Fertility-Preserving Treatments and Patient- and Parental Satisfaction on Fertility Counseling in a Cohort of Newly Diagnosed Boys and Girls with Childhood Hodgkin Lymphoma

 , , , , , ,
, , , , , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
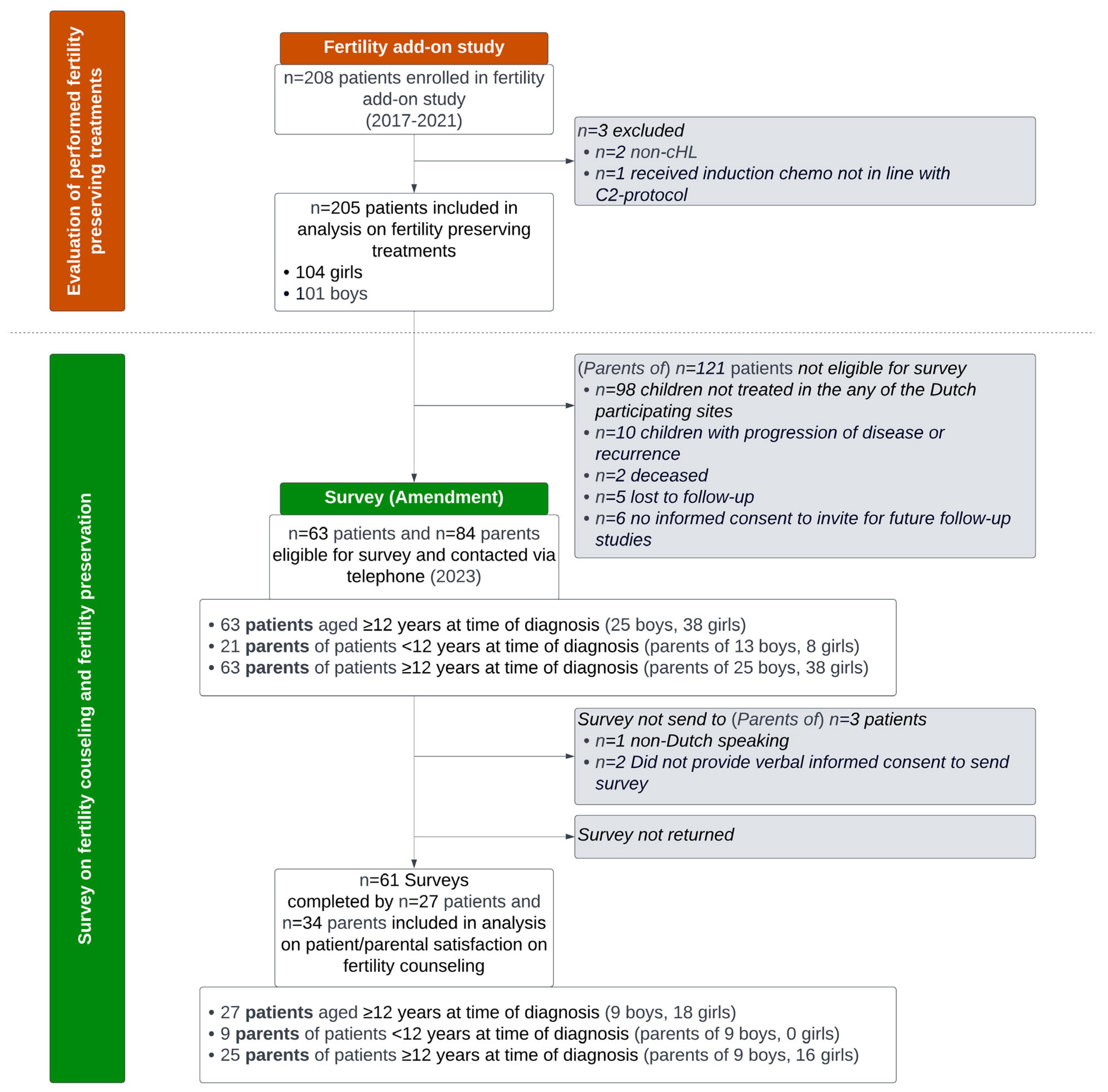
2.1. Study Design and Study Population
2.2. Data Collection and Measurements
2.2.1. Fertility-Preserving Treatments in the Fertility Add-On Study Cohort
2.2.2. Fertility Questionnaire
2.2.3. Other Patient Characteristics, cHL Treatment Data, and Estimated Risk of Infertility
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Fertility Preservation in Boys
3.3. Fertility Preservation in Girls
3.4. Fertility Counseling
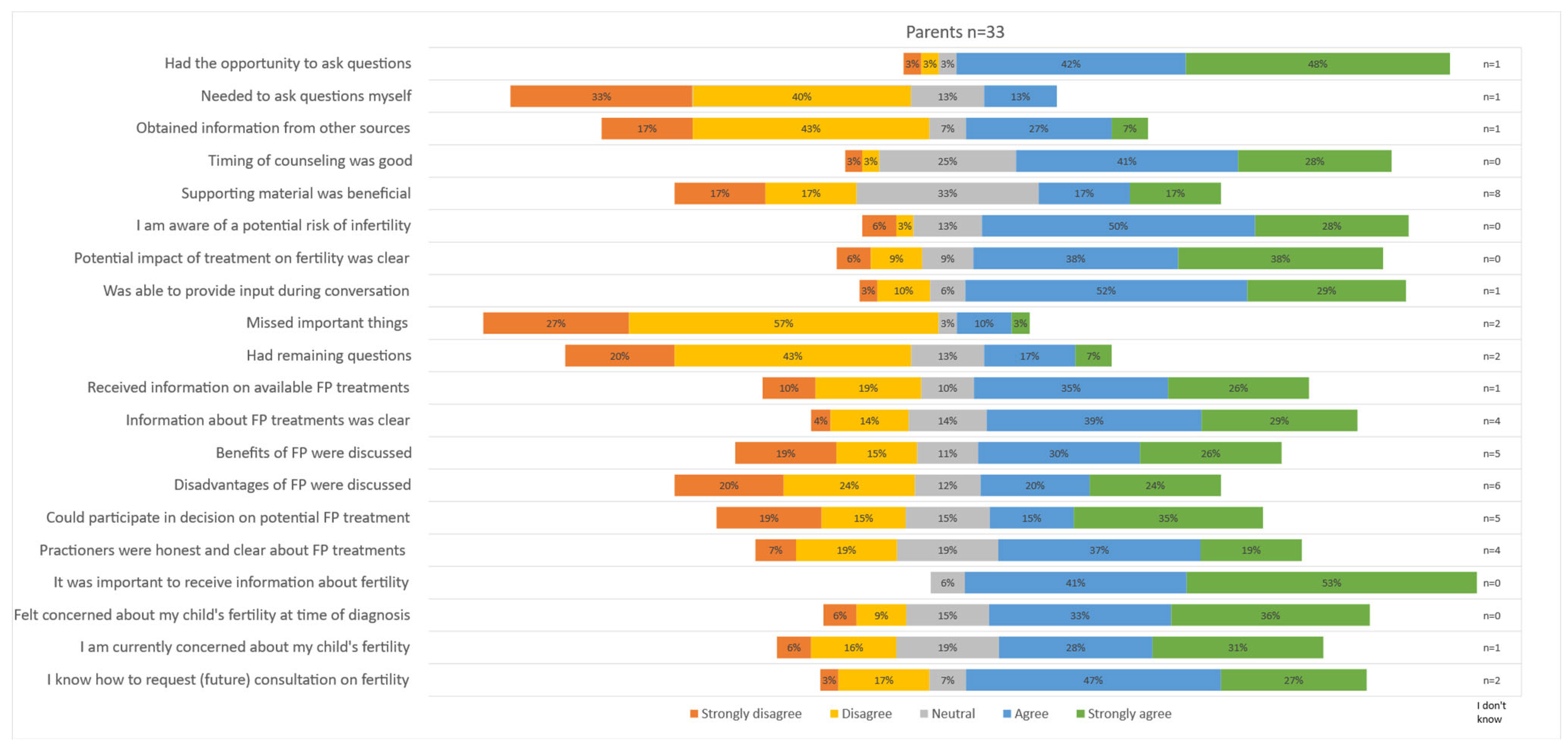
3.4.1. Parental Satisfaction on Offered Counseling
3.4.2. Patient Satisfaction on Offered Counseling
3.4.3. Parental Satisfaction on Decision about Fertility Preservation
4. Discussion
4.1. Strengths and Limitations
4.2. Summarizing Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mauz-Körholz, C.; Landman-Parker, J.; Balwierz, W.; Ammann, R.A.; Anderson, R.A.; Attarbaschi, A.; Bartelt, J.M.; Beishuizen, A.; Boudjemaa, S.; Cepelova, M.; et al. Response-Adapted Omission of Radiotherapy and Comparison of Consolidation Chemotherapy in Children and Adolescents with Intermediate-Stage and Advanced-Stage Classical Hodgkin Lymphoma (EuroNet-PHL-C1): A Titration Study with an Open-Label, Embedded, Multinational, Non-Inferiority, Randomised Controlled Trial. Lancet Oncol. 2022, 23, 125–137. [Google Scholar] [CrossRef]
- Flerlage, J.E.; Hiniker, S.M.; Armenian, S.; Benya, E.C.; Bobbey, A.J.; Chang, V.; Cooper, S.; Coulter, D.W.; Cuglievan, B.; Hoppe, B.S.; et al. Pediatric Hodgkin Lymphoma, Version 3.2021. JNCCN J. Natl. Compr. Cancer Netw. 2021, 19, 733–754. [Google Scholar] [CrossRef]
- Antal, Z.; Sklar, C.A. Gonadal Function and Fertility Among Survivors of Childhood Cancer. Endocrinol. Metab. Clin. N. Am. 2015, 44, 739–749. [Google Scholar] [CrossRef]
- Reinmuth, S.; Hohmann, C.; Rendtorff, R.; Balcerek, M.; Holzhausen, S.; Müller, A.; Henze, G.; Keil, T.; Borgmann-Staudt, A. Impact of Chemotherapy and Radiotherapy in Childhood on Fertility in Adulthood: The FeCt—Survey of Childhood Cancer Survivors in Germany. J. Cancer Res. Clin. Oncol. 2013, 139, 2071–2078. [Google Scholar] [CrossRef]
- van Kalsbeek, R.J.; Hudson, M.M.; Mulder, R.L.; Ehrhardt, M.; Green, D.M.; Mulrooney, D.A.; Hakkert, J.; den Hartogh, J.; Nijenhuis, A.; van Santen, H.M.; et al. A Joint International Consensus Statement for Measuring Quality of Survival for Patients with Childhood Cancer. Nat. Med. 2023, 29, 1340–1348. [Google Scholar] [CrossRef]
