
Chemotherapy and Radiotherapy Long-Term Adverse Effects on Oral Health of Childhood Cancer Survivors: A Systematic Review and Meta-Analysis

 ,
, 
 ,
,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Focused Questions and Eligibility Criteria
- “What is the prevalence of late oral health adverse effects in childhood cancer survivors with a history of chemotherapy and radiotherapy”?
- “Are children who undergo cancer therapy more likely to have late oral health adverse effects when compared with healthy controls counterparts”?
2.3. Data Search Strategy and Study Selection
2.4. Data Extraction Process and Data Items
2.5. Risk of Bias (RoB) Assessment
2.6. Summary Measures and Synthesis of Results
3. Results
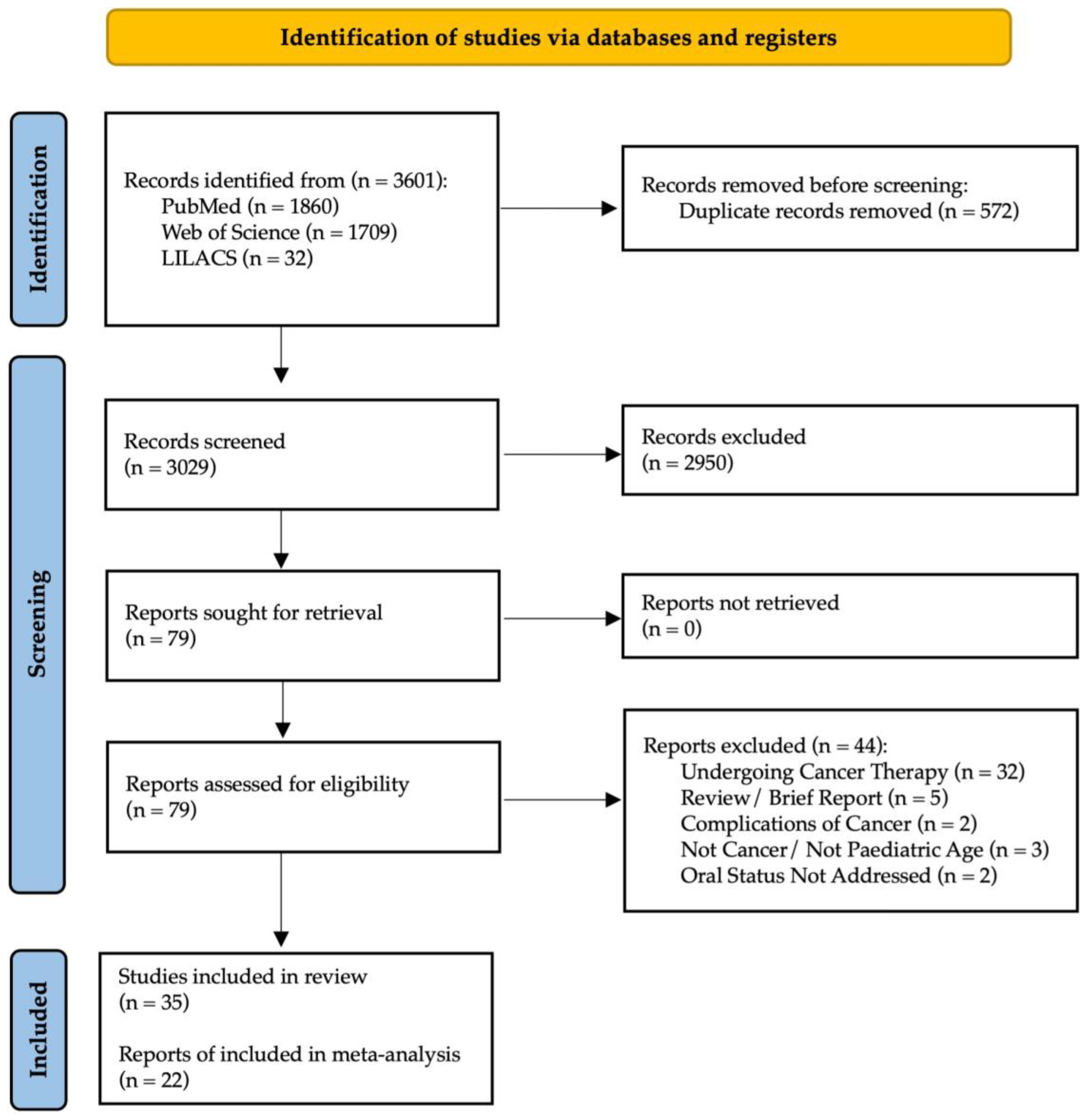
3.1. Study Selection
3.2. Studies’ Characteristics

{kind=link}
| Study | Design | Country | Sample | Oral Health Conditions Case Definition Setting | Cancer Type | Treatment Modality | Study Funding |
|---|---|---|---|---|---|---|---|
| Halperson et al. (2022) [4] | Cross-sectional | Israel | 121 | Dental caries; Dental developmental anomalies (DDA—includes five major groups: no disturbance identified, hypomineralization or hypoplasia, microdontia, root changes, and an absent tooth bud categorized as hypodontia); DMFT index | leukemia\lymphoma in 53 (45%) patients, solid tumors in 35 (29%) and other hematological conditions leading to BMT in 31 (26%) | Most patients (83, 69%) had received ChemoT without radiotherapy. Thirty-eight (31%) had received radiation therapy only or in combination with ChemoT. Fourteen (12%) of the cohort had received total body irradiation (TBI) 12 Gray and 15 (13%) radiation to the head and/or neck area (range of 27–70 Gray). The remaining nine patients had received radiotherapy to other areas (range of 30–70 Gray). Thirty percent of the cohort had undergone BMT | NR |
| Shayani et al. (2022) [31] | Retrospective | Spain | 109 | DDE, microdontia, taurodontism, agenesis, root shortening (RS) | leukemias and lymphomas (41.3%) followed by solid non-CNS tumors (38.5%) and, finally, solid CNS tumors (20.2%) | ChemoT (CT); CT combined with radiotherapy (CT + RT); and CT + RT combined with hematopoietic stem cell transplantation (HSCT) | NI |
| Rabassa-Blanco et al. (2022) [23] | Retrospective | Chile | 23 | missing or filled teeth index and the presence of gingivitis | ALL | ChemoT | NI |
| Stolze et al. (2022) [25] | Cross-sectional | The Netherlands | 291 | unstimulated (UWS) and stimulated whole salivary flow rates (SWS) were measured according to internationally standardized procedures—categorized into ‘hyposalivation’ (<0.2 mL/min and <0.7 mL/min, respectively) and ‘severe hyposalivation’ (<0.1 mL/min and <0.5 mL/min, respectively); partic- ipants were asked to fill out the Dutch translation of the Xerostomia Inventory (XI) | Hematological malignancy (n = 216); brain tumor (n = 19); solid tumor (n = 57) | head and neck radiotherapy (H&N RT) or total body irradiation (TBI) without chronic graft versus host disease (cGVHD), a group of CCS with (a history of) cGVHD after HSCT, and a group of CCS treated with ChemoT and no H&N RT or TBI | NI |
| Tanem et al. (2022) [47] | Cross-sectional | Norway | 46 | decayed-missing-filled index (DMFT), oral dryness, maximum mouth opening (MMO), fungal infection, and registration of dental developmental disturbances (DDD) in the form of hypodontia, microdontia, and enamel hypoplasia | brain tumors medulloblastoma (MB) and central nervous system supratentorial primitive neuroectodermal tumor (CNS-PNET). | ChemoT + craniospinal irradiation | Research Grant |
| Guagnano et al. (2022) [46] | Cross-sectional | Italy | 52 | Decayed-missing-filled teeth (dmft/DMFT) index; Disturbances of enamel mineralisation using Aine rating scale; dental age estimation using panoramic radiographs; dental abnormalities using the Höltta Defect Index on panoramic radiographs—Valores médios para cada sexo, tipo de terapêutica e idade no diagnóstico (<5 anos ou ≥5 anos), os valores apresentados à frente são média da populção toda | ALL Acute Myeloblastic Leukemia Medulloblastoma Familiar Hemophagocitic Lymphohistiocitosis Lymphoma Juvenile Myelomonocytic Leukemia Wilms tumour Epatoblastoma Rhabdomyosarcoma Ewing-PNET Sarcoma Severe Aplastic Anaemia Xantoastocitoma Wide Cells Anaplastic Lymphoma Histiocytosis | CT and/or RT, Hematopoietic Stem Cell Transplantation (HSCT) or Bone Marrow Transplantation (BMT) | NI |
| Seremidi et al. (2021) [32] | Retrospective | Greece | 70 | Microdontia, Malformed teeth, Oligodontia, Hypodontia, Enamel defects, Dental caries | central nervous system tumor, Solid Tumors and Lymphomas | ChemoT, or hemopoietic stem cell transplantatio | None |
| Proc et al. (2019) [3] | Cross-sectional | Poland | 75 | dmft; DMFT; plaque index by silness and loe | ALL; Wilms tumor; Neuroblastoma; Rhabdosarcoma (RMS); Brain tumor; Hepatoblastoma; Acute non-lymphoblastic leukemia (ANLL) Non-Hodgkin’s lymphoma (B-NHL) Hodgkin’s lymphoma (HL); Primitive neuroectodermal tumor (PNET) Germinal tumour; Tumor ovari | RadioT & ChemoT | NI |
| Alnuaimi et al. (2018) [15] | Retrospective | United Arab Emirates | 120 | Oral health problem: oral mucositis & ulceration, candidiasis, herpes and herpetic gingivo-stomatitis, gigival bleeding, gigivites, oral petechiae, dental caries, poor oral hygiene, facial pain/palsy, other | Leukaemic | ChemoT | NI |
| Çetiner et al. (2019) [28] | Retrospective | Turkey | 53 | Gingival Index, Plaque Index, dmft/DMFT, dmfs/DMFS, craniofacial development | Hodgkin lymphoma, Non-Hodgkin lymphoma, Neuroblastoma, Wilms tumor, Retinoblastoma, Rhabdomyosarcoma, Nasopharynx carcinoma | ChemoT | NI |
