
Expression of 3q Oncogene SEC62 Predicts Survival in Head and Neck Squamous Cell Carcinoma Patients Treated with Primary Chemoradiation

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tissue Samples
2.2. Immunohistochemistry
2.3. Statistical Analysis
3. Results
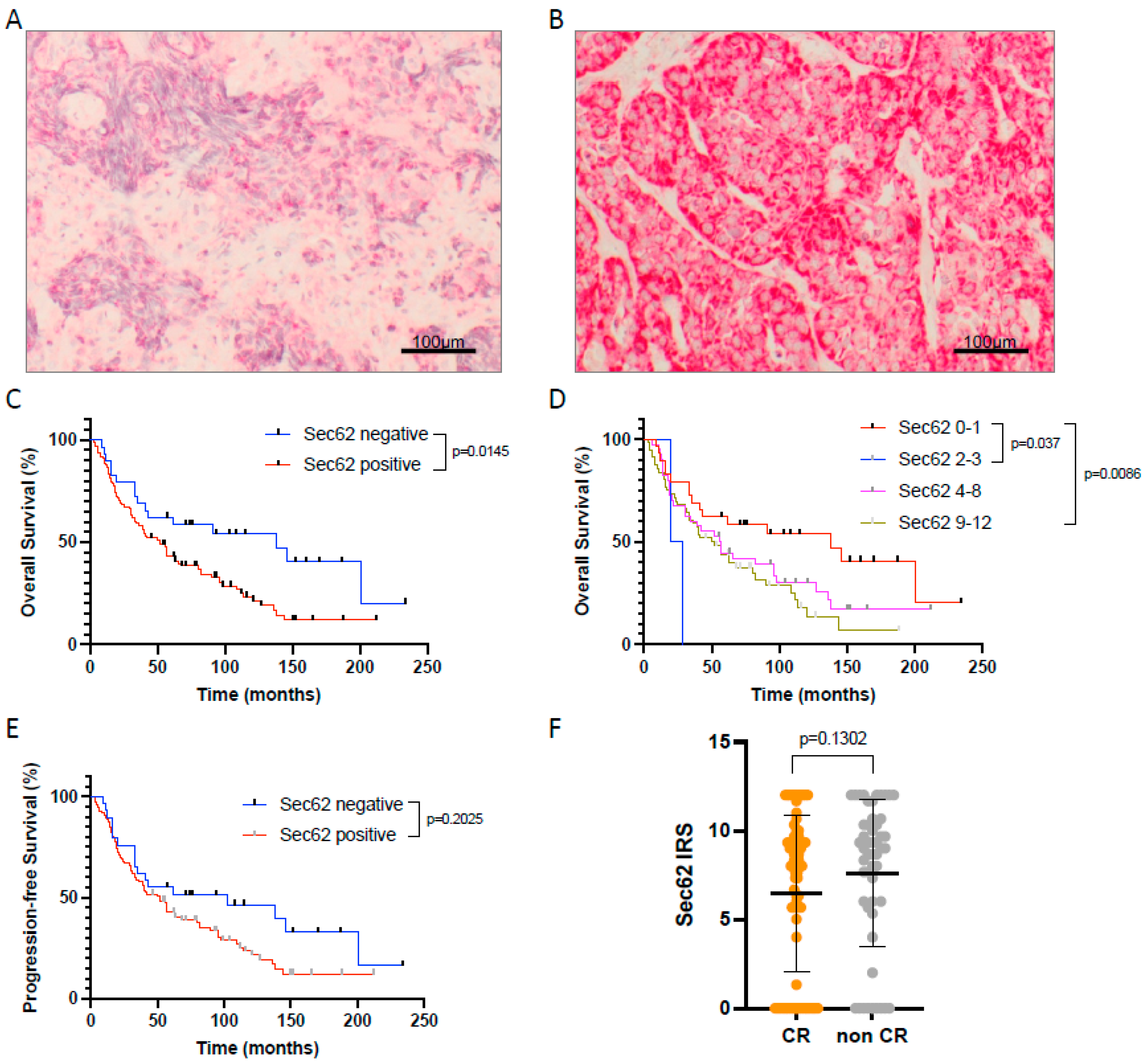
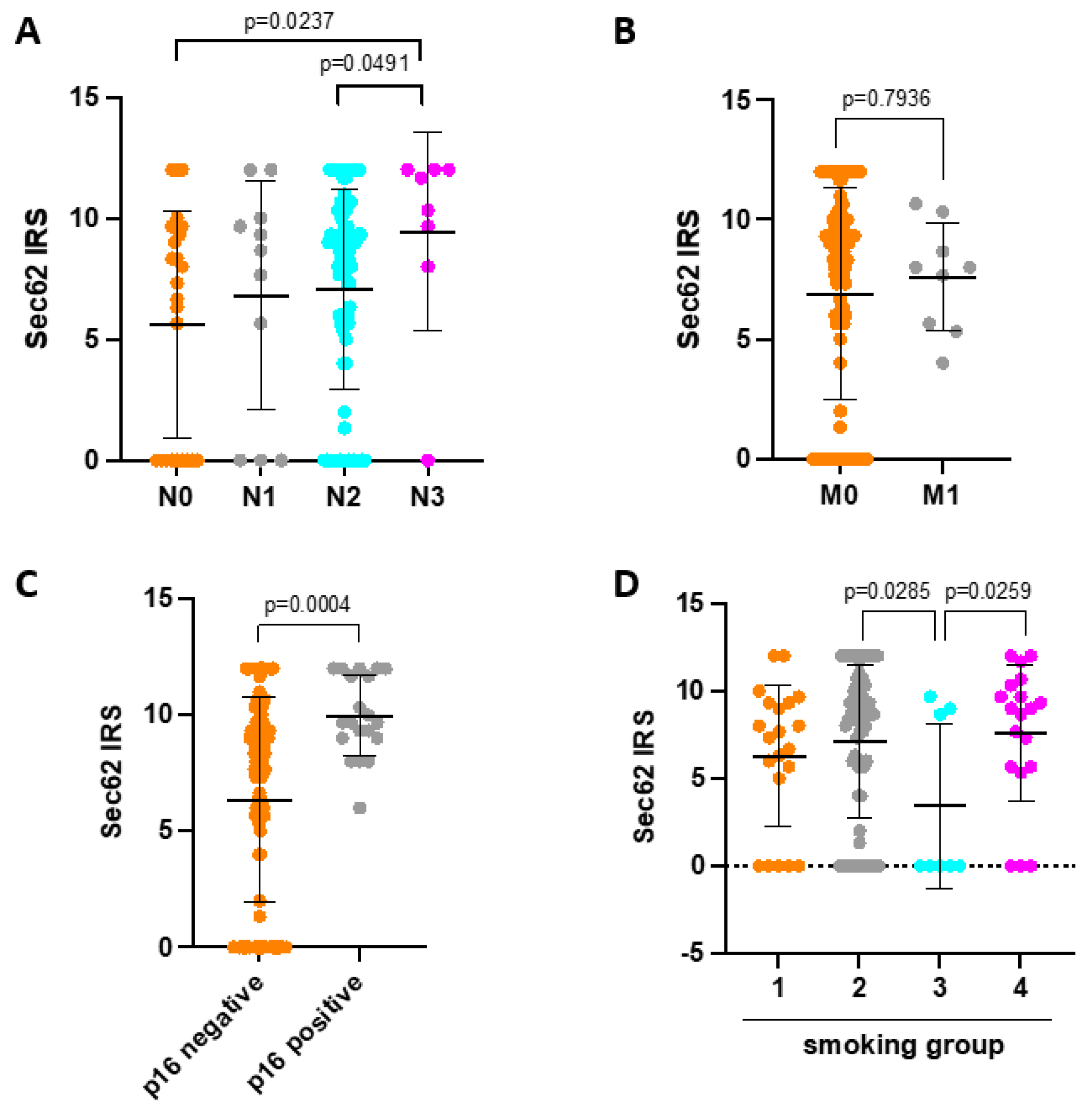
3.1. SEC62 Expression in HNSCC Patients and Correlation with Clinical Data as Well as Patient Outcome
3.2. Prognostic Factors Influencing Overall Survival of HNSCC Patients Undergoing Primary CRT
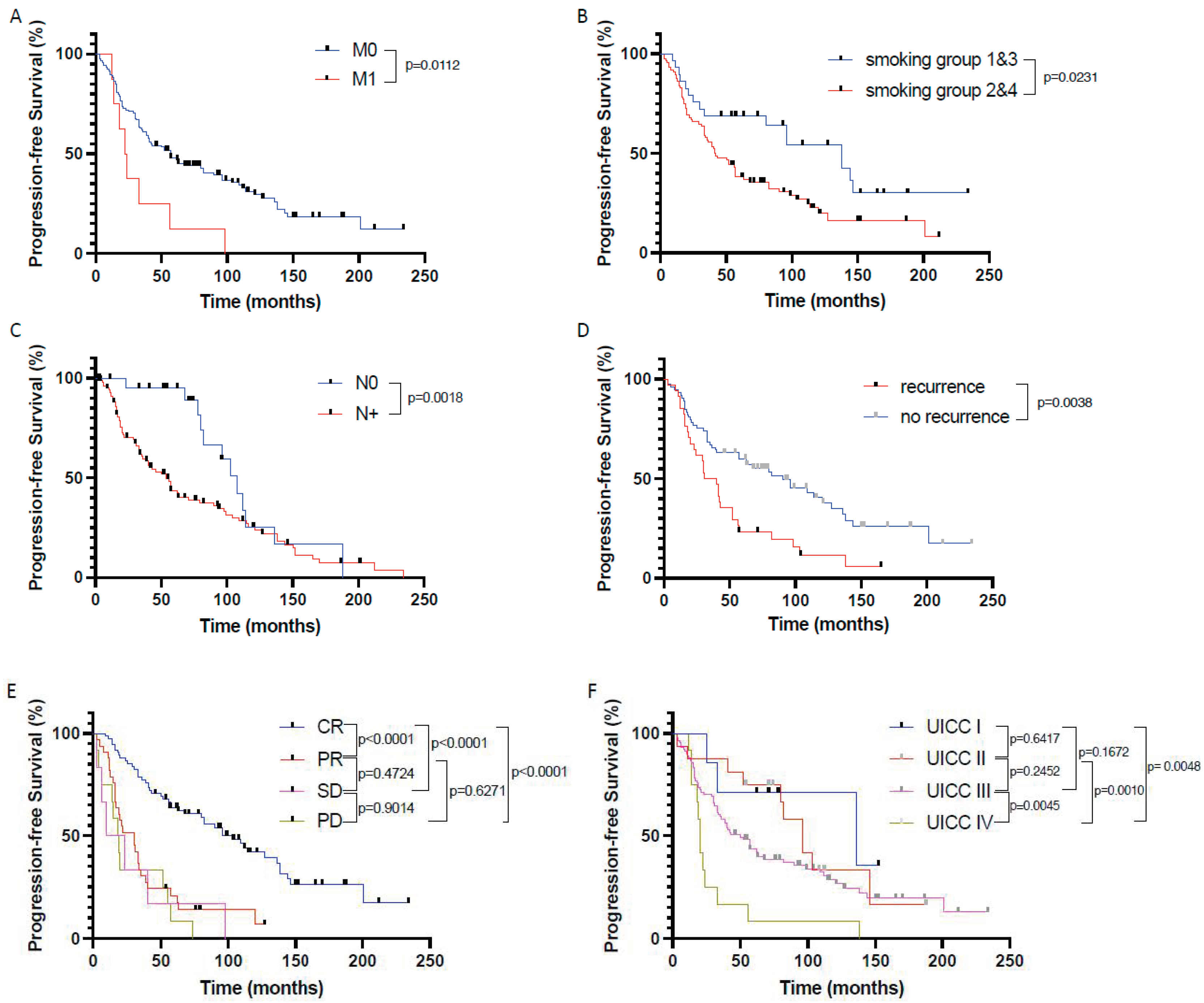
3.3. Prognostic Factors influencing Progression-Free Survival of HNSCC Patients Undergoing Primary Crt
3.4. Identification of Independent Prognostic Factors in the Primary CRT Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Zhang, Q.; Weber, R.S.; Maor, M.H.; Goepfert, H.; Pajak, T.F.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; et al. Long-term results of RTOG 91-11: A comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer. J. Clin. Oncol. 2013, 31, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Bauml, J.M.; Vinnakota, R.; Park, Y.H.A.; Bates, S.E.; Fojo, T.; Aggarwal, C.; Limaye, S.; Damjanov, N.; Di Stefano, J.; Ciunci, C.; et al. Cisplatin Every 3 Weeks Versus Weekly with Definitive Concurrent Radiotherapy for Squamous Cell Carcinoma of the Head and Neck. J. Natl. Cancer Inst. 2019, 111, 490–497. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, I.; Nardone, V.; Reginelli, A.; Cappabianca, S. Chemoradiotherapy for Head and Neck Cancer. Cancers 2023, 15, 2820. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Lacas, B.; Carmel, A.; Landais, C.; Wong, S.J.; Licitra, L.; Tobias, J.S.; Burtness, B.; Ghi, M.G.; Cohen, E.E.W.; Grau, C.; et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 107 randomized trials and 19,805 patients, on behalf of MACH-NC Group. Radiother. Oncol. 2021, 156, 281–293. [Google Scholar] [CrossRef]
