
Prognostic Value of Inflammatory and Nutritional Biomarkers of Immune Checkpoint Inhibitor Treatment for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient and Data Collection
2.2. Definitions of Inflammatory and Nutritional Biomarkers
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
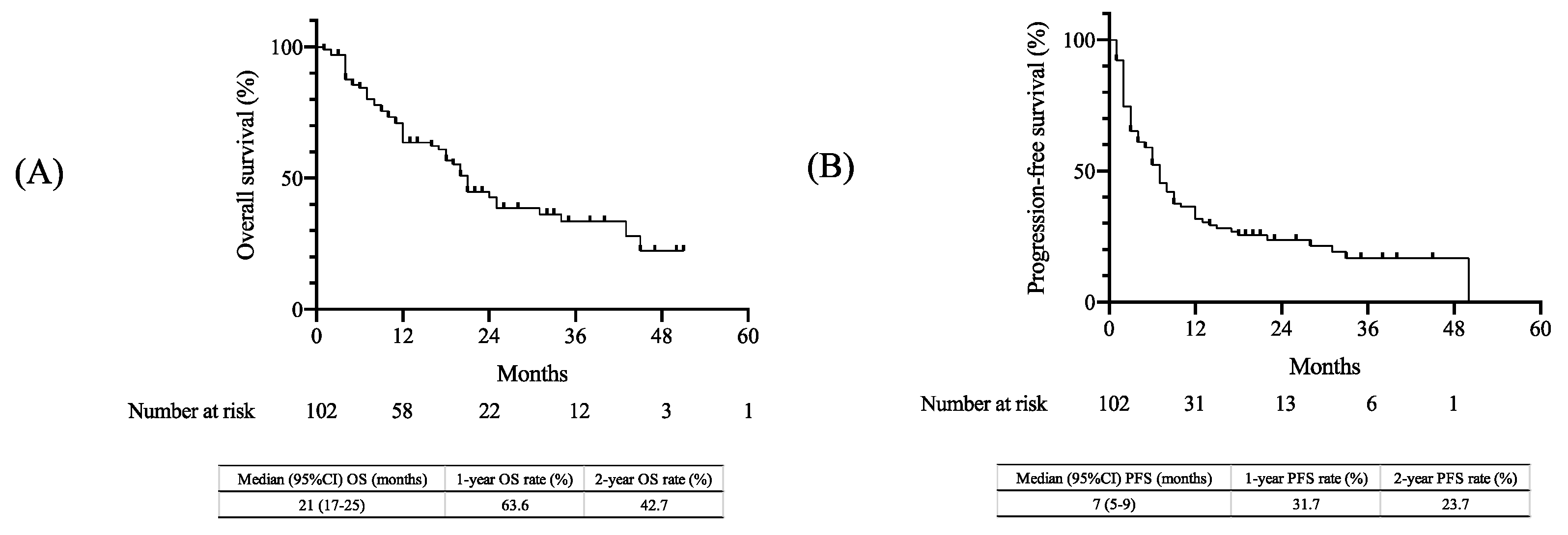
3.2. Treatment Outcomes
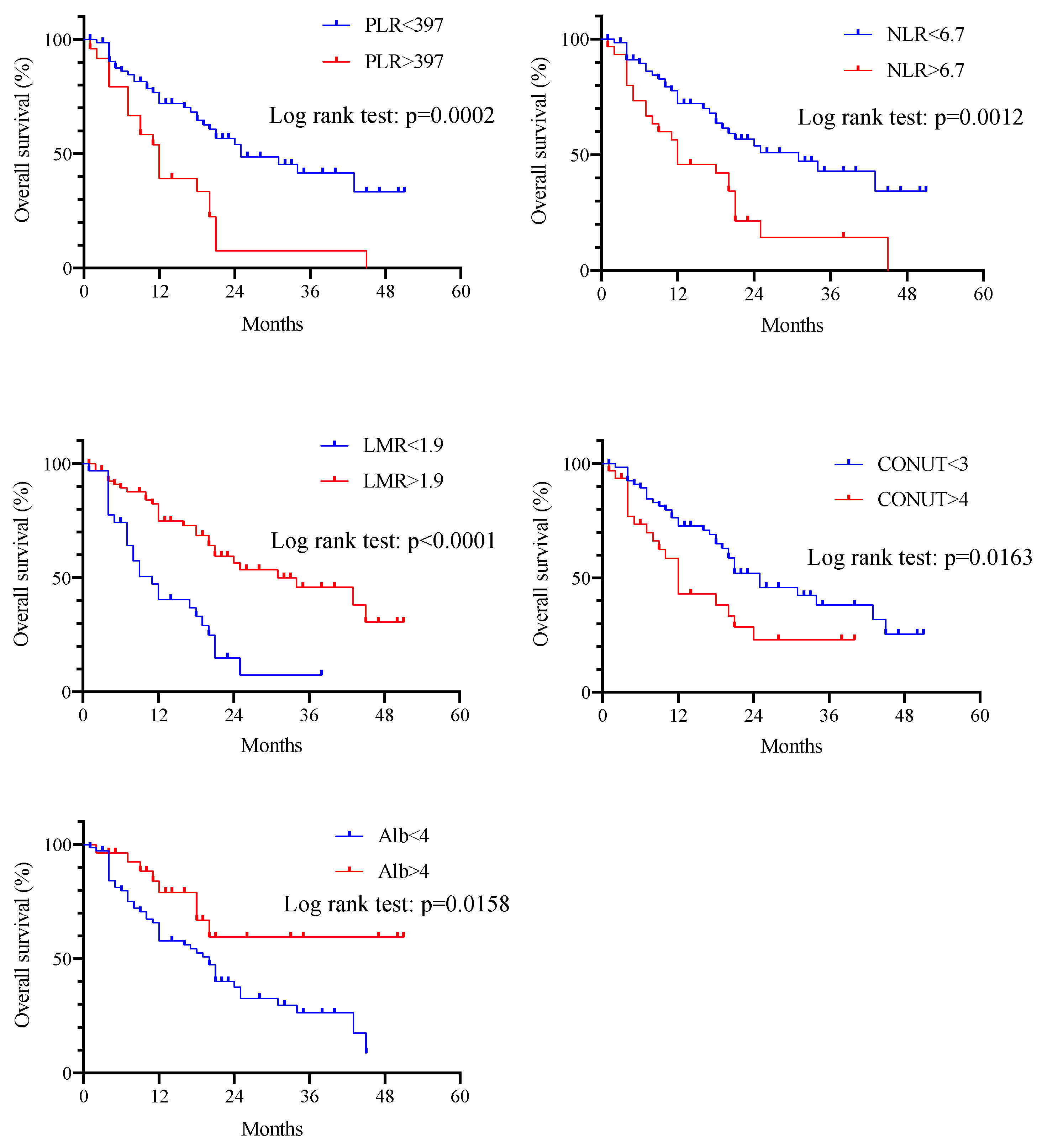
3.3. Analysis of Inflammatory and Nutritional Biomarkers
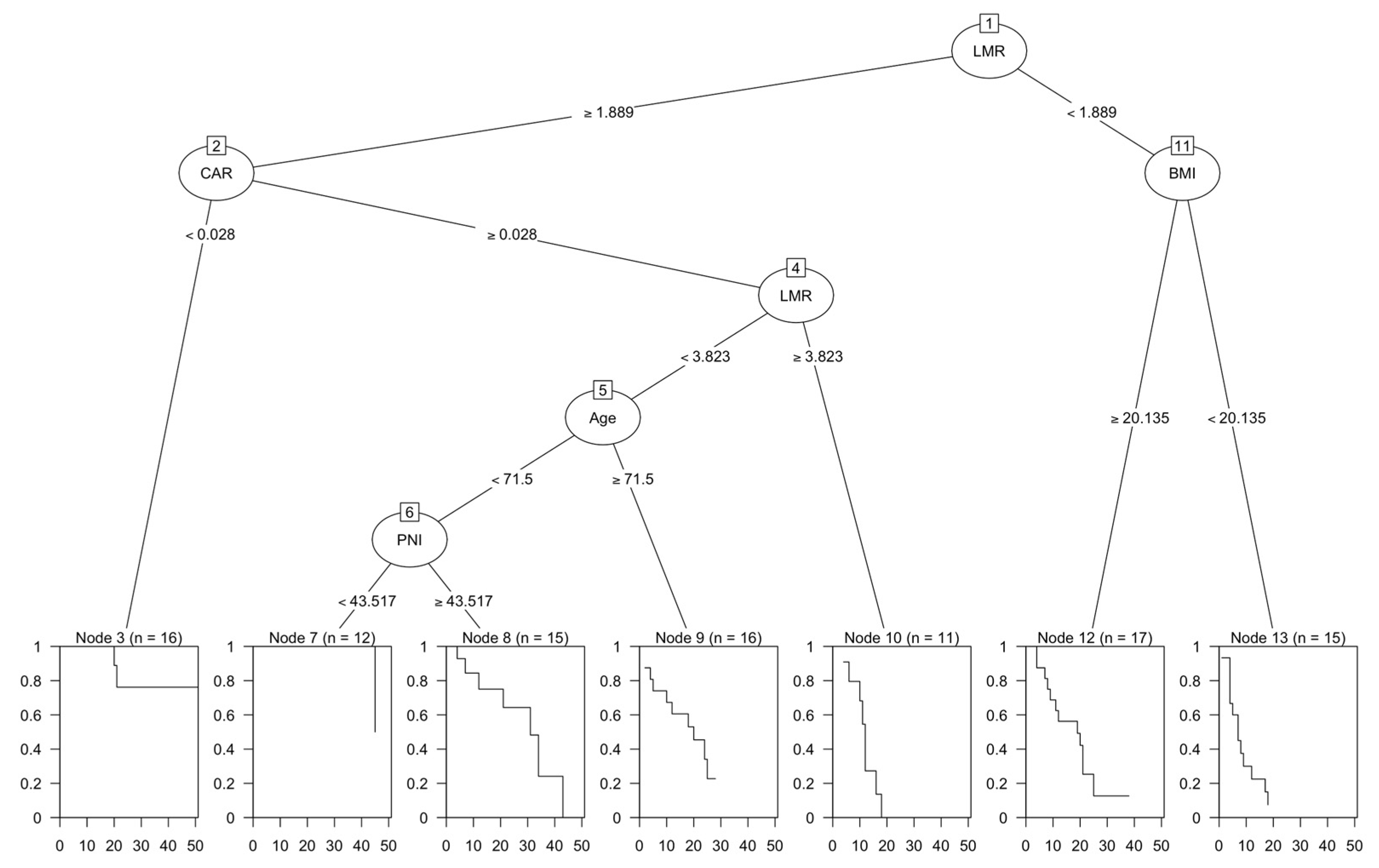
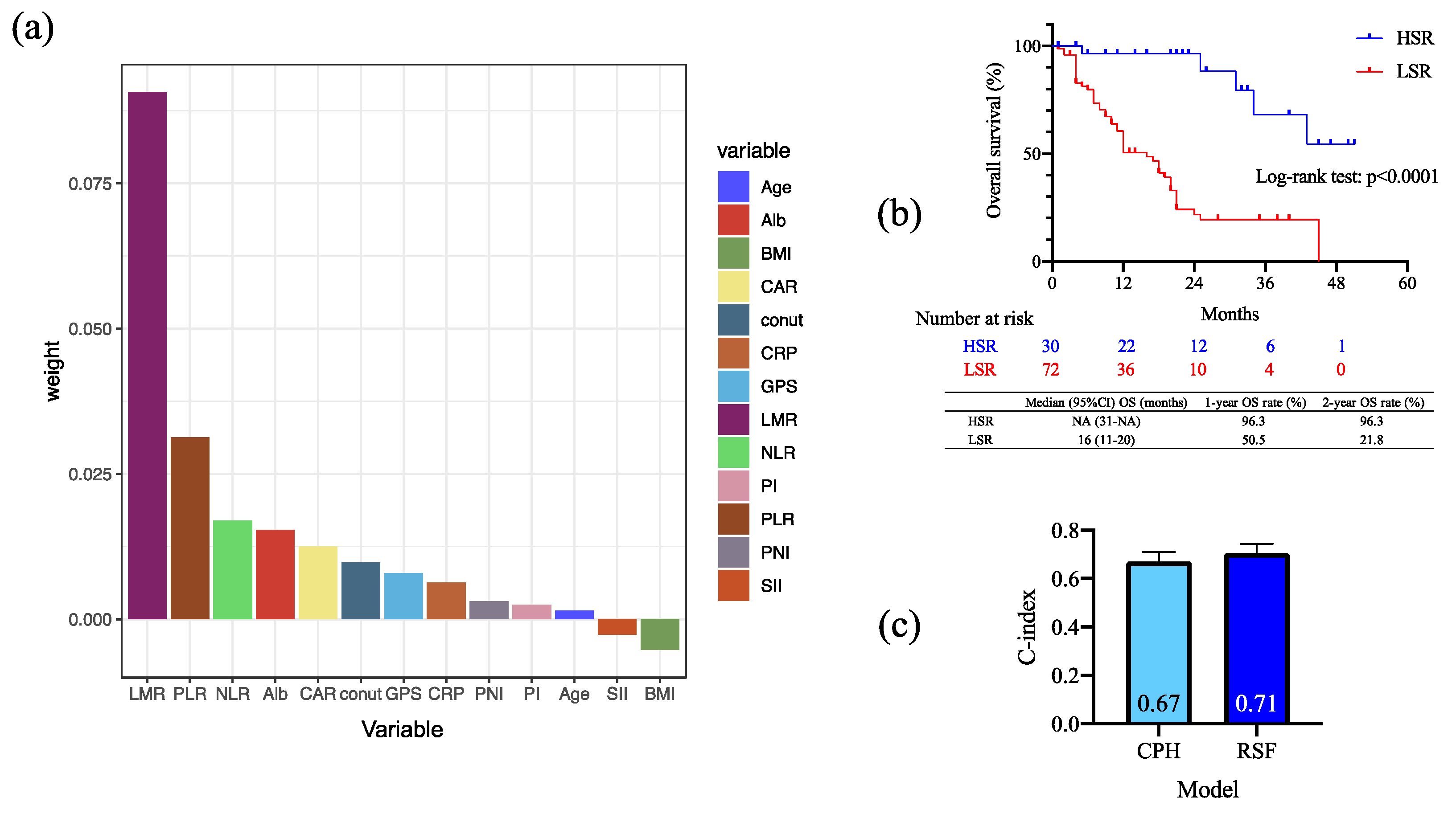
3.4. Importance of Inflammatory and Nutritional Biomarkers Using Machine Learning Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Baste, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomized, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Matsuo, M.; Yasumatsu, R.; Masuda, M.; Toh, S.; Wakasaki, T.; Hashimoto, K.; Taura, M.; Uchi, R.; Nakagawa, T. Relationship between immune-related adverse events and the long-term outcomes in recurrent/metastatic head and neck squamous cell carcinoma treated with nivolumab. Oral Oncol. 2020, 101, 104525. [Google Scholar] [CrossRef]
- Matsuki, T.; Okamoto, I.; Fushimi, C.; Takahashi, H.; Okada, T.; Kondo, T.; Sato, H.; Ito, T.; Tokashiki, K.; Tsukahara, K.; et al. Real-World, Long-Term Outcomes of Nivolumab Therapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck and Impact of the Magnitude of Best Overall Response: A Retrospective Multicenter Study of 88 Patients. Cancers 2020, 12, 3427. [Google Scholar] [CrossRef]
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Gavrielatou, N.; Doumas, S.; Economopoulou, P.; Foukas, P.G.; Psyrri, A. Biomarkers for immunotherapy response in head and neck cancer. Cancer Treat. Rev. 2020, 84, 101977. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Bell, R.B.; Bifulco, C.B.; Burtness, B.; Gillison, M.L.; Harrington, K.J.; Le, Q.T.; Lee, N.Y.; Leidner, R.; Lewis, R.L.; et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of squamous cell carcinoma of the head and neck (HNSCC). J. Immunother. Cancer 2019, 7, 184. [Google Scholar] [CrossRef]
- Patel, S.P.; Kurzrock, R. PD-L1 Expression as a Predictive Biomarker in Cancer Immunotherapy. Mol. Cancer Ther. 2015, 14, 847–856. [Google Scholar] [CrossRef]
