
Flow Cytometry Profiling of Plasmacytoid Dendritic Cell Neoplasms



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
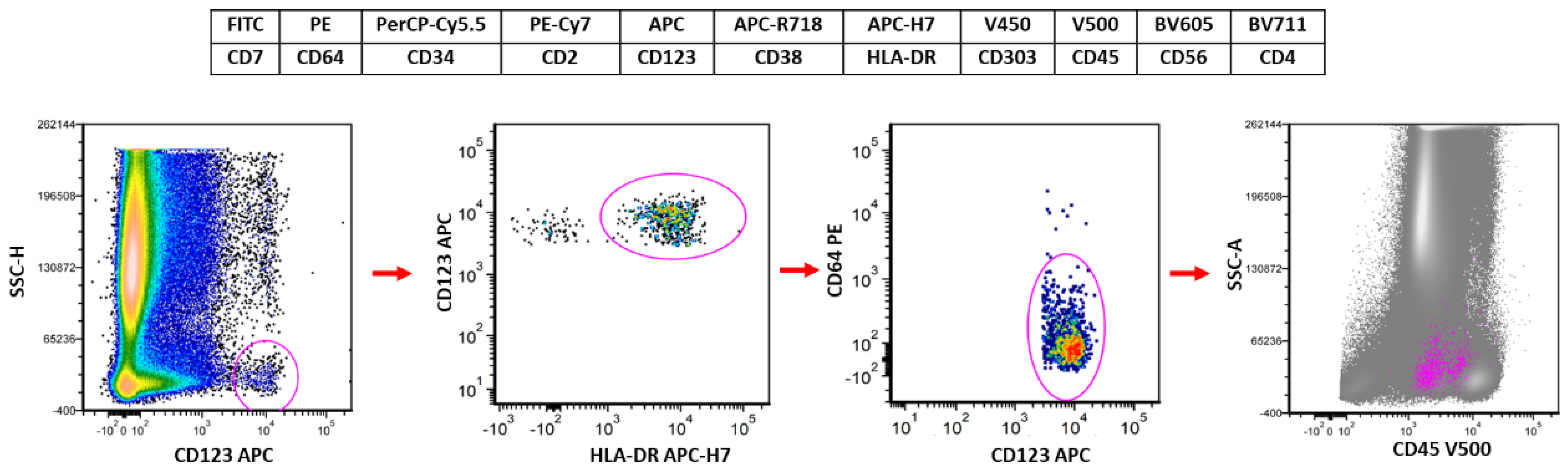
2. The Suggested Flow Cytometry Panel and Gating Strategy for Evaluation of pDCs
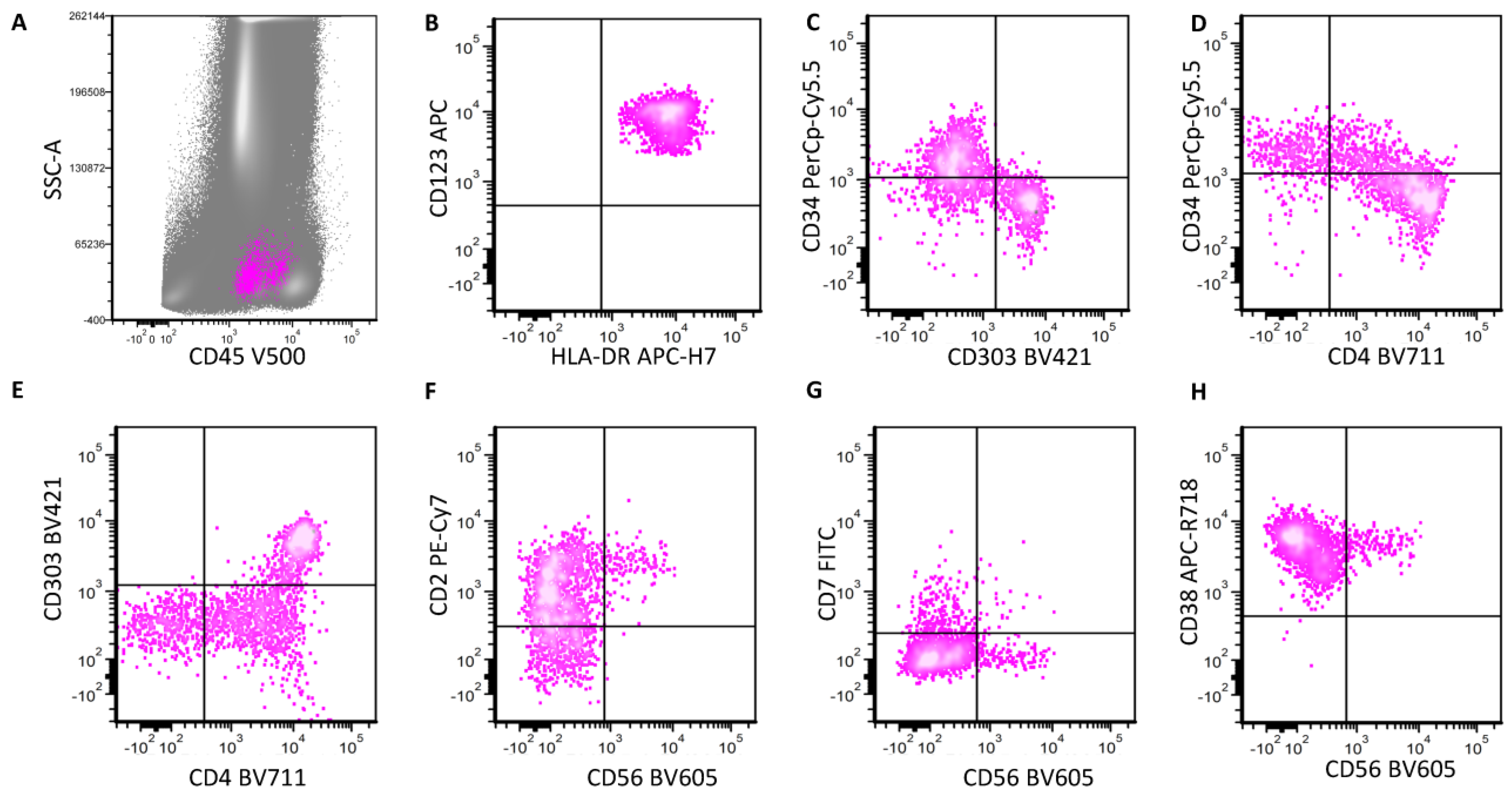
3. Normal and Neoplastic pDCs: Stages of Maturation
4. BPDCN
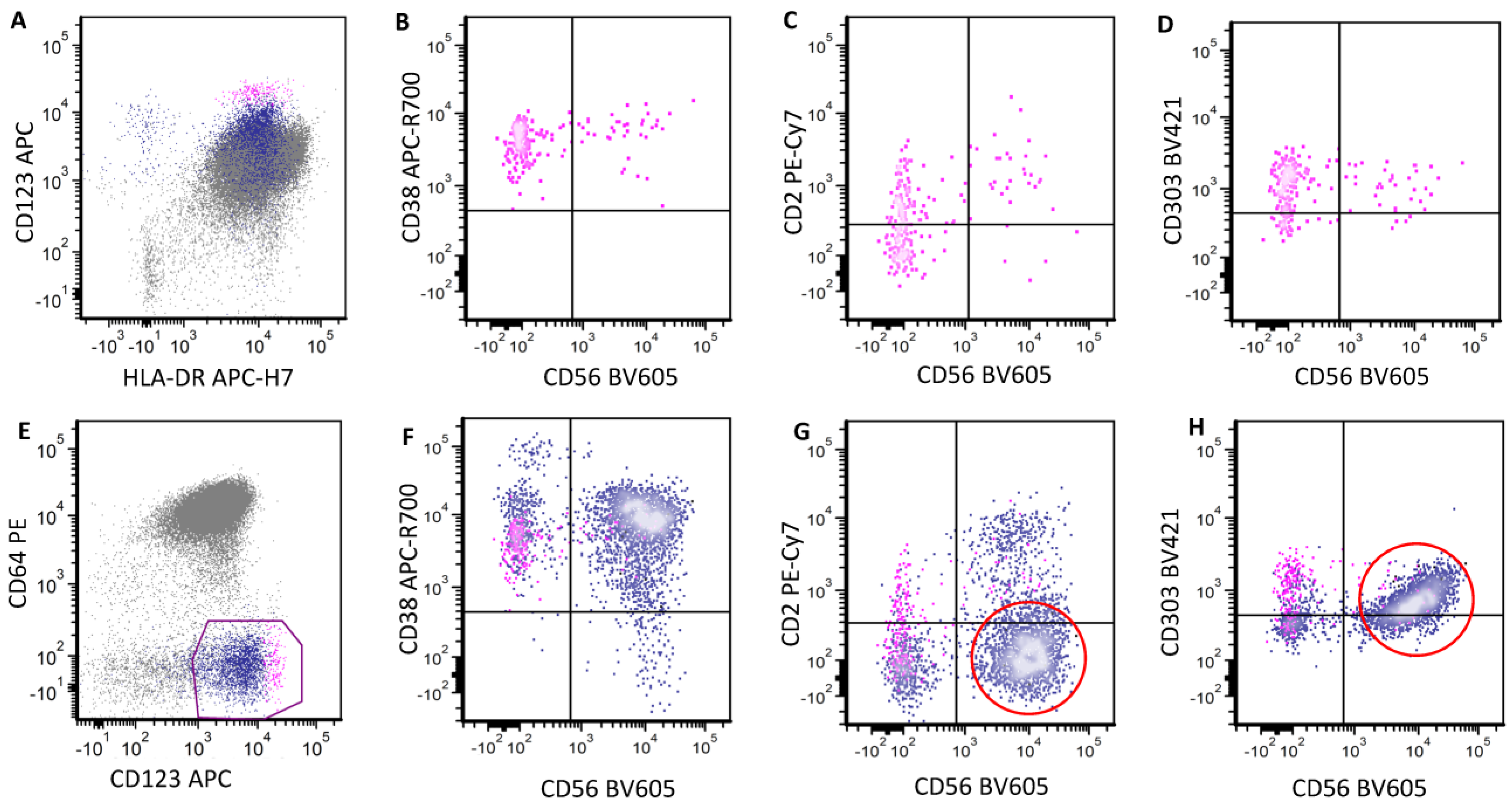
5. BPDCN Minimal Residual Disease
6. Mature Plasmacytoid Dendritic Cell Proliferation
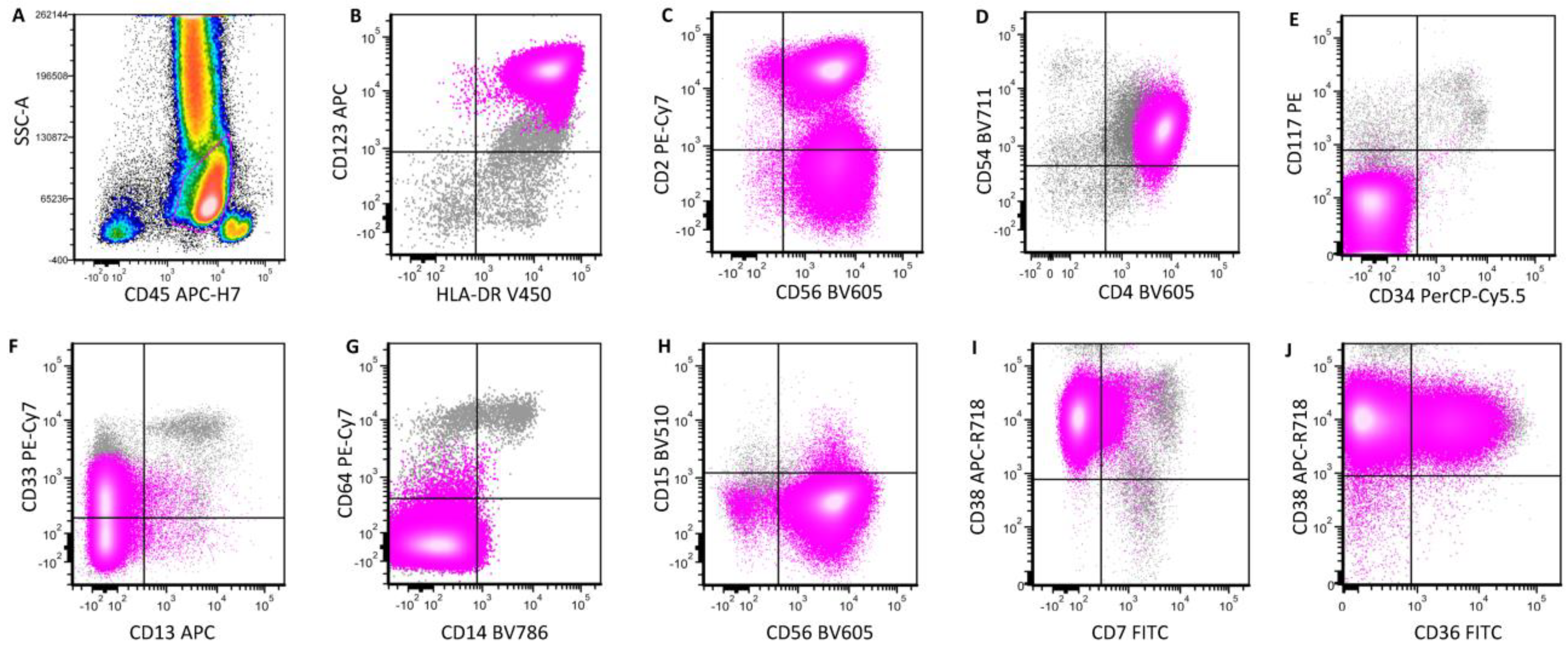
7. Myeloid Neoplasms with pDC Differentiation
8. AML and T-ALL with a pDC-like Phenotype
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lucas, N.; Duchmann, M.; Rameau, P.; Noël, F.; Michea, P.; Saada, V.; Kosmider, O.; Pierron, G.; Fernandez-Zapico, M.E.; Howard, M.T.; et al. Biology and prognostic impact of clonal plasmacytoid dendritic cells in chronic myelomonocytic leukemia. Leukemia 2019, 33, 2466–2480. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Khoury, J.D.; Miranda, R.N.; Jorgensen, J.L.; Xu, J.; Loghavi, S.; Li, S.; Pemmaraju, N.; Nguyen, T.; Medeiros, L.J.; et al. Immunophenotypic characterization of reactive and neoplastic plasmacytoid dendritic cells permits establishment of a 10-color flow cytometric panel for initial workup and residual disease evaluation of blastic plasmacytoid dendritic cell neoplasm. Haematologica 2021, 106, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Goldberg, A.D.; Famulare, C.A.; Devlin, S.M.; Nguyen, N.T.; Sim, S.; Kabel, C.C.; Patel, M.A.; McGovern, E.M.; Patel, A.; et al. Loss of plasmacytoid dendritic cell differentiation is highly predictive for post-induction measurable residual disease and inferior outcomes in acute myeloid leukemia. Haematologica 2019, 104, 1378–1387. [Google Scholar] [CrossRef] [PubMed]
