


Cognitive Sparing in Proton versus Photon Radiotherapy for Pediatric Brain Tumor Is Associated with White Matter Integrity: An Exploratory Study

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Measures
2.3. Neuroimaging Procedures
2.4. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics
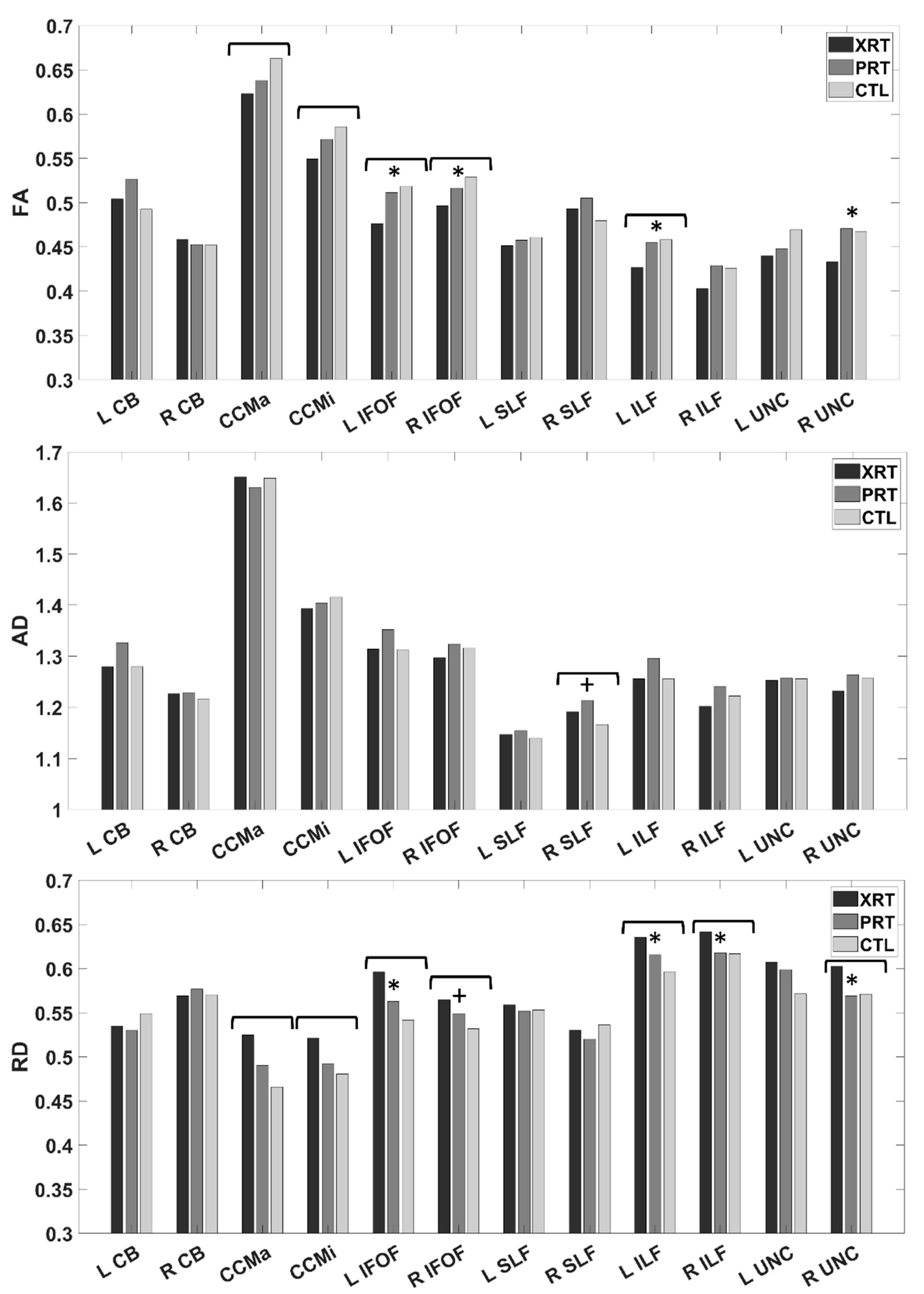
3.2. Group Differences in White Matter Integrity
3.3. Supplemental Analyses: Time since Radiation and White Matter Integrity
3.4. Group Differences in Neuropsychological Performance
3.5. Relationships between Neuropsychological Performance and White Matter Integrity
4. Discussion
4.1. Reduced White Matter Integrity following XRT, but Not PRT
4.2. Tract-Specific Findings
4.3. Time since Treatment Does Not Predict Within-Group White Matter Integrity
4.4. Cognitive Sparing in PRT
4.5. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Curtin, S.C.; Minino, A.M.; Anderson, R.N. Declines in Cancer Death Rates Among Children and Adolescents in the United States, 1999–2014. NCHS Data Brief 2016, 1–8. [Google Scholar]
- de Ruiter, M.A.; van Mourik, R.; Schouten-van Meeteren, A.Y.; Grootenhuis, M.A.; Oosterlaan, J. Neurocognitive consequences of a paediatric brain tumour and its treatment: A meta-analysis. Dev. Med. Child Neurol. 2013, 55, 408–417. [Google Scholar] [CrossRef]
- Robinson, K.E.; Fraley, C.E.; Pearson, M.M.; Kuttesch, J.F., Jr.; Compas, B.E. Neurocognitive late effects of pediatric brain tumors of the posterior fossa: A quantitative review. J. Int. Neuropsychol. Soc. 2013, 19, 44–53. [Google Scholar] [CrossRef]
- Robinson, K.E.; Kuttesch, J.F.; Champion, J.E.; Andreotti, C.F.; Hipp, D.W.; Bettis, A.; Barnwell, A.; Compas, B.E. A quantitative meta-analysis of neurocognitive sequelae in survivors of pediatric brain tumors. Pediatr. Blood Cancer 2010, 55, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Girardi, F.; Allemani, C.; Coleman, M.P. Worldwide Trends in Survival From Common Childhood Brain Tumors: A Systematic Review. J. Glob. Oncol. 2019, 5, 1–25. [Google Scholar] [CrossRef]
- King, A.A.; Seidel, K.; Di, C.; Leisenring, W.M.; Perkins, S.M.; Krull, K.R.; Sklar, C.A.; Green, D.M.; Armstrong, G.T.; Zeltzer, L.K.; et al. Long-term neurologic health and psychosocial function of adult survivors of childhood medulloblastoma/PNET: A report from the Childhood Cancer Survivor Study. Neuro Oncol. 2017, 19, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Schulte, F.; Kunin-Batson, A.S.; Olson-Bullis, B.A.; Banerjee, P.; Hocking, M.C.; Janzen, L.; Kahalley, L.S.; Wroot, H.; Forbes, C.; Krull, K.R. Social attainment in survivors of pediatric central nervous system tumors: A systematic review and meta-analysis from the Children’s Oncology Group. J. Cancer Surviv. 2019, 13, 921–931. [Google Scholar] [CrossRef]
- Warren, E.A.H.; Raghubar, K.P.; Cirino, P.T.; Child, A.E.; Lupo, P.J.; Grosshans, D.R.; Paulino, A.C.; Okcu, M.F.; Minard, C.G.; Ris, M.D.; et al. Cognitive predictors of social adjustment in pediatric brain tumor survivors treated with photon versus proton radiation therapy. Pediatr. Blood Cancer 2022, 69, e29645. [Google Scholar] [CrossRef]
- Roth, A.K.; Ris, M.D.; Orobio, J.; Xue, J.; Mahajan, A.; Paulino, A.C.; Grosshans, D.; Okcu, M.F.; Chintagumpala, M.; Kahalley, L.S. Cognitive mediators of adaptive functioning outcomes in survivors of pediatric brain tumors treated with proton radiotherapy. Pediatr. Blood Cancer 2020, 67, e28064. [Google Scholar] [CrossRef]
