

Circulating Tumour DNA (ctDNA) as a Predictor of Clinical Outcome in Non-Small Cell Lung Cancer Undergoing Targeted Therapies: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methodology
2.1. Eligibility Criteria
2.2. Search Strategy and Sources
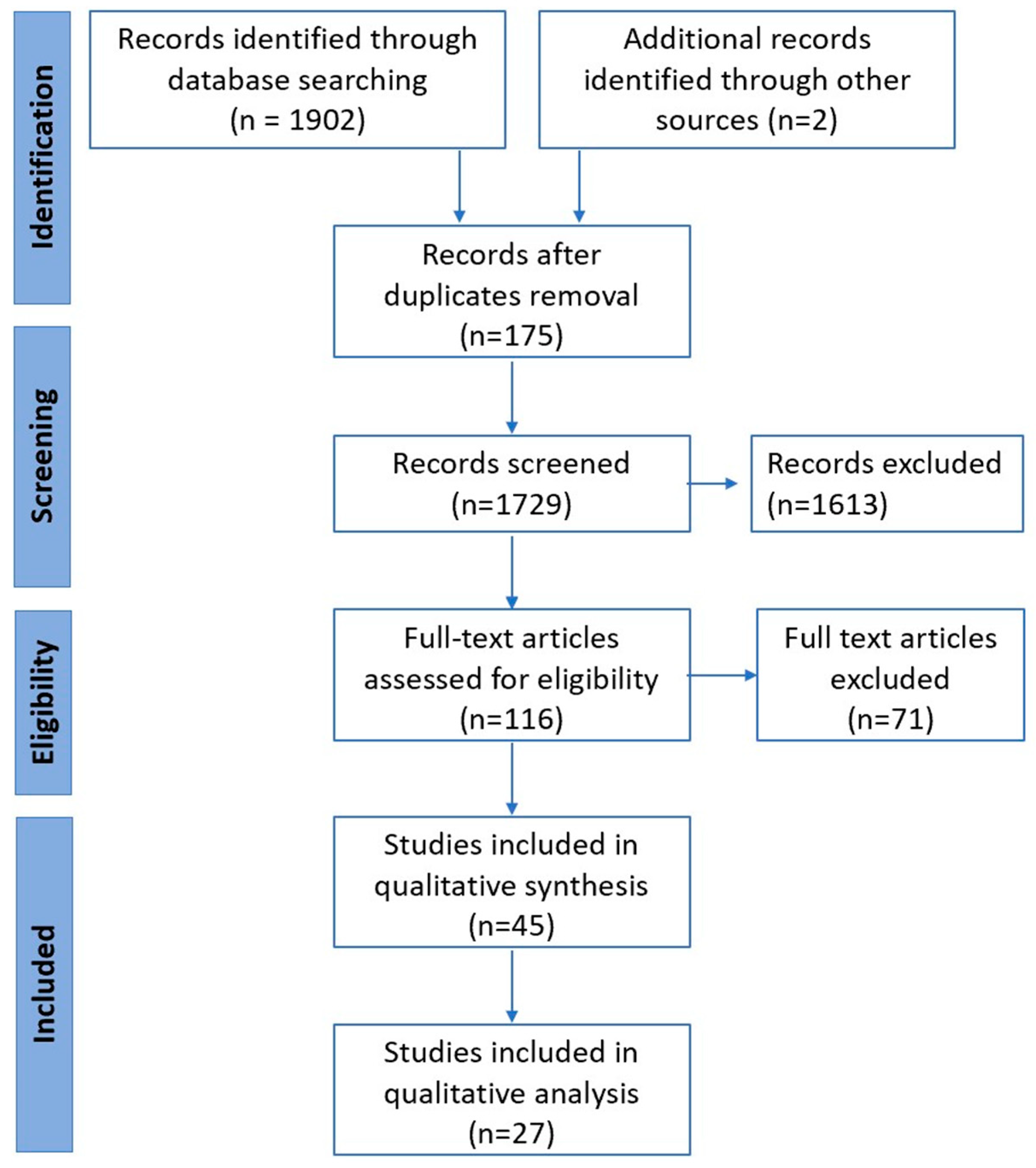
2.3. Study Selection and Data Extraction
2.4. Quality Assessment and Risk of Bias in Individual Studies
2.5. Study Aims and Outcomes
2.6. Data Collection and Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Patient Demographics
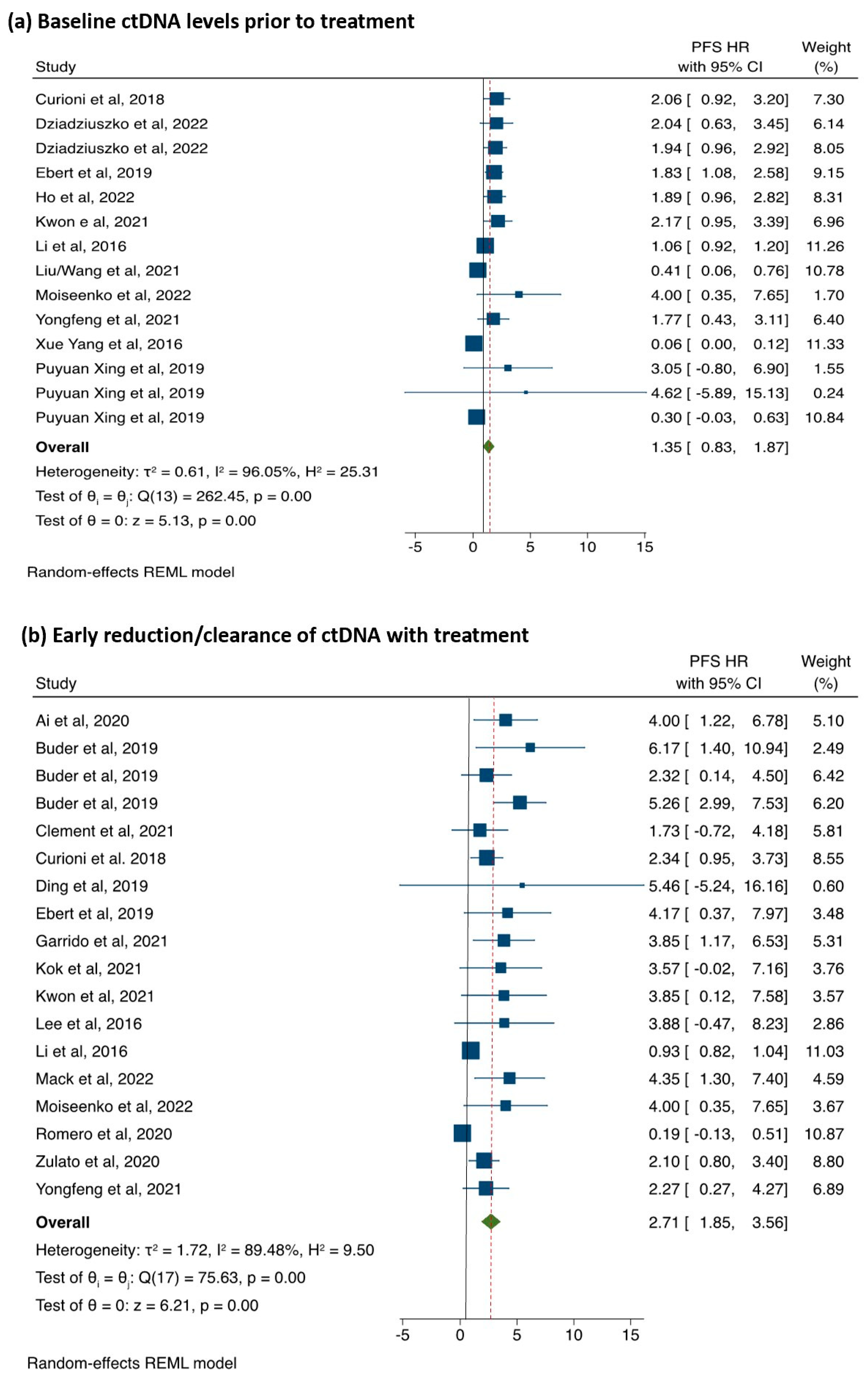
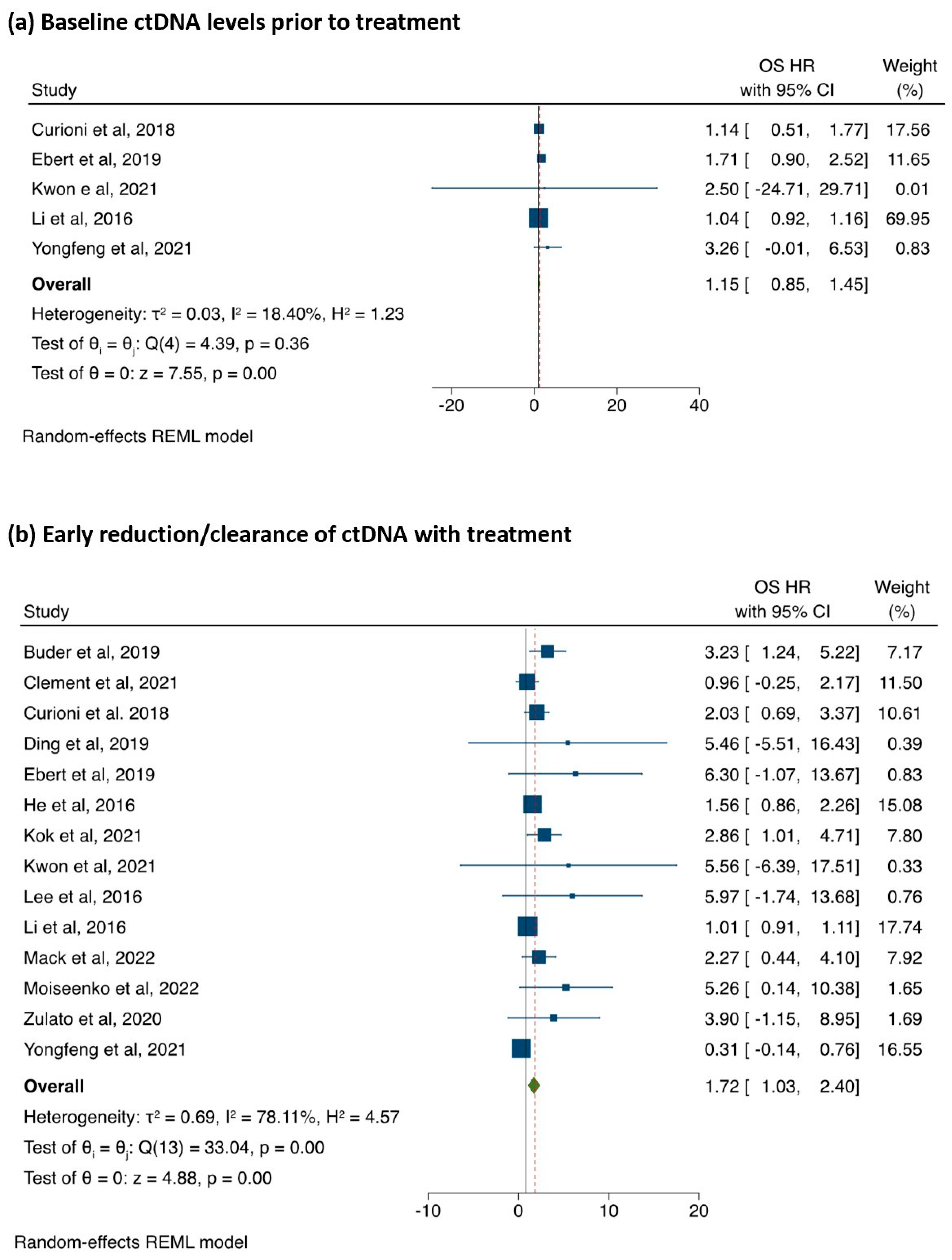
3.3. The Association between ctDNA Detection and PFS
3.4. Subgroup Analysis
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Declarations
List of Abbreviations
| ALK | Anaplastic lymphoma kinase |
| AMP | Association for Molecular Pathology |
| BRAF | v-raf murine sarcoma viral oncogene homolog B1 |
| CAP | College of American Pathologists |
| cfDNA | Cell-free DNA |
| ctDNA | Circulating-tumour DNA |
| CI | Confidence interval |
| CNV | Copy number variation |
| ddPCR | Droplet digital polymerase chain reaction |
| ECOG | Eastern Cooperative Oncology Group |
| EGFR | Epidermal growth factor receptor |
| HER2 | Human epidermal growth factor receptor 2 |
| HR | Hazard ratio |
| IASLC | International Association for the Study of Lung Cancer |
| KRAS | Kirsten rat sarcoma |
| LB | Liquid biopsy |
| MeSH | Medical subject headings |
| MET | Mesenchymal–epithelial transition factor |
| mOS | Medial overall survival |
| mPFS | Median progression-free survival |
| MRD | Minimal residual disease |
| NGS | Next-generation sequencing |
| NSCLC | Non-small-cell lung cancer |
| NOS | Newcastle–Ottawa Scale |
| NTRK | Neurotrophic tyrosine receptor kinase |
| ORR | Overall response rate |
| OS | Overall survival |
| PCR | Polymerase chain reaction |
| PD-L1 | Programmed-death-ligand 1 |
| PFS | Progression-free survival |
| pHR | Pooled hazard ratio |
| PRISMA | Preferred Reporting Items for Systemic Review and Meta-Analyses |
| RET | Rearranged during transfection |
| ROS-1 | C-ros oncogene 1 |
| TKI | Tyrosine kinase inhibitor |
| TSG | Tumour suppressor gene |
| VAF | Variant allele frequency |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients with Non–Small Cell Lung Cancer in the US. JAMA Oncol. 2021, 7, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Abdel Karim, N.; Kelly, K. Role of Targeted Therapy and Immune Checkpoint Blockers in Advanced Non-Small Cell Lung Cancer: A Review. Oncologist 2019, 24, 1270–1284. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, C.; Mack, P.C.; Scagliotti, G.V.; Baas, P.; Barlesi, F.; Bivona, T.G.; Herbst, R.S.; Mok, T.S.; Peled, N.; Pirker, R.; et al. Liquid Biopsy for Advanced Non-Small Cell Lung Cancer (NSCLC): A Statement Paper from the IASLC. J. Thorac. Oncol. 2018, 13, 1248–1268. [Google Scholar] [CrossRef]
- Heitzer, E.; van den Broek, D.; Denis, M.G.; Hofman, P.; Hubank, M.; Mouliere, F.; Paz-Ares, L.; Schuuring, E.; Sultmann, H.; Vainer, G.; et al. Recommendations for a practical implementation of circulating tumor DNA mutation testing in metastatic non-small-cell lung cancer. ESMO Open 2022, 7, 100399. [Google Scholar] [CrossRef]