- Schüttrumpf, L.; Marschner, S.; Scheu, K.; Hess, J.; Rietzler, S.; Walch, A.; Baumeister, P.; Kirchner, T.; Ganswindt, U.; Zitzelsberger, H.; et al. Definitive chemoradiotherapy in patients with squamous cell cancers of the head and neck—Results from an unselected cohort of the clinical cooperation group "Personalized Radiotherapy in Head and Neck Cancer". Radiat. Oncol. 2020, 15, 7. [Google Scholar] [CrossRef]
- Bourhis, J.; Sire, C.; Graff, P.; Grégoire, V.; Maingon, P.; Calais, G.; Gery, B.; Martin, L.; Alfonsi, M.; Desprez, P.; et al. Concomitant chemoradiotherapy versus acceleration of radiotherapy with or without concomitant chemotherapy in locally advanced head and neck carcinoma (GORTEC 99-02): An open-label phase 3 randomised trial. Lancet Oncol. 2012, 13, 145–153. [Google Scholar] [CrossRef]
- Budach, V.; Stuschke, M.; Budach, W.; Baumann, M.; Geismar, D.; Grabenbauer, G.; Lammert, I.; Jahnke, K.; Stueben, G.; Herrmann, T.; et al. Hyperfractionated accelerated chemoradiation with concurrent fluorouracil-mitomycin is more effective than dose-escalated hyperfractionated accelerated radiation therapy alone in locally advanced head and neck cancer: Final results of the radiotherapy cooperative clinical trials group of the German Cancer Society 95-06 Prospective Randomized Trial. J. Clin. Oncol. 2005, 23, 1125–1135. [Google Scholar] [CrossRef]
- Noronha, V.; Joshi, A.; Patil, V.M.; Agarwal, J.; Ghosh-Laskar, S.; Budrukkar, A.; Murthy, V.; Gupta, T.; D’Cruz, A.K.; Banavali, S.; et al. Once-a-Week Versus Once-Every-3-Weeks Cisplatin Chemoradiation for Locally Advanced Head and Neck Cancer: A Phase III Randomized Noninferiority Trial. J. Clin. Oncol. 2018, 36, 1064–1072. [Google Scholar] [CrossRef] [PubMed]