- Partanen, M.; Bouffet, E.; Laughlin, S.; Strother, D.; Hukin, J.; Skocic, J.; Szulc-Lerch, K.; Mabbott, D.J. Early changes in white matter predict intellectual outcome in children treated for posterior fossa tumors. Neuroimage Clin. 2018, 20, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Kahalley, L.S.; Ris, M.D.; Grosshans, D.R.; Okcu, M.F.; Paulino, A.C.; Chintagumpala, M.; Moore, B.D.; Guffey, D.; Minard, C.G.; Stancel, H.H.; et al. Comparing Intelligence Quotient Change After Treatment With Proton Versus Photon Radiation Therapy for Pediatric Brain Tumors. J. Clin. Oncol. 2016, 34, 1043–1049. [Google Scholar] [CrossRef]
- Mulhern, R.K.; White, H.A.; Glass, J.O.; Kun, L.E.; Leigh, L.; Thompson, S.J.; Reddick, W.E. Attentional functioning and white matter integrity among survivors of malignant brain tumors of childhood. J. Int. Neuropsychol. Soc. 2004, 10, 180–189. [Google Scholar] [CrossRef]
- Palmer, S.L.; Glass, J.O.; Li, Y.; Ogg, R.; Qaddoumi, I.; Armstrong, G.T.; Wright, K.; Wetmore, C.; Broniscer, A.; Gajjar, A.; et al. White matter integrity is associated with cognitive processing in patients treated for a posterior fossa brain tumor. Neuro Oncol. 2012, 14, 1185–1193. [Google Scholar] [CrossRef]
- Kahalley, L.S.; Conklin, H.M.; Tyc, V.L.; Hudson, M.M.; Wilson, S.J.; Wu, S.; Xiong, X.; Hinds, P.S. Slower processing speed after treatment for pediatric brain tumor and acute lymphoblastic leukemia. Psychooncology 2013, 22, 1979–1986. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.E.; Pearson, M.M.; Cannistraci, C.J.; Anderson, A.W.; Kuttesch, J.F.; Wymer, K.; Smith, S.E.; Compas, B.E. Neuroimaging of executive function in survivors of pediatric brain tumors and healthy controls. Neuropsychology 2014, 28, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Conklin, H.M.; Ashford, J.M.; Di Pinto, M.; Vaughan, C.G.; Gioia, G.A.; Merchant, T.E.; Ogg, R.J.; Santana, V.; Wu, S. Computerized assessment of cognitive late effects among adolescent brain tumor survivors. J. Neurooncol. 2013, 113, 333–340. [Google Scholar] [CrossRef]
- Raghubar, K.P.; Mahone, E.M.; Yeates, K.O.; Cecil, K.M.; Makola, M.; Ris, M.D. Working memory and attention in pediatric brain tumor patients treated with and without radiation therapy. Child Neuropsychol. 2017, 23, 642–654. [Google Scholar] [CrossRef]
- Scantlebury, N.; Cunningham, T.; Dockstader, C.; Laughlin, S.; Gaetz, W.; Rockel, C.; Dickson, J.; Mabbott, D. Relations between white matter maturation and reaction time in childhood. J. Int. Neuropsychol. Soc. 2014, 20, 99–112. [Google Scholar] [CrossRef]
- Bells, S.; Lefebvre, J.; Longoni, G.; Narayanan, S.; Arnold, D.L.; Yeh, E.A.; Mabbott, D.J. White matter plasticity and maturation in human cognition. Glia 2019, 67, 2020–2037. [Google Scholar] [CrossRef] [PubMed]
- Mabbott, D.J.; Noseworthy, M.; Bouffet, E.; Laughlin, S.; Rockel, C. White matter growth as a mechanism of cognitive development in children. Neuroimage 2006, 33, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Connaughton, M.; Whelan, R.; O’Hanlon, E.; McGrath, J. White matter microstructure in children and adolescents with ADHD. Neuroimage Clin. 2022, 33, 102957. [Google Scholar] [CrossRef]