| Olczak-Kowalczyk et al. (2018) [45] | Case–control | Poland | 60 | DMFT; dmft; DMFS; dmfs: teeth/surfaces with white spot lesions–WSL (D1 + 2/d1 + 2), following the ICDAS-II criteria | neoplasm; medulloblastoma (12.5%), nephroblastoma (Wilms’tumour,10.8%), Burkitt’s lymphoma (10.8%), neuroblastoma (8.3%), rhab- domyosarcoma (RMS, 6.6%), Ewing’s sarcoma (5.8%), and less frequently: chondrosarcoma, hepatoblastoma, glioblas- toma, ependimoma, and osteosarcoma. | Multidrug therapy, adapted to each neoplasm type and including vincristine, cyclophosphamide, adriamycin, etopo- side, cisplatin, ifosfamide, actomycin, and methotrexate; ChemoT for the others | NI |
| Bica et al. (2017) [16] | Retrospective | Romania | 36 | hypoplasia (hypomineralisation) of the enamel, microdontia and atypical eruption. | limphoblastic leukemia | ChemoT | NI |
| Krasuska-Sławińska et al. (2016) [38] | Case–control | Poland | 60 | oral hygiene, gingiva (PI), dentition, and potential visible decrease in salivary secretion. | Different neoplasms | PCH—60 patients after at least 1 year ChemoT CG—60 generally healthy patients. | NR |
| Owosho et al. (2016) [21] | Retrospective | United States of America | 13 | Facial asymmetry and jaw hypoplasia; Effects on the dental tissue causing tooth agenesis/hypodontia, root agenesis/stunting/malformation, and/or enamel hypoplasia; trismus, hyposalivation/xerostomia. | head and neck rhabdomyosarcoma (HNRMS)—Tumor sites were orbit in 1 patient and parameningeal in 12 (infratemporal fossa in 5, nasopharynx in 5, parapharyngeal in 1, and middle ear in 1) | multiagent ChemoT and IMRT—median radiation dose to the primary tumor was 50.4 Gy (range: 45–50.4 Gy), and the ChemoT agents were vincristine, doxorubicin, cyclophosphamide, ifosfamide, and etoposide | NI |
| Nemeth et al. (2014) [43] | Case–control | Hungary | 38 | DMFT; unstimulated saliva flow rate—spitting method (USF); stimulated saliva flow rate—spitting method (SSF); palatal saliva flow rate using a Periotron meter (Oraflow Inc., Plainview, NY, USA) (PS); salivary buffer capacity using CRT buffer (Ivoclar Vivadent AG, Schaan, Lichtenstein) | NI | 18 patients BFM-95 = protocol for acute lymphoblastic lymphoma, Berlin-Frankfurt-Munster; 5 patients NBL-2 = protocol for neuroblastoma; 4 patients CWS 96 = protocol of Cooperative Soft Tissue Sarcoma Study Group; 4 patients SIOP 93 = international protocol of the Interna- tional Society of Paediatric Oncology; 3 patients BFM-98 = protocol for acute lymphoblastic lymphoma, Berlin-Frankfurt-Munster; 2 patients COSS-96 = protocol of Cooperative Os- teosarcoma Study Group; 2 patients DAL-HD 90 = protocol for Hodgkins disease, No patients had radiotherapy treatment, nor bone marrow transplantation, nor stem cell transplantation | NI |
| Nemeth et al. (2013) [42] | Case–control | Hungary | 38 | DMFT; CPI; radiographic dental examination was used to analyze dental malforma- tions: agenesis, without third molars, microdontia, macrodontia, unerrupted teeth; root malformation | NI | 18 patients BFM-95 = protocol for acute lymphoblastic lymphoma, Berlin-Frankfurt-Munster; 5 patients NBL-2 = protocol for neuroblastoma; 4 patients CWS 96 = protocol of Cooperative Soft Tissue Sarcoma Study Group; 4 patients SIOP 93 = international protocol of the Interna- tional Society of Paediatric Oncology; 3 patients BFM-98 = protocol for acute lymphoblastic lymphoma, Berlin-Frankfurt-Munster; 2 patients COSS-96 = protocol of Cooperative Os- teosarcoma Study Group; 2 patients DAL-HD 90 = protocol for Hodgkins disease, No patients had radiotherapy treatment, nor bone marrow transplantation, nor stem cell transplantation | NI |
| Lauritano et al. (2012) [29] | Prospective | Italy | 52 | DMFT, microdontia, enamel hypoplasia, dental agenesis, v-shaped roots | Thirty- nine patients were affected by lymphoblastic leukaemia (ALL), the remaining ones were affected by acute myeloblastic leukaemia (AML) | Patients were treated according to Italian Association of Paediatric Hematoncology (AIEOP)—Methotrexate + Vincristine + Daunoblastine + Prednisone + Desamethasone. Seven patients with ALL received cranial irradiation (18 Gy) in addition to ChemoT and cytotoxic treatment | NR |
| Hutton et al. (2010) [17] | Retrospective | United Kingdom | 120 | DMFT index; dmft index; enamel opacities, fissure sealed, microdont; traumatized teeth; basic periodontal examination and gingival bleeding score in patients with fully erupted permanent incisors and first molars | Wilm’s tumour—29 patients (24.2%), rhabdomyosarcoma—10 patients (8.3%), Hodgkin’s lymphoma—14 patients (11.7%), non-Hodgkin’s lymphoma—10 patients (8.3%), neuroblastoma—21 patients (17.5%), and other solid tumour types—36 patients (30.0%) | ChemoT—four principal groups of chemo- therapeutic agent used: high-dose chemo- therapy with stem-cell rescue (HDCSCR); anthracycline drugs; alkylating agents; platinum drugs; and overlapping regimes | NR |
| Maciel et. al. (2009) [39] | Case–control | Brazil | 56 | agenesis, microdontia, macrodontia, short roots, tapering roots, enlarged pulp chambers, supernumerary teeth, taurodontism, DMFT score, visible plaque index (VPI), gingival bleeding index (GBI), saliva flow | ALL | ChemoT, Chemo/radiotherapy, Chemo/radio/BMT | Research Grant |
| Çubukçu et al. (2008) [33] | Case–control | Turkey | 62 | DMF/T, dmf/t | Non-Hodgkin lymphoma, Retinablastoma, Hodgkin lymphoma, Fibroma, Medulloblastoma, Wilms tumor, Nasopharyngeal carcinoma, Langerhans cell histiocytoma, Neuroblastoma, Malignant teratoma, Optical glioma, Rhabdomyosarcoma, Disgerminoma, Leiomyosarcoma, Hepatoblastoma | ChemoT | NI |
