
Surgical Approach to Liver Metastases in GEP-NET in a Tertiary Reference Center

 , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Demographic and Clinical Data
2.2. Statistical Analysis
3. Results
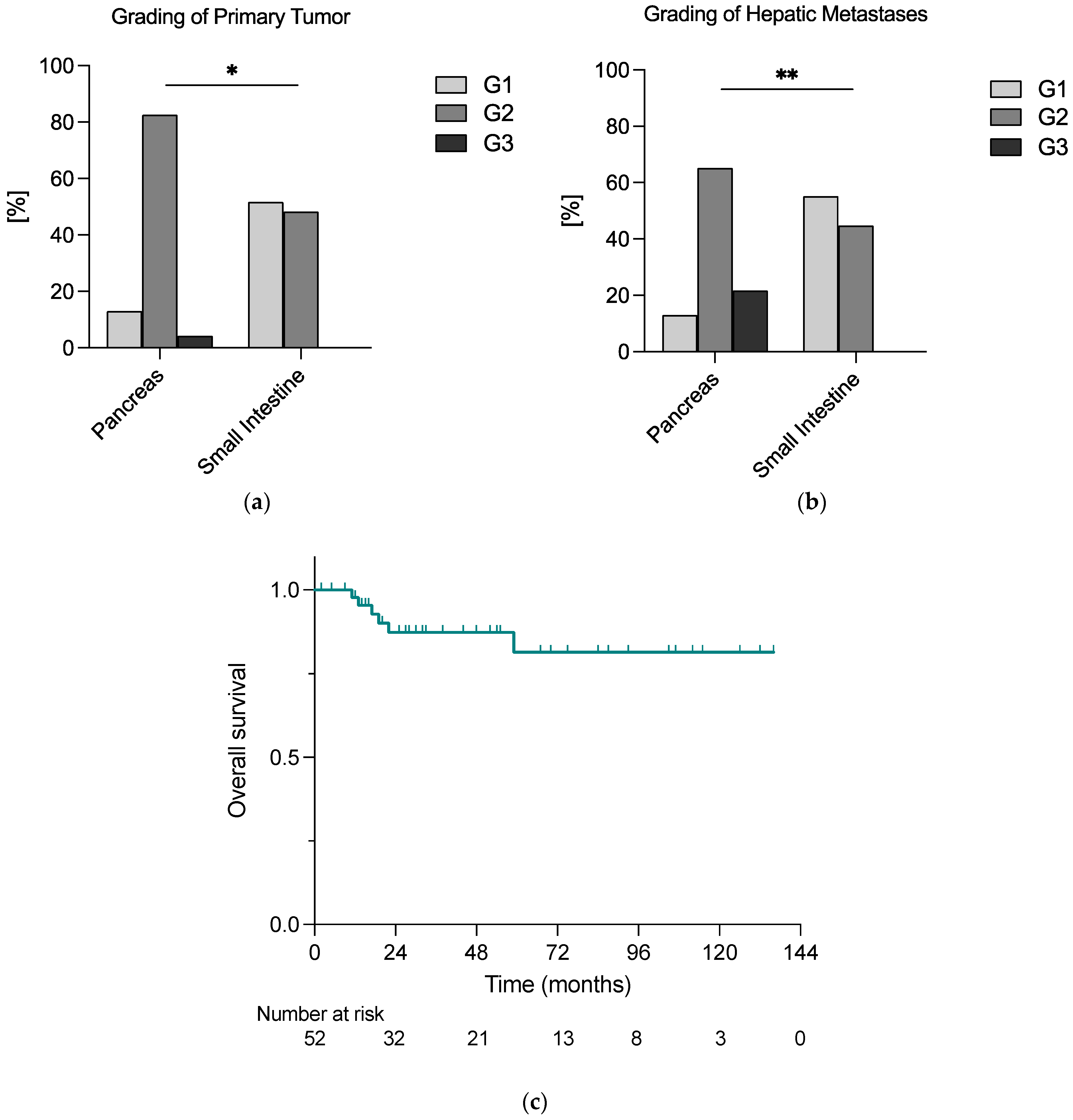
3.1. Patient Characteristics
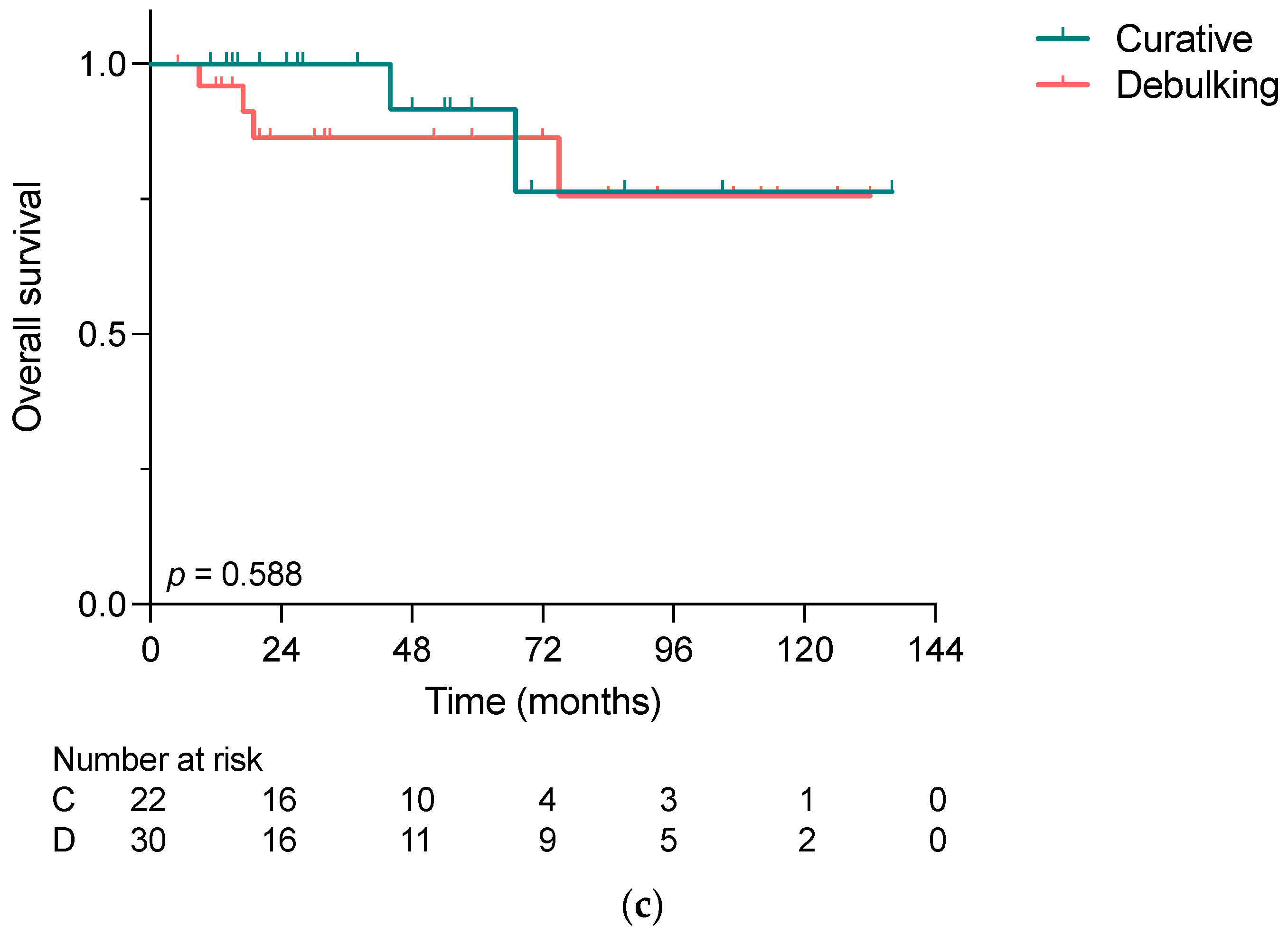
3.2. Outcome according to the Indication for Liver-Directed Surgery in NELM
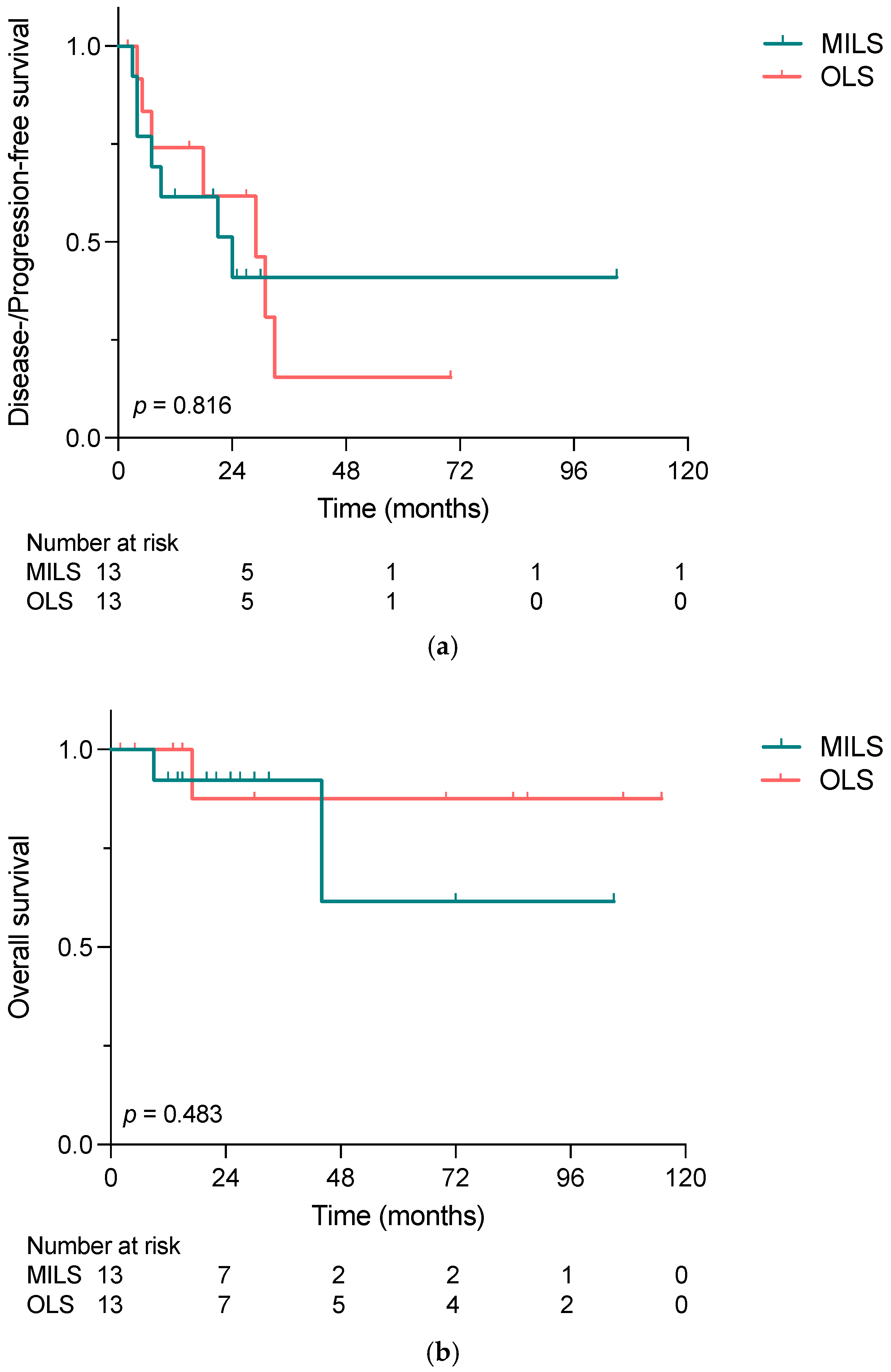
3.3. Comparison of Minimally Invasive and Open Liver Surgery: Propensity Score Matching
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Riihimaki, M.; Hemminki, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. The epidemiology of metastases in neuroendocrine tumors. Int. J. Cancer 2016, 139, 2679–2686. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Bagante, F.; Aldrighetti, L.; Poultsides, G.; Bauer, T.W.; Field, R.C.; Marques, H.P.; Weiss, M.; Maithel, S.K.; Pawlik, T.M. Neuroendocrine Liver Metastasis: Prognostic Implications of Primary Tumor Site on Patients Undergoing Curative Intent Liver Surgery. J. Gastrointest. Surg. 2017, 21, 2039–2047. [Google Scholar] [CrossRef] [PubMed]
- Selberherr, A.; Freermann, S.; Koperek, O.; Niederle, M.B.; Riss, P.; Scheuba, C.; Niederle, B. Neuroendocrine liver metastasis from the small intestine: Is surgery beneficial for survival? Orphanet J. Rare Dis. 2021, 16, 30. [Google Scholar] [CrossRef]
- Beaumont, J.L.; Cella, D.; Phan, A.T.; Choi, S.; Liu, Z.; Yao, J.C. Comparison of health-related quality of life in patients with neuroendocrine tumors with quality of life in the general US population. Pancreas 2012, 41, 461–466. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Frilling, A.; Clift, A.K. Therapeutic strategies for neuroendocrine liver metastases. Cancer 2015, 121, 1172–1186. [Google Scholar] [CrossRef]
