
Cost-Effectiveness Analysis of HPV Extended versus Partial Genotyping for Cervical Cancer Screening in Singapore
 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
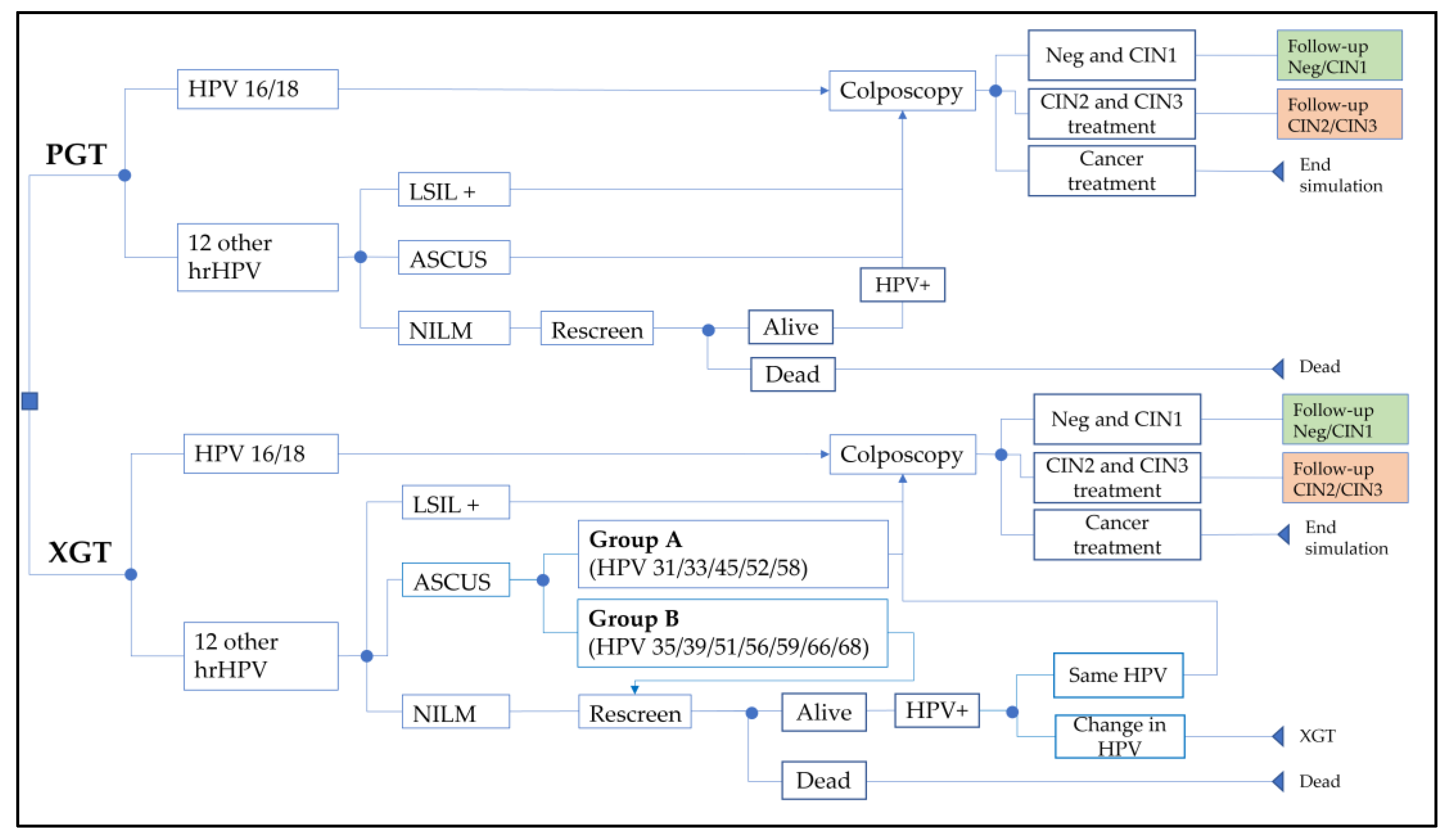
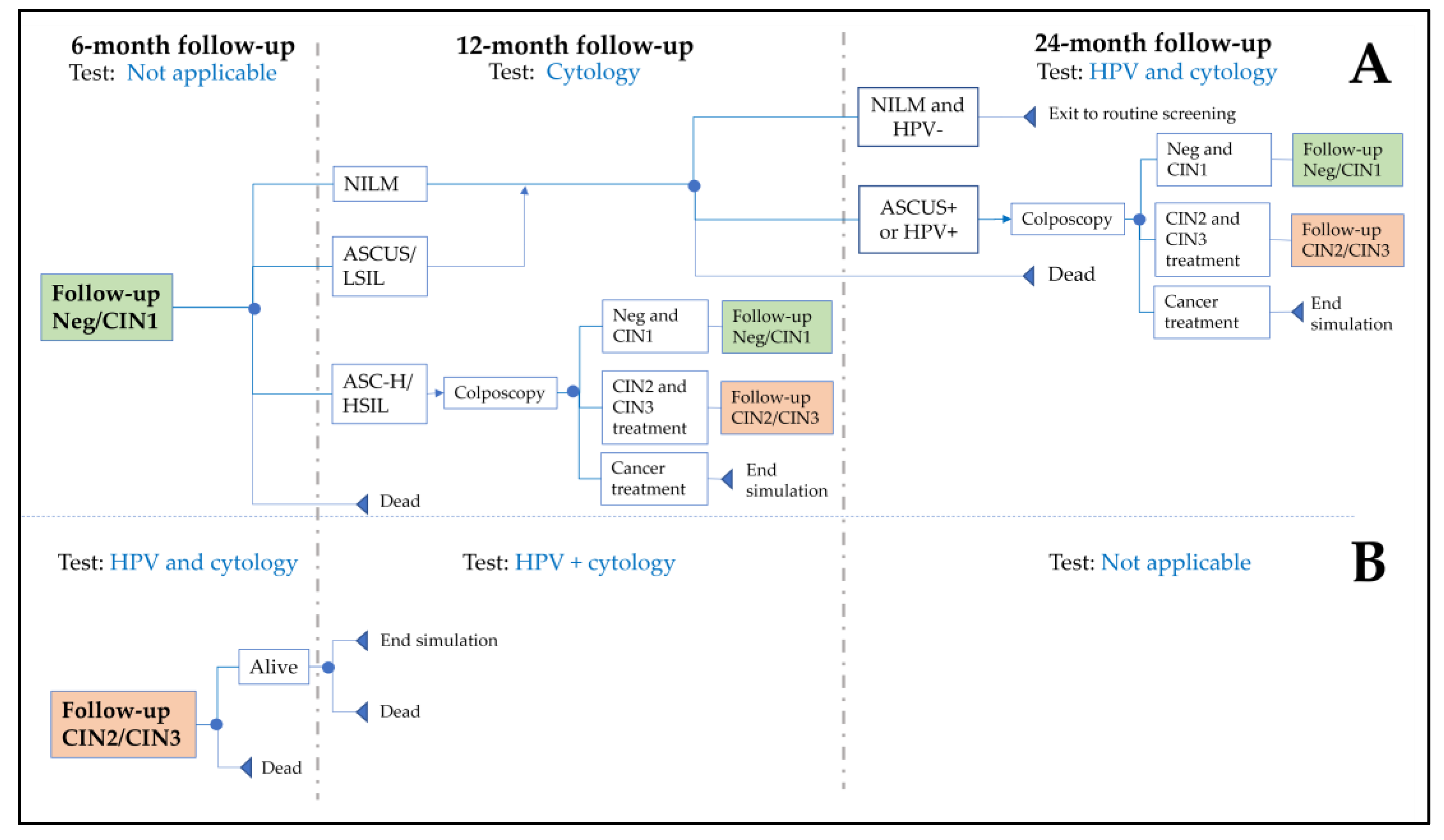
2.1. Model Schematics and Screening Algorithm
2.2. Model Inputs

{kind=link}
{kind=link}
{kind=link}
| Input | Base Case | Lower Limit | Upper Limit | Distribution | Reference |
|---|---|---|---|---|---|
| Number eligible | 1,037,598 | - | - | - | [27,28] |
| Screening coverage | 48.2% | 45.8% | 50.7% | Beta | [30] |
| Follow-up non-adherence * | 25.0% | 0% | 40% | - | [28] † |
| Clinical inputs | |||||
| hrHPV | |||||
| Prevalence | 9.2% | 7.9% | 10.5% | Beta | [28] |
| % non-HPV16/18 | 80.8% | 70.3% | 83.0% | Beta | [28] |
| % Group B | 56.6% | 51.0% | 61.0% | Beta | [41] |
| % NILM | 56.1% | - | - | - | [42] |
| ASCUS among: | |||||
| Group B | 31.8% | - | - | - | [42] |
| Group A | 40.6% | - | - | - | [42] |
| CIN1 regressing in 1 year | 60.0% | 45.0% | 73.0% | Beta | [43] |
| Cancers among: | |||||
| CIN2+ diagnosis | 2.6% | 2.3% | 2.9% | Beta | [44] |
| CIN2+ of Group B with ASCUS | 2.6% | 0.0% | 10.0% | - | [44,45,46,47] |
| CIN2+ risk with: | |||||
| Group B with ASCUS | 6.1% | 2.6% | 9.5% | Beta | [45,46,47,48] |
| Group A with ASCUS | 14.2% | - | - | - | [48] |
| HPV16/18 | 21.9% | - | - | - | [48] |
| Non-HPV16/18 with LSIL+ | 16.4% | - | - | - | [48] |
| PSGI at repeat screening | 57.1% | 54.2% | 60.1% | Beta | [49,50,51] |
| hrHPV 1 yr persistence | 43.3% | 41.8% | 44.8% | Beta | [52] |
| HSIL/ASC-H 1 year post CIN1/negative for CIN | 6.7% | 5.7% | 7.7% | Beta | [53] |
| ASCUS+/HPV+ 2 years post CIN1/negative for CIN | 15.4% | 13.8% | 17.1% | Beta | [28] |
| Proportion stage I cancer | 40.8% | - | - | - | [54] |
| Proportion stage II cancer | 24.4% | - | - | - | [54] |
| Proportion stage III cancer | 18.1% | - | - | - | [54] |
| Proportion stage IV cancer | 16.7% | - | - | - | [54] |
| 10-year cancer survival | 45.4% | - | - | - | [40] |
| XGT repeat screenings | 2 | 1 | 5 | - | † |
| Annualized CIN2+ risk for | |||||
| HPV genotype persistence | |||||
| Same | 5.7% | - | - | - | [55] |
| Change | 1.9% | - | - | - | [55] |
| Regardless of genotype | 3.3% | - | - | - | [55] |
| Multiplier for CIN2+ risk | 1 | 0.7 | 1.38 | Normal | † |
| Annualized CIN2+ risk for CIN1/negative for CIN | |||||
| 1 negative pap smear | 1.1% | - | - | - | [56] |
| ASCUS/LSIL upon follow-up | 2.1% | - | - | - | [56] |
| ASC-H upon follow-up | 5.3% | - | - | - | [56] |
| HSIL+ upon follow-up | 3.4% | - | - | - | [56] |
| Cost inputs SGD (USD) | |||||
| Clinic visit | 75 (89) | 37 (44) | 113 (134) | Normal | [34] |
| Cytology | 79 (94) | 39 (46) | 119 (141) | Normal | [34] |
| HPV DNA (PGT) | 115 (137) | 57 (68) | 173 (206) | Normal | [34] |