| Avşar et al. (2007) [27] | Retrospective | Turkey | 96 | DMFT, The Silness-Loe Plaque Index (PI) and Gingival Index (GI), Saliva assessment included salivary flow rate, salivary buffer capacity, mutans streptococci, and lactobacilli counting, disturbances of enamel mineralization, disturbances in dental development | Hodgkin’s or non-Hodgkin’s lymphoma | ChemoT | NI |
| Marec-Berard et al. (2005) [40] | Case–control | France | 27 | microdontia, excessive caries, root stunting, hypodontia, and enamel hypoplasia | nephroblastoma | Institutional protocol (SIOP 93 protocol) consisting of poly ChemoT with vincristine, actinomycin ± doxorubicin without any head and/or neck ir- radiation or high-dose ChemoT | NR |
| Oguz et al. (2004) [44] | Case–control | Turkey | 36 | DMFT; DMFS; Loe–Silness GI; Sillnes–Loe PI; enamel defects and discolorations; root malformations; eruption status; agenesis; premature apexifications and microdontia | non- Hodgkin’s lymphomas (NHL) | Twenty-seven patients were treated according to BFM-90 B cell protocol; while the LSA2 L2 protocol was used in 4 patients, and the LMT-89 protocol was administered in five patients | NI |
| Duggal et al. (2003) [35] | Case–control | United Kingdom | 69 | Calculation of root surface areas of mandibular teeth | Acute lymphoblastic leukaemia (43.3%); Wilms tumor (14.4%), Hodgkin’s disease (9.3%); CNS tumors (8.2%) Non Hodgkins lymphoma, acute myeloid leukaemia and other diagnoses | ChemoT, radiotherapy, and both chemo-and prophylactic cranial irradiation of between 16 and 22GY, or had received fractionated total body irradiation and a bone marrow transplant | NR |
| Pajari et al. (2001) [22] | Retrospective | Finland | 36 | DMFT | 18 suffering from leukemia and 18 from solid tumors | combination ChemoT and 4 patients also received cranial irradiation | NI |
| Alpaslan et al. (1999) [26] | Retrospective | NI | 32 | discoloration, enamel hypoplasia, crown/root malformation, unerupted teeth, premature apexification, microdontia, agenesis, gingival and plaque indexes, denatal caries, craniofacial growth | Hodgkin’s or non-Hodgkin’s lymphoma | ChemoT | NI |
| Kaste et al. (1998) [20] | Retrospective | United States of America | 52 | dental abnormalities | Neuroblastoma | 8 received head and/or neck irradiation, either as part of a preparative regimen for bone marrow transplantation (n= 2) or as local therapy of a metastasis (n = 6) | NR |
| Duggal et al. (1997) [36] | Case–control | United Kingdom | 46 | Enamel defects—modified developmental defects of enamel index (DDE index); DMFTS index; avaliação gengival | 22 acute lymphoblastic leukaemia; 6 Hodgkins disease; 4 Non- Hodgkins lymphoma; 6 brain tumours, 4 Wilm’s tumour; 4 other childhood malignancies. | Multi-drug ChemoT with or without cranial irradiation | NR |
| Kaste et al. (1997) [18] | Retrospective | United States of America | 423 | Dental abnormalities: root stunting (abnormally shortened roots), microdontia (abnormallly small teeth), or hypodontia (absent teeth) | ALL | Multiagent ChemoT; In addition, cranial irradiation (1800 or 2400 cGy) was given to 243 of the 423 children (55.6%). | NR |
| Kaste et al. (1995) [19] | Retrospective | United States of America | 22 | Dental abnormalities: root stunting, microdontia and hypodontia; multiple abnormalities. | Head and neck rhabdomyosarcoma | Multiagent ChemoT (including cyclophosphamide, Adriamy- cin, vincristine, and dactinomycin) and radiotherapy on four successive treatment regimens | NR |
| Sonis et al. (1995) [24] | Case–control | Belgium | 52 | DMFT; dmft: Gengival index; Plaque index | 27 acute lymphoblastic leukaemia; 7 non-Hodgkin’s lymphoma; 7 Wilms’ tumour; 5 rhabdomyosarcoma; 6 different childhood cancers | ChemoT. Patients had not received any radiotherapy to the oral or the salivary gland region | NI |
| Dens et al. (1995) [34] | Retrospective | NI | 64 | dmft; DMFT; OHI-S; modified loe and silness gingival index score | ALL | Varied combinations of chemotherapeutic agents: ChemoT alone (group 1); 1800 cGy (group 2); 2400 cGy (group 3) | NI |
| Näsman et al. (1994) [41] | Case–control | Sweden | 76 | Dental caries, salivary flow, salivary microbial counts, enamel disturbances, and disturbances in dental development | BMT group: 15 children were treated for acute leukemia, 1 for a B-cell lymphoma,3 for Gaucher’s disease, 1 for a severe combined immunodeficiency. ChT group: 21 were treated for acute leukemia, 9 for lymphoma,6 for Wilm’s tumor, 6 for rhabdomyosarcoma,3 for histiocytosis-X, 3 for neuroblastoma, 3 for optic glioma, 3 for other CNS-tumors, and 3 for other tumors | Bone marrow transplantation (BMT group); ChemoT | NR |
| Fleming et al. (1993) [37] | Case–control | Northern Ireland | 54 | Regularity of dental attendance; type of dentist visited; toothbrushing frequency; plaque presence on buccal and lingual surfaces; gengivitis (através do sangramento gengival ao passar com a sonda); DMFT index; dmft index | ALL | ChemoT | NR |
| Purdell-Lewis et al. (1988) [30] | Cohort | United Kingdom | 45 | oral hygiene index; papilllary bleeding index; number of erupted teeth relative to age; number of carious or filled primary and permanent teeth; percentage of primary teeth with initial lesions; percentage of erupted incisors, canines or permanent first molars with opacities (1), rough surfaces (2), vertical grooves (3), hypoplastic horizontal grooves and pits scored using DDE-index | acute lymphatic leukaemia, neuroblastoma, wilm’s tumor, rhabdomyosarcoma, Histiocytosis X, acute non-lymphatic leukemia | poly ChemoT | NI |