- Ejaz, A.; Reames, B.N.; Maithel, S.; Poultsides, G.A.; Bauer, T.W.; Fields, R.C.; Weiss, M.J.; Marques, H.P.; Aldrighetti, L.; Pawlik, T.M. Cytoreductive debulking surgery among patients with neuroendocrine liver metastasis: A multi-institutional analysis. HPB 2018, 20, 277–284. [Google Scholar] [CrossRef]
- Spolverato, G.; Bagante, F.; Wagner, D.; Buettner, S.; Gupta, R.; Kim, Y.; Maqsood, H.; Pawlik, T.M. Quality of life after treatment of neuroendocrine liver metastasis. J. Surg. Res. 2015, 198, 155–164. [Google Scholar] [CrossRef]
- Mayo, S.C.; de Jong, M.C.; Pulitano, C.; Clary, B.M.; Reddy, S.K.; Gamblin, T.C.; Celinksi, S.A.; Kooby, D.A.; Staley, C.A.; Stokes, J.B.; et al. Surgical management of hepatic neuroendocrine tumor metastasis: Results from an international multi-institutional analysis. Ann. Surg. Oncol. 2010, 17, 3129–3136. [Google Scholar] [CrossRef]
- Gangi, A.; Howe, J.R. The Landmark Series: Neuroendocrine Tumor Liver Metastases. Ann. Surg. Oncol. 2020, 27, 3270–3280. [Google Scholar] [CrossRef]
- Schmelzle, M.; Krenzien, F.; Schoning, W.; Pratschke, J. Laparoscopic liver resection: Indications, limitations, and economic aspects. Langenbecks Arch. Surg. 2020, 405, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Lan, X.; Zhang, H.L.; Zhang, H.; Peng, Y.F.; Liu, F.; Li, B.; Wei, Y.G. Four-year experience with more than 1000 cases of total laparoscopic liver resection in a single center. World J. Gastroenterol. 2022, 28, 2968–2980. [Google Scholar] [CrossRef] [PubMed]
- Knitter, S.; Andreou, A.; Kradolfer, D.; Beierle, A.S.; Pesthy, S.; Eichelberg, A.C.; Kastner, A.; Feldbrugge, L.; Krenzien, F.; Schulz, M.; et al. Minimal-Invasive Versus Open Hepatectomy for Colorectal Liver Metastases: Bicentric Analysis of Postoperative Outcomes and Long-Term Survival Using Propensity Score Matching Analysis. J. Clin. Med. 2020, 9, 4027. [Google Scholar] [CrossRef] [PubMed]
- Kandil, E.; Noureldine, S.I.; Koffron, A.; Yao, L.; Saggi, B.; Buell, J.F. Outcomes of laparoscopic and open resection for neuroendocrine liver metastases. Surgery 2012, 152, 1225–1231. [Google Scholar] [CrossRef]
