
Age-Stratified Analysis of First-Line Chemoimmunotherapy for Extensive-Stage Small Cell Lung Cancer: Real-World Evidence from a Multicenter Retrospective Study

 , , , , , , and
, , , , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment with First-Line Chemoimmunotherapy and Response Evaluation
2.3. Data Collection
2.4. Study Variables
2.5. Statistical Analysis
3. Results
3.1. Patient Selection Diagram (Figure 1) and the Characteristics of Patients Treated with Platinum Doublet Chemotherapy (Table 1)
3.2. Characteristics of Patients Treated with Chemoimmunotherapy (Table 2)
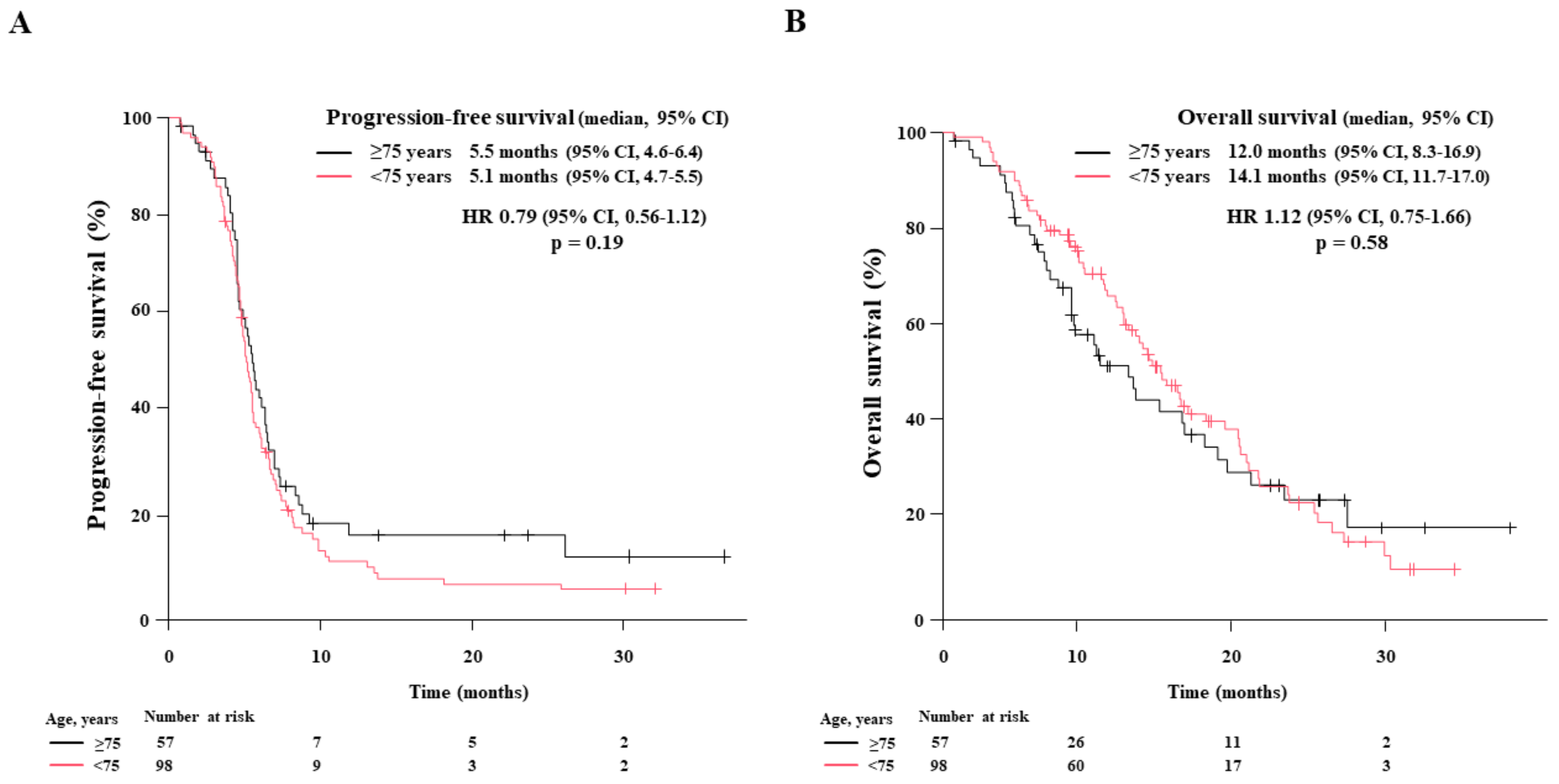
3.3. Objective Response Rate, Progression-Free Survival, and Overall Survival Outcomes (Figure 2 and Figure 3)
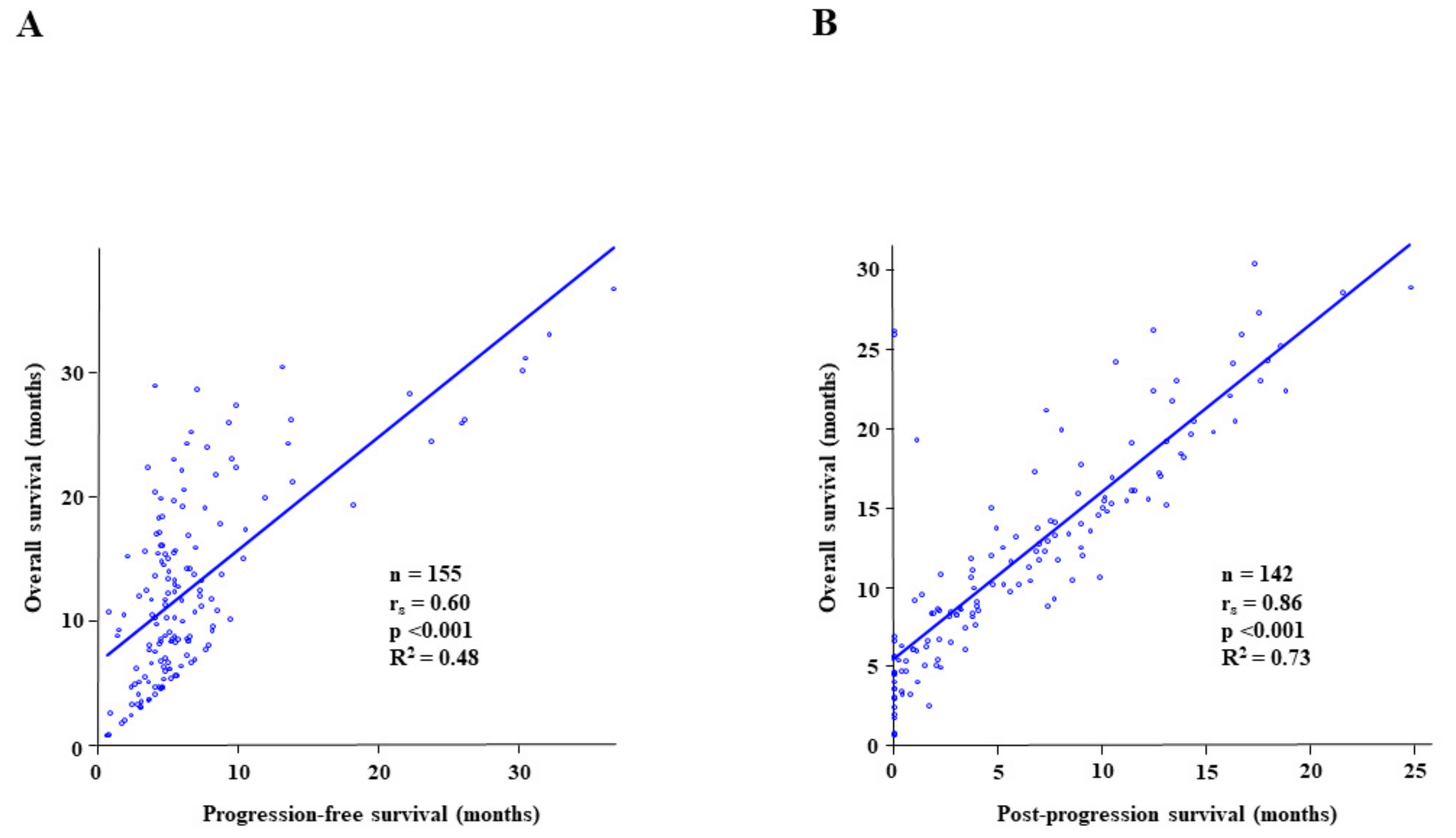
3.4. Relationship between Overall Survival and Progression-Free Survival or Post-Progression Survival after First-Line Chemoimmunotherapy (Figure 4)
3.5. Adverse Events and Dose Reduction during Induction Therapy
3.6. Relationship between the Baseline Characteristics or Candidate Predictive Biomarkers and Progression-Free Survival or Overall Survival among 155 Patients (Table 3), Elderly Patients Aged ≥ 75 (Table 4), and Non-Elderly Patients < 75 Years (Table 5)
3.7. Relationship between Eastern Cooperative Oncology Group Performance Status at Disease Progression or at Second-Line Therapy Initiation and the Post-Progression Survival after First-Line Chemoimmunotherapy (Figure 5)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Farago, A.F.; Keane, F.K. Current standards for clinical management of small cell lung cancer. Transl. Lung Cancer Res. 2018, 7, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, M.; Furuse, K.; Saijo, N.; Nishiwaki, Y.; Ikegami, H.; Tamura, T.; Shimoyama, M.; Suemasu, K. Randomized trial of cyclophosphamide, doxorubicin, and vincristine versus cisplatin and etoposide versus alternation of these regimens in small-cell lung cancer. J. Natl. Cancer Inst. 1991, 83, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Noda, K.; Nishiwaki, Y.; Kawahara, M.; Negoro, S.; Sugiura, T.; Yokoyama, A.; Fukuoka, M.; Mori, K.; Watanabe, K.; Tamura, T.; et al. Irinotecan plus cisplatin compared with etoposide plus cisplatin for extensive small-cell lung cancer. N. Engl. J. Med. 2002, 346, 85–91. [Google Scholar] [CrossRef]
- Hanna, N.; Bunn, P.A.; Langer, C.; Einhorn, L.; Guthrie, T., Jr.; Beck, T.; Ansari, R.; Ellis, P.; Byrne, M.; Morrison, M.; et al. Randomized phase III trial comparing irinotecan/cisplatin with etoposide/cisplatin in patients with previously untreated extensive-stage disease small-cell lung cancer. J. Clin. Oncol. 2006, 24, 2038–2043. [Google Scholar] [CrossRef]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H.; et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): A randomised, controlled, open-label, phase 3 trial. Lancet 2019, 394, 1929–1939. [Google Scholar] [CrossRef]