3.3. Methodological Quality of the Included Studies
3.4. Data Synthesis
3.4.1. Dental Anomalies Prevalence
3.4.2. Dental Anomalies Risk in Pediatric Cancer Patient Survivors Compared to Controls
3.5. Additional Analysis
4. Discussion
4.1. Summary of Main Findings
4.2. Implications for Practice and Research
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.G.; Moreno, F.; Dolya, A.; Bray, F.; Hesseling, P.; Shin, H.Y.; Stiller, C.A.; Bouzbid, S.; et al. International Incidence of Childhood Cancer, 2001–2010: A Population-Based Registry Study. Lancet Oncol. 2017, 18, 719–731. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. CureAll Framework: WHO Global Initiative for Childhood Cancer: Increasing Access, Advancing Quality, Saving Lives; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-002527-1. [Google Scholar]
- Proc, P.; Szczepańska, J.; Herud, A.; Zubowska, M.; Fendler, W.; Młynarski, W. Dental Caries among Childhood Cancer Survivors. Medicine 2019, 98, e14279. [Google Scholar] [CrossRef] [PubMed]
- Halperson, E.; Matalon, V.; Goldstein, G.; Saieg Spilberg, S.; Herzog, K.; Fux-Noy, A.; Shmueli, A.; Ram, D.; Moskovitz, M. The Prevalence of Dental Developmental Anomalies among Childhood Cancer Survivors According to Types of Anticancer Treatment. Sci. Rep. 2022, 12, 4485. [Google Scholar] [CrossRef] [PubMed]
- Carl, W.; Sako, K.; Schaaf, N.G. Dental Complications in the Treatment of Rhabdomyosarcoma of the Oral Cavity in Children. Oral Surg. Oral Med. Oral Pathol. 1974, 38, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.B.; Themudo, R.; Botelho, J.; Machado, V. Oral and Dental Abnormalities Caused by a Pediatric Rhabdomyosarcoma Tumor Treatment: A Clinical Case Report. Dent. J. 2020, 8, 59. [Google Scholar] [CrossRef]
- Dury, D.C.; Roberts, M.W.; Miser, J.S.; Folio, J. Dental Root Agenesis Secondary to Irradiation Therapy in a Case of Rhabdomyosarcoma of the Middle Ear. Oral Surg. Oral Med. Oral Pathol. 1984, 57, 595–599. [Google Scholar] [CrossRef]
- Jawad, H.; Hodson, N.A.; Nixon, P.J. A Review of Dental Treatment of Head and Neck Cancer Patients, before, during and after Radiotherapy: Part 2. Br. Dent. J. 2015, 218, 69–74. [Google Scholar] [CrossRef]
- Mod, D.; Mod, H.; Jha, A.K. Oral and Dental Complications of Head and Neck Radiotherapy and Their Management. J. Nepal. Health Res. Counc. 2013, 11, 300–304. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological Guidance for Systematic Reviews of Observational Epidemiological Studies Reporting Prevalence and Cumulative Incidence Data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, G. Meta: An R Package for Meta-Analysis. R News 2007, 7, 40–45. [Google Scholar]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Alnuaimi, E.; Al Halabi, M.; Khamis, A.; Kowash, M. Oral Health Problems in Leukaemic Paediatric Patients in the United Arab Emirates: A Retrospective Study. Eur. J. Paediatr. Dent. 2018, 19, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Bica, C.; Chincesan, M.; Esian, D.; Martha, K.; Ion, V.; Marinescu, L.A.; Earar, K.; Matei, M.N. Dental Development in Children After Chemotherapy. Rev. Chim. 2017, 68, 1397–1400. [Google Scholar] [CrossRef]
- Hutton, A.; Bradwell, M.; English, M.; Chapple, I. The Oral Health Needs of Children after Treatment for a Solid Tumour or Lymphoma: Oral Health Needs of Children. Int. J. Paediatr. Dent. 2010, 20, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Kaste, S.; Hopkins, K.; Jones, D.; Crom, D.; Greenwald, C.; Santana, V. Dental Abnormalities in Children Treated for Acute Lymphoblastic Leukemia. Leukemia 1997, 11, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Kaste, S.C.; Hopkins, K.P.; Bowman, L.C. Dental Abnormalities in Long-Term Survivors of Head and Neck Rhabdomyosarcoma. Med. Pediatr. Oncol. 1995, 25, 96–101. [Google Scholar] [CrossRef]
- Kaste, S.C.; Hopkins, K.P.; Bowman, L.C.; Santana, V.M. Dental Abnormalities in Children Treated for Neuroblastoma. Med. Pediatr. Oncol. 1998, 30, 22–27. [Google Scholar] [CrossRef]
- Owosho, A.A.; Brady, P.; Wolden, S.L.; Wexler, L.H.; Antonescu, C.R.; Huryn, J.M.; Estilo, C.L. Long-Term Effect of Chemotherapy–Intensity-Modulated Radiation Therapy (Chemo-IMRT) on Dentofacial Development in Head and Neck Rhabdomyosarcoma Patients. Pediatr. Hematol. Oncol. 2016, 33, 383–392. [Google Scholar] [CrossRef]
- Pajari, U.; Yliniemi, R.; Möttönen, M. The Risk of Dental Caries in Childhood Cancer Is Not High If the Teeth Are Caries-Free at Diagnosis. Pediatr. Hematol. Oncol. 2001, 18, 181–185. [Google Scholar] [CrossRef]
- Rabassa-Blanco, J.; Brunet-Llobet, L.; Marcote-Sinclair, P.; Balsells-Mejía, S.; Correa-Llano, M.G.; Miranda-Rius, J. Prevalence of, and Risk Factors for, Dental Sequelae in Adolescents Who Underwent Cancer Therapy during Childhood. Oral Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Sonis, A.L.; Waber, D.P.; Sallan, S.; Tarbell, N.J. The Oral Health of Long-Term Survivors of Acute Lymphoblastic Leukaemia: A Comparison of Three Treatment Modalities. Eur. J. Cancer Part B Oral Oncol. 1995, 31, 250–252. [Google Scholar] [CrossRef] [PubMed]
- Stolze, J.; Teepen, J.C.; Raber-Durlacher, J.E.; Loonen, J.J.; Kok, J.L.; Tissing, W.J.E.; de Vries, A.C.H.; Neggers, S.J.C.M.M.; van Dulmen-den Broeder, E.; van den Heuvel-Eibrink, M.M.; et al. Prevalence and Risk Factors for Hyposalivation and Xerostomia in Childhood Cancer Survivors Following Different Treatment Modalities—A Dutch Childhood Cancer Survivor Study Late Effects 2 Clinical Study (DCCSS LATER 2). Cancers 2022, 14, 3379. [Google Scholar] [CrossRef] [PubMed]