- Fietkau, R.; Hecht, M.; Hofner, B.; Lubgan, D.; Iro, H.; Gefeller, O.; Rödel, C.; Hautmann, M.G.; Kölbl, O.; Salay, A.; et al. Randomized phase-III-trial of concurrent chemoradiation for locally advanced head and neck cancer comparing dose reduced radiotherapy with paclitaxel/cisplatin to standard radiotherapy with fluorouracil/cisplatin: The PacCis-trial. Radiother. Oncol. 2020, 144, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, B.; Huang, S.H.; Siu, L.L.; Waldron, J.; Zhao, H.; Perez-Ordonez, B.; Weinreb, I.; Kim, J.; Ringash, J.; Bayley, A.; et al. Deintensification candidate subgroups in human papillomavirus-related oropharyngeal cancer according to minimal risk of distant metastasis. J. Clin. Oncol. 2013, 31, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Rühle, A.; Grosu, A.L.; Wiedenmann, N.; Stoian, R.; Haehl, E.; Zamboglou, C.; Baltas, D.; Werner, M.; Kayser, G.; Nicolay, N.H. Immunohistochemistry-based hypoxia-immune prognostic classifier for head-and-neck cancer patients undergoing chemoradiation—Post-hoc analysis from a prospective imaging trial. Radiother. Oncol. 2021, 159, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Lakkaraju, A.K.; Thankappan, R.; Mary, C.; Garrison, J.L.; Taunton, J.; Strub, K. Efficient secretion of small proteins in mammalian cells relies on Sec62-dependent posttranslational translocation. Mol. Biol. Cell 2012, 23, 2712–2722. [Google Scholar] [CrossRef]
- Lang, S.; Benedix, J.; Fedeles, S.V.; Schorr, S.; Schirra, C.; Schäuble, N.; Jalal, C.; Greiner, M.; Hassdenteufel, S.; Tatzelt, J.; et al. Different effects of Sec61α, Sec62 and Sec63 depletion on transport of polypeptides into the endoplasmic reticulum of mammalian cells. J. Cell Sci. 2012, 125, 1958–1969. [Google Scholar] [CrossRef]
- Körner, S.; Pick, T.; Bochen, F.; Wemmert, S.; Körbel, C.; Menger, M.D.; Cavalié, A.; Kühn, J.P.; Schick, B.; Linxweiler, M. Antagonizing Sec62 function in intracellular Ca(2+) homeostasis represents a novel therapeutic strategy for head and neck cancer. Front. Physiol. 2022, 13, 880004. [Google Scholar] [CrossRef]
