
Osteosarcoma Arising as a Secondary Malignancy following Treatment for Hematologic Cancer: A Report of 33 Affected Patients from the Cooperative Osteosarcoma Study Group (COSS)

 , , , , , , , ,
, , , , , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Selection and Data Collection
2.2. Statistical Analyses
3. Results
Patients
- -
- 20 (61%) lymphomas (13 Hodgkin (HL), 7 non-Hodgkin (NHL), 3 diffuse large B-cell (DLBCL), 1 anaplastic large-cell (ALCL), 1 lymphoblastic, 1 mucosa-associated lymphoid tissue (MALT), and 1 unspecified NHL). Among the 20 lymphomas, 16 (80%) were known to have involved the trunk, 4 (20%) the head and neck (incl. 1 with involvement of both regions), and 1 (5%) an extremity.
- -
- 13 (29%) leukemias (12 acute lymphoblastic (ALL)—7 B-precursor, 4 T-, 1 unspecified; 1 acute myeloid leukemia (AML)).
- -
- 1 benign tumor (adenoma of the thyroid treated by surgery);
- -
- 3 borderline tumors (2 basal cell carcinomas of the skin, 1 phylloides tumors of the breast, all treated by surgery only);
- -
- 1 solid malignancy (1 breast cancer treated by surgery and local radiotherapy);
- -
- 2 hematologic malignancies (1 untreated large-cell NHL, 1 chronic lymphocytic leukemia treated by chemotherapy).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pui, C.-H.; Yang, J.J.; Hunger, S.P.; Pieters, R.; Schrappe, M.; Biondi, A.; Vora, A.; Baruchel, A.; Silverman, L.B.; Schmiegelow, K.; et al. Childhood Acute Lymphoblastic Leukemia: Progress Through Collaboration. J. Clin. Oncol. 2015, 33, 2938–2948. [Google Scholar] [CrossRef] [PubMed]
- Armitage, J.O.; Gascoyne, R.D.; Lunning, M.A.; Cavalli, F. Non-Hodgkin lymphoma. Lancet 2017, 390, 298–310. [Google Scholar] [CrossRef]
- Connors, J.M.; Cozen, W.; Steidl, C.; Carbone, A.; Hoppe, R.T.; Flechtner, H.-H.; Bartlett, N.L. Hodgkin lymphoma. Nat. Rev. Dis. Prim. 2020, 6, 1–25. [Google Scholar] [CrossRef]
- Cortes, J.; Pavlovsky, C.; Saußele, S. Chronic myeloid leukaemia. Lancet 2021, 398, 1914–1926. [Google Scholar] [CrossRef] [PubMed]
- Shimony, S.; Stahl, M.; Stone, R.M. Acute myeloid leukemia: 2023 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2023, 98, 502–526. [Google Scholar] [CrossRef]
- Fulbright, J.M.; Raman, S.; McClellan, W.S.; August, K.J. Late effects of childhood leukemia therapy. Curr. Hematol. Malign- Rep. 2011, 6, 195–205. [Google Scholar] [CrossRef]
- Langer, T.; Grabow, D.; Steinmann, D.; Wörmann, B.; Calaminus, G. Late Effects and Long-Term Follow-Up after Cancer in Childhood. Oncol. Res. Treat. 2017, 40, 746–750. [Google Scholar] [CrossRef]