| CIN2/3 treatment | 3662 (4354) | 1832 (2178) | 5492 (6530) | Normal | [34] |
| Colposcopy | 350 (416) | 174 (207) | 526 (625) | Normal | [34] |
| Biopsy | 500 (595) | 250 (297) | 750 (892) | Normal | [34] |
| Colposcopies with biopsies | 8% | - | - | - | † |
| Stage I cancer treatment | 28,350 (33,710) | 14,176 (16,856) | 42,524 (50,564) | - | [34] |
| Stage II cancer treatment | 34,568 (41,103) | 17,284 (20,552) | 51,852 (61,655) | - | [34] |
| Stage III cancer treatment | 34,568 (41,103) | 17,284 (20,552) | 51,852 (61,655) | - | [34] |
| Stage IV cancer line 1 treatment | 43,016 (51,149) | 21,508 (25,574) | 64,524 (76,723) | - | [34] |
| Stage IV cancer line 2 treatment | 75,552 (89,836) | 37,776 (44,918) | 113,328 (134,754) | - | [34] |
| Cancer treatment ‡ | 37,227 (44,265) | 29,781 (35,412) | 44,672 (53,118) | Normal | Calculated |
| XGT cost factor | 1.15 | 1.00 | 1.30 | - | † |
| Utility | |||||
| Screening | 0.980 | 0.970 | 0.990 | - | [34] |
| Colposcopy normal results | 0.950 | 0.924 | 0.976 | - | [34] |
| CIN1 | 0.910 | 0.888 | 0.954 | - | [34] |
| CIN2/3 | 0.870 | 0.804 | 0.936 | - | [34] |
| Cancer Stage I | 0.650 | 0.490 | 0.810 | - | [34] |
| Cancer Stage II/III | 0.560 | 0.420 | 0.700 | - | [34] |
| Cancer Stage IV | 0.480 | 0.360 | 0.600 | - | [34] |
| Cancer stage I survivor | 0.970 | 0.730 | 0.990 | - | [34] |
| Cancer stage II/III survivor | 0.900 | 0.680 | 0.990 | - | [34] |
| Cancer stage IV survivor | 0.620 | 0.470 | 0.780 | - | [34] |
| QALY loss | |||||
| Screening | 0.000769 | 0.000384 | 0.00115 | Normal | Calculated |
| CIN1 or negative for CIN1 | 0.00538 | 0.00269 | 0.00723 | Normal | Calculated |
| CIN2/3 | 0.0200 | 0.00985 | 0.0302 | Normal | Calculated |
| Cancer treatment ‡ | 0.0930 | 0.0640 | 0.121 | Normal | Calculated |
| Average lifetime QALY loss for cancer ‡ | 18.7 | 14.9 | 22.4 | Normal | Calculated |
2.3. Cost-Effectiveness Analysis
2.4. Validation and Verification
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, D.; Vignat, J.; Lorenzoni, V.; Eslahi, M.; Ginsburg, O.; Lauby-Secretan, B.; Arbyn, M.; Basu, P.; Bray, F.; Vaccarella, S. Global estimates of incidence and mortality of cervical cancer in 2020: A baseline analysis of the WHO Global Cervical Cancer Elimination Initiative. Lancet Glob. Health 2022, 11, e197–e206. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Cervical Cancer Elimination Initiative. Available online: https://www.who.int/initiatives/cervical-cancer-elimination-initiative (accessed on 4 October 2022).
- Schiffman, M.; Clifford, G.; Buonaguro, F.M. Classification of weakly carcinogenic human papillomavirus types: Addressing the limits of epidemiology at the borderline. Infect. Agents Cancer 2009, 4, 8. [Google Scholar] [CrossRef]