- Back, S.A. White matter injury in the preterm infant: Pathology and mechanisms. Acta Neuropathol. 2017, 134, 331–349. [Google Scholar] [CrossRef] [PubMed]
- Kourtidou, P.; McCauley, S.R.; Bigler, E.D.; Traipe, E.; Wu, T.C.; Chu, Z.D.; Hunter, J.V.; Li, X.; Levin, H.S.; Wilde, E.A. Centrum semiovale and corpus callosum integrity in relation to information processing speed in patients with severe traumatic brain injury. J. Head Trauma Rehabil. 2013, 28, 433–441. [Google Scholar] [CrossRef]
- Wozniak, J.R.; Krach, L.; Ward, E.; Mueller, B.A.; Muetzel, R.; Schnoebelen, S.; Kiragu, A.; Lim, K.O. Neurocognitive and neuroimaging correlates of pediatric traumatic brain injury: A diffusion tensor imaging (DTI) study. Arch. Clin. Neuropsychol. 2007, 22, 555–568. [Google Scholar] [CrossRef]
- Govindarajan, S.T.; Liu, Y.; Parra Corral, M.A.; Bangiyev, L.; Krupp, L.; Charvet, L.; Duong, T.Q. White matter correlates of slowed information processing speed in unimpaired multiple sclerosis patients with young age onset. Brain Imaging Behav. 2021, 15, 1460–1468. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wu, E.X.; Qiu, D.; Leung, L.H.; Lau, H.F.; Khong, P.L. Longitudinal diffusion tensor magnetic resonance imaging study of radiation-induced white matter damage in a rat model. Cancer Res. 2009, 69, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Nieman, B.J.; de Guzman, A.E.; Gazdzinski, L.M.; Lerch, J.P.; Chakravarty, M.M.; Pipitone, J.; Strother, D.; Fryer, C.; Bouffet, E.; Laughlin, S.; et al. White and Gray Matter Abnormalities After Cranial Radiation in Children and Mice. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.L.; Reddick, W.E.; Glass, J.O.; Gajjar, A.; Goloubeva, O.; Mulhern, R.K. Decline in corpus callosum volume among pediatric patients with medulloblastoma: Longitudinal MR imaging study. Am. J. Neuroradiol. 2002, 23, 1088–1094. [Google Scholar]
- Makale, M.T.; McDonald, C.R.; Hattangadi-Gluth, J.A.; Kesari, S. Mechanisms of radiotherapy-associated cognitive disability in patients with brain tumours. Nat. Rev. Neurol. 2017, 13, 52–64. [Google Scholar] [CrossRef]
- Connor, M.; Karunamuni, R.; McDonald, C.; White, N.; Pettersson, N.; Moiseenko, V.; Seibert, T.; Marshall, D.; Cervino, L.; Bartsch, H.; et al. Dose-dependent white matter damage after brain radiotherapy. Radiother. Oncol. 2016, 121, 209–216. [Google Scholar] [CrossRef]
- Reddick, W.E.; Russell, J.M.; Glass, J.O.; Xiong, X.; Mulhern, R.K.; Langston, J.W.; Merchant, T.E.; Kun, L.E.; Gajjar, A. Subtle white matter volume differences in children treated for medulloblastoma with conventional or reduced dose craniospinal irradiation. Magn. Reson. Imaging 2000, 18, 787–793. [Google Scholar] [CrossRef]
- Connor, M.; Karunamuni, R.; McDonald, C.; Seibert, T.; White, N.; Moiseenko, V.; Bartsch, H.; Farid, N.; Kuperman, J.; Krishnan, A.; et al. Regional susceptibility to dose-dependent white matter damage after brain radiotherapy. Radiother. Oncol. 2017, 123, 209–217. [Google Scholar] [CrossRef]
- Mabbott, D.J.; Noseworthy, M.D.; Bouffet, E.; Rockel, C.; Laughlin, S. Diffusion tensor imaging of white matter after cranial radiation in children for medulloblastoma: Correlation with IQ. Neuro Oncol. 2006, 8, 244–252. [Google Scholar] [CrossRef]