- Reizis, B. Plasmacytoid Dendritic Cells: Development, Regulation, and Function. Immunity 2019, 50, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Murthy, H.S.; Zhang, M.-J.; Chen, K.; Ahmed, S.; Deotare, U.; Ganguly, S.; Kansagra, A.; Michelis, F.V.; Nishihori, T.; Patnaik, M.; et al. Allogeneic hematopoietic cell transplantation for blastic plasmacytoid dendritic cell neoplasm: A CIBMTR analysis. Blood Adv. 2023, 7, 7007–7016. [Google Scholar] [CrossRef] [PubMed]
- Collin, M.; Bigley, V. Human dendritic cell subsets: An update. Immunology 2018, 154, 3–20. [Google Scholar] [CrossRef]
- Martin-Martin, L.; Almeida, J.; Hernandez-Campo, P.M.; Sanchez, M.L.; Lecrevisse, Q.; Orfao, A. Immunophenotypical, morphologic, and functional characterization of maturation-associated plasmacytoid dendritic cell subsets in normal adult human bone marrow. Transfusion 2009, 49, 1692–1708. [Google Scholar] [CrossRef] [PubMed]
- El Hussein, S.; Wang, W. Plasmacytoid dendritic cells in the setting of myeloid neoplasms: Diagnostic guide to challenging pathologic presentations. Br. J. Haematol. 2023, 200, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, Y.; Chang, Y.; Yuan, X.; Hao, L.; Shi, H.; Lai, Y.; Huang, X.; Liu, Y. Myeloid Neoplasms with Elevated Plasmacytoid Dendritic Cell Differentiation Reflect the Maturation Process of Dendritic Cells. Cytom. A 2020, 97, 61–69. [Google Scholar] [CrossRef]
- Comeau, M.R.; Van der Vuurst de Vries, A.-R.; Maliszewski, C.R.; Galibert, L. CD123bright plasmacytoid predendritic cells: Progenitors undergoing cell fate conversion? J. Immunol. 2002, 169, 75–83. [Google Scholar] [CrossRef]
