
Outcome of Patients with Locally Advanced Rectal Cancer Pursuing Non-Surgical Strategy in National Cancer Database
 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Source
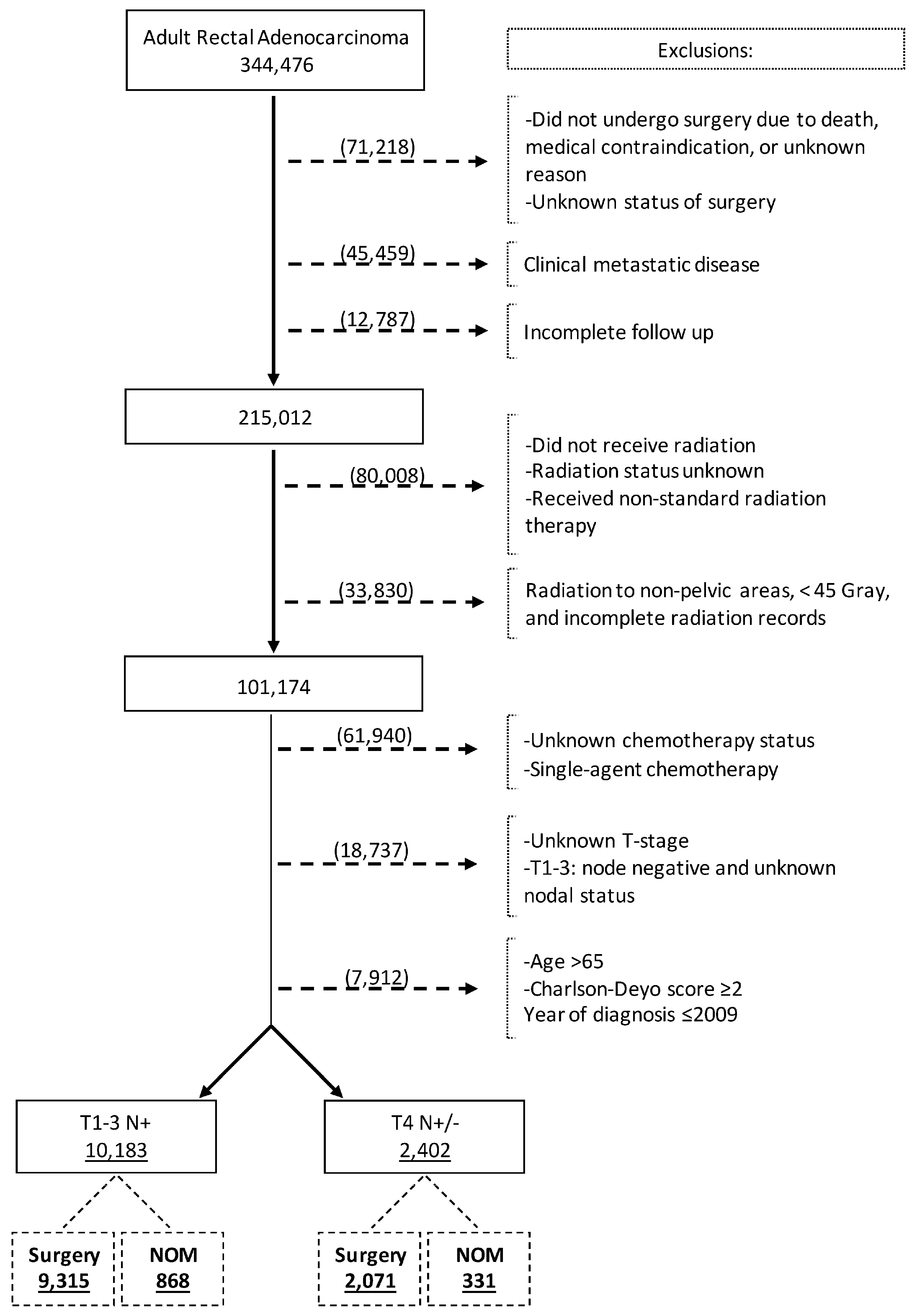
2.2. Study Population
2.3. Variables and Outcomes Measures
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Cohort
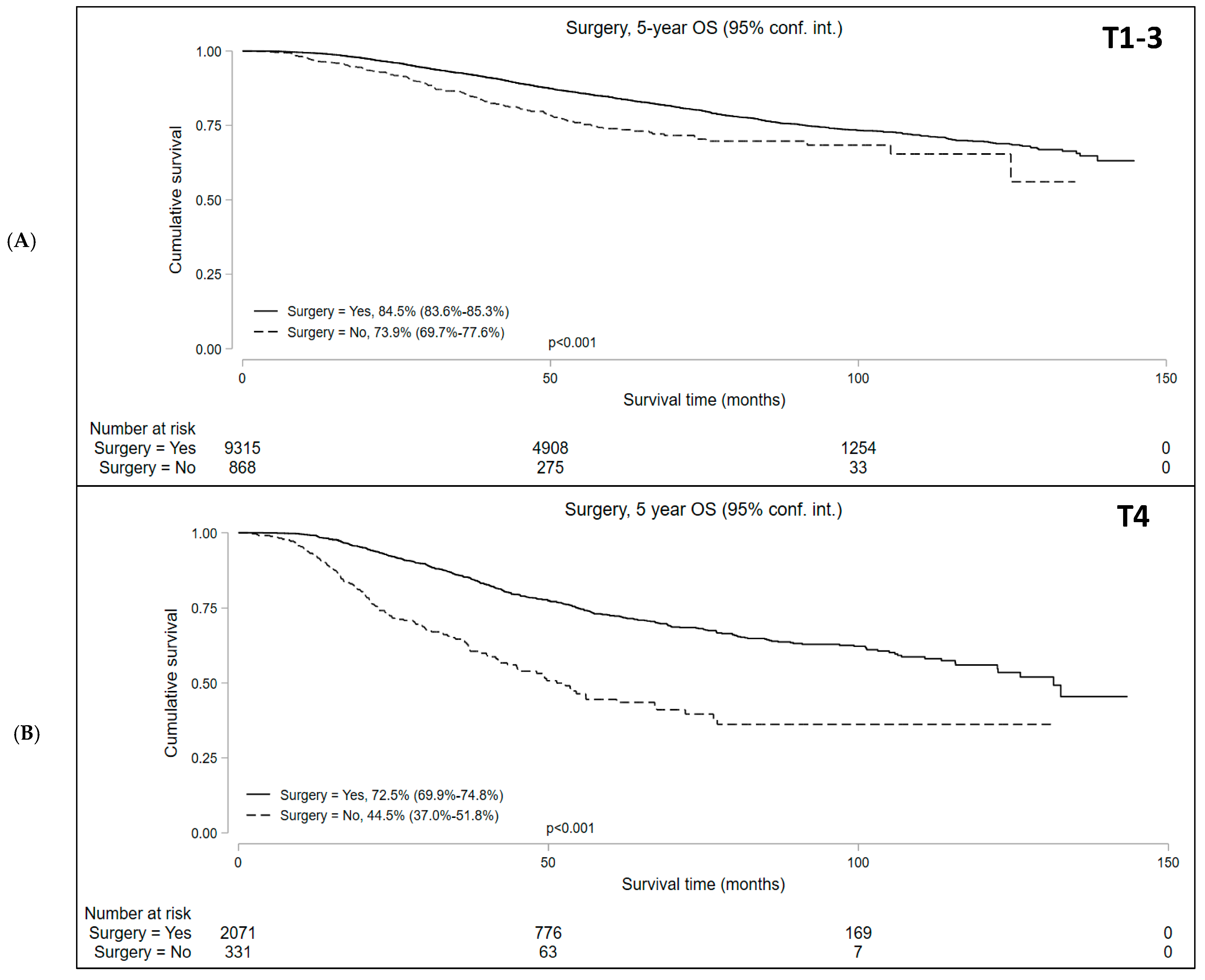
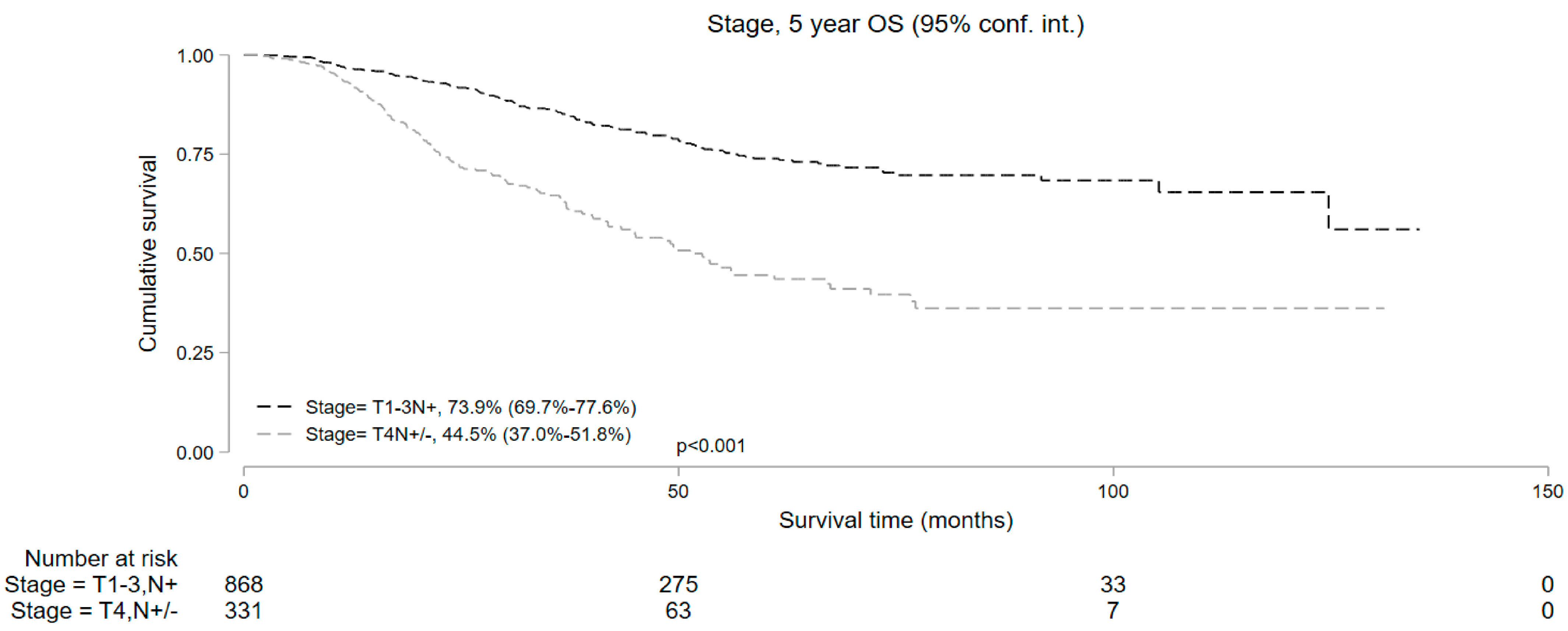
3.2. Survival Analysis
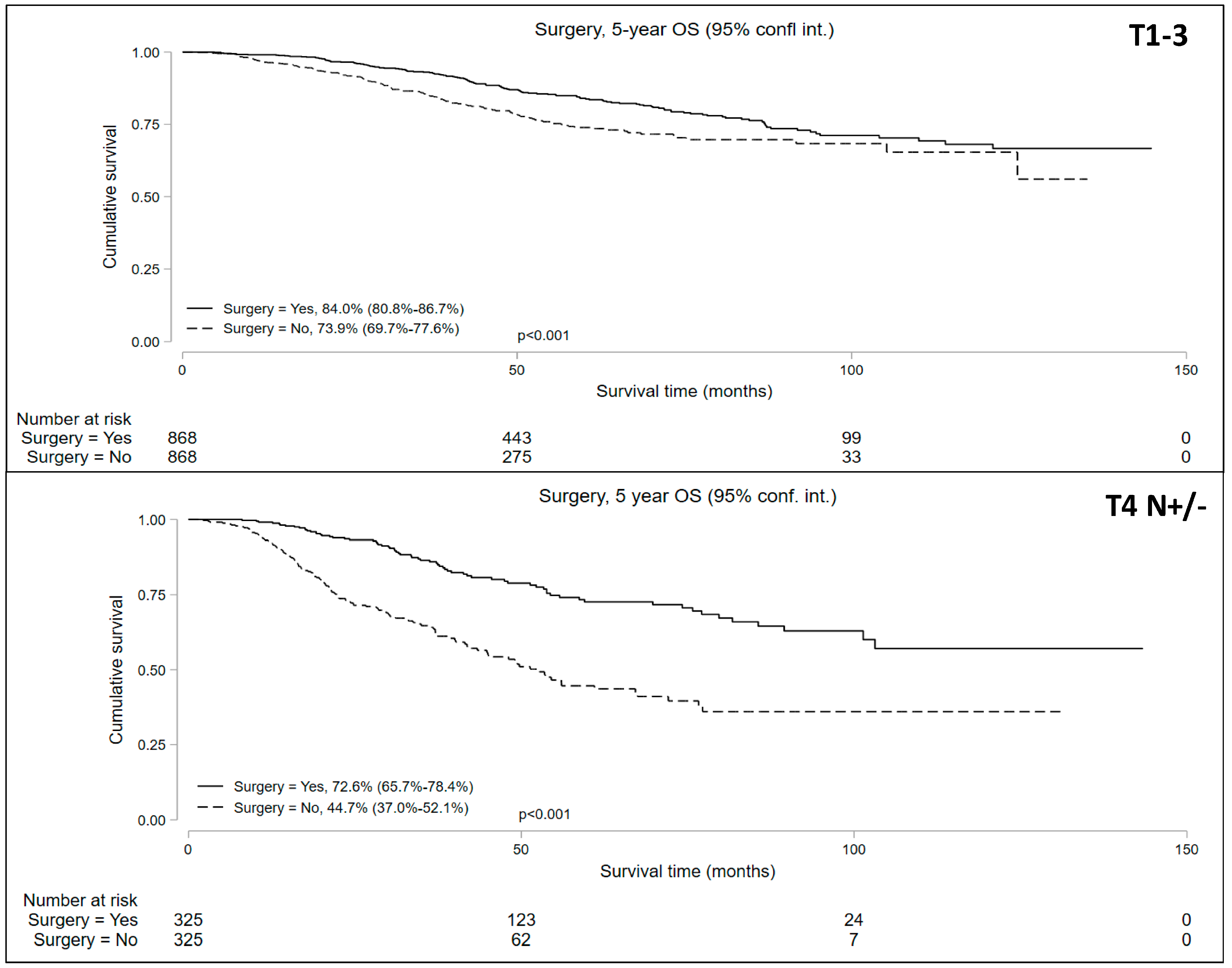
3.3. Propensity Matched Comparison of Surgery and NOM
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Azad, N.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Garrido-Laguna, I.; et al. Rectal Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 1139–1167. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Ladbury, C.; Glaser, S.; Fakih, M.; Kaiser, A.M.; Chen, Y.-J.; Williams, T.M.; Amini, A. Patterns of Care for Patients with Locally Advanced Rectal Cancer Treated with Total Neoadjuvant Therapy at Predominately Academic Centers between 2016–2020: An NCDB Analysis. Clin. Color. Cancer 2023, 22, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Unuvar, M.; Blansfield, J.; Wang, S.; Hoffman, R.L. Trends in adoption of total neoadjuvant therapy for locally advanced rectal cancer. Am. J. Surg. 2023, 227, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Bosset, J.-F.; Etienne, P.-L.; Rio, E.; François, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Appelt, A.L.; Pløen, J.; Harling, H.; Jensen, F.S.; Jensen, L.H.; Jørgensen, J.C.R.; Lindebjerg, J.; Rafaelsen, S.R.; Jakobsen, A. High-dose chemoradiotherapy and watchful waiting for distal rectal cancer: A prospective observational study. Lancet Oncol. 2015, 16, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Habr-Gama, A.; Gama-Rodrigues, J.; Julião, G.P.S.; Proscurshim, I.; Sabbagh, C.; Lynn, P.B.; Perez, R.O. Local recurrence after complete clinical response and watch and wait in rectal cancer after neoadjuvant chemoradiation: Impact of salvage therapy on local disease control. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Habr-Gama, A.; Perez, R.O. Non-operative management of rectal cancer after neoadjuvant chemoradiation. Br. J. Surg. 2009, 96, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Habr-Gama, A.; Perez, R.O.; Nadalin, W.; Sabbaga, J.; Ribeiro, U., Jr.; e Sousa, A.H.S., Jr.; Gama-Rodrigues, J. Operative versus Non-operative Treatment for Stage 0 Distal Rectal Cancer Following Chemoradiation Therapy: Long-term Results. Ann. Surg. 2004, 240, 711–718. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Perez, R.; Proscurshim, I.; Campos, F.; Nadalin, W.; Kiss, D.; Gamarodrigues, J. Patterns of failure and survival for non-operative treatment of stage c0 distal rectal cancer following neoadjuvant chemoradiation therapy. J. Gastrointest. Surg. 2006, 10, 1319–1328. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Sabbaga, J.; Gama-Rodrigues, J.; Guilherme, P.S.J.; Perez, R.O. Watch and wait approach following extended neoadjuvant chemoradiation for distal rectal cancer: Are we getting closer to anal cancer management? Dis. Colon Rectum 2013, 56, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Beets-Tan, R.G.; Lambregts, D.M.; Lammering, G.; Nelemans, P.J.; Engelen, S.M.; van Dam, R.M.; Jansen, R.L.; Sosef, M.; Leijtens, J.W.; et al. Wait-and-See Policy for Clinical Complete Responders after Chemoradiation for Rectal Cancer. J. Clin. Oncol. 2011, 29, 4633–4640. [Google Scholar] [CrossRef] [PubMed]
- Martens, M.H.; Maas, M.; Heijnen, L.A.; Lambregts, D.M.J.; Leijtens, J.W.A.; Stassen, L.P.S.; Breukink, S.O.; Hoff, C.; Belgers, E.J.; Melenhorst, J.; et al. Long-term Outcome of an Organ Preservation Program After Neoadjuvant Treatment for Rectal Cancer. J. Natl. Cancer Inst. 2016, 108, djw171. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J.; Strombom, P.; Chow, O.S.; Roxburgh, C.S.; Lynn, P.; Anne, E.; Maria, W.; Karuna, G.; Rona, Y.; Andrea, C. Assessment of a Watch-and-Wait Strategy for Rectal Cancer in Patients with a Complete Response after Neoadjuvant Therapy. JAMA Oncol. 2019, 5, e185896. [Google Scholar] [CrossRef] [PubMed]
