
Standardized Digital Image Analysis of PD-L1 Expression in Head and Neck Squamous Cell Carcinoma Reveals Intra- and Inter-Sample Heterogeneity with Therapeutic Implications

 , , , ,
, , , , 

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Tissue Microarray Construction
2.3. Immunohistochemical Staining
2.4. Immunohistochemical Scoring
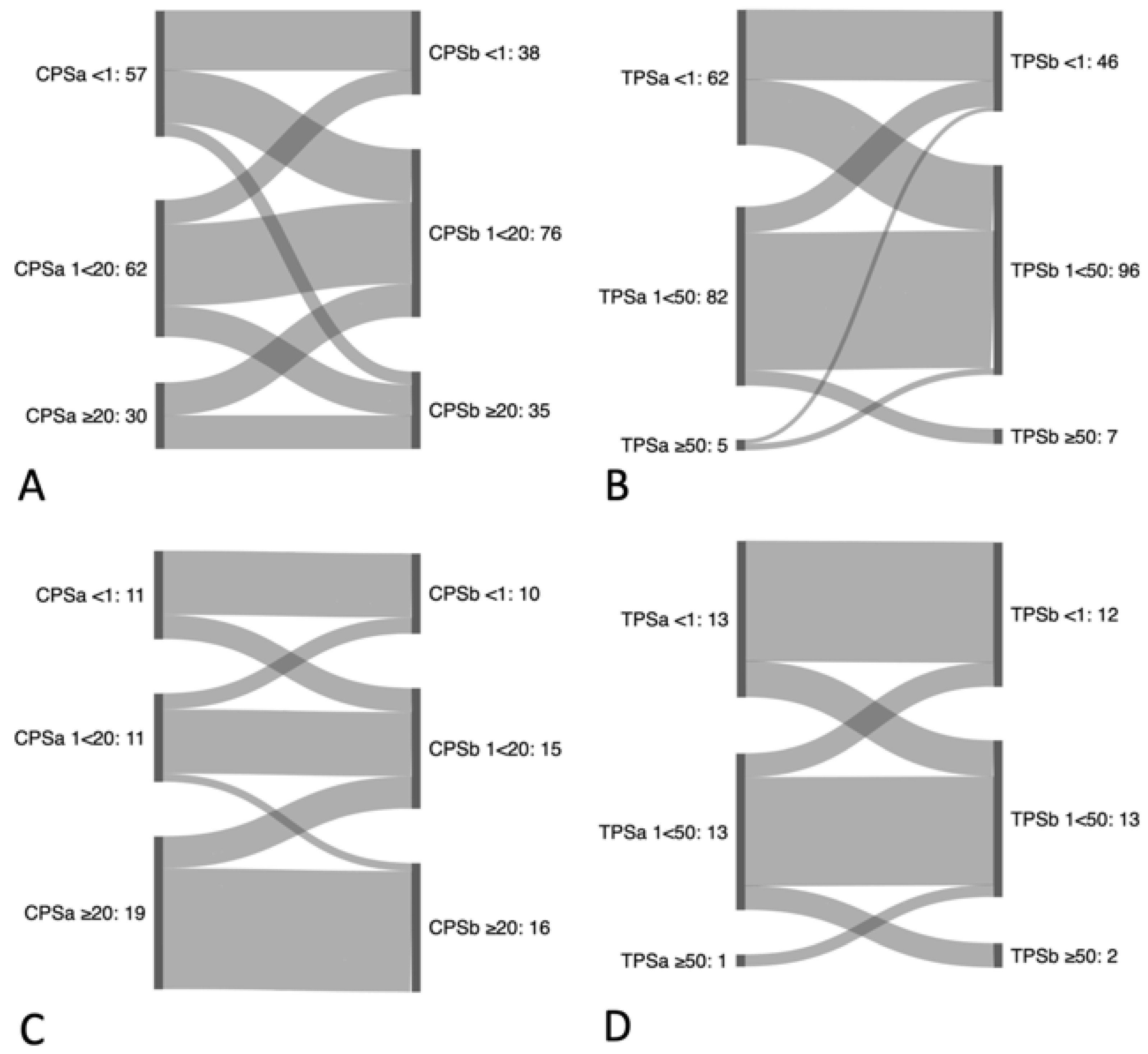
2.5. Assessment of Heterogeneity and Reclassification
2.6. Statistical Analysis
3. Results
3.1. Patients
3.2. PD-L1 Scoring and Overall Expression
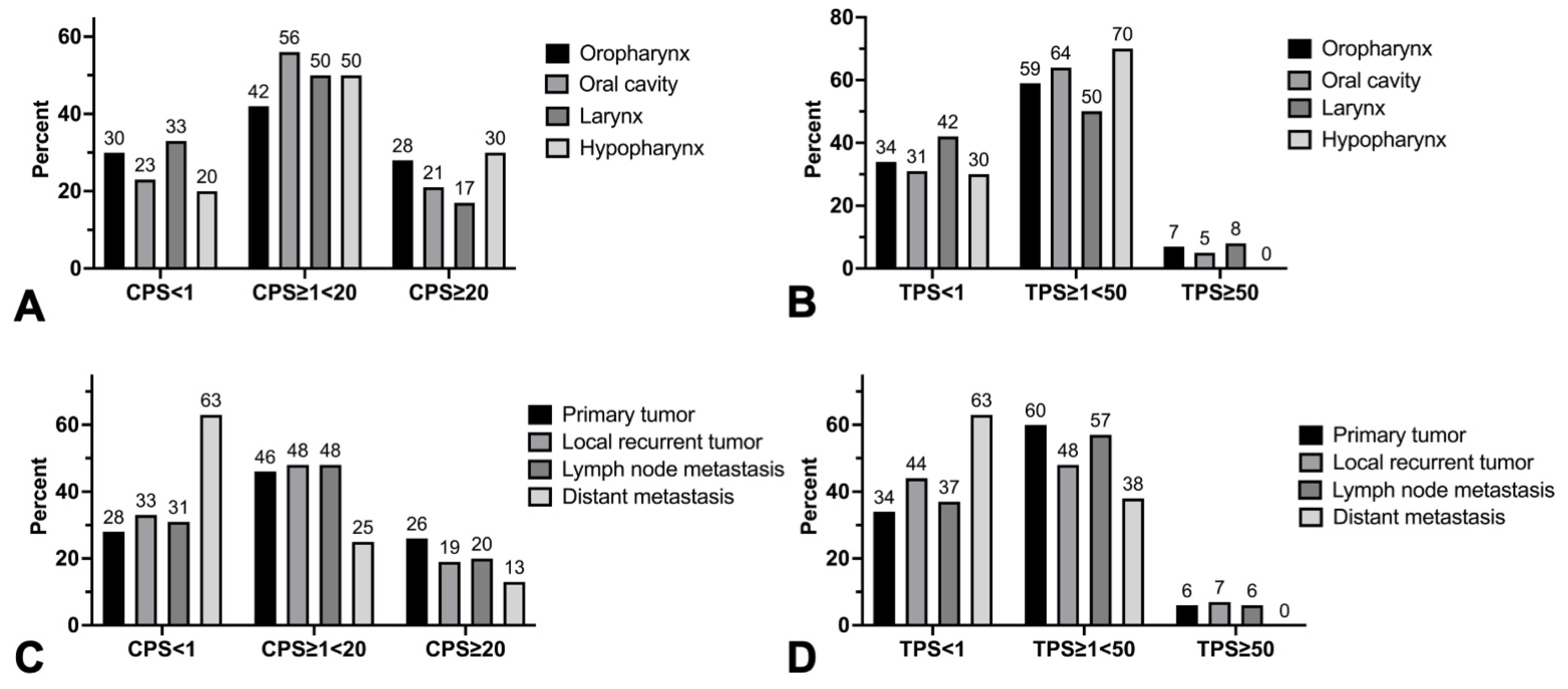
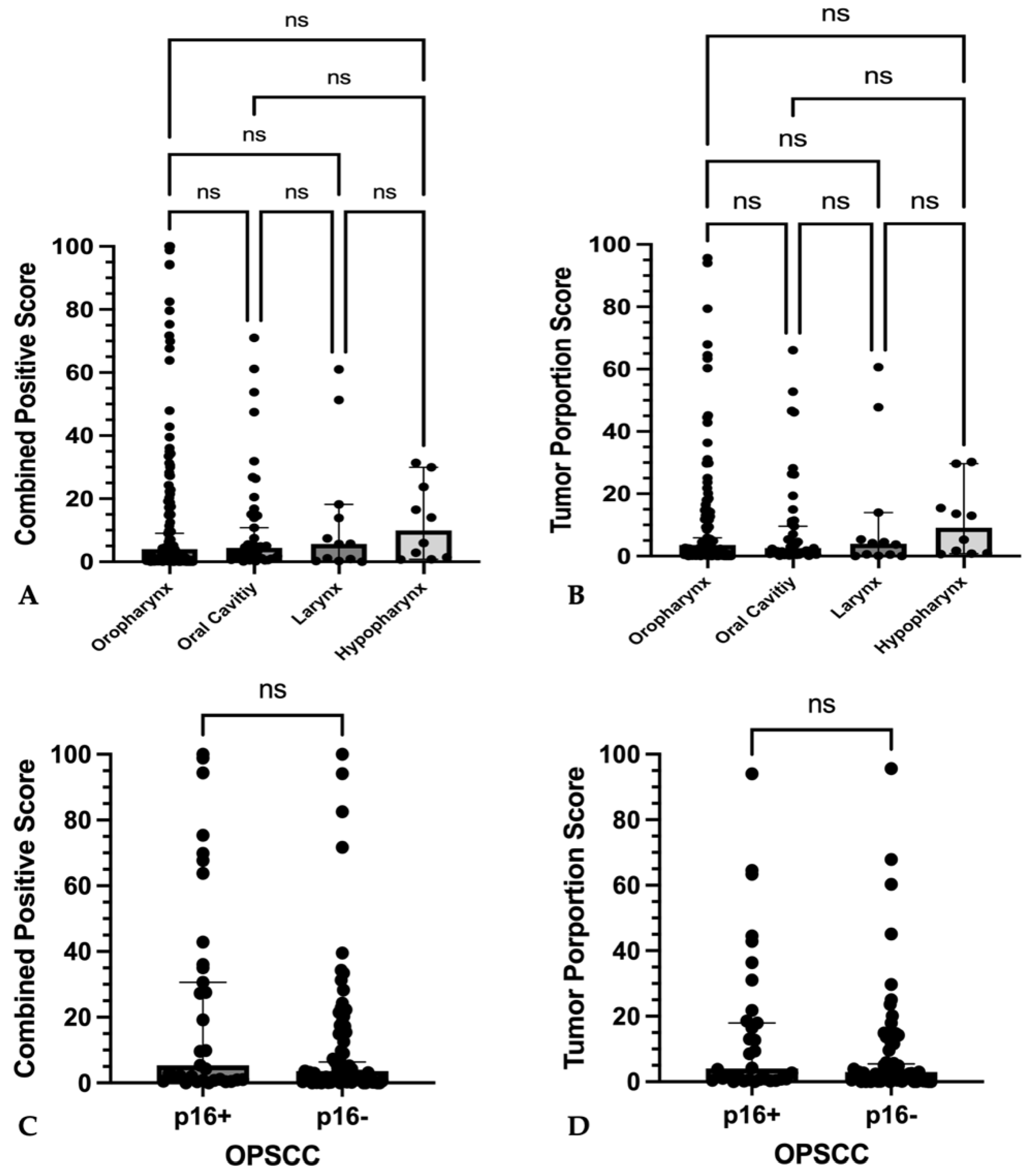
3.3. PD-L1 Expression according to Tumor Locations
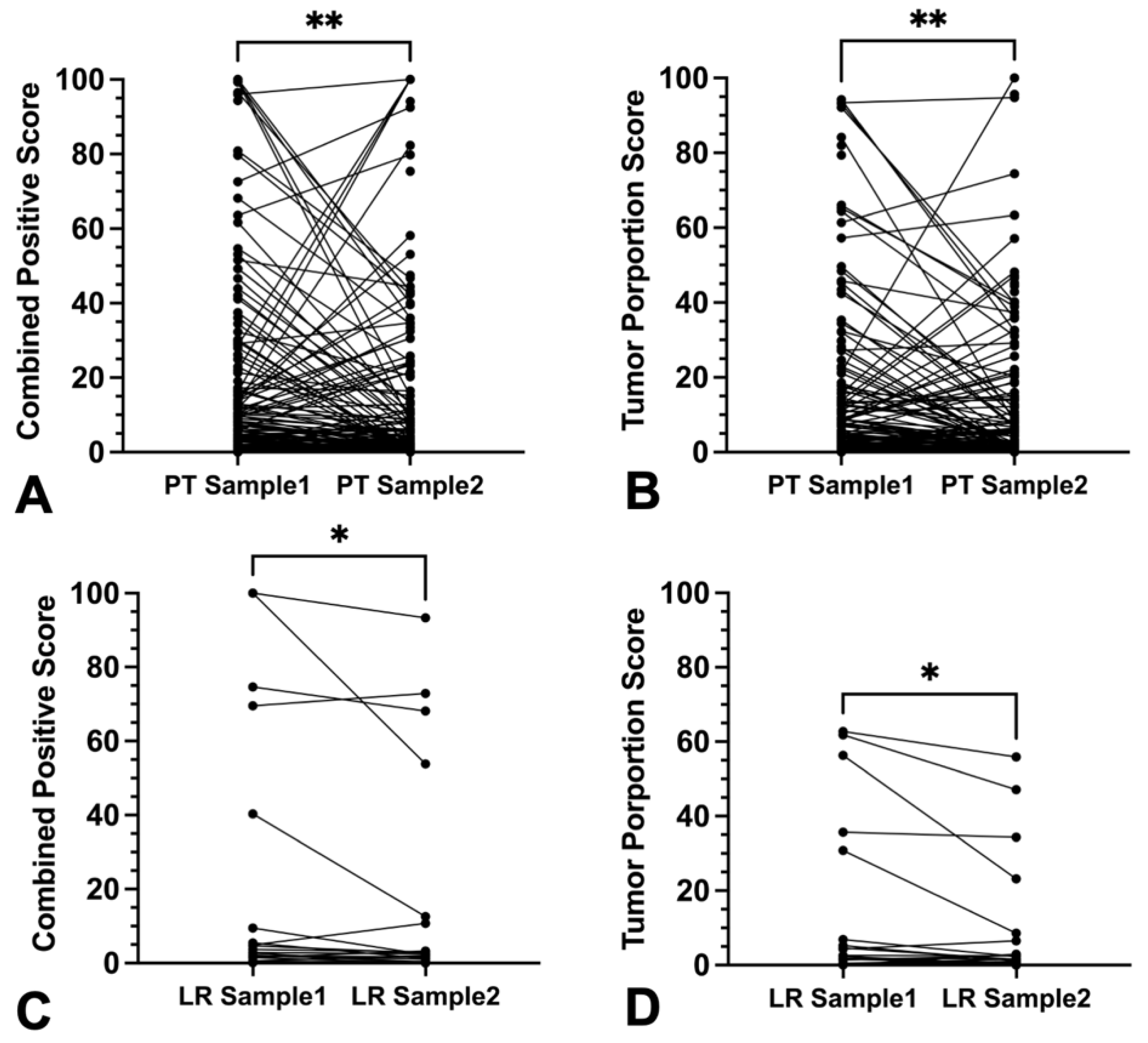
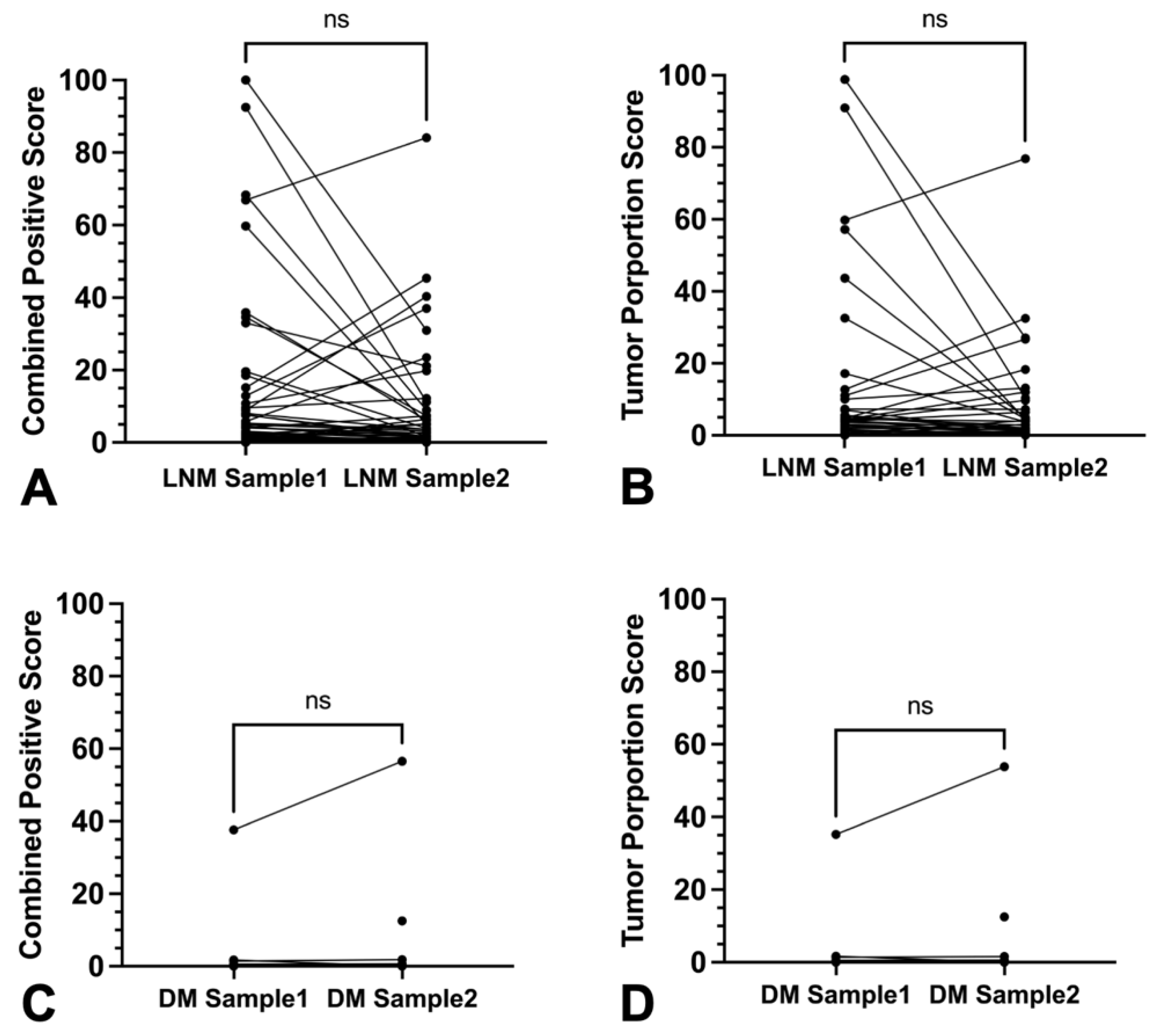
3.4. Intra-Tumoral Heterogeneity of Primary Tumors, Local Recurrent Tumors, and Metastases
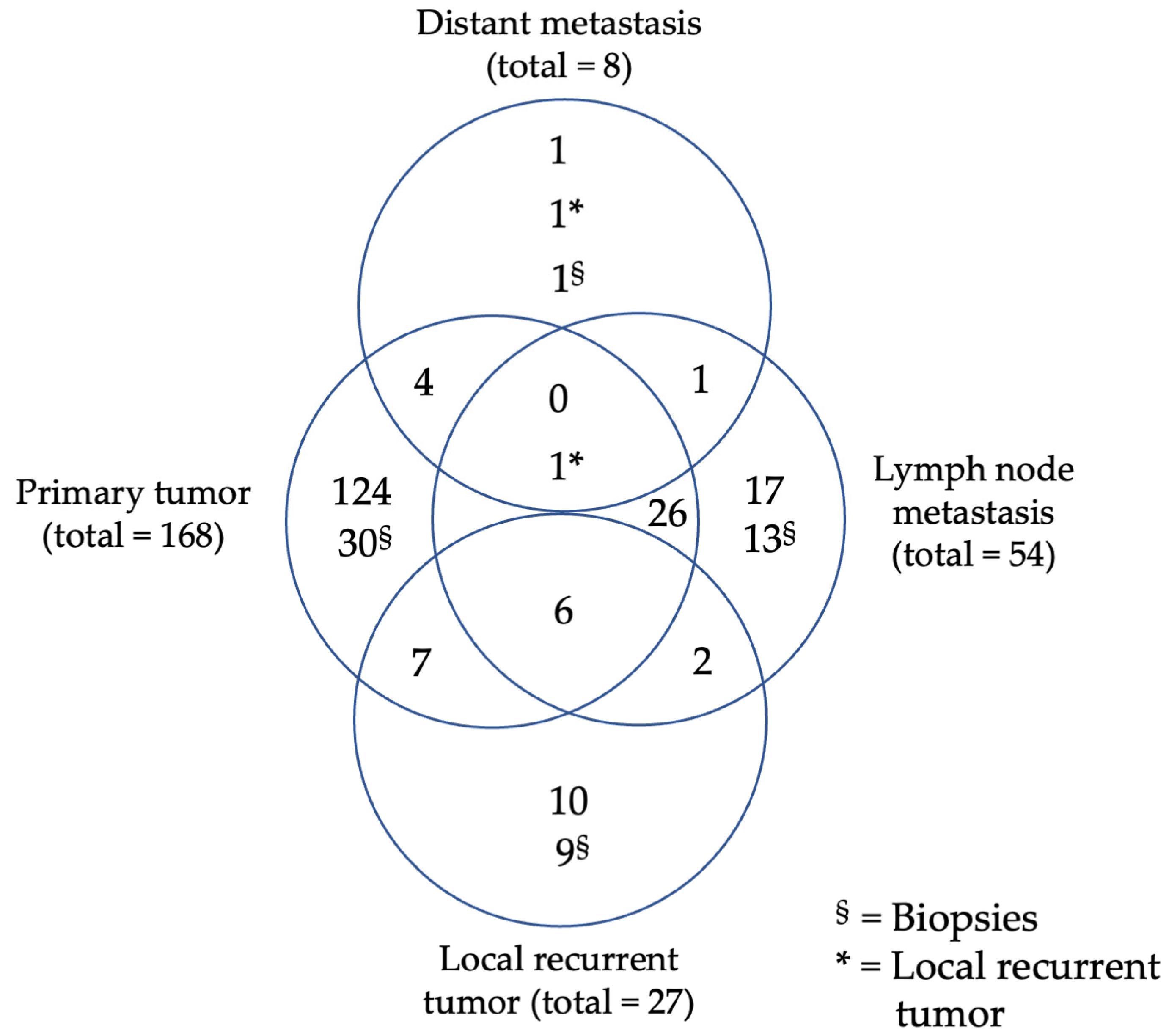
3.5. Scoring Concordance between Primary Tumors and Recurrences as Well as Primary Tumors and Their Metastases
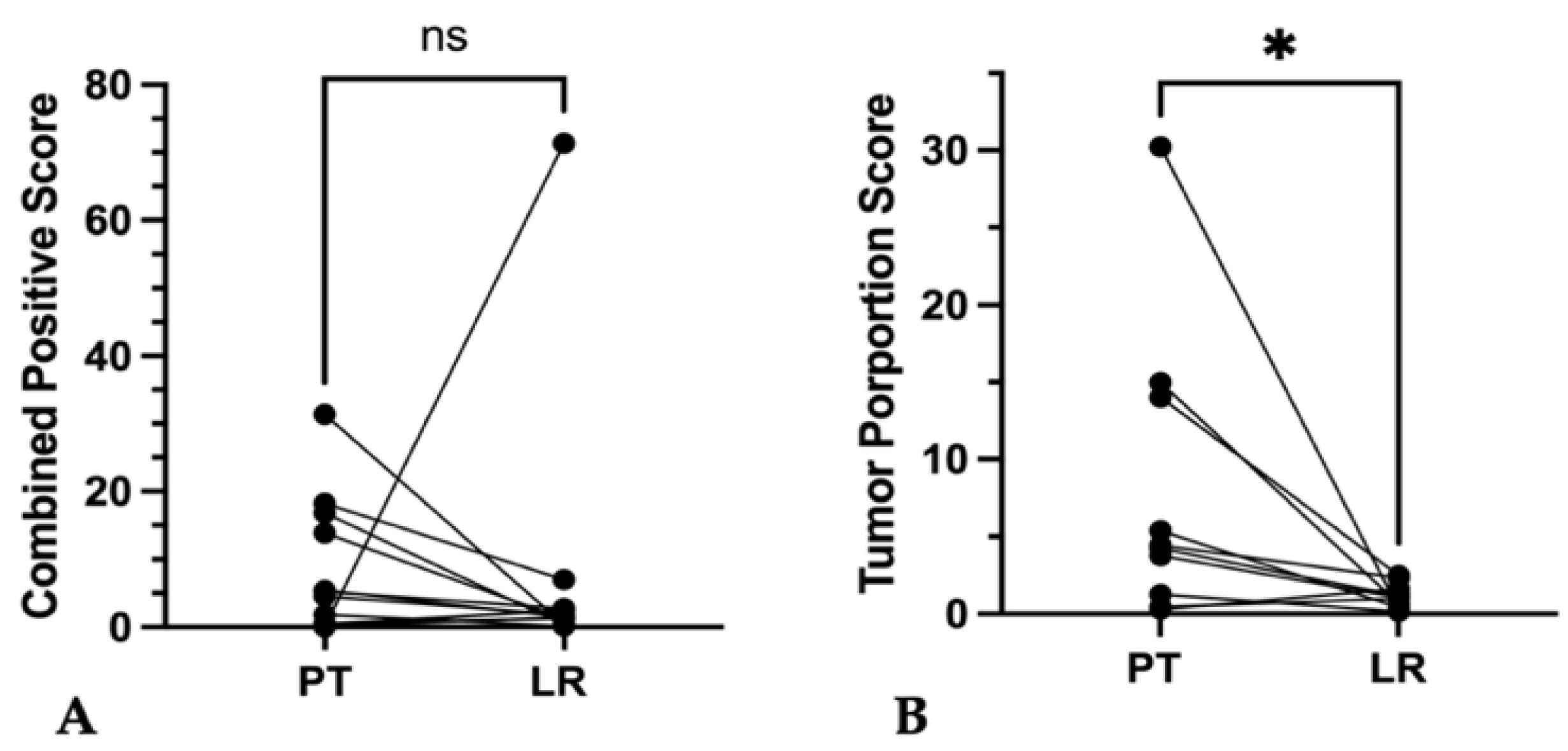
3.5.1. Primary Tumor vs. Local Recurrence
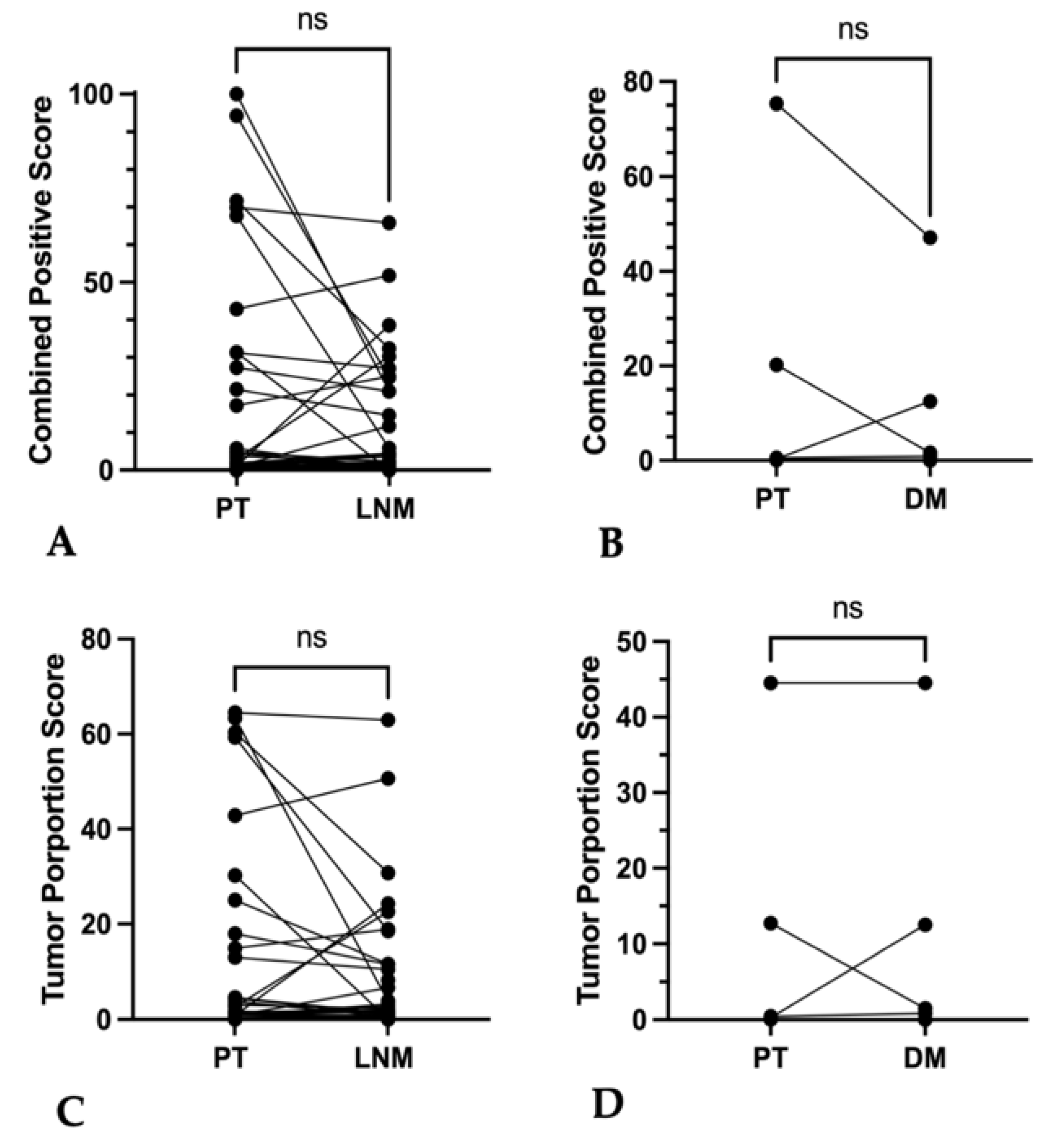
3.5.2. Primary Tumor vs. Associated Lymph Node Metastases and Distant Metastases
3.6. Clinicopathological Correlations
3.6.1. CPS and TPS Expression and Its Association with Recurrence and Metastases
3.6.2. CPS and TPS Expression and Its Association with Clinicopathological Features
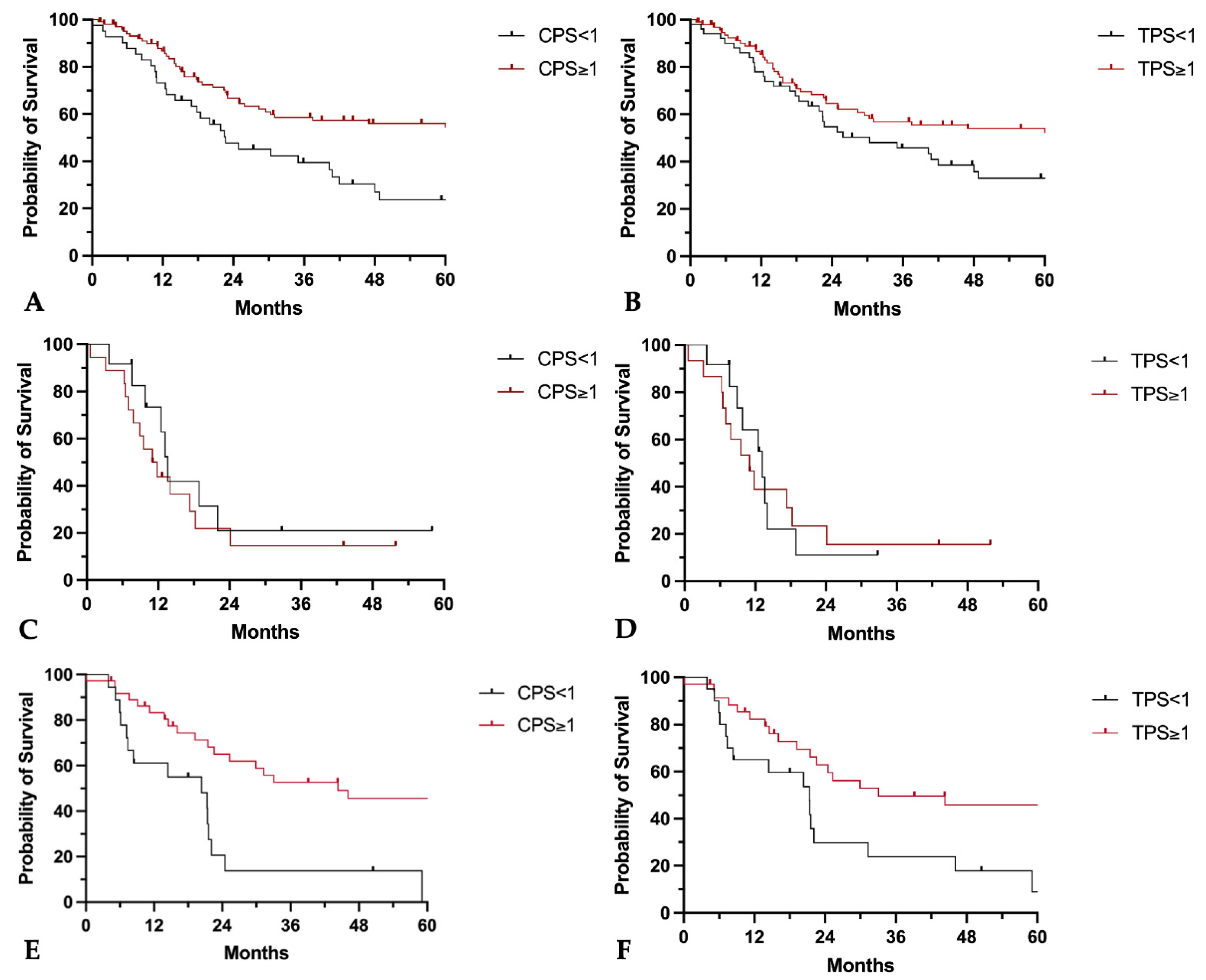
3.7. CPS and TPS Scores and Their Association with Patient Survival
3.8. CPS and TPS Scores and Their Association with Response to Therapy
4. Discussion
4.1. Intra-Tumoral Heterogeneity
4.2. Discrepancies between Primary Tumors, Lymph Nodes, and Distant Metastases
4.3. Discrepancies between Primary Tumors and Recurrent Tumors
4.4. PD-L1 Expression and Survival
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CD8 | Cluster of differentiation 8 |
| CI | Confidence interval |
| CPS | Combined positive score |
| DAB | 3,3′-Diaminobenzidin |
| DM | Distant metastasis |
| EGFR | Epithelial growth factor receptor |
| FFPE | Formalin fixed paraffin embedded |
| HE | hematoxylin eosin |
| HIER | Heat induced epitope retrieval |
| HNSCC | Head and neck squamous cell carcinoma |
| HPV | Human papilloma virus |
| HR | Hazard ratio |
| LNM | Lymph node metastasis |
| LR | local recurrence |
| µL | Microliter |
| OPSCC | Oropharyngeal squamous cell carcinoma |
| OSCC | Oral squamous cell carcinoma |
| PD-L1 | Programmed cell death 1 Ligand 1 |
| PT | Primary tumor |
| RECIST 1.1 | Response Evaluation Criteria in Solid Tumors 1.1 |
| RM-HNSCC | Recurrent and metastatic head and neck squamous cell carcinoma |
| RTU | Ready to use |
| TBS | Tris-buffered saline |
| TMA | Tissue micro array |