- El Alaoui-Lasmaili, K.; Nguyen-Thi, P.L.; Demogeot, N.; Lighezzolo-Alnot, J.; Gross, M.J.; Mansuy, L.; Chastagner, P.; Koscinski, I. Fertility Discussions and Concerns in Childhood Cancer Survivors, a Systematic Review for Updated Practice. Cancer Med. 2023, 12, 6023–6039. [Google Scholar] [CrossRef]
- Mulder, R.L.; Font-Gonzalez, A.; Green, D.M.; Loeffen, E.A.H.; Hudson, M.M.; Loonen, J.; Yu, R.; Ginsberg, J.P.; Mitchell, R.T.; Byrne, J.; et al. Fertility Preservation for Male Patients with Childhood, Adolescent, and Young Adult Cancer: Recommendations from the PanCareLIFE Consortium and the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2021, 22, e57–e67. [Google Scholar] [CrossRef]
- Hussein, A.A.; Tran, N.D.; Smith, J.F. Fertility Preservation for Boys and Adolescents Facing Sterilizing Medical Therapy. Transl. Androl. Urol. 2014, 3, 382–390. [Google Scholar]
- Kenney, L.B.; Antal, Z.; Ginsberg, J.P.; Hoppe, B.S.; Bober, S.L.; Yu, R.N.; Constine, L.S.; van Santen, H.M.; Skinner, R.; Green, D.M. Improving Male Reproductive Health after Childhood, Adolescent, and Young Adult Cancer: Progress and Future Directions for Survivorship Research. J. Clin. Oncol. 2018, 36, 2160–2168. [Google Scholar] [CrossRef]
- Mulder, R.L.; Font-Gonzalez, A.; Hudson, M.M.; van Santen, H.M.; Loeffen, E.A.H.; Burns, K.C.; Quinn, G.P.; van Dulmen-den Broeder, E.; Byrne, J.; Haupt, R.; et al. Fertility Preservation for Female Patients with Childhood, Adolescent, and Young Adult Cancer: Recommendations from the PanCareLIFE Consortium and the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2021, 22, e45–e56. [Google Scholar] [CrossRef]
- Senra, J.C.; Roque, M.; Talim, M.C.T.; Reis, F.M.; Tavares, R.L.C. Gonadotropin-Releasing Hormone Agonists for Ovarian Protection during Cancer Chemotherapy: Systematic Review and Meta-Analysis. Ultrasound Obs. Gynecol. 2018, 51, 77–86. [Google Scholar] [CrossRef]
- Lambertini, M.; Moore, H.C.F.; Leonard, R.C.F.; Loibl, S.; Munster, P.; Bruzzone, M.; Boni, L.; Unger, J.M.; Anderson, R.A.; Mehta, K.; et al. Gonadotropin-Releasing Hormone Agonists during Chemotherapy for Preservation of Ovarian Function and Fertility in Premenopausal Patients with Early Breast Cancer: A Systematic Review and Meta-Analysis of Individual Patient–Level Data. J. Clin. Oncol. 2018, 36, 1981–1990. [Google Scholar] [CrossRef]