- Pemmaraju, N.; Kantarjian, H.M.; Khoury, J.D.; Loghavi, S.; O’Brien, S.; Cortes, J.E.; Garcia-Manero, G.; Jabbour, E.; Verstovsek, S.; Jain, N.; et al. Blastic Plasmacytoid Dendritic Cell Neoplasm (BPDCN) Commonly Presents in the Setting of Prior or Concomitant Hematologic Malignancies (PCHM): Patient Characteristics and Outcomes in the Rapidly Evolving Modern Targeted Therapy Era. Blood 2019, 134, 2723. [Google Scholar] [CrossRef]
- El Hussein, S.; Yabe, M.; Wang, W.; Pemmaraju, N.; Loghavi, S.; Jelloul, F.Z.; Fang, H.; Medeiros, L.J.; Burack, W.R.; Evans, A.G.; et al. Blastic plasmacytoid dendritic cell neoplasm (BPDCN) arising in the setting of polycythemia vera (PV): An illustration of the emerging role of flow cytometry analysis in monitoring progression of myeloproliferative neoplasms. EJHaem 2022, 3, 954–957. [Google Scholar] [CrossRef]
- Facchetti, F.; Cigognetti, M.; Fisogni, S.; Rossi, G.; Lonardi, S.; Vermi, W. Neoplasms derived from plasmacytoid dendritic cells. Mod. Pathol. 2016, 29, 98–111. [Google Scholar] [CrossRef]
- Vitte, F.; Fabiani, B.; Benet, C.; Dalac, S.; Balme, B.; Delattre, C.; Vergier, B.; Beylot-Barry, M.; Vignon-Pennamen, D.; Ortonne, N.; et al. Specific skin lesions in chronic myelomonocytic leukemia: A spectrum of myelomonocytic and dendritic cell proliferations: A study of 42 cases. Am. J. Surg. Pathol. 2012, 36, 1302–1316. [Google Scholar] [CrossRef]
- Zalmaï, L.; Viailly, P.-J.; Biichle, S.; Cheok, M.; Soret, L.; Angelot-Delettre, F.; Petrella, T.; Collonge-Rame, M.-A.; Seilles, E.; Geffroy, S.; et al. Plasmacytoid dendritic cells proliferation associated with acute myeloid leukemia: Phenotype profile and mutation landscape. Haematologica 2021, 106, 3056–3066. [Google Scholar] [CrossRef]