- Makola, M.; Douglas Ris, M.; Mahone, E.M.; Yeates, K.O.; Cecil, K.M. Long-term effects of radiation therapy on white matter of the corpus callosum: A diffusion tensor imaging study in children. Pediatr. Radiol. 2017, 47, 1809–1816. [Google Scholar] [CrossRef]
- Redmond, K.J.; Hildreth, M.; Sair, H.I.; Terezakis, S.; McNutt, T.; Kleinberg, L.; Cohen, K.J.; Wharam, M.; Horska, A.; Mahone, E.M. Association of Neuronal Injury in the Genu and Body of Corpus Callosum After Cranial Irradiation in Children With Impaired Cognitive Control: A Prospective Study. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Mulhern, R.K.; Palmer, S.L.; Reddick, W.E.; Glass, J.O.; Kun, L.E.; Taylor, J.; Langston, J.; Gajjar, A. Risks of young age for selected neurocognitive deficits in medulloblastoma are associated with white matter loss. J. Clin. Oncol. 2001, 19, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Mulhern, R.K.; Reddick, W.E.; Palmer, S.L.; Glass, J.O.; Elkin, T.D.; Kun, L.E.; Taylor, J.; Langston, J.; Gajjar, A. Neurocognitive deficits in medulloblastoma survivors and white matter loss. Ann. Neurol. 1999, 46, 834–841. [Google Scholar] [CrossRef]
- King, T.Z.; Wang, L.; Mao, H. Disruption of White Matter Integrity in Adult Survivors of Childhood Brain Tumors: Correlates with Long-Term Intellectual Outcomes. PLoS ONE 2015, 10, e0131744. [Google Scholar] [CrossRef] [PubMed]
- Rueckriegel, S.M.; Bruhn, H.; Thomale, U.W.; Hernaiz Driever, P. Cerebral white matter fractional anisotropy and tract volume as measured by MR imaging are associated with impaired cognitive and motor function in pediatric posterior fossa tumor survivors. Pediatr. Blood Cancer 2015, 62, 1252–1258. [Google Scholar] [CrossRef]
- Reddick, W.E.; Taghipour, D.J.; Glass, J.O.; Ashford, J.; Xiong, X.; Wu, S.; Bonner, M.; Khan, R.B.; Conklin, H.M. Prognostic factors that increase the risk for reduced white matter volumes and deficits in attention and learning for survivors of childhood cancers. Pediatr. Blood Cancer 2014, 61, 1074–1079. [Google Scholar] [CrossRef]
- Reddick, W.E.; White, H.A.; Glass, J.O.; Wheeler, G.C.; Thompson, S.J.; Gajjar, A.; Leigh, L.; Mulhern, R.K. Developmental model relating white matter volume to neurocognitive deficits in pediatric brain tumor survivors. Cancer 2003, 97, 2512–2519. [Google Scholar] [CrossRef]
- Jacola, L.M.; Ashford, J.M.; Reddick, W.E.; Glass, J.O.; Ogg, R.J.; Merchant, T.E.; Conklin, H.M. The relationship between working memory and cerebral white matter volume in survivors of childhood brain tumors treated with conformal radiation therapy. J. Neurooncol. 2014, 119, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Law, N.; Bouffet, E.; Laughlin, S.; Laperriere, N.; Briere, M.E.; Strother, D.; McConnell, D.; Hukin, J.; Fryer, C.; Rockel, C.; et al. Cerebello-thalamo-cerebral connections in pediatric brain tumor patients: Impact on working memory. Neuroimage 2011, 56, 2238–2248. [Google Scholar] [CrossRef] [PubMed]
- Aukema, E.J.; Caan, M.W.; Oudhuis, N.; Majoie, C.B.; Vos, F.M.; Reneman, L.; Last, B.F.; Grootenhuis, M.A.; Schouten-van Meeteren, A.Y. White matter fractional anisotropy correlates with speed of processing and motor speed in young childhood cancer survivors. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Scantlebury, N.; Bouffet, E.; Laughlin, S.; Strother, D.; McConnell, D.; Hukin, J.; Fryer, C.; Laperriere, N.; Montour-Proulx, I.; Keene, D.; et al. White matter and information processing speed following treatment with cranial-spinal radiation for pediatric brain tumor. Neuropsychology 2016, 30, 425–438. [Google Scholar] [CrossRef] [PubMed]