- Temmink, S.J.D.; Peeters, K.C.M.J.; Bahadoer, R.R.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Melenhorst, J.; Burger, J.W.A.; Wolthuis, A.; Renehan, A.G.; Figueiredo, N.L.; et al. Watch and wait after neoadjuvant treatment in rectal cancer: Comparison of outcomes in patients with and without a complete response at first reassessment in the International Watch & Wait Database (IWWD). Br. J. Surg. 2023, 110, 676–684. [Google Scholar] [PubMed]
- van der Valk, M.J.M.; Hilling, D.E.; Bastiaannet, E.; Meershoek-Klein Kranenbarg, E.; Beets, G.L.; Figueiredo, N.L.; Habr-Gama, A.; Perez, R.O.; Renehan, A.G.; van de Velde, C.J.H.; et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): An international multicentre registry study. Lancet 2018, 391, 2537–2545. [Google Scholar] [PubMed]
- Garcia-Aguilar, J.; Patil, S.; Gollub, M.J.; Kim, J.K.; Yuval, J.B.; Thompson, H.M.; Verheij, F.S.; Omer, D.M.; Lee, M.; Dunne, R.F.; et al. Organ Preservation in Patients with Rectal Adenocarcinoma Treated with Total Neoadjuvant Therapy. J. Clin. Oncol. 2022, 40, 2546–2556. [Google Scholar] [CrossRef] [PubMed]
- Verheij, F.S.; Omer, D.M.; Williams, H.; Lin, S.T.; Qin, L.-X.; Buckley, J.T.; Thompson, H.M.; Yuval, J.B.; Kim, J.K.; Dunne, R.F.; et al. Long-Term Results of Organ Preservation in Patients with Rectal Adenocarcinoma Treated with Total Neoadjuvant Therapy: The Randomized Phase II OPRA Trial. J. Clin. Oncol. 2023, 42, 5. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Cho, J.R.; Jeong, S.; Oh, J.H.; Ahn, S.; Choi, S.; Kim, D.; Lee, B.H.; Youk, E.G.; Park, S.C.; et al. Quality of life after sphincter preservation surgery or abdominoperineal resection for low rectal cancer (ASPIRE): A long-term prospective, multicentre, cohort study. Lancet Reg. Health West. Pac. 2021, 6, 100087. [Google Scholar] [CrossRef]
- Peeters, K.; van de Velde, C.; Leer, J.; Martijn, H.; Junggeburt, J.; Kranenbarg, E.K.; Steup, W.; Wiggers, T.; Rutten, H.; Marijnen, C. Late side effects of short-course preoperative radiotherapy combined with total mesorectal excision for rectal cancer: Increased bowel dysfunction in irradiated patients—A Dutch colorectal cancer group study. J. Clin. Oncol. 2005, 23, 6199–6206. [Google Scholar] [CrossRef]