- Hamadeh, F.; Awadallah, A.; Meyerson, H.J.; Beck, R.C. Flow Cytometry Identifies a Spectrum of Maturation in Myeloid Neoplasms Having Plasmacytoid Dendritic Cell Differentiation. Cytom. B Clin. Cytom. 2020, 98, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Vermi, W.; Facchetti, F.; Rosati, S.; Vergoni, F.; Rossi, E.; Festa, S.; Remotti, D.; Grigolato, P.; Massarelli, G.; Frizzera, G. Nodal and extranodal tumor-forming accumulation of plasmacytoid monocytes/interferon-producing cells associated with myeloid disorders. Am. J. Surg. Pathol. 2004, 28, 585–595. [Google Scholar] [CrossRef]
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703–1719. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.M.; Munir, A.; Raval, M.; Mehdi, S. Blastic plasmacytoid dendritic cell neoplasm in the background of myeloproliferative disorder and chronic lymphocytic leukaemia. BMJ Case Rep. 2019, 12, e230332. [Google Scholar] [CrossRef]
- Osaki, Y.; Yokohama, A.; Saito, A.; Tahara, K.; Yanagisawa, K.; Ogawa, Y.; Ishizaki, T.; Mitsui, T.; Koiso, H.; Takizawa, M.; et al. Characterization of CD56+ dendritic-like cells: A normal counterpart of blastic plasmacytoid dendritic cell neoplasm? PLoS ONE 2013, 8, e81722. [Google Scholar] [CrossRef]
- Petrella, T.; Comeau, M.R.; Maynadie, M.; Couillault, G.; De Muret, A.; Maliszewski, C.R.; Dalac, S.; Durlach, A.; Galibert, L. ‘Agranular CD4+ CD56+ hematodermic neoplasm’ (blastic NK-cell lymphoma) originates from a population of CD56+ precursor cells related to plasmacytoid monocytes. Am. J. Surg. Pathol. 2002, 26, 852–862. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.R.; Konopleva, M.; Khoury, J.D.; Pemmaraju, N. Novel Therapeutic Approaches in Blastic Plasmacytoid Dendritic Cell Neoplasm (BPDCN): Era of Targeted Therapy. Clin. Lymphoma Myeloma Leuk. 2021, 21, 734–740. [Google Scholar] [CrossRef]
