in EGFR-mutant NSCLC patients. Transl. Cancer Res. 2019, 8, S23–S47. [Google Scholar] [CrossRef]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Harvey, R.D.; Adams, V.R.; Beardslee, T.; Medina, P. Afatinib for the treatment of EGFR mutation-positive NSCLC: A review of clinical findings. J. Oncol. Pharm. Pract. 2020, 26, 1461–1474. [Google Scholar] [CrossRef] [PubMed]
- Okuma, Y.; Kubota, K.; Shimokawa, M.; Hashimoto, K.; Kawashima, Y.; Sakamoto, T.; Wakui, H.; Murakami, S.; Okishio, K.; Hayashihara, K.; et al. First-Line Osimertinib for Previously Untreated Patients with NSCLC and Uncommon EGFR Mutations: The UNICORN Phase 2 Nonrandomized Clinical Trial. JAMA Oncol. 2023, 10, 43–51. [Google Scholar] [CrossRef]
- Wang, V.E.; Gainor, J.F. Osimertinib in Patients with Non-Small Cell Lung Cancer and Uncommon EGFR Mutations-Chasing Unicorns? JAMA Oncol. 2023, 10, 52–53. [Google Scholar] [CrossRef]
- Chon, K.; Larkins, E.; Chatterjee, S.; Mishra-Kalyani, P.S.; Aungst, S.; Wearne, E.; Subramaniam, S.; Li, Y.; Liu, J.; Sun, J.; et al. FDA Approval Summary: Amivantamab for the Treatment of Patients with Non-Small Cell Lung Cancer with EGFR Exon 20 Insertion Mutations. Clin. Cancer Res. 2023, 29, 3262–3266. [Google Scholar] [CrossRef]
- FDA. 2024. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-amivantamab-vmjw-egfr-exon-20-insertion-mutated-non-small-cell-lung-cancer-indications (accessed on 30 May 2024).
- Cohen, M.H.; Gootenberg, J.; Keegan, P.; Pazdur, R. FDA drug approval summary: Bevacizumab (Avastin) plus Carboplatin and Paclitaxel as first-line treatment of advanced/metastatic recurrent nonsquamous non-small cell lung cancer. Oncologist 2007, 12, 713–718. [Google Scholar] [CrossRef]
- Giaccone, G.; Herbst, R.S.; Manegold, C.; Scagliotti, G.; Rosell, R.; Miller, V.; Natale, R.B.; Schiller, J.H.; Von Pawel, J.; Pluzanska, A.; et al. Gefitinib in combination with gemcitabine and cisplatin in advanced non-small-cell lung cancer: A phase III trial--INTACT 1. J. Clin. Oncol. 2004, 22, 777–784. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; Schiller, J.H.; Natale, R.B.; Miller, V.; Manegold, C.; Scagliotti, G.; Rosell, R.; Oliff, I.; Reeves, J.A.; et al. Gefitinib in combination with paclitaxel and carboplatin in advanced non-small-cell lung cancer: A phase III trial—INTACT 2. J. Clin. Oncol. 2004, 22, 785–794. [Google Scholar] [CrossRef]
- Herbst, R.S.; Prager, D.; Hermann, R.; Fehrenbacher, L.; Johnson, B.E.; Sandler, A.; Kris, M.G.; Tran, H.T.; Klein, P.; Li, X.; et al. TRIBUTE: A phase III trial of erlotinib hydrochloride (OSI-774) combined with carboplatin and paclitaxel chemotherapy in advanced non-small-cell lung cancer. J. Clin. Oncol. 2005, 23, 5892–5899. [Google Scholar] [CrossRef]
- Gatzemeier, U.; Pluzanska, A.; Szczesna, A.; Kaukel, E.; Roubec, J.; De Rosa, F.; Milanowski, J.; Karnicka-Mlodkowski, H.; Pesek, M.; Serwatowski, P.; et al. Phase III study of erlotinib in combination with cisplatin and gemcitabine in advanced non-small-cell lung cancer: The Tarceva Lung Cancer Investigation Trial. J. Clin. Oncol. 2007, 25, 1545–1552. [Google Scholar] [CrossRef]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef]