- Deshpande, N.A.; Braun, I.M.; Meyer, F.L. Impact of Fertility Preservation Counseling and Treatment on Psychological Outcomes among Women with Cancer: A Systematic Review. Cancer 2015, 121, 3938–3947. [Google Scholar] [CrossRef]
- Skaczkowski, G.; White, V.; Thompson, K.; Bibby, H.; Coory, M.; Orme, L.M.; Conyers, R.; Phillips, M.B.; Osborn, M.; Harrup, R.; et al. Factors Influencing the Provision of Fertility Counseling and Impact on Quality of Life in Adolescents and Young Adults with Cancer. J. Psychosoc. Oncol. 2018, 36, 484–502. [Google Scholar] [CrossRef]
- Letourneau, J.M.; Ebbel, E.E.; Katz, P.P.; Katz, A.; Ai, W.Z.; Chien, A.J.; Melisko, M.E.; Cedars, M.I.; Rosen, M.P. Pretreatment Fertility Counseling and Fertility Preservation Improve Quality of Life in Reproductive Age Women with Cancer. Cancer 2012, 118, 1710–1717. [Google Scholar] [CrossRef]
- Kremer, L.C.; Mulder, R.L.; Oeffinger, K.C.; Bhatia, S.; Landier, W.; Levitt, G.; Constine, L.S.; Wallace, W.H.; Caron, H.N.; Armenian, S.H.; et al. A Worldwide Collaboration to Harmonize Guidelines for the Long-Term Follow-up of Childhood and Young Adult Cancer Survivors: A Report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Pediatr. Blood Cancer 2013, 60, 543–549. [Google Scholar] [CrossRef]
- Byrne, J.; Grabow, D.; Campbell, H.; O’Brien, K.; Bielack, S.; am Zehnhoff-Dinnesen, A.; Calaminus, G.; Kremer, L.; Langer, T.; van den Heuvel-Eibrink, M.M.; et al. PanCareLIFE: The Scientific Basis for a European Project to Improve Long-Term Care Regarding Fertility, Ototoxicity and Health-Related Quality of Life after Cancer Occurring among Children and Adolescents. Eur. J. Cancer 2018, 103, 227–237. [Google Scholar] [CrossRef]
- European Network-Paediatric Hodgkin Lymphoma Study Group (EuroNet-PHL). Second International Inter-Group Study for Classical Hodgkin Lymphoma in Children and Adolescent: EuroNet-PHL-C2; 2015. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT02684708 (accessed on 24 April 2024).
- van der Perk, M.E.M.; Stukaitė-Ruibienė, E.; Bumbulienė, Ž.; Vaitkevičienė, G.E.; Bos, A.M.E.; van den Heuvel-Eibrink, M.M.; Rascon, J. Development of a Questionnaire to Evaluate Female Fertility Care in Pediatric Oncology, a TREL Initiative. BMC Cancer 2022, 22, 450. [Google Scholar] [CrossRef]
- Brehaut, J.C.; O’Connor, A.M.; Wood, T.J.; Hack, T.F.; Siminoff, L.; Gordon, E.; Feldman-Stewart, D. Validation of a Decision Regret Scale. Med. Decis. Mak. 2003, 23, 281–292. [Google Scholar] [CrossRef]
- O’Connor, A.M. Validation of a Decisional Conflict Scale. Med. Decis. Mak. 1995, 15, 25–30. [Google Scholar] [CrossRef]
