

The Prognostic Role of BRD4 Expression in High-Grade Serous Ovarian Cancer
 , , , ,
, , , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials
3. Methods
3.1. One-Step RT-qPCR
| Gene | Primer | Sequence 5′→3′ | References |
| BRD4 | BRD4_F | CCATGGACATGAGCACAATC | Wu T et al., 2015 [11] |
| BRD4_R | TGGAGAACATCAATCGGACA | ||
| GAPDH | GAPDH_F | TTCACCACCATGGAGAAGGC | |
| GAPDH_R | CCCTTTTGGCTCCACCCT |
| Reaction Kit | Concentration |
| Primer (Forward) 10 pmol | 200 nM |
| Primer (Reverse) 10 pmol | 200 nM |
| dUTP (10 mM) | 0.2 mM |
| KAPA SYBR FAST qPCR Master Mix 2Χ | 1× |
| 50X KAPA RT Mix | 1× |
| RNA template | 75 ng |
| ddH2O | Up to 10 μL |
3.2. Protein Isolation from Ascitic Cancer Cells
3.3. Protein Quantification with ELISA
4. Statistical Analysis
5. Results
5.1. Clinicopathological Characteristics
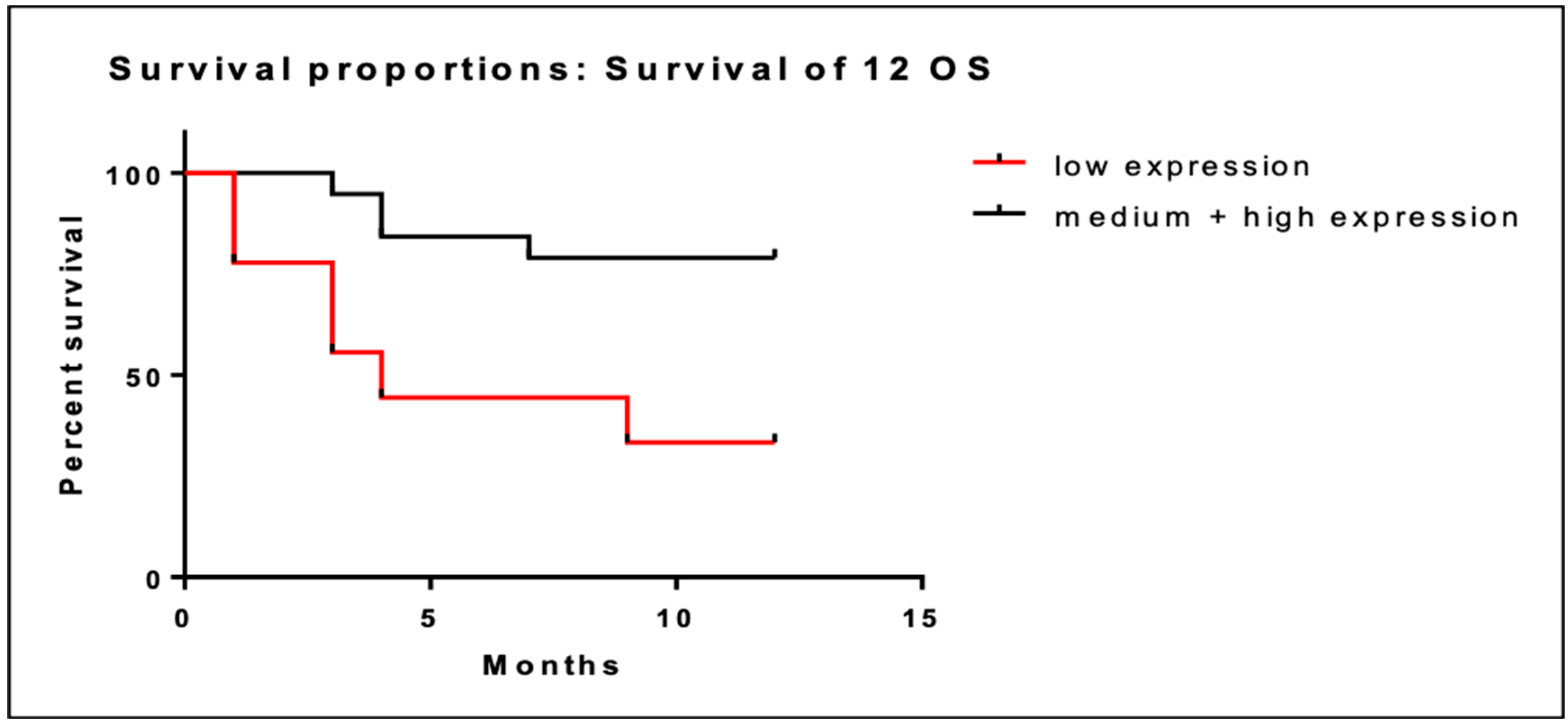
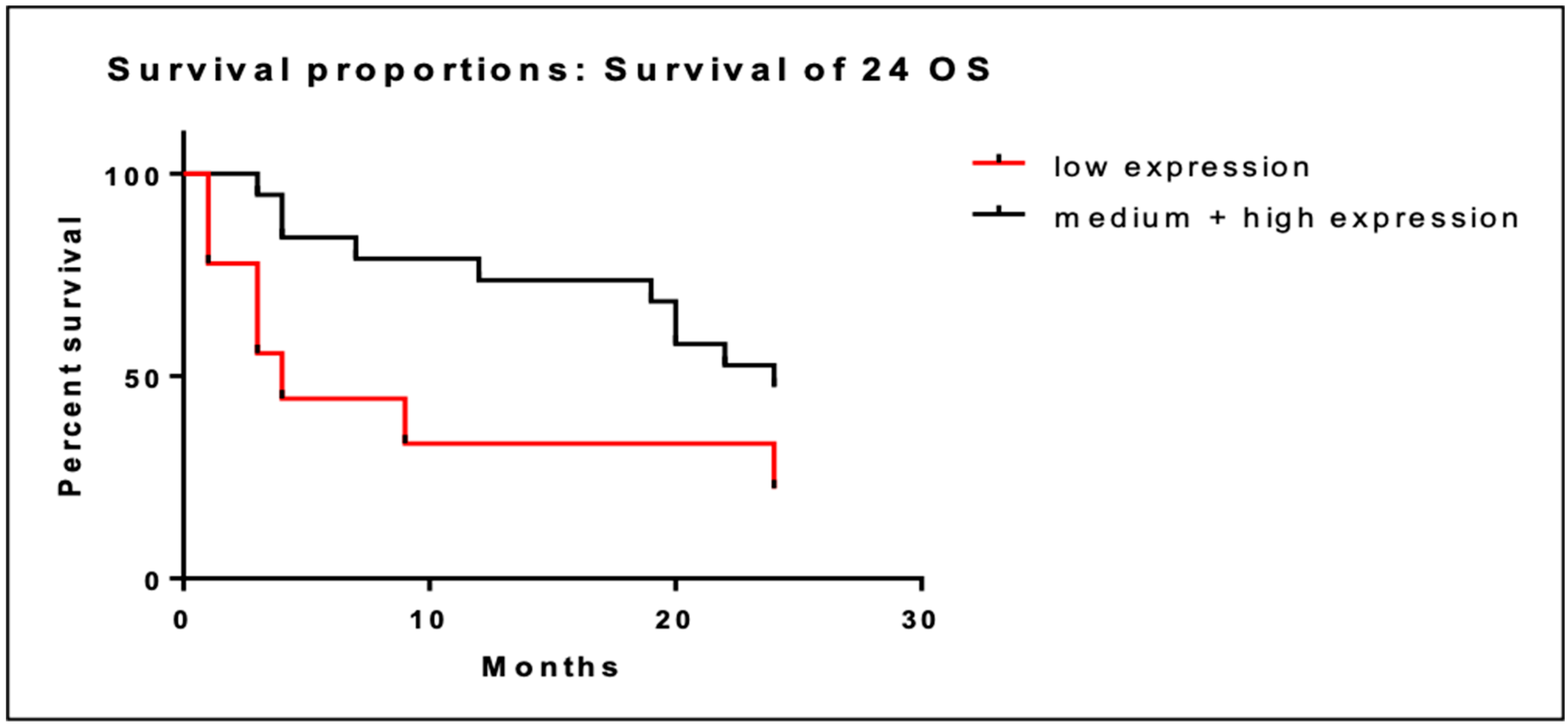
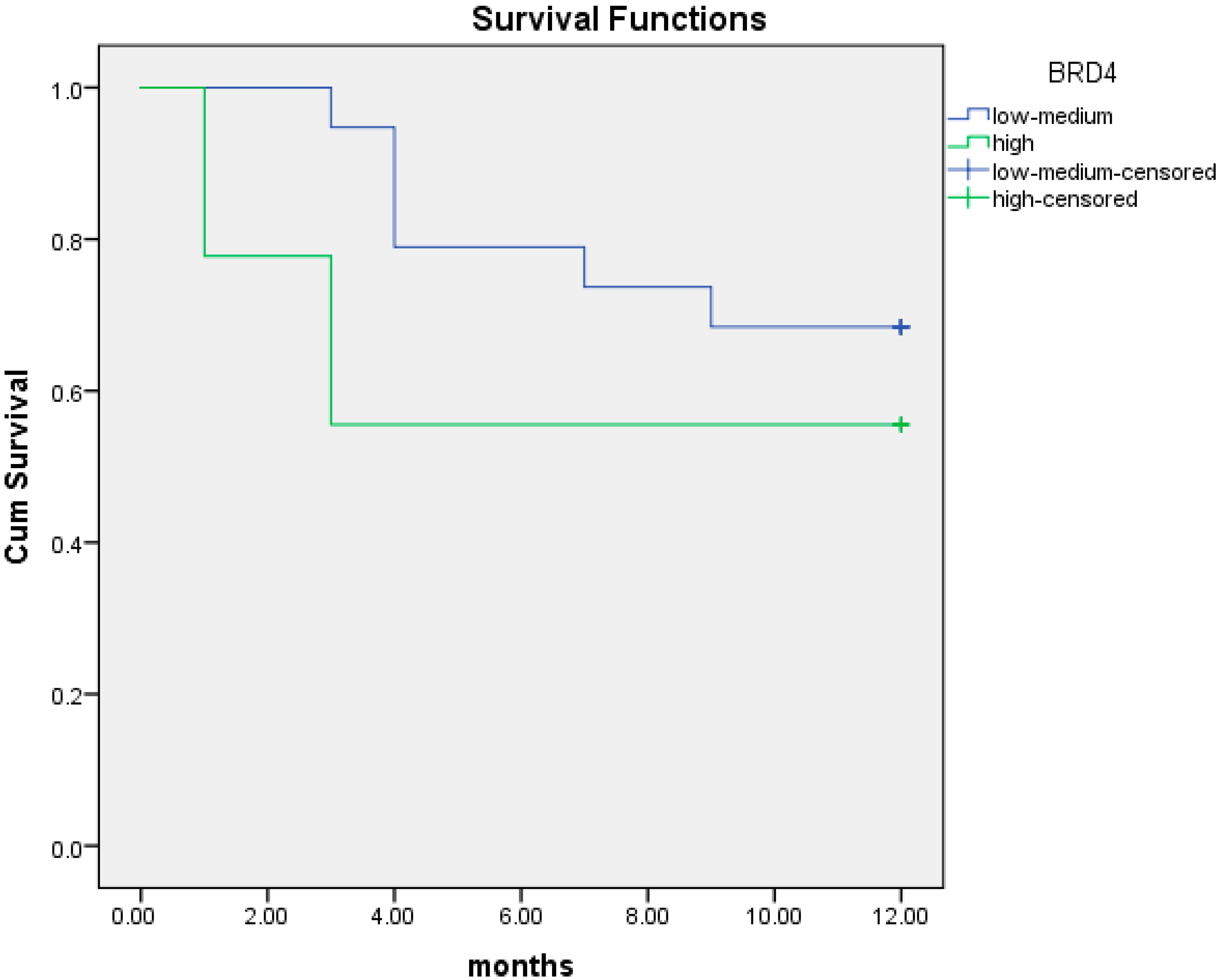
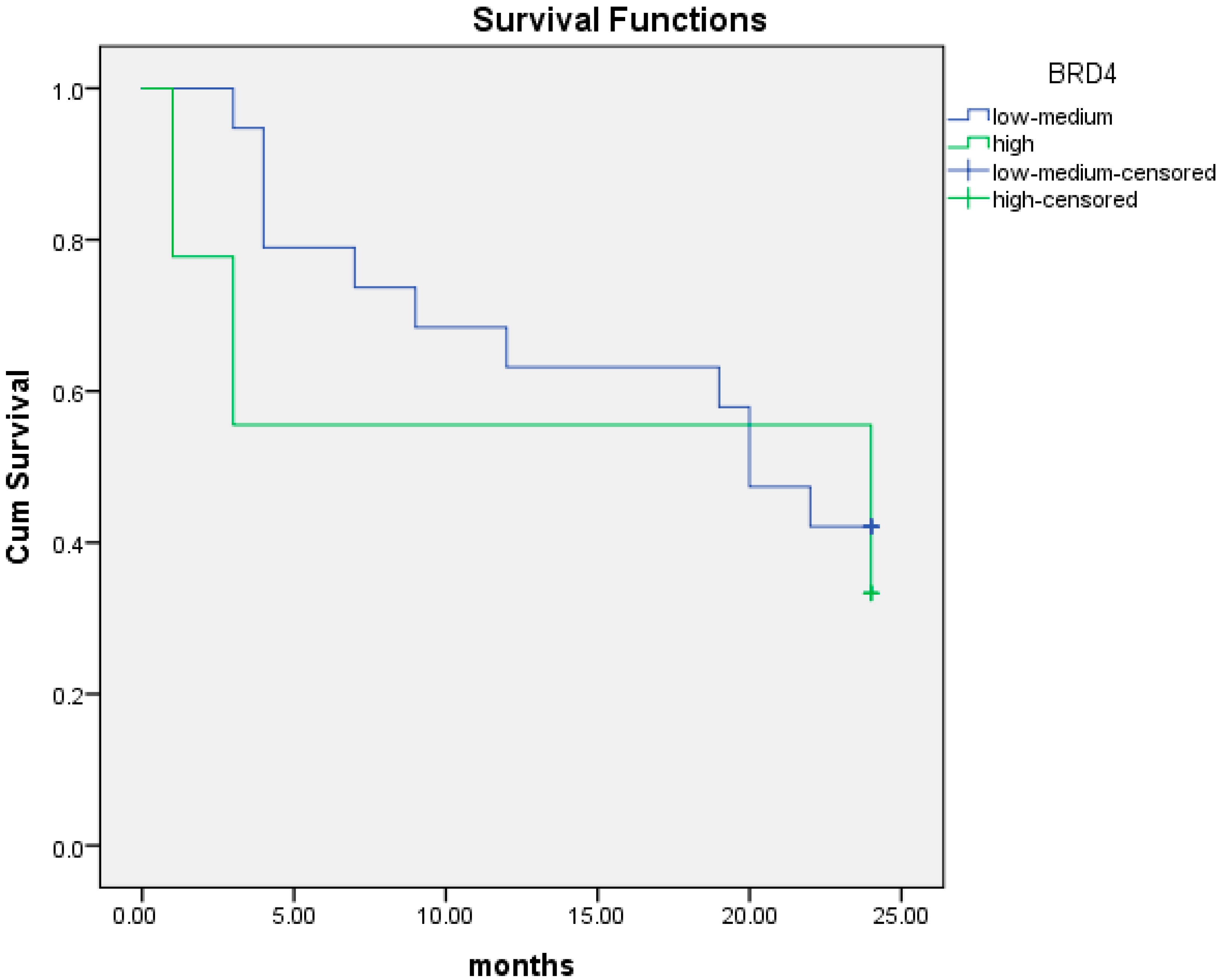
