

Outcomes and Pattern of Care for Spinal Myxopapillary Ependymoma in the Modern Era—A Population-Based Observational Study

 ,
,  , , , , ,
, , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Study Design
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Study Population and Treatment Characteristics
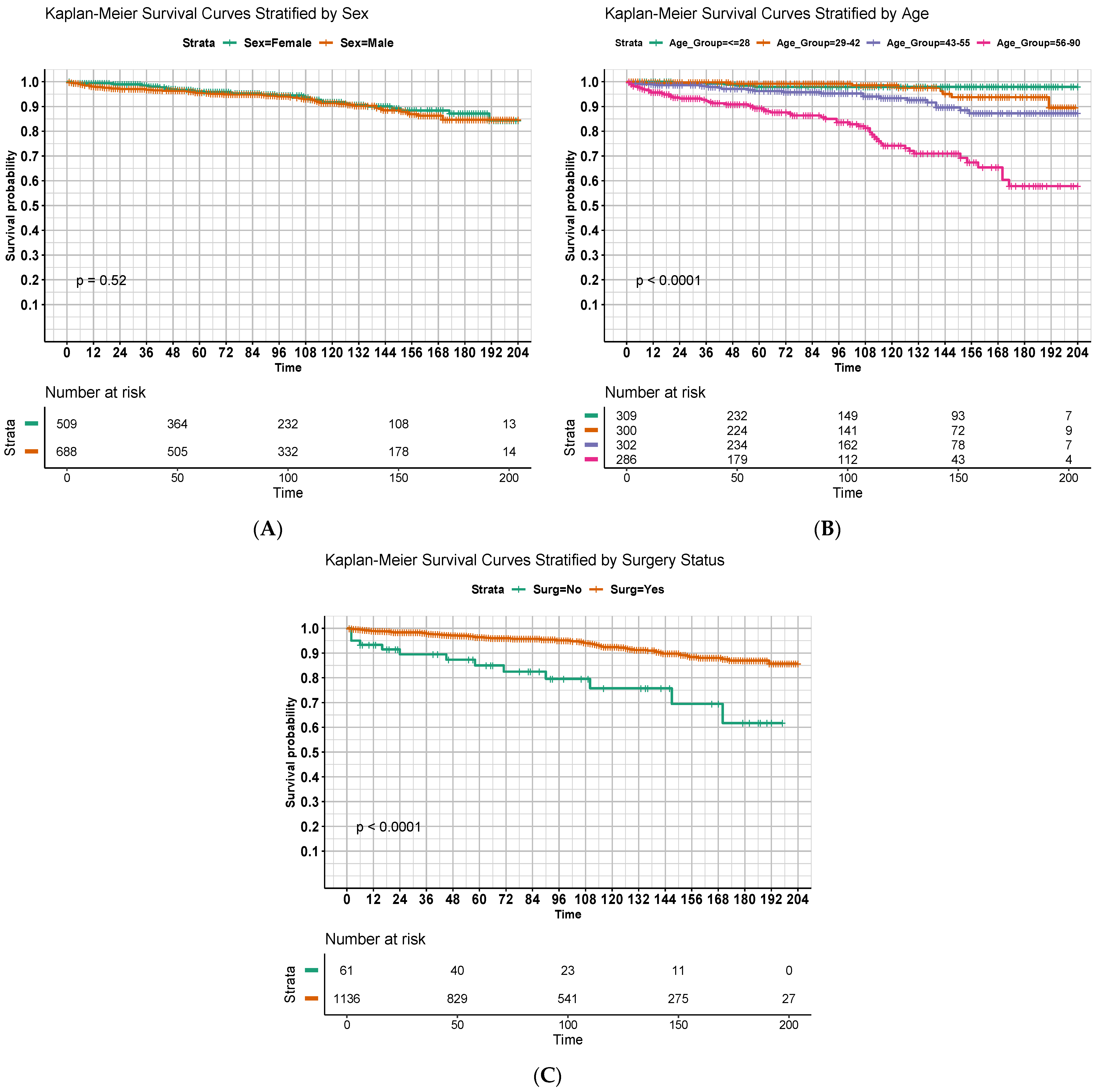
3.2. Survival Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sonneland, P.R.; Scheithauer, B.W.; Onofrio, B.M. Myxopapillary Ependymoma. A Clinicopathologic and Immunocytochemical Study of 77 Cases. Cancer 1985, 56, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Kanno, H.; Kanetsuna, Y.; Shinonaga, M. Anaplastic Myxopapillary Ependymoma: A Case Report and Review of Literature. World J. Clin. Oncol. 2021, 12, 1072–1082. [Google Scholar] [CrossRef] [PubMed]
- Bates, J.E.; Peterson, C.R.; Yeaney, G.A.; Walter, K.A.; Lundquist, T.; Rosenzweig, D.; Milano, M.T. Spinal Drop Metastasis in Myxopapillary Ependymoma: A Case Report and a Review of Treatment Options. Rare Tumors 2014, 6, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Kraetzig, T.; McLaughlin, L.; Bilsky, M.H.; Laufer, I. Metastases of Spinal Myxopapillary Ependymoma: Unique Characteristics and Clinical Management. J. Neurosurg. Spine 2018, 28, 201–208. [Google Scholar] [CrossRef]
- Fassett, D.R.; Pingree, J.; Kestle, J.R.W. The High Incidence of Tumor Dissemination in Myxopapillary Ependymoma in Pediatric Patients: Report of Five Cases and Review of the Literature. J. Neurosurg. Pediatr. 2005, 102, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.R.; VanLandingham, M.; O’Brien, T.; Boop, F.A.; Arnautović, K. Primary Seeding of Myxopapillary Ependymoma: Different Disease in Adult Population? Case Report and Review of Literature. World Neurosurg. 2017, 99, 812.e21–812.e26. [Google Scholar] [CrossRef]
- Batich, K.A.; Riedel, R.F.; Kirkpatrick, J.P.; Tong, B.C.; Eward, W.C.; Tan, C.L.; Pittman, P.D.; McLendon, R.E.; Peters, K.B. Recurrent Extradural Myxopapillary Ependymoma with Oligometastatic Spread. Front. Oncol. 2019, 9, 1322. [Google Scholar] [CrossRef]
- Bockmayr, M.; Harnisch, K.; Pohl, L.C.; Schweizer, L.; Mohme, T.; Körner, M.; Alawi, M.; Suwala, A.K.; Dorostkar, M.M.; Monoranu, C.M.; et al. Comprehensive Profiling of Myxopapillary Ependymomas Identifies a Distinct Molecular Subtype with Relapsing Disease. Neuro Oncol. 2022, 24, 1689–1699. [Google Scholar] [CrossRef]
- Nakamura, M.; Ishii, K.; Watanabe, K.; Tsuji, T.; Matsumoto, M.; Toyama, Y.; Chiba, K. Long-Term Surgical Outcomes for Myxopapillary Ependymomas of the Cauda Equina. Spine 2009, 34, E756–E760. [Google Scholar] [CrossRef] [PubMed]