- Garvelink, M.M.; ter Kuile, M.M.; Louwé, L.A.; Hilders, C.G.; Stiggelbout, A.M. Validation of a Dutch Version of the Reproductive Concerns Scale (RCS) in Three Populations of Women. Health Care Women Int. 2015, 36, 1143–1159. [Google Scholar] [CrossRef]
- Green, D.M.; Nolan, V.G.; Goodman, P.J.; Whitton, J.A.; Srivastava, D.K.; Leisenring, W.M.; Neglia, J.P.; Sklar, C.A.; Kaste, S.C.; Hudson, M.M.; et al. The Cyclophosphamide Equivalent Dose as an Approach for Quantifying Alkylating Agent Exposure: A Report from the Childhood Cancer Survivor Study. Pediatr. Blood Cancer 2014, 61, 53–67. [Google Scholar] [CrossRef]
- Romao, R.L.P.; Lorenzo, A.J. Fertility Preservation Options for Children and Adolescents with Cancer. Can. Urol. Assoc. J. 2017, 11, S97–S102. [Google Scholar] [CrossRef]
- Drechsel, K.; Pilon, M.; Stoutjesdijk, F.; Meivis, S.; Schoonmade, L.J.; Wallace, W.; van Dulmen-den Broeder, E.; Beishuizen, A.; Kaspers, G.; Broer, S.; et al. Reproductive Ability in Survivors of Childhood, Adolescent and Young Adult Hodgkin Lymphoma: A Review. Hum. Reprod. Update 2023, 29, 486–517. [Google Scholar] [CrossRef]
- Muller, I.; Oude Ophuis, R.J.A.; Broekmans, F.J.M.; Lock, T.M.T.W. Semen Cryopreservation and Usage Rate for Assisted Reproductive Technology in 898 Men with Cancer. Reprod. Biomed. Online 2016, 32, 147–153. [Google Scholar] [CrossRef]
- Wnuk, K.; Świtalski, J.; Miazga, W.; Tatara, T.; Religioni, U.; Olszewski, P.; Augustynowicz, A. The Usage of Cryopreserved Reproductive Material in Cancer Patients Undergoing Fertility Preservation Procedures. Cancers 2023, 15, 5348. [Google Scholar] [CrossRef]
- Laven, J.S.E.; Louwers, Y.V. Can We Predict Menopause and Premature Ovarian Insufficiency? Fertil. Steril. 2024, 121, 737–741. [Google Scholar] [CrossRef]
- Stacey, D.; Lewis, K.B.; Smith, M.; Carley, M.; Volk, R.; Douglas, E.E.; Pacheco-Brousseau, L.; Finderup, J.; Gunderson, J.; Barry, M.J.; et al. Decision Aids for People Facing Health Treatment or Screening Decisions. Cochrane Database Syst. Rev. 2024, 2024, CD001431. [Google Scholar] [CrossRef]
- Jones, G.L.; Moss, R.H.; Darby, F.; Mahmoodi, N.; Phillips, B.; Hughes, J.; Vogt, K.S.; Greenfield, D.M.; Brauten-Smith, G.; Gath, J.; et al. Cancer, Fertility and Me: Developing and Testing a Novel Fertility Preservation Patient Decision Aid to Support Women at Risk of Losing Their Fertility Because of Cancer Treatment. Front. Oncol. 2022, 12, 896939. [Google Scholar] [CrossRef] [PubMed]