- Cristescu, R.; Mogg, R.; Ayers, M.; Albright, A.; Murphy, E.; Yearley, J.; Sher, X.; Liu, X.Q.; Lu, H.; Nebozhyn, M.; et al. Pan-tumor genomic biomarkers for PD-1 checkpoint blockade-based immunotherapy. Science 2018, 362, eaar3593. [Google Scholar] [CrossRef] [PubMed]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; Heath, K.; McClanahan, T.; Lunceford, J.; Gause, C.; et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): An open-label, multicentre, phase 1b trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.J.; Van Waes, C.; Allen, C.T. Overcoming barriers to effective immunotherapy: MDSCs, TAMs, and Tregs as mediators of the immunosuppressive microenvironment in head and neck cancer. Oral Oncol. 2016, 58, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br. J. Cancer 2003, 89, 1028–1030. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Li, C.; Lin, X.; Lin, S.; Chen, W.; Chen, X.; Huang, X.; Wang, D. Prognostic Value of Controlling Nutritional Status Score in Advanced Hypopharyngeal Cancer. Laryngoscope 2023, 1–8. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Luo, Z.; Zhou, L.; Balde, A.I.; Li, Z.; He, L.; ZhenWei, C.; Zou, Z.; Huang, S.; Han, S.; Wei Zhou, M.; et al. Prognostic impact of preoperative prognostic nutritional index in resected advanced gastric cancer: A multicenter propensity score analysis. Eur. J. Surg. Oncol. 2019, 45, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, R.; Sakamoto, Y.; Nakagawa, S.; Ohuchi, M.; Izumi, D.; Kosumi, K.; Taki, K.; Higashi, T.; Miyamoto, Y.; Yoshida, N.; et al. CONUT: A novel independent predictive score for colorectal cancer patients undergoing potentially curative resection. Int. J. Color. Dis. 2017, 32, 99–106. [Google Scholar] [CrossRef]
- Mariani, P.; Russo, D.; Maisto, M.; Troiano, G.; Caponio, V.C.A.; Annunziata, M.; Laino, L. Pretreatment neutrophil-to-lymphocyte ratio is an independent prognostic factor in head and neck squamous cell carcinoma: Meta-analysis and trial sequential analysis. J. Oral. Pathol. Med. 2022, 51, 39–51. [Google Scholar] [CrossRef]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Fruh, M. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer 2017, 111, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; He, A.; Liu, A.; Tong, W.; Cao, D. Evaluation of the prognostic role of platelet-lymphocyte ratio in cancer patients treated with immune checkpoint inhibitors: A systematic review and meta-analysis. Int. Immunopharmacol. 2019, 77, 105957. [Google Scholar] [CrossRef]