- Bagley, C.A.; Wilson, S.; Kothbauer, K.F.; Bookland, M.J.; Epstein, F.; Jallo, G.I. Long Term Outcomes Following Surgical Resection of Myxopapillary Ependymomas. Neurosurg. Rev. 2009, 32, 321–334; discussion 334. [Google Scholar] [CrossRef]
- Montero, A.-S.; Tran, S.; Amelot, A.; Berriat, F.; Lot, G.; Gaillard, S.; Villa, C.; Polivka, M.; Adam, C.; Idbaih, A.; et al. Clinical Characteristics and Long-Term Surgical Outcome of Spinal Myxopapillary Ependymoma: A French Cohort of 101 Patients. J. Neuro-Oncol. 2021, 152, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Scarpelli, D.B.; Turina, C.B.; Kelly, P.D.; Khudanyan, A.; Jaboin, J.J.; McClelland, S. National Trends in Management of Adult Myxopapillary Ependymomas. J. Clin. Neurosci. 2020, 73, 162–167. [Google Scholar] [CrossRef]
- Abdulaziz, M.; Mallory, G.W.; Bydon, M.; De la Garza Ramos, R.; Ellis, J.A.; Laack, N.N.; Marsh, W.R.; Krauss, W.E.; Jallo, G.; Gokaslan, Z.L.; et al. Outcomes Following Myxopapillary Ependymoma Resection: The Importance of Capsule Integrity. Neurosurg. Focus 2015, 39, E8. [Google Scholar] [CrossRef] [PubMed]
- Jahanbakhshi, A.; Najafi, M.; Jafari, F.; Moshtaghian, M.; Gomar, M.; Anbarlouei, M.; Naderi, S. Adjunctive Treatment of Myxopapillary Ependymoma. Oncol. Rev. 2021, 15, 518. [Google Scholar] [CrossRef]
- Bates, J.E.; Choi, G.; Milano, M.T. Myxopapillary Ependymoma: A SEER Analysis of Epidemiology and Outcomes. J. Neuro-Oncol. 2016, 129, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Doll, K.M.; Rademaker, A.; Sosa, J.A. Practical Guide to Surgical Data Sets: Surveillance, Epidemiology, and End Results (SEER) Database. JAMA Surg. 2018, 153, 588. [Google Scholar] [CrossRef]
- Schemper, M.; Smith, T.L. A Note on Quantifying Follow-up in Studies of Failure Time. Control Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Kukreja, S.; Ambekar, S.; Sharma, M.; Sin, A.H.; Nanda, A. Outcome Predictors in the Management of Spinal Myxopapillary Ependymoma: An Integrative Survival Analysis. World Neurosurg. 2015, 83, 852–859. [Google Scholar] [CrossRef]
- Cimino, P.J.; Agarwal, A.; Dehner, L.P. Myxopapillary Ependymoma in Children: A Study of 11 Cases and a Comparison with the Adult Experience. Pediatr. Blood Cancer 2014, 61, 1969–1971. [Google Scholar] [CrossRef] [PubMed]