- Loria, A.; Tejani, M.A.; Temple, L.K.; Justiniano, C.F.; Melucci, A.D.; Becerra, A.Z.; Monson, J.R.T.; Aquina, C.T.; Fleming, F.J. Practice Patterns for Organ Preservation in US Patients With Rectal Cancer, 2006–2020. JAMA Oncol. 2023, 10, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Merkow, R.P.; Rademaker, A.W.; Bilimoria, K.Y. Practical Guide to Surgical Data Sets: National Cancer Database (NCDB). JAMA Surg. 2018, 153, 850–851. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Reif de Paula, T.; Haas, E.M.; Keller, D.S. Colorectal cancer in the 45-to-50 age group in the United States: A National Cancer Database (NCDB) analysis. Surg. Endosc. 2022, 36, 6629–6637. [Google Scholar] [CrossRef] [PubMed]
- Coffey, M.R.; Bachman, K.C.; Ho, V.P.; Worrell, S.G.; Moorman, M.L.; Linden, P.A.; Towe, C.W. Iatrogenic rib fractures and the associated risks of mortality. Eur. J. Trauma Emerg. Surg. 2022, 48, 231–241. [Google Scholar] [CrossRef]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Fokas, E.; Allgäuer, M.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.-L.; et al. Randomized Phase II Trial of Chemoradiotherapy Plus Induction or Consolidation Chemotherapy as Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer: CAO/ARO/AIO-12. J. Clin. Oncol. 2019, 37, 3212–3222. [Google Scholar] [CrossRef] [PubMed]
- Bosset, J.-F.; Calais, G.; Mineur, L.; Maingon, P.; Stojanovic-Rundic, S.; Bensadoun, R.-J.; Bardet, E.; Beny, A.; Ollier, J.-C.; Bolla, M.; et al. Fluorouracil-based adjuvant chemotherapy after preoperative chemoradiotherapy in rectal cancer: Long-term results of the EORTC 22921 randomised study. Lancet Oncol. 2014, 15, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Gérard, J.-P.; Conroy, T.; Bonnetain, F.; Bouché, O.; Chapet, O.; Closon-Dejardin, M.-T.; Untereiner, M.; LeDuc, B.; Francois, É.; Maurel, J.; et al. Preoperative Radiotherapy with or without Concurrent Fluorouracil and Leucovorin in T3-4 Rectal Cancers: Results of FFCD 9203. J. Clin. Oncol. 2006, 24, 4620–4625. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus Postoperative Chemoradiotherapy for Rectal Cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef]