- Rao, A.; Sharma, N.; Gajra, A. Management of Lung Cancer in the Elderly. Cancer Treat. Res. 2016, 170, 251–284. [Google Scholar] [CrossRef]
- National Cancer Institute. SEER Cancer Stat Facts: Lung and Bronchus Cancer. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 20 December 2022).
- Cabinet Office, Government of Japan. Current Status of Aging Population. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2020/html/gaiyou/s1_1.html (accessed on 20 December 2022).
- National Cancer Center Japan Statistical Data about Cancer. Available online: http://ganjoho.jp/reg_stat/statistics/dl/index.html (accessed on 20 December 2022).
- Morimoto, K.; Yamada, T.; Takeda, T.; Shiotsu, S.; Date, K.; Harada, T.; Tamiya, N.; Chihara, Y.; Hiranuma, O.; Yamada, T.; et al. Efficacy and safety of programmed death-ligand 1 inhibitor plus platinum-etoposide chemotherapy in patients with extensive-stage SCLC: A prospective observational study. JTO Clin. Res. Rep. 2022, 3, 100353. [Google Scholar] [CrossRef]
- Ferrara, R.; Mezquita, L.; Auclin, E.; Chaput, N.; Besse, B. Immunosenescence and immunecheckpoint inhibitors in non-small cell lung cancer patients: Does age really matter. Cancer Treat. Rev. 2017, 60, 60–68. [Google Scholar] [CrossRef]
- Takigawa, N.; Ochi, N.; Nakagawa, N.; Nagasaki, Y.; Taoka, M.; Ichiyama, N.; Mimura, A.; Nakanishi, H.; Kohara, H.; Yamane, H. Do elderly lung cancer patients aged ≥ 75 years benefit from immune checkpoint inhibitors. Cancers 2020, 12, 1995. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; Gross, S.; Kirchberger, M.C.; Erdmann, M.; Schuler, G.; Heinzerling, L. Senescence markers: Predictive for response to checkpoint inhibitors. Int. J. Cancer 2019, 144, 1147–1150. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.X.; Xiang, Y.; Zhao, S.; Chen, J. Assessment of systematic inflammatory and nutritional indexes in extensive-stage small-cell lung cancer treated with first-line chemotherapy and atezolizumab. Cancer Immunol. Immunother. 2021, 70, 3199–3206. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Jiang, J.; Ren, C. The clinicopathological and prognostic value of the pretreatment neutrophil-to-lymphocyte ratio in small cell lung cancer: A meta-analysis. PLoS ONE 2020, 15, e0230979. [Google Scholar] [CrossRef]
- Drpa, G.; Sutic, M.; Baranasic, J.; Jakopovic, M.; Samarzija, M.; Kukulj, S.; Knezevic, J. Neutrophil-to-lymphocyte ratio can predict outcome in extensive-stage small cell lung cancer. Radiol. Oncol. 2020, 54, 437–446. [Google Scholar] [CrossRef]