- Strasberg, S.M. Nomenclature of hepatic anatomy and resections: A review of the Brisbane 2000 system. J. Hepatobiliary Pancreat Surg. 2005, 12, 351–355. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibanes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Knigge, U.; Capdevila, J.; Bartsch, D.K.; Baudin, E.; Falkerby, J.; Kianmanesh, R.; Kos-Kudla, B.; Niederle, B.; Nieveen van Dijkum, E.; O’Toole, D.; et al. ENETS Consensus Recommendations for the Standards of Care in Neuroendocrine Neoplasms: Follow-Up and Documentation. Neuroendocrinology 2017, 105, 310–319. [Google Scholar] [CrossRef]
- Bacchetti, S.; Pasqual, E.M.; Bertozzi, S.; Londero, A.P.; Risaliti, A. Curative versus palliative surgical resection of liver metastases in patients with neuroendocrine tumors: A meta-analysis of observational studies. Gland Surg. 2014, 3, 243–251. [Google Scholar] [CrossRef]
- Graff-Baker, A.N.; Sauer, D.A.; Pommier, S.J.; Pommier, R.F. Expanded criteria for carcinoid liver debulking: Maintaining survival and increasing the number of eligible patients. Surgery 2014, 156, 1369–1377. [Google Scholar] [CrossRef]
- Morgan, R.E.; Pommier, S.J.; Pommier, R.F. Expanded criteria for debulking of liver metastasis also apply to pancreatic neuroendocrine tumors. Surgery 2018, 163, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, J.E.; Sherman, S.K.; O’Dorisio, T.M.; Bellizzi, A.M.; Howe, J.R. Liver-directed surgery of neuroendocrine metastases: What is the optimal strategy? Surgery 2016, 159, 320–333. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, R.; Kabir, I.; Hodson, J.; Raza, S.; Shah, T.; Pandanaboyana, S.; Dasari, B.V.M. Impact of the extent of resection of neuroendocrine tumor liver metastases on survival: A systematic review and meta-analysis. Ann. Hepatobiliary Pancreat Surg. 2022, 26, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Poirier, J.; Chivukula, S.; Pappas, S.G.; Hertl, M.; Schadde, E.; Keutgen, X. Primary Tumor Site Affects Survival in Patients with Gastroenteropancreatic and Neuroendocrine Liver Metastases. Int. J. Endocrinol. 