- Alpaslan, G.; Alpaslan, C.; Gögen, H.; Aynur, O.; Çetiner, S.; Karadeniz, C. Disturbances in Oral and Dental Structures in Patients with Pediatric Lymphoma after chemotherapyA Preliminary Report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1999, 87, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Avşar, A.; Elli, M.; Darka, Ö.; Pinarli, G. Long-Term Effects of Chemotherapy on Caries Formation, Dental Development, and Salivary Factors in Childhood Cancer Survivors. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Çetiner, D.; Çetiner, S.; Uraz, A.; Alpaslan, G.H.; Alpaslan, C.; Toygar Memikoğlu, T.U.; Karadeniz, C. Oral and Dental Alterations and Growth Disruption Following Chemotherapy in Long-Term Survivors of Childhood Malignancies. Support. Care Cancer 2019, 27, 1891–1899. [Google Scholar] [CrossRef]
- Lauritano, D.; Petruzzi, M. Decayed, Missing and Filled Teeth Index and Dental Anomalies in Long-Term Survivors Leukaemic Children: A Prospective Controlled Study. Med. Oral 2012, 17, e977–e980. [Google Scholar] [CrossRef]
- Purdell-Lewis, D.J.; Stalman, M.S.; Leeuw, J.A.; Humphrey, G.B.; Kalsbeek, H. Long Term Results of Chemotherapy on the Developing Dentition: Caries Risk and Developmental Aspects. Commun. Dent. Oral Epidemiol. 1988, 16, 68–71. [Google Scholar] [CrossRef]
- Shayani, A.; Aravena, P.C.; Rodríguez-Salinas, C.; Escobar-Silva, P.; Diocares-Monsálvez, Y.; Angulo-Gutiérrez, C.; Rivera, C. Chemotherapy as a Risk Factor for Caries and Gingivitis in Children with Acute Lymphoblastic Leukemia: A Retrospective Cohort Study. Int. J. Paediatr. Dent. 2022, 32, 538–545. [Google Scholar] [CrossRef]
- Seremidi, K.; Kavvadia, K.; Kattamis, A.; Polychronopoulou, A. Dental Late Effects of Antineoplastic Treatment on Childhood Cancer Survivors: Radiographic Findings. Int. J. Paediatr. Dent. 2021, 31, 742–751. [Google Scholar] [CrossRef]
- Çubukçu, Ç.E.; Sevinir, B. Dental Health Indices of Long-Term Childhood Cancer Survivors Who Had Oral Supervision during Treatment: A Case–Control Study. Pediatr. Hematol. Oncol. 2008, 25, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Dens, F.; Boute, P.; Otten, J.; Vinckier, F.; Declerck, D. Dental Caries, Gingival Health, and Oral Hygiene of Long Term Survivors of Paediatric Malignant Diseases. Arch. Dis. Child. 1995, 72, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Duggal, M.S. Root Surface Areas in Long-Term Survivors of Childhood Cancer. Oral Oncol. 2003, 39, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Duggal, M.S.; Curzon, M.E.J.; Bailey, C.C. Dental Parameters in the Long Term Survivors of Childhood Cancer Compared with Siblings. Oral Oncol. 1997, 33, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.; Kinirons, M.J. Study of the Dental Health of Children in Remission from Acute Lymphoblastic Leukaemia in Northern Ireland. Commun. Dent. Oral Epidemiol. 1993, 21, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Krasuska-Sławińska, E.; Brożyna, A.; Dembowska-Bagińska, B.; Olczak-Kowalczyk, D. Factors Influencing Caries Incidence in Permanent Teeth in Children/Adolescents under and after Anti-Neoplastic Treatment. Contemp. Oncol. Współczesna Onkol. 2016, 1, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Maciel, J.C.C.; de Castro, C.G.; Brunetto, A.L.; Di Leone, L.P.; da Silveira, H.E.D. Oral Health and Dental Anomalies in Patients Treated for Leukemia in Childhood and Adolescence: Dental Anomalies in Leukemia Patients. Pediatr. Blood Cancer 2009, 53, 361–365. [Google Scholar] [CrossRef]
- Marec-Berard, P.; Azzi, D.; Chaux-Bodard, A.G.; Lagrange, H.; Gourmet, R.; Bergeron, C. Long-Term Effects on Chemotherapy on Dental Status in Children Treated for Nephroblastoma. Pediatr. Hematol. Oncol. 2005, 22, 581–588. [Google Scholar] [CrossRef]
- Näsman, M.; Björk, O.; Söderhäll, S.; Ringdén, O.; Dahllöf, G. Disturbances in the Oral Cavity in Pediatric Long-Term Survivors after Different Forms of Antineoplastic Therapy. Pediatr. Dent. 1994, 16, 217–223. [Google Scholar]
- Nemeth, O.; Hermann, P.; Kivovics, P.; Garami, M. Long-Term Effects of Chemotherapy on Dental Status of Children Cancer Survivors. Pediatr. Hematol. Oncol. 2013, 30, 208–215. [Google Scholar] [CrossRef]
- Nemeth, O.; Kivovics, M.; Pinke, I.; Marton, K.; Kivovics, P.; Garami, M. Late Effects of Multiagent Chemotherapy on Salivary Secretion in Children Cancer Survivors. J. Am. Coll. Nutr. 2014, 33, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Oguz, A.; Cetiner, S.; Karadeniz, C.; Alpaslan, G.; Alpaslan, C.; Pinarli, G. Long-Term Effects of Chemotherapy on Orodental Structures in Children with Non-Hodgkin’s Lymphoma. Eur. J. Oral Sci. 2004, 112, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Olczak-Kowalczyk, D.; Krasuska-Sławińska, E.; Brożyna, A.; Turska-Szybka, A.; Dembowska-Bagińska, B. Dental Caries in Children and Adolescents During and After Antineoplastic Chemotherapy. J. Clin. Pediatr. Dent. 2018, 42, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Guagnano, R.; Romano, F.; Berger, M.; Fagioli, F.; Vallone, V.; Bello, L.; Vitale, M.C.; Defabianis, P. Long-Term Effect of Anticancer Therapy on Dentition of Italian Children in Remission from Malignant Disease: A Cross-Sectional Study. Eur. J. Paediatr. Dent. 2022, 23, 131–136. [Google Scholar] [CrossRef]
- Tanem, K.E.; Stensvold, E.; Wilberg, P.; Skaare, A.B.; Brandal, P.; Herlofson, B.B. Oral and Dental Late Effects in Long-Term Survivors of Childhood Embryonal Brain Tumors. Support. Care Cancer 2022, 30, 10233–10241. [Google Scholar] [CrossRef]