- Jiang, A.M.; Zhao, R.; Liu, N.; Ma, Y.Y.; Ren, M.D.; Tian, T.; Yao, Y. The prognostic value of pretreatment prognostic nutritional index in patients with small cell lung cancer and it’s influencing factors: A meta-analysis of observational studies. J. Thorac. Dis. 2020, 12, 5718–5728. [Google Scholar] [CrossRef]
- Wang, C.; Jin, S.; Xu, S.; Cao, S. The combination of pretreatment prognostic nutritional index and neuron-specific enolase enhances prognosis predicting value of small cell lung cancer. Clin. Respir. J. 2021, 15, 264–271. [Google Scholar] [CrossRef]
- Hong, X.; Cui, B.; Wang, M.; Yang, Z.; Wang, L.; Xu, Q. Systemic Immune-inflammation Index, Based on Platelet Counts and Neutrophil-Lymphocyte Ratio, Is Useful for Predicting Prognosis in Small Cell Lung Cancer. Tohoku J. Exp. Med. 2015, 236, 297–304. [Google Scholar] [CrossRef]
- Ozyurek, B.A.; Ozdemirel, T.S.; Ozden, S.B.; Erdogan, Y.; Kaplan, B.; Kaplan, T. Prognostic Value of the Neutrophil to Lymphocyte Ratio (NLR) in Lung Cancer Cases. Asian Pac. J. Cancer Prev. 2017, 18, 1417–1421. [Google Scholar] [CrossRef]
- Masubuchi, K.; Imai, H.; Wasamoto, S.; Tsuda, T.; Minemura, H.; Nagai, Y.; Yamada, Y.; Kishikawa, T.; Umeda, Y.; Shiono, A.; et al. Post-progression survival after atezolizumab plus carboplatin and etoposide as first-line chemotherapy in small cell lung cancer has a significant impact on overall survival. Thorac. Cancer 2022, 13, 2776–2785. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1-Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wu, Y.; Wang, Z.; Yao, Y.; Chen, F.; Zhang, H.; Wang, Y.; Song, Y. Pretreatment platelet-to-lymphocyte ratio (PLR) as a predictor of response to first-line platinum-based chemotherapy and prognosis for patients with non-small cell lung cancer. J. Thorac. Dis. 2013, 5, 783–789. [Google Scholar] [CrossRef]
- Ogura, Y.; Kataoka, N.; Kunimatsu, Y.; Tachibana, Y.; Sugimoto, T.; Tani, N.; Sato, I.; Hirose, K.; Kato, D.; Takeda, T. Predictors of survival among Japanese patients receiving first-line chemoimmunotherapy for advanced non-small cell lung cancer. Thorac. Cancer 2021, 12, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Sharaiha, R.Z.; Halazun, K.J.; Mirza, F.; Port, J.L.; Lee, P.C.; Neugut, A.I.; Altorki, N.K.; Abrams, J.A. Elevated preoperative neutrophil: Lymphocyte ratio as a predictor of postoperative disease recurrence in esophageal cancer. Ann. Surg. Oncol. 2011, 18, 3362–3369. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Chan, S.L.; Wong, G.L.; Wong, V.W.; Chong, C.C.; Lai, P.B.; Chan, H.L.; To, K.F. Prognostic nutritional index (PNI) predicts tumor recurrence of very early/early stage hepatocellular carcinoma after surgical resection. Ann. Surg. Oncol. 2015, 22, 4138–4148. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Deng, C.; Zhang, N.; Wang, Y.; Jiang, S.; Lu, M.; Huang, Y.; Ma, J.; Hu, C.; Hou, T. High systemic immune-inflammation index predicts poor prognosis in advanced lung adenocarcinoma patients treated with EGFR-TKIs. Medicine 2019, 98, e16875. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Langer, C.J.; Manola, J.; Bernardo, P.; Kugler, J.W.; Bonomi, P.; Cella, D.; Johnson, D.H. Cisplatin-based therapy for elderly patients with advanced non-small-cell lung cancer: Implications of Eastern Cooperative Oncology Group 5592, a randomized trial. J. Natl. Cancer Inst. 2002, 94, 173–181. [Google Scholar] [CrossRef]
- Hensing, T.A.; Peterman, A.H.; Schell, M.J.; Lee, J.H.; Socinski, M.A. The impact of age on toxicity, response rate, quality of life, and survival in patients with advanced, Stage IIIB or IV nonsmall cell lung carcinoma treated with carboplatin and paclitaxel. Cancer 2003, 98, 779–788. [Google Scholar] [CrossRef]
- Belani, C.P.; Fossella, F. Elderly subgroup analysis of a randomized phase III study of docetaxel plus platinum combinations versus vinorelbine plus cisplatin for first-line treatment of advanced nonsmall cell lung carcinoma (TAX 326). Cancer 2005, 104, 2766–2774. [Google Scholar] [CrossRef] [PubMed]
- Ansari, R.H.; Socinski, M.A.; Edelman, M.J.; Belani, C.P.; Gonin, R.; Catalano, R.B.; Marinucci, D.M.; Comis, R.L.; Obasaju, C.K.; Chen, R.; et al. Alpha Oncology Research Network. A retrospective analysis of outcomes by age in a three-arm phase III trial of gemcitabine in combination with carboplatin or paclitaxel vs. paclitaxel plus carboplatin for advanced non-small cell lung cancer. Crit. Rev. Oncol. Hematol. 2011, 78, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Soubeyran, P.; Fonck, M.; Blanc-Bisson, C.; Blanc, J.F.; Ceccaldi, J.; Mertens, C.; Imbert, Y.; Cany, L.; Vogt, L.; Dauba, J.; et al. Predictors of early death risk in older patients treated with first-line chemotherapy for cancer. J. Clin. Oncol. 2012, 30, 1829–1834. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, S.; Rainfray, M.; Fonck, M.; Hoppenreys, L.; Blanc, J.F.; Ceccaldi, J.; Mertens, C.; Blanc-Bisson, C.; Imbert, Y.; Cany, L.; et al. Functional decline in older patients with cancer receiving first-line chemotherapy. J. Clin. Oncol. 2013, 31, 3877–3882. [Google Scholar] [CrossRef]
- Kenis, C.; Decoster, L.; Bastin, J.; Bode, H.; Van Puyvelde, K.; De Grève, J.; Conings, G.; Fagard, K.; Flamaing, J.; Milisen, K.; et al. Functional decline in older patients with cancer receiving chemotherapy: A multicenter prospective study. J. Geriatr. Oncol. 2017, 8, 196–205. [Google Scholar] [CrossRef]