- Fumagalli, F.; Noack, J.; Bergmann, T.J.; Cebollero, E.; Pisoni, G.B.; Fasana, E.; Fregno, I.; Galli, C.; Loi, M.; Soldà, T.; et al. Translocon component Sec62 acts in endoplasmic reticulum turnover during stress recovery. Nat. Cell Biol. 2016, 18, 1173–1184. [Google Scholar] [CrossRef]
- Sicking, M.; Lang, S.; Bochen, F.; Roos, A.; Drenth, J.P.H.; Zakaria, M.; Zimmermann, R.; Linxweiler, M. Complexity and Specificity of Sec61-Channelopathies: Human Diseases Affecting Gating of the Sec61 Complex. Cells 2021, 10, 1036. [Google Scholar] [CrossRef] [PubMed]
- Bochen, F.; Adisurya, H.; Wemmert, S.; Lerner, C.; Greiner, M.; Zimmermann, R.; Hasenfus, A.; Wagner, M.; Smola, S.; Pfuhl, T.; et al. Effect of 3q oncogenes SEC62 and SOX2 on lymphatic metastasis and clinical outcome of head and neck squamous cell carcinomas. Oncotarget 2017, 8, 4922–4934. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.S.L.; Pföhler, C.; Wahl, M.; Bochen, F.; Körner, S.; Kühn, J.P.; Bozzato, A.; Schick, B.; Linxweiler, M. Expression of SEC62 Oncogene in Benign, Malignant and Borderline Melanocytic Tumors-Unmasking the Wolf in Sheep’s Clothing? Cancers 2021, 13, 1645. [Google Scholar] [CrossRef] [PubMed]
- Takacs, F.Z.; Radosa, J.C.; Linxweiler, M.; Kasoha, M.; Bohle, R.M.; Bochen, F.; Unger, C.; Solomayer, E.F.; Schick, B.; Juhasz-Böss, I. Identification of 3q oncogene SEC62 as a marker for distant metastasis and poor clinical outcome in invasive ductal breast cancer. Arch. Gynecol. Obstet. 2019, 299, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Linxweiler, M.; Linxweiler, J.; Barth, M.; Benedix, J.; Jung, V.; Kim, Y.J.; Bohle, R.M.; Zimmermann, R.; Greiner, M. Sec62 bridges the gap from 3q amplification to molecular cell biology in non-small cell lung cancer. Am. J. Pathol. 