- Kano, S.; Homma, A.; Hatakeyama, H.; Mizumachi, T.; Sakashita, T.; Kakizaki, T.; Fukuda, S. Pretreatment lymphocyte-to-monocyte ratio as an independent prognostic factor for head and neck cancer. Head Neck 2017, 39, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Wang, Y.T.; Kuo, L.T.; Weng, H.H.; Hsu, C.M.; Tsai, M.S.; Chang, G.H.; Lee, Y.C.; Huang, E.I.; Tsai, Y.T. Systemic Immun e-Inflammation Index as a Predictor for Head and Neck Cancer Prognosis: A Meta-Analysis. Front. Oncol. 2022, 12, 899518. [Google Scholar] [CrossRef] [PubMed]
- Tanoue, K.; Tamura, S.; Kusaba, H.; Shinohara, Y.; Ito, M.; Tsuchihashi, K.; Shirakawa, T.; Otsuka, T.; Ohmura, H.; Isobe, T.; et al. Predictive impact of C-reactive protein to albumin ratio for recurrent or metastatic head and neck squamous cell carcinoma receiving nivolumab. Sci. Rep. 2021, 11, 2741. [Google Scholar] [CrossRef] [PubMed]
- Ikoma, T.; Shimokawa, M.; Matsumoto, T.; Boku, S.; Yasuda, T.; Shibata, N.; Kurioka, Y.; Takatani, M.; Nobuhisa, T.; Namikawa, T.; et al. Inflammatory prognostic factors in advanced or recurrent esophageal squamous cell carcinoma treated with nivolumab. Cancer Immunol. Immunother. 2022, 72, 427–435. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Migita, K.; Matsumoto, S.; Wakatsuki, K.; Ito, M.; Kunishige, T.; Nakade, H.; Kitano, M.; Nakatani, M.; Sho, M. The prognostic significance of inflammation-based markers in patients with recurrent gastric cancer. Surg. Today 2018, 48, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Xiu, Y.; Zhang, S.; Yu, X.; Qiao, K.; Huang, Y. A Novel Inflammatory and Nutritional Prognostic Scoring System for Nonpathological Complete Response Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy. Dis. Markers 2022, 2022, 8044550. [Google Scholar] [CrossRef]
- Kasymjanova, G.; MacDonald, N.; Agulnik, J.S.; Cohen, V.; Pepe, C.; Kreisman, H.; Sharma, R.; Small, D. The predictive value of pretreatment inflammatory markers in advanced non-small-cell lung cancer. Curr. Oncol. 2010, 17, 52–58. [Google Scholar] [CrossRef]
- Matsuo, M.; Yasumatsu, R.; Masuda, M.; Toh, S.; Wakasaki, T.; Hashimoto, K.; Jiromaru, R.; Manako, T.; Nakagawa, T. Inflammation-based Prognostic Score as a Prognostic Biomarker in Patients With Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma Treated With Nivolumab Therapy. Vivo 2022, 36, 907–917. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M.; Statistics Subcommittee of the NCI-EORTC Working Group on Cancer Diagnostics. REporting recommendations for tumour MARKer prognostic studies (REMARK). Br. J. Cancer 2005, 93, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Ishwaran, H.; Kogalur, U.B.; Blackstone, E.H.; Lauer, M.S. Random survival forests. Ann. Appl. Stat. 2008, 2, 841–860. [Google Scholar] [CrossRef]