2019, 2019, 9871319. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, M.S.; Gonen, M.; Klimstra, D.S. The ENETS/WHO grading system for neuroendocrine neoplasms of the gastroenteropancreatic system: A review of the current state, limitations and proposals for modifications. Int. J. Endocr. Oncol. 2016, 3, 203–219. [Google Scholar] [CrossRef]
- Scarpa, A.; Mantovani, W.; Capelli, P.; Beghelli, S.; Boninsegna, L.; Bettini, R.; Panzuto, F.; Pederzoli, P.; delle Fave, G.; Falconi, M. Pancreatic endocrine tumors: Improved TNM staging and histopathological grading permit a clinically efficient prognostic stratification of patients. Mod. Pathol. 2010, 23, 824–833. [Google Scholar] [CrossRef]
- Keck, K.J.; Choi, A.; Maxwell, J.E.; Li, G.; O’Dorisio, T.M.; Breheny, P.; Bellizzi, A.M.; Howe, J.R. Increased Grade in Neuroendocrine Tumor Metastases Negatively Impacts Survival. Ann. Surg. Oncol. 2017, 24, 2206–2212. [Google Scholar] [CrossRef]
- Van Den Heede, K.; Chidambaram, S.; Van Slycke, S.; Brusselaers, N.; Warfvinge, C.F.; Ohlsson, H.; Nordenstrom, E.; Almquist, M. Effect of primary tumour resection without curative intent in patients with metastatic neuroendocrine tumours of the small intestine and right colon: Meta-analysis. Br. J. Surg. 2022, 109, 191–199. [Google Scholar] [CrossRef]
- Tierney, J.F.; Chivukula, S.V.; Wang, X.; Pappas, S.G.; Schadde, E.; Hertl, M.; Poirier, J.; Keutgen, X.M. Resection of primary tumor may prolong survival in metastatic gastroenteropancreatic neuroendocrine tumors. Surgery 2019, 165, 644–651. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Hyer, J.M.; Paredes, A.Z.; Ejaz, A.; Cloyd, J.M.; Beane, J.D.; Dillhoff, M.; Tsung, A.; Pawlik, T.M. Resection of Primary Gastrointestinal Neuroendocrine Tumor Among Patients with Non-Resected Metastases Is Associated with Improved Survival: A SEER-Medicare Analysis. J. Gastrointest. Surg. 2021, 25, 2368–2376. [Google Scholar] [CrossRef]