2012, 180, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Linxweiler, M.; Schorr, S.; Schäuble, N.; Jung, M.; Linxweiler, J.; Langer, F.; Schäfers, H.J.; Cavalié, A.; Zimmermann, R.; Greiner, M. Targeting cell migration and the endoplasmic reticulum stress response with calmodulin antagonists: A clinically tested small molecule phenocopy of SEC62 gene silencing in human tumor cells. BMC Cancer 2013, 13, 574. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Shi, Y.T.; Chu, Y.; Jiang, M.Z.; Wu, N.; Xu, B.; Zhou, H.; Lin, J.C.; Jin, Y.R.; Li, X.F.; et al. Sec62 promotes gastric cancer metastasis through mediating UPR-induced autophagy activation. Cell Mol. Life Sci. 2022, 79, 133. [Google Scholar] [CrossRef]
- Jin, Y.; Han, Y.; Yang, S.; Cao, J.; Jiang, M.; Liang, J. Endoplasmic reticulum-resident protein Sec62 drives colorectal cancer metastasis via MAPK/ATF2/UCA1 axis. Cell Prolif. 2022, 55, e13253. [Google Scholar] [CrossRef]
- Weng, L.; Du, J.; Zhou, Q.; Cheng, B.; Li, J.; Zhang, D.; Ling, C. Identification of cyclin B1 and Sec62 as biomarkers for recurrence in patients with HBV-related hepatocellular carcinoma after surgical resection. Mol. Cancer 2012, 11, 39. [Google Scholar] [CrossRef]
- Kim, W.; Lee, S.; Seo, D.; Kim, D.; Kim, K.; Kim, E.; Kang, J.; Seong, K.M.; Youn, H.; Youn, B. Cellular Stress Responses in Radiotherapy. Cells 2019, 8, 1105. [Google Scholar] [CrossRef]
- Dadey, D.Y.; Kapoor, V.; Khudanyan, A.; Urano, F.; Kim, A.H.; Thotala, D.; Hallahan, D.E. The ATF6 pathway of the ER stress response contributes to enhanced viability in glioblastoma. Oncotarget 2016, 7, 2080–2092. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Kim, E.; Kim, W.; Seong, K.M.; Youn, H.; Kim, J.W.; Kim, J.; Youn, B. Rhamnetin and cirsiliol induce radiosensitization and inhibition of epithelial-mesenchymal transition (EMT) by miR-34a-mediated suppression of Notch-1 expression in non-small cell lung cancer cell lines. J. Biol. Chem. 2013, 288, 27343–27357. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Wang, Y.; Pang, X.; Su, Y.; Ai, G.; Wang, T. ER stress induced by ionising radiation in IEC-6 cells. Int. J. Radiat. Biol. 2010, 86, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Wemmert, S.; Lindner, Y.; Linxweiler, J.; Wagenpfeil, S.; Bohle, R.; Niewald, M.; Schick, B. Initial evidence for Sec62 as a prognostic marker in advanced head and neck squamous cell carcinoma. Oncol. Lett. 2016, 11, 1661–1670. [Google Scholar] [CrossRef] [PubMed]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar] [PubMed]
- Liu, X.; Su, K.; Sun, X.; Jiang, Y.; Wang, L.; Hu, C.; Zhang, C.; Lu, M.; Du, X.; Xing, B. Sec62 promotes stemness and chemoresistance of human colorectal cancer through activating Wnt/β-catenin pathway. J. Exp. Clin. Cancer Res. 2021, 40, 132. [Google Scholar] [CrossRef]
- Körbel, C.; Linxweiler, M.; Bochen, F.; Wemmert, S.; Schick, B.; Meyer, M.; Maurer, H.; Menger, M.D.; Zimmermann, R.; Greiner, M. Treatment of SEC62 over-expressing tumors by Thapsigargin and Trifluoperazine. Biomol. Concepts 2018, 9, 53–63. [Google Scholar] [CrossRef]
- Mahalingam, D.; Wilding, G.; Denmeade, S.; Sarantopoulas, J.; Cosgrove, D.; Cetnar, J.; Azad, N.; Bruce, J.; Kurman, M.; Allgood, V.E.; et al. Mipsagargin, a novel thapsigargin-based PSMA-activated prodrug: Results of a first-in-man phase I clinical trial in patients with refractory, advanced or metastatic solid tumours. Br. J. Cancer 2016, 114, 986–994. [Google Scholar] [CrossRef]
- Gupta, T.; Kannan, S.; Ghosh-Laskar, S.; Agarwal, J.P. Concurrent chemoradiotherapy with cisplatin given once-a-week versus every-three weekly in head and neck squamous cell carcinoma: Non-inferior, equivalent, or superior? Oral. Oncol. 2022, 134, 106130. [Google Scholar] [CrossRef]