- Lim, Z.F.; Ma, P.C. Emerging insights of tumor heterogeneity and drug resistance mechanisms in lung cancer targeted therapy. J. Hematol. Oncol. 2019, 12, 134. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabieres, C.; Pantel, K. Liquid biopsy: From discovery to clinical application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef]
- Lone, S.N.; Nisar, S.; Masoodi, T.; Singh, M.; Rizwan, A.; Hashem, S.; El-Rifai, W.; Bedognetti, D.; Batra, S.K.; Haris, M.; et al. Liquid biopsy: A step closer to transform diagnosis, prognosis and future of cancer treatments. Mol. Cancer 2022, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Gilson, P.; Merlin, J.L.; Harle, A. Deciphering Tumour Heterogeneity: From Tissue to Liquid Biopsy. Cancers 2022, 14, 1384. [Google Scholar] [CrossRef]
- Sacher, A.G.; Oxnard, G.R.; Mach, S.L.; Melissa, M.M.; Jackman, D.M.; Janne, P.A.; Paweletz, C. Prediction of lung cancer genotype noninvasively using droplet digital PCR (ddPCR) analysis of cell-free plasma DNA (cfDNA). J. Clin. Oncol. Conf. 2014, 32, 8059. [Google Scholar] [CrossRef]
- Sacher, A.G. Fundamental concepts in the application of plasma genotyping (liquid biopsy) to EGFR mutation detection in non-small-cell lung cancer. JCO Precis. Oncol. 2018, 2, 1–12. [Google Scholar] [CrossRef]
- Batra, U.; Nathany, S.; Sharma, M.; Jain, P.; Dhanda, S.; Singh, H.; Jain, A.; Mehta, A. EGFR detection by liquid biopsy: Ripe for clinical usage. Future Oncol. 2022, 18, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.; Okamoto, I.; Sriuranpong, V.; Vansteenkiste, J.; Imamura, F.; Lee, J.S.; Pang, Y.; Cobo, M.; Kasahara, K.; Hodge, R.; et al. Osimertinib vs. SoC EGFR-TKI as first-line treatment in patients with EGFRm advanced NSCLC (FLAURA): Plasma ctDNA analysis. J. Thorac. Oncol. 2017, 12 (Suppl. S2), S1754–S1755. [Google Scholar] [CrossRef]
- Reungwetwattana, T.; Gray, J.; Markovets, A.; Nogami, N.; Lee, J.S.; Cho, B.C.; Chewaskulyong, B.; Majem, M.; Peled, N.; Vishwanathan, K.; et al. Longitudinal circulating tumour DNA (ctDNA) monitoring for early detection of disease progression and resistance in advanced NSCLC in FLAURA. Ann. Oncol. 2019, 30 (Suppl. S9), ix199. [Google Scholar] [CrossRef]
- Bischoff, H.; Zhou, C.; Imamura, F.; Cheng, Y.; Okamoto, I.; Cho, B.C.; Lin, M.C.; Majem, M.; Gautschi, O.; Gray, J.E.; et al. Early clearance of plasma EGFR mutations as a predictor of response to osimertinib and comparator EGFR-TKIS in the flaura trial. Oncol. Res. Treat. 2020, 43 (Suppl. S1), 122. [Google Scholar]
- Pascual, J.; Attard, G.; Bidard, F.C.; Curigliano, G.; De Mattos-Arruda, L.; Diehn, M.; Italiano, A.; Lindberg, J.; Merker, J.D.; Montagut, C.; et al. ESMO recommendations on the use of circulating tumour DNA assays for patients with cancer: A report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2022, 33, 750–768. [Google Scholar] [CrossRef]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. J. Thorac. Oncol. 2018, 13, 323–358. [Google Scholar] [CrossRef] [PubMed]