- Machan, S.; Alonso-Dominguez, J.M.; Sanchez Garcia, F.J.; Nieves Salgado, R.; Soto, C.; Castro, Y.; Pajares, R.; Manso, R.; Santonja, C.; Serrano Del Castillo, C.; et al. Plasmacytoid Dendritic Cell Dermatosis Associated to Myeloproliferative/Myelodysplastic Neoplasms. Am. J. Surg. Pathol. 2022, 46, 1623–1632. [Google Scholar] [CrossRef] [PubMed]
- Dargent, J.-L.; Henne, S.; Pranger, D.; Balzarini, P.; Sartenaer, D.; Bulliard, G.; Rack, K.; Facchetti, F. Tumor-forming plasmacytoid dendritic cells associated with myeloid neoplasms. Report of a peculiar case with histopathologic features masquerading as lupus erythematosus. J. Cutan. Pathol. 2016, 43, 280–286. [Google Scholar] [CrossRef]
- Tzankov, A.; Hebeda, K.; Kremer, M.; Leguit, R.; Orazi, A.; van der Walt, J.; Gianelli, U. Plasmacytoid dendritic cell proliferations and neoplasms involving the bone marrow: Summary of the workshop cases submitted to the 18th Meeting of the European Association for Haematopathology (EAHP) organized by the European Bone Marrow Working Group, Basel 2016. Ann. Hematol. 2017, 96, 765–777. [Google Scholar] [CrossRef]
- Chan, A.; Liu, Y.; Devlin, S.; Gao, Q.; Baik, J.; Sigler, A.; Londono, D.; Arcila, M.; Levine, R.; Dogan, A.; et al. Reduced Plasmacytoid Dendritic Cell Output Is Associated With High Risk in Low-grade Myelodysplastic Syndrome. Hemasphere 2022, 6, e685. [Google Scholar] [CrossRef]