- Harrington, K.J.; Burtness, B.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Brana, I.; Baste, N.; Neupane, P.; et al. Pembrolizumab With or Without Chemotherapy in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: Updated Results of the Phase III KEYNOTE-048 Study. J. Clin. Oncol. 2023, 41, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral. Oncol. 2018, 81, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Politz, S.; Wagner, M.; Schwub, D.; Cattenberg, S.; Thurnheer, R.; Schelosky, L. Enhancing Visibility of the Hypopharyngeal-Esophageal Region by Introduction of a Physiological Eructation Maneuver. Biomed. Hub 2019, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yasumatsu, R.; Shimizu, Y.; Hanai, N.; Kariya, S.; Yokota, T.; Fujii, T.; Tsukahara, K.; Ando, M.; Hanyu, K.; Ueda, T.; et al. Outcomes of long-term nivolumab and subsequent chemotherapy in Japanese patients with head and neck cancer: 2-year follow-up from a multicenter real-world study. Int. J. Clin. Oncol. 2022, 27, 95–104. [Google Scholar] [CrossRef]
- Otsuki, S.; Hori, R.; Shinohara, S.; Kojima, T.; Tamaki, H.; Asato, R.; Kitamura, M.; Ichimaru, K.; Kitani, Y.; Kumabe, Y.; et al. Real-world 2-year long-term outcomes and prognostic factors in patients receiving nivolumab therapy for recurrent or metastatic squamous cell carcinoma of the head and neck. Auris Nasus Larynx 2022, 49, 834–844. [Google Scholar] [CrossRef]
- Takahashi, S.; Oridate, N.; Tanaka, K.; Shimizu, Y.; Fujimoto, Y.; Matsumoto, K.; Yokota, T.; Yamazaki, T.; Takahashi, M.; Ueda, T.; et al. First-line pembrolizumab +/− chemotherapy for recurrent/metastatic head and neck cancer: Japanese subgroup of KEYNOTE-048. Int. J. Clin. Oncol. 2022, 27, 1805–1817. [Google Scholar] [CrossRef]
- Chalker, C.; Voutsinas, J.M.; Wu, Q.V.; Santana-Davila, R.; Hwang, V.; Baik, C.S.; Lee, S.; Barber, B.; Futran, N.D.; Houlton, J.J.; et al. Performance status (PS) as a predictor of poor response to immune checkpoint inhibitors (ICI) in recurrent/metastatic head and neck cancer (RMHNSCC) patients. Cancer Med. 2022, 11, 4104–4111. [Google Scholar] [CrossRef] [PubMed]