- Chatterjee, M.; Turner, D.C.; Felip, E.; Lena, H.; Cappuzzo, F.; Horn, L.; Garon, E.B.; Hui, R.; Arkenau, H.T.; Gubens, M.A.; et al. Systematic evaluation of pembrolizumab dosing in patients with advanced non-small-cell lung cancer. Ann. Oncol. 2016, 27, 1291–1298. [Google Scholar] [CrossRef]
- Hui, R.; Garon, E.B.; Goldman, J.W.; Leighl, N.B.; Hellmann, M.D.; Patnaik, A.; Gandhi, L.; Eder, J.P.; Ahn, M.J.; Horn, L.; et al. Pembrolizumab as first-line therapy for patients with PD-L1-positive advanced non-small cell lung cancer: A phase 1 trial. Ann. Oncol. 2017, 28, 874–881. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Langer, C.J.; Gadgeel, S.M.; Borghaei, H.; Papadimitrakopoulou, V.A.; Patnaik, A.; Powell, S.F.; Gentzler, R.D.; Martins, R.G.; Stevenson, J.P.; Jalal, S.I.; et al. Carboplatin and pemetrexed with or without pembrolizumab for advanced, non-squamous non-small-cell lung cancer: A randomised, phase 2 cohort of the open-label KEYNOTE-021 study. Lancet Oncol. 2016, 17, 1497–1508. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab Versus Chemotherapy for Metastatic Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score >/= 50. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- de Castro, G., Jr.; Kudaba, I.; Wu, Y.L.; Lopes, G.; Kowalski, D.M.; Turna, H.Z.; Caglevic, C.; Zhang, L.; Karaszewska, B.; Laktionov, K.K.; et al. Five-Year Outcomes with Pembrolizumab Versus Chemotherapy as First-Line Therapy in Patients with Non-Small-Cell Lung Cancer and Programmed Death Ligand-1 Tumor Proportion Score >/= 1% in the KEYNOTE-042 Study. J. Clin. Oncol. 2023, 41, 1986–1991. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Sezer, A.; Kilickap, S.; Gumus, M.; Bondarenko, I.; Ozguroglu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Garassino, M.C.; Gadgeel, S.; Speranza, G.; Felip, E.; Esteban, E.; Domine, M.; Hochmair, M.J.; Powell, S.F.; Bischoff, H.G.; Peled, N.; et al. Pembrolizumab Plus Pemetrexed and Platinum in Nonsquamous Non-Small-Cell Lung Cancer: 5-Year Outcomes from the Phase 3 KEYNOTE-189 Study. J. Clin. Oncol. 2023, 41, 1992–1998. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Socinski, M.A.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; et al. IMpower150 Final Overall Survival Analyses for Atezolizumab Plus Bevacizumab and Chemotherapy in First-Line Metastatic Nonsquamous NSCLC. J. Thorac. Oncol. 2021, 16, 1909–1924. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gumus, M.; Mazieres, J.; Hermes, B.; Cay Senler, F.; Csoszi, T.; Fulop, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Novello, S.; Kowalski, D.M.; Luft, A.; Gumus, M.; Vicente, D.; Mazieres, J.; Rodriguez-Cid, J.; Tafreshi, A.; Cheng, Y.; Lee, K.H.; et al. Pembrolizumab Plus Chemotherapy in Squamous Non-Small-Cell Lung Cancer: 5-Year Update of the Phase III KEYNOTE-407 Study. J. Clin. Oncol. 2023, 41, 1999–2006. [Google Scholar] [CrossRef]