- Fernandez, L.M.; Julião, G.P.S.; Renehan, A.G.; Beets, G.L.; Papoila, A.L.; Vailati, B.B.; Bahadoer, R.R.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Figueiredo, N.L.; et al. The Risk of Distant Metastases in Patients with Clinical Complete Response Managed by Watch and Wait after Neoadjuvant Therapy for Rectal Cancer: The Influence of Local Regrowth in the International Watch and Wait Database. Dis. Colon Rectum 2023, 66, 41–49. [Google Scholar] [CrossRef]
- Shi, D.D.; Mamon, H.J. Playing With Dynamite? A Cautious Assessment of TNT. J. Clin. Oncol. 2021, 39, 103–106. [Google Scholar] [CrossRef]
- Berglund, Å.; Cedermark, B.; Glimelius, B. Is it deleterious to delay the start of adjuvant chemotherapy in colon cancer stage III? Ann. Oncol. 2008, 19, 400–402. [Google Scholar] [CrossRef]
- Biagi, J.; Raphael, M.; Mackillop, W.; Kong, W.; King, W.; Booth, C. Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: A systematic review and meta-analysis. JAMA 2011, 305, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Guetz, G.D.; Nicolas, P.; Perret, G.-Y.; Morere, J.-F.; Uzzan, B. Does delaying adjuvant chemotherapy after curative surgery for colorectal cancer impair survival? A meta-analysis. Eur. J. Cancer 2010, 46, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Huang, X.-Z.; Song, Y.-X.; Sun, J.-X.; Chen, X.-W.; Sun, Y.; Jiang, Y.-M.; Wang, Z.-N. Impact of timing of adjuvant chemotherapy on survival in stage III colon cancer: A population-based study. BMC Cancer 2018, 18, 234. [Google Scholar] [CrossRef]
- Bahadoer, R.R.; Hospers, G.A.; Marijnen, C.A.; Peeters, K.C.; Putter, H.; Dijkstra, E.A.; Kranenbarg, E.M.-K.; Roodvoets, A.G.; van Etten, B.; Nilsson, P.J.; et al. Risk and location of distant metastases in patients with locally advanced rectal cancer after total neoadjuvant treatment or chemoradiotherapy in the RAPIDO trial. Eur. J. Cancer 2023, 185, 139–149. [Google Scholar] [CrossRef]
- Fokas, E.; Schlenska-Lange, A.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.-L. Chemoradiotherapy Plus Induction or Consolidation Chemotherapy as Total Neoadjuvant Therapy for Patients with Locally Advanced Rectal Cancer: Long-term Results of the CAO/ARO/AIO-12 Randomized Clinical Trial. JAMA Oncol. 2022, 8, e215445. [Google Scholar] [CrossRef]