- Lewis, A.; Raoof, M.; Ituarte, P.H.G.; Williams, J.; Melstrom, L.; Li, D.; Lee, B.; Singh, G. Resection of the Primary Gastrointestinal Neuroendocrine Tumor Improves Survival with or Without Liver Treatment. Ann. Surg. 2019, 270, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, F.; Rawashdeh, M.; Ahmed, M.; Armstrong, T.; Pearce, N.W.; Abu Hilal, M. Oncological outcomes of laparoscopic surgery of liver metastases: A single-centre experience. Updates Surg. 2015, 67, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Luo, Y.; Qi, W.; Yuan, C.; Xiu, D. Determination of surgical margins in laparoscopic parenchyma-sparing hepatectomy of neuroendocrine tumors liver metastases using indocyanine green fluorescence imaging. Surg. Endosc. 2022, 36, 4408–4416. [Google Scholar] [CrossRef] [PubMed]
- Fretland, A.A.; Dagenborg, V.J.; Bjornelv, G.M.W.; Kazaryan, A.M.; Kristiansen, R.; Fagerland, M.W.; Hausken, J.; Tonnessen, T.I.; Abildgaard, A.; Barkhatov, L.; et al. Laparoscopic Versus Open Resection for Colorectal Liver Metastases: The OSLO-COMET Randomized Controlled Trial. Ann. Surg. 2018, 267, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Mogl, M.T.; Ollinger, R.; Jann, H.; Gebauer, B.; Fehrenbach, U.; Amthauer, H.; Wetz, C.; Schmelzle, M.; Raschzok, N.; Krenzien, F.; et al. Differentiated Strategies for the Therapy of Liver Metastases in Gastro-entero-pancreatic Neuroendocrine Neoplasia. Zentralbl. Chir. 2022, 147, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Okumura, S.; Goumard, C.; Gayet, B.; Fuks, D.; Scatton, O. Laparoscopic versus open two-stage hepatectomy for bilobar colorectal liver metastases: A bi-institutional, propensity score-matched study. Surgery 2019, 166, 959–966. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender 1 | Female Male | 30 (68%) 22 (42%) |
| Age (years) 2 | 60 (21–80) | |
| BMI (kg/m2) 2 | 25 (19–36) | |