- Dall’Olio, F.G.; Maggio, I.; Massucci, M.; Mollica, V.; Fragomeno, B.; Ardizzoni, A. ECOG performance status >/=2 as a prognostic factor in patients with advanced non small cell lung cancer treated with immune checkpoint inhibitors-A systematic review and meta-analysis of real world data. Lung Cancer 2020, 145, 95–104. [Google Scholar] [CrossRef]
- Khaki, A.R.; Li, A.; Diamantopoulos, L.N.; Bilen, M.A.; Santos, V.; Esther, J.; Morales-Barrera, R.; Devitt, M.; Nelson, A.; Hoimes, C.J.; et al. Impact of performance status on treatment outcomes: A real-world study of advanced urothelial cancer treated with immune checkpoint inhibitors. Cancer 2020, 126, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, K.; Gill, R.R.; Widick, P.; Bindal, P.; McDonald, D.C.; Shea, M.; Rangachari, D.; Costa, D.B. Association of Performance Status With Survival in Patients With Advanced Non-Small Cell Lung Cancer Treated With Pembrolizumab Monotherapy. JAMA Netw. Open 2021, 4, e2037120. [Google Scholar] [CrossRef]
- Ying, H.Q.; Deng, Q.W.; He, B.S.; Pan, Y.Q.; Wang, F.; Sun, H.L.; Chen, J.; Liu, X.; Wang, S.K. The prognostic value of preoperative NLR, d-NLR, PLR and LMR for predicting clinical outcome in surgical colorectal cancer patients. Med. Oncol. 2014, 31, 305. [Google Scholar] [CrossRef]
- Yasumatsu, R.; Wakasaki, T.; Hashimoto, K.; Nakashima, K.; Manako, T.; Taura, M.; Matsuo, M.; Nakagawa, T. Monitoring the neutrophil-to-lymphocyte ratio may be useful for predicting the anticancer effect of nivolumab in recurrent or metastatic head and neck cancer. Head Neck 2019, 41, 2610–2618. [Google Scholar] [CrossRef] [PubMed]
- Olingy, C.E.; Dinh, H.Q.; Hedrick, C.C. Monocyte heterogeneity and functions in cancer. J. Leukoc. Biol. 2019, 106, 309–322. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.A. Progress in human tumour immunology and immunotherapy. Nature 2001, 411, 380–384. [Google Scholar] [CrossRef]
- Aoyama, J.; Kuwahara, T.; Sano, D.; Fujisawa, T.; Tokuhisa, M.; Shimizu, M.; Sakagami, T.; Ichikawa, Y.; Iwai, H.; Oridate, N. Combination of Performance Status and Lymphocyte-monocyte Ratio as a Novel Prognostic Marker for Patients With Recurrent/Metastatic Squamous Cell Carcinoma of the Head and Neck. Cancer Diagn. Progn. 2021, 1, 353–361. [Google Scholar] [CrossRef]