- Jotte, R.; Cappuzzo, F.; Vynnychenko, I.; Stroyakovskiy, D.; Rodriguez-Abreu, D.; Hussein, M.; Soo, R.; Conter, H.J.; Kozuki, T.; Huang, K.C.; et al. Atezolizumab in Combination with Carboplatin and Nab-Paclitaxel in Advanced Squamous NSCLC (IMpower131): Results from a Randomized Phase III Trial. J. Thorac. Oncol. 2020, 15, 1351–1360. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Ciuleanu, T.E.; Pluzanski, A.; Lee, J.S.; Otterson, G.A.; Audigier-Valette, C.; Minenza, E.; Linardou, H.; Burgers, S.; Salman, P.; et al. Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden. N. Engl. J. Med. 2018, 378, 2093–2104. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Lee, J.-S.; Ciuleanu, T.-E.; Caro, R.B.; Nishio, M.; Urban, L.; Audigier-Valette, C.; Lupinacci, L.; Sangha, R.; Pluzanski, A.; et al. Five-Year Survival Outcomes with Nivolumab Plus Ipilimumab Versus Chemotherapy as First-Line Treatment for Metastatic Non–Small-Cell Lung Cancer in CheckMate 227. J. Clin. Oncol. 2023, 41, 1200–1212. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef]
- Carbone, D.P.; Ciuleanu, T.E.; Schenker, M.; Cobo, M.; Bordenave, S.; Juan-Vidal, O.; Menezes, J.; Reinmuth, N.; Richardet, E.; Cheng, Y.; et al. Four-year clinical update and treatment switching-adjusted outcomes with first-line nivolumab plus ipilimumab with chemotherapy for metastatic non-small cell lung cancer in the CheckMate 9LA randomized trial. J. Immunother. Cancer 2024, 12, e008189. [Google Scholar] [CrossRef]
- Gogishvili, M.; Melkadze, T.; Makharadze, T.; Giorgadze, D.; Dvorkin, M.; Penkov, K.; Laktionov, K.; Nemsadze, G.; Nechaeva, M.; Rozhkova, I.; et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: A randomized, controlled, double-blind phase 3 trial. Nat. Med. 2022, 28, 2374–2380. [Google Scholar] [CrossRef]
- Johnson, M.L.; Cho, B.C.; Luft, A.; Alatorre-Alexander, J.; Geater, S.L.; Laktionov, K.; Kim, S.W.; Ursol, G.; Hussein, M.; Lim, F.L.; et al. Durvalumab with or Without Tremelimumab in Combination with Chemotherapy as First-Line Therapy for Metastatic Non-Small-Cell Lung Cancer: The Phase III POSEIDON Study. J. Clin. Oncol. 2023, 41, 1213–1227. [Google Scholar] [CrossRef]
- Wang, Z.; Wu, L.; Li, B.; Cheng, Y.; Li, X.; Wang, X.; Han, L.; Wu, X.; Fan, Y.; Yu, Y.; et al. Toripalimab Plus Chemotherapy for Patients with Treatment-Naive Advanced Non-Small-Cell Lung Cancer: A Multicenter Randomized Phase III Trial (CHOICE-01). J. Clin. Oncol. 2023, 41, 651–663. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Z.; Wu, L.; Li, B.; Cheng, Y.; Li, X.; Wang, X.; Han, L.; Wu, X.; Fan, Y.; et al. Final overall survival and biomarker analyses of CHOICE-01: A double-blind randomized phase 3 study of toripalimab versus placebo in combination chemotherapy for advanced NSCLC without EGFR/ALK mutations. J. Clin. Oncol. 2023, 41, 9003. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef]