- Decoster, L.; Kenis, C.; Schallier, D.; Vansteenkiste, J.; Nackaerts, K.; Vanacker, L.; Vandewalle, N.; Flamaing, J.; Lobelle, J.P.; Milisen, K.; et al. Geriatric Assessment and Functional Decline in Older Patients with Lung Cancer. Lung 2017, 195, 619–626. [Google Scholar] [CrossRef]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting chemotherapy toxicity in older adults with cancer: A prospective multicenter study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.S.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical assessment and management of vulnerabilities in older patients receiving chemotherapy: ASCO guideline for geriatric oncology. J. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef]
- Mohile, S.G.; Mohamed, M.R.; Xu, H.; Culakova, E.; Loh, K.P.; Magnuson, A.; Flannery, M.A.; Obrecht, S.; Gilmore, N.; Ramsdale, E.; et al. Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): A cluster-randomised study. Lancet 2021, 398, 1894–1904. [Google Scholar] [CrossRef] [PubMed]
- Rudin, C.M.; Awad, M.M.; Navarro, A.; Gottfried, M.; Peters, S.; Csőszi, T.; Cheema, P.K.; Rodriguez-Abreu, D.; Wollner, M.; Yang, J.C.; et al. Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung cancer: Randomized, double-blind, phase III KEYNOTE-604 study. J. Clin. Oncol. 2020, 38, 2369–2379. [Google Scholar] [CrossRef]
- Mansfield, A.S.; Każarnowicz, A.; Karaseva, N.; Sánchez, A.; De Boer, R.; Andric, Z.; Reck, M.; Atagi, S.; Lee, J.S.; Garassino, M.; et al. Safety and patient-reported outcomes of atezolizumab, carboplatin, and etoposide in extensive-stage small-cell lung cancer (IMpower133): A randomized phase I/III trial. Ann. Oncol. 2020, 31, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.W.; Garassino, M.C.; Chen, Y.; Özgüroğlu, M.; Dvorkin, M.; Trukhin, D.; Statsenko, G.; Hotta, K.; Ji, J.H.; Hochmair, M.J.; et al. Patient-reported outcomes with first-line durvalumab plus platinum-etoposide versus platinum-etoposide in extensive-stage small-cell lung cancer (CASPIAN): A randomized, controlled, open-label, phase III study. Lung Cancer 2020, 149, 46–52. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, D.E.; Cheung, W.Y.; Syed, I.A.; Moldaver, D.; Shanahan, M.K.; Bebb, D.G.; Sit, C.; Brenner, D.R.; Boyne, D.J. Real-world treatment patterns, clinical outcomes, and health care resource utilization in extensive-stage small cell lung cancer in Canada. Curr. Oncol. 2021, 28, 3091–3103. [Google Scholar] [CrossRef] [PubMed]
- Elegbede, A.A.; Gibson, A.J.; Fung, A.S.; Cheung, W.Y.; Dean, M.L.; Bebb, D.G.; Pabani, A. A real-world evaluation of atezolizumab plus platinum-etoposide chemotherapy in patients with extensive-stage SCLC in Canada. JTO Clin. Res. Rep. 2021, 2, 100249. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total: n = 70 | Non-Elderly Patients (<75 Years): n = 26 | Elderly Patients (≥75 Years): n = 44 | p-Value |