| ASA 1 | 2 3 | 32 (62%) 20 (38%) |
| Localization of primary 1 | Pancreas Small intestine | 23 (44%) 29 (56%) |
| Resection of Primary 1 | 51 (98%) | |
| Grading of Primary 1 | G1 G2 G3 | 18 (35%) 33 (63%) 1 (2%) |
| Appearance of metastases 1 | Synchronous Metachronous | 38 (73%) 14 (27%) |
| Indication 1 | Curative Debulking | 22 (42%) 30 (58%) |
| Technique 1 | Open Minimally invasive | 39 (75%) 13 (25%) |
| Duration of surgery (minutes) 2 | 267 (90–575) | |
| Extent of surgery 1 | Major resection Minor resection | 17 (33%) 35 (67%) |
| Simultaneous surgery of primary | 23 (44%) | |
| ICU 1 | 44 (85%) | |
| Length of ICU stay 2 | 1 (0–35) | |
| Length of hospital stay 2 | 11 (6–132) | |
| 90-day complications 1 | 24 (46%) | |
| 90-day major complications 1 | 17 (32%) | |
| 90-day mortality 1 | 0 (0%) | |
| Grading of hepatic metastases 1 | G1 G2 G3 | 19 (36%) 28 (54%) 5 (10%) |
| R status 1 | R0 R1 R2 | 21 (40%) 1 (2%) 30 (58%) |
| Neoadjuvant therapy 1 | 22 (42%) | |
| Adjuvant therapy 1 | 41 (79%) | |
| >1 adjuvant therapy modalities 1 | 26 (50%) | |
| >2 adjuvant therapy modalities 1 | 15 (29%) |
| Curative (n = 22) | Debulking (n = 30) | p | ||
|---|---|---|---|---|
| Gender 1 | Female Male | 16 (73%) 6 (27%) | 14 (47%) 16 (53%) | 0.060 |
| Age (years) 2 | 63 (31–80) | 59 (21–75) | 0.270 | |
| BMI (kg/m2) 2 | 25 (20–33) | 26 (19–36) | 0.977 | |
| ASA 1 | 1 2 3 | 0 (0%) 15 (68%) 7 (32%) | 0 (0%) 16 (53%) 14 (47%) | 0.399 |
| Localization of primary 1 | Pancreas Small intestine | 8 (36%) 14 (64%) | 15 (50%) 15 (50%) | 0.328 |
| Resection of Primary 1 | 22 (100%) | 29 (97%) | 0.387 | |
| Grading of Primary 1 | G1 G2 G3 | 8 (36%) 14 (64%) 0 | 10 (33%) 19 (64%) 1 (3%) | 0.681 |
| Appearance of metastases 1 | Synchronous Metachronous | 15 (68%) 7 (32%) | 23 (77%) 7 (23%) | 0.496 |
| Technique 1 | Open Minimally invasive | 17 (77%) 5 (23%) | 22 (73%) 8 (27%) | 0.746 |
| Duration of surgery (minutes) 2 | 251 (90–575) | 288 (130–499) | 0.476 | |