| TPS | Tumor proportion score |
| UICC | Union for International Cancer Control |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lacas, B.; Carmel, A.; Landais, C.; Wong, S.J.; Licitra, L.; Tobias, J.S.; Burtness, B.; Ghi, M.G.; Cohen, E.E.W.; Grau, C.; et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 107 randomized trials and 19,805 patients, on behalf of MACH-NC Group. Radiother. Oncol. 2021, 156, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-associated oropharyngeal cancer: Epidemiology, molecular biology and clinical management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Uppaluri, R.; Campbell, K.M.; Egloff, A.M.; Zolkind, P.; Skidmore, Z.L.; Nussenbaum, B.; Paniello, R.C.; Rich, J.T.; Jackson, R.; Pipkorn, P.; et al. Neoadjuvant and Adjuvant Pembrolizumab in Resectable Locally Advanced, Human Papillomavirus-Unrelated Head and Neck Cancer: A Multicenter, Phase II Trial. Clin. Cancer Res. 2020, 26, 5140–5152. [Google Scholar] [CrossRef]
- Vos, J.L.; Elbers, J.B.W.; Krijgsman, O.; Traets, J.J.H.; Qiao, X.; van der Leun, A.M.; Lubeck, Y.; Seignette, I.M.; Smit, L.A.; Willems, S.M.; et al. Neoadjuvant immunotherapy with nivolumab and ipilimumab induces major pathological responses in patients with head and neck squamous cell carcinoma. Nat. Commun. 2021, 12, 7348. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Haddad, R.I.; Worden, F.P.; Weiss, J.; Mehra, R.; Chow, L.Q.M.; Liu, S.V.; Kang, H.; Saba, N.F.; Wirth, L.J.; et al. Biomarkers predictive of response to pembrolizumab in head and neck cancer. Cancer Med. 2022, 12, 6603–6614. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Oridate, N.; Tanaka, K.; Shimizu, Y.; Fujimoto, Y.; Matsumoto, K.; Yokota, T.; Yamazaki, T.; Takahashi, M.; Ueda, T.; et al. First-line pembrolizumab ± chemotherapy for recurrent/metastatic head and neck cancer: Japanese subgroup of KEYNOTE-048. Int. J. Clin. Oncol. 2022, 27, 1805–1817. [Google Scholar] [CrossRef]
- Rasmussen, J.H.; Lelkaitis, G.; Håkansson, K.; Vogelius, I.R.; Johannesen, H.H.; Fischer, B.M.; Bentzen, S.M.; Specht, L.; Kristensen, C.A.; von Buchwald, C.; et al. Intratumor heterogeneity of PD-L1 expression in head and neck squamous cell carcinoma. Br. J. Cancer 2019, 120, 1003–1006. [Google Scholar] [CrossRef] [PubMed]
- Deuss, E.; Gößwein, D.; Gül, D.; Zimmer, S.; Foersch, S.; Eger, C.S.; Limburg, I.; Stauber, R.H.; Künzel, J. Growth Factor Receptor Expression in Oropharyngeal Squamous Cell Cancer: Her1-4 and c-Met in Conjunction with the Clinical Features and Human Papillomavirus (p16) Status. Cancers 2020, 12, 3358. [Google Scholar] [CrossRef] [PubMed]