|---|---|---|---|---|
| Sex: male/female | 53 (75.7%)/17 (24.3%) | 16 (61.5%)/10 (38.5%) | 37 (84.1%)/7 (15.9%) | 0.05 |
| Age (years): median (range) | 76 (61–86) | 70 (61–73) | 78 (75–86) | N/A |
| ECOG-PS: 0/1/2/3/4 | 7 (10.0%)/40 (57.1%)/11 (15.7%)/12 (17.1%)/0 | 3 (11.5%)/13 (50.0%)/2 (7.7%)/8 (30.8%)/0 | 4 (9.1%)/27 (61.4%)/9 (20.5%)/4 (9.1%)/0 | 0.09 |
| Regimen | ||||
| CBDCA + etoposide | 64 (91.4%) | 20 (76.9%) | 44 (100%) | 0.002 |
| CDDP + etoposide | 3 (4.3%) | 3 (11.5%) | 0 | 0.04 |
| CDDP + irinotecan | 3 (4.3%) | 3 (11.5%) | 0 | 0.04 |
| Reasons for adopting chemotherapy | ||||
| Patient’s preference | 5 (7.1%) | 5 (19.2%) | 0 | 0.005 |
| Interstitial lung disease | 33 (47.1%) | 11 (42.3%) | 22 (50.0%) | 0.62 |
| Poor ECOG-PS | 13 (18.6%) | 6 (23.1%) | 7 (15.9%) | 0.53 |
| Age | 8 (11.4%) | 1 (3.8%) | 7 (15.9%) | 0.24 |
| Rheumatoid arthritis | 2 (2.9%) | 2 (7.7%) | 0 | 0.14 |
| IgA nephritis | 1 (1.4%) | 1 (3.8%) | 0 | 0.37 |
| Dermatomyositis | 1 (1.4%) | 0 | 1 (2.3%) | 1.00 |
| Congestive heart failure | 3 (4.3%) | 0 | 3 (6.8%) | 0.29 |
| Sick sinus syndrome | 1 (1.4%) | 0 | 1 (2.3%) | 1.00 |
| Cognitive impairment | 1 (1.4%) | 0 | 1 (2.3%) | 1.00 |
| Liver dysfunction | 1 (1.4%) | 0 | 1 (2.3%) | 1.00 |
| Renal dysfunction | 1 (1.4%) | 0 | 1 (2.3%) | 1.00 |
| Characteristics | Total: n = 155 | Non-Elderly Patients (<75 Years): n = 98 | Elderly Patients (≥75 Years): n = 57 | p-Value |
|---|---|---|---|---|
| Sex: male/female | 125 (80.6%)/30 (19.4%) | 74 (75.5%)/24 (24.5%) | 51 (89.5%)/6 (10.5%) | 0.04 |
| Age (years): median (range) | 72 (43–87) | 69 (43–74) | 79 (75–87) | |
| ECOG-PS: 0/1/2/3/4 | 39 (25.2%)/94 (60.6%)/17 (11.0%)/5 (3.2%)/0 | 32 (32.7%)/52 (53.1%)/11 (11.2%)/3 (3.1%)/0 | 7 (12.3%)/42 (73.7%)/6 (10.5%)/2 (3.5%)/0 | 0.03 |
| Smoking: current/former/never | 54 (34.8%)/96 (61.9%)/5 (3.2%) | 38 (38.8%)/55 (56.1%)/5 (5.1%) | 16 (28.1%)/41 (71.9%)/0 | 0.04 |
| Stage: III/IVA/IVB/recurrence | 9 (5.8%)/40 (25.8%)/103 (66.5%)/3 (1.9%) | 5 (5.1%)/22 (22.4%)/68 (69.4%)/3 (3.1%) | 4 (7.0%)/18 (31.6%)/35 (61.4%)/0 | 0.35 |
| Brain metastasis at baseline: (+)/(—) | 33 (21.3%)/122 (78.7%) | 25 (25.5%)/73 (74.5%) | 8 (14.0%)/49 (86.0%) | 0.11 |
| Liver metastasis at baseline: (+)/(—) | 37 (23.9%)/118 (76.1%) | 24 (24.5%)/74 (75.5%) | 13 (22.8%)/44 (77.2%) | 0.85 |
| ILD at baseline: (+)/(—) | 6 (3.9%)/149 (96.1%) | 2 (2.0%)/96 (98.0%) | 4 (7.0%)/53 (93.0%) | 0.19 |
| Autoimmune disease: (+)/(—) | 2 (1.3%)/153 (98.7%) | 1 (1.0%)/97 (99.0%) | 1 (1.8%)/56 (98.2%) | 1.00 |
| Steroid treatment at baseline: (+)/(—) | 7 (4.5%)/148 (95.5%) | 7 (7.1%)/91 (92.9%) | 0/57 (100%) | 0.04 |