- Seremidi, K.; Kloukos, D.; Polychronopoulou, A.; Kattamis, A.; Kavvadia, K. Late Effects of Chemo and Radiation Treatment on Dental Structures of Childhood Cancer Survivors. A Systematic Review and Meta-analysis. Head Neck 2019, 41, 3422–3433. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Aggarwal, A.; Pai, K.M. Orofacial Mani-festations of Leukemic Children on Treatment: A Descriptive Study. Int J Clin Pediatr Dent 2018, 11, 193–198. [Google Scholar]
- Alberth, M.; Kovalecz, G.; Nemes, J.; Math, J.; Kiss, C.; Marton, I.J. Oral Health of Long-Term Childhood Cancer Survivors. Pediatr Blood Cancer 2004, 43, 88–90. [Google Scholar] [CrossRef]
- Ali, M.; Nurelhuda, N. Oral health status and its determinants in children with leukaemia at the Radiation and Isotope Center Khartoum, Khartoum State, Sudan. Sudan. J. Paediatr. 2019, 19, 93–100. [Google Scholar] [CrossRef]
- Azher, U.; Shiggaon, N. Oral health status of children with acute lymphoblastic leukemia undergoing chemotherapy. Indian J. Dent. Res. 2013, 24, 523. [Google Scholar] [CrossRef] [PubMed]
- Velten, D.B.; Zandonade, E.; Miotto, M.H.M.d.B. Prevalence of oral manifestations in children and adolescents with cancer submitted to chemotherapy. BMC Oral Heal. 2016, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Childers, N.K.; Stinnett, E.A.; Wheeler, P.; Wright, J.; Castleberry, R.P.; Dasanayake, A.P. Oral complications in children with cancer. Oral Surgery, Oral Med. Oral Pathol. 1993, 75, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.C.; Bezerra, P.M.M.; Damascena, L.C.L.; Ribeiro, I.L.A.; Bonan, P.R.F.; de Sousa, S.A.; Almeida, L.d.F.D.; Valença, A.M.G. Impact of Saliva and Cariogenic Microbiota on the Chemotherapy-Induced Oral Mucositis in Oncopediatric Patients: A Preliminary Longitudinal Study. Int. J. Dent. 2020, 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Curtis, A.B. Childhood Leukemias: Initial Oral Manifestations. J. Am. Dent. Assoc. 1971, 83, 159–164. [Google Scholar] [CrossRef]
- El-Housseiny, A.A.; Saleh, S.M.; El-Masry, A.A.; Allam, A.A. Assessment of Oral Complications in Children Receiving Chemotherapy. J. Clin. Pediatr. Dent. 2007, 31, 267–273. [Google Scholar] [CrossRef]
- Fayle, S.A.; Curzon, M.E. Oral complications in pediatric oncology patients. Pediatr Dent. 1991, 13, 289–295. [Google Scholar]
- Gandhi, K.; Datta, G.; Ahuja, S.; Saxena, T.; Datta, A.G. Prevalence of Oral Complications occurring in a Popu-lation of Pediatric Cancer Patients receiving Chemotherapy. Int Int. J. Clin. Pediatr. Dent. 2017, 10, 166–171. [Google Scholar]
- Gravina, H.G.; De Morán, E.G.; Zambrano, O.; Chourio, M.L.; De Valero, S.R.; Robertis, S.; Mesa, L. Oral Candidiasis in children and adolescents with cancer. Med. Oral. Patol. Oral. Cir. Bucal. 2007, 12, e419-423. [Google Scholar]
- Gupta, A.; Marwaha, M.; Bansal, K.; Sachdeva, A.; Gupta, A. Dental Awareness among Parents and Oral Health of Paediatric Cancer Patients Receiving Chemotherapy. J Clin Diagn Res. 2016, 10, 92–95. [Google Scholar] [CrossRef]
- Hegde, A.; Joshi, S.; Rai, K.; Shetty, S. Evaluation of Oral Hygiene Status, Salivary Characteristics and Dental Caries Experience in Acute Lymphoblastic Leukemic (ALL) Children. J. Clin. Pediatr. Dent. 2011, 35, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Hovi, L.; Saarinen, U.M.; Donner, U.; Lindqvist, C. Opportunistic Osteomyelitis in the Jaws of Children on Immunosuppressive Chemotherapy. J. Pediatr. Hematol. 1996, 18, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Kaste, S.C.; Hopkins, K.P.; Jenkins, J.J. Abnormal odontogenesis in children treated with radiation and chemotherapy: Imaging findings. Am. J. Roentgenol. 1994, 162, 1407–1411. [Google Scholar] [CrossRef] [PubMed]
- Kowlessar, A.; Naidu, R.; Ramroop, V.; Nurse, J.; Dookie, K.; Bodkyn, C.; Lalchandani, S. Oral health among children attending an oncology clinic in Trinidad. Clin. Exp. Dent. Res. 2019, 5, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Kung, A.Y.; Zhang, S.; Zheng, L.W.; Wong, G.H.; Chu, C.H. Oral Health Status of Chinese Paediatric and Adolescent Oncology Patients with Chemotherapy in Hong Kong: A Pilot Study. Open Dent. J. 2015, 9, 21–30. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Levy-Polack, M.P.; Sebelli, P.; Polack, N.L. Incidence of oral complications and application of a preventive protocol in children with acute leukemia. Spéc. Care Dent. 1998, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Lula, E.C.O.; Lula, C.E.O.; Alves, C.M.C.; Lopes, F.F.; Pereira, A.L.A. Chemotherapy-induced oral complications in leukemic patients. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 1681–1685. [Google Scholar] [CrossRef]
- Marangoni-Lopes, L.; Rodrigues, L.; Mendonça, R.; Santos, M.N.-D. Radiotherapy changes salivary properties and impacts quality of life of children with Hodgkin disease. Arch. Oral Biol. 2016, 72, 99–105. [Google Scholar] [CrossRef]
- Mathur, V.P.; Kalra, G.; Dhillon, J.K. Oral health in children with leukemia. Indian J. Palliat. Care 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Morais, E.F.; Lira, J.A.S.; Macedo, R.A.P.; Santos, K.S.; Elias, C.T.V.; Arruda-Morais, M.L.S. Oral manifestations resulting from chemotherapy in children with acute lymphoblastic leukemia. Braz. J. Otorhinolaryngol. 2014, 80, 78–85. [Google Scholar]
- Mougeot, J.-L.C.; Stevens, C.B.; Almon, K.G.; Paster, B.J.; Lalla, R.V.; Brennan, M.T.; Mougeot, F.B. Caries-associated oral microbiome in head and neck cancer radiation patients: A longitudinal study. J. Oral Microbiol. 2019, 11, 1586421. [Google Scholar] [CrossRef] [PubMed]