- Omerhodžić, I. Myxopapillary Ependymoma of the Spinal Cord in Adults: A Report of Personal Series and Review of Literature. Acta Clin. Croat. 2020, 59, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Stephen, J.H.; Sievert, A.J.; Madsen, P.J.; Judkins, A.R.; Resnick, A.C.; Storm, P.B.; Rushing, E.J.; Santi, M. Spinal Cord Ependymomas and Myxopapillary Ependymomas in the First 2 Decades of Life: A Clinicopathological and Immunohistochemical Characterization of 19 Cases: Clinical Article. J. Neurosurg. Pediatr. 2012, 9, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Kucia, E.J.; Maughan, P.H.; Kakarla, U.K.; Bambakidis, N.C.; Spetzler, R.F. Surgical Technique and Outcomes in the Treatment of Spinal Cord Ependymomas: Part II: Myxopapillary Ependymoma. Oper. Neurosurg. 2011, 68, ons90–ons94. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, M.C.; Sandhu, M.R.S.; Teferi, N.; Noeller, J.L.; Rosinski, C.L.; Park, B.J.; Menezes, A.H.; Nourski, K.V.; Hitchon, P.W. Surgical Outcomes and Risk Factors for Recurrence of Myxopapillary Ependymoma: A Single-Center Experience. J. Neurosurg. Spine 2023, 39, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Zhou, J.; Zheng, Y.; Liu, S.; Tang, Z.; Wang, Y. Clinical Features, Treatments, and Prognostic Factors of Spinal Myxopapillary Ependymoma. World Neurosurg. 2021, 149, e1105–e1111. [Google Scholar] [CrossRef] [PubMed]
- Boström, A.; Von Lehe, M.; Hartmann, W.; Pietsch, T.; Feuss, M.; Boström, J.P.; Schramm, J.; Simon, M. Surgery for Spinal Cord Ependymomas: Outcome and Prognostic Factors. Neurosurgery 2011, 68, 302–309. [Google Scholar] [CrossRef]
- Zhang, Y.-W.; Wang, B.; An, S.-Y.; Liu, W.-H.; Wang, C.; Yan, H.; Xu, Y.-L.; Wang, Y.-Z.; Jia, W.-Q. Clinical Management and Prognosis of Spinal Myxopapillary Ependymoma: A Single-Institution Cohort of 72 Patients. Eur. Spine J. 2023, 32, 2459–2467. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.J.; Wang, Y.; Allen, P.K.; Mahajan, A.; McCutcheon, I.E.; Rao, G.; Rhines, L.D.; Tatsui, C.E.; Armstrong, T.S.; Maor, M.H.; et al. Outcomes After Surgery and Radiotherapy for Spinal Myxopapillary Ependymoma: Update of the MD Anderson Cancer Center Experience. Neurosurgery 2014, 75, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.C.; Wang, Y.; Miller, R.; Villà, S.; Zaucha, R.; Pica, A.; Poortmans, P.; Anacak, Y.; Ozygit, G.; Baumert, B.; et al. Long-Term Outcome of Patients with Spinal Myxopapillary Ependymoma: Treatment Results from the MD Anderson Cancer Center and Institutions from the Rare Cancer Network. Neuro Oncol. 2015, 17, 588–595. [Google Scholar] [CrossRef]
- Pica, A.; Miller, R.; Villà, S.; Kadish, S.P.; Anacak, Y.; Abusaris, H.; Ozyigit, G.; Baumert, B.G.; Zaucha, R.; Haller, G.; et al. The Results of Surgery, with or without Radiotherapy, for Primary Spinal Myxopapillary Ependymoma: A Retrospective Study from the Rare Cancer Network. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1114–1120. [Google Scholar] [CrossRef] [PubMed]
