
Incidence and Risk Factors for Development of Cardiac Toxicity in Adult Patients with Newly Diagnosed Acute Myeloid Leukemia

 , , , , , , , , , , , ,
, , , , , , , , , , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods and Patients
2.1. Study Design and Population
2.2. Study Objectives and Variables
2.3. Definitions
2.4. Statistical Analyses
3. Results
3.1. Patient Disposition and AML Characteristics
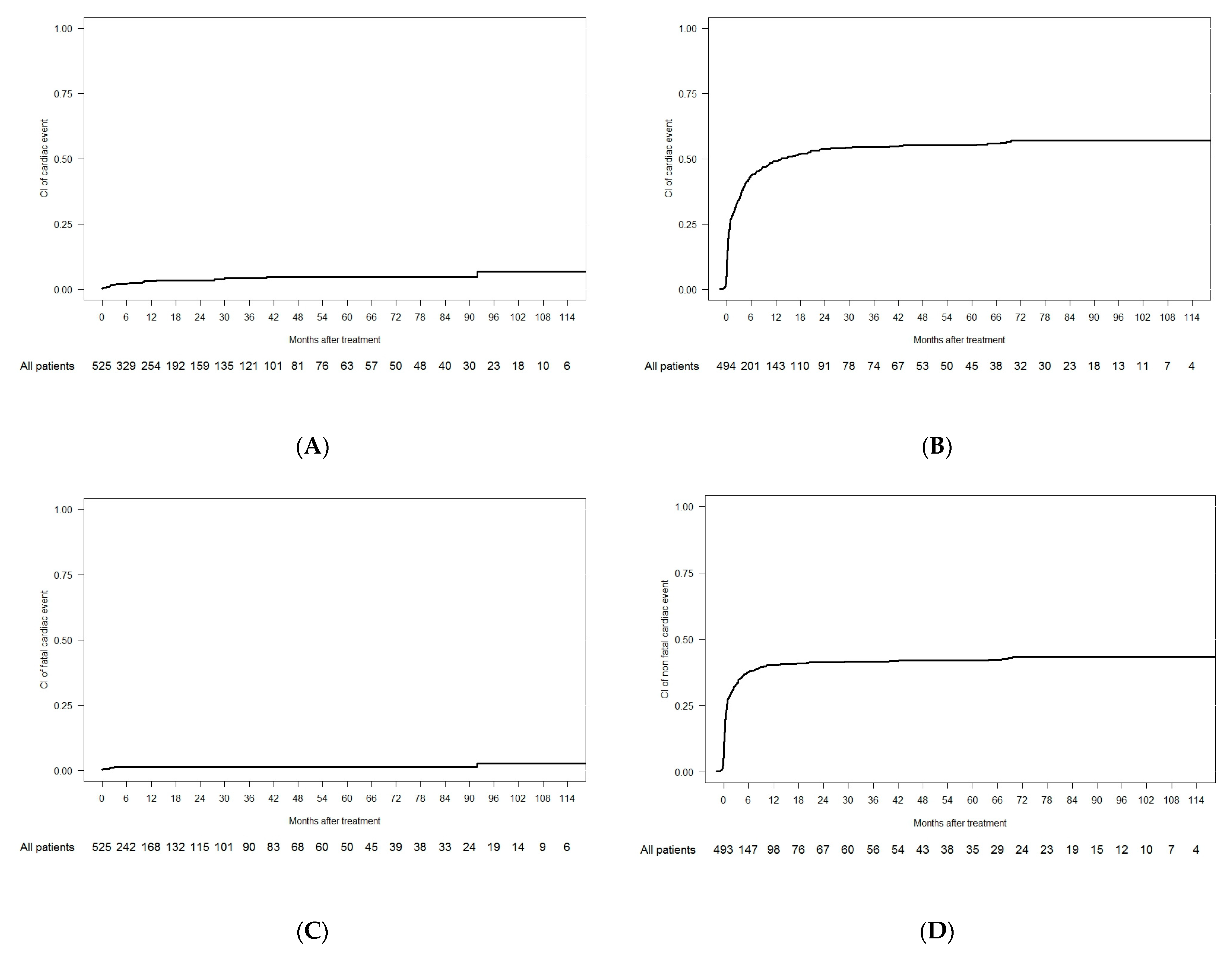
3.2. Fatal Cardiac Events in the Overall Cohort
3.3. Non-Fatal Cardiac Events in the Overall Cohort
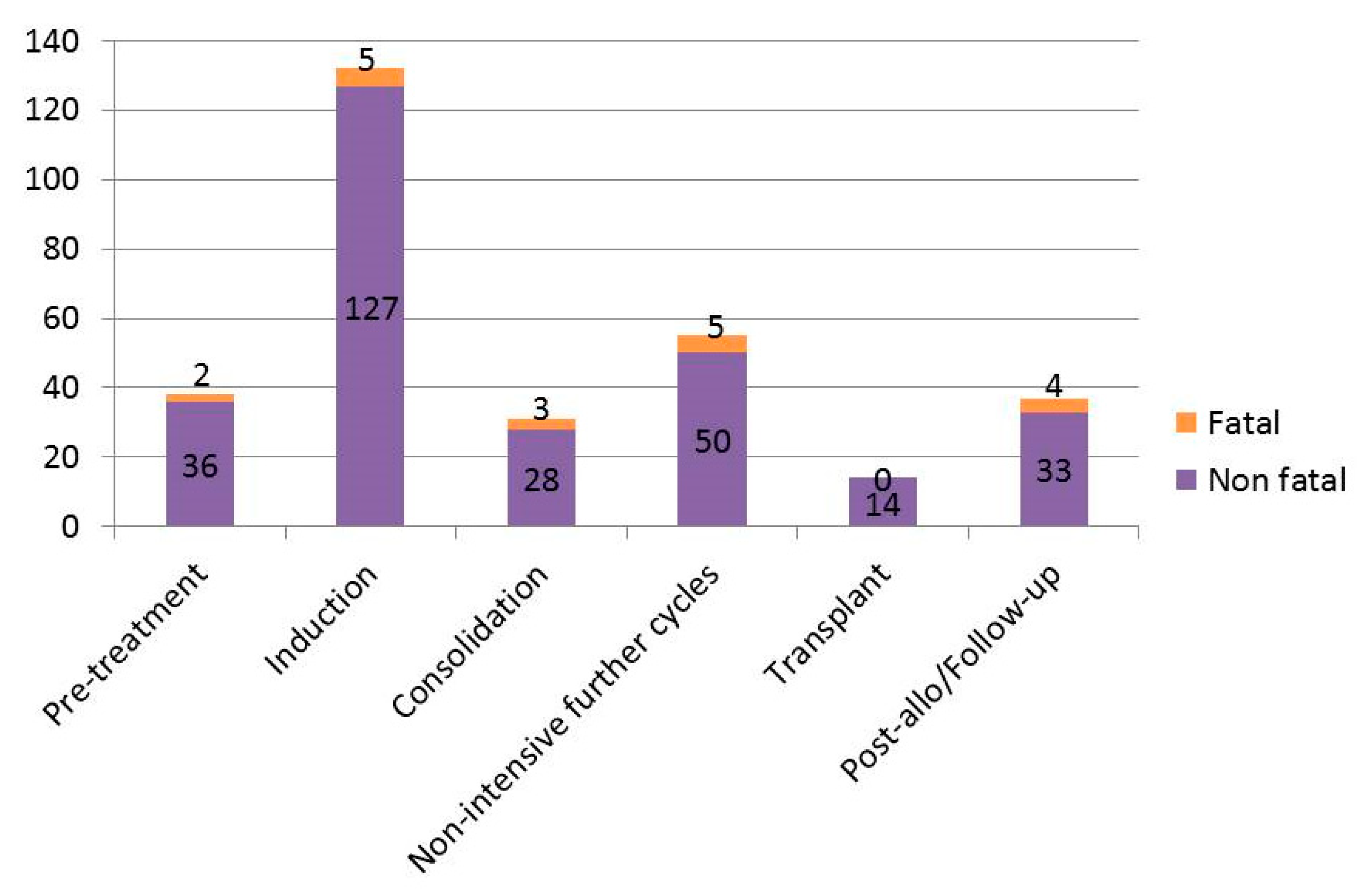
3.4. Timing of Cardiac Events
3.5. Cardiac Events in Intensive Versus Non-Intensive Front-Line Cohorts
3.6. QTc Prolongation Events in the Overall Cohort
3.7. Arrhythmia Events in the Overall Cohort
3.8. Heart Failure and Myocardial Ischemic Events in the Overall Cohort
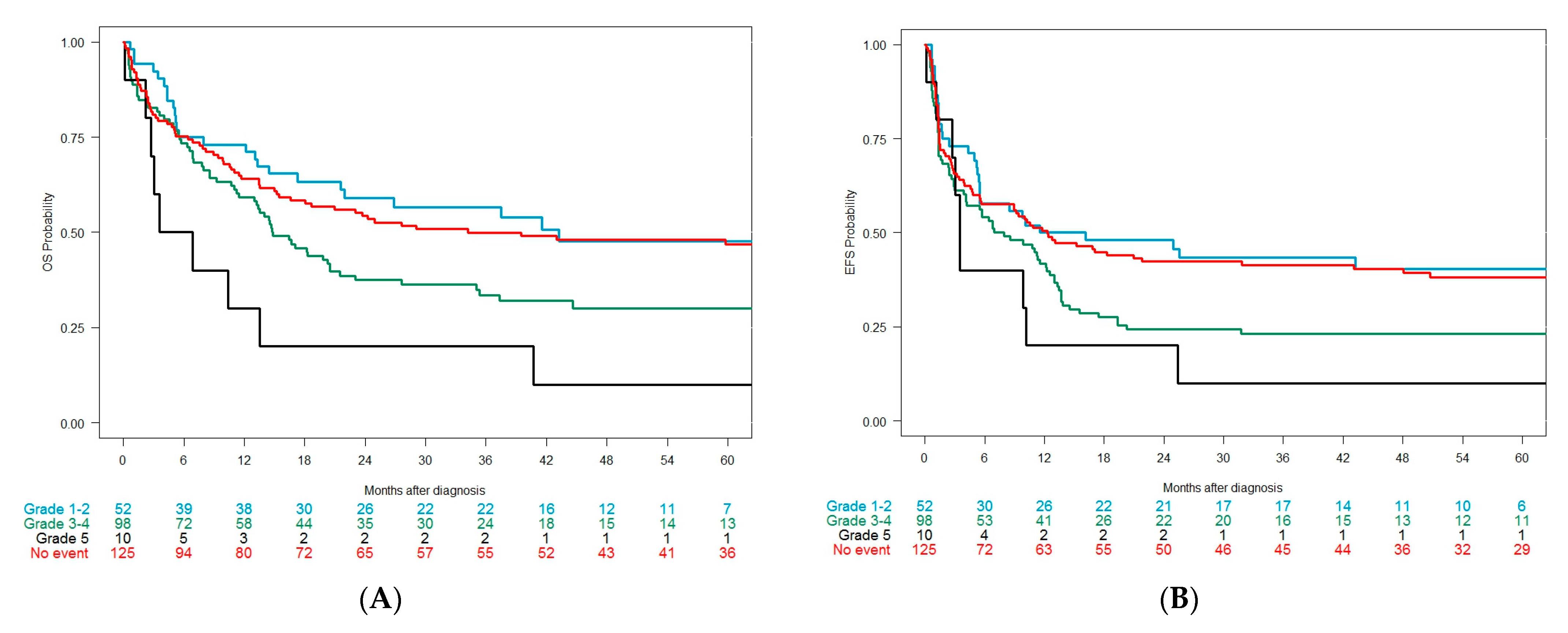
3.9. Clinical Outcomes after Intensive Approaches According to the Development of Cardiac Events
3.10. Cardiac Events in the 1L Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Short, N.J.; Rytting, M.E.; Cortes, J.E. Acute Myeloid Leukaemia. Lancet 2018, 392, 593–606. [Google Scholar] [CrossRef] [PubMed]
- Megías-Vericat, J.E.; Martínez-Cuadrón, D.; Sanz, M.Á.; Montesinos, P. Salvage Regimens Using Conventional Chemotherapy Agents for Relapsed/refractory Adult AML Patients: A Systematic Literature Review. Ann. Hematol. 2018, 97, 1115–1153. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Assuncao, B.L.; Denduluri, S.; McCurdy, S.; Luger, S.; Lefebvre, B.; Carver, J.; Scherrer-Crosbie, M. Symptomatic Heart Failure in Acute Leukemia Patients Treated With Anthracyclines. JACC CardioOncology 2019, 1, 208–217. [Google Scholar] [CrossRef] [PubMed]