- Merchant, T.E. Proton beam therapy in pediatric oncology. Cancer J. 2009, 15, 298–305. [Google Scholar] [CrossRef]
- Merchant, T.E.; Farr, J.B. Proton beam therapy: A fad or a new standard of care. Curr. Opin. Pediatr. 2014, 26, 3–8. [Google Scholar] [CrossRef]
- Baliga, S.; Yock, T.I. Proton beam therapy in pediatric oncology. Curr. Opin. Pediatr. 2019, 31, 28–34. [Google Scholar] [CrossRef]
- Child, A.E.; Warren, E.A.; Grosshans, D.R.; Paulino, A.C.; Okcu, M.F.; Ris, M.D.; Mahajan, A.; Orobio, J.; Cirino, P.T.; Minard, C.G.; et al. Long-term cognitive and academic outcomes among pediatric brain tumor survivors treated with proton versus photon radiotherapy. Pediatr. Blood Cancer 2021, 68, e29125. [Google Scholar] [CrossRef]
- Gross, J.P.; Powell, S.; Zelko, F.; Hartsell, W.; Goldman, S.; Fangusaro, J.; Lulla, R.R.; Smiley, N.P.; Chang, J.H.; Gondi, V. Improved neuropsychological outcomes following proton therapy relative to X-ray therapy for pediatric brain tumor patients. Neuro Oncol. 2019, 21, 934–943. [Google Scholar] [CrossRef]
- Antonini, T.N.; Ris, M.D.; Grosshans, D.R.; Mahajan, A.; Okcu, M.F.; Chintagumpala, M.; Paulino, A.; Child, A.E.; Orobio, J.; Stancel, H.H.; et al. Attention, processing speed, and executive functioning in pediatric brain tumor survivors treated with proton beam radiation therapy. Radiother. Oncol. 2017, 124, 89–97. [Google Scholar] [CrossRef]
- Pulsifer, M.B.; Duncanson, H.; Grieco, J.; Evans, C.; Tseretopoulos, I.D.; MacDonald, S.; Tarbell, N.J.; Yock, T.I. Cognitive and Adaptive Outcomes After Proton Radiation for Pediatric Patients With Brain Tumors. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 391–398. [Google Scholar] [CrossRef]
- Kahalley, L.S.; Douglas Ris, M.; Mahajan, A.; Fatih Okcu, M.; Chintagumpala, M.; Paulino, A.C.; Whitehead, W.E.; Minard, C.G.; Stancel, H.H.; Orobio, J.; et al. Prospective, longitudinal comparison of neurocognitive change in pediatric brain tumor patients treated with proton radiotherapy versus surgery only. Neuro Oncol. 2019, 21, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Kahalley, L.S.; Peterson, R.; Ris, M.D.; Janzen, L.; Okcu, M.F.; Grosshans, D.R.; Ramaswamy, V.; Paulino, A.C.; Hodgson, D.; Mahajan, A.; et al. Superior Intellectual Outcomes After Proton Radiotherapy Compared with Photon Radiotherapy for Pediatric Medulloblastoma. J. Clin. Oncol. 2020, 38, 454–461. [Google Scholar] [CrossRef]
- Dünger, L.; Seidlitz, A.; Jentsch, C.; Platzek, I.; Kotzerke, J.; Beuthien-Baumann, B.; Baumann, M.; Krause, M.; Troost, E.G.C.; Raschke, F. Reduced diffusion in white matter after radiotherapy with photons and protons. Radiother. Oncol. 2021, 164, 66–72. [Google Scholar] [CrossRef]
- Weschler, D. Wechsler Intelligence Scale for Children, 5th ed.; Pearson: Bloomington, MN, USA, 2014. [Google Scholar]
- Weschler, D. Wechsler Intelligence Scale for Children, 4th ed.; The Psychological Corporation: San Antonio, TX, USA, 2003. [Google Scholar]
- Weschler, D. Weschler Adult Intelligence Scale, 4th ed.; Pearson: San Antonio, TX, USA, 2009. [Google Scholar]
- Standardization Data from the Weschler Intelligence Scale for Children, 5th ed.; Pearson: Bloomington, MN, USA, 2014.