- Nasim, V.S.; Shetty, Y.R.; Hegde, A.M. Dental Health Status in Children with Acute Lymphoblastic Leukemia. J. Clin. Pediatr. Dent. 2007, 31, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Neto, A.E.M.; Westphalen, F.H. Analysis of oral complications related to cancer therapy. Arch. Oral Res. 2013, 9, 159. [Google Scholar] [CrossRef]
- Nikoui, M.; Lalonde, B. Manifestations bucco-dentaires de la leucémie chez l'enfant [Oro-dental manifestations of leukemia in children]. J. Can Dent Assoc. 1996, 62, 443–450. [Google Scholar] [PubMed]
- O'Sullivan, E.A.; Duggal, M.S.; Bailey, C.C. Changes in the oral health of children during treatment for acute lymphoblastic leukaemia. Int. J. Paediatr. Dent. 2009, 4, 31–34. [Google Scholar] [CrossRef]
- Olszewska, K.; Mielnik-Błaszczak, M. An Assessment of the Number of Cariogenic Bacteria in the Saliva of Children with Chemotherapy-Induced Neutropenia. Adv. Clin. Exp. Med. 2016, 25, 11–19. [Google Scholar] [CrossRef]
- Orback, R.; Orbak, Z. Oral condition of patients with leukemia and lymphoma J. Nihon. Univ. Sch. Dent. 1997, 39, 67–70. [Google Scholar] [CrossRef]
- Ou-Yang, L.-W.; Chang, P.-C.; Tsai, A.; Jaing, T.-H.; Lin, S.-Y. Salivary microbial counts and buffer capacity in children with acute lymphoblastic leukemia. Pediatr. Dent. 2010, 32. [Google Scholar]
- Parra, J.J.; Alvarado, M.C.; Monsalve, P.; Costa, A.L.F.; Montesinos, G.A.; Parra, P.A. Oral health in children with acute lymphoblastic leukaemia: Before and after chemotherapy treatment. Eur. Arch. Paediatr. Dent. 2019, 21, 129–136. [Google Scholar] [CrossRef]
- Ponce-Torres, E.; Ruíz-Rodríguez, M.d.S.; Alejo-González, F.; Hernández-Sierra, J.F.; de Pozos-Guillén, A. Oral Manifestations in Pediatric Patients Receiving Chemotherapy for Acute Lymphoblastic Leukemia. J. Clin. Pediatr. Dent. 2010, 34, 275–279. [Google Scholar] [CrossRef]
- Ribeiro, I.L.A.; Silva, S.M.; Limeira, R.R.T.; Bonan, P.R.F.; Valença, A.M.G.; Neto, E.A.d.L.; de Castro, R.D. Differences between the oral changes presented by patients with solid and hematologic tumors during the chemotherapeutic treatment. J. Appl. Oral Sci. 2020, 28, e20190020. [Google Scholar] [CrossRef] [PubMed]
- Ritwik, P. Dental Care for Patients With Childhood Cancers. Ochsner J. 2018, 18, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.E.; Hopkins, K.; Wilbur, R.B. Acute necrotizing Ulcerative Gengivitis in Children with Cancer. Am. J. Dis. Child. 1983, 137. [Google Scholar]
- Sahai, P.; Mohanti, B.K.; Sharma, A.; Thakar, A.; Bhasker, S.; Kakkar, A.; Sharma, M.C.; Upadhyay, A.D. Clinical outcome and morbidity in pediatric patients with nasopharyngeal cancer treated with chemoradiotherapy. Pediatr. Blood Cancer 2016, 64, 259–266. [Google Scholar] [CrossRef]
- Sepúlveda-Tebache, E.; Brethauer-Meier, U.; Jiménez-Moraga, M.; Mora- les-Figueroa, R.; Rojas-Castro, J.; Le Fort-Canales, P. Detección del virus herpes simple en lesiones de la mucosa oral en pacientes con terapia oncológica. Med. Oral. 2003, 8, 329–333. [Google Scholar] [PubMed]
- Tao, C.-J.; Liu, X.; Tang, L.-L.; Mao, Y.-P.; Chen, L.; Li, W.-F.; Yu, X.-L.; Liu, L.-Z.; Zhang, R.; Lin, A.-H.; et al. Long-term outcome and late toxicities of simultaneous integrated boost-intensity modulated radiotherapy in pediatric and adolescent nasopharyngeal carcinoma. Chin. J. Cancer 2013, 32, 525–532. [Google Scholar] [CrossRef]
- Velten, D.B.; Zandonade, E.; Miotto, M.H.M.d.B. Prevalence of oral manifestations in children and adolescents with cancer submitted to chemotherapy. BMC Oral Heal. 2017, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Visnapuu, V.; Peltonen, S.; Alivuotila, L.; Happonen, R.-P.; Peltonen, J. Craniofacial and oral alterations in patients with Neurofibromatosis 1. Orphanet J. Rare Dis. 2018, 13, 1–9. [Google Scholar] [CrossRef]
- Wang, Y.; Zeng, X.; Yang, X.; Que, J.; Du, Q.; Zhang, Q.; Zou, J. Oral Health, Caries Risk Profiles, and Oral Microbiome of Pediatric Patients with Leukemia Submitted to Chemotherapy. BioMed Res. Int. 2021, 2021, 1–11. [Google Scholar] [CrossRef]
- White, G.E.; Cambridge, M. Oral manifestations of leukemia in children. Oral. Surg. 1970, 29. [Google Scholar] [CrossRef]

| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Overall |
|---|---|---|---|---|---|---|---|---|---|
| Halperson et al. (2022) [4] | U | Y | Y | Y | Y | N | Y | Y | High |
| Shayani et al. (2022) [31] | Y | N | Y | Y | Y | N | Y | Y | High |
| Rabassa-Blanco et al. (2022) [23] | Y | N | Y | Y | N | N | Y | Y | High |
| Stolze et al. (2022) [25] | Y | Y | Y | Y | N | N | Y | Y | High |
| Tanem et al. (2022) [47] | Y | Y | Y | Y | Y | N | Y | Y | High |
| Guagnano et al. (2022) [46] | N | N | Y | Y | N | N | Y | Y | High |
| Seremidi et al. (2021) [32] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Proc et al. (2019) [3] | U | Y | Y | Y | Y | Y | Y | Y | Unclear |
| Alnuaimi et al. (2018) [15] | U | N | U | Y | Y | N | Y | Y | High |
| Çetiner et al. (2019) [28] | U | Y | Y | Y | Y | Y | Y | Y | Unclear |
| Olczak-Kowalczyk et al. (2018) [45] | Y | Y | Y | Y | Y | N | Y | Y | High |
| Bica et al. (2017) [16] | Y | U | Y | Y | N | N | Y | Y | High |
| Krasuska-Sławińska et al. (2016) [38] | U | Y | Y | Y | Y | N | Y | Y | High |
| Owosho et al. (2016) [21] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Nemeth et al. (2014) [43] | Y | Y | Y | Y | Y | N | N | Y | High |
| Nemeth et al. (2013) [42] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Lauritano et al. (2012) [29] | U | Y | Y | Y | Y | Y | Y | Y | Unclear |
| Hutton et al. (2010) [17] | U | Y | Y | Y | N | N | Y | Y | High |
| Maciel et. al. (2009) [39] | U | Y | Y | Y | N | N | Y | Y | High |