5.2. BRD4 Gene Expression and Overall Survival (OS)
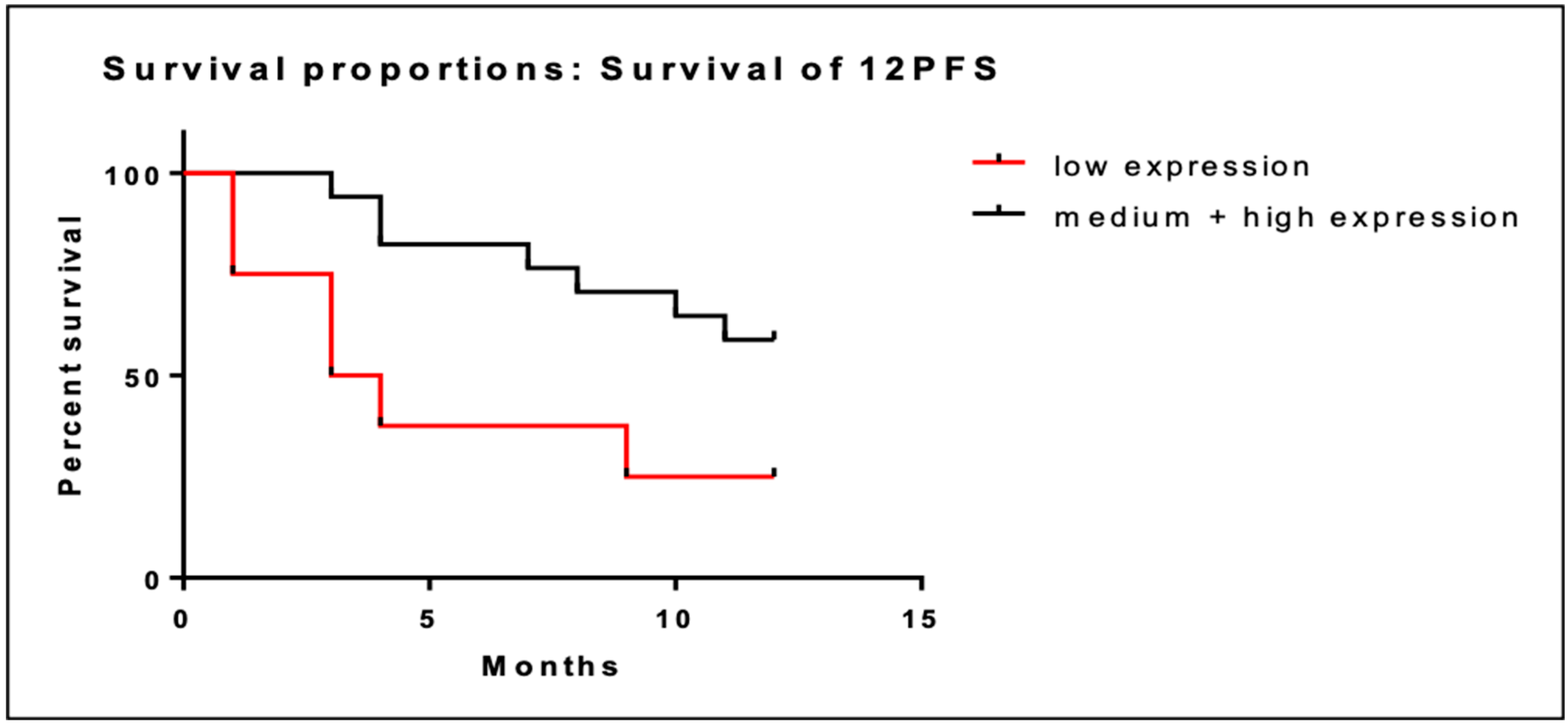
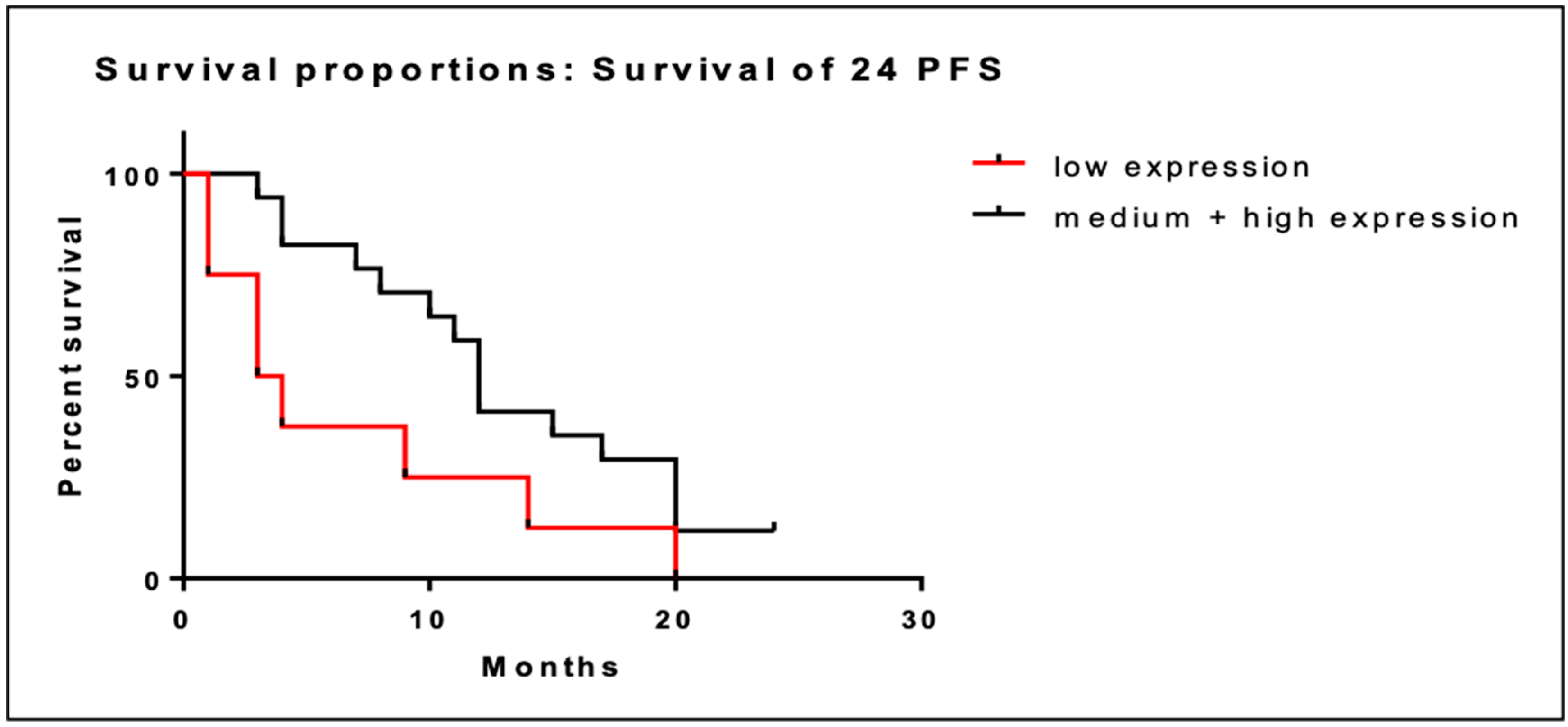
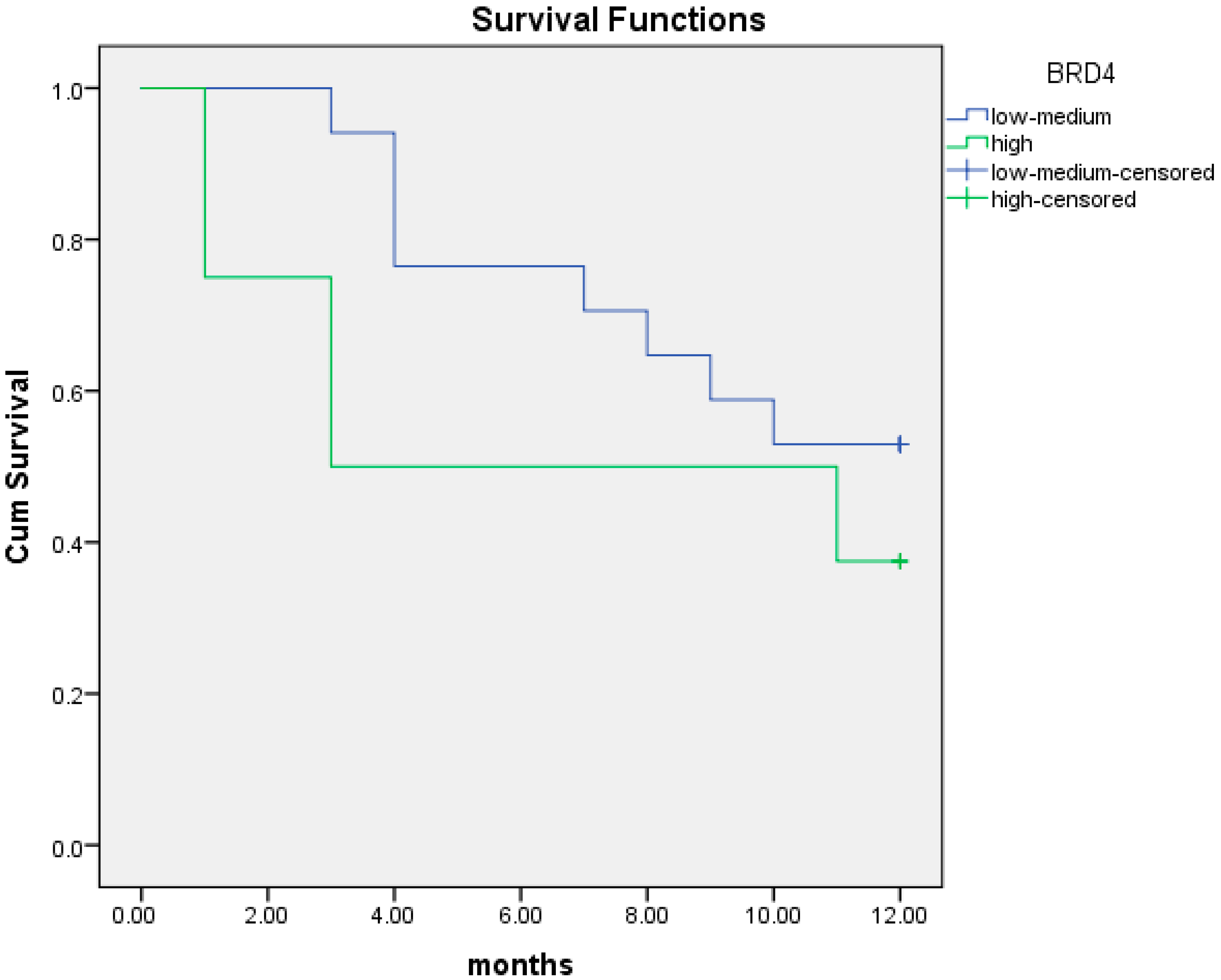
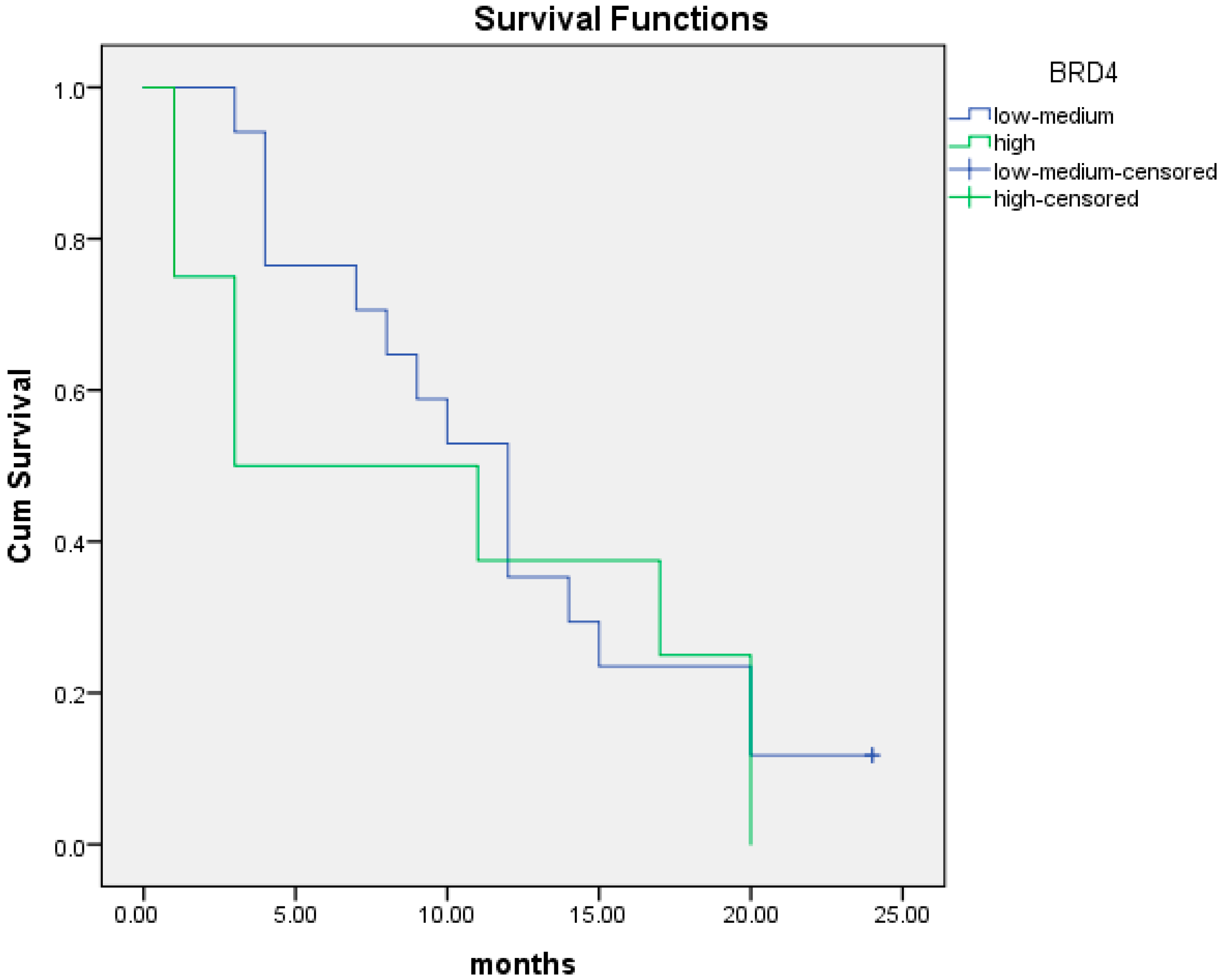
5.3. BRD4 Gene Expression and Progression-Free Survival (PFS)
5.4. BRD4 Protein Expression and Overall Survival