- Beery, K.E.; Buktenica, N.A.; Beery, N.A. The Beery-Buktenica Developmental Test of Visual-Motor Integration, 6th ed.; Pearson: Minneapolis, MN, USA, 2010. [Google Scholar]
- Andersson, J.L.; Skare, S.; Ashburner, J. How to correct susceptibility distortions in spin-echo echo-planar images: Application to diffusion tensor imaging. Neuroimage 2003, 20, 870–888. [Google Scholar] [CrossRef]
- Andersson, J.L.R.; Graham, M.S.; Zsoldos, E.; Sotiropoulos, S.N. Incorporating outlier detection and replacement into a non-parametric framework for movement and distortion correction of diffusion MR images. Neuroimage 2016, 141, 556–572. [Google Scholar] [CrossRef]
- Andersson, J.L.R.; Sotiropoulos, S.N. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage 2016, 125, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Andersson, J.L.R.; Graham, M.S.; Drobnjak, I.; Zhang, H.; Filippini, N.; Bastiani, M. Towards a comprehensive framework for movement and distortion correction of diffusion MR images: Within volume movement. Neuroimage 2017, 152, 450–466. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M. Fast robust automated brain extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef]
- Yeatman, J.D.; Dougherty, R.F.; Myall, N.J.; Wandell, B.A.; Feldman, H.M. Tract profiles of white matter properties: Automating fiber-tract quantification. PLoS ONE 2012, 7, e49790. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Field, A.S. Diffusion tensor imaging of the brain. Neurotherapeutics 2007, 4, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Song, S.K.; Yoshino, J.; Le, T.Q.; Lin, S.J.; Sun, S.W.; Cross, A.H.; Armstrong, R.C. Demyelination increases radial diffusivity in corpus callosum of mouse brain. Neuroimage 2005, 26, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Lalkovicova, M. Neuroprotective agents effective against radiation damage of central nervous system. Neural Regen Res 2022, 17, 1885–1892. [Google Scholar] [CrossRef]
- Shahsavani, N.; Kataria, H.; Karimi-Abdolrezaee, S. Mechanisms and repair strategies for white matter degeneration in CNS injury and diseases. Biochim. Et Biophys. Acta (BBA)—Mol. Basis Dis. 2021, 1867, 166117. [Google Scholar] [CrossRef]
- Tamnes, C.K.; Roalf, D.R.; Goddings, A.-L.; Lebel, C. Diffusion MRI of white matter microstructure development in childhood and adolescence: Methods, challenges and progress. Dev. Cogn. Neurosci. 2018, 33, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Buyanova, I.S.; Arsalidou, M. Cerebral White Matter Myelination and Relations to Age, Gender, and Cognition: A Selective Review. Front. Hum. Neurosci. 2021, 15, 662031. [Google Scholar] [CrossRef]
- Banich, M.T.; Brown, W.S. A Life-Span Perspective on Interaction Between the Cerebral Hemispheres. Dev. Neuropsychol. 2000, 18, 1–10. [Google Scholar] [CrossRef]
- Leng, Y.; Shi, Y.; Yu, Q.; Van Horn, J.D.; Tang, H.; Li, J.; Xu, W.; Ge, X.; Tang, Y.; Han, Y.; et al. Phenotypic and Genetic Correlations Between the Lobar Segments of the Inferior Fronto-occipital Fasciculus and Attention. Sci. Rep. 2016, 6, 33015. [Google Scholar] [CrossRef]
- Mandonnet, E.; Nouet, A.; Gatignol, P.; Capelle, L.; Duffau, H. Does the left inferior longitudinal fasciculus play a role in language? A brain stimulation study. Brain 2007, 130, 623–629. [Google Scholar] [CrossRef]