- Arbyn, M.; Simon, M.; Peeters, E.; Xu, L.; Meijer, C.; Berkhof, J.; Cuschieri, K.; Bonde, J.; Ostrbenk Vanlencak, A.; Zhao, F.H.; et al. 2020 list of human papillomavirus assays suitable for primary cervical cancer screening. Clin. Microbiol. Infect. 2021, 27, 1083–1095. [Google Scholar] [CrossRef]
- Serrano, B.; Ibáñez, R.; Robles, C.; Peremiquel-Trillas, P.; de Sanjosé, S.; Bruni, L. Worldwide use of HPV self-sampling for cervical cancer screening. Prev. Med. 2022, 154, 106900. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Depuydt, C.; Benoy, I.; Bogers, J.; Cuschieri, K.; Schmitt, M.; Pawlita, M.; Geraets, D.; Heard, I.; Gheit, T.; et al. VALGENT: A protocol for clinical validation of human papillomavirus assays. J. Clin. Virol. 2016, 76 (Suppl. 1), S14–S21. [Google Scholar] [CrossRef] [PubMed]
- Bonde, J.H.; Pedersen, H.; Quint, W.; Xu, L.; Arbyn, M.; Ejegod, D.M. Clinical and Analytical Performance of the BD Onclarity HPV Assay with SurePath Screening Samples from the Danish Cervical Screening Program Using the VALGENT Framework. J. Clin. Microbiol. 2020, 58, e01518–e01519. [Google Scholar] [CrossRef] [PubMed]
- Bonde, J.H.; Sandri, M.T.; Gary, D.S.; Andrews, J.C. Clinical Utility of Human Papillomavirus Genotyping in Cervical Cancer Screening: A Systematic Review. J. Low Genit. Tract. Dis. 2020, 24, 1–13. [Google Scholar] [CrossRef]
- Bonde, J.; Bottari, F.; Iacobone, A.D.; Cocuzza, C.E.; Sandri, M.T.; Bogliatto, F.; Khan, K.S.; Ejegod, D.M.; Gary, D.S.; Andrews, J.C. Human Papillomavirus Same Genotype Persistence and Risk: A Systematic Review. J. Low Genit. Tract. Dis. 2021, 25, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Chua, B.W.B.; Ma, V.Y.; Alcántar-Fernández, J.; Wee, H.L. Is It Time to Genotype Beyond HPV16 and HPV18 for Cervical Cancer Screening? Int. J. Public Health 2022, 67, 1604621. [Google Scholar] [CrossRef]
- Liverani, C.A.; Di Giuseppe, J.; Giannella, L.; Delli Carpini, G.; Ciavattini, A. Cervical Cancer Screening Guidelines in the Postvaccination Era: Review of the Literature. J. Oncol. 2020, 2020, 8887672. [Google Scholar] [CrossRef]
- Nayar, R. Precision Prevention: The 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J. Mol. Pathol. 2021, 2, 274–280. [Google Scholar] [CrossRef]
- Hampson, I.N. Effects of the Prophylactic HPV Vaccines on HPV Type Prevalence and Cervical Pathology. Viruses 2022, 14, 757. [Google Scholar] [CrossRef]
- Ährlund-Richter, A.; Cheng, L.; Hu, Y.O.O.; Svensson, M.; Pennhag, A.A.L.; Ursu, R.G.; Haeggblom, L.; Grün, N.; Ramqvist, T.; Engstrand, L.; et al. Changes in Cervical Human Papillomavirus (HPV) Prevalence at a Youth Clinic in Stockholm, Sweden, a Decade After the Introduction of the HPV Vaccine. Front. Cell. Infect. Microbiol. 2019, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Centre for Research Excellence in Cervical Cancer Control. 2022 Cervical Cancer Elimination Progress Report. Available online: https://report.cervicalcancercontrol.org.au/ (accessed on 3 January 2023).