- Henderson, T.O.; Oeffinger, K.C. Paediatrics: Addressing the health burden of childhood cancer survivors-improvements are needed. Nat. Rev. Clin. Oncol. 2018, 15, 137–138. [Google Scholar] [CrossRef] [PubMed]
- Meadows, A.T.; Friedman, D.L.; Neglia, J.P.; Mertens, A.C.; Donaldson, S.S.; Stovall, M.; Hammond, S.; Yasui, Y.; Inskip, P.D. Second neoplasms in survivors of childhood cancer: Findings from the Childhood Cancer Survivor Study cohort. J. Clin. Oncol. 2009, 27, 2356–2362. [Google Scholar] [CrossRef]
- Beird, H.C.; Bielack, S.S.; Flanagan, A.M.; Gill, J.; Heymann, D.; Janeway, K.A.; Livingston, J.A.; Roberts, R.D.; Strauss, S.J.; Gorlick, R. Osteosarcoma. Nat. Rev. Dis. Prim. 2022, 8, 77. [Google Scholar] [CrossRef]
- Bielack, S.S.; Kempf-Bielack, B.; Heise, U.; Schwenzer, D.; Winkler, K. Combined modality treatment for osteosarcoma occurring as a second malignant disease. Cooperative German-Austrian-Swiss Osteosarcoma Study Group. J. Clin. Oncol. 1999, 17, 1164. [Google Scholar] [CrossRef] [PubMed]
- Tabone, M.-D.; Terrier, P.; Pacquement, H.; Brunat-Mentigny, M.; Schmitt, C.; Babin-Boilletot, A.; Mahmoud, H.H.; Kalifa, C. Outcome of radiation-related osteosarcoma after treatment of childhood and adolescent cancer: A study of 23 cases. J. Clin. Oncol. 1999, 17, 2789. [Google Scholar] [CrossRef]
- Kratz, C.P.; Achatz, M.I.; Brugières, L.; Frebourg, T.; Garber, J.E.; Greer, M.-L.C.; Hansford, J.R.; Janeway, K.A.; Kohlmann, W.K.; McGee, R.; et al. Cancer Screening Recommendations for Individuals with Li-Fraumeni Syndrome. Clin. Cancer Res. 2017, 23, e38–e45. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Zhu, B.; Koster, R.; Karlins, E.; Dean, M.; Yeager, M.; Gianferante, M.; Spector, L.G.; Morton, L.M.; Karyadi, D.; et al. Frequency of Pathogenic Germline Variants in Cancer-Susceptibility Genes in Patients with Osteosarcoma. JAMA Oncol. 2020, 6, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Bielack, S.S.; Kager, L.; Kühne, T.; Langer, T.; Reichardt, P.; Blattmann, C.; Kevric, M.; Mettmann, V.; Sorg, B.; Hecker-Nolting, S. Establishment, Maintenance, and Performance of the Cooperative Osteosarcoma Study Group (COSS). Cancers 2023, 15, 1520. [Google Scholar] [CrossRef] [PubMed]