- Tham, T.; Olson, C.; Khaymovich, J.; Herman, S.W.; Costantino, P.D. The lymphocyte-to-monocyte ratio as a prognostic indicator in head and neck cancer: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol 2018, 275, 1663–1670. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number (n = 102) | % |
|---|---|---|
| Sex | ||
| Male | 93 | 91.2 |
| Female | 9 | 8.8 |
| Median age (range) | 70 (47–87) | |
| Primary site | ||
| Oral | 8 | 7.8 |
| Nasopharynx | 6 | 5.9 |
| Oropharynx | 24 | 23.5 |
| Hypopharynx | 40 | 39.2 |
| Larynx | 12 | 11.8 |
| Others | 12 | 11.8 |
| ECOG performance status | ||
| 0 or 1 | 100 | 98.0 |
| >2 | 2 | 2.0 |
| Type of Recurrence | ||
| Locoregional | 71 | 69.6 |
| Distant | 21 | 20.6 |
| Locoregional+Distant | 10 | 9.8 |
| ICI line | ||
| 1st | 11 | 10.8 |
| 2nd | 47 | 46.1 |
| 3rd | 36 | 35.3 |
| >4th | 8 | 7.8 |
| Previous treatment | ||
| Nivolumab | 76 | 74.5 |
| Pembrolizumab | 26 | 25.5 |
| Prior treatment | ||
| Surgery | 31 | 30.4 |
| Radiation | 77 | 75.5 |
| Chemo | 81 | 79.4 |
| Cetaximub | 16 | 15.7 |
| irAE | ||
| Yes | 20 | 19.6 |
| No | 82 | 80.4 |
| PLR | ||
| ≦397 | 77 | 75.4 |
| >397 | 25 | 24.5 |
| NLR | ||
| ≦6.7 | 71 | 69.6 |
| >6.7 | 31 | 30.3 |
| LMR | ||
| ≦1.88 | 32 | 31.3 |
| >1.88 | 70 | 68.6 |
| SII | ||
| ≦107.5 | 54 | 52.9 |
| >107.5 | 48 | 47 |
| CAR | ||
| ≦0.14 | 52 | 50.9 |
| >0.14 | 50 | 49 |
| CONUT | ||
| ≦3 | 70 | 68.6 |
| ≧4 | 32 | 31.3 |
| PNI | ||
| ≦37.7 | 18 | 17.6 |
| >37.7 | 84 | 82.3 |
| PI | ||
| 0 | 68 | 66.6 |
| ≧1 | 34 | 33.3 |
| GPS | ||
| 0 | 87 | 85.2 |
| ≧1 | 15 | 14.7 |
| BMI | ||
| ≦20 | 45 | 44.1 |
| >20 | 57 | 55.8 |
| Alb | ||
| ≦4.1 | 74 | 72.5 |
| >4.1 | 28 | 27.4 |
| CRP | ||
| ≦0.89 | 66 | 64.7 |
| >0.89 | 36 | 35.2 |
| Variables | All | % |
|---|---|---|
| Number of patients (%) | 102 | |
| Best response (%) | ||
| Complete response | 16 | 15.7 |
| Partial response | 38 | 37.3 |
| Stable disease | 22 | 21.6 |
| Progressive disease | 26 | 25.5 |
| ORR | 54 | 52.9 |
| DCR | 76 | 74.5 |
| (a) Overall Response Rate | ||||||
|---|---|---|---|---|---|---|
| Univariate | ||||||
| Odds Ratio | 95% CI | p-Value | ||||
| Age (<70 or >70) | 0.997 | 0.458–2.17 | 0.9940 | |||
| BMI (Cutoff: 20) | 0.527 | 0.211–1.32 | 0.1720 | |||
| Alb (Cutoff:4.1) | 0.676 | 0.289–1.58 | 0.3650 | |||
| CRP (Cutoff:0.89) | 1.35 | 0.582–3.11 | 0.4880 | |||
| PLR (Cutoff: 397) | 0.736 | 0.337–1.61 | 0.4410 | |||
| NLR (Cutoff: 6.7) | 0.732 | 0.336–1.6 | 0.4330 | |||
| LMR (cutoff: 1.88) | 0.892 | 0.386–2.06 | 0.7890 | |||
| SII (Cutoff: 107.5) | 1.44 | 0.518–4.02 | 0.4830 | |||