- Shing, J.Z.; Hu, S.; Herrero, R.; Hildesheim, A.; Porras, C.; Sampson, J.N.; Schussler, J.; Schiller, J.T.; Lowy, D.R.; Sierra, M.S.; et al. Precancerous cervical lesions caused by non-vaccine-preventable HPV types after vaccination with the bivalent AS04-adjuvanted HPV vaccine: An analysis of the long-term follow-up study from the randomised Costa Rica HPV Vaccine Trial. Lancet Oncol. 2022, 23, 940–949. [Google Scholar] [CrossRef]
- Chan, P.K.; Ho, W.C.; Chan, M.C.; Wong, M.C.; Yeung, A.C.; Chor, J.S.; Hui, M. Meta-analysis on prevalence and attribution of human papillomavirus types 52 and 58 in cervical neoplasia worldwide. PLoS ONE 2014, 9, e107573. [Google Scholar] [CrossRef] [PubMed]
- Quek, S.C.; Lim, B.K.; Domingo, E.; Soon, R.; Park, J.S.; Vu, T.N.; Tay, E.H.; Le, Q.T.; Kim, Y.T.; Vu, B.Q.; et al. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical intraepithelial neoplasia across 5 countries in Asia. Int. J. Gynecol. Cancer 2013, 23, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Chua, B.W.B.; Neo, P.; Ma, V.Y.; Lim, L.M.; Ng, J.S.Y.; Wee, H.L. Health care provider’s experience and perspective of cervical cancer screening in Singapore: A qualitative study. Front. Public Health 2022, 10, 853453. [Google Scholar] [CrossRef] [PubMed]
- Caro, J.J.; Maconachie, R.; Woods, M.; Naidoo, B.; McGuire, A. Leveraging DICE (Discretely-Integrated Condition Event) Simulation to Simplify the Design and Implementation of Hybrid Models. Value Health 2020, 23, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Caro, J.J. Discretely Integrated Condition Event (DICE) Simulation for Pharmacoeconomics. Pharmacoeconomics 2016, 34, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Kansal, A.R.; Reifsnider, O.S.; Brand, S.B.; Hawkins, N.; Coughlan, A.; Li, S.; Cragin, L.; Paramore, C.; Dietz, A.C.; Caro, J.J. Economic evaluation of betibeglogene autotemcel (Beti-cel) gene addition therapy in transfusion-dependent β-thalassemia. J. Mark. Access. Health Policy 2021, 9, 1922028. [Google Scholar] [CrossRef] [PubMed]
- Arlegui, H.; Nachbaur, G.; Praet, N.; Bégaud, B.; Caro, J.J. Using Discretely Integrated Condition Event Simulation to Construct Quantitative Benefit-Risk Models: The Example of Rotavirus Vaccination in France. Clin. Ther. 2020, 42, 1983–1991.e2. [Google Scholar] [CrossRef]
- Ganz, M.L.; Chavan, A.; Dhanda, R.; Serbin, M.; Yonan, C. Cost-effectiveness of valbenazine compared with deutetrabenazine for the treatment of tardive dyskinesia. J. Med. Econ. 2021, 24, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Ghabri, S.; Binard, A.; Pers, Y.M.; Maunoury, F.; Caro, J.J. Economic Evaluation of Sequences of Biological Treatments for Patients with Moderate-to-Severe Rheumatoid Arthritis and Inadequate Response or Intolerance to Methotrexate in France. Value Health 2020, 23, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Caro, J.J.; Möller, J.; Santhirapala, V.; Gill, H.; Johnston, J.; El-Boghdadly, K.; Santhirapala, R.; Kelly, P.; McGuire, A. Predicting Hospital Resource Use During COVID-19 Surges: A Simple but Flexible Discretely Integrated Condition Event Simulation of Individual Patient-Hospital Trajectories. Value Health 2021, 24, 1570–1577. [Google Scholar] [CrossRef]
- Department of Statistics Singapore. Singapore Residents by Age Group, Ethnic Group and Sex, End June. Available online: https://tablebuilder.singstat.gov.sg/table/TS/M810011 (accessed on 19 July 2022).
- Tay, S.K.; Lin, L.E.; Goh, R.C. Detection Rate of High-Grade Cervical Neoplasia and Cost-Effectiveness of High-Risk Human Papillomavirus Genotyping with Reflex Liquid-based Cytology in Cervical Cancer Screening. Ann. Acad. Med. Singap. 2017, 46, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. HPV School-Based Programme. Available online: https://www.moh.gov.sg/news-highlights/details/hpv-school-based-programme (accessed on 3 January 2023).