- Gale, D.; Heider, K.; Ruiz-Valdepenas, A.; Hackinger, S.; Perry, M.; Marsico, G.; Rundell, V.; Wulff, J.; Sharma, G.; Knock, H.; et al. Residual ctDNA after treatment predicts early relapse in patients with early-stage non-small cell lung cancer. Ann. Oncol. 2022, 33, 500–510. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Eriksen, M.; Frandsen, T. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 February 2023).
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Hebert, A.E.; Kreaden, U.S.; Yankovsky, A.; Guo, D.; Li, Y.; Lee, S.H.; Liu, Y.; Soito, A.B.; Massachi, S.; Slee, A.E. Methodology to standardize heterogeneous statistical data presentations for combining time-to-event oncologic outcomes. PLoS ONE 2022, 17, e0263661. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Yang, X.; Zhuo, M.; Ye, X.; Bai, H.; Wang, Z.; Sun, Y.; Zhao, J.; An, T.; Duan, J.; Wu, M.; et al. Quantification of mutant alleles in circulating tumor DNA can predict survival in lung cancer. Oncotarget 2016, 7, 20810–20824. [Google Scholar] [CrossRef]
- Curioni, A.; Felip, E.; Dafni, U.; Molina, M.A.; Gautschi, O.; Peters, S.; Massuti, B.; Palmero, R.; Ponce, S.; Carcereny, E.; et al. Evolution and clinical impact of EGFR mutations in circulating free DNA in the BELIEF trial. Ann. Oncol. 2018, 29 (Suppl. S8), viii513. [Google Scholar] [CrossRef]
- Dziadziuszko, R.; Hung, T.; Wang, K.; Choeurng, V.; Drilon, A.; Doebele, R.C.; Barlesi, F.; Wu, C.; Dennis, L.; Skoletsky, J.; et al. Pre- and post-treatment blood-based genomic landscape of patients with ROS1 or NTRK fusion-positive solid tumours treated with entrectinib. Mol. Oncol. 2022, 16, 2000–2014. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.-L.; Huang, C.-C.; Ku, W.-H.; Ho, C.-L.; Lin, C.-H.; Yu, S.-L.; Chou, T.-Y. Liquid biopsy for detection of EGFR T790M mutation in nonsmall cell lung cancer: An experience of proficiency testing in Taiwan. J. Chin. Med. Assoc. 2019, 82, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.; Ku, B.M.; Olsen, S.; Park, S.; Lefterova, M.; Odegaard, J.; Jung, H.A.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; et al. Longitudinal monitoring by next-generation sequencing of plasma cell-free DNA in ALK rearranged NSCLC patients treated with ALK tyrosine kinase inhibitors. Cancer Med. 2022, 11, 2944–2956. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Meng, Z.; Wu, Y.; Wang, S.; Jin, G.; Qin, Y.; Wang, F.; Wang, J.; Zhou, H.; Su, X.; et al. Plasma EGFR mutation abundance affects clinical response to first-line EGFR-TKIs in patients with advanced non-small cell lung cancer. Ann. Transl. Med. 2021, 9, 635. [Google Scholar]
- Moiseenko, F.V.; Volkov, N.M.; Zhabina, A.S.; Stepanova, M.L.; Rysev, N.A.; Klimenko, V.V.; Myslik, A.V.; Artemieva, E.V.; Egorenkov, V.V.; Abduloeva, N.H.; et al. Monitoring of the presence of EGFR-mutated DNA during EGFR-targeted therapy may assist in the prediction of treatment outcome. Cancer Treat. Res. Commun. 2022, 31, 100524. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Ren, Y.; Fang, J.; Cao, L.; Liang, Z.; Guo, Q.; Han, S.; Ji, Z.; Wang, Y.; Sun, Y.; et al. CtDNA analysis in the savolitinib phase II study in Non-Small Cell Lung Cancer (NSCLC) patients (pts) harboring MET exon 14 skipping alterations (METex14). Cancer Res. 2021, 81, CT158. [Google Scholar] [CrossRef]