5.5. BRD4 Protein Expression and Progression-Free Survival
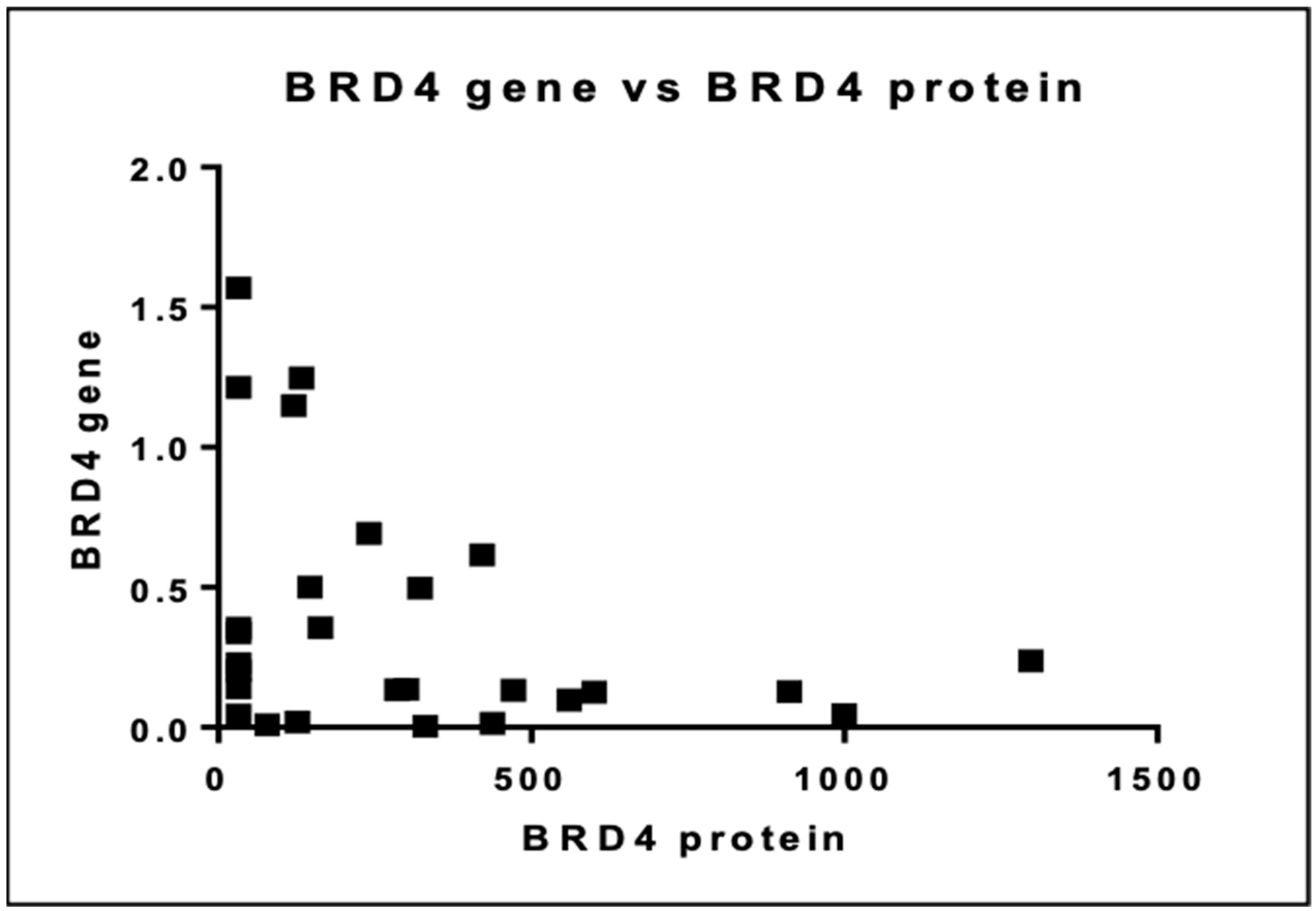
5.6. Association between BRD4 Gene and Protein Expression
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Today. Available online: https://gco.iarc.who.int/today/en/dataviz/tables?mode=cancer&sexes=2&group_populations=1&populations=991_992_993_994_995_996&multiple_populations=1 (accessed on 25 February 2024).
- Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow/graphic-isotype?type=1&type_sex=0&mode=population&sex=2&populations=900&cancers=25&age_group=value&apc_male=0&apc_female=0&single_unit=50000&print=0 (accessed on 4 May 2020).