- Ministry of Health. National Population Health Survey 2019/20. Available online: https://www.moh.gov.sg/resources-statistics/reports/national-survey-2019-20 (accessed on 29 December 2022).
- Caro, J.J.; Briggs, A.H.; Siebert, U.; Kuntz, K.M. Modeling good research practices--overview: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force--1. Value Health 2012, 15, 796–803. [Google Scholar] [CrossRef]
- The Society for Colposcopy & Cervical Pathology of Singapore. Management Guidelines for Cervical Screening & Preinvasive Disease of the Cervix. Available online: https://www.sccps.org/wp-content/uploads/2019/03/CSS-Clinical-Mgt-Guidelines-2019_March-Release.pdf (accessed on 20 December 2022).
- Katki, H.A.; Schiffman, M.; Castle, P.E.; Fetterman, B.; Poitras, N.E.; Lorey, T.; Cheung, L.C.; Raine-Bennett, T.; Gage, J.C.; Kinney, W.K. Five-year risk of recurrence after treatment of CIN 2, CIN 3, or AIS: Performance of HPV and Pap cotesting in posttreatment management. J. Low Genit. Tract. Dis. 2013, 17, S78–S84. [Google Scholar] [CrossRef] [PubMed]
- Phua, L.C.; Choi, H.C.W.; Wu, J.; Jit, M.; Low, J.; Ng, K.; Pearce, F.; Hall, C.; Abdul Aziz, M.I. Cost-effectiveness analysis of the nonavalent human papillomavirus vaccine for the prevention of cervical cancer in Singapore. Vaccine 2021, 39, 2255–2263. [Google Scholar] [CrossRef]
- Organisation for Economic Co-Operation and Development. Purchasing Power Parities (PPP). Available online: https://data.oecd.org/conversion/purchasing-power-parities-ppp.htm (accessed on 14 January 2023).
- Insinga, R.P.; Glass, A.G.; Myers, E.R.; Rush, B.B. Abnormal outcomes following cervical cancer screening: Event duration and health utility loss. Med. Decis. Mak. 2007, 27, 414–422. [Google Scholar] [CrossRef]
- Myers, E.; Green, S.; Lipkus, I. Patient preferences for health states related to HPV infection: Visual analogue scales vs. time trade-off elicitation. In Proceedings of the 21st International Papillomavirus Conference, Mexico City, Mexico, 20–27 February 2004. [Google Scholar]
- Department of Statistics Singapore. Complete Life Tables for Singapore Resident Population, 2020–2021. Available online: https://www.singstat.gov.sg/publications/population/complete-life-table (accessed on 19 July 2022).
- Arndt, V.; Koch-Gallenkamp, L.; Jansen, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Schmid-Höpfner, S.; Waldmann, A.; Zeissig, S.R.; Brenner, H. Quality of life in long-term and very long-term cancer survivors versus population controls in Germany. Acta Oncol. 2017, 56, 190–197. [Google Scholar] [CrossRef]
- National Registry of Diseases Office. Singapore Cancer Registry: Cancer survival in Singapore 1973–2012. Available online: https://www.nrdo.gov.sg/docs/librariesprovider3/default-document-library/cancersurv_030915_final-w-appendices.pdf?sfvrsn=0 (accessed on 29 December 2022).
- Tay, S.K.; Oon, L.L. Prevalence of cervical human papillomavirus infection in healthy women is related to sexual behaviours and educational level: A cross-sectional study. Int. J. STD AIDS 2014, 25, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Nah, E.H.; Cho, S.; Kim, S.; Cho, H.I. Human Papillomavirus Genotype Distribution Among 18,815 Women in 13 Korean Cities and Relationship with Cervical Cytology Findings. Ann. Lab. Med. 2017, 37, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Loopik, D.L.; Bentley, H.A.; Eijgenraam, M.N.; IntHout, J.; Bekkers, R.L.M.; Bentley, J.R. The Natural History of Cervical Intraepithelial Neoplasia Grades 1, 2, and 3: A Systematic Review and Meta-analysis. J. Low Genit. Tract. Dis. 2021, 25, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Loopik, D.L.; Koenjer, L.M.; Siebers, A.G.; Melchers, W.J.G.; Bekkers, R.L.M. Benefit and burden in the Dutch cytology-based vs high-risk human papillomavirus-based cervical cancer screening program. Am. J. Obstet. Gynecol. 2021, 224, 200.e201–200.e209. [Google Scholar] [CrossRef]
- Jiang, W.; Austin, R.M.; Zhang, H.; He, Y.; Xu, L.; Wu, X.; Kuang, W.; Tong, L.; Li, L.; Zhao, C. The Clinical Utility of Extended High-Risk HPV Genotyping in Women with ASC-US Cytology. Am. J. Clin. Pathol. 2022, 158, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.; Dong, B.; Gao, H.; Mao, X.; Xue, H.; Sun, P. The Triage Effectiveness of an Extended High-Risk Human Papillomavirus Genotyping Assay for Women with Cytology Showing Atypical Squamous Cells of Undetermined Significance in China. Risk Manag. Healthc. Policy 2020, 13, 1747–1756. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Austin, R.M.; Yu, T.; Zhong, F.; Zhou, X.; Cong, Q.; Sui, L.; Zhao, C. Risk stratification for cervical neoplasia using extended high-risk HPV genotyping in women with ASC-US cytology: A large retrospective study from China. Cancer Cytopathol. 2022, 130, 248–258. [Google Scholar] [CrossRef]
- Stoler, M.H.; Wright, T.C., Jr.; Parvu, V.; Vaughan, L.; Yanson, K.; Eckert, K.; Karchmer, T.; Kodsi, S.; Cooper, C.K. The Onclarity Human Papillomavirus Trial: Design, methods, and baseline results. Gynecol. Oncol. 2018, 149, 498–505. [Google Scholar] [CrossRef]