- Naso, J.R.; Povshedna, T.; Wang, G.; Banyi, N.; MacAulay, C.; Ionescu, D.N.; Zhou, C. Automated PD-L1 Scoring for Non-Small Cell Lung Carcinoma Using Open-Source Software. Pathol. Oncol. Res. 2021, 27, 609717. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.; Nogueira, C.; Marinho, L.C.; Velozo, G.; Sousa, J.; Silva, P.G.; Tavora, F. Computer-assisted tumor grading, validation of PD-L1 scoring, and quantification of CD8-positive immune cell density in urothelial carcinoma, a visual guide for pathologists using QuPath. Surg. Exp. Pathol. 2022, 5, 12. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed]
- Paver, E.C.; Cooper, W.A.; Colebatch, A.J.; Ferguson, P.M.; Hill, S.K.; Lum, T.; Shin, J.S.; O’Toole, S.; Anderson, L.; Scolyer, R.A.; et al. Programmed death ligand-1 (PD-L1) as a predictive marker for immunotherapy in solid tumours: A guide to immunohistochemistry implementation and interpretation. Pathology 2021, 53, 141–156. [Google Scholar] [CrossRef]
- de Ruiter, E.J.; Mulder, F.J.; Koomen, B.M.; Speel, E.J.; van den Hout, M.; de Roest, R.H.; Bloemena, E.; Devriese, L.A.; Willems, S.M. Comparison of three PD-L1 immunohistochemical assays in head and neck squamous cell carcinoma (HNSCC). Mod. Pathol. 2021, 34, 1125–1132. [Google Scholar] [CrossRef]
- Chen, T.C.; Wu, C.T.; Wang, C.P.; Hsu, W.L.; Yang, T.L.; Lou, P.J.; Ko, J.Y.; Chang, Y.L. Associations among pretreatment tumor necrosis and the expression of HIF-1α and PD-L1 in advanced oral squamous cell carcinoma and the prognostic impact thereof. Oral. Oncol. 2015, 51, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Tian, S.; Lin, L.; Zhang, J.; Ding, H. Prognostic and clinicopathological significance of PD-L1 and tumor infiltrating lymphocytes in hypopharyngeal squamous cell carcinoma. Oral. Oncol. 2020, 102, 104560. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Canteli, M.; Granda-Díaz, R.; Del Rio-Ibisate, N.; Allonca, E.; López-Alvarez, F.; Agorreta, J.; Garmendia, I.; Montuenga, L.M.; García-Pedrero, J.M.; Rodrigo, J.P. PD-L1 expression correlates with tumor-infiltrating lymphocytes and better prognosis in patients with HPV-negative head and neck squamous cell carcinomas. Cancer Immunol. Immunother. 2020, 69, 2089–2100. [Google Scholar] [CrossRef] [PubMed]
- Scognamiglio, T.; Chen, Y.T. Beyond the Percentages of PD-L1-Positive Tumor Cells: Induced Versus Constitutive PD-L1 Expression in Primary and Metastatic Head and Neck Squamous Cell Carcinoma. Head Neck Pathol. 2018, 12, 221–229. [Google Scholar] [CrossRef]
- Jeong, J.Y.; Park, T.I.; Ahn, D. Comprehensive Analysis and Clinical Implication of PD-L1 Expression Considering HPV Status in Oropharyngeal Squamous Cell Carcinoma. Anticancer. Res. 2020, 40, 4001–4010. [Google Scholar] [CrossRef] [PubMed]