- Bielack, S.; Jürgens, H.; Jundt, G.; Kevric, M.; Kühne, T.; Reichardt, P.; Zoubek, A.; Werner, M.; Winkelmann, W.; Kotz, R. Osteosarcoma: The COSS experience. Cancer Treat Res. 2009, 152, 289–308. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.; Bielack, S.S.; Smeland, S.; Longhi, A.; Egerer, G.; Hall, K.S.; Donati, D.; Kevric, M.; Brosjö, O.; Comandone, A.; et al. EURO-B.O.S.S.: A European study on chemotherapy in bone-sarcoma patients aged over 40: Outcome in primary high-grade osteosarcoma. Tumori J. 2018, 104, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Smeland, S.; Bielack, S.S.; Whelan, J.; Bernstein, M.; Hogendoorn, P.; Krailo, M.D.; Gorlick, R.; Janeway, K.A.; Ingleby, F.C.; Anninga, J.; et al. Survival and prognosis with osteosarcoma: Outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur. J. Cancer 2019, 109, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. Clin. Orthop. Relat. Res. 1980, 153, 106–120. [Google Scholar] [CrossRef]
- Salzer-Kuntschik, M.; Brand, G.; Delling, G. Bestimmung des morphologischen Regressionsgrades nach Chemotherapie bei malignen Knochentumoren. Pathologe 1983, 4, 135–141. [Google Scholar]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Mantel, M. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother. Rep. 1966, 50, 163–170. [Google Scholar] [PubMed]
- PDQ Pediatric Treatment Editorial Board. Osteosarcoma and Undifferentiated Pleomorphic Sarcoma of Bone Treatment (PDQ®): Health Professional Version. 2023 Apr 5. In PDQ Cancer Information Summaries [Internet]; Bethesda, M.D., Ed.; National Cancer Institute (US): Bethesda, MD, USA, 2002. [Google Scholar]
- Bhagat, A.; Kleinerman, E.S. Anthracycline-induced cardiotoxicity: Causes, mechanisms, and prevention. Adv. Exp. Med. Biol. 2020, 1257, 181–192. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| No. | Gender | Hematological Malignancy | Intercurrent | |||
|---|---|---|---|---|---|---|
| Age | Type | Radiotherapy | Chemotherapy | Neoplasm | ||
| 1 | male | 14.2 | HL | yes | none | none |
| 2 | male | 2.9 | NHL (NFS) | yes | yes | none |
| 3 | male | 29.7 | HL | yes | none | none |
| 4 | male | 12.6 | HL | yes | yes | none |
| 5 | male | 16.6 | HL | yes | yes | none |
| 6 | male | 10.8 | ALL (B-precursor) | yes (TBI) | yes | none |
| 7 | female | 20.8 | HL | yes | none | none |
| 8 | male | 15.1 | HL | yes | yes | none |
| 9 | male | 5.6 | ALL (B-precursor) | none | yes | none |
| 10 | male | 7.4 | ALL (NFS) | yes (TBI) | yes | none |
| 11 1 | male | 9.4 | NHL (ALCL) | none | yes | NHL (B-large-cell) |
| 12 | male | 5.8 | HL | yes | yes | none |
| 13 | female | 10.5 | ALL (T-) | yes (TBI) | yes | none |
| 14 | male | 12.9 | ALL (T-) | yes | yes | none |
| 15 | male | 33.4 | HL | yes | none | basal-cell carcinoma |
| 16 | male | 22.4 | HL | yes | yes | none |
| 17 | female | 49.8 | NHL (DLBCL) | yes | yes | none |
| 18 | male | 37.1 | HL | yes | none | none |
| 19 | male | 0.8 | ALL (B-precursor) | yes (TBI) | yes | none |