- Ebert, E.B.F.; McCulloch, T.; Hansen, K.H.; Linnet, H.; Sorensen, B.; Meldgaard, P. Clearing of circulating tumour DNA predicts clinical response to first line tyrosine kinase inhibitors in advanced epidermal growth factor receptor mutated non-small cell lung cancer. Lung Cancer 2020, 141, 37–43. [Google Scholar] [CrossRef]
- Ai, X.; Chen, R.; Cui, J.; Lin, W.; Xie, C.; Hu, X.; Zhang, J.; Jiao, X.; Rao, C.; Yang, W.; et al. Clonal dominance of EGFR and efficacy of EGFR-tyrosine kinase inhibitors (EGFR-TKIs) in NSCLC. J. Clin. Oncol. Conf. 2020, 38, e21501. [Google Scholar] [CrossRef]
- Buder, A.; Hochmair, M.J.; Setinek, U.; Filipits, M. Tracking of activating EGFR mutations predicts progression-free survival in advanced EGFR-mutated NSCLC patients treated with osimertinib. Ann. Oncol. 2019, 30 (Suppl. S9), ix167. [Google Scholar] [CrossRef]
- Clement, M.S.; Ebert, E.B.F.; Meldgaard, P.; Sorensen, B.S. Co-occurring MET Amplification Predicts Inferior Clinical Response to First-Line Erlotinib in Advanced Stage EGFR-Mutated NSCLC Patients. Clin. Lung Cancer 2021, 22, e870–e877. [Google Scholar] [CrossRef]
- Ding, P.N.; Becker, T.M.; Bray, V.J.; Chua, W.; Ma, Y.F.; Lynch, D.; Po, J.; Luk, A.W.S.; Caixeiro, N.; de Souza, P.; et al. The predictive and prognostic significance of liquid biopsy in advanced epidermal growth factor receptor-mutated non-small cell lung cancer: A prospective study. Lung Cancer 2019, 134, 187–193. [Google Scholar] [CrossRef]
- Garrido, P.; Paz-Ares, L.; Majem, M.; Moran, T.; Trigo, J.M.; Bosch-Barrera, J.; Garcia-Campelo, R.; Gonzalez-Larriba, J.L.; Sanchez-Torres, J.M.; Isla, D.; et al. LungBEAM: A prospective multicenter study to monitor stage IV NSCLC patients with EGFR mutations using BEAMing technology. Cancer Med. 2021, 10, 5878–5888. [Google Scholar] [CrossRef]
- He, J.; Tan, W.; Tang, X.; Ma, J. Variations in EGFR ctDNA Correlates to the Clinical Efficacy of Afatinib in Non Small Cell Lung Cancer with Acquired Resistance. Pathol. Oncol. Res. 2017, 23, 307–315. [Google Scholar] [CrossRef]
- Kok, P.-S.; Lee, K.; Lord, S.; Yang, J.C.-H.; Rosell, R.; Goto, K.; John, T.; Wu, Y.-L.; Mok, T.S.K.; Lee, C.K. Clinical utility of plasma EGFR mutation detection with quantitative PCR in advanced lung cancer: A meta-analysis. Lung Cancer 2021, 154, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Drilon, A.; Johnson, M.L.; Hsu, M.; Sima, C.S.; McGinn, C.; Sugita, H.; Kris, M.G.; Azzoli, C.G. A prospective study of total plasma cell-free DNA as a predictive biomarker for response to systemic therapy in patients with advanced non-small-cell lung cancers. Ann. Oncol. 2016, 27, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Mack, P.C.; Miao, J.; Redman, M.W.; Moon, J.; Goldberg, S.B.; Herbst, R.S.; Melnick, M.A.; Walther, Z.; Hirsch, F.R.; Politi, K.; et al. Circulating tumor DNA (ctDNA) kinetics predict progression-free and overall survival in EGFR TKI-treated patients with EGFR-mutant NSCLC (SWOG S1403). Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2022, 17, 3752–3760. [Google Scholar] [CrossRef] [PubMed]