- Kareer, R.; Ahuja, S.; Chaudhary, N.; Arora, R. Association of PD-L1 and p16 expression with clinicopathological parameters in oral cavity and oropharyngeal squamous cell carcinoma. Pathol. Res. Pract. 2023, 241, 154266. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.J.; Levy, D.A.; Nguyen, S.A.; Knochelmann, H.M.; Day, T.A. Impact of PD-L1 expression and human papillomavirus status in anti-PD1/PDL1 immunotherapy for head and neck squamous cell carcinoma-Systematic review and meta-analysis. Head Neck 2020, 42, 774–786. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini-Spaltro, A.; Limarzi, F.; Gaudio, M.; Calpona, S.; Meccariello, G. PD-L1 expression in head and neck carcinoma by combined positive score: A comparison among preoperative biopsy, tumor resection, and lymph node metastasis. Virchows Arch. 2022, 481, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Hirshoren, N.; Al-Kharouf, I.; Weinberger, J.M.; Eliashar, R.; Popovtzer, A.; Knaanie, A.; Fellig, Y.; Neuman, T.; Meir, K.; Maly, A.; et al. Spatial Intratumoral Heterogeneity Expression of PD-L1 Antigen in Head and Neck Squamous Cell Carcinoma. Oncology 2021, 99, 464–470. [Google Scholar] [CrossRef]
- Paintal, A.S.; Brockstein, B.E. PD-L1 CPS Scoring Accuracy in Small Biopsies and Aspirate Cell Blocks from Patients with Head and Neck Squamous Cell Carcinoma. Head Neck Pathol. 2020, 14, 657–665. [Google Scholar] [CrossRef]
- De Keukeleire, S.J.; Vermassen, T.; Deron, P.; Huvenne, W.; Duprez, F.; Creytens, D.; Van Dorpe, J.; Ferdinande, L.; Rottey, S. Concordance, Correlation, and Clinical Impact of Standardized PD-L1 and TIL Scoring in SCCHN. Cancers 2022, 14, 2431. [Google Scholar] [CrossRef] [PubMed]
- Kalpakoff, M.; Hund, S.; Musser, J.; Roach, C.; Apostolaki, A.; Vilardo, M.; Peltz, L.; Watts, B.; LaPlaca, C.; Tabuena-Frolli, S.; et al. Intrapatient Tumor Heterogeneity in IHC Interpretation Using PD-L1 IHC 22C3 pharmDx. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Nuti, S.; Zhang, Y.; Zerrouki, N.; Roach, C.; Bänfer, G.; Kumar, G.L.; Manna, E.; Diezko, R.; Kersch, K.; Rüschoff, J.; et al. High interobserver and intraobserver reproducibility among pathologists assessing PD-L1 CPS across multiple indications. Histopathology 2022, 81, 732–741. [Google Scholar] [CrossRef] [PubMed]
- Leduc, C.; Adam, J.; Louvet, E.; Sourisseau, T.; Dorvault, N.; Bernard, M.; Maingot, E.; Faivre, L.; Cassin-Kuo, M.S.; Boissier, E.; et al. TPF induction chemotherapy increases PD-L1 expression in tumour cells and immune cells in head and neck squamous cell carcinoma. ESMO Open 2018, 3, e000257. [Google Scholar] [CrossRef] [PubMed]