- Borghaei, H.; Langer, C.J.; Gadgeel, S.; Papadimitrakopoulou, V.A.; Patnaik, A.; Powell, S.F.; Gentzler, R.D.; Martins, R.G.; Stevenson, J.P.; Jalal, S.I.; et al. 24-Month Overall Survival from KEYNOTE-021 Cohort G: Pemetrexed and Carboplatin with or without Pembrolizumab as First-Line Therapy for Advanced Nonsquamous Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2019, 14, 124–129. [Google Scholar] [CrossRef]
- Gadgeel, S.; Rodriguez-Abreu, D.; Speranza, G.; Esteban, E.; Felip, E.; Domine, M.; Hui, R.; Hochmair, M.J.; Clingan, P.; Powell, S.F.; et al. Updated Analysis From KEYNOTE-189: Pembrolizumab or Placebo Plus Pemetrexed and Platinum for Previously Untreated Metastatic Nonsquamous Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 1505–1517. [Google Scholar] [CrossRef]
- Fukumura, D.; Kloepper, J.; Amoozgar, Z.; Duda, D.G.; Jain, R.K. Enhancing cancer immunotherapy using antiangiogenics: Opportunities and challenges. Nat. Rev. Clin. Oncol. 2018, 15, 325–340. [Google Scholar] [CrossRef]
- Voron, T.; Colussi, O.; Marcheteau, E.; Pernot, S.; Nizard, M.; Pointet, A.L.; Latreche, S.; Bergaya, S.; Benhamouda, N.; Tanchot, C.; et al. VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors. J. Exp. Med. 2015, 212, 139–148. [Google Scholar] [CrossRef]
- Hassel, J.C.; Heinzerling, L.; Aberle, J.; Bahr, O.; Eigentler, T.K.; Grimm, M.O.; Grunwald, V.; Leipe, J.; Reinmuth, N.; Tietze, J.K.; et al. Combined immune checkpoint blockade (anti-PD-1/anti-CTLA-4): Evaluation and management of adverse drug reactions. Cancer Treat. Rev. 2017, 57, 36–49. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Carbone, D.P.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.M.; Ciuleanu, T.E.; Badin, F.; et al. First-Line Nivolumab in Stage IV or Recurrent Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef]
- Rizvi, N.; Chul Cho, B.; Reinmuth, N.; Lee, K.; Ahn, M.; Luft, A.; van den Heuvel, M.; Cobo, M.; Smolin, A.; Vicente, D.; et al. LBA6 Durvalumab with or without tremelimumab vs platinum-based chemotherapy as first-line treatment for metastatic non-small cell lung cancer: MYSTIC. Ann. Oncol. 2018, 29, x40–x41. [Google Scholar] [CrossRef]
- Barlesi, F.; Vansteenkiste, J.; Spigel, D.; Ishii, H.; Garassino, M.; de Marinis, F.; Ozguroglu, M.; Szczesna, A.; Polychronis, A.; Uslu, R.; et al. Avelumab versus docetaxel in patients with platinum-treated advanced non-small-cell lung cancer (JAVELIN Lung 200): An open-label, randomised, phase 3 study. Lancet Oncol. 2018, 19, 1468–1479. [Google Scholar] [CrossRef] [PubMed]
- Lisberg, A.; Cummings, A.; Goldman, J.W.; Bornazyan, K.; Reese, N.; Wang, T.; Coluzzi, P.; Ledezma, B.; Mendenhall, M.; Hunt, J.; et al. A Phase II Study of Pembrolizumab in EGFR-Mutant, PD-L1+, Tyrosine Kinase Inhibitor Naive Patients with Advanced NSCLC. J. Thorac. Oncol. 2018, 13, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Cho, B.C.; Kim, J.H.; Mazieres, J.; Vansteenkiste, J.; Lena, H.; Corral Jaime, J.; Gray, J.E.; Powderly, J.; Chouaid, C.; et al. Durvalumab as third-line or later treatment for advanced non-small-cell lung cancer (ATLANTIC): An open-label, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 521–536. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; Reynolds, C.; Waterhouse, D.; Garon, E.B.; Chandler, J.; Babu, S.; Thurmes, P.; Spira, A.; Jotte, R.; Zhu, J.; et al. Phase 1/2 Study of the Safety and Tolerability of Nivolumab Plus Crizotinib for the First-Line Treatment of Anaplastic Lymphoma Kinase Translocation—Positive Advanced Non-Small Cell Lung Cancer (CheckMate 370). J. Thorac. Oncol. 2018, 13, 682–688. [Google Scholar] [CrossRef]
- Ahn, M.-J.; Yang, J.; Yu, H.; Saka, H.; Ramalingam, S.; Goto, K.; Kim, S.W.; Yang, L.; Walding, A.; Oxnard, G.R. Osimertinib combined with durvalumab in EGFR-mutant non-small cell lung cancer: Results from the TATTON phase Ib trial. J. Thorac. Oncol. 2016, 11, S115. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Strategy for Patient Population | Clinical Trial Identifier (Name) | Sample Size (n) | Biomarker | Assay (Vendor) | Experimental vs. Control Regimen | Median OS (mos) | Median PFS (mos) | Tumor Response (ORR, CR/PR) | Author (Year) | |
|---|---|---|---|---|---|---|---|---|---|---|
| ICI monotherapy for stage IV or recurrent NSCLC with no sensitizing EGFR mutations or ALK translocations | NCT02142738 (KEYNOTE-024) | 305 | PD-L1 TPS ≥50% | 22C3 (Dako) | Pembrolizumab 200 mg Q3W × 35 cycles vs. investigator’s choice of platinum-based CT × 4–6 cycles | 30.0 vs. 14.2 | 10.3 vs. 6.0 | 44.8% vs. 27.8% | Reck (2016, 2019, 2021) [59,62,63] | |
| 5-year OS: 26.3 vs. 13.4 | 7.7 vs. 5.5 | 5-year: 46.1% (4.5/41.6%) vs. 31.1% (0/31.1%) | ||||||||
| 5-year OS rate: 31.9% vs. 16.3% | PFS2: 24.1 vs. 8.5 | |||||||||
| NCT02220894 (KEYNOTE-042) | 1274 | PD-L1 TPS ≥ 50% | 22C3 (Dako) | Pembrolizumab 200 mg Q3W × 35 cycles vs. investigator’s choice of platinum-based CT × 4–6 cycles | 20.0 vs. 12.2 | 7.1 vs. 6.4 | 27.3% vs. 26.5%; 39.1% vs. 32.3% | Mok (2019 [64]; Castro (2022) [65] | ||
| PD-L1 TPS ≥ 20% | 17.7 vs. 13.0 | 6.2 vs. 6.6 | 33.2% vs. 29.1% | |||||||
| PD-L1 TPS ≥ 1% | 16.7 vs. 12.1 | 5.4 vs. 6.5 | 27.3% vs. 26.7% | |||||||
| All cohorts | 5-year OS rate: 21.9% vs. 19.4% vs. 16.6% | 15.2% for retreatment | ||||||||
| NCT02409342 (Impower-110) | 572 | High PD-L1 (TC3 ≥ 50% or IC3 ≥ 10%) | SP142 (VENTANA) | Atezolizumab 1200 mg Q3W vs. CT | 20.2 vs. 13.1 | 8.1 vs. 5.0 | 68.3% vs. 35.7% | Herbst (2020) [66] | ||
| High + intermediate PD-L1 (≥5% of TC or IC) | 18.2 vs. 14.9 | 7.2 vs. 5.5 | 30.7% vs. 32.1%; Any 29.2 vs. 31.8% | |||||||
| NCT03088540 (EMPOWER-Lung 1) | 710 | PD-L1 TPS ≥50% | SP263 (VENTANA) | Cemiplimab 350 mg Q3W vs. CT | NR vs. 14.2 (HR, 0.57) | 8.2 vs. 5.7 | 39% (2/37) vs. 20% (1/19) | Sezer (2021) [67] | ||
| ICI-chemotherapy for non-squamous NSCLC with no EGFR or ALK genomic tumor aberrations | NCT02578680 (KEYNOTE-189) | 616 | PD-L1 TPS ≥1% vs. <1% | 22C3 (Dako) | Pembrolizumab 200 mg Q3W vs. placebo × 35 + CT | NR vs. 11.3 (0.49); 1-year OS: 69.2% vs. 49.4% | 8.8 vs. 4.9 | 47.6% vs. 18.9% | Gandhi (2018) [68]; Garassin o (2023) [69] | |