- Gage, J.C.; Schiffman, M.; Solomon, D.; Wheeler, C.M.; Castle, P.E. Comparison of measurements of human papillomavirus persistence for postcolposcopic surveillance for cervical precancerous lesions. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1668–1674. [Google Scholar] [CrossRef]
- Castle, P.E.; Rodríguez, A.C.; Burk, R.D.; Herrero, R.; Wacholder, S.; Alfaro, M.; Morales, J.; Guillen, D.; Sherman, M.E.; Solomon, D.; et al. Short term persistence of human papillomavirus and risk of cervical precancer and cancer: Population based cohort study. Bmj 2009, 339, b2569. [Google Scholar] [CrossRef]
- Skinner, S.R.; Wheeler, C.M.; Romanowski, B.; Castellsagué, X.; Lazcano-Ponce, E.; Del Rosario-Raymundo, M.R.; Vallejos, C.; Minkina, G.; Pereira Da Silva, D.; McNeil, S.; et al. Progression of HPV infection to detectable cervical lesions or clearance in adult women: Analysis of the control arm of the VIVIANE study. Int. J. Cancer 2016, 138, 2428–2438. [Google Scholar] [CrossRef]
- Li, M.; Liu, T.; Luo, G.; Sun, X.; Hu, G.; Lu, Y.; Xu, R.H.; Zou, H.; Luo, X. Incidence, persistence and clearance of cervical human papillomavirus among women in Guangdong, China 2007-2018: A retrospective cohort study. J. Infect. Public Health 2021, 14, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Ouh, Y.T.; Park, J.J.; Kang, M.; Kim, M.; Song, J.Y.; Shin, S.J.; Shim, S.H.; Yoo, H.J.; Lee, M.; Lee, S.J.; et al. Discrepancy between Cytology and Histology in Cervical Cancer Screening: A Multicenter Retrospective Study (KGOG 1040). J. Korean Med. Sci. 2021, 36, e164. [Google Scholar] [CrossRef] [PubMed]
- National Registry of Diseases Office. Singapore Cancer Registry Report 2018. Available online: https://www.nrdo.gov.sg/docs/librariesprovider3/default-document-library/scr-annual-report-2018.pdf?sfvrsn=bcf56c25_0 (accessed on 29 December 2022).
- Kitchener, H.C.; Canfell, K.; Gilham, C.; Sargent, A.; Roberts, C.; Desai, M.; Peto, J. The clinical effectiveness and cost-effectiveness of primary human papillomavirus cervical screening in England: Extended follow-up of the ARTISTIC randomised trial cohort through three screening rounds. Health Technol. Assess. 2014, 18, 1–196. [Google Scholar] [CrossRef] [PubMed]
- Katki, H.A.; Gage, J.C.; Schiffman, M.; Castle, P.E.; Fetterman, B.; Poitras, N.E.; Lorey, T.; Cheung, L.C.; Raine-Bennett, T.; Kinney, W.K. Follow-up testing after colposcopy: Five-year risk of CIN 2+ after a colposcopic diagnosis of CIN 1 or less. J. Low Genit. Tract. Dis. 2013, 17, S69–S77. [Google Scholar] [CrossRef]
- Agency of Care Effectiveness. Medical Technologies Evaluation Methods and Process Guide. Available online: https://www.ace-hta.gov.sg/docs/default-source/process-methods/ace-med-tech-evaluation-methods-and-process-guide-(mar-2022).pdf (accessed on 29 December 2022).
- Department of Statistics Singapore. National Accounts. Available online: https://www.singstat.gov.sg/find-data/search-by-theme/economy/national-accounts/latest-data (accessed on 29 December 2022).
- Sousa, H.; Tavares, A.; Campos, C.; Marinho-Dias, J.; Brito, M.; Medeiros, R.; Baldaque, I.; Lobo, C.; Leça, L.; Monteiro, P.; et al. High-Risk human papillomavirus genotype distribution in the Northern region of Portugal: Data from regional cervical cancer screening program. Papillomavirus Res. 2019, 8, 100179. [Google Scholar] [CrossRef]
- Asti, L.; Hopley, C.; Avelis, C.; Bartsch, S.M.; Mueller, L.E.; Domino, M.; Cox, S.N.; Andrews, J.C.; Randall, S.L.; Stokes-Cawley, O.J.; et al. The Potential Clinical and Economic Value of a Human Papillomavirus Primary Screening Test That Additionally Identifies Genotypes 31, 45, 51, and 52 Individually. Sex Transm. Dis. 2021, 48, 370–380. [Google Scholar] [CrossRef]
- Thamsborg, L.H.; Napolitano, G.; Larsen, L.G.; Lynge, E. Impact of HPV vaccination on outcome of cervical cytology screening in Denmark-A register-based cohort study. Int. J. Cancer 2018, 143, 1662–1670. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Ploner, A.; Lehtinen, M.; Sparén, P.; Dillner, J.; Elfström, K.M. Impact of HPV vaccination on cervical screening performance: A population-based cohort study. Br. J. Cancer 2020, 123, 155–160. [Google Scholar] [CrossRef]
- Lukic, A.; De Vincenzo, R.; Ciavattini, A.; Ricci, C.; Senatori, R.; Ruscito, I.; Frega, A. Are We Facing a New Colposcopic Practice in the HPV Vaccination Era? Opportunities, Challenges, and New Perspectives. Vaccines 2021, 9, 1081. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Ma, X.; Li, H.; Li, B.; Wang, C.; Fan, X.; Fan, A.; Xue, F. Which is the best management for women with normal cervical cytologic findings despite positivity for non-16/18 high risk human papillomaviruses? Front. Public Health 2022, 10, 950610. [Google Scholar] [CrossRef]
- Kaushik, D. COVID-19 and health care workers burnout: A call for global action. EClinicalMedicine 2021, 35, 100808. [Google Scholar] [CrossRef]
- Singapore Business Federation. Uplifting Women in the Workforce: Investing in the Success of Women in Singapore. Available online: https://sustainable-employment.sbf.org.sg/wp-content/uploads/2021/12/Uplifting-Women-in-the-Workforce-Investing-in-the-Success-of-Women-in-Singapore.pdf (accessed on 26 January 2023).