- McGowan, J.V.; Chung, R.; Maulik, A.; Piotrowska, I.; Walker, J.M.; Yellon, D.M. Anthracycline Chemotherapy and Cardiotoxicity. Cardiovasc. Drugs Ther. 2017, 31, 63–75. [Google Scholar] [CrossRef]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive Heart Failure in Patients Treated with Doxorubicin: A Retrospective Analysis of Three Trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Auner, H.W.; Tinchon, C.; Linkesch, W.; Tiran, A.; Quehenberger, F.; Link, H.; Sill, H. Prolonged Monitoring of Troponin T for the Detection of Anthracycline Cardiotoxicity in Adults with Hematological Malignancies. Ann. Hematol. 2003, 82, 218–222. [Google Scholar] [CrossRef]
- Anderlini, P.; Benjamin, R.S.; Wong, F.C.; Kantarjian, H.M.; Andreeff, M.; Kornblau, S.M.; O’Brien, S.; Mackay, B.; Ewer, M.S.; Pierce, S.A.; et al. Idarubicin Cardiotoxicity: A Retrospective Study in Acute Myeloid Leukemia and Myelodysplasia. J. Clin. Oncol. 1995, 13, 2827–2834. [Google Scholar] [CrossRef]
- Larrosa-Garcia, M.; Baer, M.R. FLT3 Inhibitors in Acute Myeloid Leukemia: Current Status & Future Directions. Mol. Cancer Ther. 2017, 16, 991–1001. [Google Scholar]
- Coppola, C.; Rienzo, A.; Piscopo, G.; Barbieri, A.; Arra, C.; Maurea, N. Management of QT Prolongation Induced by Anti-Cancer Drugs: Target Therapy and Old Agents. Different Algorithms for Different Drugs. Cancer Treat. Rev. 2018, 63, 135–143. [Google Scholar] [CrossRef]