| 22.0 vs. 10.6; 5-year OS rates: 19.4% vs. 11.3% | 9.0 vs. 4.9; 5-year PFS rates: 7.5% vs. 0.6% | |||||||||
| NCT02366143 (IMpower150) | 1202 | Teff wild-type (WT) population | T-effector gene signature; SP142 and SP263 | Atezolizumab 1200 mg Q3W to control arm (ABCP) vs. BCP | WT: 19.2 vs. 14.7 | WT: 8.3 vs. 6.8 | 63.5% vs. 48% | Socinski (2018, 2021) [70,71] | ||
| Teff-high WT population | Teff-high: NA | Teff-high: 11.3 vs. 6.8 | ||||||||
| NCT02367781 (IMpower130) | 724 | PD-L1 TPS ≥1% or <1% | SP142 and SP263 | Atezolizumab + CT vs. CT | 18.6 vs. 13.9 | 7.0 vs. 5.5 | 49.2% vs. 31.9% | West (2019) [72] | ||
| ICI-chemotherapy for squamous NSCLC | NCT02775435 (KEYNOTE-407) | 506 | PD-L1 TPS ≥1% or <1% | 22C3 (Dako) | Pembrolizumab + CT × 35 cycles vs. CT | 7.8-month FU: 15.9 vs. 11.3 | 6.4 vs. 4.8 | 57.9% vs. 38.4% | Paz-Ares (2018, 2020) [73]; Novello (2023) [74] | |
| 14-month FU: 17.1 vs. 11.6; | 8.0 vs. 5.1 | |||||||||
| 17.2 vs. 11.6; 5-year OS rates: 18.4% vs. 9.7% | 8.0 vs. 5.1 | |||||||||
| NCT02367794 (IMpower 131) | 1021 | Tumor Gene Expression and PD-L1 TPS ≥1%, 10% or 50% | Gene profiling; SP142 and SP263 | Atezolizumab + SoC Chemo vs. Soc Chemo × 4–6 cycles | 14.2 vs. 13.5 | 6.3 vs. 5.6 | 49.7% vs. 41% | Jotte (2020) [75] | ||
| ICI-chemotherapy for NSCLC regardless of PD-L1 expression and histology subtypes | NCT02477826 (CheckMate 227) | 1739 | Co-Primary: PFS in TMB ≥10 muts/mb (n = 679) | FoundationOne CDx and 28-8 (Dako) | Nivolumab (nivo) 3 mg/kg IV Q2W and Ipilimumab (ipi) 1 mg/kg Q6W vs. CT | NA | 7.2 vs. 5.5 | 45.3% vs. 26.9% | Hellmann (2018)[76] | |
| OS in PD-L1 TPS ≥1% or <1% | 61-mo FU: 17.1 vs. 14.9 (PD-L1 ≥ 1%) and 17.4 vs. 12.2 (PD-L1 < 1%) | 61-mo FU: 5.1 vs. 5.6 (PD-L1 ≥ 1%) and 5.1 vs. 4.7 (PD-L1 < 1%) | 36% vs. 30% (PD-L1 ≥ 1%) and 27% vs. 23% (PD-L1 < 1%) | Hellmann (2019) [77] | ||||||
| OS in PD-L1 TPS ≥1% or <1% | 5-yr OS rates: 24% vs. 14% (PD-L1 ≥ 1%) and 19% vs. 7% (PD-L1 < 1%) | Brahmer (2022) [78] | ||||||||
| NCT03215706 (CheckMate-9LA) | 1150 enrolled, 719 randomized | Two co-primary endpoints: PD-L1 < 1% and PD-L1 ≥1% | 28-8 pharmDx assay (Agilent Dako) | Nivo 360 mg Q3W + Ipi 1 mg/kg Q6W + CT × 2 cycles vs. CT | 9.7-month FU: 14.1 vs. 10.3 After 2 more weeks; 15.6 vs. 10.9 | 6.8 vs. 5 | 37.7% vs. 25.1% | Paz-Arez (2021, 2023) [79]; Carbone (2024) [80] | ||
| At the 4-year follow-up, OS 21% vs. 16% | ||||||||||
| NCT03409614 (EMPOWER-Lung 3) | 466 | Any level of PD-L1 expression | VENTANA PD-L1(SP263) assay | Cemiplimab 350 mg ×108 weeks + CT Q3W vs. CT | 21.9 vs. 13.0 | 8.2 vs. 5.0 | 43.3% vs. 22.7% | Gogishvili (2022) [81] | ||
| NCT NCT03164616 (POSEIDON) | 1013 | PD-L1 ≥50% of TCs or PD-L1 <50% of TCs | VENTANA PD-L1(SP263) assay | T 75 mg + D 1500 mg + CT × 4 and T×1 | 14.0 | 6.2 | 38.8% | Johnson (2022) [82] | ||
| D+CT × 4, followed by D Q4W | 13.3 | 5.5 | 41.5% | |||||||
| CT | 11.7 | 4.8 | 24.4% | |||||||