- Romero, A.; Molina-Vila, M.A.; Jantus-Lewintre, E.; Insa, A.; Cruz, P.; Collazo, A.; Altozano, J.P.; Juan-Vidal, O.; Diz, P.; Cobo, M.; et al. Comprehensive cross-platform comparison of methodologies for noninvasive EGFR mutation testing: Results of the RING observational trial. J. Clin. Oncology. Conf. 2020, 38, e21518. [Google Scholar] [CrossRef]
- Zulato, E.; Attili, I.; Pavan, A.; Nardo, G.; Del Bianco, P.; Boscolo Bragadin, A.; Verza, M.; Pasqualini, L.; Pasello, G.; Fassan, M.; et al. Early assessment of KRAS mutation in cfDNA correlates with risk of progression and death in advanced non-small-cell lung cancer. Br. J. Cancer 2020, 123, 81–91. [Google Scholar] [CrossRef]
- Lee, J.Y.; Qing, X.; Xiumin, W.; Yali, B.; Chi, S.; Bak, S.H.; Lee, H.Y.; Sun, J.-M.; Lee, S.-H.; Ahn, J.S.; et al. Longitudinal monitoring of EGFR mutations in plasma predicts outcomes of NSCLC patients treated with EGFR TKIs: Korean Lung Cancer Consortium (KLCC-12-02). Oncotarget 2016, 7, 6984–6993. [Google Scholar] [CrossRef] [PubMed]
- Dziadziuszko, R.; Peters, S.; Mok, T.; Camidge, D.R.; Gadgeel, S.M.; Ou, S.-H.I.; Konopa, K.; Noe, J.; Nowicka, M.; Bordogna, W.; et al. Circulating Cell-free DNA as a Prognostic Biomarker in Patients with Advanced ALK+ Non-small Cell Lung Cancer in the Global Phase III ALEX Trial. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2022, 28, 1800–1808. [Google Scholar] [CrossRef]
- Perez-Callejo, D.; Romero, A.; Provencio, M.; Torrente, M. Liquid biopsy based biomarkers in non-small cell lung cancer for diagnosis and treatment monitoring. Transl. Lung Cancer Res. 2016, 5, 455–465. [Google Scholar] [CrossRef]
- Zografos, E.; Dimitrakopoulos, F.I.; Koutras, A. Prognostic Value of Circulating Tumor DNA (ctDNA) in Oncogene-Driven NSCLC: Current Knowledge and Future Perspectives. Cancers 2022, 14, 4954. [Google Scholar] [CrossRef]
- Pender, A.; Hughesman, C.; Law, E.; Kristanti, A.; McNeil, K.; Wong, S.; Tucker, T.; Bosdet, I.; Young, S.; Laskin, J.; et al. EGFR circulating tumour DNA testing: Identification of predictors of ctDNA detection and implications for survival outcomes. Transl. Lung Cancer Res. 2020, 9, 1084–1092. [Google Scholar] [CrossRef]
- Jamal-Hanjani, M.; Wilson, G.A.; McGranahan, N.; Birkbak, N.J.; Watkins, T.B.K.; Veeriah, S.; Shafi, S.; Johnson, D.H.; Mitter, R.; Rosenthal, R.; et al. Tracking the Evolution of Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2109–2121. [Google Scholar] [CrossRef]
- Yu, H.A.; Paz-Ares, L.G.; Yang, J.C.H.; Lee, K.H.; Garrido, P.; Park, K.; Kim, J.H.; Lee, D.H.; Mao, H.; Wijayawardana, S.R.; et al. Phase I Study of the Efficacy and Safety of Ramucirumab in Combination with Osimertinib in Advanced T790M-positive EGFR-mutant Non-small Cell Lung Cancer. Clin. Cancer Res. 2021, 27, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Noronha, V.; Patil, V.M.; Joshi, A.; Menon, N.; Chougule, A.; Mahajan, A.; Janu, A.; Purandare, N.; Kumar, R.; More, S.; et al. Gefitinib Versus Gefitinib Plus Pemetrexed and Carboplatin Chemotherapy in EGFR-Mutated Lung Cancer. J. Clin. Oncol. 2020, 38, 124–136. [Google Scholar] [CrossRef]