- Cortes, J.E.; Khaled, S.; Martinelli, G.; Perl, A.E.; Ganguly, S.; Russell, N.; Krämer, A.; Dombret, H.; Hogge, D.; Jonas, B.A.; et al. Quizartinib versus Salvage Chemotherapy in Relapsed or Refractory FLT3-ITD Acute Myeloid Leukaemia (QuANTUM-R): A Multicentre, Randomised, Controlled, Open-Label, Phase 3 Trial. Lancet Oncol. 2019, 20, 984–997. [Google Scholar] [CrossRef]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3 -Mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef] [PubMed]
- Montesinos, P.; Recher, C.; Vives, S.; Zarzycka, E.; Wang, J.; Bertani, G.; Heuser, M.; Calado, R.T.; Schuh, A.C.; Yeh, S.-P.; et al. Ivosidenib and Azacitidine in IDH1 -Mutated Acute Myeloid Leukemia. N. Engl. J. Med. 2022, 386, 1519–1531. [Google Scholar] [CrossRef] [PubMed]
- Giudice, V.; Vecchione, C.; Selleri, C. Cardiotoxicity of Novel Targeted Hematological Therapies. Life 2020, 10, 344. [Google Scholar] [CrossRef] [PubMed]
- Ning, Y.; Shen, Q.; Herrick, K.A.; Mikkelsen, R. Cause of Death in Cancer Survivors. Cancer Res. 103rd Annu. Meet. Am. Assoc. Cancer Res. 2012, 72, LB-339. [Google Scholar]
- Albini, A.; Pennesi, G.; Donatelli, F.; Cammarota, R.; De Flora, S.; Noonan, D.M. Cardiotoxicity of Anticancer Drugs: The Need for Cardio-Oncology and Cardio-Oncological Prevention. J. Natl. Cancer Inst. 2010, 102, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on Cancer Treatments and Cardiovascular Toxicity Developed under the Auspices of the ESC Committee for Practice Guidelines. Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; International Agency for Research on Cancer: Lyon, France, 2008; Volume 4, ISBN 9789283224310. [Google Scholar]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 14 December 2022).