- Huynh, T.R.; Lu, C.; Drazin, D.; Lekovic, G. Myxopapillary Ependymoma with Anaplastic Features: A Case Report with Review of the Literature. Surg. Neurol. Int. 2018, 9, 191. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Count (%) | |
|---|---|
| n = 1197 | |
| Age in years (median [IQR]) | 42.00 [28.00, 55.00] |
| Sex | |
| Female | 509 (42.5) |
| Male | 688 (57.5) |
| Year of Diagnosis | 81 (6.8) |
| 2004 | 77 (6.4) |
| 2005 | 78 (6.5) |
| 2006 | 67 (5.6) |
| 2007 | 71 (5.9) |
| 2008 | 61 (5.1) |
| 2009 | 76 (6.3) |
| 2010 | 79 (6.6) |
| 2011 | 73 (6.1) |
| 2012 | 63 (5.3) |
| 2013 | 69 (5.8) |
| 2014 | 73 (6.1) |
| 2015 | 69 (5.8) |
| 2016 | 61 (5.1) |
| 2017 | 66 (5.5) |
| 2018 | 71 (5.9) |
| 2019 | 62 (5.2) |
| 2020 | 58 (5.1) |
| Race | |
| American Indian Alaska Native | 12 (1.0) |
| Asian or Pacific Islander | 59 (4.9) |
| Black | 50 (4.2) |
| White | 1076 (89.9) |
| Marital Status | |
| Unmarried | 558 (46.6) |
| Married | 639 (53.4) |
| Income | |
| <USD 70,000 | 538 (41.9) |
| USD 70,000 or more | 659 (55.1) |
| City Population Size | |
| <1 million | 538 (44.9) |
| 1 million or more | 696 (58.1) |
| Receipt of Surgery | |
| No | 61 (5.1) |
| Yes | 1136 (94.9) |
| Sex | Receipt of Surgery | |||||
|---|---|---|---|---|---|---|
| Female (%) | Male (%) | p Value | No Surgery (%) | Surgery (%) | p Value | |
| n = 509 | n = 688 | n = 61 | n = 1136 | |||
| Age in years (median [IQR]) | 45.00 [29.00, 57.00] | 40.00 [28.00, 53.00] | 0.004 | 53.00 [37.00, 64.00] | 41.00 [28.00, 54.00] | <0.001 |
| Sex | ||||||
| Female | -- | -- | 25 (41) | 484 (42.6) | ||
| Male | -- | -- | 36 (59) | 652 (57.4) | ||
| Year of Diagnosis | 0.624 | 0.222 | ||||
| 2004 | 35 (6.9) | 46 (6.7) | 2 (3.3) | 79 (7.0) | ||
| 2005 | 28 (5.5) | 49 (7.1) | 6 (9.8) | 71 (6.2) | ||
| 2006 | 36 (7.1) | 42 (6.1) | 6 (9.8) | 72 (6.3) | ||
| 2007 | 24 (4.7) | 43 (6.2) | 2 (3.3) | 65 (5.7) | ||
| 2008 | 32 (6.3) | 39 (5.7) | 2 (3.3) | 69 (6.1) | ||
| 2009 | 26 (5.1) | 35 (5.1) | 7 (11.5) | 54 (4.8) | ||
| 2010 | 32 (6.3) | 44 (6.4) | 0 (0.0) | 76 (6.7) | ||
| 2011 | 30 (5.9) | 49 (7.1) | 3 (4.9) | 76 (6.7) | ||
| 2012 | 35 (6.9) | 38 (5.5) | 4 (6.6) | 69 (6.1) | ||
| 2013 | 29 (5.7) | 34 (4.9) | 6 (9.8) | 57 (5.0) | ||
| 2014 | 33 (6.5) | 36 (5.2) | 3 (4.9) | 66 (5.8) | ||
| 2015 | 31 (6.1) | 42 (6.1) | 3 (4.9) | 70 (6.2) | ||
| 2016 | 25 (4.9) | 44 (6.4) | 3 (4.9) | 66 (5.8) | ||
| 2017 | 29 (5.7) | 32 (4.7) | 4 (6.6) | 57 (5.0) | ||
| 2018 | 36 (7.1) | 30 (4.4) | 1 (1.6) | 65 (5.7) | ||
| 2019 | 25 (4.9) | 46 (6.7) | 5 (8.2) | 66 (5.8) | ||