- Bell, D.; Berchuck, A.; Birrer, M.; Chien, J.; Cramer, D.W.; Dao, F.; Dhir, R.; DiSaia, P.; Gabra, H.; Glenn, P.; et al. Integrated genomic analyses of ovarian carcinoma. Nature 2011, 474, 609–615. [Google Scholar]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Liyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, B.; Shapira-Frommer, R.; Schmutzler, R.K.; Audeh, M.W.; Friedlander, M.; Balmaña, J.; Mitchell, G.; Fried, G.; Stemmer, S.M.; Hubert, A.; et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J. Clin. Oncol. 2015, 33, 244–250. [Google Scholar] [CrossRef]
- Waddington, C.H. The Epigenotype. Int. J. Epidemiol. 2012, 41, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Filippakopoulos, P.; Qi, J.; Picaud, S.; Shen, Y.; Smith, W.B.; Fedorov, O.; Morse, E.M.; Keates, T.; Hickman, T.T.; Felletar, I.; et al. Selective inhibition of BET bromodomains. Nature 2010, 468, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Rhyasen, G.W.; Yao, Y.; Zhang, J.; Dulak, A.; Castriotta, L.; Jacques, K.; Zhao, W.; Gharahdaghi, F.; Hattersley, M.M.; Lyne, P.D.; et al. BRD4 amplification facilitates an oncogenic gene expression program in high-grade serous ovarian cancer and confers sensitivity to BET inhibitors. PLoS ONE 2018, 13, e0200826. [Google Scholar] [CrossRef]
- Wang, Z.Q.; Zhang, Z.C.; Wu, Y.Y.; Pi, Y.N.; Lou, S.H.; Liu, T.B.; Lou, G.; Yang, C. Bromodomain and extraterminal (BET) proteins: Biological functions, diseases, and targeted therapy. Signal Transduct. Target. Ther. 2023, 8, 420. [Google Scholar] [CrossRef]
- Andrikopoulou, A.; Liontos, M.; Koutsoukos, K.; Dimopoulos, M.A.; Zagouri, F. Clinical perspectives of BET inhibition in ovarian cancer. Cell. Oncol. 2021, 44, 237–249. [Google Scholar] [CrossRef]
- Wu, T.; Pinto, H.B.; Kamikawa, Y.F.; Donohoe, M.E. The BET family member BRD4 interacts with OCT4 and regulates pluripotency gene expression. Stem Cell Rep. 2015, 4, 390–403. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Maenpaa, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, Y.; Shan, W.; Hu, Z.; Yuan, J.; Pi, J.; Wang, Y.; Fan, L.; Tang, Z.; Li, C.; et al. Repression of BET activity sensitizes homologous recombination-proficient cancers to PARP inhibition. Sci. Transl. Med. 2017, 9, eaal1645. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Zhu, H.; Lee, J.H.; Kossenkov, A.V.; Wu, S.Y.; Wickramasinghe, J.M.; Yin, X.; Palozola, K.C.; Gardini, A.; Showe, L.C.; et al. BET inhibitors suppress ALDH activity by targeting ALDH1A1 super-enhancer in ovarian cancer. Cancer Res. 2016, 76, 6320–6330. [Google Scholar] [CrossRef]
- Li, G.-Q.; Guo, W.-Z.; Zhang, Y.; Seng, J.-J.; Zhang, H.-P.; Ma, X.-X.; Zhang, G.; Li, J.; Yan, B.; Tang, H.-W.; et al. Suppression of BRD4 inhibits human hepatocellular carcinoma by repressing MYC and enhancing BIM expression. Oncotarget 2015, 7, 2462–2474. [Google Scholar] [CrossRef]
- Suzuki, C.; Yamada, A.; Adachi, S.; Shima, H.; Kida, K.; Oshi, M.; Sugae, S.; Yamamoto, S.; Narui, K.; Tanabe, M.; et al. Bromodomain-containing Protein 4 Is a Favourable Prognostic Factor in Breast Cancer Patients. Anticancer Res. 2021, 41, 3597–3606. [Google Scholar] [CrossRef]
- Petersen, S.; Wilson, A.J.; Hirst, J.; Roby, K.F.; Fadare, O.; Crispens, M.A.; Beeghly-Fadiel, A.; Khabele, D. CCNE1 and BRD4 co-amplification in high-grade serous ovarian cancer is associated with poor clinical outcomes. Gynecol. Oncol. 2020, 157, 405. [Google Scholar] [CrossRef]
- Ucar, D.; Lin, D.I. Amplification of the bromodomain-containing protein 4 gene in ovarian high-grade serous carcinoma is associated with worse prognosis and survival. Mol. Clin. Oncol. 2015, 3, 1291–1294. [Google Scholar] [CrossRef]
- Goundiam, O.; Gestraud, P.; Popova, T.; De la Motte Rouge, T.; Fourchotte, V.; Gentien, D.; Hupe, P.; Becette, V.; Houdayer, C.; Roman-Roman, S.; et al. Histo-genomic stratification reveals the frequent amplification/overexpression of CCNE 1 and BRD 4 genes in non-BRCAness high grade ovarian carcinoma. Int. J. Cancer 2015, 137, 1890–1900. [Google Scholar] [CrossRef]
- Sung, C.O.; Song, I.H.; Sohn, I. A distinctive ovarian cancer molecular subgroup characterized by poor prognosis and somatic focal copy number amplifications at chromosome 19. Gynecol. Oncol. 2014, 132, 343–350. [Google Scholar] [CrossRef]
- George, J.; Alsop, K.; Etemadmoghadam, D.; Hondow, H.; Mikeska, T.; Dobrovic, A.; de Fazio, A.; Smyth, G.K.; Levine, D.A.; Mitchell, G.; et al. Nonequivalent gene expression and copy number alterations in high-grade serous ovarian cancers with BRCA1 and BRCA2 mutations. Clin Cancer Res. 2013, 19, 3474–3484. [Google Scholar] [CrossRef]