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and Management of AML in Adults: 2017 ELN Recommendations from an International Expert Panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and Management of Acute Myeloid Leukemia in Adults: Recommendations from an International Expert Panel, on Behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Mort, M.K.; Sen, J.M.; Morris, A.L.; DeGregory, K.A.; McLoughlin, E.M.; Mort, J.F.; Dunn, S.P.; Abuannadi, M.; Keng, M.K. Evaluation of Cardiomyopathy in Acute Myeloid Leukemia Patients Treated with Anthracyclines. J. Oncol. Pharm. Pract. 2020, 26, 680–687. [Google Scholar] [CrossRef]
- Getz, K.D.; Sung, L.; Ky, B.; Gerbing, R.B.; Leger, K.J.; Barz Leahy, A.; Sack, L.; Woods, W.G.; Alonzo, T.; Gamis, A.; et al. Occurrence of Treatment-Related Cardiotoxicity and Its Impact on Outcomes among Children Treated in the AAML0531 Clinical Trial: A Report from the Children’s Oncology Group. J. Clin. Oncol. 2019, 37, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Roboz, G.J.; Ritchie, E.K.; Carlin, R.F.; Samuel, M.; Gale, L.; Provenzano-Gober, J.L.; Curcio, T.J.; Feldman, E.J.; Kligfield, P.D. Prevalence, Management, and Clinical Consequences of QT Interval Prolongation during Treatment with Arsenic Trioxide. J. Clin. Oncol. 2014, 32, 3723–3728. [Google Scholar] [CrossRef] [PubMed]
- Erba, H.P.; Montesinos, P.; Vrhovac, R.; Patkowska, E.; Kim, H.-J.; Zak, P.; Wang, P.; Mitov, T.; Hanyok, J.; Liu, L.; et al. Quizartinib Prolonged Survival vs Placebo plus Intensive Induction and Consolidation Therapy Followed by Single-Agent Continuation in Patients Aged 18–75 Years with Newly Diagnosed FLT3-ITD+ AML. Present. EHA Congr. 2022, 6, 1–2. [Google Scholar] [CrossRef]
- Rodríguez-Veiga, R.; Igual, B.; Montesinos, P.; Tormo, M.; Sayas, M.J.; Linares, M.; Fernández, J.M.; Salvador, A.; Maceira-González, A.; Estornell, J.; et al. Assessment of Late Cardiomyopathy by Magnetic Resonance Imaging in Patients with Acute Promyelocytic Leukaemia Treated with All-Trans Retinoic Acid and Idarubicin. Ann. Hematol. 2017, 96, 1077–1084. [Google Scholar] [CrossRef]
- Hegazy, M.; Ghaleb, S.; Das, B.B. Diagnosis and Management of Cancer Treatment-Related Cardiac Dysfunction and Heart Failure in Children. Children 2023, 10, 149. [Google Scholar] [CrossRef]
- Narayan, H.K.; Getz, K.D.; Leger, K.J. Minimizing Car Diac Tox Ic Ity in Chil Dren with Acute Mye Loid Leu Ke Mia. Hematology 2021, 2021, 368–375. [Google Scholar] [CrossRef]
- Mir, A.; Badi, Y.; Bugazia, S.; Nourelden, A.Z.; Fathallah, A.H.; Ragab, K.M.; Alsillak, M.; Elsayed, S.M.; Hagrass, A.I.; Bawek, S.; et al. Efficacy and Safety of Cardioprotective Drugs in Chemotherapy-Induced Cardiotoxicity: An Updated Systematic Review & Network Meta-Analysis. Cardio-Oncology 2023, 9, 1–34. [Google Scholar] [CrossRef]
- Gupta, V.; Kumar Singh, S.; Agrawal, V.; Bali Singh, T. Role of ACE Inhibitors in Anthracycline-Induced Cardiotoxicity: A Randomized, Double-Blind, Placebo-Controlled Trial. Pediatr. Blood Cancer 2018, 65, e27308. [Google Scholar] [CrossRef]
- Lin, T.L.; Newell, L.F.; Stuart, R.K.; Michaelis, L.C.; Rubenstein, E.; Pentikis, H.S.; Callahan, T.; Alvarez, D.; Liboiron, B.D.; Mayer, L.D.; et al. A Phase 2 Study to Assess the Pharmacokinetics and Pharmacodynamics of CPX-351 and Its Effects on Cardiac Repolarization in Patients with Acute Leukemias. Cancer Chemother. Pharmacol. 2019, 84, 163–173. [Google Scholar] [CrossRef]
- Johnson, I.M.; Bezerra, E.D.; Farrukh, F.; McCullough, K.; Al-Kali, A.; Alkhateeb, H.B.; Begna, K.H.; Litzow, M.R.; Hogan, W.J.; Shah, M.V.; et al. Cardiac Events in Patients with Acute Myeloid Leukemia Treated with Venetoclax in Combination with Hypomethylating Agents. Blood 2021, 138, 219. [Google Scholar] [CrossRef]