- Mulder, R.L.; Font-Gonzalez, A.; van Dulmen-den Broeder, E.; Quinn, G.P.; Ginsberg, J.P.; Loeffen, E.A.H.; Hudson, M.M.; Burns, K.C.; Van Santen, H.M.; Berger, C.; et al. Communication and Ethical Considerations for Fertility Preservation for Patients with Childhood, Adolescent, and Young Adult Cancer: Recommendations from the PanCareLIFE Consortium and the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2021, 22, e68–e80. [Google Scholar] [PubMed]
- Quinn, G.P.; Vadaparampil, S.T. Fertility Preservation and Adolescent/Young Adult Cancer Patients: Physician Communication Challenges. J. Adolesc. Health 2009, 44, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Van Den Berg, M.; Baysal, Ö.; Nelen, W.L.D.M.; Braat, D.D.M.; Beerendonk, C.C.M.; Hermens, R.P.M.G. Professionals’ Barriers in Female Oncofertility Care and Strategies for Improvement. Hum. Reprod. 2019, 34, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- van der Perk, M.E.; van der Kooi, A.-L.L.F.; van de Wetering, M.D.; IJgosse, I.M.; van Dulmen-Den Broeder, E.; Broer, S.L.; Klijn, A.J.; Versluys, A.B.; Arends, B.; Oude Ophuis, R.J.A.; et al. Oncofertility Care for Newly Diagnosed Girls with Cancer in a National Pediatric Oncology Setting, the First Full Year Experience from the Princess Máxima Center, the PEARL Study. PLoS ONE 2021, 16, e0246344. [Google Scholar] [CrossRef] [PubMed]
- Benedict, C.; Thom, B.; Friedman, D.N.; Pottenger, E.; Raghunathan, N.; Kelvin, J.F. Fertility Information Needs and Concerns Post-Treatment Contribute to Lowered Quality of Life among Young Adult Female Cancer Survivors. Support Care Cancer 2018, 26, 2209–2215. [Google Scholar] [CrossRef]
- Yeomanson, D.J.; Morgan, S.; Pacey, A.A. Discussing Fertility Preservation at the Time of Cancer Diagnosis: Dissatisfaction of Young Females. Pediatr. Blood Cancer 2013, 60, 1996–2000. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients Included in the Fertility Add-On Study | Surveys Completed by Parents (n = 34) | Surveys Completed by Patients (n = 27) | ||||
|---|---|---|---|---|---|---|
| Girls (n = 104) | Boys (n = 101) | Parents of Girls (n = 16) | Parents of Boys (n = 18) | Girls (n = 18) | Boys (n = 9) | |
| HL diagnosis | ||||||
| Age at diagnosis (in years), median (IQR) | 15.6 [13.7;17.1] | 14.8 [11.5;16.1] | 15.9 [13.7;17.1] | 12.0 [9.3;17.1] | 15.9 [13.8;17.3] | 15.6 [13.6;17.0] |
| Post-pubertal at diagnosis a | 99 (95.2%) | 73 (72.3%) | 16 (100%) | 9 (50.0%) | 18 (100.0%) | 8 (88.9%) |
| Assigned Treatment level | ||||||
| - TL1 (early-stage disease) | 18 (17.3%) | 14 (13.9%) | 3 (18.8%) | 1 (95.6%) | 3 (16.7%) | 0 (0.0%) |
| - TL2 (intermediate-stage disease) | 50 (48.1%) | 36 (35.6%) | 7 (43.8%) | 3 (16.7%) | 8 (44.4%) | 1 (11.1%) |