| 20 | female | 22.6 | HL | yes | yes | none |
| 21 | male | 58.2 | NHL (MALT) | yes | none | CLL |
| 22 | female | 38.1 | NHL (DLBCL) | yes | yes | none |
| 23 | male | 3.3 | ALL (T-) | yes (TBI) | yes | none |
| 24 | male | 15.0 | HL | none | yes | none |
| 25 | male | 1.4 | ALL (B-precursor) | yes (TBI) | yes | thyroid adenoma |
| 26 | female | 1.2 | ALL (B-precursor) | yes (TBI) | yes | none |
| 27 | male | 9.4 | ALL (T-) | yes (TBI) | yes | none |
| 28 | female | 45.7 | NHL (DLBC) | yes | none | breast cancer |
| 29 | male | 11.1 | NHL (lymphoblastic) | yes | yes | basal-cell carcinoma |
| 30 2 | female | 5.4 | ALL (B-precursor) | none | yes | none |
| 31 2 | female | 12.4 | ALL (B-precursor) | yes (TBI) | yes | phylloides tumor |
| 32 | female | 4.0 | AML | ND | yes | none |
| 33 | m | 15.3 | HL | yes | yes | none |
| No. | Inter- | Osteosarcoma | Follow-up | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| val | Age | Type | RX-rel | Prim mets | Surg | Response | Rx | Chem | Years | Further neopl | Outcome | |
| 1 | 5.5 | 19.7 | HGC | yes | none | yes | good | none | yes | 4.1 | none | DOD 2nd rec |
| 2 | 9.8 | 12.7 | EOS | yes | none | no | NOP | none | yes | 0.8 | none | DOD no CR |
| 3 | 18.0 | 47.7 | EOS | yes | none | yes | POP | none | yes | 3.1 | none | DOD 1st rec |
| 4 | 4.6 | 17.2 | HGC | yes | none | yes | good | none | yes | 4.6 | none | alive CR1 |
| 5 | 19.0 | 35.6 | HGC | yes | none | yes | NFS | none | yes | 3.1 | none | DOD 1st rec |
| 6 | 8.2 | 19.0 | HGC | yes | none | no | NOP | yes | yes | 7.2 | MDS | DOD SMD 1 |
| 7 | 17.7 | 38.5 | HGC | yes | none | yes | poor | none | yes | 1.5 | none | DOD 1st rec |
| 8 | 3.9 | 18.9 | HGC | yes | none | yes | good | none | yes | 11.0 | none | alive CR2 |
| 9 | 7.5 | 13.1 | HGC | no | lung | yes | good | none | yes | 6.2 | none | DOD 2nd rec |
| 10 | 8.8 | 16.1 | POS | yes | bone | yes | poor | none | yes | 4.4 | none | DOD 1st rec |
| 11 | 5.3 | 14.7 | HGC | no | none | yes | good | none | yes | 7.2 | T-ALL | DOC SMD 2 |
| 12 | 13.3 | 19.1 | HGC | yes | none | yes | poor | none | yes | 8.7 | none | alive CR3 |
| 13 | 3.2 | 13.6 | HGC | yes | lung | yes | poor | none | yes | 2.4 | none | DOD 1st rec |
| 14 | 7.0 | 19.8 | HGC | no | lung | yes | NFS | none | yes | 3.5 | none | DOD 2nd rec |
| 15 | 27.1 | 60.5 | HGC | yes | none | yes | poor | none | yes | 12.0 | SCC | alive CR1 3 |
| 16 | 16.1 | 38.6 | UPS | no | none | yes | good | none | yes | 8.8 | BCC | alive CR1 3 |
| 17 | 6.9 | 56.7 | UPS | yes | none | yes | POP | yes | yes | 10.5 | none | alive CR1 |