| CAR (Cutoff: 0.14) | 0.623 | 0.272–1.43 | 0.2640 | |||
| CONUT (Cutoff: 3) | 0.78 | 0.26–2.34 | 0.6570 | |||
| PNI (Cutoff: 37.7) | 1.72 | 0.781–3.78 | 0.1780 | |||
| PI (Cutoff: 0) | 2.01 | 0.817–4.92 | 0.1290 | |||
| GPS (Cutoff: 0) | 0.627 | 0.277–1.42 | 0.2630 | |||
| (b) Disease control rate | ||||||
| Univariate | Multivariate | |||||
| Odds ratio | 95% CI | p-value | Odds ratio | 95% CI | p-value | |
| Age (<70 or >70) | 0.452 | 0.179–1.14 | 0.0925 | 0.391 | 0.145–1.06 | 0.651 |
| BMI (Cutoff: 20) | 0.393 | 0.149–1.04 | 0.0598 | 1.82 | 0.682–4.86 | 0.232 |
| Alb (Cutoff:4.1) | 0.487 | 0.192–1.24 | 0.1300 | |||
| CRP (Cutoff:0.89) | 2.4 | 0.952–6.05 | 0.0635 | |||
| PLR (Cutoff: 397) | 0.365 | 0.144–0.923 | 0.0332 | 0.397 | 0.117–1.41 | 0.157 |
| NLR (Cutoff: 6.7) | 0.626 | 0.255–1.54 | 0.3070 | |||
| LMR (cutoff: 1.88) | 0.521 | 0.206–1.31 | 0.1670 | |||
| SII (Cutoff: 107.5) | 2.93 | 1.01–8.52 | 0.0478 | 0.613 | 0.186–2.02 | 0.420 |
| CAR (Cutoff: 0.14) | 0.382 | 0.152–0.957 | 0.0399 | 0.619 | 0221–1.74 | 0.360 |
| CONUT (Cutoff: 3) | 0.448 | 0.142–1.41 | 0.1700 | |||
| PNI (Cutoff: 37.7) | 2.09 | 0.847–5.16 | 0.1100 | |||
| PI (Cutoff: 0) | 2.54 | 0.788–8.18 | 0.1190 | |||
| GPS (Cutoff: 0) | 0.434 | 0.174–1.08 | 0.0726 |
| Overall Survival | ||||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Age (<70 or >70) | 0.7737 | 0.4308–1.389 | 0.3904 | 1.189 | 0.6783–2.086 | 0.545 |
| BMI (Cutoff: 20) | 0.8211 | 0.4776–1.412 | 0.4757 | |||
| Alb (Cutoff:4.1) | 0.4133 | 0.1938–0.8813 | 0.0222 | 0.5297 | 0.2353–1.192 | 0.1248 |
| CRP (Cutoff:0.89) | 1.792 | 1.039–3.093 | 0.0361 | |||
| PLR (Cutoff: 397) | 2.77 | 1.568–4.891 | 0.0004 | 1.776 | 0.7779–4.057 | 0.1726 |
| NLR (Cutoff: 6.7) | 2.349 | 1.361–4.053 | 0.0022 | 0.9184 | 0.4027–2.095 | 0.8397 |
| LMR (cutoff: 1.88) | 0.3117 | 0.1776–0.5473 | 0.0000 | 0.4275 | 0.2073–0.8816 | 0.02139 |
| SII (Cutoff: 107.5) | 1.774 | 1.023–3.079 | 0.0414 | |||
| CAR (Cutoff: 0.14) | 1.479 | 0.8541–2.56 | 0.1625 | |||
| CONUT (Cutoff: 3) | 1.942 | 1.104–3.417 | 0.0213 | 1.083 | 0.5665–2.069 | 0.8098 |
| PNI (Cutoff: 37.7) | 0.543 | 0.2887–1.022 | 0.0582 | |||
| PI (Cutoff: 0) | 1.729 | 0.9952–3.005 | 0.0520 | |||
| GPS (Cutoff: 0) | 1.653 | 0.847–3.227 | 0.1407 | |||
| Progression-Free Survival | ||||||
| Univariate | Multivariate | |||||
| Hazard ratio | 95% CI | p-value | Hazard ratio | 95% CI | p-value | |