| - TL3 (advanced-stage disease) | 36 (34.6%) | 51 (50.5%) | 6 (37.5%) | 14 (77.8%) | 7 (38.9%) | 8 (88.9%) |
| Anticipated high risk of infertility based on CED score of planned chemotherapy | 0 (0.0%) | 51 (50.5%) | 0 (0.0%) | 14 (77.8%) | 0 (0.0%) | 8 (88.9%) |
| Involved tumor sites in abdominal b (girls) or inguinal (boys) region | 28 (26.9%) | 5 (5.0%) | 7 (43.8%) | 2 (11.1%) | 8 (44.4%) | 1 (11.1%) |
| Received HL treatment | ||||||
| Chemotherapy | ||||||
| - 2xOEPA (CED score 0 mg/m2) | 2 (1.9%) | 4 (4.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| - 2xOEPA-1xCOPDAC-28 (CED score 1000 mg/m2) | 16 (15.4%) | 10 (9.9%) | 3 (18.8%) | 1 (5.6%) | 3 (16.7%) | 0 (0.0%) |
| - 2xOEPA-2xCOPDAC-28 (CED score 2000 mg/m2) | 35 (33.7%) | 20 (19.8%) | 5 (31.3%0 | 3 (16.7%) | 6 (33.3%) | 1 (11.1%) |
| - 2xOEPA-2xDECOPDAC-21 (CED score 2500 mg/m2) | 15 (14.4%) | 16 (15.8%) | 2 (12.5%) | 0 (0.0%) | 2 (11.1%) | 0 (0.0%) |
| - 2xOEPA-4xCOPDAC-28 (CED score 4000 mg/m2) | 22 (21.2%) | 28 (27.7%) | 3 (18.8%) | 7 (38.9%) | 4 (22.2%) | 5 (55.6%) |
| - 2xOEPA-4xDECOPDAC-21 (CED score 5000 mg/m2) | 14 (13.5%) | 23 (22.8%) | 3 (18.8%) | 7 (38.9%) | 3 (16.7%) | 3 (33.3%) |
| Radiotherapy | 21 (20.2%) | 25 (24.8%) | 5 (31.3%) | 4 (22.2%) | 5 (27.8%) | 2 (22.2%) |
| Pelvic radiotherapy c | 5 (4.8%) | 6 (5.9%) | 2 (12.5%) | 1 (5.6%) | 2 (11.1%) | 0 (0.0%) |
| Questionnaire | ||||||
| Time since diagnosis (in years), median (IQR) | 4.5 [3.5;5.1] | 3.5 [3.0;4.2] | 4.5 [3.8;5.4] | 3.2 [3.0;4.2] | ||
| Age of child at time of questionnaire (in years), median (IQR) | 19.8 [19.0;21.0] | 16.0 [13.3;20.0] | 20.0 [19.2;21.4] | 20.0 [19.8;20.4] | ||
| Number of surveys completed/invited (response rate) | 16/45 (36%) | 18/38 (47%) | 18/38 (47%) | 9/25 (36%) | ||
| Males (n = 101) | Females (n = 104) e | |||||||
|---|---|---|---|---|---|---|---|---|
| Semen Cryopreservation (n = 48) | Testicular Biopsy (n = 5) | No Fertility Preservation (n = 48) | Ovariopexy (n = 2) | Ovarian Tissue Cryopreservation (OTC) (n = 11) | Oocyte Cryopreservation (n = 4) | GNRH-a Co-Treatment (n = 17) | No Fertility Preservation or GNRH-a Co-Treatment (n = 76) | |
| Age at diagnosis in years, median (range) | 16.0 [13.6;18.7] | 12.8 [3.9;14.8] | 11.8 [3.4;17.8] | 16.3 [15.4;17.2] | 15.5 [13.2;17.8] | 16.0 [15.4;17.4] | 16.9 [13.0;18.8] | 15.4 [7.2;18.0] |
| Tanner stage P/M, median (range) | 5.0 [3.0;5.0] | 2.0 [1.0;4.0] | 1.0 [1.0;5.0] | 3.5 [3.0;4.0] | 4.0 [2.0;5.0] | 5.0 [3.0;5.0] | 4.0 [3.0;5.0] | 4.0 [1.0;5.0] |
| Testicular volume (mL) | 20.0 [15.0;22.8] | 6.0 [5.0;12.0] | 5.0 [2.0;10.0] | NA | NA | NA | NA | NA |