- Planchard, D.; Feng, P.H.; Karaseva, N.; Kim, S.W.; Kim, T.M.; Lee, C.K.; Poltoratskiy, A.; Yanagitani, N.; Marshall, R.; Huang, X.; et al. Osimertinib plus platinum—Pemetrexed in newly diagnosed epidermal growth factor receptor mutation-positive advanced/metastatic non-small-cell lung cancer: Safety run-in results from the FLAURA2 study. ESMO Open 2021, 6, 100271. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhao, H.; Shi, Y.; Yang, F.; Wang, L.T.; Kang, G.; Nie, Y.; Wang, J. Perioperative Dynamic Changes in Circulating Tumor DNA in Patients with Lung Cancer (DYNAMIC). Clin. Cancer Res. 2019, 25, 7058–7067. [Google Scholar] [CrossRef] [PubMed]
- Bartels, S.; Persing, S.; Hasemeier, B.; Schipper, E.; Kreipe, H.; Lehmann, U. Molecular Analysis of Circulating Cell-Free DNA from Lung Cancer Patients in Routine Laboratory Practice: A Cross-Platform Comparison of Three Different Molecular Methods for Mutation Detection. J. Mol. Diagn. 2017, 19, 722–732. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Gridelli, C.; Rossi, A. EURTAC first-line phase III randomized study in advanced non-small cell lung cancer: Erlotinib works also in European population. J. Thorac. Dis. 2012, 4, 219–220. [Google Scholar]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.-H.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.-M.; Boyer, M.; et al. Phase III Study of Afatinib or Cisplatin Plus Pemetrexed in Patients with Metastatic Lung Adenocarcinoma with EGFR Mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Sequist, L.V.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Schuler, M.; Mok, T.; et al. EGFR mutation detection in circulating cell-free DNA of lung adenocarcinoma patients: Analysis of LUX-Lung 3 and 6. Br. J. Cancer 2017, 116, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Tan, E.-H.; O’Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.-H.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): A phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016, 17, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, C.; Mack, P.; Scagliotti, G.V.; Aggarwal, C.; Arcila, M.E.; Barlesi, F.; Bivona, T.; Diehn, M.; Dive, C.; Dziadziuszko, R.; et al. Liquid Biopsy for Advanced NSCLC: A Consensus Statement from the International Association for the Study of Lung Cancer. J. Thorac. Oncol. 2021, 16, 1647–1662. [Google Scholar] [CrossRef]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics. 2018, 74, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, L.; Dal Maso, A.; Pavan, A.; Zulato, E.; Calvetti, L.; Pasello, G.; Guarneri, V.; Conte, P.; Indraccolo, S. Liquid biopsy and non-small cell lung cancer: Are we looking at the tip of the iceberg? Br. J. Cancer 2022, 127, 383–393. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | Patients | Molecular Alteration | LB Technique | Mean Age (SD) * | ECOG 0-1 Total (%) | Female’ Total (%) | Never Smoked (%) | Stage 4 Cancer (%) | Adenocarcinoma Histology (%) | NOS Grading |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Category A Studies | |||||||||||
| Curioni 2018 [29] | Switzerland | 91 | EGFR | PCR | 65.4 | 87 (95.6) | 61 (67.0) | 60.3 | - | 97.8 | Good |
| Dziadziuszko 2022 [30] | Poland | 303 | ALK | NGS | 57.8 [44.4] | 258 (85.1) | - | 57.4 | - | - | Good |
| Dziadziuszko 2022 [49] | Poland | 303 | ALK | NGS | 57.8 [44.4] | 258 (85.1) | - | 57.4 | - | - | Good |
| Ebert 2019 [36] | Denmark | 225 | EGFR | PCR | 65.0 | - | - | - | - | - | Good |