- Ma, L.; Delforge, M.; van Duppen, V.; Verhoef, G.; Emanuel, B.; Boogaerts, M.; Hagemeijer, A.; Vandenberghe, P. Circulating myeloid and lymphoid precursor dendritic cells are clonally involved in myelodysplastic syndromes. Leukemia 2004, 18, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Marafioti, T.; Paterson, J.C.; Ballabio, E.; Reichard, K.K.; Tedoldi, S.; Hollowood, K.; Dictor, M.; Hansmann, M.-L.; Pileri, S.A.; Dyer, M.J.; et al. Novel markers of normal and neoplastic human plasmacytoid dendritic cells. Blood 2008, 111, 3778–3792. [Google Scholar] [CrossRef]
- Xiao, W.; Chan, A.; Waarts, M.R.; Mishra, T.; Liu, Y.; Cai, S.F.; Yao, J.; Gao, Q.; Bowman, R.L.; Koche, R.P.; et al. Plasmacytoid dendritic cell expansion defines a distinct subset of RUNX1-mutated acute myeloid leukemia. Blood 2021, 137, 1377–1391. [Google Scholar] [CrossRef]
- Wang, W.; Xu, J.; Khoury, J.D.; Pemmaraju, N.; Fang, H.; Miranda, R.N.; Yin, C.C.; Hussein, S.E.; Jia, F.; Tang, Z.; et al. Immunophenotypic and Molecular Features of Acute Myeloid Leukemia with Plasmacytoid Dendritic Cell Differentiation Are Distinct from Blastic Plasmacytoid Dendritic Cell Neoplasm. Cancers 2022, 14, 3375. [Google Scholar] [CrossRef]
- Wang, W.; Thakral, B. CD123+CD4+CD56+ neoplasm: Blastic plasmacytoid dendritic cell neoplasm or acute myeloid leukemia? Blood 2020, 136, 1565. [Google Scholar] [CrossRef] [PubMed]
- Germans, S.K.; Chen, W. The great mimicker: Leukemic presentation of blastic plasmacytoid dendritic cell neoplasm with PVT1::SUPT3H fusion. EJHaem 2024, 5, 280. [Google Scholar] [CrossRef] [PubMed]