| 2020 | 23 (4.5) | 39 (5.7) | 4 (6.6) | 58 (5.1) | ||
| Race | 0.476 | 0.631 | ||||
| American Indian Alaska Native | 7 (1.4) | 5 (0.7) | 0 (0.0) | 12 (1.1) | ||
| Asian or Pacific Islander | 29 (5.7) | 30 (4.4) | 3 (4.9) | 56 (4.9) | ||
| Black | 22 (4.3) | 28 (4.1) | 1 (1.6) | 49 (4.3) | ||
| White | 451 (88.6) | 625 (90.8) | 57 (93.4) | 1019 (89.7) | ||
| Marital Status | 0.466 | 0.193 | ||||
| Unmarried | 244 (47.9) | 314 (45.6) | 23 (37.7) | 535 (47.1) | ||
| Married | 265 (52.1) | 374 (54.4) | 38 (62.3) | 601 (52.9) | ||
| Income | 0.9 | 0.613 | ||||
| <USD 70,000 | 229 (45) | 314 (45.6) | 25 (41) | 513 (45.2) | ||
| USD 70,000 or more | 280 (55) | 374 (54.4) | 36 (59) | 623 (54.8) | ||
| City Population Size | 0.085 | 0.18 | ||||
| <1 million | 198 (38.9) | 303 (44) | 20 (32.8) | 481 (42.3) | ||
| 1 million or more | 311 (61.1) | 385 (56) | 41 (67.2) | 655 (57.7) | ||
| Receipt of Surgery | 0.907 | |||||
| No | 25 (4.9) | 36 (5.2) | -- | -- | ||
| Yes | 484 (95.1) | 652 (94.8) | -- | -- | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Rooney, M.K.; Alvarez-Breckenridge, C.; Beckham, T.H.; Chung, C.; De, B.S.; Ghia, A.J.; Grosshans, D.; Majd, N.K.; McAleer, M.F.; et al. Outcomes and Pattern of Care for Spinal Myxopapillary Ependymoma in the Modern Era—A Population-Based Observational Study. Cancers 2024, 16, 2013. https://doi.org/10.3390/cancers16112013
Wang C, Rooney MK, Alvarez-Breckenridge C, Beckham TH, Chung C, De BS, Ghia AJ, Grosshans D, Majd NK, McAleer MF, et al. Outcomes and Pattern of Care for Spinal Myxopapillary Ependymoma in the Modern Era—A Population-Based Observational Study. Cancers. 2024; 16(11):2013. https://doi.org/10.3390/cancers16112013
Chicago/Turabian StyleWang, Chenyang, Michael K. Rooney, Christopher Alvarez-Breckenridge, Thomas H. Beckham, Caroline Chung, Brian S. De, Amol J. Ghia, David Grosshans, Nazanin K. Majd, Mary F. McAleer, and et al. 2024. "Outcomes and Pattern of Care for Spinal Myxopapillary Ependymoma in the Modern Era—A Population-Based Observational Study" Cancers 16, no. 11: 2013. https://doi.org/10.3390/cancers16112013
APA StyleWang, C., Rooney, M. K., Alvarez-Breckenridge, C., Beckham, T. H., Chung, C., De, B. S., Ghia, A. J., Grosshans, D., Majd, N. K., McAleer, M. F., McGovern, S. L., North, R. Y., Paulino, A. C., Perni, S., Reddy, J. P., Rhines, L. D., Swanson, T. A., Tatsui, C. E., Tom, M. C., ... Li, J. (2024). Outcomes and Pattern of Care for Spinal Myxopapillary Ependymoma in the Modern Era—A Population-Based Observational Study. Cancers, 16(11), 2013. https://doi.org/10.3390/cancers16112013