- Rödel, C.; Graeven, U.; Fietkau, R.; Hohenberger, W.; Hothorn, T.; Arnold, D.; Hofheinz, R.-D.; Ghadimi, M.; Wolff, H.A.; Lang-Welzenbach, M.; et al. Oxaliplatin added to fluorouracil-based preoperative chemoradiotherapy and postoperative chemotherapy of locally advanced rectal cancer (the German CAO/ARO/AIO-04 study): Final results of the multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2015, 16, 979–989. [Google Scholar] [CrossRef]
- Gunderson, L.L.; Jessup, J.M.; Sargent, D.J.; Greene, F.L.; Stewart, A.K. Revised TN categorization for colon cancer based on national survival outcomes data. J. Clin. Oncol. 2009, 28, 264–271. [Google Scholar] [CrossRef]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; et al. Improved Overall Survival with Oxaliplatin, Fluorouracil, and Leucovorin As Adjuvant Treatment in Stage II or III Colon Cancer in the MOSAIC Trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef]
- Gunderson, L.L.; Sargent, D.J.; Tepper, J.E.; Wolmark, N.; O‘Connell, M.J.; Begovic, M.; Allmer, C.; Colangelo, L.; Smalley, S.R.; Haller, D.G.; et al. Impact of T and N Stage and Treatment on Survival and Relapse in Adjuvant Rectal Cancer. J. Clin. Oncol. 2004, 22, 1785–1796. [Google Scholar] [CrossRef]
- Roth, A.D.; Delorenzi, M.; Tejpar, S.; Yan, P.; Klingbiel, D.; Fiocca, R.; D’ario, G.; Cisar, L.; Labianca, R.; Cunningham, D.; et al. Integrated analysis of molecular and clinical prognostic factors in stage II/III colon cancer. J. Natl. Cancer Inst. 2012, 104, 1635–1646. [Google Scholar] [CrossRef]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Baxter, N.N.; Kennedy, E.B.; Bergsland, E.; Berlin, J.; George, T.J.; Gill, S.; Gold, P.J.; Hantel, A.; Jones, L.; Lieu, C.; et al. Adjuvant Therapy for Stage II Colon Cancer: ASCO Guideline Update. J. Clin. Oncol. 2022, 40, 892–910. [Google Scholar] [CrossRef]
- Benson, A.I.; Venook, A.; Al-Hawary, M. NCCN Guidelines Version 1. 2023 Colon Cancer. Available online: https://wwwnccnorg/guidelines/guidelines-detail?category=1&id=1428 (accessed on 9 May 2024).