- Jaiswal, S.; Natarajan, P.; Silver, A.J.; Gibson, C.J.; Bick, A.G.; Shvartz, E.; McConkey, M.; Gupta, N.; Gabriel, S.; Ardissino, D.; et al. Clonal Hematopoiesis and Risk of Atherosclerotic Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.; Metzeler, K.; Kubasch, A.S.; Rommel, K.P.; Desch, S.; Buettner, P.; Rosolowski, M.; Cross, M.; Platzbecker, U.; Thiele, H. Clonal Hematopoiesis and Cardiovascular Disease: Deciphering Interconnections. Basic Res. Cardiol. 2022, 117, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Megias-Vericat, J.E.; Martinez-Cuadron, D.; Herrero, M.J.; Alino, S.F.; Poveda, J.L.; Sanz, M.A.; Montesinos, P. Pharmacogenetics of Metabolic Genes of Anthracyclines in Acute Myeloid Leukemia. Curr. Drug Metab. 2017, 19, 55–74. [Google Scholar] [CrossRef] [PubMed]
- Megías-Vericat, J.E.; Martínez-Cuadrón, D.; Herrero, M.J.; Rodríguez-Veiga, R.; Solana-Altabella, A.; Boluda, B.; Ballesta-López, O.; Cano, I.; Acuña-Cruz, E.; Cervera, J.; et al. Impact of Combinations of Single-Nucleotide Polymorphisms of Anthracycline Transporter Genes upon the Efficacy and Toxicity of Induction Chemotherapy in Acute Myeloid Leukemia. Leuk. Lymphoma 2021, 62, 659–668. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Therapeutic Approach | Schedule | Number of Patients n = 571 (%) |
|---|---|---|
| Intensive chemotherapy | 218 (38) | |
| IDA 1 + Ara-C 2 (3 + 7) | 195 (34) | |
| IDA + Ara-C (2 + 5) | 3 (1) | |
| FLAG-IDA (fludarabine + Ara-C + IDA) | 10 (2) | |
| IDA + Ara-C (3 + 7) + midostaurin | 4 (1) | |
| Allogeneic transplant | 4 (1) | |
| Other intensive chemotherapy | 2 (0.3) | |
| Non-intensive therapy | 75 (13) | |
| Azacitidine | 6 (1) | |
| Decitabine | 1 (0.2) | |
| FLUGA (fludarabine + LD-Ara-C) | 68 (12) | |
| Clinical Trial | 232 (41) | |
| Intensive | 67 (12) | |
| Intensive + FLT3 inhibitor/ placebo | 31 (5) | |
| Intensive without FLT3 inhibitor | 36 (6) | |
| Non-intensive | 165 (29) | |
| Non-intensive + FLT3 inhibitor | 1 (0.2) | |
| Non-intensive without FLT3 inhibitor | 164 (29) | |
| Supportive care only | 46 (8) |
| Characteristic | Overall | Relevant Cardiac Comorbidities | No Cardiac Comorbidities | p | |||
|---|---|---|---|---|---|---|---|
| Median (Range) | n (%) | Median (Range) | n (%) | Median (Range) | n (%) | ||
| N | 571 (100) | 82 (14) | 489 (86) | ||||
| Age, years | 65 (18–98) | 72 (37–98) | 64 (18–92) | <0.001 * | |||
| <65 | 272 (48) | 25 (30) | 247 (51) | 0.001 | |||
| ≥65 | 299 (52) | 57 (70) | 242 (49) | ||||
| Gender | 571 | 82 | 489 | ||||
| Male | 331 (58) | 60 (73) | 271 (55) | 0.004 | |||
| Female | 240 (42) | 22 (27) | 218 (45) | ||||
| ECOG | 1 (0–4) | 571 | 1 (0–4) | 82 | 1 (0–4) | 489 | 0.001 * |
| 0–1 | 432 (76) | 54 (66) | 378 (77) | 0.04 | |||
| ≥2 | 139 (24) | 28 (34) | 111 (23) | ||||
| Comorbidities | 571 | 82 | 489 | ||||
| Yes | 379 (66) | 75 (91) | 304 (62) | <0.001 | |||
| No | 192 (34) | 7 (9) | 185 (38) | ||||
| Type of AML | 571 | 82 | 489 | ||||
| De novo | 350 (61) | 45 (55) | 305 (62) | 0.298 | |||
| Therapy-related | 91 (16) | 13 (16) | 78 (16) | ||||
| Previous MDS/MPN | 130 (23) | 24 (29) | 106 (22) | ||||
| WHO classification | 571 | 82 | 489 | ||||
| AML-RGA | 154 (27) | 20 (24) | 134 (27) | 0.819 | |||
| AML-NOS | 68 (12) | 10 (12) | 58 (12) | ||||
| AML-MRC | 240 (42) | 41 (50) | 199 (41) | ||||
| t-AML | 52 (9) | 5 (6) | 47 (10) | ||||
| Myeloid sarcoma | 2 (0.4) | 0 | 2 (0.4) | ||||
| Ambiguous lineage | 8 (1) | 1 (1) | 7 (1) | ||||
| BPDCN | 2 (0.4) | 0 | 2 (0.4) | ||||
| Not available | 45 (8) | 5 (6) | 40 (8) | ||||
| Extramedullary disease | 569 | 82 | 487 | ||||
| Yes | 100 (18) | 14 (17) | 86 (18) | 0.978 | |||
| No | 469 (82) | 68 (83) | 401 (82) | ||||
| WBC, ×109/L | 8 (0.3–434.3) | 571 | 8.2 (0.3–300.2) | 82 | 8 (0.3–434.3) | 489 | 0.640 * |
| ≤5 | 241 (42) | 35 (43) | 206 (42) | 0.705 | |||
| 5–10 | 68 (12) | 11 (13) | 57 (12) | ||||
| 10–50 | 153 (27) | 24 (29) | 129 (26) | ||||
| > 50 | 109 (19) | 12 (15) | 97 (20) | ||||
| Hemoglobin, g/dL | 8.8 (2.9–15.5) | 571 | 8.4 (5–12.9) | 82 | 8.8 (2.9–15.5) | 489 | 0.078 * |
| ≤10 | 434 (76) | 70 (85) | 364 (74) | 0.044 | |||
| >10 | 137 (24) | 12 (15) | 125 (26) | ||||
| Platelet count, ×109/L | 53 (1–1442) | 570 | 47 (8–816) | 81 | 54 (1–1442) | 489 | 0.275 * |
| ≤20 | 109 (19) | 16 (20) | 93 (19) | 0.997 | |||
| > 20 | 461 (81) | 65 (80) | 396 (81) | ||||
| PB blasts, % | 563 | 82 | 481 | ||||
| ≤50 | 417 (74) | 64 (78) | 353 (73) | 0.451 | |||
| > 50 | 146 (26) | 18 (22) | 128 (27) | ||||
| BM blasts, % | 47 (0–100) | 559 | 43 (14–100) | 81 | 48 (0–100) | 478 | 0.239 * |