- Shin, J.; Rowley, J.; Chowdhury, R.; Jolicoeur, P.; Klein, D.; Grova, C.; Rosa-Neto, P.; Kobayashi, E. Inferior Longitudinal Fasciculus’ Role in Visual Processing and Language Comprehension: A Combined MEG-DTI Study. Front. Neurosci. 2019, 13, 875. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Wu, S.; Ashford, J.M.; Tinkle, C.L.; Lucas, J.T.; Qaddoumi, I.; Gajjar, A.; Krasin, M.J.; Conklin, H.M.; Merchant, T.E. Association between hippocampal dose and memory in survivors of childhood or adolescent low-grade glioma: A 10-year neurocognitive longitudinal study. Neuro Oncol. 2019, 21, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Fujie, S.; Namiki, C.; Nishi, H.; Yamada, M.; Miyata, J.; Sakata, D.; Sawamoto, N.; Fukuyama, H.; Hayashi, T.; Murai, T. The role of the uncinate fasciculus in memory and emotional recognition in amnestic mild cognitive impairment. Dement Geriatr. Cogn. Disord. 2008, 26, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.K.; Corsello, C.; Kennedy, D.P.; Adolphs, R. Agenesis of the corpus callosum and autism: A comprehensive comparison. Brain 2014, 137, 1813–1829. [Google Scholar] [CrossRef] [PubMed]
- Helson, L. Radiation-induced Demyelination and Remyelination in the Central Nervous System: A Literature Review. Anticancer Res. 2018, 38, 4999–5002. [Google Scholar] [CrossRef]
- Liu, F.; Scantlebury, N.; Tabori, U.; Bouffet, E.; Laughlin, S.; Strother, D.; McConnell, D.; Hukin, J.; Fryer, C.; Briere, M.E.; et al. White matter compromise predicts poor intellectual outcome in survivors of pediatric low-grade glioma. Neuro Oncol. 2015, 17, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Askins, M.A.; Moore, B.D., 3rd. Preventing neurocognitive late effects in childhood cancer survivors. J. Child Neurol. 2008, 23, 1160–1171. [Google Scholar] [CrossRef]


{kind=link}
| XRT (n = 10) | PRT (n = 12) | CTL (n = 23) | Χ2 | p | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Sex | 1.97 | 0.373 | ||||||
| Male | 7 | 70 | 6 | 50 | 10 | 43 | ||
| Female | 3 | 30 | 6 | 50 | 13 | 57 | ||
| Handedness | 8.84 | 0.012 | ||||||
| Right | 10 | 100 | 9 | 75 | 23 | 100 | ||
| Left | 0 | 0 | 3 | 25 | 0 | 0 | ||
| Race | 0.41 | 0.814 | ||||||
| White | 9 | 90 | 10 | 83 | 19 | 83 | ||
| Black | 1 | 10 | 2 | 17 | 2 | 9 | ||
| Unknown | 0 | 0 | 0 | 0 | 2 | 9 | ||
| Ethnicity | 1.47 | 0.479 | ||||||
| Hispanic/Latino | 5 | 50 | 3 | 25 | 8 | 35 | ||
| Not Hispanic/Latino | 5 | 50 | 9 | 75 | 13 | 57 | ||
| Unknown | 0 | 0 | 0 | 0 | 2 | 9 | ||
| Maternal Education | 4.39 | 0.625 | ||||||
| <High school | 0 | 0 | 2 | 17 | 1 | 4 | ||
| High school | 6 | 60 | 5 | 42 | 12 | 52 | ||
| 4-year college degree | 1 | 10 | 4 | 33 | 4 | 17 | ||
| Advanced degree | 1 | 10 | 1 | 8 | 3 | 13 | ||
| Unknown | 2 | 20 | 0 | 0 | 3 | 13 | ||
| Family Income ($) | 10.26 | 0.114 | ||||||
| <40,000 | 2 | 20 | 2 | 17 | 8 | 35 | ||
| 40,000–79,999 | 3 | 30 | 3 | 25 | 8 | 35 | ||
| 80,000+ | 3 | 30 | 7 | 58 | 7 | 30 | ||
| Unknown | 2 | 20 | 0 | 0 | 0 | 0 | ||
| Tumor location | 0.22 | 0.639 | ||||||
| Supratentorial | 4 | 40 | 6 | 50 | --- | |||
| Infratentorial | 6 | 60 | 6 | 50 | --- | |||
| Tumor type | 0.35 | 0.950 | ||||||
| Low Grade Glioma | 2 | 20 | 3 | 25 | --- | |||
| Embryonal Tumor | 4 | 40 | 4 | 33 | --- | |||
| Ependymoma | 1 | 10 | 2 | 17 | --- | |||
| Other | 3 | 30 | 3 | 25 | --- | |||
| RT technique | ||||||||
| CSI | 5 | 50 | 4 | 33 | --- | 0.63 | 0.429 | |
| Focal | 5 | 50 | 8 | 67 | --- | |||
| Ventriculoperitoneal Shunt | 1.56 | 0.211 | ||||||
| Yes | 6 | 60 | 4 | 33 | --- | |||
| No | 4 | 40 | 8 | 67 | --- | |||
| Chemotherapy | 3.32 | 0.069 | ||||||
| Yes | 8 | 80 | 5 | 42 | --- | |||
| No | 2 | 20 | 7 | 58 | --- | |||
| XRT (n = 10) | PRT (n = 12) | CTL (n = 23) | F | p | ||||
| Mean (SD) | Min-Max | Mean (SD) | Min-Max | Mean (SD) | Min-Max | |||
| Age at evaluation (yrs) | 21.7 (5.7) | 15.3–34.5 | 16.9 (4.6) | 10.4–23.7 | 15.5 (5.3) | 6.8–29.3 | 4.91 | 0.012 |
| Household size | 4.4 (1.2) | 2–6 | 4.3 (1.2) | 3–7 | 4.8 (1.5) | 2– 8 | 0.67 | 0.517 |
| Age at diagnosis (yrs) | 5.9 (3.8) | 0.8–12.7 | 7.1 (4.2) | 1.8–16.1 | --- | 0.52 | 0.479 | |
| Time since RT (yrs) | 14.7 (2.4) | 12.2–18.5 | 8.9 (1.5) | 7.1–11.8 | --- | 47.65 | <0.001 | |
| Total RT dose for primary tumor (cGy) | 5338 (370) | 4500–5940 | 5355 (308) | 5040–5940 | --- | 0.01 | 0.908 | |