- Lim, J.H.; Huh, J.W.; Lee, W.Y.; Yun, S.H.; Kim, H.C.; Cho, Y.B.; Park, Y.A.; Shin, J.K. Comparison of Long-Term Survival Outcomes of T4a and T4b Colorectal Cancer. Front. Oncol. 2022, 11, 780684. [Google Scholar] [CrossRef]
- Roh, M.S.; Colangelo, L.H.; O’Connell, M.J.; Yothers, G.; Deutsch, M.; Allegra, C.J.; Kahlenberg, M.S.; Baez-Diaz, L.; Ursiny, C.S.; Petrelli, N.J.; et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J. Clin. Oncol. 2009, 27, 5124–5130. [Google Scholar] [CrossRef] [PubMed]
- Habr-Gama; Juliao, A.; Pagin Gama-Rodrigues, G.; Joaquim, V.; BorbaOrtega, B.; Cinthia, F.; Araujo, L.M.; Eduardo Perez, S.; Oliva, R.B.T. Classification Predicts Early Tumor Regrowth after Non-operative Management in Distal Rectal Cancer after Extended Neoadjuvant Chemoradiation and Initial Complete Clinical Response. Dis. Colon Rectum 2017, 60, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Boffa, D.J.; Rosen, J.E.; Mallin, K.; Loomis, A.; Gay, G.; Palis, B.; Thoburn, K.; Gress, D.; McKellar, D.P.; Shulman, L.N.; et al. Using the National Cancer Database for Outcomes Research: A Review. JAMA Oncol. 2017, 3, 1722–1728. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | T1-3 N+, n (%) | T4 N+/−, n (%) | ||||
|---|---|---|---|---|---|---|
| Surgery | NOM | p-Value * | Surgery | NOM | p-Value * | |
| Total | 9315 | 868 | 2071 | 331 | ||
| Age, Median (Interquartile range) | 53 (47, 59) | 53 (46, 60) | 0.065 | 54 (47, 60) | 55 (47, 60) | 0.720 |
| Sex | ||||||
| Male | 5815 (62.4%) | 581 (66.9%) | 0.009 | 1177 (56.8%) | 200 (60.4%) | 0.220 |
| Female | 3500 (37.6%) | 287 (33.1%) | 894 (43.2%) | 131 (39.6%) | ||
| Race | ||||||
| Non-Hispanic White | 7226 (77.6%) | 659 (75.9%) | 0.220 | 1553 (75.0%) | 206 (62.2%) | <0.001 |
| Non-Hispanic Black | 664 (7.1%) | 59 (6.8%) | 154 (7.4%) | 51 (15.4%) | ||
| Asian | 429 (4.6%) | 35 (4.0%) | 93 (4.5%) | 20 (6.0%) | ||
| Hispanic | 690 (7.4%) | 79 (9.1%) | 214 (10.3%) | 49 (14.8%) | ||
| Others/Unknown | 306 (3.3%) | 36 (4.1%) | 57 (2.8%) | 5 (1.5%) | ||
| Charlson Comorbidity Index | ||||||
| 0 | 8118 (87.1%) | 766 (88.2%) | 0.350 | 1742 (84.1%) | 304 (91.8%) | <0.001 |
| 1 | 1197 (12.9%) | 102 (11.8%) | 329 (15.9%) | 27 (8.2%) | ||
| Radiation dose | ||||||
| ≤5040 | 8886 (95.4%) | 801 (92.3%) | <0.001 | 1943 (93.8%) | 290 (87.6%) | <0.001 |
| >5040 | 429 (4.6%) | 67 (7.7%) | 128 (6.2%) | 41 (12.4%) | ||
| Cancer Program Type | ||||||
| Community | 456 (4.9%) | 46 (5.3%) | <0.001 | 93 (4.5%) | 27 (8.2%) | 0.001 |
| Comprehensive Community | 2945 (31.6%) | 213 (24.5%) | 617 (29.8%) | 88 (26.6%) | ||
| Academic | 3145 (33.8%) | 411 (47.4%) | 783 (37.8%) | 129 (39.0%) | ||
| Integrated Network | 1834 (19.7%) | 122 (14.1%) | 396 (19.1%) | 45 (13.6%) | ||
| Unknown | 935 (10.0%) | 76 (8.8%) | 182 (8.8%) | 42 (12.7%) | ||
| Insurance Status | ||||||
| Uninsured | 452 (4.9%) | 34 (3.9%) | <0.001 | 174 (8.4%) | 41 (12.4%) | 0.005 |