| Cycles of induction: 1–2/3/4/5–6 | 13 (8.4%)/13 (8.4%)/126 (81.3%)/3 (1.9%) | 4 (4.1%)/9 (9.2%)/83 (84.7%)/2 (2.0%) | 9 (15.8%)/4 (7.0%)/43 (75.4%)/1 (1.8%) | 0.08 |
| Reduced dose at 1st cycle: (+)/(—) | 45 (29.0%)/110 (71.0%) | 20 (20.4%)/78 (79.6%) | 25 (43.9%)/32 (56.1%) | 0.003 |
| Dose reduction during Tx.: (+)/(—) | 62 (40.0%)/93 (60.0%) | 35 (35.7%)/63 (64.3%) | 27 (47.4%)/30 (52.6%) | 0.18 |
| G-CSF during induction Tx.: (+)/(—) | 91 (58.7%)/64 (41.3%) | 58 (59.2%)/40 (40.8%) | 33 (57.9%)/24 (42.1%) | 1.00 |
| Reason for discontinuation of 1st-line | ||||
| Disease progression | 112 (72.3%) | 80 (81.6%) | 32 (56.1%) | <0.001 |
| Adverse events | 3 (1.9%) | 1 (1.0%) | 2 (3.5%) | 0.55 |
| Immune-related adverse events | 9 (5.8%) | 5 (5.1%) | 4 (7.0%) | 0.73 |
| Others | 18 (11.6%) | 5 (5.1%) | 13 (22.8%) | 0.001 |
| Ongoing Tx. | 13 (8.4%) | 7 (7.1%) | 6 (10.5%) | 0.55 |
| 2nd-line Tx.: (+)/(—)/on 1st-line Tx. | 99 (63.9%)/43 (27.7%)/13 (8.4%) | 70 (71.4%)/21 (21.4%)/7 (7.1%) | 29 (50.9%)/22 (38.6%)/6 (10.5%) | 0.04 |
| Progression-Free Survival | Overall Survival | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||||
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age (<75/≥75) | 0.79 | 0.56–1.12 | 0.19 | 0.81 | 0.55–1.19 | 0.28 | 1.12 | 0.75–1.66 | 0.58 | 1.18 | 0.76–1.84 | 0.47 |
| Sex (female/male) | 1.25 | 0.82–1.90 | 0.31 | 1.18 | 0.73–1.91 | 0.49 | 1.23 | 0.73–2.06 | 0.45 | 1.05 | 0.60–1.85 | 0.86 |
| Smoking (—/+) | 1.21 | 0.49–2.95 | 0.68 | 1.53 | 0.50–4.72 | 0.45 | 1.68 | 0.61–4.59 | 0.31 | 1.92 | 0.58–6.34 | 0.29 |
| ECOG-PS (<2/≥2) | 0.94 | 0.58–1.54 | 0.82 | 0.75 | 0.42–1.32 | 0.32 | 0.43 | 0.25–0.74 | 0.002 | 0.55 | 0.30–1.03 | 0.06 |
| Reduced dose at 1st cycle (—/+) | 1.04 | 0.71–1.51 | 0.84 | 0.94 | 0.63–1.39 | 0.75 | 1.21 | 0.79–1.85 | 0.39 | 0.97 | 0.62–1.54 | 0.90 |
| Cycles of induction (≥4/<4) | 0.38 | 0.25–0.59 | <0.001 | 0.45 | 0.27–0.73 | 0.001 | 0.30 | 0.19–0.49 | <0.001 | 0.31 | 0.18–0.54 | <0.001 |
| PLR (<250/≥250) | 0.92 | 0.65–1.30 | 0.62 | 0.88 | 0.59–1.32 | 0.55 | ||||||
| NLR (<5/≥5) | 0.72 | 0.50–1.02 | 0.07 | 0.84 | 0.55–1.30 | 0.44 | 0.65 | 0.43–0.98 | 0.04 | 0.96 | 0.58–1.58 | 0.84 |
| PNI (≥40/<40) | 0.64 | 0.45–0.92 | 0.02 | 0.70 | 0.46–1.07 | 0.10 | 0.38 | 0.25–0.57 | <0.001 | 0.36 | 0.22–0.59 | <0.001 |
| SII (<1000/≥1000) | 0.77 | 0.55–1.08 | 0.13 | 0.89 | 0.61–1.30 | 0.55 | ||||||
| Univariate Analysis (≥75 Years) | ||||||
|---|---|---|---|---|---|---|
| Progression-Free Survival | Overall Survival | |||||
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Sex (female/male) | 1.24 | 0.49–3.14 | 0.65 | 1.68 | 0.51–5.47 | 0.39 |
| ECOG-PS (<2/≥2) | 0.79 | 0.35–1.78 | 0.57 | 0.38 | 0.16–0.90 | 0.03 |
| Reduced dose at 1st cycle (—/+) | 1.06 | 0.60–1.87 | 0.85 | 1.07 | 0.56–2.05 | 0.84 |