| Sperm collection expected to be feasible a | 46 (97.9%) | 1 (20.0%) | 8 (16.7%) | NA | NA | NA | NA | NA |
| Post-menarchal | NA | NA | NA | 2 (100.0%) | 9 (81.8%) | 4 (100.0%) | 17 (100.0%) | 59 (77.6%) |
| Assigned Treatment level | ||||||||
| - TL1 (early-stage disease) | 3 (6.3%) | 2 (40.0%) | 9 (18.8%) | 0 (0.0%) | 0 (0.0%) | 2 (50.0%) | 3 (17.6%) | 13 (17.1%) |
| - TL2 (intermediate-stage disease) | 21 (43.8%) | 2 (40.0%) | 13 (27.1%) | 2 (100.0%) | 8 (72.7%) | 2 (50.0%) | 11 (64.7%) | 32 (42.1%) |
| - TL3 (advanced-stage disease) | 24 (50.0%) | 1 (20.0%) | 26 (54.2%) | 0 (0.0%) | 3 (27.3%) | 0 (0.0%) | 3 (17.6%) | 31 (40.8%) |
| Anticipated high risk of infertility based on assigned chemotherapy b | 24 (50.0%) | 1 (20.0%) | 26 (54.2%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Involved tumor sites in abdominal c (girls) or inguinal (boys) region | 2 (4.2%) | 0 (40.0%) | 3 (6.3%) | 0 (0.0%) | 2 (18.2%) | 0 (0.0%) | 3 (17.6%) | 24 (31.6%) |
| Pelvic radiotherapy d | 4 (8.3%) | 0 (0.0%) | 2 (4.2%) | 0 (0.0%) | 1 (9.1%) | 0 (%) | 2 (11.8%) | 3 (3.9%) |
| Treated in country | ||||||||
| - The Netherlands | 21 | 3 | 23 | 0 | 2 | 1 | 0 | 57 |
| - Belgium | 16 | 2 | 11 | 1 | 6 | 3 | 1 | 12 |
| - Germany | 1 | 0 | 2 | 1 | 3 | 0 | 4 | 6 |
| - Czech Republic | 10 | 0 | 12 | 0 | 0 | 0 | 9 | 0 |
| - Austria | - | - | - | 0 | 0 | 0 | 3 | 1 |
| As Reported by Parents of | ||
|---|---|---|
| Boys (n = 18) | Girls (n = 16) | |
| Reported fertility counseling | 17 (94.4%) | 16 (100.0%) |
| Timing counseling | ||
| - At diagnosis | 2 (11.8%) | 4 (26.7%) |
| - After diagnosis, but before start treatment | 13 (76.5%) | 12 (80.0%) |
| - During treatment | 2 (11.8%) | 4 (26.7%) |
| - During follow-up | 0 (0.0%) | 2 (13.3%) |
| Fertility discussed by | ||
| - Treating physician | 10 (58.8%) | 10 (71.4%) |
| - Nurse practitioner | 6 (35.3%) | 5 (35.7%) |
| - Gynecologist/urologist | 2 (11.8%) | 7 (50.0%) |
| - Missing | 0 | 2 |
| Child involved in conversation about fertility | 13 (76.5%) | 15 (93.8%) |
| Reasons not involved | ||
| - Too young | 3 (75.0%) | 1 (100.0%) |
| - Too sick | 0 (0.0%) | 1 (100.0%) |
| - No interest | 0 (0.0%) | 0 (0.0%) |
| - Felt uncomfortable | 0 (0.0%) | 0 (0.0%) |
| - Missing | 1 | |
| Reported that fertility preservation was offered | 7 (41.2%) | 8 (50.0%) |
| Type of fertility preservation treatment offered/performed | ||
| - Ovariopexy | - | 3 (42.9%)/0 (0%) |
| - Oocyte cryopreservation | - | 4 (57.1%)/0 (0%) |
| - Ovarian tissue cryopreservation | - | 5 (71.4%)/0 (0%) |