- Heinonen, A.; Tapper, A.M.; Leminen, A.; Sintonen, H.; Roine, R.P. Health-related quality of life and perception of anxiety in women with abnormal cervical cytology referred for colposcopy: An observational study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 387–391. [Google Scholar] [CrossRef]
- Hellsten, C.; Lindqvist, P.G.; Sjöström, K. A longitudinal study of sexual functioning in women referred for colposcopy: A 2-year follow up. Bjog 2008, 115, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.M.; Iftner, T.; Cuschieri, K.; Kaufmann, A.M.; Arbyn, M.; de Sanjose, S.; Poljak, M.; Dillner, J.; Unger, E.R.; Stanley, M. IPVS policy statement on HPV nucleic acid testing guidance for those utilising/considering HPV as primary precancer screening: Quality Assurance and Quality Control issues. J. Clin. Virol. 2022, 159, 105349. [Google Scholar] [CrossRef] [PubMed]
- Piña-Sánchez, P. Human Papillomavirus: Challenges and Opportunities for the Control of Cervical Cancer. Arch. Med. Res. 2022, 53, 753–769. [Google Scholar] [CrossRef]
- Vorsters, A.; Bosch, F.X.; Poljak, M.; Waheed, D.E.; Stanley, M.; Garland, S.M. HPV prevention and control—The way forward. Prev. Med. 2022, 156, 106960. [Google Scholar] [CrossRef]
- Demarco, M.; Hyun, N.; Carter-Pokras, O.; Raine-Bennett, T.R.; Cheung, L.; Chen, X.; Hammer, A.; Campos, N.; Kinney, W.; Gage, J.C.; et al. A study of type-specific HPV natural history and implications for contemporary cervical cancer screening programs. EClinicalMedicine 2020, 22, 100293. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, M.; Gage, J.C.; Clifford, G.M.; Demarco, M.; Cheung, L.C.; Chen, Z.; Yeager, M.; Cullen, M.; Boland, J.F.; Chen, X.; et al. Association of HPV35 with cervical carcinogenesis among women of African ancestry: Evidence of viral-host interaction with implications for disease intervention. Int. J. Cancer 2020, 147, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Rohner, E.; Edelman, C.; Sanusi, B.; Schmitt, J.W.; Baker, A.; Chesko, K.; Faherty, B.; Gregory, S.M.; Romocki, L.S.; Sivaraman, V.; et al. Extended HPV Genotyping to Compare HPV Type Distribution in Self- and Provider-Collected Samples for Cervical Cancer Screening. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2651–2661. [Google Scholar] [CrossRef]
- Volesky, K.D.; Magnan, S.; Mayrand, M.H.; Isidean, S.D.; El-Zein, M.; Comète, E.; Franco, E.L.; Coutlée, F. Clinical Performance of the BD Onclarity Extended Genotyping Assay for the Management of Women Positive for Human Papillomavirus in Cervical Cancer Screening. Cancer Epidemiol. Biomark. Prev. 2022, 31, 851–857. [Google Scholar] [CrossRef]
- Ejegod, D.M.; Pedersen, H.; Pedersen, B.T.; Jonassen, C.M.; Lie, A.K.; Hulleberg, L.S.; Arbyn, M.; Bonde, J. Clinical Validation of the Onclarity Assay After Assay Migration to the High-Throughput COR Instrument Using SurePath Screening Samples from the Danish Cervical Cancer Screening Program. Am. J. Clin. Pathol. 2022, 157, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Bottari, F.; Iacobone, A.D.; Radice, D.; Preti, E.P.; Preti, M.; Franchi, D.; Boveri, S.; Sandri, M.T.; Passerini, R. HPV Tests Comparison in the Detection and Follow-Up after Surgical Treatment of CIN2+ Lesions. Diagnostics 2022, 12, 2359. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.B.; Guido, R.S.; Castle, P.E.; Chelmow, D.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Kim, J.J.; Moscicki, A.B.; Nayar, R.; et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J. Low Genit. Tract. Dis. 2020, 24, 102–131. [Google Scholar] [CrossRef]