- Zhang, Z.; Ma, P.; Jing, Y.; Yan, Y.; Cai, M.C.; Zhang, M.; Zhang, S.; Peng, H.; Ji, Z.-L.; Di, W.; et al. BET bromodomain inhibition as a therapeutic strategy in ovarian cancer by downregulating foxm1. Theranostics 2016, 6, 219–230. [Google Scholar] [CrossRef]
- Wu, S.Y.; Lee, C.F.; Lai, H.T.; Yu, C.T.; Lee, J.E.; Zuo, H.; Tsai, S.Y.; Tsai, M.-J.; Ge, K.; Wan, Y.; et al. Opposing Functions of BRD4 Isoforms in Breast Cancer. Mol. Cell 2020, 78, 1114–1132.e10. [Google Scholar] [CrossRef]
- Drumond-Bock, A.L.; Bieniasz, M. The role of distinct BRD4 isoforms and their contribution to high-grade serous ovarian carcinoma pathogenesis. Mol. Cancer 2021, 20, 145. [Google Scholar] [CrossRef]
- Alsarraj, J.; Faraji, F.; Geiger, T.R.; Mattaini, K.R.; Williams, M.; Wu, J.; Ha, N.-H.; Merlino, T.; Walker, R.C.; Bosley, A.D.; et al. BRD4 Short Isoform Interacts with RRP1B, SIPA1 and Components of the LINC Complex at the Inner Face of the Nuclear Membrane. PLoS ONE 2013, 8, e80746. [Google Scholar] [CrossRef]
- Ana Luiza, D.-B.; Luyao, W.; Lin, W.; Magdalena, C.; Maria, R.; Michael, K.; Magdalena, B. Increased expression of BRD4 isoforms long (BRD4-L) and short (BRD4-S) promotes chemotherapy resistance in high-grade serous ovarian carcinoma. Genes Cancer 2023, 14, 56–76. [Google Scholar] [CrossRef]
- Liu, N.; Ling, R.; Tang, X.; Yu, Y.; Zhou, Y.; Chen, D. Post-Translational Modifications of BRD4: Therapeutic Targets for Tumor. Front. Oncol. 2022, 12, 1. [Google Scholar] [CrossRef]
- Sanz-Álvarez, M.; Cristóbal, I.; Luque, M.; Santos, A.; Zazo, S.; Madoz-Gúrpide, J.; Carames, C.; Chiang, C.-M.; Garcia-Foncillas, J.; Eroles, P.; et al. Expression of Phosphorylated BRD4 Is Markedly Associated with the Activation Status of the PP2A Pathway and Shows a Strong Prognostic Value in Triple Negative Breast Cancer Patients. Cancers 2021, 13, 1246. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total N = 28, n (%) |
|---|---|
| Age at diagnosis, median (range), years | 66 (42–86) |
| Histology | |
| High-Grade Serous carcinoma | 28 (100%) |
| Other | 0 (0) |
| Initial Stage (FIGO) | |
| IIIC | 28 (100%) |
| IV | 0 (0) |
| Family History | |
| Yes | 7 (25%) |
| No | 21 (75%) |
| Debulking Surgery | |
| Primary Debulking Surgery | 10 (36%) |
| Interval Debulking Surgery | 12 (43%) |
| No surgery | 6 (21%) |
| ECOG Performance status | |
| 0/1 | 25 (89%) |
| 2/3 | 3 (11%) |
| Progression-free survival on first-line chemotherapy, median (range), months | 11 (1–33) |
| Sites at relapse | |
| Peritoneum | 20 (71%) |
| Lymph node | 11 (39%) |
| Mediastinum | 0 (0) |
| Other | 7 (25) |
| Prior bevacizumab treatment | 12 (43%) |
| Prior PARP inhibitor treatment | 18 (64%) |
| BRCA mutations | |
| BRCA1 somatic | 5 (18%) |
| BRCA2 somatic | 1 (4%) |
| Wild-type | 22 (78%) |
| Means and Medians for Survival Time | ||||||||
|---|---|---|---|---|---|---|---|---|
| BRD4 | Mean | Median | ||||||
| Estimate | Std. Error | 95% Confidence Interval | Estimate | Std. Error | 95% Confidence Interval | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
| Low | 6.333 | 1.523 | 3.347 | 9.319 | 4.000 | 1.491 | 1.078 | 6.922 |
| Medium High | 10.421 | 0.719 | 9.012 | 11.830 | ||||
| Overall | 9.107 | 0.780 | 7.579 | 10.635 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrikopoulou, A.; Bletsa, G.; Rouvalis, A.; Tsakogiannis, D.; Kaparelou, M.; Papatheodoridi, A.; Haidopoulos, D.; Liontos, M.; Dimopoulos, M.-A.; Zagouri, F. The Prognostic Role of BRD4 Expression in High-Grade Serous Ovarian Cancer. Cancers 2024, 16, 1962. https://doi.org/10.3390/cancers16111962
Andrikopoulou A, Bletsa G, Rouvalis A, Tsakogiannis D, Kaparelou M, Papatheodoridi A, Haidopoulos D, Liontos M, Dimopoulos M-A, Zagouri F. The Prognostic Role of BRD4 Expression in High-Grade Serous Ovarian Cancer. Cancers. 2024; 16(11):1962. https://doi.org/10.3390/cancers16111962
Chicago/Turabian StyleAndrikopoulou, Angeliki, Garyfalia Bletsa, Angeliki Rouvalis, Dimitris Tsakogiannis, Maria Kaparelou, Alkistis Papatheodoridi, Dimitrios Haidopoulos, Michalis Liontos, Meletios-Athanasios Dimopoulos, and Flora Zagouri. 2024. "The Prognostic Role of BRD4 Expression in High-Grade Serous Ovarian Cancer" Cancers 16, no. 11: 1962. https://doi.org/10.3390/cancers16111962
APA StyleAndrikopoulou, A., Bletsa, G., Rouvalis, A., Tsakogiannis, D., Kaparelou, M., Papatheodoridi, A., Haidopoulos, D., Liontos, M., Dimopoulos, M.-A., & Zagouri, F. (2024). The Prognostic Role of BRD4 Expression in High-Grade Serous Ovarian Cancer. Cancers, 16(11), 1962. https://doi.org/10.3390/cancers16111962