| Extent of surgery 1 | Major resection Minor resection | 8 (37%) 14 (64%) | 9 (30%) 21 (70%) | 0.483 |
| Simultaneous surgery of primary 1 | 7 (32%) | 16 (53%) | 0.123 | |
| ICU 1 | 18 (82%) | 26 (87%) | 0.632 | |
| Length of ICU stay 2 | 2 (0–8) | 1 (0–35) | 0.503 | |
| Length of hospital stay 2 | 11 (6–42) | 12 (6–132) | 0.558 | |
| 90-day complications 1 | 10 (45%) | 14 (47%) | 0.931 | |
| 90-day major complications 1 | 7 (32%) | 10 (33%) | 0.908 | |
| 90-day mortality 1 | 0 (0%) | 0 (0%) | 1.0 | |
| Grading of hepatic metastases 1 | G1 G2 G3 | 9 (41%%) 10 (45%) 3 (14%) | 10 (33%) 18 (60%) 2 (7%) | 0.512 |
| R status 1 | R0 R1 R2 | 21 (96%) 1 (4%) 0 (0%) | 0 (0%) 0 (0%) 30 (100%) | <0.001 |
| Neoadjuvant therapy 1 | 6 (27%) | 16 (53%) | 0.049 | |
| Adjuvant therapy 1 | 16 (73%) | 25 (83%) | 0.147 | |
| >1 adjuvant therapy modalities 1 | 7 (32%) | 19 (63%) | 0.025 | |
| >2 adjuvant therapy modalities 1 | 4 (18%) | 11 (37%) | 0.146 |
| MILS (n = 13) | OLS (n = 13) | p | ||
|---|---|---|---|---|
| Gender 1 | Female Male | 6 (46%) 7 (54%) | 6 (46%) 7 (54%) | 1.0 |
| Age (years) 2 | 57 (46–73) | 61 (31–76) | 0.960 | |
| BMI (kg/m2) 2 | 25 (20–36) | 24 (19–29) | 0.801 | |
| ASA 1 | 2 3 | 5 (38%) 8 (62%) | 6 (46%) 7 (54%) | 0.691 |
| Localization of primary 1 | Pancreas Small intestine | 6 (46%) 7 (54%) | 5 (38%) 8 (62%) | 0.691 |
| Appearance of metastases 1 | Synchronous Metachronous | 10 (77%) 3 (23%) | 8 (62%) 5 (38%) | 0.395 |
| Indication 1 | Curative Debulking | 5 (38%) 8 (62%) | 5 (38%) 8 (62%) | 1.0 |
| Duration of surgery (minutes) 2 | 285 (130–504) | 245 (209–431) | 0.880 | |
| Extent of surgery 1 | Major resection Minor resection | 3 (23%) 10 (77%) | 5 (38%) 8 (62%) | 0.395 |
| Simultaneous resection of primary 1 | 4 (31%) | 3 (23%) | 0.658 | |
| ICU 1 | 11 (85%) | 12 (92%) | 0.539 | |
| Length of ICU stay 2 | 1 (0–6) | 1 (0–35) | 0.579 | |
| Length of hospital stay 2 | 10 (7–20) | 14 (9–87) | 0.034 | |