| Ho 2022 [31] | Taiwan | 136 | EGFR | PCR | - | 97 (71.3) | 76 (55.9) | 72.8 | 99.3 | 100 | Good |
| Kwon 2021 [32] | Korea | 92 | ALK | PCR | - | - | 62 (67.4) | 68.5 | 100 | 95.7 | Fair |
| Li 2016 [44] | USA | 103 | EGFR | PCR | 57.4 | - | - | N/A | - | - | Poor |
| Liu 2021 [33] | China | 135 | EGFR, KRAS, ALK | NGS | - | 42 (77.8) | 29 (53.7) | 79.6 | - | - | Poor |
| Moiseenko 2022 [34] | Russia | 99 | EGFR | PCR | - | 79 (79.8) | 79 (79.8) | 92.9 | 100 | 100 | Good |
| Yongfeng Yu 2022 [35] | China | 66 | METex14 | NGS | - | 65 (98.5) | 26 (39.4) | 59.1 | 92.4 | N/A | Good |
| Xue Yang 2016 [28] | China | 73 | EGFR | PCR/NGS | 69.4 | - | 44 (60.3) | 72.6 | - | 100 | Poor |
| Category B Studies | |||||||||||
| Ai 2020 [37] | China | 300 | EGFR, ALK | NGS | 59.0 [37.0] | - | - | 57 | 84 | 96.3 | Fair |
| Buder 2019 [38] | Austria | 106 | EGFR T790M | PCR | 60.3 | - | - | - | - | - | Poor |
| Buder 2019 [38] | Austria | 141 | EGFR | PCR | 64.7 [28.1] | - | 80 (56.7) | - | - | - | Poor |
| Clement 2021 [39] | Denmark | 76 | EGFR | PCR | 65.3 [28.1] | - | 47 (61.8) | 36.8 | - | - | Good |
| Curioni 2018 [29] | Switzerland | 91 | EGFR | PCR | 65.4 | 87 (95.6) | 61 (67.0) | 60.3 | - | 97.8 | Good |
| Ding 2019 [40] | Australia | 28 | EGFR | PCR | 67.0 | 22 (78.6) | 16 (57.1) | 75.0 | 100 | 100 | Fair |
| Ebert 2019 [36] | Denmark | 225 | EGFR | PCR | 65.0 | - | - | - | - | - | Good |
| Garrido 2021 [41] | Spain | 110 | EGFR | PCR | 65.5 | 102 (92.7) | 79 (71.8) | 61.8 | - | - | Fair |
| He 2016 * [42] | China | 200 | EGFR | PCR | - | 182 (91) | 54 (27) | 6.0 | 78 | 100 | Poor |
| Kok 2021 [43] | Australia/ China | 86 | EGFR | PCR | - | 86 (100) | 49 (57.0) | 72.1 | 97.7 | 93 | Good |
| Kwon 2021 [32] | Korea | 92 | ALK | PCR | 51.7 [43.0] | - | 62 (67.4) | 68.5 | 100 | 95.7 | Fair |
| Lee 2016 [48] | Korea | 81 | EGFR | PCR | 57.1 [36.3] | - | 50 (61.7) | 63.0 | 84 | 98.8 | Poor |
| Li 2016 [44] | USA | 103 | EGFR | PCR | 57.4 | - | - | - | - | - | Poor |
| Mack 2022 [45] | USA | 106 | EGFR | PCR | 64.3 | 96 (90.6) | 69 (65.1) | - | 100 | 93.4 | Fair |
| Moiseenko 2022 [34] | Russia | 99 | EGFR | PCR | 67.7 | 79 (79.8) | 79 (79.8) | 92.9 | 100 | 100 | Good |
| Romero 2020 [46] | Spain | 22 | EGFR T790M | PCR/NGS | 55.6 | 19 (86.4) | 13 (59.1) | - | 81.8 | 100 | Poor |
| Zulato 2020 [47] | Italy | 58 | KRAS | PCR | 67.3 | 54 (93.1) | 27 (46.6) | 63.8 | - | - | Poor |
| Yongfeng 2021 [35] | China | 66 | METex14 | NGS | 69.4 | 65 (98.5) | 26 (39.4) | 59.1 | 92.4 | - | Good |
| Covariate | Studies | Regression Coefficient (95%-CI) | p-Value |
|---|---|---|---|
| Category A Studies | |||
| Age | 10 | −0.01 (−1.07 to 1.05) | 0.98 |
| Study quality | 10 | 0.75 (0.27 to 1.25) | 0.003 |
| NGS status | 10 | 0.17 (−0.81 to 1.14) | 0.74 |
| EGFR status | 10 | 0.06 (−1.20 to 1.75) | 0.72 |
| Category B studies | |||
| Age | 17 | 0.98 (−1.12 to 3.08) | 0.36 |
| Study quality | 17 | −0.25 (−1.69 to 1.19) | 0.73 |
| NGS status | 17 | −0.81 (−1.70 to 3.32) | 0.53 |
| EGFR status | 17 | −1.26 (−3.29 to 0.77) | 0.22 |
| Study | OS ctDNA Positive (Months) | OS ctDNA Negative (Months) | ORR ctDNA Positive (%) | ORR ctDNA Negative (%) | Sensitivity | Specificity | Resistance Mechanism |