| Çubukçu et al. (2008) [33] | U | Y | Y | Y | N | N | Y | Y | High |
| Avşar et al. (2007) [27] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Marec-Berard et al. (2005) [40] | U | Y | Y | Y | N | N | Y | Y | High |
| Oguz et al. (2004) [44] | U | Y | Y | Y | Y | Y | Y | Y | Unclear |
| Duggal et al. (2003) [35] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Pajari et al. (2001) [22] | U | Y | N | N | Y | N | Y | Y | High |
| Alpaslan et al. (1999) [26] | U | Y | Y | Y | Y | N | Y | Y | High |
| Kaste et al. (1998) [20] | U | N | Y | Y | Y | N | Y | Y | High |
| Duggal et al. (1997) [36] | Y | Y | Y | Y | N | N | Y | Y | High |
| Kaste et al. (1997) [18] | U | N | Y | Y | N | N | Y | Y | High |
| Kaste et al. (1995) [19] | U | N | Y | Y | N | N | Y | Y | High |
| Sonis et al. (1995) [24] | U | Y | Y | Y | Y | Y | Y | Y | Unclear |
| Dens et al. (1995) [34] | U | Y | Y | Y | Y | Y | Y | Y | Unclear |
| Näsman et al. (1994) [41] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Fleming et al. (1993) [37] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Purdell-Lewis et al. (1988) [30] | Y | Y | Y | Y | Y | Y | Y | Y | Low |
| Clinical Alteration | Studies (n) | Cases (n) | Effect | I2 | p-Value | Egger Test |
|---|---|---|---|---|---|---|
| Root development alteration | 10 | 595 | 0.29 (0.16; 0.43) | 92 | <0.0001 | 0.6154 |
| Crown-root malformation | 11 | 1052 | 0.31 (0.20; 0.44) | 92 | <0.0001 | 0.4814 |
| Unerupted teeth | 4 | 159 | 0.24 (0.15; 0.34) | 49 | 0.1176 | - |
| Enamel hypoplasia | 13 | 695 | 0.32 (0.21; 0.45) | 91 | <0.0001 | 0.1060 |
| Hypodontia | 6 | 765 | 0.13(0.05; 0.23) | 89 | <0.0001 | - |
| Discoloration | 4 | 241 | 0.53 (0.42; 0.65) | 64 | 0.0397 | - |
| Agenesis | 10 | 521 | 0.36 (0.27; 0.45) | 77 | <0.0001 | 0.0677 |
| Microdontia | 14 | 1237 | 0.16 (0.09; 0.24) | 91 | <0.0001 | 0.6624 |
| Macrodontia | 5 | 722 | 0.07 (0.04; 0.12) | 71 | 0.0077 | - |
| Clinical Alteration | Studies (n) | Cases/Controls (n/n) | Effect | I2 | p-Value | Egger Test |
|---|---|---|---|---|---|---|
| Root development alteration | 5 | 272/260 | 6.91 (3.89; 12.29) | 0 | 0.4406 | 6.91 (3.89; 12.29) |
| Crown-root malformation | 5 | 269/244 | 1.60 (0.32; 7.98) | 95 | <0.0001 | 1.61 (0.24; 10.61) |
| Unerupted teeth | 3 | 121/96 | 1.50 (0.62; 3.60) | 40 | 0.1877 | 1.50 (0.62; 3.60) |
| Enamel hypoplasia | 7 | 401/310 | 1.95 (1.32; 2.88) | 0 | 0.6990 | 1.95 (1.32; 2.88) |
| Discoloration | 3 | 121/96 | 5.68 (3.02; 10.7) | 0 | 0.6825 | 5.68 (3.02; 10.7) |
| Agenesis | 8 | 415/392 | 3.50 (1.98; 6.16) | 52 | 0.0333 | 3.50 (1.98; 6.19) |
| Microdontia | 7 | 362/352 | 9.49 (3.13; 28.70) | 22 | 0.2983 | 9.13 (3.17; 26.30) |
| Macrodontia | 3 | 190/192 | 1.90 (0.60; 5.99) | 0 | 0.5527 | 1.90 (0.60; 5.99) |
| Sensitivity Analysis | Studies (n) | Cases (n) | Effect | I2 (%) | p-Value |
|---|---|---|---|---|---|
| Root development alteration | |||||
| Low ROB | 2 | 109 | 0.59 (0.49; 0.68) | 0 | <0.0001 |
| High or Unclear ROB | 8 | 486 | 0.22 (0.11; 0.35) | 90 | |
| Crown-root malformation | |||||
| Low ROB | 2 | 134 | 0.40 (0.18; 0.63) | 84 | 0.7064 |
| High or Unclear ROB | 9 | 848 | 0.35 (0.26; 0.44) | 82 | |
| Unerupted teeth | |||||
| Low ROB | 1 | 38 | 0.15 (0.06; 0.29) | - | 0.1848 |
| High or Unclear ROB | 3 | 121 | 0.27 (0.17; 0.39) | 48 | |
| Enamel hypoplasia | |||||
| Low ROB | 4 | 230 | 0.27 (0.04; 0.60) | 96 | 0.6724 |
| High or Unclear ROB | 9 | 465 | 0.35 (0.23; 0.47) | 87 | |
| Low ROB | 3 | 147 | 0.38 (0.16; 0.62) | 85 | 0.8598 |
| High or Unclear ROB | 7 | 374 | 0.35 (0.26; 0.46) | 76 | |
| Microdontia | |||||
| Low ROB | 2 | 134 | 0.16 (0.00; 0.48) | 93 | 0.9748 |
| High or Unclear ROB | 12 | 1103 | 0.16 (0.09; 0.25) | 91 | |
| Macrodontia | |||||
| Low ROB | 2 | 134 | 0.04 (0.01; 0.09) | 0 | 0.2247 |
| High or Unclear ROB | 3 | 722 | 0.10 (0.03; 0.18) | 84 |
| Clinical Alteration | Estimate | 95% CI | p-Value |
|---|---|---|---|
| Root development alteration | −0.16 | −0.25; −0.07 | 0.0004 |
| Crown-root malformation | 0.01 | −0.08; 0.09 | 0.8895 |
| Unerupted teeth | 0.04 | −0.09; 0.16 | 0.5626 |
| Enamel hypoplasia | 0.13 | 0.07; 0.20 | 0.0001 |
| Hypodontia | −0.15 | −0.50; 0.20 | 0.3901 |
| Discoloration | 0.08 | 0.02; 0.13 | 0.0047 |
| Agenesis | 0.04 | −0.05; 0.13 | 0.3825 |
| Microdontia | −0.09 | −0.16; −0.01 | 0.0204 |
| Macrodontia | −0.01 | −0.41; 0.39 | 0.9632 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pombo Lopes, J.; Rodrigues, I.; Machado, V.; Botelho, J.; Bandeira Lopes, L. Chemotherapy and Radiotherapy Long-Term Adverse Effects on Oral Health of Childhood Cancer Survivors: A Systematic Review and Meta-Analysis. Cancers 2024, 16, 110. https://doi.org/10.3390/cancers16010110
Pombo Lopes J, Rodrigues I, Machado V, Botelho J, Bandeira Lopes L. Chemotherapy and Radiotherapy Long-Term Adverse Effects on Oral Health of Childhood Cancer Survivors: A Systematic Review and Meta-Analysis. Cancers. 2024; 16(1):110. https://doi.org/10.3390/cancers16010110
Chicago/Turabian StylePombo Lopes, Joana, Inês Rodrigues, Vanessa Machado, João Botelho, and Luísa Bandeira Lopes. 2024. "Chemotherapy and Radiotherapy Long-Term Adverse Effects on Oral Health of Childhood Cancer Survivors: A Systematic Review and Meta-Analysis" Cancers 16, no. 1: 110. https://doi.org/10.3390/cancers16010110
APA StylePombo Lopes, J., Rodrigues, I., Machado, V., Botelho, J., & Bandeira Lopes, L. (2024). Chemotherapy and Radiotherapy Long-Term Adverse Effects on Oral Health of Childhood Cancer Survivors: A Systematic Review and Meta-Analysis. Cancers, 16(1), 110. https://doi.org/10.3390/cancers16010110