- Paolino, G.; Pantanowitz, L.; Barresi, V.; Pagni, F.; Munari, E.; Moretta, L.; Brunelli, M.; Bariani, E.; Vigliar, E.; Pisapia, P. PD-L1 evaluation in head and neck squamous cell carcinoma: Insights regarding specimens, heterogeneity and therapy. Pathol. Res. Pract. 2021, 226, 153605. [Google Scholar] [CrossRef] [PubMed]
- Brcic, I.; Gallob, M.; Schwantzer, G.; Zrnc, T.; Weiland, T.; Thurnher, D.; Wolf, A.; Brcic, L. Concordance of tumor infiltrating lymphocytes, PD-L1 and p16 expression in small biopsies, resection and lymph node metastases of oropharyngeal squamous cell carcinoma. Oral. Oncol. 2020, 106, 104719. [Google Scholar] [CrossRef] [PubMed]
- De Meulenaere, A.; Vermassen, T.; Creytens, D.; Aspeslagh, S.; Deron, P.; Duprez, F.; Rottey, S.; Van Dorpe, J.A.; Ferdinande, L. Importance of choice of materials and methods in PD-L1 and TIL assessment in oropharyngeal squamous cell carcinoma. Histopathology 2018, 73, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Kaur, A.; Kuchta, K.; Watkin, W.; Sullivan, M.; Liu, L.; Jamshidi, P.; Campbell, N.; Brockstein, B.; Paintal, A. Programmed Death Ligand-1 Combined Positive Score Concordance and Interrater Reliability in Primary Tumors and Synchronous Lymph Node Metastases in Resected Cases of p16+ Oropharyngeal Squamous Cell Carcinoma. Arch. Pathol. Lab. Med. 2022, 147, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Straub, M.; Drecoll, E.; Pfarr, N.; Weichert, W.; Langer, R.; Hapfelmeier, A.; Götz, C.; Wolff, K.D.; Kolk, A.; Specht, K. CD274/PD-L1 gene amplification and PD-L1 protein expression are common events in squamous cell carcinoma of the oral cavity. Oncotarget 2016, 7, 12024–12034. [Google Scholar] [CrossRef]
- Moratin, J.; Metzger, K.; Safaltin, A.; Herpel, E.; Hoffmann, J.; Freier, K.; Hess, J.; Horn, D. Upregulation of PD-L1 and PD-L2 in neck node metastases of head and neck squamous cell carcinoma. Head Neck 2019, 41, 2484–2491. [Google Scholar] [CrossRef]
- Muralidharan, S.; Sehgal, M.; Soundharya, R.; Mandal, S.; Majumdar, S.S.; Yeshwanth, M.; Saha, A.; Jolly, M.K. PD-L1 Activity Is Associated with Partial EMT and Metabolic Reprogramming in Carcinomas. Curr. Oncol. 2022, 29, 8285–8301. [Google Scholar] [CrossRef] [PubMed]
- Okada, S.; Itoh, K.; Ishihara, S.; Shimada, J.; Kato, D.; Tsunezuka, H.; Miyata, N.; Hirano, S.; Teramukai, S.; Inoue, M. Significance of PD-L1 expression in pulmonary metastases from head and neck squamous cell carcinoma. Surg. Oncol. 2018, 27, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Karabajakian, A.; Bouaoud, J.; Michon, L.; Kamal, M.; Crozes, C.; Zrounba, P.; Auclair-Perossier, J.; Gadot, N.; Attignon, V.; Le Tourneau, C. Longitudinal assessment of PD-L1 expression and gene expression profiles in patients with head and neck cancer reveals temporal heterogeneity. Oral Oncol. 2021, 119, 105368. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.F.; Wong, M.C.M.; Thomson, P.J.; Li, K.Y.; Su, Y.X. The prognostic role of PD-L1 expression for survival in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral Oncol. 2018, 86, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, Y.; Someya, M.; Nakata, K.; Hori, M.; Kitagawa, M.; Hasegawa, T.; Tsuchiya, T.; Gocho, T.; Ikeda, H.; Hirohashi, Y.; et al. Influence of PD-L1 expression in immune cells on the response to radiation therapy in patients with oropharyngeal squamous cell carcinoma. Radiother. Oncol. 2018, 129, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Lenouvel, D.; González-Moles, M.; Ruiz-Ávila, I.; Gonzalez-Ruiz, L.; Gonzalez-Ruiz, I.; Ramos-García, P. Prognostic and clinicopathological significance of PD-L1 overexpression in oral squamous cell carcinoma: A systematic review and comprehensive meta-analysis. Oral Oncol. 2020, 106, 104722. [Google Scholar] [CrossRef] [PubMed]
- Pai, S.I.; Cohen, E.E.W.; Lin, D.; Fountzilas, G.; Kim, E.S.; Mehlhorn, H.; Baste, N.; Clayburgh, D.; Lipworth, L.; Resteghini, C.; et al. SUPREME-HN: A retrospective biomarker study assessing the prognostic value of PD-L1 expression in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck. J. Transl. Med. 2019, 17, 429. [Google Scholar] [CrossRef] [PubMed]
- Wuerdemann, N.; Gültekin, S.E.; Pütz, K.; Wittekindt, C.; Huebbers, C.U.; Sharma, S.J.; Eckel, H.; Schubotz, A.B.; Gattenlöhner, S.; Büttner, R.; et al. PD-L1 Expression and a High Tumor Infiltrate of CD8+ Lymphocytes Predict Outcome in Patients with Oropharyngeal Squamous Cells Carcinoma. Int. J. Mol. Sci. 2020, 21, 5228. [Google Scholar] [CrossRef] [PubMed]
- Lenouvel, D.; González-Moles, M.; Ruiz-Ávila, I.; Chamorro-Santos, C.; González-Ruiz, L.; González-Ruiz, I.; Ramos-García, P. Clinicopathological and prognostic significance of PD-L1 in oral cancer: A preliminary retrospective immunohistochemistry study. Oral Dis. 2021, 27, 173–182. [Google Scholar] [CrossRef]
- Kim, H.R.; Ha, S.J.; Hong, M.H.; Heo, S.J.; Koh, Y.W.; Choi, E.C.; Kim, E.K.; Pyo, K.H.; Jung, I.; Seo, D.; et al. PD-L1 expression on immune cells, but not on tumor cells, is a favorable prognostic factor for head and neck cancer patients. Sci. Rep. 2016, 6, 36956. [Google Scholar] [CrossRef]
- Soopanit, T.; Laokulrath, N.; Chayopasakul, V.; Pongsapich, W. Prognostic value and clinicopathological status of PD-L1 expression and CD8+ TILs in oral squamous cell cancer patients with or without traditional risk factors. Head Neck 2023, 45, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Grasso, C.S.; Tsoi, J.; Onyshchenko, M.; Abril-Rodriguez, G.; Ross-Macdonald, P.; Wind-Rotolo, M.; Champhekar, A.; Medina, E.; Torrejon, D.Y.; Shin, D.S.; et al. Conserved Interferon-γ Signaling Drives Clinical Response to Immune Checkpoint Blockade Therapy in Melanoma. Cancer Cell 2020, 38, 500–515.e503. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.; Young, R.J.; Rischin, D. Head and neck squamous cell carcinoma: Genomics and emerging biomarkers for immunomodulatory cancer treatments. Semin. Cancer Biol. 2018, 52, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Kürten, C.H.L.; Kulkarni, A.; Cillo, A.R.; Santos, P.M.; Roble, A.K.; Onkar, S.; Reeder, C.; Lang, S.; Chen, X.; Duvvuri, U.; et al. Investigating immune and non-immune cell interactions in head and neck tumors by single-cell RNA sequencing. Nat. Commun. 2021, 12, 7338. [Google Scholar] [CrossRef] [PubMed]
- Hecht, M.; Gostian, A.O.; Eckstein, M.; Rutzner, S.; von der Grün, J.; Illmer, T.; Hautmann, M.G.; Klautke, G.; Laban, S.; Brunner, T.; et al. Safety and efficacy of single cycle induction treatment with cisplatin/docetaxel/ durvalumab/tremelimumab in locally advanced HNSCC: First results of CheckRad-CD8. J. Immunother. Cancer 2020, 8, e001378. [Google Scholar] [CrossRef]
- Li, S.; Li, K.; Wang, K.; Yu, H.; Wang, X.; Shi, M.; Liang, Z.; Yang, Z.; Hu, Y.; Li, Y.; et al. Low-dose radiotherapy combined with dual PD-L1 and VEGFA blockade elicits antitumor response in hepatocellular carcinoma mediated by activated intratumoral CD8+ exhausted-like T cells. Nat. Commun. 2023, 14, 7709. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue Samples | Specimen No. (%) | Patients No. (%) |
|---|---|---|
| primary tumors | 198 (63.9) | 168 (65.4) |
| local recurrent tumors | 36 (11.6) | 27 (10.5) |
| lymph node metastasis | 67 (21.6) | 54 (21.0) |
| distant metastasis | 9 (2.9) | 8 (3.1) |
| Sex | No. (%) |
| female | 53 (31.5) |
| male | 115 (68.5) |
| Age in years median (range) | |
| female | 62 (39–80) |
| male | 60 (19–80) |
| Body mass index | |
| median (range) | 24.9 (13.1–43) |
| Overall survival in months | |
| median (range) | 25 (1–137) |
| Primary tumor site | No. (%) |
| oropharynx | 107 (63.7) |
| p16 positive | 35 (32.7) |
| p16 negative | 72 (67.3) |
| oral cavitiy | 39 (23.2) |
| larynx | 12 (7.1) |
| hypopharynx | 10 (6.0) |
| T (UICC 7. edition) | No. (%) |
| 1 | 51 (30.4) |
| 2 | 52 (31.0) |
| 3 | 34 (20.2) |
| 4 | 31 (18.5) |
| N (UICC 7. edition) | No. (%) |
| 0 | 59 (35.1) |
| 1 | 31 (18.5) |
| 2a | 8 (4.8) |
| 2b | 42 (25.0) |
| 2c | 26 (15.5) |
| 3 | 2 (1.2) |
| Stage (UICC 7. edition) | No. (%) |
| I | 20 (11.9) |
| II | 24 (14.3) |
| III | 35 (20.8) |
| IVa | 68 (40.5) |
| IVb | 3 (1.8) |
| IVc | 18 (10.7) |
| Grading | |
| I | 6 (3.6) |
| II | 89 (53.0) |
| III | 52 (31.0) |
| Lymphnode ratio | |
| median (range) with ≥ 15 resected lymph nodes | 0.08 (0–0.6) |