| - Semen cryopreservation | 6 (85.7%)/6 (100%) | - |
| - Testicular biopsy | 1 (14.3%)/1 (100%) | - |
| Reported reason(s) for not performing fertility preservation | ||
| - Too young | - | 0 (0.0%) |
| - Too sick/high burden | - | 4 (50.0%) |
| - Felt uncomfortable | - | 0 (0.0%) |
| - Uncertainty about use in the future | - | 2 (25.0%) |
| - Expected low risk | - | 3 (37.5%) |
| Child was involved in the final decision | 6 (85.7%) | 7 (87.5%) |
| As reported by patients | ||
| Boys (n = 9) | Girls (n = 18) | |
| Recalls conversation about fertility | 7 (77.8%) | 17 (94.4%) |
| Fertility discussed by | ||
| - Parents | 1 (14.3%) | 8 (47.1%) |
| - Caregiver | 7 (100.0%) | 17 (100.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drechsel, K.C.E.; IJgosse, I.M.; Slaats, S.; Raasen, L.; Stoutjesdijk, F.S.; van Dulmen-den Broeder, E.; Wallace, W.H.; Beishuizen, A.; Körholz, D.; Mauz-Körholz, C.; et al. Fertility-Preserving Treatments and Patient- and Parental Satisfaction on Fertility Counseling in a Cohort of Newly Diagnosed Boys and Girls with Childhood Hodgkin Lymphoma. Cancers 2024, 16, 2109. https://doi.org/10.3390/cancers16112109
Drechsel KCE, IJgosse IM, Slaats S, Raasen L, Stoutjesdijk FS, van Dulmen-den Broeder E, Wallace WH, Beishuizen A, Körholz D, Mauz-Körholz C, et al. Fertility-Preserving Treatments and Patient- and Parental Satisfaction on Fertility Counseling in a Cohort of Newly Diagnosed Boys and Girls with Childhood Hodgkin Lymphoma. Cancers. 2024; 16(11):2109. https://doi.org/10.3390/cancers16112109
Chicago/Turabian StyleDrechsel, Katja C. E., Irene M. IJgosse, Sofie Slaats, Lisanne Raasen, Francis S. Stoutjesdijk, Eline van Dulmen-den Broeder, W. Hamish Wallace, Auke Beishuizen, Dieter Körholz, Christine Mauz-Körholz, and et al. 2024. "Fertility-Preserving Treatments and Patient- and Parental Satisfaction on Fertility Counseling in a Cohort of Newly Diagnosed Boys and Girls with Childhood Hodgkin Lymphoma" Cancers 16, no. 11: 2109. https://doi.org/10.3390/cancers16112109
APA StyleDrechsel, K. C. E., IJgosse, I. M., Slaats, S., Raasen, L., Stoutjesdijk, F. S., van Dulmen-den Broeder, E., Wallace, W. H., Beishuizen, A., Körholz, D., Mauz-Körholz, C., Cepelova, M., Uyttebroeck, A., Ronceray, L., Kaspers, G. J. L., Broer, S. L., & Veening, M. A., on behalf of the EuroNet-PHL-C2 Study Group. (2024). Fertility-Preserving Treatments and Patient- and Parental Satisfaction on Fertility Counseling in a Cohort of Newly Diagnosed Boys and Girls with Childhood Hodgkin Lymphoma. Cancers, 16(11), 2109. https://doi.org/10.3390/cancers16112109