- Cuglievan, B.; Connors, J.; He, J.; Khazal, S.; Yedururi, S.; Dai, J.; Garces, S.; Quesada, A.E.; Roth, M.; Garcia, M.; et al. Blastic plasmacytoid dendritic cell neoplasm: A comprehensive review in pediatrics, adolescents, and young adults (AYA) and an update of novel therapies. Leukemia 2023, 37, 1767–1778. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Valentini, C.G.; Pulsoni, A.; Fisogni, S.; Carluccio, P.; Mannelli, F.; Lunghi, M.; Pica, G.; Onida, F.; Cattaneo, C.; et al. Blastic plasmacytoid dendritic cell neoplasm with leukemic presentation: An Italian multicenter study. Haematologica 2013, 98, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cao, J.; Hong, X. Blastic plasmacytoid dendritic cell neoplasm without cutaneous lesion at presentation: Case report and literature review. Acta Haematol. 2012, 127, 124–127. [Google Scholar] [CrossRef]
- Rauh, M.J.; Rahman, F.; Good, D.; Silverman, J.; Brennan, M.K.; Dimov, N.; Liesveld, J.; Ryan, D.H.; Burack, W.R.; Bennett, J.M. Blastic plasmacytoid dendritic cell neoplasm with leukemic presentation, lacking cutaneous involvement: Case series and literature review. Leuk. Res. 2012, 36, 81–86. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Hussein, S.; Wang, W. Flow Cytometry Profiling of Plasmacytoid Dendritic Cell Neoplasms. Cancers 2024, 16, 2118. https://doi.org/10.3390/cancers16112118
El Hussein S, Wang W. Flow Cytometry Profiling of Plasmacytoid Dendritic Cell Neoplasms. Cancers. 2024; 16(11):2118. https://doi.org/10.3390/cancers16112118
Chicago/Turabian StyleEl Hussein, Siba, and Wei Wang. 2024. "Flow Cytometry Profiling of Plasmacytoid Dendritic Cell Neoplasms" Cancers 16, no. 11: 2118. https://doi.org/10.3390/cancers16112118
APA StyleEl Hussein, S., & Wang, W. (2024). Flow Cytometry Profiling of Plasmacytoid Dendritic Cell Neoplasms. Cancers, 16(11), 2118. https://doi.org/10.3390/cancers16112118