| Extranodal extension | |
| Yes | 30 (17.3) |
| Toxicant use | No. (%) |
| smoking | 119 (70.8) |
| alcohol abuse | 58 (34.5) |
| Therapy | |
| surgery | 24 (14.3) |
| surgery ± postoperative radio(chemo-)therapy | 47 (28.0) |
| radio(chemo-)therapy | 29 (17.3) |
| Tumor Site | Covariates | N | Hazard Ratio | 95% Confidence Intervall | p-Value |
|---|---|---|---|---|---|
| HNSCC | univariate | 149 | 0.4553 | 0.2885 to 0.7261 | 0.0008 |
| staging | 147 | 0.5385 | 0.3372 to 0.8693 | 0.01 | |
| OPSCC | univariate | 107 | 0.4418 | 0.2422 to 0.8126 | 0.008 |
| staging, p16 | 107 | 0.4561 | 0.2419 to 0.8708 | 0.016 | |
| OSCC | univariate | 32 | 0.2328 | 0.08298 to 0.6685 | 0.005 |
| staging | 32 | 0.2344 | 0.08326 to 0.6751 | 0.006 |
| Tumor Site | Covariates | N | Hazard Ratio | 95% Confidence Intervall | p-Value |
|---|---|---|---|---|---|
| HNSCC | univariate | 149 | 0.6192 | 0.3938 to 0.9789 | 0.04 |
| staging | 147 | 0.689 | 0.4342 to 1.100 | 0.12 | |
| OPSCC | univariate | 96 | 0.5373 | 0.2944 to 0.9834 | 0.04 |
| staging, p16 | 92 | 0.4957 | 0.2629 to 0.9399 | 0.03 | |
| OSCC | univariate | 32 | 0.3885 | 0.1422 to 1.061 | 0.06 |
| staging | 32 | 0.5015 | 0.1756 to 1.432 | 0.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deuss, E.; Kürten, C.; Fehr, L.; Kahl, L.; Zimmer, S.; Künzel, J.; Stauber, R.H.; Lang, S.; Hussain, T.; Brandau, S. Standardized Digital Image Analysis of PD-L1 Expression in Head and Neck Squamous Cell Carcinoma Reveals Intra- and Inter-Sample Heterogeneity with Therapeutic Implications. Cancers 2024, 16, 2103. https://doi.org/10.3390/cancers16112103
Deuss E, Kürten C, Fehr L, Kahl L, Zimmer S, Künzel J, Stauber RH, Lang S, Hussain T, Brandau S. Standardized Digital Image Analysis of PD-L1 Expression in Head and Neck Squamous Cell Carcinoma Reveals Intra- and Inter-Sample Heterogeneity with Therapeutic Implications. Cancers. 2024; 16(11):2103. https://doi.org/10.3390/cancers16112103
Chicago/Turabian StyleDeuss, Eric, Cornelius Kürten, Lara Fehr, Laura Kahl, Stefanie Zimmer, Julian Künzel, Roland H. Stauber, Stephan Lang, Timon Hussain, and Sven Brandau. 2024. "Standardized Digital Image Analysis of PD-L1 Expression in Head and Neck Squamous Cell Carcinoma Reveals Intra- and Inter-Sample Heterogeneity with Therapeutic Implications" Cancers 16, no. 11: 2103. https://doi.org/10.3390/cancers16112103
APA StyleDeuss, E., Kürten, C., Fehr, L., Kahl, L., Zimmer, S., Künzel, J., Stauber, R. H., Lang, S., Hussain, T., & Brandau, S. (2024). Standardized Digital Image Analysis of PD-L1 Expression in Head and Neck Squamous Cell Carcinoma Reveals Intra- and Inter-Sample Heterogeneity with Therapeutic Implications. Cancers, 16(11), 2103. https://doi.org/10.3390/cancers16112103