- Kiyota, N.; Tahara, M.; Mizusawa, J.; Kodaira, T.; Fujii, H.; Yamazaki, T.; Mitani, H.; Iwae, S.; Fujimoto, Y.; Onozawa, Y.; et al. Weekly Cisplatin Plus Radiation for Postoperative Head and Neck Cancer (JCOG1008): A Multicenter, Noninferiority, Phase II/III Randomized Controlled Trial. J. Clin. Oncol. 2022, 40, 1980–1990. [Google Scholar] [CrossRef]
- Kühn, J.P.; Speicher, S.; Linxweiler, B.; Körner, S.; Rimbach, H.; Wagner, M.; Solomayer, E.F.; Schick, B.; Linxweiler, M. Dual Sec62/Ki67 immunocytochemistry of liquid-based cytological preparations represents a highly valid biomarker for non-invasive detection of head and neck squamous cell carcinomas. Cytopathology 2023, 35, 113–121. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | ||
|---|---|---|
| Number of HNSCC Patients | 127 | |
| Sex | male | 103 (81.1%) |
| female | 24 (18.9%) | |
| age [years] + | 59.98 | |
| Tumor localization | Oral cavity | 8 (6.3%) |
| Oropharynx | 55 (43.3%) | |
| Hypopharynx | 34 (26.8%) | |
| Larynx | 30 (23.6%) | |
| T-Stage | T1 | 4 (3.2%) |
| T2 | 21 (16.5%) | |
| T3 | 30 (23.6%) | |
| T4 | 72 (56.7%) | |
| N-Stage | N0 | 25 (19.7%) |
| N1 | 12 (9.4%) | |
| N2 | 84 (66.2%) | |
| N3 | 6 (4.7%) | |
| M-Stage | M0 | 117 (92.1%) |
| M1 | 10 (7.9%) | |
| Grading | G1 | 2 (1.6%) |
| G2 | 65 (51.1%) | |
| G3 | 60 (47.3%) | |
| UICC-Stage | I | 6 (4.7%) |
| II | 16 (12.6%) | |
| III | 92 (72.4%) | |
| IV | 13 (10.3%) | |
| P16 expression | negative | 107 (84.3%) |
| positive | 20 (15.7%) | |
| Alcohol abuse | yes | 41 (32.3%) |
| no | 74 (58.3%) | |
| no information | 12 (9.4%) | |
| Smoking | Lifelong non-smoker | 21 (16.6%) |
| Current smoker | 70 (55.1%) | |
| Current reformed smoker for >15 years | 8 (6.3%) | |
| Current reformed smoker for 15 ≤ years | 19 (14.9%) | |
| Response to therapy (RECIST 1.1) * | CR | 75 (59.1%) |
| PR | 33 (26%) | |
| SD | 6 (4.7%) | |
| PD | 13 (10.2%) | |
| Body Mass Index [kg/m2] + | 24.31 | |
| TSH [μIU/mL] + | 2.02 |
| Variable | Hazard Ratio (HR) | 95% CI | p Value |