| Age (<70 or >70) | 0.9701 | 0.6128–1.536 | 0.8969 | 0.9409 | 0.5804–1.525 | 0.8047 |
| BMI (Cutoff: 20) | 0.9565 | 0.6021–1.519 | 0.8504 | |||
| Alb (Cutoff 4.1) | 0.4661 | 0.2636–0.8244 | 0.0087 | 0.5468 | 0.2933–1.019 | 0.05749 |
| CRP (Cutoff 0.89) | 1.644 | 1.019–2.653 | 0.0416 | |||
| PLR (Cutoff: 397) | 1.899 | 1.152–3.133 | 0.0120 | 1.396 | 0.6435–3.028 | 0.3986 |
| NLR (Cutoff: 6.7) | 1.773 | 1.103–2.85 | 0.0180 | 1.156 | 0.5495–2.434 | 0.7019 |
| LMR (cutoff: 1.88) | 0.6033 | 0.372–0.9786 | 0.0406 | |||
| SII (Cutoff: 107.5) | 1.364 | 0.861–2.162 | 0.1859 | |||
| CAR (Cutoff: 0.14) | 1.483 | 0.9355–2.352 | 0.0937 | |||
| CONUT (Cutoff: 3) | 1.848 | 1.131–3.019 | 0.0142 | 0.8504 | 0.4017–1.8 | 0.672 |
| PNI (Cutoff: 37.7) | 0.3622 | 0.2048–0.6404 | 0.0005 | 0.3856 | 0.07537–1.973 | 0.2525 |
| PI (Cutoff: 0) | 1.492 | 0.9179–2.425 | 0.1065 | |||
| GPS (Cutoff: 0) | 2.602 | 1.437–4.709 | 0.0016 | 0.8807 | 0.1881–4.123 | 0.8718 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakai, A.; Iijima, H.; Ebisumoto, K.; Yamauchi, M.; Teramura, T.; Yamazaki, A.; Watanabe, T.; Inagi, T.; Maki, D.; Okami, K. Prognostic Value of Inflammatory and Nutritional Biomarkers of Immune Checkpoint Inhibitor Treatment for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck. Cancers 2023, 15, 2021. https://doi.org/10.3390/cancers15072021
Sakai A, Iijima H, Ebisumoto K, Yamauchi M, Teramura T, Yamazaki A, Watanabe T, Inagi T, Maki D, Okami K. Prognostic Value of Inflammatory and Nutritional Biomarkers of Immune Checkpoint Inhibitor Treatment for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck. Cancers. 2023; 15(7):2021. https://doi.org/10.3390/cancers15072021
Chicago/Turabian StyleSakai, Akihiro, Hiroaki Iijima, Koji Ebisumoto, Mayu Yamauchi, Takanobu Teramura, Aritomo Yamazaki, Takane Watanabe, Toshihide Inagi, Daisuke Maki, and Kenji Okami. 2023. "Prognostic Value of Inflammatory and Nutritional Biomarkers of Immune Checkpoint Inhibitor Treatment for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck" Cancers 15, no. 7: 2021. https://doi.org/10.3390/cancers15072021
APA StyleSakai, A., Iijima, H., Ebisumoto, K., Yamauchi, M., Teramura, T., Yamazaki, A., Watanabe, T., Inagi, T., Maki, D., & Okami, K. (2023). Prognostic Value of Inflammatory and Nutritional Biomarkers of Immune Checkpoint Inhibitor Treatment for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck. Cancers, 15(7), 2021. https://doi.org/10.3390/cancers15072021