| 90-day complications 1 | 6 (46%) | 6 (46%) | 1.0 | |
| 90-day major complications 1 | 5 (38%) | 4 (31%) | 0.680 | |
| 90-day mortality 1 | 0 (0%) | 0 (0%) | 1.0 | |
| Grading Hepatic Metastases 1 | G1 G2 G3 | 4 (31%) 8 (61%) 1 (8%) | 4 (31%) 8 (61%) 1 (8%) | 1.0 |
| R status 1 | R0 R1 R2 | 4 (31%) 1 (8%) 8 (61%) | 5 (38%) 0 (0%) 8 (62%) | 0.574 |
| Resection of Primary 1 | 12 (92%) | 13 (100%) | 0.308 | |
| Grading Primary 1 | G1 G2 G3 | 4 (31%) 8 (61%) 1 (8%) | 4 (31%) 9 (69%) 0 (0%) | 0.589 |
| Neoadjuvant therapy 1 | 3 (23%) | 4 (31%) | 0.658 | |
| Adjuvant therapy 1 | 11 (85%) | 11 (85%) | 1.0 | |
| >1 adjuvant therapy modalities 1 | 6 (46%) | 8 (61%) | 0.431 | |
| >2 adjuvant therapy modalities 1 | 3 (23%) | 4 (31%) | 0.658 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butz, F.; Dukaczewska, A.; Jann, H.; Dobrindt, E.M.; Reinhard, L.; Lurje, G.; Pratschke, J.; Goretzki, P.E.; Schöning, W.; Mogl, M.T. Surgical Approach to Liver Metastases in GEP-NET in a Tertiary Reference Center. Cancers 2023, 15, 2048. https://doi.org/10.3390/cancers15072048
Butz F, Dukaczewska A, Jann H, Dobrindt EM, Reinhard L, Lurje G, Pratschke J, Goretzki PE, Schöning W, Mogl MT. Surgical Approach to Liver Metastases in GEP-NET in a Tertiary Reference Center. Cancers. 2023; 15(7):2048. https://doi.org/10.3390/cancers15072048
Chicago/Turabian StyleButz, Frederike, Agata Dukaczewska, Henning Jann, Eva Maria Dobrindt, Lisa Reinhard, Georg Lurje, Johann Pratschke, Peter E. Goretzki, Wenzel Schöning, and Martina T. Mogl. 2023. "Surgical Approach to Liver Metastases in GEP-NET in a Tertiary Reference Center" Cancers 15, no. 7: 2048. https://doi.org/10.3390/cancers15072048
APA StyleButz, F., Dukaczewska, A., Jann, H., Dobrindt, E. M., Reinhard, L., Lurje, G., Pratschke, J., Goretzki, P. E., Schöning, W., & Mogl, M. T. (2023). Surgical Approach to Liver Metastases in GEP-NET in a Tertiary Reference Center. Cancers, 15(7), 2048. https://doi.org/10.3390/cancers15072048