| Cycles of induction (≥4/<4) | 0.35 | 0.18–0.69 | 0.003 | 0.25 | 0.12–0.52 | <0.001 |
| PLR (<250/≥250) | 0.92 | 0.51–1.68 | 0.79 | 0.87 | 0.44–1.71 | 0.68 |
| NLR (<5/≥5) | 0.59 | 0.32–1.09 | 0.09 | 0.40 | 0.20–0.82 | 0.01 |
| PNI (≥40/<40) | 0.58 | 0.32–1.05 | 0.07 | 0.28 | 0.14–0.55 | <0.001 |
| SII (<1000/≥1000) | 0.93 | 0.52–1.65 | 0.79 | 0.84 | 0.44–1.59 | 0.59 |
| Univariate Analysis (<75 Years) | ||||||
|---|---|---|---|---|---|---|
| Progression-Free Survival | Overall Survival | |||||
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Sex (female/male) | 1.29 | 0.80–2.09 | 0.30 | 1.05 | 0.58–1.90 | 0.88 |
| ECOG-PS (<2/≥2) | 1.28 | 0.70–2.35 | 0.43 | 0.48 | 0.24–0.96 | 0.03 |
| Reduced dose at 1st cycle (-/+) | 0.99 | 0.57–1.71 | 0.98 | 1.26 | 0.68–2.33 | 0.46 |
| Cycles of induction (≥4/<4) | 0.41 | 0.23–0.75 | 0.003 | 0.37 | 0.20–0.70 | 0.002 |
| PLR (<250/≥250) | 1.18 | 0.76–1.81 | 0.46 | 0.91 | 0.55–1.49 | 0.70 |
| NLR (<5/≥5) | 0.80 | 0.51–1.24 | 0.32 | 0.83 | 0.50–1.39 | 0.48 |
| PNI (≥40/<40) | 0.77 | 0.49–1.19 | 0.24 | 0.45 | 0.27–0.76 | 0.002 |
| SII (<1000/≥1000) | 1.48 | 0.97–2.27 | 0.07 | 1.36 | 0.84–2.21 | 0.21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeda, T.; Yamada, T.; Kunimatsu, Y.; Tanimura, K.; Morimoto, K.; Shiotsu, S.; Chihara, Y.; Okada, A.; Horiuchi, S.; Hibino, M.; et al. Age-Stratified Analysis of First-Line Chemoimmunotherapy for Extensive-Stage Small Cell Lung Cancer: Real-World Evidence from a Multicenter Retrospective Study. Cancers 2023, 15, 1543. https://doi.org/10.3390/cancers15051543
Takeda T, Yamada T, Kunimatsu Y, Tanimura K, Morimoto K, Shiotsu S, Chihara Y, Okada A, Horiuchi S, Hibino M, et al. Age-Stratified Analysis of First-Line Chemoimmunotherapy for Extensive-Stage Small Cell Lung Cancer: Real-World Evidence from a Multicenter Retrospective Study. Cancers. 2023; 15(5):1543. https://doi.org/10.3390/cancers15051543
Chicago/Turabian StyleTakeda, Takayuki, Tadaaki Yamada, Yusuke Kunimatsu, Keiko Tanimura, Kenji Morimoto, Shinsuke Shiotsu, Yusuke Chihara, Asuka Okada, Shigeto Horiuchi, Makoto Hibino, and et al. 2023. "Age-Stratified Analysis of First-Line Chemoimmunotherapy for Extensive-Stage Small Cell Lung Cancer: Real-World Evidence from a Multicenter Retrospective Study" Cancers 15, no. 5: 1543. https://doi.org/10.3390/cancers15051543
APA StyleTakeda, T., Yamada, T., Kunimatsu, Y., Tanimura, K., Morimoto, K., Shiotsu, S., Chihara, Y., Okada, A., Horiuchi, S., Hibino, M., Uryu, K., Honda, R., Yamanaka, Y., Yoshioka, H., Kurata, T., & Takayama, K. (2023). Age-Stratified Analysis of First-Line Chemoimmunotherapy for Extensive-Stage Small Cell Lung Cancer: Real-World Evidence from a Multicenter Retrospective Study. Cancers, 15(5), 1543. https://doi.org/10.3390/cancers15051543