| ≤30 | 158 (28) | 28 (35) | 130 (27) | 0.339 | |||
| >30≤70 | 234 (42) | 29 (36) | 205 (43) | ||||
| >70 | 167 (30) | 24 (30) | 143 (30) | ||||
| Creatinine, mg/dL | 0.9 (0.1–7.4) | 570 | 1 (0.2–5.4) | 82 | 0.8 (0.1–7.4) | 488 | <0.001 * |
| ≤1.3 | 482 (85) | 58 (71) | 424 (87) | <0.001 | |||
| > 1.3 | 88 (15) | 24 (29) | 64 (13) | ||||
| Urea, mg/dL | 36 (6–174) | 554 | 45 (18–158) | 81 | 35 (6–174) | 473 | <0.001 * |
| ≤50 | 429 (77) | 46 (57) | 383 (81) | <0.001 | |||
| >50 | 125 (23) | 35 (43) | 90 (19) | ||||
| Uric acid, mg/dL | 5 (1–29) | 489 | 5.8 (1.4–17.1) | 68 | 4.9 (1–29) | 421 | 0.002 * |
| ≤7 | 398 (81) | 48 (71) | 350 (83) | 0.022 | |||
| >7 | 91 (19) | 20 (29) | 71 (17) | ||||
| Bilirubin, mg/dL | 0.6 (0.1–6.2) | 553 | 0.7 (0.1–2.3) | 77 | 0.6 (0.1–6.2) | 472 | 0.313 * |
| ≤1.2 | 484 (88) | 68 (86) | 416 (88) | 0.813 | |||
| >1.2 | 69 (12) | 11 (14) | 58 (12) | ||||
| AST, U/L | 22 (6–1085) | 549 | 22 (7–185) | 77 | 22 (6–1085) | 472 | 0.061 * |
| ≤50 | 482 (88) | 69 (90) | 413 (88) | 0.821 | |||
| >50 | 66 (12) | 8 (10) | 58 (12) | ||||
| ALT, U/L | 18 (3–714) | 566 | 16 (3–125) | 80 | 19 (3–714) | 486 | 0.68 * |
| ≤50 | 504 (89) | 75 (94) | 429 (88) | 0.207 | |||
| >50 | 62 (11) | 5 (6) | 57 (12) | ||||
| Albumin, g/dL | 3.7 (1.6–5.2) | 518 | 3.7 (2.2–4.8) | 69 | 3.7 (1.6–5.2) | 449 | 0.148 * |
| ≤3.5 | 204 (39) | 31 (45) | 173 (39) | 0.379 | |||
| >3.5 | 314 (61) | 38 (55) | 276 (61) | ||||
| LDH, U/L | 521 (101–42630) | 558 | 627 (149–11800) | 509 (101–42630) | 0.984 * | ||
| ≤600 | 307 (55) | 38 (48) | 269 (56) | 0.181 | |||
| >600 | 251 (45) | 42 (53) | 209 (44) | ||||
| Fibrinogen | 487 (34–1150) | 548 | 493 (162–1002) | 79 | 487 (34–1150) | 469 | 0.947 * |
| ≤170 | 6 (1) | 1 (1) | 5 (1) | 0.67 | |||
| >170 | 542 (99) | 78 (99) | 464 (99) | ||||
| Prothrombin time | 501 | 70 | 431 | ||||
| Prolonged | 175 (35) | 33 (47) | 142 (33) | 0.03 | |||
| Normal | 326 (65) | 37 (53) | 289 (67) | ||||
| APTT | 541 | 76 | 465 | ||||
| Prolonged | 73 (13) | 10 (13) | 63 (14) | 0.917 | |||
| Normal | 468 (87) | 66 (87) | 401 (86) | ||||
| Cytogenetics | 571 | 82 | 489 | ||||
| Normal | 211 (37) | 34 (41) | 177 (36) | 0.8 | |||
| Abnormal | 293 (51) | 38 (46) | 255 (52) | ||||
| No metaphases | 47 (8) | 7 (9) | 40 (8) | ||||
| Not available | 20 (4) | 3 (4) | 17 (3) | ||||
| MRC Cytogenetic risk | 517 | 74 | 443 | ||||
| Favorable | 27 (5) | 1 (1) | 26 (6) | 0.185 | |||
| Intermediate | 307 (59) | 49 (66) | 258 (58) | ||||
| Adverse | 183 (35) | 24 (32) | 159 (36) | ||||
| FLT3-ITD | 517 | 77 | 440 | ||||
| Positive | 79 (15) | 9 (12) | 70 (16) | 0.437 | |||
| Negative | 438 (85) | 68 (88) | 370 (84) | ||||
| FLT3-ITD ratio | 517 | 77 | 440 | ||||
| <0.05 | 452 (87) | 70 (91) | 382 (87) | 0.752 | |||
| 0.05–0.5 | 24 (5) | 2 (3) | 22 (5) | ||||
| 0.5–0.8 | 23 (4) | 3 (4) | 20 (5) | ||||
| ≥0.8 | 18 (3) | 2 (3) | 16 (4) | ||||
| FLT3-TKD | 505 | 75 | 430 | ||||
| Positive | 26 (13) | 6 (8) | 20 (5) | 0.217 | |||
| Negative | 479 (93) | 69 (92) | 410 (93) | ||||
| NPM1 | 514 | 77 | 437 | ||||
| Positive | 119 (23) | 18 (23) | 101 (23) | 0.924 | |||
| Negative | 395 (77) | 59 (77) | 336 (77) | ||||
| CEBPA | 571 | 82 | 489 | ||||
| Positive | 14 (2) | 2 (2) | 12 (2) | 0.427 | |||
| Negative | 317 (56) | 47 (57) | 270 (55) | ||||
| Not available | 240 (42) | 33 (40) | 207 (42) | ||||
| IDH | 571 | 82 | 489 | ||||
| IDH1 positive | 23 (4) | 3 (4) | 20 (4) | 0.67 | |||
| IDH2 positive | 54 (9) | 6 (7) | 48 (10) | ||||
| Negative | 266 (47) | 43 (52) | 223 (46) | ||||
| Not available | 228 (40) | 30 (37) | 198 (40) | ||||
| Therapeutic approach | 571 | 82 | 489 | ||||
| Intensive | 218 (38) | 19 (23) | 199 (41) | 0.043 | |||
| HMA | 7 (1) | 2 (2) | 5 (1) | ||||
| LDAC-based | 68 (12) | 11 (13) | 57 (12) | ||||
| Clinical trial, intensive | 67 (12) | 9 (11) | 58 (12) | ||||
| Clinical trial, non-intensive | 165 (29) | 32 (39) | 133 (27) | ||||
| BSC | 46 (8) | 9 (11) | 37 (8) | ||||
| No Cardiac event | p-Value * | Fatal Cardiac Event | Non-Fatal Cardiac Event | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | N (%) | Crude incidence N (%) | Cumulative Incidence | Crude incidence N (%) | Cumulative Incidence | |||||