| 18 | 24.4 | 61.5 | HGC | yes | lung, bone | yes | POP | none | yes | 0.9 | none | DOD no CR |
| 19 | 13.7 | 14.5 | HGC | yes | none | yes | good | none | yes | 10.1 | none | alive CR1 |
| 20 | 7.7 | 30.3 | HGC | yes | none | no | NFS | NFS | NFS | 0.4 | none | alive no CR |
| 21 | 11.4 | 69.6 | HGC | yes | lung, bone | no | NFS | NFS | NFS | 0.4 | B-NHL 4 | DUC no CR |
| 22 | 11.2 | 49.3 | HGC | yes | none | yes | POP | none | yes | 1.1 | none | alive CR1 |
| 23 | 13.9 | 17.2 | HGC | yes | none | yes | poor | none | yes | 2.8 | none | DOD 2nd rec |
| 24 | 0.5 | 15.5 | HGC | no | lung | yes | good | none | yes | 10.3 | none | alive CR1 |
| 25 | 16.6 | 18.1 | POS | yes | none | yes | poor | none | yes | 3.9 | none | alive CR1 |
| 26 | 5.6 | 6.8 | HGC | yes | none | yes | poor | none | yes | 8.5 | none | alive CR1 |
| 27 | 9.5 | 18.9 | HGC | yes | none | yes | NFS | none | yes | 5.0 | none | alive CR1 |
| 28 | 19.3 | 65.0 | HGC | yes | none | yes | poor | none | yes | 2.3 | none | alive CR1 |
| 29 | 41.6 | 52.7 | HGC | yes | lung | yes | NFS | yes | yes | 2.6 | none | alive no CR |
| 30 | 9.3 | 14.8 | HGC | no | none | yes | NFS | none | yes | 4.9 | none | alive CR1 |
| 31 | 9.4 | 21.9 | HGC | yes | none | no | NOP | none | yes | 1.2 | none | alive no CR |
| 32 | 6.0 | 9.9 | HGC | NFS | none | yes | good | none | yes | 3.2 | none | DOD 1st rec |
| 33 | 7.8 | 23.1 | HGC | yes | none | no | NOP | none | yes | 0.3 | none | alive no CR |
| Patients (%) | 5-Year Overall Survival | 5-Year Event-Free Survival | |||
|---|---|---|---|---|---|
| Estimate (SE) | p 1 | Estimate (SE) | p 1 | ||
| all | |||||
| all eligible patients | 33 (100%) | 56% (10%) | - | 40% (9%) | - |
| gender | |||||
| male | 23 (70%) | 57% (11%) | 0.831 | 39% (10%) | 0.71 |
| female | 10 (30%) | 51% (20%) | 44% (18%) | ||
| age at leukemia/lymphoma | |||||
| below 12 years | 15 (45%) | 64% (13%) | 0.991 | 40% (13%) | 0.983 |
| 12 years and above | 18 (55%) | 48% (14%) | 40% (12%) | ||
| type of hematological malignancy | |||||
| lymphoma | 20 (61%) | 57% (13%) | 0.856 | 42% (12%) | 0.735 |
| leukemia | 13 (39%) | 57% (15%) | 39% (14%) | ||
| chemotherapy for hematological malignancy | |||||
| yes | 26 (79%) | 67% (10%) | 0.024 | 45% (10%) | 0.477 |
| no | 7 (21%) | 19% (17%) | 19% (17%) | ||
| interval hematological malignancy to osteosarcoma | |||||
| below 10 years | 19 (58%) | 63% (12%) | 0.736 | 42% (11%) | 0.967 |
| 10 years or more | 14 (42%) | 49% (15%) | 36% (14%) | ||
| age at osteosarcoma | |||||
| below 18 years | 12 (36%) | 58% (14%) | 0.797 | 50% (14%) | 0.265 |