|---|---|---|---|---|---|---|---|
| Category A Studies | |||||||
| Curioni et al., 2018 [29] | 27.0 | 36.6 | - | - | - | - | - |
| Dziadziuszko et al., 2022 [30] | - | - | 86.6 | 88.7 | - | - | - |
| Dziadziuszko et al., 2022 [49] | - | - | 72.3 | 80.3 | - | - | - |
| Ebert et al., 2019 [36] | 25.3 | 42.4 | - | - | - | - | - |
| Ho et al., 2022 [31] | - | - | N/A | 94.5 | - | - | - |
| Kwon et al., 2021 [32] | 39.5 | NR | - | - | - | - | - |
| Moiseenko et al., 2022 [34] | 51.7 | 56.2 | 28.0 | 67.0 | - | - | T790M |
| Yongfeng et al., 2021 [35] | 10.9 | NR | 52.2 | 30.0 | - | - | - |
| Xue Yang et al., 2016 [28] | 35.6 | 23.8 | - | - | - | - | - |
| Category B Studies | |||||||
| Buder et al., 2019 [38] | - | - | - | - | - | - | T790M |
| Buder et al., 2019 [38] | - | - | - | - | - | - | T790M |
| Buder et al., 2019 [38] | 15.3 | NR | - | - | - | - | T790M |
| Clement et al., 2021 [39] | 30.2 | 30.5 | - | - | - | - | - |
| Curioni et al., 2018 [29] | 21.7 | 37.4 | - | - | - | - | - |
| Ding et al., 2019 [40] | 10.4 | NR | - | - | 69.0 | 100 | T790M |
| Ebert et al., 2019 [36] | 7.5 | 36.2 | - | - | - | ||
| Garrido et al., 2021 [41] | - | - | - | - | 70.9 | 98.0 | T790M |
| He et al., 2016 [42] | 27 | 34 | - | - | - | - | T790M |
| Kok et al., 2021 [43] | 15.8 | 30.1 | 5.0 | 32.0 | - | - | - |
| Kwon et al., 2021 [32] | 26.1 | NR | - | - | - | - | - |
| Lee et al., 2016 [48] | 11.2 | 23.7 | - | - | 74.1 | 100 | - |
| Mack et al., 2022 [45] | 15.9 | 32.6 | - | - | - | - | |
| Moiseenko et al., 2022 [34] | 15.4 | NR | 28.0 | 67.0 | - | T790M | |
| Romero et al., 2020 [46] | - | - | - | - | - | - | T790M |
| Zulato et al., 2020 [47] | 8.3 | 22.1 | - | - | - | - | - |
| Yongfeng Yu et al., 2021 [35] | 9.5 | 35.8 | 36.4 | 92.3 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaman, F.Y.; Subramaniam, A.; Afroz, A.; Samoon, Z.; Gough, D.; Arulananda, S.; Alamgeer, M. Circulating Tumour DNA (ctDNA) as a Predictor of Clinical Outcome in Non-Small Cell Lung Cancer Undergoing Targeted Therapies: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 2425. https://doi.org/10.3390/cancers15092425
Zaman FY, Subramaniam A, Afroz A, Samoon Z, Gough D, Arulananda S, Alamgeer M. Circulating Tumour DNA (ctDNA) as a Predictor of Clinical Outcome in Non-Small Cell Lung Cancer Undergoing Targeted Therapies: A Systematic Review and Meta-Analysis. Cancers. 2023; 15(9):2425. https://doi.org/10.3390/cancers15092425
Chicago/Turabian StyleZaman, Farzana Y., Ashwin Subramaniam, Afsana Afroz, Zarka Samoon, Daniel Gough, Surein Arulananda, and Muhammad Alamgeer. 2023. "Circulating Tumour DNA (ctDNA) as a Predictor of Clinical Outcome in Non-Small Cell Lung Cancer Undergoing Targeted Therapies: A Systematic Review and Meta-Analysis" Cancers 15, no. 9: 2425. https://doi.org/10.3390/cancers15092425
APA StyleZaman, F. Y., Subramaniam, A., Afroz, A., Samoon, Z., Gough, D., Arulananda, S., & Alamgeer, M. (2023). Circulating Tumour DNA (ctDNA) as a Predictor of Clinical Outcome in Non-Small Cell Lung Cancer Undergoing Targeted Therapies: A Systematic Review and Meta-Analysis. Cancers, 15(9), 2425. https://doi.org/10.3390/cancers15092425