|---|---|---|---|
| N Stage (N+ vs. N0) | 7.279 | 0.2169–737.4 | 0.4724 |
| M Stage (M1 vs. M0) | 1.707 | 0.8633–3.205 | 0.1076 |
| UICC Stage (1&2 vs. 3&4) | 0.197 | 0.002–6.919 | 0.5558 |
| RECIST 1.1 (non-CR vs. CR) | 2.723 | 1.709–4.354 | <0.0001 |
| Recurrence (yes vs. no) | 1.39 | 0.859–2.211 | 0.1705 |
| SEC62 (pos. vs. neg.) | 1.79 | 1.035–3.276 | 0.0462 |
| Tobacco exposure (2&4 vs. 1&3) | 1.178 | 0.706–2.037 | 0.5439 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linxweiler, M.; Schneider, M.; Körner, S.; Knebel, M.; Brust, L.A.; Braun, F.L.; Wemmert, S.; Wagner, M.; Hecht, M.; Schick, B.; et al. Expression of 3q Oncogene SEC62 Predicts Survival in Head and Neck Squamous Cell Carcinoma Patients Treated with Primary Chemoradiation. Cancers 2024, 16, 98. https://doi.org/10.3390/cancers16010098
Linxweiler M, Schneider M, Körner S, Knebel M, Brust LA, Braun FL, Wemmert S, Wagner M, Hecht M, Schick B, et al. Expression of 3q Oncogene SEC62 Predicts Survival in Head and Neck Squamous Cell Carcinoma Patients Treated with Primary Chemoradiation. Cancers. 2024; 16(1):98. https://doi.org/10.3390/cancers16010098
Chicago/Turabian StyleLinxweiler, Maximilian, Matthias Schneider, Sandrina Körner, Moritz Knebel, Lukas Alexander Brust, Felix Leon Braun, Silke Wemmert, Mathias Wagner, Markus Hecht, Bernhard Schick, and et al. 2024. "Expression of 3q Oncogene SEC62 Predicts Survival in Head and Neck Squamous Cell Carcinoma Patients Treated with Primary Chemoradiation" Cancers 16, no. 1: 98. https://doi.org/10.3390/cancers16010098
APA StyleLinxweiler, M., Schneider, M., Körner, S., Knebel, M., Brust, L. A., Braun, F. L., Wemmert, S., Wagner, M., Hecht, M., Schick, B., & Kühn, J. P. (2024). Expression of 3q Oncogene SEC62 Predicts Survival in Head and Neck Squamous Cell Carcinoma Patients Treated with Primary Chemoradiation. Cancers, 16(1), 98. https://doi.org/10.3390/cancers16010098