| # of Craniotomies | 1.3 (0.48) | 1–2 | 1.2 (1.1) | 0–4 | --- | 0.12 | 0.730 | |
| Karnofsky–Lansky | 72.9 (13.8) | 50.0–90.0 | 84.5 (16.9) | 50.0–100.0 | --- | 2.33 | 0.147 | |
| XRT vs. PRT | PRT vs. CTL | |||||
|---|---|---|---|---|---|---|
| β | t | p | β | t | p | |
| FA | −0.027 | −2.58 | 0.010 | 0.006 | 0.65 | 0.515 |
| AD | −0.004 | −0.19 | 0.853 | −0.019 | −1.20 | 0.229 |
| RD | 0.035 | 4.21 | <0.001 | −0.012 | −1.80 | 0.073 |
| XRT (n = 10) | PRT (n = 12) | CTL (n = 23) | ||||
|---|---|---|---|---|---|---|
| Mean (SD) | Min-Max | Mean (SD) | Min-Max | Mean (SD) | Min-Max | |
| FSIQ | 80.0 (14.5) | 61–106 | 98.6 (14.6) | 76–129 | 99.7 (10.9) | 84–125 |
| VCI | 83.9 (11.4) | 68–107 | 101.3 (17.1) | 76–136 | 98.1 (12.8) | 78–118 |
| PRI | 89.6 (16.6) | 69–119 | 103.8 (12.2) | 83–125 | 100.0 (12.3) | 79–125 |
| WMI | 81.5 (16.2) | 58–105 | 101.0 (15.9) | 79–135 | 102.2 (10.3) | 88–122 |
| PSI | 75.2 (16.8) | 59–103 | 89.2 (18.1) | 68–126 | 101.0 (11.2) | 75–123 |
| VMI | 69.0 (20.7 | 45–103 | 92.0 (9.4) | 78–112 | 86.5 (11.5) | 50–104 |
| MC | 66.8 (13.4) | 45–89 | 85.3 (12.6) | 64–102 | 88.1 (11.4) | 61–102 |
| XRT vs. PRT | PRT vs. CTL | |||||
| t | p | t | p | |||
| FSIQ | −3.15 | 0.003 | 0.59 | 0.561 | ||
| VCI | −2.48 | 0.018 | 0.15 | 0.883 | ||
| PRI | −2.38 | 0.022 | −0.10 | 0.920 | ||
| WMI | −2.84 | 0.007 | 0.50 | 0.617 | ||
| PSI | −2.52 | 0.016 | 1.33 | 0.192 | ||
| VMI | −3.10 | 0.004 | −0.92 | 0.363 | ||
| MC | −3.83 | <0.001 | −0.06 | 0.951 | ||
| R CB | CCMa | L IFOF | L ILF | |||||
|---|---|---|---|---|---|---|---|---|
| # of Domains | 1/7 | 4/7 | 1/7 | 4/7 | ||||
| r | p | r | p | r | p | r | p | |
| FSIQ | --- | --- | 0.39 | 0.010 | --- | --- | 0.38 | 0.011 |
| VCI | --- | --- | --- | --- | --- | --- | 0.41 | 0.006 |
| PRI | --- | --- | --- | --- | --- | --- | --- | --- |
| WMI | --- | --- | 0.31 | 0.037 | --- | --- | --- | --- |
| PSI | −0.34 | 0.028 | 0.51 | <0.001 | --- | --- | 0.44 | 0.003 |
| VMI | --- | --- | --- | --- | --- | --- | --- | --- |
| MC | --- | --- | 0.41 | 0.005 | 0.39 | 0.010 | 0.39 | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mash, L.E.; Kahalley, L.S.; Raghubar, K.P.; Goodrich-Hunsaker, N.J.; Abildskov, T.J.; De Leon, L.A.; MacLeod, M.; Stancel, H.; Parsons, K.; Biekman, B.; et al. Cognitive Sparing in Proton versus Photon Radiotherapy for Pediatric Brain Tumor Is Associated with White Matter Integrity: An Exploratory Study. Cancers 2023, 15, 1844. https://doi.org/10.3390/cancers15061844
Mash LE, Kahalley LS, Raghubar KP, Goodrich-Hunsaker NJ, Abildskov TJ, De Leon LA, MacLeod M, Stancel H, Parsons K, Biekman B, et al. Cognitive Sparing in Proton versus Photon Radiotherapy for Pediatric Brain Tumor Is Associated with White Matter Integrity: An Exploratory Study. Cancers. 2023; 15(6):1844. https://doi.org/10.3390/cancers15061844
Chicago/Turabian StyleMash, Lisa E., Lisa S. Kahalley, Kimberly P. Raghubar, Naomi J. Goodrich-Hunsaker, Tracy J. Abildskov, Luz A. De Leon, Marianne MacLeod, Heather Stancel, Kelley Parsons, Brian Biekman, and et al. 2023. "Cognitive Sparing in Proton versus Photon Radiotherapy for Pediatric Brain Tumor Is Associated with White Matter Integrity: An Exploratory Study" Cancers 15, no. 6: 1844. https://doi.org/10.3390/cancers15061844
APA StyleMash, L. E., Kahalley, L. S., Raghubar, K. P., Goodrich-Hunsaker, N. J., Abildskov, T. J., De Leon, L. A., MacLeod, M., Stancel, H., Parsons, K., Biekman, B., Desai, N. K., Grosshans, D. R., Paulino, A. C., Chu, Z. D., Whitehead, W. E., Okcu, M. F., Chintagumpala, M., & Wilde, E. A. (2023). Cognitive Sparing in Proton versus Photon Radiotherapy for Pediatric Brain Tumor Is Associated with White Matter Integrity: An Exploratory Study. Cancers, 15(6), 1844. https://doi.org/10.3390/cancers15061844