| At 6 months, % | At Last FU, % | p | At 6 months, % | At Last FU, % | p | |||||
| N | 218 (42) | 19 * (3.6) | 2 | 6.7 | 288 (54.9) | 43.7 | 56.9 | |||
| Age, N | 218 | 19 | 288 | |||||||
| <65 years | 128 (48.5) | 0.005 | 9 (3.4) | 1.6 | 5.9 | 0.25 | 127 (48.1) | 37.8 | 49.9 | <0.001 |
| ≥65 years | 90 (34.5) | 10 (3.8) | 2.5 | 6.8 | 161 (61.7) | 49.7 | 64.4 | |||
| Relevant cardiologic antecedents | 218 | 19 | 288 | |||||||
| No | 202 (44.7) | <0.001 | 10 (2.2) | 1.2 | 4.9 | <0.001 | 240 (53.1) | 41.8 | 54.6 | 0.004 |
| Yes | 16 (21.9) | 9 (12.3) | 7.2 | 20.1 | 48 (65.8) | 56.4 | 73 | |||
| All cardiologic antecedents | 218 | 19 | 288 | |||||||
| No | 163 (49.7) | <0.001 | 6 (1.8) | 0.7 | 4.1 | 0.0004 | 159 (48.5) | 37.6 | 49.7 | <0.001 |
| Yes | 55 (27.9) | 13 (6.6) | 4.4 | 10.7 | 129 (65.5) | 54.2 | 70.6 | |||
| Previous anthracycline treatment | 218 | 19 | 288 | |||||||
| No | 207 (42.1) | 0.51 | 17 (3.5) | 1.7 | 6.5 | 0.22 | 268 (54.5) | 43.3 | 56.3 | 0.49 |
| Yes | 11 (33.3) | 2 (6.1) | 6.7 | 6.7 | 20 (60.6) | 50.5 | 60.7 | |||
| ECOG at diagnosis | 218 | 19 | 288 | |||||||
| <2 | 173 (41.4) | 0.99 | 15 (3.6) | 2 | 6.7 | 0.56 | 230 (55) | 43.3 | 57.2 | 0.63 |
| ≥2 | 45 (42.1) | 4 (3.7) | 1.9 | 5.5 | 58 (54.2) | 45.5 | 56.1 | |||
| FLT3-ITD status | 197 | 19 | 269 | |||||||
| Negative | 161 (39.5) | 0.44 | 17 (4.2) | 2.3 | 7.8 | 0.53 | 230 (56.4) | 44.2 | 58.8 | 0.52 |
| Positive | 36 (46.8) | 2 (2.6) | 1.4 | 3.1 | 39 (50.7) | 43.1 | 51.3 | |||
| Treatment approach | 218 | 19 | 288 | |||||||
| Intensive | 125 (43.9) | 0.5 | 10 (3.5) | 1.9 | 6.3 | 0.37 | 150 (52.6) | 42.5 | 54.7 | 0.17 |
| Non-intensive | 93 (38.8) | 9 (3.8) | 2.2 | 6.8 | 138 (57.5) | 45.2 | 59.6 | |||
| Inclusion in clinical trial | 218 | 19 | 288 | |||||||
| No | 140 (47.8) | 0.004 | 8 (2.7) | 1.1 | 5.4 | 0.06 | 145 (49.5) | 37.4 | 50.8 | <0.001 |
| Yes | 78 (33.6) | 11 (4.7) | 3.2 | 6.5 | 143 (61.6) | 51.8 | 65.2 | |||
| Use of FLT3 inhibitors | 218 | 19 | 288 | |||||||
| No | 204 (41.9) | 0.75 | 18 (3.7) | 2.2 | 4.8 | 0.76 | 265 (54.4) | 42.8 | 56.3 | 0.28 |
| Yes | 14 (36.8) | 1 (2.6) | 0 | 3.1 | 23 (60.5) | 55.3 | 60.7 | |||
| No Cardiac Event | p-Value * | Non-Life-Threatening | Life-Threatening | Fatal | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | N (%) | Crude Incidence N (%) | Cumulative Incidence | Crude Incidence N (%) | Cumulative Incidence | Crude Incidence N (%) | Cumulative Incidence | |||||||
| At 6 months, % | At Last FU, % | p | At 6 months, % | At Last FU, % | p | At 6 months, % | At Last FU, % | p | ||||||
| N | 218 (41.5) | 261 (49.7) | 40 | 53.1 | 27 (5.1) | 4.1 | 6.4 | 19 (3.6) | 2 | 6.7 | ||||
| Age | 218 | 261 | 27 | 19 | ||||||||||
| <65 years | 128 (48.5) | <0.001 | 108 (40.9) | 32.9 | 43.8 | <0.001 | 19 (7.2) | 4.7 | 8.2 | 0.11 | 9 (3.4) | 1.6 | 5.9 | 0.25 |
| ≥65 years | 90 (34.5) | 153 (58.6) | 47.2 | 62.9 | 8 (3.1) | 3.5 | 3.5 | 10 (3.8) | 2.5 | 6.8 | ||||
| Relevant cardiologic antecedents | 218 | 261 | 27 | 19 | ||||||||||
| No | 202 (44.7) | <0.001 | 215 (47.6) | 37.9 | 50.4 | 0.001 | 25 (5.5) | 4.4 | 6.6 | 0.45 | 10 (2.2) | 1.2 | 4.9 | <0.001 |
| Yes | 16 (21.9) | 46 (63) | 53.4 | 71.7 | 2 (2.7) | 1.9 | 4 | 9 (12.3) | 7.2 | 20.1 | ||||
| Previous anthracycline treatment | 218 | 261 | 27 | 19 | ||||||||||
| No | 207 (42.1) | 0.6 | 242 (49.2) | 39.5 | 52.3 | 0.33 | 26 (5.3) | 4.1 | 6.5 | 0.7 | 17 (3.5) | 1.7 | 6.5 | 0.22 |
| Yes | 11 (33.3) | 19 (57.6) | 47.5 | 58.8 | 1 (3) | 4 | 4 | 2 (6.1) | 6.7 | 6.7 | ||||
| ECOG at diagnosis | 218 | 261 | 27 | 19 | ||||||||||
| <2 | 173 (41.4) | 0.99 | 209 (50) | 39.6 | 53.3 | 0.6 | 21 (5) | 3.8 | 6.1 | 0.56 | 15 (3.6) | 2 | 6.7 | 0.56 |
| ≥2 | 45 (42.1) | 52 (48.6) | 41.3 | 52.6 | 6 (5.6) | 5.5 | 7.5 | 4 (3.7) | 1.9 | 5.5 | ||||
| FLT3-ITD status | 197 | 243 | 26 | 19 | ||||||||||
| Negative | 161 (39.5) | 0.55 | 209 (51.2) | 40.3 | 55.3 | 0.34 | 21 (5.2) | 4.2 | 6.1 | 0.63 | 17 (4.2) | 2.3 | 7.8 | 0.53 |
| Positive | 36 (46.8) | 34 (44.2) | 38.2 | 45.5 | 5 (6.5) | 5.6 | 7.3 | 2 (2.6) | 1.4 | 3.1 | ||||
| Treatment chemotherapy | 218 | 261 | 27 | 19 | ||||||||||