| NCT03856411 (CHOICE-01) | 465 | TMB (n = 394), H-TMB (≥10 mutations/Mb) | PD-L1 (JS311 antibody) (MEDx, China) | Toripalimab 240 mg vs. Placebo + CT × 4-6, followed by toripalimab vs. placebo Q3W | Not reached vs. 17.1 (HR 0.69); 23.8 vs. 17.0 | 8.4 vs. 5.6; H-TMB: 13.1 vs. 5.5 | 65.7% vs. 46.2% H-TMB: 72.7% vs. 46.7% | Wang (2023) [83,84] | ||
| Clinical Trial Identifier (Name) | Phase of Clinical Trial | Sample Size (No. Patients) | Biomarker | Assay (Marker) | Regimen | Control Regimen | Tumor Response (ORR) | Median PFS (mos) (HR) | Median OS (months) | Author (Year) Reference: |
|---|---|---|---|---|---|---|---|---|---|---|
| NCT02041533 (Checkmate 026) | Phase III | 423 | PD-L1 TPS ≥5% or <5%; TMB | 28–8 (Dako) | Nivolumab 3 mg/kg IV Q2W | SoC platinum-based chemotherapy | 26.6% vs. 33% | 4.2 vs. 5.9 (1.5) | 14.4 vs. 13.2 | Carbone (2017) [92] |
| NCT02453282 (MYSTIC) | Phase III | 1118 | PD-L1 TPS ≥25% or <25% | SP263 (Ventana) | Durvalumab 10 mg/kg IV Q2W for up to 12 months and tremelimumab 1 mg/kg IV Q4W for up to 4 doses | SoC platinum-based chemotherapy | 22.0% | NR (0.85) | NR | Rizvi (2018) [93] |
| NCT02395172 (JAVELIN Lung 200) | Phase III | 396 | PD-L1 PS ≥1% or <1% | 73–10 | Avelumab 10 mg/kg IV Q2W | Docetaxel 75 mg/m2 every 3 weeks. | 15.0% | 2.8 vs. 4.2 (0.9) | 11.4 vs. 10.3 | Barlesi (2018) [94] |
| NCT02879994 | Phase II | 25 | PD-L1 TPS ≥50% or <50%; EGFR+ | 22C3 (Dako) | Pembrolizumab 200 mg IV Q3W | / | 9.0% | / | / | Lsiberg (2018) [95] |
| NCT02087423 (ATLANTIC) | Phase II | 111 | PD-L1 TPS ≥25% or <25%; EGFR+ or ALK+ | SP263 (Ventana) | Durvalumab 10 mg/kg IV Q2W (EGFR+/ALK+) | Durvalumab 10 mg/kg IV every 2 weeks (EGFR-/ALK-) | 12.2% vs. 16.4% | 1.9 vs. 3.3 | 13.3 vs. 10.9 | Garassino (2018) [96] |
| CheckMate 370 | Phase I | 13 | PD-L1 positive tumor cells; ALK+ | 28–8 (Dako) | Nivolumab 240 mg Q2W and crizotinib 250 mg twice daily | / | 38.0% | / | / | Spigel (2018) [97] |
| NCT02143466 (TATTON) | Phase I | 34 | EGFR+ | SP263 (Ventana) | Osimertinib 80 mg QD and durvalumab 3 mg/kg Q2W | / | PR: 53% | / | / | Anh (2016) [98] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, T.; Ma, W.; Al-Obeidi, E. Evolving Precision First-Line Systemic Treatment for Patients with Unresectable Non-Small Cell Lung Cancer. Cancers 2024, 16, 2350. https://doi.org/10.3390/cancers16132350
Li T, Ma W, Al-Obeidi E. Evolving Precision First-Line Systemic Treatment for Patients with Unresectable Non-Small Cell Lung Cancer. Cancers. 2024; 16(13):2350. https://doi.org/10.3390/cancers16132350
Chicago/Turabian StyleLi, Tianhong, Weijie Ma, and Ebaa Al-Obeidi. 2024. "Evolving Precision First-Line Systemic Treatment for Patients with Unresectable Non-Small Cell Lung Cancer" Cancers 16, no. 13: 2350. https://doi.org/10.3390/cancers16132350
APA StyleLi, T., Ma, W., & Al-Obeidi, E. (2024). Evolving Precision First-Line Systemic Treatment for Patients with Unresectable Non-Small Cell Lung Cancer. Cancers, 16(13), 2350. https://doi.org/10.3390/cancers16132350