- De Brot, L.; Pellegrini, B.; Moretti, S.T.; Carraro, D.M.; Soares, F.A.; Rocha, R.M.; Baiocchi, G.; da Cunha, I.W.; de Andrade, V.P. Infections with multiple high-risk HPV types are associated with high-grade and persistent low-grade intraepithelial lesions of the cervix. Cancer Cytopathol. 2017, 125, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Pista, A.; Oliveira, A.; Verdasca, N.; Ribeiro, F. Single and multiple human papillomavirus infections in cervical abnormalities in Portuguese women. Clin. Microbiol. Infect. 2011, 17, 941–946. [Google Scholar] [CrossRef]



| Outcomes | PGT | XGT | Incremental |
|---|---|---|---|
| Cancers treated | 106 | 98 | −8 |
| CIN2/3 treated | 3993 | 3701 | −292 |
| CIN2+ treated | 4099 | 3799 | −300 |
| Colposcopies conducted | 36,809 | 29,679 | −7130 |
| HPV tests conducted | 540,799 | 543,245 | 2446 |
| Cytology conducted | 86,419 | 80,392 | −6027 |
| Clinic consultations | 601,796 | 592,009 | −9787 |
| Cost of HPV tests | SGD 62,106,581 (USD 73,848,491) | SGD 71,753,834 (USD 85,319,660) | SGD 9,647,253 (USD 11,471,169) |
| Cost of cytology | SGD 5,953,061 (USD 7,078,551) | SGD 5,658,456 (USD 6,728,247) | −SGD 294,605 (−USD 350,303) |
| Cost of colposcopy | SGD 14,259,917 (USD 16,955,906) | SGD 11,486,606 (USD 13,658,271) | −SGD 2,773,311 (−USD 3,297,635) |
| Cost of clinic consultation | SGD 45,038,254 (USD 53,553,215) | SGD 44,310,726 (USD 52,688,140) | −SGD 727,528 (−USD 865,075) |
| Total cost | SGD 145,904,751 (USD 173,489,597) | SGD 150,396,871 (USD 178,831,000) | SGD 4,492,120 (USD 5,341,403) |
| Total QALY loss | −6528.3 | −6253.88 | 274.42 |
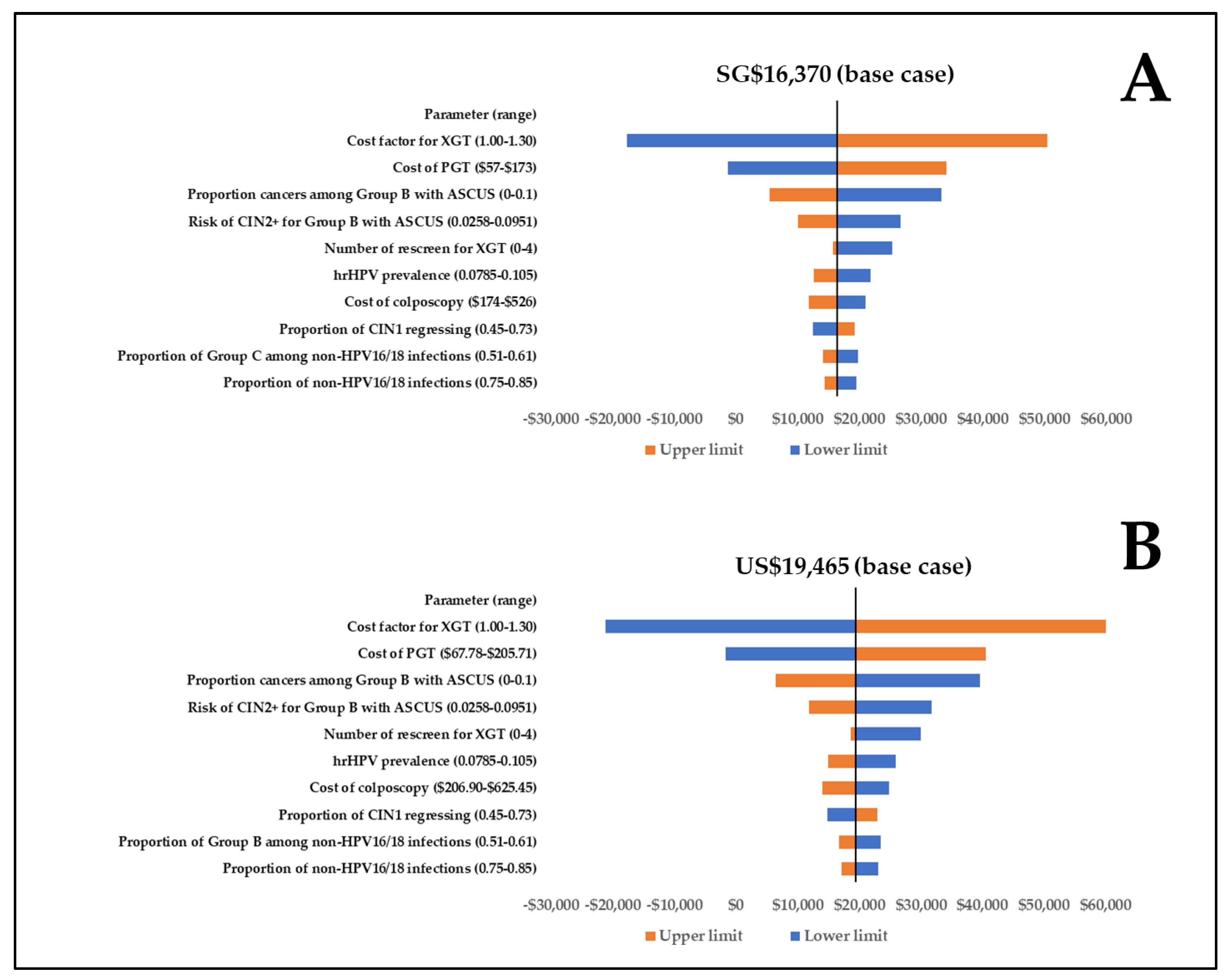
| ICER | - | - | SGD 16,370/QALY (USD 19,465/QALY) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chua, B.; Lim, L.M.; Ng, J.S.Y.; Ma, Y.; Wee, H.L.; Caro, J.J. Cost-Effectiveness Analysis of HPV Extended versus Partial Genotyping for Cervical Cancer Screening in Singapore. Cancers 2023, 15, 1812. https://doi.org/10.3390/cancers15061812
Chua B, Lim LM, Ng JSY, Ma Y, Wee HL, Caro JJ. Cost-Effectiveness Analysis of HPV Extended versus Partial Genotyping for Cervical Cancer Screening in Singapore. Cancers. 2023; 15(6):1812. https://doi.org/10.3390/cancers15061812
Chicago/Turabian StyleChua, Brandon, Li Min Lim, Joseph Soon Yau Ng, Yan Ma, Hwee Lin Wee, and J. Jaime Caro. 2023. "Cost-Effectiveness Analysis of HPV Extended versus Partial Genotyping for Cervical Cancer Screening in Singapore" Cancers 15, no. 6: 1812. https://doi.org/10.3390/cancers15061812
APA StyleChua, B., Lim, L. M., Ng, J. S. Y., Ma, Y., Wee, H. L., & Caro, J. J. (2023). Cost-Effectiveness Analysis of HPV Extended versus Partial Genotyping for Cervical Cancer Screening in Singapore. Cancers, 15(6), 1812. https://doi.org/10.3390/cancers15061812