| 18 years and above | 21 (64%) | 55% (13%) | 34% (11%) | ||
| osteosarcoma in radiation-field 2,3 | |||||
| yes | 26 (81%) | 51% (11%) | 0.596 | 35% (10%) | 0.273 |
| no | 6 (19%) | 82% (15%) | 67% (19%) | ||
| osteosarcoma site | |||||
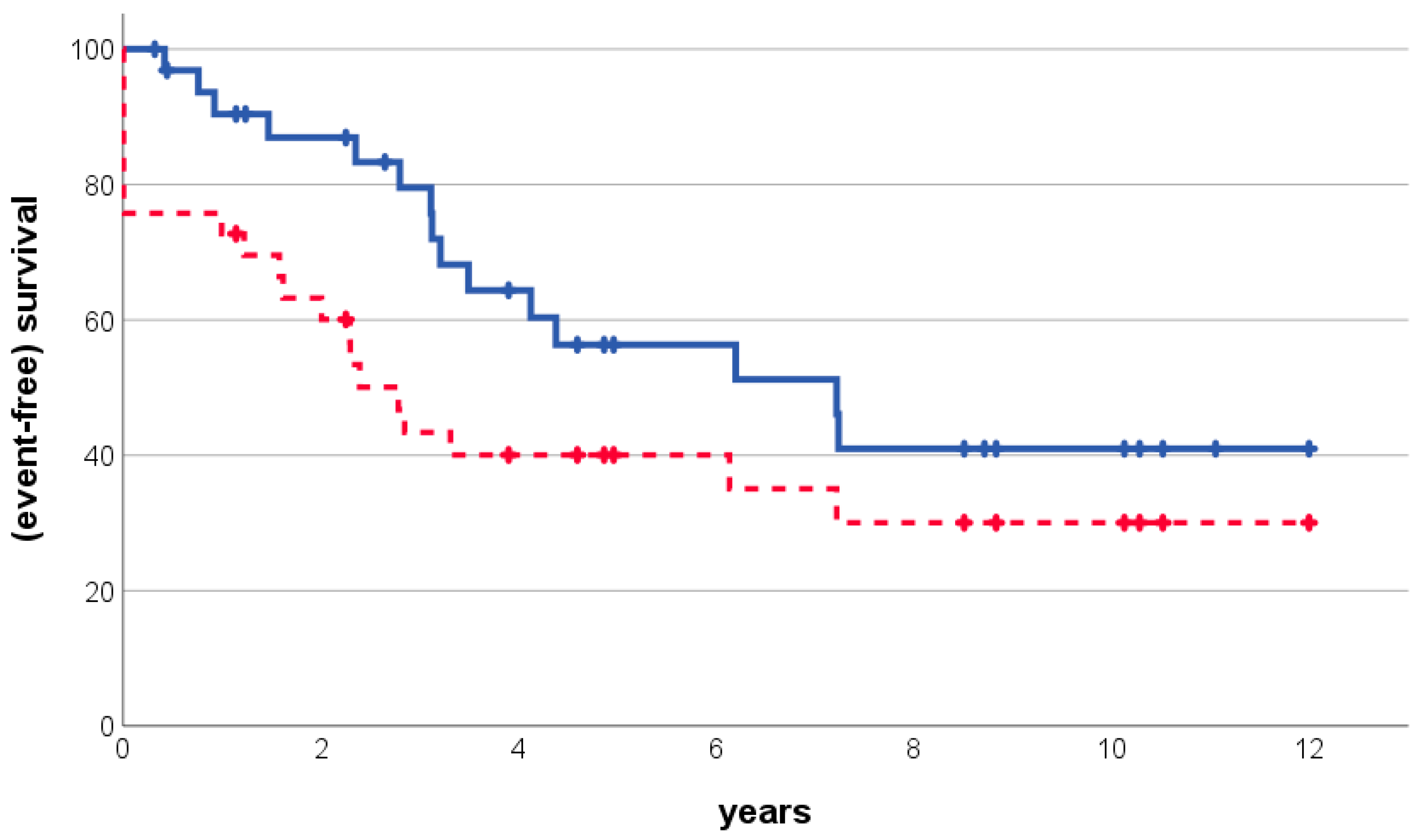
| extremity | 19 (58%) | 56% (11%) | 0.225 | 56% (12%) | 0.011 |
| trunk or head and neck | 14 (42%) | 40% (17%) | 18% (11%) | ||
| primary osteosarcoma metastases | |||||
| absent | 25 (76%) | 65% (11%) | 0.05 | 49% (10%) | 0.063 |
| present | 8 (24%) | 31% (18%) | 13% (12%) | ||
| macroscopic surgical remission | |||||
| achieved | 25 (76%) | 60% (10%) | 0.017 | NA | |
| not achieved | 8 (24%) | 51% (20%) | |||
| additional malignancies 4 | |||||
| no | 28 (85%) | 52% (11%) | 0.807 | 38% (9%) | 0.893 |
| yes | 5 (15%) | 80% (18%) | 60% (22%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bielack, S.S.; Mettmann, V.; Baumhoer, D.; Blattmann, C.; Burkhardt, B.; Deinzer, C.K.W.; Kager, L.; Kevric, M.; Mauz-Körholz, C.; Müller-Abt, P.; et al. Osteosarcoma Arising as a Secondary Malignancy following Treatment for Hematologic Cancer: A Report of 33 Affected Patients from the Cooperative Osteosarcoma Study Group (COSS). Cancers 2024, 16, 1836. https://doi.org/10.3390/cancers16101836
Bielack SS, Mettmann V, Baumhoer D, Blattmann C, Burkhardt B, Deinzer CKW, Kager L, Kevric M, Mauz-Körholz C, Müller-Abt P, et al. Osteosarcoma Arising as a Secondary Malignancy following Treatment for Hematologic Cancer: A Report of 33 Affected Patients from the Cooperative Osteosarcoma Study Group (COSS). Cancers. 2024; 16(10):1836. https://doi.org/10.3390/cancers16101836
Chicago/Turabian StyleBielack, Stefan S., Vanessa Mettmann, Daniel Baumhoer, Claudia Blattmann, Birgit Burkhardt, Christoph K. W. Deinzer, Leo Kager, Matthias Kevric, Christine Mauz-Körholz, Peter Müller-Abt, and et al. 2024. "Osteosarcoma Arising as a Secondary Malignancy following Treatment for Hematologic Cancer: A Report of 33 Affected Patients from the Cooperative Osteosarcoma Study Group (COSS)" Cancers 16, no. 10: 1836. https://doi.org/10.3390/cancers16101836
APA StyleBielack, S. S., Mettmann, V., Baumhoer, D., Blattmann, C., Burkhardt, B., Deinzer, C. K. W., Kager, L., Kevric, M., Mauz-Körholz, C., Müller-Abt, P., Reinhardt, D., Sabo, A.-A., Schrappe, M., Sorg, B., Windhager, R., & Hecker-Nolting, S. (2024). Osteosarcoma Arising as a Secondary Malignancy following Treatment for Hematologic Cancer: A Report of 33 Affected Patients from the Cooperative Osteosarcoma Study Group (COSS). Cancers, 16(10), 1836. https://doi.org/10.3390/cancers16101836