| Intensive | 125 (43.9) | 0.07 | 130 (45.6) | 37.6 | 48.8 | 0.025 | 20 (7) | 4.8 | 8.3 | 0.088 | 10 (3.5) | 1.9 | 6.3 | 0.37 |
| Non-intensive | 93 (38.8) | 131 (54.6) | 42.7 | 58.1 | 7 (2.9) | 3.2 | 3.2 | 9 (3.8) | 2.2 | 6.8 | ||||
| Inclusion in clinical trial | 218 | 261 | 27 | 19 | ||||||||||
| No | 140 (47.8) | <0.001 | 125 (42.7) | 32.8 | 45.4 | <0.001 | 20 (6.8) | 5 | 8 | 0.096 | 8 (2.7) | 1.1 | 5.4 | 0.06 |
| Yes | 78 (33.6) | 136 (58.6) | 49.2 | 63.5 | 7 (3) | 2.9 | 3.5 | 11 (4.7) | 3.2 | 6.5 | ||||
| Use of FLT3 inhibitors | 218 | 0.71 | 261 | 27 | 19 | |||||||||
| No | 204 (41.9) | 239 (49.1) | 38.9 | 52.3 | 0.19 | 26 (5.3) | 4.2 | 6.7 | 0.43 | 18 (3.7) | 2.2 | 4.8 | 0.76 | |
| Yes | 14 (36.8) | 22 (57.9) | 53 | 58.8 | 1 (2.6) | 2.7 | 2.7 | 1 (2.6) | 0 | 3.1 | ||||
| All Patients | Cardiac Event | No Cardiac Event | p | |||
|---|---|---|---|---|---|---|
| Grades 1–2 | Grades 3–4 | Grade 5 | ||||
| N (%) | N (%) | N (%) | N (%) | N (%) | ||
| Response, n (%) | 285 (100) | 52 (100) | 98 (100) | 10 (100) | 125 (100) | |
| ORR (CR + CRi) | 193 (67.7) | 39 (75) | 62 (63.3) | 8 (80) | 84 (67.2) | 0.426 |
| CR | 184 (64.6) | 35 (67.3) | 58 (59.2) | 7 (70) | 84 (67.2) | |
| CRi | 9 (3.1) | 4 (7.7) | 4 (4.1) | 1 (10) | 0 (0) | |
| PR | 12 (4.2) | 1 (1.9) | 4 (4.1) | 0 (0) | 7 (5.6) | |
| Resistance | 50 (17.5) | 10 (19.2) | 19 (19.4) | 1 (10) | 20 (16) | |
| Induction death | 30 (10.5) | 2 (3.8) | 13 (13.3) | 1 (10) | 14 (11.2) | |
| OS, n (%) | ||||||
| Median (CI95), months | 21.6 (15.5–37.5) | 43.2 (21.6-NA) | 14.8 (13–21.5) | 5.2 (2.8-NA) | 34.2 (18-NA) | <0.001 |
| 1 year (CI95), % | 63 (57–68) | 73 (62–86) | 59 (50–70) | 30 (12–77) | 64 (56–73) | |
| 2 years (CI95), % | 48 (42–54) | 59 (47–74) | 38 (29–49) | 20 (6–69) | 64 (46–64) | |
| 3 years (CI95), % | 44 (39–50) | 57 (44–72) | 34 (25–45) | 20 (6–69) | 50 (42–60) | |
| 5 years (CI95), % | 39 (34–46) | 48 (35–65) | 30 (22–42) | 10 (2–64) | 47 (39–57) | |
| EFS, n (%) | ||||||
| Median (CI95), months | 10.2 (6.4–13) | 13.9 (5.5-NA) | 7.5 (4.1–12.6) | 3.5 (2.8-NA) | 12.3 (5.7–48) | 0.015 |
| 1 year (CI95), % | 46 (41–52) | 50 (38–66) | 42 (33–53) | 20 (6–69) | 50 (42–60) | |
| 2 years (CI95), % | 36 (31–42) | 48 (36–64) | 24 (17–35) | 20 (6–69) | 42 (35–52) | |
| 3 years (CI95), % | 34 (29–40) | 43 (32–60) | 23 (16–33) | 10 (2–64) | 41 (34–51) | |
| 5 years (CI95), % | 32 (26–38) | 40 (29–57) | 23 (16–33) | 10 (2–64) | 38 (30–48) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boluda, B.; Solana-Altabella, A.; Cano, I.; Martínez-Cuadrón, D.; Acuña-Cruz, E.; Torres-Miñana, L.; Rodríguez-Veiga, R.; Navarro-Vicente, I.; Martínez-Campuzano, D.; García-Ruiz, R.; et al. Incidence and Risk Factors for Development of Cardiac Toxicity in Adult Patients with Newly Diagnosed Acute Myeloid Leukemia. Cancers 2023, 15, 2267. https://doi.org/10.3390/cancers15082267
Boluda B, Solana-Altabella A, Cano I, Martínez-Cuadrón D, Acuña-Cruz E, Torres-Miñana L, Rodríguez-Veiga R, Navarro-Vicente I, Martínez-Campuzano D, García-Ruiz R, et al. Incidence and Risk Factors for Development of Cardiac Toxicity in Adult Patients with Newly Diagnosed Acute Myeloid Leukemia. Cancers. 2023; 15(8):2267. https://doi.org/10.3390/cancers15082267
Chicago/Turabian StyleBoluda, Blanca, Antonio Solana-Altabella, Isabel Cano, David Martínez-Cuadrón, Evelyn Acuña-Cruz, Laura Torres-Miñana, Rebeca Rodríguez-Veiga, Irene Navarro-Vicente, David Martínez-Campuzano, Raquel García-Ruiz, and et al. 2023. "Incidence and Risk Factors for Development of Cardiac Toxicity in Adult Patients with Newly Diagnosed Acute Myeloid Leukemia" Cancers 15, no. 8: 2267. https://doi.org/10.3390/cancers15082267
APA StyleBoluda, B., Solana-Altabella, A., Cano, I., Martínez-Cuadrón, D., Acuña-Cruz, E., Torres-Miñana, L., Rodríguez-Veiga, R., Navarro-Vicente, I., Martínez-Campuzano, D., García-Ruiz, R., Lloret, P., Asensi, P., Osa-Sáez, A., Aguero, J., Rodríguez-Serrano, M., Buendía-Fuentes, F., Megías-Vericat, J. E., Martín-Herreros, B., Barragán, E., ... Montesinos, P. (2023). Incidence and Risk Factors for Development of Cardiac Toxicity in Adult Patients with Newly Diagnosed Acute Myeloid Leukemia. Cancers, 15(8), 2267. https://doi.org/10.3390/cancers15082267