| Private Insurance | 6955 (74.7%) | 605 (69.7%) | 1288 (62.2%) | 192 (58.0%) | ||
| Medicaid | 1014 (10.9%) | 102 (11.8%) | 370 (17.9%) | 62 (18.7%) | ||
| Medicare | 696 (7.5%) | 101 (11.6%) | 188 (9.1%) | 20 (6.0%) | ||
| Others/Unknown | 198 (2.1%) | 26 (3.0%) | 51 (2.5%) | 16 (4.8%) | ||
| Variable | T1-3 N+ | T4 N+/− | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | p-Value | 95% Confidence Interval | Hazard Ratio | p-Value | 95% Confidence Interval | |
| Age (18–59 = ref) | 1.01 | 0.005 | 1.00–1.01 | 1.01 | 0.104 | 1.00–1.02 |
| Sex (Male = ref) | ||||||
| Female | 0.69 | <0.001 | 0.62–0.77 | 0.84 | 0.041 | 0.72–0.99 |
| Race (Non-Hispanic White = ref) | ||||||
| Non-Hispanic Black | 1.28 | 0.005 | 1.08–1.52 | 1.19 | 0.182 | 0.92–1.54 |
| Asian | 1.01 | 0.912 | 0.80–1.28 | 0.74 | 0.184 | 0.48–1.15 |
| Hispanic | 0.96 | 0.649 | 0.79–1.16 | 0.81 | 0.147 | 0.61–1.08 |
| Others/Unknown | 1.18 | 0.176 | 0.93–1.51 | 0.78 | 0.370 | 0.45–1.35 |
| Charlson Comorbidity Index (0 = ref) | ||||||
| 1 | 1.43 | <0.001 | 1.26–1.62 | 1.13 | 0.289 | 0.90–1.40 |
| Surgery Status (Yes = ref) | ||||||
| Non-operative Management | 1.65 | <0.001 | 1.40–1.94 | 2.73 | <0.001 | 2.24–3.32 |
| Insurance Status (Private = ref) | - | |||||
| Uninsured | 1.77 | <0.001 | 1.47–2.13 | 1.32 | 0.038 | 1.01–1.72 |
| Medicaid | 1.60 | <0.001 | 1.38–1.86 | 1.25 | 0.040 | 1.01–1.56 |
| Medicare | 1.54 | <0.001 | 1.31–1.81 | 1.26 | 0.122 | 0.94–1.68 |
| Others/Unknown | 1.32 | 0.077 | 0.97–1.80 | 1.64 | 0.012 | 1.11–2.43 |
| Radiation Dose (≤5040 = ref) | ||||||
| >5040 | 1.13 | 0.259 | 0.91–1.39 | 1.07 | 0.680 | 0.79–1.44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kakish, H.; Ahmed, F.A.; Ocuin, L.M.; Miller-Ocuin, J.L.; Steinhagen, E.; Hoehn, R.S.; Mahipal, A.; Towe, C.W.; Chakrabarti, S. Outcome of Patients with Locally Advanced Rectal Cancer Pursuing Non-Surgical Strategy in National Cancer Database. Cancers 2024, 16, 2194. https://doi.org/10.3390/cancers16122194
Kakish H, Ahmed FA, Ocuin LM, Miller-Ocuin JL, Steinhagen E, Hoehn RS, Mahipal A, Towe CW, Chakrabarti S. Outcome of Patients with Locally Advanced Rectal Cancer Pursuing Non-Surgical Strategy in National Cancer Database. Cancers. 2024; 16(12):2194. https://doi.org/10.3390/cancers16122194
Chicago/Turabian StyleKakish, Hanna, Fasih A. Ahmed, Lee M. Ocuin, Jennifer L. Miller-Ocuin, Emily Steinhagen, Richard S. Hoehn, Amit Mahipal, Christopher W. Towe, and Sakti Chakrabarti. 2024. "Outcome of Patients with Locally Advanced Rectal Cancer Pursuing Non-Surgical Strategy in National Cancer Database" Cancers 16, no. 12: 2194. https://doi.org/10.3390/cancers16122194
APA StyleKakish, H., Ahmed, F. A., Ocuin, L. M., Miller-Ocuin, J. L., Steinhagen, E., Hoehn, R. S., Mahipal, A., Towe, C. W., & Chakrabarti, S. (2024). Outcome of Patients with Locally Advanced Rectal Cancer Pursuing Non-Surgical Strategy in National Cancer Database. Cancers, 16(12), 2194. https://doi.org/10.3390/cancers16122194